50225452.pdf
7
Shoulder injuries in athletes Br J Sports Med 2010;44:300–305. doi:10.1136/bjsm.2009.058834 300 Shoulder Center of Kentucky, Lexington, Kentucky, USA Correspondence to Aaron Sciascia, Shoulder Center of Kentucky, 700 Bob- O-Link, Lexington, KY 40504, USA; [email protected] Accepted 13 October 2009 Current concepts: scapular dyskinesis W Ben Kibler, Aaron Sciascia ABSTRACT The scapula serves many roles in order for proper shoulder function to occur. These roles include providing synchronous scapular rotation during humeral motion, serving as a stable base for rotator cuff activation and functioning as a link in the kinetic chain. Each role is vital to proper arm function and can only occur when the anatomy around the shoulder is uncompromised. The presence of bony and soft tissue injury as well as muscle weakness and inflexibility can alter the roles of the scapula and alter scapular resting position and/ or dynamic motion. This altered scapular position/ movement has been termed ‘scapular dyskinesis’. Although it occurs in a large number of shoulder injuries, it appears that scapular dyskinesis is a non-specific response to a painful condition in the shoulder rather than a specific response to certain glenohumeral pathology. The presence or absence of scapular dyskinesis needs to be determined during the clinical examination. An examination consisting of visual inspection of the scapular position at rest and during dynamic humeral movements, along with the performance of objective posture measurements and scapular corrective maneuvers, will help the clinician ascertain the extent to which the scapula is involved in the shoulder injury. Treatment of scapular dyskinesis should begin with optimised anatomy and then progress to the restoration of dynamic scapular stability by strengthening of the scapular stabilisers utilising kinetic chain-based rehabilitation protocols. Normal scapulohumeral rhythm, the coordinated movement of the scapula and humerus to achieve shoulder motion, is the key to efficient shoulder function. Scapular position and motion are closely integrated with arm motion to accomplish most shoulder functions. Scapular movement is a com- posite of three motions—upward/downward rotation around a horizontal axis perpendicu- lar to the plane of the scapula, internal/external rotation around a vertical axis through the plane of the scapula and anterior/posterior tilt around a horizontal axis in the plane of the scapula. 1 The clavicle acts as a strut for the shoulder com- plex, connecting the scapula to the central por- tion of the body. This allows two translations to occur—upward/downward translation on the thoracic wall and retraction/protraction around the rounded thorax. 1 When the humerus moves into elevation, clavicular elevation, retraction and posterior axial rotation occur at the sternoclavicu- lar joint, while scapular internal rotation, upward rotation and posterior tilting occur at the acro- mioclavicular joint. 2 Both the acromioclavicular and sternoclavicular joints contribute to scapular upward rotation with up to 31° of clavicular pos- terior rotation occurring at the sternoclavicular joint. 2 The acromioclavicular joint is primarily responsible for the occurrence of scapular poste- rior tilting. Sternoclavicular joint retraction and acromioclavicular joint internal rotation are off- setting motions allowing scapular internal and external rotation to occur. 2 The scapula plays several roles in normal shoul- der function. Control of static position and con- trol of the motions and translations allow the scapula to fulfi l these roles. In addition to upward rotation, the scapula must also posteriorly tilt and externally rotate to clear the acromion from the moving arm in forward elevation or abduction. Also, the scapula must synchronously internally/ externally rotate and posteriorly tilt to maintain the glenoid as a congruent socket for the moving arm and maximise concavity compression and ball and socket kinematics. The scapula must be dynamically stabilised in a position of rela- tive retraction during arm use to maximise acti- vation of all the muscles that originate on the scapula. 3 4 Finally, it is a link in the kinetic chain of integrated segment motions that starts from the ground and ends at the hand. Because of the important but minimal bony stabilisation of the scapula by the clavicle, dynamic muscle function is the major method by which the scapula is sta- bilised and purposefully moved to accomplish its roles. Muscle activation is coordinated in task- specific force couple patterns to allow stabilisa- tion of position and control of dynamic coupled motion. Abnormal scapular motion and/or position have been collectively called ‘scapular winging’, ‘scapular dyskinesia’ and more appropriately ‘scapular dyskinesis’. Scapular winging refers to prominence of the medial border of the scapula, which is most often associated with long thoracic nerve palsy, and in some cases, overt scapular muscle weakness. ‘Winging’ describes a visual abnormality but it fails to indicate whether the abnormality is static, dynamic or both. Scapular dyskinesia by strict defi nition implies that a loss of voluntary motion has occurred. However, only the scapular translations (elevation/depression and retraction/protraction) can be performed voluntarily, whereas the scapular rotations are accessory in nature. Therefore, the term ‘dyski- nesia’ is not always appropriate when describing abnormal scapular motion. Scapular dyskinesis (‘dys’—alteration of, ‘kine- sis’—movement) is a collective term that refers to movement of the scapula that is dysfunctional. Scapular dyskinesis has been identified by a group of experts as: (1) abnormal static scapular posi- tion and/or dynamic scapular motion character- ised by medial border prominence; or (2) inferior angle prominence and/or early scapular elevation
