
5.1 Strategic Framework - NHS Highland...3 3 STRATEGIC FRAMEWORK 2011/12 AND BEYOND The original...
28
Highland NHS Board 5 October 2010 Item 5.1 STRATEGIC FRAMEWORK – NHS HIGHLAND VISION Report by Roger Gibbins, Chief Executive The Board is asked to: Note that the revised Strategic Framework and NHS Highland Vision was launched at the Board Annual Event on 7 September 2010. Approve the revised Strategic Framework, NHS Highland Vision and Generic Service Model. Endorse the proposed implementation process. 1 BACKGROUND AND SUMMARY The Board approved the NHS Highland Strategic Framework 2010/2011 at its meeting in April following the work of the Board at the strategy event in March. This included a diagrammatic representation of the whole framework and approval of those aspects that had been completed. The Board approved the Quality and Safety Framework, the Efficiency and Redesign Framework, the Workforce Plan, the Board Budget and the Local Delivery Plan. A further update was presented to the Board on 1 June 2010 when it was noted that work was in progress to develop the Strategic Framework for 2011/12 and beyond. This work has continued to be a focus of the Corporate Team and there was a further discussion at the August Board Development Session. This focussed on the development of an overarching strategic statement designed to position the Board for the future. This was presented as the Board Vision and Generic Service Model. Following discussion with the Board this was further refined and presented at the Board Annual Event. The Board Annual Event was held at The Highland Council Headquarters on Tuesday 7 September and attended by over 100 delegates from the Board, the CHP/Raigmore Governance Committees, the Highland Partnership Forum and the Area Clinical Forum. As well as offering an opportunity for the various areas within NHS Highland to share good practice, the revised Strategic Framework and NHS Highland Vision was launched. The afternoon session allowed an opportunity for the various work groups to consider how NHS Highland will realise the vision. The revised Strategic Framework is attached as Appendix 1. 2 NHS HIGHLAND VISION The Board Vision and Generic Service Model is attached at Appendix 2 and presented to the Board for approval. In summary, NHS Highland, like all health boards, faces enormous challenges to meet increasing levels of health need as the population ages and health technology continues to advance at a time when public sector expenditure is severely constrained. The Board’s mission is to provide patient centred services tailored to people’s needs in a systematic and consistent way – to provide quality care to every person every day.
Transcript of 5.1 Strategic Framework - NHS Highland...3 3 STRATEGIC FRAMEWORK 2011/12 AND BEYOND The original...

Highland NHS Board5 October 2010
Item 5.1
STRATEGIC FRAMEWORK – NHS HIGHLAND VISION
Report by Roger Gibbins, Chief Executive
The Board is asked to:
Note that the revised Strategic Framework and NHS Highland Vision was launched atthe Board Annual Event on 7 September 2010.
Approve the revised Strategic Framework, NHS Highland Vision and Generic ServiceModel.
Endorse the proposed implementation process.
1 BACKGROUND AND SUMMARY
The Board approved the NHS Highland Strategic Framework 2010/2011 at its meeting inApril following the work of the Board at the strategy event in March. This included adiagrammatic representation of the whole framework and approval of those aspects that hadbeen completed. The Board approved the Quality and Safety Framework, the Efficiency andRedesign Framework, the Workforce Plan, the Board Budget and the Local Delivery Plan.
A further update was presented to the Board on 1 June 2010 when it was noted that workwas in progress to develop the Strategic Framework for 2011/12 and beyond.
This work has continued to be a focus of the Corporate Team and there was a furtherdiscussion at the August Board Development Session. This focussed on the development ofan overarching strategic statement designed to position the Board for the future. This waspresented as the Board Vision and Generic Service Model. Following discussion with theBoard this was further refined and presented at the Board Annual Event.
The Board Annual Event was held at The Highland Council Headquarters on Tuesday 7September and attended by over 100 delegates from the Board, the CHP/RaigmoreGovernance Committees, the Highland Partnership Forum and the Area Clinical Forum. Aswell as offering an opportunity for the various areas within NHS Highland to share goodpractice, the revised Strategic Framework and NHS Highland Vision was launched. Theafternoon session allowed an opportunity for the various work groups to consider how NHSHighland will realise the vision.
The revised Strategic Framework is attached as Appendix 1.
2 NHS HIGHLAND VISION
The Board Vision and Generic Service Model is attached at Appendix 2 and presented tothe Board for approval.
In summary, NHS Highland, like all health boards, faces enormous challenges to meetincreasing levels of health need as the population ages and health technology continues toadvance at a time when public sector expenditure is severely constrained.
The Board’s mission is to provide patient centred services tailored to people’s needs in asystematic and consistent way – to provide quality care to every person every day.

2
Our approach embraces the Healthcare Quality Strategy for Scotland. At its heart thisrecognises people’s priorities are for:
Caring and compassionate staff and services Clear communication and explanation about conditions and treatment Effective collaboration between clinicians, patients and others A clean and safe care environment Continuity of care and Clinical excellence
Quality is therefore at the heart of our vision. We believe that a focus on efficiency withoutattention to quality is unthinkable but equally that promoting quality with no regard forefficiency is unsustainable.
Our vision is therefore to provide quality care at all times; to support people andcommunities to maximise their own health; to develop precision driven services so that whenpeople need our care they experience timely, focused, effective services that minimises theduration and frequency of contact; and to ensure that every health pound spent deliversmaximum health gain.
Implementing this vision will require concerted effort across the whole Board. It will requirechanges to working practices for all staff as consistent systems and pathways are developed,evolved and adopted. Ultimately it will mean that health need can continue to be met as thebalance of need and resource becomes tighter. It will mean that the characteristics ofservice delivery in NHS Highland over the next five years will quickly evolve to be onesof:
1. promoting good health, self care and independence
2. high quality, integrated, equitable, needs and evidence-based, and cost-effective
3. increasingly community-based with hospital beds preserved for the most acutely illand those with specialist needs
4. integrated with, and complementary to, local authority, voluntary and independentsector care
5. run by healthy, flexible, well-motivated and well-trained staff working to theirmaximum potential and capability
6. using modern, flexible, efficient, green assets to maximum effect
7. with zero wastage and inefficiency across all services and no unnecessary overheads
Work has already begun to implement the vision in NHS Highland.
The NHS Highland Vision paper is supported by a series of supplementary paperscovering:
1. External Driver’s of Need for Health Care Services2. Possible Finance Scenarios3. The Generic Model of Care