Transcript of 50225452.pdf

Shoulder injuries in athletes
Br J Sports Med 2010;44:300–305. doi:10.1136/bjsm.2009.058834300
Shoulder Center of Kentucky, Lexington, Kentucky, USA
Correspondence to Aaron Sciascia, Shoulder Center of Kentucky, 700 Bob-O-Link, Lexington, KY 40504, USA; [email protected]
Accepted 13 October 2009
Current concepts: scapular dyskinesisW Ben Kibler, Aaron Sciascia
ABSTRACTThe scapula serves many roles in order for proper
shoulder function to occur. These roles include providing
synchronous scapular rotation during humeral motion,
serving as a stable base for rotator cuff activation and
functioning as a link in the kinetic chain. Each role is
vital to proper arm function and can only occur when
the anatomy around the shoulder is uncompromised.
The presence of bony and soft tissue injury as well as
muscle weakness and infl exibility can alter the roles
of the scapula and alter scapular resting position and/
or dynamic motion. This altered scapular position/
movement has been termed ‘scapular dyskinesis’.
Although it occurs in a large number of shoulder
injuries, it appears that scapular dyskinesis is a
non-specifi c response to a painful condition in the
shoulder rather than a specifi c response to certain
glenohumeral pathology. The presence or absence of
scapular dyskinesis needs to be determined during
the clinical examination. An examination consisting of
visual inspection of the scapular position at rest and
during dynamic humeral movements, along with the
performance of objective posture measurements and
scapular corrective maneuvers, will help the clinician
ascertain the extent to which the scapula is involved
in the shoulder injury. Treatment of scapular dyskinesis
should begin with optimised anatomy and then progress
to the restoration of dynamic scapular stability by
strengthening of the scapular stabilisers utilising kinetic
chain-based rehabilitation protocols.
Normal scapulohumeral rhythm, the coordinated movement of the scapula and humerus to achieve shoulder motion, is the key to effi cient shoulder function. Scapular position and motion are closely integrated with arm motion to accomplish most shoulder functions. Scapular movement is a com-posite of three motions—upward/downward rotation around a horizontal axis perpendicu-lar to the plane of the scapula, internal/external rotation around a vertical axis through the plane of the scapula and anterior/posterior tilt around a horizontal axis in the plane of the scapula.1 The clavicle acts as a strut for the shoulder com-plex, connecting the scapula to the central por-tion of the body. This allows two translations to occur—upward/downward translation on the thoracic wall and retraction/protraction around the rounded thorax.1 When the humerus moves into elevation, clavicular elevation, retraction and posterior axial rotation occur at the sternoclavicu-lar joint, while scapular internal rotation, upward rotation and posterior tilting occur at the acro-mioclavicular joint.2 Both the acromioclavicular and sternoclavicular joints contribute to scapular upward rotation with up to 31° of clavicular pos-terior rotation occurring at the sternoclavicular
joint.2 The acromioclavicular joint is primarily responsible for the occurrence of scapular poste-rior tilting. Sternoclavicular joint retraction and acromioclavicular joint internal rotation are off-setting motions allowing scapular internal and external rotation to occur.2
The scapula plays several roles in normal shoul-der function. Control of static position and con-trol of the motions and translations allow the scapula to fulfi l these roles. In addition to upward rotation, the scapula must also posteriorly tilt and externally rotate to clear the acromion from the moving arm in forward elevation or abduction. Also, the scapula must synchronously internally/externally rotate and posteriorly tilt to maintain the glenoid as a congruent socket for the moving arm and maximise concavity compression and ball and socket kinematics. The scapula must be dynamically stabilised in a position of rela-tive retraction during arm use to maximise acti-vation of all the muscles that originate on the scapula.3 4 Finally, it is a link in the kinetic chain of integrated segment motions that starts from the ground and ends at the hand. Because of the important but minimal bony stabilisation of the scapula by the clavicle, dynamic muscle function is the major method by which the scapula is sta-bilised and purposefully moved to accomplish its roles. Muscle activation is coordinated in task-specifi c force couple patterns to allow stabilisa-tion of position and control of dynamic coupled motion.
Abnormal scapular motion and/or position have been collectively called ‘scapular winging’, ‘scapular dyskinesia’ and more appropriately ‘scapular dyskinesis’. Scapular winging refers to prominence of the medial border of the scapula, which is most often associated with long thoracic nerve palsy, and in some cases, overt scapular muscle weakness. ‘Winging’ describes a visual abnormality but it fails to indicate whether the abnormality is static, dynamic or both. Scapular dyskinesia by strict defi nition implies that a loss of voluntary motion has occurred. However, only the scapular translations (elevation/depression and retraction/protraction) can be performed voluntarily, whereas the scapular rotations are accessory in nature. Therefore, the term ‘dyski-nesia’ is not always appropriate when describing abnormal scapular motion.
Scapular dyskinesis (‘dys’—alteration of, ‘kine-sis’—movement) is a collective term that refers to movement of the scapula that is dysfunctional. Scapular dyskinesis has been identifi ed by a group of experts as: (1) abnormal static scapular posi-tion and/or dynamic scapular motion character-ised by medial border prominence; or (2) inferior angle prominence and/or early scapular elevation
02_sm058834&sm070805.indd 30002_sm058834&sm070805.indd 300 3/13/2010 3:15:37 PM3/13/2010 3:15:37 PM

Shoulder injuries in athletes
Br J Sports Med 2010;44:300–305. doi:10.1136/bjsm.2009.058834 301
or shrugging on arm elevation; and/or (3) rapid downward rotation during arm lowering.5 However, static position and dynamic motion are two separate entities, so when describing the static appearance of the scapula and if an asymmetry is observed, it should be referred to as ‘altered scapular resting position’ rather than ‘scapular dyskinesis’.
Scapular dyskinesis is a non-specifi c response to a painful condition in the shoulder rather than a specifi c response to certain glenohumeral pathology. Scapular dyskinesis has mul-tiple causative factors, both proximally (muscle weakness/imbalance, nerve injury) and distally (acromioclavicular joint injury, superior labral tears, rotator cuff injury) based. This dyskinesis can alter the roles of the scapula in the scapula–humeral rhythm.6 It can be due to alterations in the bony sta-bilisers, alterations in muscle activation patterns or strength in the dynamic muscle stabilisers.
DYNAMIC SCAPULAR STABILITYPrimary scapular stabilisation and motion on the thorax involves coupling of the upper and lower fi bres of the trape-zius muscle with the serratus anterior and rhomboid muscles. Other muscles such as the pectoralis minor also play a role. Elevation of the scapula with arm elevation is accomplished through activation and coupling of the serratus anterior and lower trapezius with the upper trapezius and rhomboids.7 8 During this motion, the lower trapezius helps maintain the instant centre of rotation of the scapula through its attach-ment to the medial scapular spine. Its attachment to the scap-ular spine allows for a straight line of pull as the arm elevates and the scapula rotates upwardly, and creates a mechanical advantage to maintain this position. The lower trapezius has often been identifi ed as an upward rotator of the scapula because it maintains its long moment arm during the full range of upward rotation.8 However, it also plays a role as a scapular stabiliser when the arm is lowered from an elevated position. During the descent or return from upward elevation, the well-positioned lower trapezius, when operating effi ciently, helps maintain the scapula against the thorax.
The serratus anterior also plays a role as a stabiliser of the scapula. This muscle has been historically identifi ed as a pro-tractor of the scapula due to high electromyographic activity elicited during various push-up maneuvers.9 Other evidence suggests the serratus muscle helps rotate the scapula upwardly. The serratus anterior is actually multifaceted in that it con-tributes to all components of three-dimensional motion of the scapula during arm elevation. The serratus anterior helps produce scapular upward rotation, posterior tilt and external rotation while stabilising the medial border and inferior angle, which prevents scapular winging.10 This is most likely caused by the variable fi bre orientation of the serratus anterior on the scapula and thorax. The highest level of serratus anterior acti-vation occurs in the cocking phase of the throwing motion, and serratus anterior activation occurs in the earliest stages of arm elevation. It would appear that a prime role of the serra-tus in these activities is as an external rotator/stabiliser of the scapula with arm motion.