3
3 STRATEGIC FRAMEWORK 2011/12 AND BEYOND
The original Strategic Framework agreed by the Board in April 2010 was recognised as fit forpurpose for the current year. It would need to be further developed to carry the Boardthrough the next period.
The development of the Board Vision and Generic Model of care is a critical component ofthe evolving framework
It was always recognised that the broad vision would require translation into specific servicestrategies to support application and implementation. These are described as Local SupportStrategies in the Framework. As set out in the vision, care pathways will be developed formajor programmes of care characterised by those disease areas that constitute the mostsignificant demand for health care. These in turn will be further supported by three moregeneric care pathways that describe the ‘Highland Way’ in respect of:
Self care Anticipatory Care Unscheduled care Planned care
This then confirms those components of the Local Supporting Strategies that will bedeveloped over the next period.
The Framework also included key enabling tools and plans that assist the implementation ofthe service strategies. Again, these were agreed for one year only but now need to be bothamended to reflect the approach to implementation (described below) and to span the nextperiod. Effectively the ‘next period’ is likely to be defined by the three year period of theComprehensive Spending Review and the enabling plans will need to have a view to thistime frame as well as confirm the Boards approach for 2011/12.
The revised Board Strategic Framework is therefore summarised in Annex 2 and the Boardis invited to endorse this framework and to note that the components of the framework will bereported to the Board as part of the financial and service planning cycle.
4. IMPLEMENTATION
Once the Board has debated and agreed the Vision and revised Framework, the task ofimplementation needs to start immediately.
It is proposed that this work is divided into five aspects, a Communications and Engagementprocess and four major areas of Delivery. Each will need to have robust managementmechanisms and appropriate Board governance. These areas of work are outlined below.The recommendation is that the communication process begins immediately and thatprogress is reviewed at the Board Strategy day on the 2 November and that the four keyprogrammes of delivery are worked up further and finalised with the Board at the Novembermeeting.
4.1 Communications and Engagement
Effective communications and engagement is critical to the successful implementation of theBoards Strategic Framework and delivery of the NHS Highland Vision. This can only beachieved by working with the people who deliver and use our services - our staff, patients,the public and key partners. As such it has been agreed that communications andengagement is a key leadership challenge and responsibility, for the Board, the Executive

4
Team and for General Managers in Operational Units and that everyone needs to see this asa key part of their leadership role.
As a Board we have not always been successful in communicating key messages andactively involving and engaging people in the changes that we need to make. In signallingthe need for transformational change, not so much in what we do, but in how we do it, weneed to take on a reinvigorated approach to communications and engagement. Thisprocess needs to start with short simple messages about what we are planning for now andin the future.
To do this effectively we have to; develop a culture of effective staff, patient and public engagement so that we can
be confident that change is being well managed have communication and engagement as a core part of our change process and
not as an optional extra be confident that we are doing the right things for the right reasons and have
evidence to support the case for change be able to use examples from real patient stories to demonstrate the need to
change and make improvements in patient outcomes and experience be able to use examples to demonstrate the positive changes to staff roles and
staff experiences but be realistic and accept that some people won’t like the changes we need to
make
To develop a reinvigorated approach to Communications and Engagement within NHSHighland, we have summarised the main characteristics of communications within changemanagement as the seven “I”s.
1. Initial analysis – describe what is likely to change and why.2. Information – use hard evidence to support the case for change.3. Identify - the range of audiences / stakeholders.4. Impacts – explore with stakeholders the potential impacts and effects of
change, listen to how they perceive the impacts, and use this feedback torefine the messages.
5. Initiative – take the initiative and bring your messages to people. Leaddiscussions with key groups, facilitate informed debate, reflect on feedbackand respond to emerging issues, opportunities and concerns.
6. Illustrate – how the change benefits patients through real life examples fromemerging evidence within NHS Highland or from elsewhere.
7. Improve – our practice by seeking and using feedback from participants toassess the impact of our messages and our methods, and sharing thisbetween change leaders.
To support this approach the Communications Team have developed an approach tocommunications and engagement, which outlines the way we propose to take this forward;by identifying core messages and key stakeholders, developing a suite of resources, e.g.PowerPoint presentations, key documentation media etc., to support an initialCommunication and Engagement Campaign and by thinking through tactics and impactmeasures and other ways of integrating the key messages into all that we do.
4.2 The Clinical Board
The Board has agreed that there are seven characteristics of its services in the future, ofwhich the second and third are around high quality evidence-based services and integratedcare with partners. In order to implement these two characteristics, the Board proposes toset up a Clinical Board to provide clinical advice and guidance on evidence-based bestpractice and the ways in which it can be implemented across NHS Highland. The exact