The scapular position that allows optimal muscle activa-tion of the shoulder joint muscles to occur is that of retraction and external rotation. Scapular retraction is an obligatory and integral part of a normal scapula–humeral rhythm in coupled shoulder motions and functions. It results from synergistic muscle activations in patterns from the hip and trunk through the scapula to the arm, which then facilitates maximal muscle activation of the muscles attached to the scapula. The retracted
scapula can then act as a stable base for the origin of all the rotator cuff muscles.
As these roles are key components of normal shoulder function, alterations in the roles may play a part in shoulder dysfunction. Research has demonstrated alterations of scapu-lar motion and position in association with a wide variety of shoulder injuries.
SCAPULAR DYSKINESIS AND SHOULDER INJURYPatho-anatomyThe clavicle largely exists to assist the scapula in shoulder func-tion by helping maintain optimal scapular position during arm motion.2 In this manner, it acts as a strut for the shoulder as it attaches the arm to the axial skeleton via the acromioclavicu-lar and sternoclavicular joints. The scapula relies on bony and soft tissue structures for stability, and when intact these struc-tures are what allow the scapular rotations and translations to occur; therefore, an uncompromised clavicle and acromio-clavicular joint are imperative components to maintaining scapular integrity. Injury to any of the static restraints can cause the scapula to become unstable, which in turn will neg-atively affect arm function.
Acromioclavicular separationsInjuries to the stabilising ligaments of the acromioclavicu-lar joint are quite common. The dysfunction that occurs as a result of acromioclavicular joint subluxation or dislocation results from the dissociation of the scapula from the support-ing strut of the clavicle. Gravity displaces the scapula down-ward and there is a concomitant scapular protraction and internal rotation such that the scapula is displaced medial to the acromioclavicular joint creating a ‘third translation’.11 With the displacement of the scapula there are signifi cant functional consequences to the biomechanics of the shoulder. There is an uncoupling of the scapulohumeral complex such that the scapular stabilising muscles are not able to maintain appro-priate positioning of the glenohumeral and acromiohumeral joints. There is a subsequent loss of rotator cuff strength and function that can only be restored by retraction of the scapula and restoring the pivot point of the acromioclavicular joint. Surgical correction of the damaged anatomy in high-grade acromioclavicular separations should be based on restoring the coupled clavicular/scapular motion.
Clavicle fracturesFractures of the clavicle, with either non-union or shortened rotated malunion, also alter the strut function and can result in poor functional patient outcomes. The functional defi cien-cies most often seen in association with low scores on the outcomes measures in malunion and/or non-union of clavicle fractures are muscle weakness and/or loss of range of motion. The altered strut function of the clavicle allows excessive pro-traction of the scapula, which has been shown to be a position that limits rotator cuff function and the humerus’ capability of achieving full elevation. Surgical treatment for clavicle frac-tures should be based on returning clavicle length, angulation and rotational contour to normal to maintain maximal clavicle strut function.
ImpingementImpingement is the most commonly diagnosed problem around the shoulder. There are at least 10 specifi c diagnoses
02_sm058834&sm070805.indd 30102_sm058834&sm070805.indd 301 3/13/2010 3:15:37 PM3/13/2010 3:15:37 PM

Shoulder injuries in athletes
Br J Sports Med 2010;44:300–305. doi:10.1136/bjsm.2009.058834302
that may be associated with impingement.12 Each diagnosis contains a component that may either affect the width of the subacromial space or be the driving factor of pain. Scapular dyskinesis is associated with impingement by altering arm motion upon dynamic elevation and scapular position at rest.13 Scapular dyskinesis in injured patients is characterised by a loss of acromial upward rotation, excessive scapular internal rotation and excessive scapular anterior tilt.13 These positions create scapular protraction, which decreases the subacromial space and decreases demonstrated rotator cuff strength.
Activation sequencing patterns and strength of the muscles that stabilise the scapula are altered in patients with impinge-ment and scapular dyskinesis.14 Whereas each muscle attach-ing to the scapula makes a specifi c contribution to scapular function, the lower trapezius and serratus anterior appear to play the major role in stabilising the scapula during arm movement. Weakness, fatigue or injury in either of these mus-cles may cause a disruption of the dynamic stability, which can lead to abnormal kinematics thus causing symptoms of impingement.