5
structure and governance arrangements will be determined over the next few weeks inconsultation with clinicians and managers, but it will report to the Board with clear operationallinks for implementation to Highland Operational Group, DHS Operational Group and theIntegrated Planning Group; for governance and monitoring to the Clinical Governance Forumand for information on service activity to eHealth. The professional advice structure of theArea Clinical Forum will also need to be linked into this framework.
The Clinical Board will need to establish a process by which it receives requests for clinicalguidance and advice and decides on the appropriate route and format this will take. Areasfrom which requests may come include major clinical areas such as diabetes, out of areareferrals, exceptional medicines use, implementation of national guidance from SIGN andScottish Government, issues raised by local and national audit programmes, critical incidentsand complaints processes. All issues will need to be gathered by a secretariat function andscoped by a core group (membership to be decided) for size and nature of problem, amountof work needed and existing guidance. Actions available to this core group could includeproduction of a policy statement for dissemination to relevant professionals and managers,the development of a pathway or referral criteria by a working group, dissemination ofexisting guidance without further addition, or the production of a monitoring framework oraudit pro forma. This list is not exhaustive. These proposed actions would then go to theClinical Board for prioritisation and agreement on who would do the further developmentwork to a fixed timescale. Policy statements, recommendations, guidelines and pathwayswould then be forwarded to the appropriate groups for implementation and monitoring. TheClinical Board would then agree the final product and the NHSH Board would receive a list ofrecommendations made and regular updates on progress.
Further work to address this proposal in more detail is still required.
4.3 Integrated and Self Care
Improvements in responsibility for self care amongst the population are fundamental toenabling individuals, families and communities to live long and independently. In the widestsense, self care covers a range of aspects from web-based and self help information,voluntary sector guidance, sign posting and support, to making healthy choices about diet,exercise and life style. Self help must also be a key building block in the management oflong term conditions and care pathways. In order to maximise self care opportunities,organisations across the public, private and voluntary sector will be required to plan,commission, deliver and monitor services together. In the Highland Partnership much of thisis underway with the joint Transformational Change Programme, while in the Argyll & ButePartnership specific pieces of work focus on long term conditions and older people.However, there is a need to better involve Public Health and other sectors of both Councils,such as Education, Leisure and Sport, in this work. NHS Highland will be seeking to expandthese areas of work to take forward its intention to ensure that all services are promotinggood health, self care and independence. In this way, characteristics one and four of theseven characteristics in the Vision will be progressed.
4.4 Business Transformation
The redesign of services has historically been coordinated across Highland through theHighland Operational Group (formally DHS Management team), where experience andinitiatives from across all Operational Units and as a result of collaborative programmes hasbeen shared. The implementation of LEAN across the organisation is also being broughttogether under a separate Project Board which replaces the Service Improvement Group.
In addition there are separate groups coordinating the capital spend for NHS Highland, AssetManagement Group, and the IT requirements and spend through the e-Health StrategyGroup.

6
It is acknowledged that NHS Highland must increasingly get the best possible efficienciesfrom redesign initiatives through effective and rapid roll out where appropriate, and theadoption of business infrastructure and tools.
A coordinated approach to this is now required, and it is proposed that all of this work iscoordinated utilising a more formal Business Transformation methodology, bringing togetherkey individuals who are leading on these areas. This will be a mechanism for implementingcharacteristics six and seven of the Vision.
4.5 Workforce
One of the characteristics of service delivery in NHS Highland over the next five years will bethat the service is; ‘run by healthy, flexible, well-motivated and well-trained staffworking to their maximum potential and capability’. Implementing the vision will meansignificant changes for staff both in terms of what they do and how they do it.
Staff will continue to be well informed and engaged in change and improvement Staff will continue to be encouraged to be innovative and share good practice Staff will continue to be appropriately trained The direction of travel will be for care which will be directed by fewer highly skilled
staff and delivered by a more generic workforce The direction of travel will be that Staff will need to be more flexible to facilitate
service redesign The Organisational Change and Redeployment Polices will be fully utilised Staff will be accountable for adherence to Board Polices and procedures and in
delivering on NHS Highland priorities and objectives Nationally negotiated Terms, Conditions and Policies will continue to be applied in
NHS Highland Staff who are not able to perform to an agreed standard will be helped to improve or
move on The overall size and profile of the workforce will change.
The Highland Partnership Forum will continue to be the main formal Board Committee wherematters that affect the workforce are proactively and fully discussed. Strategically it will givedirection to all parts of NHS Highland around the workforce agenda. In addition it willcontinue to champion the NHS Scotland Partnership Working Model as the best method ofindustrial relations to enable all within NHS Highland to move towards the Board’s vision.The Highland Partnership Forum will be supported, and complemented, by Local PartnershipForums in the Operational Units and work closely with the Boards Health and SafetyCommittee.
Managers and the Human Resources Services Teams will work together to ensure that staffare healthy and safe, well managed, supported and developed and that where it is necessaryto refer to PIN Polices, that they are applied consistently and in a timely manner to facilitate aclear outcome.
5 CONTRIBUTION TO BOARD OBJECTIVES
The Strategic Framework underpins all of the Board’s Corporate Objectives.
6 GOVERNANCE IMPLICATIONS
The Impact on all the relevant Governance Standards will be detailed in each of thecomponent strategies which make up the Strategic Framework.

7
7 IMPACT ASSESSMENT
The plan needs to be specifically impact assessed, both in terms of equality and diversityand the impact on inequalities but also in respect of impact on partners and stakeholders. Tobe meaningful, slightly different approaches may be required for each aspect of theframework.
Impact assessments on the over-arching plans will be fully completed prior to the plans beingpulled together as the strategic framework and presented to the Board for final sign-off, butobviously any impact assessment of delivery plans will take place at a later date as these aredeveloped.
Roger GibbinsChief Executive
24 September 2010

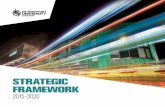
MEASURESOF
SUCCESS
ENABLINGTOOLS/PLANS
Resources to Assistin Implementing
Strategies
LOCALSUPPORTINGSTRATEGIES
NHS Highland - whatwe want to do in line
with StrategicFramework
STRATEGICFRAMEWORK
(Direction and Scope)
SLAs/Partnership Agreements/SOA
“Th
eH
igh
lan
dW
ay”
inre
sp
ec
to
f:
NHS HIGHLAND STRATEGIC FRAMEWORK
Board Vision and Generic Service Model
Quality & Patient Safety Framework
Scottish Government Strategies
LDP/Heat Targets/Local KPls
Self
Care
An
ticip
ato
ryC
are
Un
sch
ed
ule
dC
are
Operational Unit Plans
Financial Plan and Budget
Workforce Plan
Business Transformation Plan
Public/Staff Engagement Plan
Pla
nn
ed
Care
CARE PATHWAYS(to be developed)
e.g. COPD,diabetes, LTC,
maternity
APPENDIX 1

APPENDIX 2
Board Annual Event – 7 September 2010 1
NHS HIGHLAND VISION
NHS Highland, like all health boards, faces enormous challenges to meet increasing levelsof health need as the population ages and health technology continues to advance at atime when public sector expenditure is severely constrained.
The Board’s mission is to provide patient centred services tailored to people’s needs in asystematic and consistent way – to provide quality care to every person every day.
NHS Highland, in common with all Scottish health boards, has a huge advantage in beingresponsible for the total health needs of the population and for integrated care. Thismeans we are responsible for better health of our communities through population wideand individually focused initiatives to maximise health and prevent illness; for better careof our patients through quick access to modern services, in clean and infection freefacilities, by well trained and courteous staff; and for better value for the use of the publicmoney we spend by ensuring there is no waste and inefficiency, money is spent only onwhat is needed and has evident therapeutic benefits and variation from core carepathways is the exception.
We recognise the importance of keeping a balance between the three components ofbetter health, better care and better value because they are intrinsically linked andtogether constitute an effective health system. Any one area cannot be prioritised overany other.
Our approach embraces the Healthcare Quality Strategy for Scotland. At its heart thisrecognises people’s priorities are for:
Caring and compassionate staff and services Clear communication and explanation about conditions and treatment Effective collaboration between clinicians, patients and others A clean and safe care environment Continuity of care and Clinical excellence
Quality is therefore at the heart of our vision. We believe that a focus on efficiencywithout attention to quality is unthinkable but equally that promoting quality with no regardfor efficiency is unsustainable.
Our vision is therefore to provide quality care at all times; to support people andcommunities to maximise their own health; to develop precision driven services so thatwhen people need our care they experience timely, focused, effective services thatminimises the duration and frequency of contact; and to ensure that every health poundspent delivers maximum health gain.
Working in this way we believe that NHS Highland can continue to meet the health needsof our population with diminished resources. Precision driven services focused onevidenced based interventions, with all staff working to common systems and processes,will mean needs can be met with less resource.

Board Annual Event – 7 September 2010 2
This will allow us to rationalise services in order to protect the funding of essential servicesand to meet new needs. This approach means that there will be significant change - forcommunities, for patients and for our staff - in the way services are organised anddelivered.
It does not mean a change to the basics building blocks of the NHS that we hold dear at alltimes. NHS Highland works to the underlying values of the NHS that services should be
Equitable, available to the whole population of Highland according to need Accessible as far as possible in terms of culture, language and information
provision Free at the point of access Non-judgemental and non-discriminatory, delivered according to need irrespective
of age, ethnicity, religious belief, political persuasion, sexual orientation, ability/disability or gender
Respectful of the patient’s dignity and wishes, delivered in partnership with patientsand communities
Supportive of staff as the most valuable asset of the organisation
Within this solid foundation however the NHS has not stood still and is constantly evolvingto meet new and changing needs. This pace of change now needs to increase.
Therefore, it does mean that NHS Highland will accelerate work to establish everywherethe generic model of care that seeks to identify and prevent health problems as early aspossible, treats patients holistically, avoiding hospital admissions by managing patients inthe community through anticipating their health needs and by community and morespecialist staff working together. Our services will always be there at times of emergency.When hospital admission is required, it should be for explicit indications, according toagreed pathways and after alternative options have been fully explored. Any hospital stayshould be as short as possible, with a return to the community with appropriate supportand follow-up planned for from admission.
Implementing this vision and accelerating the implementation of the generic model of carewill require concerted effort across the whole Board. It will require changes to workingpractices for all staff as consistent systems and pathways are developed and adopted.Ultimately it will mean that health need can continue to be met as the balance of need andresource becomes tighter. It will mean that the characteristics of service delivery inNHS Highland over the next five years will quickly evolve to be ones of:
1. promoting good health, self care and independence
2. high quality, integrated, equitable, needs and evidence-based, and cost-effective
3. increasingly community-based with hospital beds preserved for the most acutely illand those with specialist needs
4. integrated with, and complementary to, local authority, voluntary and independentsector care
5. run by healthy, well-motivated and well-trained staff working to their maximumpotential and capability

Board Annual Event – 7 September 2010 3
6. using modern, flexible, efficient, green assets to maximum effect
7. with zero wastage and inefficiency across all services and no unnecessaryoverheads
These characteristics of service delivery may not feel radically new but the implicationsonce fully rolled out, are far reaching:
Promoting good health, self care and independence
People will become ‘expert patients’ knowledgeable as to how to improve their ownhealth and manage their long term conditions.
Staff will put more emphasis on helping people to support themselves, rather than‘doing to’.
People will make less use of hospital care Patients will contact clinicians in different ways – remotely, though technology and in
groups alongside patients with similar needs
High quality, integrated, equitable, needs and evidence-based, and cost-effective
NHS Highland will stop providing interventions and services that do not demonstratethese criteria.
We will provide what people ‘need’ clinically not necessarily what they feel they ‘want’. Clinicians will follow agreed pathways for major conditions with minimal deviation and
variation. Quality will be robustly monitored and audit focused accordingly. Clinical outcomes will be monitored routinely. Errors will be rigorously followed through and are shown to be minimised. Any services or procedures that are shown to be error prone or achieve poor outcomes
will be stopped.
Increasingly community-based with hospital beds preserved for the most acutely ill andthose with specialist needs
More people will receive their health care at home Avoidable unplanned admissions will be seen as failures Fewer in-patient beds, and resources redirected as beds are closed Activity and productivity in community care monitored and managed to ensure
effectiveness More people able to choose to die with dignity in their own homes surrounded by their
family Specialist clinicians working across secondary/primary care boundary
Integrated and complementary with local authority, voluntary and independent sectorcare
Single, integrated health and social care budgets and services. NHS funding to voluntary and independent sector will be targeted on activities to
deliver the vision Communities will need to develop greater resilience for self support

Board Annual Event – 7 September 2010 4
Run by healthy, well-motivated and well-trained staff working to their maximumpotential and capability
Skill mix will change – fewer highly skilled staff directing care that will be delivered by amore generic workforce
Staff will work to flexible contracts to facilitate redesign Greater accountability for adherence to Board policy and procedures Poorly performing staff helped to improve or helped to move on The overall workforce will shrink in line with budget reductions
Using modern, flexible, efficient, green assets to maximum effect
Our worst and least economic buildings will close, the remainder improved to the bestquality we can afford.
Services will be provided across Highland on fewer NHS sites Greater use of community facilities to support self care approach. Less office space in fewer buildings Technology significantly more advanced and supporting the model Excellent information management to ensure effective decision making and planning
With zero wastage and inefficiency across all services and no unnecessary overheads
System effectiveness assured through lean processes Business approaches and systems engineering to ensure waste and inefficiency
designed out of operational services Staff productivity and effectiveness routinely managed Slimmed down corporate and non-clinical support services More shared services with partners
Work has already begun to implement the vision in NHS Highland. There are goodexamples of all aspects somewhere. The challenge is to make these good examples thenorm, implement the vision everywhere and in so doing create the scale of changenecessary to allow services to be rationalised and resources released without detriment tothe Board’s ability to meet need. This in turn will ensure NHS Highland, our staff, and ourpatients and communities continue to enjoy excellent health care into the future.
This paper is supported by a series of supplementary papers covering:
1. External Driver’s of Need for Health Care Services2. Possible Finance Scenarios3. The Generic Model of Care