Increased upper trapezius activity, imbalance of upper trapezius/lower trapezius activation and decreased serratus anterior activity have been reported in patients with impingement.13 14 Increased upper trapezius activity is clinically observed as a shrug manoeuvre, resulting in a type III (upper medial bor-der prominence) dyskinesis pattern. This causes impingement due to lack of acromial elevation. Frequently, lower trapezius activation is inhibited or is delayed. This results in a type III/type II (entire medial border prominence) dyskinesis pattern, with impingement due to loss of acromial elevation and pos-terior tilt. Serratus anterior activation has been shown to be decreased in patients with impingement, creating a lack of external rotation.13
Rotator cuff injuryThere may be several reasons why muscles demonstrate weak-ness. Some factors, such as actual injury, disuse atrophy and inhibition due to pain, are intrinsic to the muscle and create an absolute weakness. Other factors, such as lack of a stable base of origin or decreased facilitation by proximal muscle activa-tion patterns, are extrinsic to the muscle and create an appar-ent weakness even though the muscle itself may be capable of developing strength.
Positions of scapular protraction have been shown to be limiting to maximal rotator cuff strength. Kebaetse et al15 showed that excessive scapular protraction, a posture that is frequently seen in injured patients with scapular dyski-nesis, decreased maximum rotator cuff strength by 23%. Smith et al16 showed that maximal rotator cuff strength was achieved in association with a position of ‘neutral scapular protraction/retraction’, and that the positions of excessive protraction or retraction demonstrated decreased rotator cuff abduction strength. Kibler et al3 showed supraspinatus strength increased up to 24% in a position of scapular retrac-tion in subjects with shoulder pain and 11% in subjects with-out shoulder pain.
The clinically observable fi nding in scapular dyskinesis, prominence of the medial scapular border, is associated with the biomechanical position of scapular internal rotation and protraction. The protracted scapula is a less than optimal base for muscle strength. One time evaluation or test–retest follow-up of rotator cuff strength should be performed with a stabilised scapula, in order to measure true rotator cuff activation.
Multidirectional instabilityScapular dyskinesis is often associated with an unstable gle-nohumeral joint. It is more often seen in microtraumatic types of instability such as multidirectional instability, but can also be seen in recurrent types of instability with traumatic origins. The lax capsular tissue is only one component of the unsta-ble shoulder. Altered biomechanics and muscle activations also increase the dysfunction. Studies have demonstrated that many patients with multidirectional instability have altered scapula–humeral rhythm, increased protraction of the scapula and simultaneous humeral head migration away from the cen-tre of the joint.17 18
Muscle activation studies have shown that increased pro-traction is due to a combination of increased pectoralis minor and latissimus dorsi activation and decreased lower trapezius and serratus anterior activation. Rotator cuff activation and biceps activation is seen to increase to try to compensate for the altered scapula–humeral rhythm that tends to allow the humeral head to migrate away from the joint centre.18
Labral injuryScapular dyskinesis is part of the pathological cascade of labral injury described by Burkhart et al.19 Myers et al20 reported higher incidences of labral lesions in throwing athletes who had scapular dyskinesis. The altered scapular positioning and/or movement allows undue stress to occur to the anterior shoulder structures and increases the posterior ‘peel-back’ of the biceps on the glenoid labrum.19
Another component of the pathological cascade is a defi -cit of glenohumeral internal rotation, in comparison with the opposite shoulder, and as an alteration in total rotation (inter-nal plus external rotation) in comparison with the opposite shoulder.19 These alterations have been designated as gle-nohumeral internal rotation defi cit. In addition to the known alteration of glenohumeral kinematics, glenohumeral internal rotation defi cit affects normal scapula–humeral rhythm by creating a ‘wind-up’ effect in which the glenoid and scapula are pulled in a forward inferior direction by the moving arm. This dyskinetic pattern can create an excessive amount of protraction of the scapula on the thorax as the arm continues into an adducted position in follow-through during throw-ing or into forward elevation in working. The ellipsoid shape of the thorax allows the scapula to move disproportion-ately anteriorly and inferiorly with more scapular protrac-tion. These motions subsequently decrease the subacromial space during active motion, which allows impingement-type symptoms to occur. With regard to labral pathology, exces-sive scapular protraction creates glenoid antetilt, which increases the compression and shear forces on the posterior superior labrum.21
EVALUATIONThe goals of the physical examination of the scapula are to establish the presence or absence of scapular dyskine-sis and altered scapular resting position, to evaluate prox-imal and distal causative factors, and to employ dynamic maneuvers to assess the effect of correction of dyskinesis on impingement symptoms. The results of the examination will aid in establishing the complete diagnosis of all the ele-ments of the dysfunction and will help guide treatment and rehabilitation.