APPENDIX 2
Board Annual Event – 7 September 2010 5
Board Annual Event – 7 September 2010NHS Highland Vision: Supplementary Paper 1
External Drivers of Need for Health Care Services
Health services are constantly changing in terms of the treatment and care theyprovide and the ways in which they provide it, in response to changes in the structureand disease patterns of the population they serve. Need for health care, defined asthe ability to benefit from a health care intervention, is also always changing as itbecomes possible to treat more diseases more effectively, and thresholds fortreatment change.
1. Demographic Change
The population of Highland has increased over the last 10 years, more so in theHighland Council area than Argyll and Bute, by around 6%. It is expected to continueto grow by around 10% over the next 20 years. This increase, past and predicted, isdue mainly to net in-migration to the region, rather than natural increase (births -deaths). The predicted increase does not take account of any new externalinfluences on population, such as increased inward migration due to climate change.
The proportion of people aged over 65 years in the population has been steadilyincreasing for some time and is set to continue for the next 20 years. The proportionof the population that are of pensionable age is likely to increase from 21% to 24-25% (taking account of planned changes to retirement ages). Within this group, thenumbers of people aged over 75 years is predicted to more than double and thenumbers of very elderly (aged 85 years and over) will increase even more (see figure1 below)
Data Source: GRO(S) Mid Year Estimate Population seriesand GRO(S) PopulationProjections for Administrativeareas(2008 based projection)

Board Annual Event – 7 September 2010 6
2. Epidemiological Change
MortalityCancer and circulatory diseases still account for over 60% of all deaths in NHSHighland; this figure is in line with the rest of the UK and other developed countries.Mortality from cardiovascular disease, the largest component of circulatory diseases,is falling in those aged under 75 years, but the socio-economic gap remains (seefigure below).
0
20
40
60
80
100
120
140
160
180
200
1 2 3 4 5 1 2 3 4 5 1 2 3 4 5
SIMD06 quintile
Dir
ectl
ysta
nd
ard
ise
dm
ort
ali
tyra
tep
er
10
0,0
00
1996-1998 2002-2004 2006-2008
Premature Mortality from Cardiovascular DiseaseNHSHighland, by Deprivation Quintile 1996 - 2008
Mortality from CVDhasbeen falling for the under 75 year oldsover thelast two decades, but the inequality gap remains
Cancer incidence and numbers of death from cancer continue to increase, reflectingthe ageing of the population. Cancer survival, however, is improving and the age-standardised death rate is falling, indicating that more people are living for longerwith cancer. The top four causes of cancer mortality remain breast, lung, bowel andprostate.
Of other major causes of death, those related to alcohol have trebled in the last 30years.
Life expectancyIn line with falling premature mortality rates, life expectancy continues to increase, asdoes healthy life expectancy, but the gap between the two is not closing, indicatingthat the burden of chronic ill-health in later life continues and is shifting into older agegroups. Healthy life expectancy is improving more rapidly for men than women.

Board Annual Event – 7 September 2010 7
Life Expectancy and Healthy Life Expectancy in Scotland 1980-2006
Source: ISD Scotland
Long-term conditionsDefinitions of long-term conditions vary, making estimating numbers of people withthem difficult. According to the Practice Team Information, about 54% of thepopulation aged 16 years or over consulted their GP for a potential long-termcondition in a 1 year period; however, this figure includes many who are able tomanage their condition themselves. In the Scottish Health Survey, 37% of thepopulation reported having a long-term condition, and 11% said that their conditionlimited their day to day activities.
The prevalence of LTCs increases with age; in the Scottish Health Survey 65% of theover 65s reported an LTC, with 35% reporting two or more LTCs. Practice TeamInformation also shows that people consulting their GPs about one LTC are morelikely than not to have at least one other LTC as well. For example, of thoseconsulting their GP for CHD, only 8% have no other LTC, while 67% have at leasttwo other LTCs.
This co-existence of multiple LTCs probably reflects the ageing population, and alsosuggests that treating LTCs in isolation is no longer appropriate for the majority of thepopulation suffering from them.
Lifestyle risk factorsSmoking prevalence continues to fall; the latest estimates suggest that 26% ofScottish men and 25% of Scottish women smoke regularly.
Alcohol consumption remains high at around 11.8l of pure alcohol per person peryear the equivalent of 570 pints of 4% beer or 42 bottles of vodka or 125 bottles ofwine. This level of consumption is enough for every adult in Scotland to exceed thesensible drinking guidelines for men and women every week of the year.

Board Annual Event – 7 September 2010 8
Obesity levels continue to increase in adults: in 2008, 66% of men and 60% ofwomen were overweight or obese.
These changes in risk factor levels suggest that we will continue to see a reduction insmoking-related diseases, but alcohol-related health harm, circulatory diseases,some cancers and diabetes will continue to increase.