Objective measurement
02_sm058834&sm070805.indd 30202_sm058834&sm070805.indd 302 3/13/2010 3:15:37 PM3/13/2010 3:15:37 PM

Shoulder injuries in athletes
Br J Sports Med 2010;44:300–305. doi:10.1136/bjsm.2009.058834 303
Coracoid-based infl exibility can be assessed by palpation of the pectoralis minor and the short head of the biceps bra-chii at their insertion on the coracoid tip. They will usually be tender to palpation, even if they are not symptomatic in use, can be traced to their insertions as taut bands, and will create symptoms of soreness and stiffness when the scapu-lae are manually maximally retracted and the arm is slightly abducted to approximately 40–50°. A rough measurement of pectoralis minor tightness may be obtained by standing the patient against the wall and measuring the distance from the wall to the anterior acromial tip. This can be done using a ‘double square’ device with the patient standing with his or her back against a wall (fi gure 1).22 A bilateral measurement is taken (in inches or centimetres) to determine if there is a notable difference between the involved and non-involved shoulder.
Visual observationThe scapular examination should largely be accomplished from the posterior aspect. The scapula should be exposed for complete visualisation. This can be done by gowning, a tank top, or by removing the shirt. The resting posture should be checked for side-to-side asymmetry but especially for evi-dence of inferior medial or medial border prominence. If there is diffi culty with determining the positions, marking the superior and inferior medial borders may help ascertain the position.
Dynamic scapular motions may be evaluated by hav-ing the patient move the arms in ascent and descent three to fi ve times. This will usually bring out any weakness in the muscles and display the dyskinetic patterns. Motion in forward fl exion is most likely to demonstrate medial bor-der prominence. If necessary, more repetitions, up to 10, or the addition of 3–5 lb weights will highlight the weakness even more.23 24 Prominence of any part of the medial bor-der is recorded in a ‘yes’ (present) or ‘no’ (absent) fashion.25 This evaluation system shows a clinical utility of 0.64–0.84 between the clinical examination and the biomechanical fi ndings.25
Corrective maneuversThe scapular assistance test (SAT) and scapular retraction test (SRT) are corrective maneuvers that may alter the injury symptoms and provide information about the role of scapular
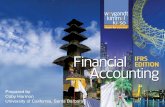
dyskinesis in the total picture of dysfunction that accompa-nies shoulder injury and needs to be restored.3 5 The SAT helps evaluate scapular contributions to impingement and rotator cuff strength and the SRT evaluates contributions to rotator cuff strength and labral symptoms. In the SAT, the exam-iner applies gentle pressure to assist scapular upward rotation and posterior tilt as the patient elevates the arm (fi gure 2).6 A positive result occurs when the painful arc of impingement symptoms is relieved and the arc of motion is increased. In the SRT, the examiner grades the supraspinatus muscle strength following standard manual muscle testing procedures or eval-uates labral injury with the dynamic labral shear test.3 The clinician then places and stabilises the scapula in a retracted position (fi gure 3). A positive test occurs when the demon-strated supraspinatus strength is increased or the symptoms of internal impingement in the labral injury are relieved in the retracted position. Although these tests are not capable of diag-nosing a specifi c form of shoulder pathology, a positive SAT or SRT shows that scapular dyskinesis is directly involved in pro-ducing the symptoms and indicates the need for the inclusion of early scapular rehabilitation exercises to improve scapular control.
TREATMENTTreatment of scapular dyskinesis will only be successful if the anatomical base is optimal. The earliest assessments in patients with scapular dyskinesis should evaluate for local problems such as nerve injury or scapular muscle detachment, which will not respond to therapy until they are repaired. Similarly, bony and/or tissue derangement issues such as acro-mioclavicular separation, fractured clavicles, labral injury, rotator cuff disease or glenohumeral instability, may require surgical repair before the dyskinesis can be addressed. The large majority of cases of dyskinesis, however, are caused by muscle weakness, inhibition or infl exibility, and can be man-aged with rehabilitation.