APPENDIX 2
Board Annual Event – 7 September 2010 9
Board Annual Event – 7 September 2010NHS Highland Vision: Supplementary Paper 2
Possible Finance Scenarios
1 BACKGROUND
In common with most NHS Boards, the Financial Plan and Local Delivery Plan (LDP) forNHS Highland envisaged an allocation uplift of 1% for 2011/12 and beyond; this was in linewith informal Scottish Government guidance. However, since submission and agreement ofthe LDP, the underlying economic position, together with some key assumptions haschanged significantly, and it is appropriate to review planning assumptions to ensure thatthey continue to reflect the best information available at this time.
It is important to recognise that there are a very small number of items and assumptionswhich have a disproportionate impact on the financial position. These relate particularly to:
resource allocation pay uplifts – inflation and increments drugs inflation
There are obviously many other factors which impact financially on a large and complexorganisation such as the Health Board, including advances in technology and demographicchanges, but the impact of the above three factors must be recognised – including thesensitivity analysis whereby a small change in any one of the factors will have a significantfinancial impact. There is also the issue of interdependences where a change in one of thefactors can impact on another – for example the level of pay uplifts and drug inflation will bereflected to some extend in the level of allocation uplift.
2 PLANNING DETAILS
Definite figures are not available at this stage, and are unlikely to be available for a numberof months, so planning must be undertaken through the identification of potential resourcescenarios. These should be realistic in terms of the indications available at this stage, butrecognising that they will evolve over the next few months, with the completion of the UKComprehensive Spending Review, and the Autumn Budget leading to the ScottishGovernment Budget, alongside consideration of the consequentials for health. In parallelwith the Spending Review / Allocation, work is ongoing regarding Public Sector Paysettlements into 2011 and beyond, and again details are likely to emerge over the next fewmonths.
However, it is important to recognise that the uncertainties outlined above do not detract fromthe overall message of increasing financial constraints within the NHS – both capital andrevenue, and that these will continue for a sustained period. This means that focus isrequired on the anticipated “Bottom Line”, and the Board should not be distracted by debatearound the finer points / detailed calculations and must focus on planning to deliver financialbalance into the future periods with significant financial challenge.
This is highlighted by the “balancing figure” of the level of Efficiency Savings required todeliver financial balance. There are many different financial positions that could be detailed,and the report below focuses on three scenarios, starting with the LDP assumptions.

Board Annual Event – 7 September 2010 10
3 SCENARIO 1 – CURRENT PLANNING ASSUMPTIONS / LEVELS
The LDP contains an Assumptions Table which, in addition to covering the three major itemsidentified above, also highlights General Price inflation and FHS uplifts. The Table forFinancial Planning Assumptions within the current LDP is:
2009/10 Assumption - % Uplift 2010/11%
2011/12%
2012/13%
2013/14%
2014/15%
Allocation UpliftPayGeneral Price InflationGP PrescribingHospital DrugsOther FHS Uplifts
2.153.071.55.56.0
2.15
1.01.01.56.04.01.0
1.01.01.56.04.01.0
1.01.01.56.04.04.0
1.01.01.56.04.04.0
These assumptions bring out an anticipated level of Savings - based on projection of “SteadyState”, with no anticipated developments or uplifts – including those which will result fromtechnological advance or demographic trends. These “standstill efficiency savings” aresummarised within the LDP as:
2010/11£m
2011/12£m
2012/13£m
2013/14£m
2014/15£m
14.6 14.3 9.8 10.0 10.2
As well as needing to fund technological advance and demographic change there are alsolikely to be pressures around overall service change – including the development of NationalServices, etc. This is illustrated below, with assumed annual costs of:
£2m for developments £3m for demographic change
SCENARIO ONE SAVINGS –BASED ON CURRENT LDP
2011/12£m
2012/13£m
2013/14£m
21014/15£m
LDP Level of Savings as above 14.3 9.8 10.0 10.2
Development/ NHS Inflation Impact 2.0 2.0 2.0 2.0Demographic Change 3.0 3.0 3.0 3.0
Effective LDP Efficiency SavingsTarget
19.3 14.8 15.0 15.2
As noted above, this is based on an allocation uplift of 1%, and it is appropriate to highlightthe potential impact of public expenditure statements made since agreement of the LDP.

Board Annual Event – 7 September 2010 11
4 SCENARIO 2 – SCOTTISH GOVERNMENT OVERALL GUIDELINES
The Emergency Budget update produced by the Scottish Government in response to theJune UK Budget highlights the potential impact for the Public Sector within Scotland. At thisstage, it does not specifically detail health, but provides an indication of the public sectoreconomic position – revenue and capital combined - in real terms within Scotland. If therevenue position was to be applied to Health Board allocations then the potential impact infuture years would be:
2011/12 2012/13 2013/14 2014/15
Effective Year on Year Real TermRevenue Reduction
-3.9% -1.6% -2.5% -2.9%
Impact on Scotland £1.0bn £0.4bn £0.6bn £0.7bn
Impact on NHS Highland £20m £8m £12m £14m
Additional NHS inflation in excess ofGDP – partic drugs (inflation+ new)
£5m £5m £5m £5m
Potential Impact on Highland £25m £13m £17m £19m
This highlights the potential impact of the Emergency Budget update to NHS Highland,noting that allowance has been made in the above table for excess NHS inflation, whichrelates mainly to drugs, in terms of inflation, levels of activity, and the introduction of newdrugs.
5 SCENARIO 3 – NO UPLIFT TO HEALTH – FLAT LINE BUDGET
It is not possible, at this stage, to predict whether either of the above scenarios will reflect thefinancial position in future years, particularly when there is uncertainty over the protectionstatus of the NHS. One final assumption to examine is that the NHS will receive a 0% “uplift”over the period.
This would remove the 1% assumption within the current LDP and, effectively, add £5m perannum to the totals reflected in scenario 1. This would result in the following savings targets;
Flat Line Budget 2011/12 2012/13 2013/14 2014/15
Savings target £24.3m £19.8m £20m £20.2m
6 CONCLUSIONS
Whilst it is obvious that the economic impact on the NHS in the coming years will besignificant, the current uncertainty around the precise application of the austerity measureson Health makes accurate financial planning somewhat difficult. However, it is reasonable toassume that savings of around £20million per annum will be required in each year for theforeseeable future.

APPENDIX 2
Board Annual Event – 7 September 2010 12
Board Annual Event – 7 September 2010NHS Highland Vision: Supplementary Paper 3
The Generic Model of Care
The Generic Model of Care will underpin the NHS Vision Statement to provide high quality,effective and sustainable patient centred services appropriate to the needs of patients in aconsistent way across NHS Highland. ‘Better Health, Better Care and Better Value’ willresult in quality of care to every patient every time. The NHS Highland Quality & PatientFramework will be the essential foundation stone. There will be continuous improvement inquality of care and outcomes, with much more emphasis on supporting patients and theircarers to maintain and sustain their own health. Where care is required, this will be providedas locally as possible and care needs will be anticipated as much as possible and thereforemore become planned. Unplanned or emergency admissions will, in some cases, beregarded as a failure of the system.
The actual model of delivering the health care element is not radically different from thecurrent existing traditional model, and is still based on the patient/health carer relationship.Traditionally this was the doctor/patient relationship and more recently expanded to thepatient/health carer relationship. It is still fundamentally based on the assessment of thepatients’ condition, examination, investigation, diagnosis and the provision of appropriatetreatment and management. The fundamental change will firstly be the great emphasisplaced on the philosophy of patient self care and responsibility. Secondly, for those patientsrequiring care an explicit health management plan will be developed and this will be readilyavailable and accessible to all those involved in care, including the patients and carers.Currently the scheduled and unscheduled (emergency) care of patients significantly involvesthose patients with a pre-existing known condition. The basis of the Model of Care will bea Long Term Condition Care Management Plan, and for appropriate patients an AnticipatoryCare Plan, with an Alert system identified [ACPA]. Thirdly, the care provided will be basedon the identified needs of the patients and this care will follow agreed pathways of care. Theimplementation will involve rollout of this concept across the whole of NHS Highland and willhave a radical effect. There are already innovative approaches to healthcare across parts ofNHS Highland and the role out of these will ensure that these are applied to patients acrossthe whole of Highland in a consistent fashion.
The Scottish Government Health Department Policy “Better Health, Better Care” (2007)suggested that ‘health services have to change if they are to keep pace with populationtrends, patient needs and medical advances’. Table 1 compares the traditional view of careto the newly evolving approach to care.
Table 1.
Traditional View Evolving ModelGeared towards Acute ConditionsHospital centredDoctor DependantEpisodic CareDisjointed CareReactive CarePatient as a Passive RecipientSelf Care InfrequentUndervalued CarersLow Tec
Geared towards Long Term ConditionsEmbedded in CommunityTeam Based ApproachContinuous CareIntegrated/Holistic CarePro-active and Anticipatory CarePatient as a Real PartnerSelf Care Encouraged & FacilitatedCarers Supported as PartnersHigh Tec

Board Annual Event – 7 September 2010 13
The traditional Model of Care is provided by a number of distinct and discreet HealthcareProviders in different sectors across the organisation, as identified in Figure 1 below.
Figure 1: Sectors of Care.
While the patient appears at the centre of care, services have often been developed to meetthe needs of the service providers. Previously there has been little emphasis placed onpatient and/or care or self-care to maintain and develop health. There are real boundariesand barriers between GP Practices, Community Health Services, Contractor Services, LocalAuthority Care and the hospital based Specialist Services.
These traditional sectors have differences in training and expertise, objectives andexpectations, funding and management/accountability processes and care is accesseddifferently. As there is no single and integrated IT system across the NHS, effectivecommunication is difficult. NHS Highland services do not easily translate into a seamlessModel of Care for the patient. The new proposed Model of Care ensures that the barriersbetween the different sectors are removed and patients will flow between different parts of anintegrated system, as identified in Figure 2.

Board Annual Event – 7 September 2010 14
Figure 2: The Generic Model of Care.

Board Annual Event – 7 September 2010 15
The approach is to reduce the barriers between the providers along the spectrum of care, sothat the patient experience is seamless and transition of care from one sector to another issmooth, consistent and continuous.
Patient self-care
Community Based Care by different providers
Hospital Based Specialist and Tertiary Care
Patient Focussed Care will mean more emphasis on the patient and carer takingresponsibility for their own health and care, having more knowledge and support to ensurethat this happens. The ‘expert patient’ will understand their base line health status and bemore aware of when to seek or initiate appropriate increased healthcare.
For the patient with an LTC or ongoing healthcare need, there will an Anticipatory Care Plan[ACP] and an Anticipatory Care Plan Alert [ACPA], which will be available to all involved intheir care. These will identify the person’s base line condition and disease status, whatchanges a patient can and should make, ascertains when to seek additional advice and care,and what criteria may lead to accessing Specialist Care in both the scheduled andunscheduled situation.
Care in the Community Setting is the next level of care provided in the local setting. Theproviders of this care are the GP and Practice, Contractor Services (including Dentists,Pharmacists, and Optometrists etc.), Community Health Services (Nursing, Midwifery, AHPs)and Local Authority Services.
The concept of developing multidisciplinary working in the Extended Primary Care Team,whether real of virtual, will facilitate seamless and integrated care. This care will be providedin a range of settings within the home and community and the types of care have beenidentified in Figure 2.
Care in the Specialist or Secondary/Tertiary Care Setting is also identified in Figure 2and more Specialist Care will be provided out of the traditional hospital setting, within a moremultidisciplinary local approach. A fundamental concept to underpin the Generic Model ofCare is the development of agreed Conditions Specific Management Pathways, which willidentify the:
Natural history and progression of the disease or condition. The role of patient self-care and management. The role of health care professionals in supporting self-care and self-management. Method of assessment of the condition, current appropriate investigation, diagnosis,
management, treatment, maintenance, discharge and follow up, throughout thespectrum of care for that condition.
Criteria for escalation and management of progressing and complex disease. Aspects of Specialist Care. Discharge planning.
Within the Generic Model of Care, there will be a number of ‘Modules of Care’ as identified inFigure 3 below, which will be developed for different types of conditions and care. Withinthese developed modules, the range and types of care and management from patient’s self-care through to complex Specialist and Tertiary care will be identified, so that the patientescalation along the care pathway is quite explicit.

Board Annual Event – 7 September 2010 16
This will result in a clear Framework of Care for NHS Highland identifying what patients arebeing treated for what conditions, by specified providers at each and every location.
Figure 3: Modules of Care.