Rehabilitation emphasis for scapular dyskinesis should start proximally and end distally. The goal of initial therapy is to achieve the position of optimal scapular function—posterior tilt, external rotation and upward elevation. Proximal control of core stability, which leads to control of three-dimensional scapular motion, is achieved through an integrated rehabilita-tion regimen in which the larger muscles of the lower extrem-ity and trunk are utilised during the treatment of the scapula
Figure 1 Double square posture measure. Figure 2 Scapular assistance test.
02_sm058834&sm070805.indd 30302_sm058834&sm070805.indd 303 3/13/2010 3:15:38 PM3/13/2010 3:15:38 PM

Shoulder injuries in athletes
Br J Sports Med 2010;44:300–305. doi:10.1136/bjsm.2009.058834304
and shoulder.26 Hip and trunk fl exion help facilitate scapular protraction, whereas hip and trunk extension along with trunk rotation aid in facilitating scapular retraction. It is important to note that if strength or fl exibility defi cits exist within the proximal segments (core, pelvis, hip, etc) then they should be addressed before treating the scapula and/or shoulder.
The serratus anterior is most important as an external rota-tor of the scapula, and the lower trapezius acts as a stabiliser of the acquired scapular position. Scapular stabilisation protocols should focus on re-educating these muscles to act as dynamic scapula stabilisers, fi rst by the implementation of short lever, kinetic chain assisted exercises then progress to long lever movements. Maximal rotator cuff strength is achieved off a stabilised, retracted scapula. Rotator cuff emphasis in rehabil-itation should be after scapular control is achieved and should emphasise closed chain, humeral head co-contractions.26 An increase in impingement pain when doing open chain rota-tor cuff exercises indicates the wrong emphasis at the wrong stage of the rehabilitation protocol. A logical progression of exercises (going from isometric to dynamic) focused on strengthening the lower trapezius and serratus anterior while minimising upper trapezius activation has been described in the literature.27 All of the exercises may be implemented in a preoperative therapy protocol designed to correct defi cits and prepare for postoperative rehabilitation; however, in the event the anatomy needs to be protected, such as after labral or rota-tor cuff repair, dynamic exercises can be started later and pro-gressed as healing allows.
Competing interests None.
Patient consent Not obtained.
Provenance and peer review Commissioned; not externally peer reviewed.
REFERENCES 1. McClure PM, Michener LA, Sennett BJ, et al. Direct 3-dimensional
measurement of scapular kinematics during dynamic movements in vivo. J
Shoulder Elbow Surg 2001;10:269–77.
2. Ludewig PM, Phadke V, Braman JP, et al. Motion of the shoulder complex during
multiplanar humeral elevation. J Bone Joint Surg Am 2009;91:378–89.
3. Kibler WB, Sciascia A, Dome D. Evaluation of apparent and absolute
supraspinatus strength in patients with shoulder injury using the scapular
retraction test. Am J Sports Med 2006;34:1643–7.
4. Smith J, Dietrich CT, Kotajarvi BR, et al. The effect of scapular protraction on
isometric shoulder rotation strength in normal subjects. J Shoulder Elbow Surg
2006;15:339–43.
5. Second Scapula Summit. Unpublished consensus statement. Lexington,
Kentucky, USA. 20 July 2006.
6. Kibler WB. The role of the scapula in shoulder function. Am J Sports Med
1998;26:325–37.
7. Bagg SD, Forrest WJ. Electromyographic study of the scapular rotators during
arm abduction in the scapular plane. Am J Phys Med 1986;65:111–24.
8. Bagg SD, Forrest WJ. A biomechanical analysis of scapular rotation during arm
abduction in the scapular plane. Am J Phys Med Rehabil 1988;67:238–45.
9. Decker MJ, Hintermeister RA, Faber KJ, et al. Serratus anterior muscle activity
during selected rehabilitation exercises. Am J Sports Med 1999;27:784–91.
10. Ludewig PM, Cook TM, Nawoczenski D. Three dimensional scapular orientation
and muscle activity at selected positions of humeral elevation. J Ortho Sports
Phys Ther 1996;24:57–65 .
11. Kibler WB, Sciascia AD, Wolf B, et al. Nonacute shoulder injuries. In: Kibler
WB, ed. Orthopedic knowledge update: sports medicine 4 American academy
of orthopaedic surgeons. Rosemont, Illinois, USA: American Academy of
Orthopaedic Surgeons, 2009:19–40.
12. Kibler WB, Sciascia A. What went wrong and what to do about it: pitfalls in the
treatment of shoulder impingement. In: Duwelius PJ, Azar FM, eds. Instructional
course lectures. Rosemont, Illinois, USA: American Academy of Orthopaedic
Surgeons, 2008:103–12.
What is already known about this topic
▶ Scapular dyskinesis can exist in the presence of shoulder injury.
▶ Scapular dyskinesis is a non-specifi c response to a painful condition in the shoulder rather than a specifi c response to certain glenohumeral pathology.
▶ Scapular dyskinesis can be effectively treated through conservative treatment.
What this study adds
▶ This paper provides a clear defi nition of scapular dyskinesis and why this term should be use when describing altered scapular motion.
▶ This paper identifi es the scapular alterations and/or dysfunction that may occur when the surrounding bony and/or soft tissue anatomy of the shoulder girdle is compromised due to various types of injury.
▶ This paper summarises various evidence-based methods of establishing the presence or absence of scapular dyskinesis, all of which have been documented in recent literature.
Figure 3 (A, B) Scapular retraction test.
B
A
02_sm058834&sm070805.indd 30402_sm058834&sm070805.indd 304 3/13/2010 3:15:40 PM3/13/2010 3:15:40 PM

Shoulder injuries in athletes
305Br J Sports Med April 2010 Vol 44 No 5
13. Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated
muscle activity in people with symptoms of shoulder impingement. Phys Ther
2000;80:276–91.
14. Cools AM, Witvrouw EE, Declercq GA, et al. Scapular muscle recruitment
patterns: trapezius muscle latency with and without impingement symptoms.
Am J Sports Med 2003;31:542–9.
15. Kebaetse M, McClure P, Pratt NA. Thoracic position effect on shoulder range
of motion, strength, and three-dimensional scapular kinematics. Arch Phys Med
Rehabil 1999;80:945–50.
16. Smith J, Kotajarvi BR, Padgett DJ, et al. Effect of scapular protraction and retraction
on isometric shoulder elevation strength. Arch Phys Med Rehabil 2002;83:367–70.
17. Ogston JB, Ludewig PM. Differences in 3-dimensional shoulder kinematics
between persons with multidirectional instability and asymptomatic controls.
Am J Sports Med 2007;35:1361–70.
18. Illyés A, Kiss RM. Kinematic and muscle activity characteristics of
multidirectional shoulder joint instability during elevation. Knee Surg Sports
Traumatol Arthrosc 2006;14:673–85.
19. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of
pathology Part I: pathoanatomy and biomechanics. Arthroscopy 2003;19:404–20.
20. Myers JB, Laudner KG, Pasquale MR, et al. Scapular position and orientation in
throwing athletes. Am J Sports Med 2005;33:263–71.
21. Burkhart SS, Morgan CD, Kibler WB. Shoulder injuries in overhead
athletes. The “dead arm” revisited. Clin Sports Med 2000;
19:125–58.
22. Kluemper M, Uhl TL, Hazelrigg H. Effect of stretching and strengthening shoulder
muscles on forward shoulder posture in competitive swimmers. J Sport Rehabil
2006;15:58–70.
23. McClure P, Tate AR, Kareha S, et al. A clinical method for identifying scapular
dyskinesis, part 1: reliability. J Athl Train 2009;44:160–4.
24. Tate AR, McClure P, Kareha S, et al. A clinical method for identifying scapular
dyskinesis, part 2: validity. J Athl Train 2009;44:165–73.
25. Uhl TL, Kibler WB, Gecewich B, et al. Evaluation of clinical assessment methods
for scapular dyskinesis. Arthroscopy 2009;25:1240–8.
26. Kibler WB, McMullen J, Uhl TL. Shoulder rehabilitation strategies, guidelines,
and practice. Oper Tech Sports Med 2000;8:258–67.
27. Kibler WB, Sciascia AD, Uhl TL, et al. Electromyographic analysis of specifi c
exercises for scapular control in early phases of shoulder rehabilitation. Am J
Sports Med 2008;36:1789–98.
02_sm058834&sm070805.indd 30502_sm058834&sm070805.indd 305 3/13/2010 3:15:45 PM3/13/2010 3:15:45 PM

Copyright of British Journal of Sports Medicine is the property of BMJ Publishing Group and its content may
not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.