Board Annual Event – 7 September 2010 17
Figure 4: Triangle of Care

Board Annual Event – 7 September 2010 18
If the Triangle of Care for a Long Term Condition with Anticipatory Care needs is considered,as identified in Figure 4, then a respiratory disease such as Chronic Obstructive AirwaysDisease (know as COPD) or Asthma will clearly illustrate the pathway. Guided by theCondition Specific Care Pathway, the patient experience for COPD or Asthma would be asfollows:
Patient Self Care would mean that the patient +/- carer would have a good knowledge andworking expertise of their asthma or COPD. The disease and progression would bearticulated in the ACPA. The patient and carer would know what their normal disease statuswould be in terms of i.e. general wellbeing, exercise tolerance, sleep pattern, cough, wheeze,breathlessness, sputum production, spirometry assessment and other various signs. Selfassessment would be regularly carried out and enable the patient to self monitor theirprogress. Coincidentally these assessments would be relayed to the local LTC carer, usuallya LTC trained nurse, who would monitor trends over time, the frequency of monitoring beingdependant on the severity of the condition. An ACPA would have been agreed and baselinecare documented, and also what patient treatment should change if the conditiondeteriorated slightly. If the assessments indicated a significant deterioration either thepatient would manage as previously agreed, with augmented treatment such as antibiotictherapy, steroid therapy or oxygen. The frequency of the self reported assessment would beincreased and early intervention would result. The LTC Local Nurse would be aware of thedisease deterioration and would increase support either by indirect contact (telephone/VC) ora direct patient face-to-face review. The ACPA would have identified trigger alerts for theescalation of care and access to augmented Primary or Secondary Care Services, asappropriate.
If resolution of the episode of disease deterioration did not occur, then the ACPA would detailwhat subsequent management or treatment should occur and a review could take placeeither by the Primary Healthcare Team or a Specialist. This review could take place by aSpecialist in consultation from a distance by telephone or VC, in conjunction with the LTCLocal Nurse or the Primary Health Team. Subsequently if the episode of care deterioratedsignificantly, then the patient could be seen by a Specialist in a virtual community ward, at anoutpatient clinic or as an inpatient within the hospital, and this would follow the specificcriteria laid out in the ACPA. With this system, the Specialist will have had access to thedeteriorating episode of care with all the assessments and subsequent changes inmanagement documented, and therefore Anticipatory Care would ensue. The emergencyconsultation or admission would be averted and hopefully any admission relatively wellplanned, along the lines identified within the ACPA. Appropriate care would have beeninstigated at an early stage following early assessment and alerts. All details of agreed carewill be included such as DNAR, palliation and the discharge planning process will alreadyhave been discussed and documented, and therefore if the patient is admitted to hospital,the planned discharge process will result in a more effective discharge resulting in shorterlengths of stay and improved continuity of care within the community setting.
Pilots of this process have already been implemented such as within Argyll & Bute forpatients with COPD and the Nairn Long Term Conditions Project. These projects have beenevaluated and have shown an increased quality of care, reduced emergency admissions, ashorter length of stay, a more efficient discharge planning process, and the patients havebeen able to be maintained appropriately within the community setting for a longer timeperiod.
The Condition Specific Care Pathway would be developed identifying the natural history ofthe disease, how to manage deterioration of that episode across the escalating pathway ofcare in terms of assessment, diagnosis, treatment, referral and maintenance. This modularapproach is therefore applicable to most types of care.

Board Annual Event – 7 September 2010 19
This Model of Care is not in itself a radical change, but the implications imply:
1. The needs of patients will be responded to in a consistent and holistic fashion, asopposed to being influenced by the wants and demands of patients and staff.
2. Services will be re-configured and re-designed to meet the needs of patients asquickly and locally as possible, but the implementation will be consistent across NHSHighland.
3. Care will be provided by agreed pathways of care, so that care will be consistentacross NHS Highland, with duplication and inefficiencies avoided and a reduction inany identified variation.
4. Outcomes of care will be robustly monitored to ensure compliance and accountabilityto the care pathways and that high quality of care is being provided.
5. There will be an organisational consensus approach to care management by allinvolved partners including the patient, health care, local authority, voluntary sectorand all other stakeholders.
6. Health carers will be required to adapt to new and innovative ways of working acrosstraditional boundaries of care to ensure a seamless, integrated approach as locallyprovided as possible.
7. Technologies will support this shift in care.
8. Using the agreed care pathways, criteria for referral and an increased day care/daycase approach will result in a requirement for fewer beds in different locations in NHSHighland.
9. Implementation will be developed across the whole of NHS Highland, so thateveryone will know what care will be delivered to which patients, by whom, where andthe point of access to care will be clear. This will result in a clearly identified clinicalframework.
10. Implementation will be lead by both clinicians and patients, for clinicians and patients.The Board will establish a Clinical Board to guide this.
What Developments Are Now Required:
1. Fully develop the concept of Long Term Condition Management as a fundamentalcornerstone of providing care in NHS Highland.
2. Extend Anticipatory Care Plan and Alerts (ACPA) to cover all Long Term Conditionsand patients with ongoing healthcare needs, and perhaps consider for all thosepatients in the over 75 year old age group.
3. Develop agreed Integrated Pathways of Care and Management for commonconditions.
4. Develop conditions specific referral criteria and a Triage Referral ManagementSystem.

Board Annual Event – 7 September 2010 20
5. Build a rehabilitation approach and capacity into services.
6. Develop real integrated and multidisciplinary Extended Primary Healthcare Teamsincluding all partners in care.
7. Implement robust audit, monitoring and clinical governance of all care provisionthroughout NHS Highland.
8. Develop integrated IT Systems with easy access to all involved in care to provide acomprehensive and timely common record.
9. Training of locally based generic staff by more specialist experts to ensureappropriate skills and competence.
10. Staff working practices will be different as there will be fewer direct patient contacts,more generic training for staff, and an increase in multidisciplinary joint care sessions,as well as an increased utilisation of tele/eHealth, especially for consultation andadvice. This will inevitably impact on the working practices of all staff and have aneffect on the job planning process for all staff.












![Highland Strategic Commissioning Plan for Older People ... · removed from the final version]. Content Foreword Part 1 The Context Strategic commissioning plan for Highland Introduction](https://static.fdocuments.us/doc/165x107/5f788ba355cb2444f42bf39c/highland-strategic-commissioning-plan-for-older-people-removed-from-the-final.jpg)


