5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel
29
5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease David T. Rubin, MD Associate Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Ui it f Chi M di lC t University of Chicago Medical Center
Transcript of 5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel

5-ASA Therapy, Steroids and Antibiotics in
Inflammatory Bowel Disease
David T. Rubin, MDAssociate Professor of Medicine
Co-Director, Inflammatory Bowel Disease CenterU i it f Chi M di l C tUniversity of Chicago Medical Center

Relevant DisclosuresP t d G bl Ph ti l• Procter and Gamble Pharmaceuticals: consulting and grant support
• Salix Pharmaceuticals: grant support• Shire Pharmaceuticals: consulting

Treatment Goals 2008… and beyondCURRENTCURRENT• Early accurate diagnosis• Rapid effective induction of remission • Stable steroid-free maintenance of remission• Prevention of complications
Disease related– Disease related– Therapy related
• Improved quality of life
NEAR FUTURE….• Incorporation of mucosal healing into plans for better outcomesIncorporation of mucosal healing into plans for better outcomes• Understanding of the “right” therapy at the “right” time (use of
prognostic markers and individualized therapies early in disease course)

Outdated “Therapeutic Pyramids”Ulcerative ColitisCrohn’s Disease Ulcerative Colitis
Surgery
Crohn’s Disease
SurgeryInfliximab Severe
Fulminant
Systemic Corticosteroids
Cyclosporine
InfliximabMTX
AZA/6-MPSystemic Steroids
Moderate
Aminosalicylates
BudesonideAntibiotics
5-ASAMild

“Conventional” Therapeutic ApproachS it d f t di t t fi t li th i• Severity and safety dictate first line therapies
– NOT prognosis or likelihood of response• Patients have to prove they need something
“stronger” or “riskier”• The chronicity of the disease is sometimes an
afterthought– Induction therapy dictates choice of
maintenance therapyBetter long term outcomes are an added– Better long term outcomes are an added bonus
• Usually less expensive (in the short run)

5-ASA Therapy in IBD• Effective in induction and maintenance of
mild-moderate UC– May have benefit in mild CD- insufficient
evidence • E l ti f lti l d d t• Evolution from multiple doses per day to
single dose• Simplified dosing regimen = increased patient
adherence• Topical therapy plus oral therapy is betterTopical therapy plus oral therapy is better
than oral alone• Unclear whether switching is effective• Chemopreventive benefits

Details of Mesalamine Delivery Systems
5-ASA 5-ASAN=N5-ASAN N
N=N
SulfasalazineNHSO2
Sulfapyridine
COOH
CH
Olsalazine
MesalamineControlled-release capsules
Su apy d e
5-ASA5-ASA 5-ASA
Balsalazide disodiumcapsules
(ABA)
NaOOC
OH5-ASA
MesalamineRectal suspension enema/
suppositoryMesalamine
Gastro-resistant/pH(Lialda)
MesalamineDelayed-release capsules
(Asacol)
(ABA)inert
carrier
OH
EthylcelluloseMicrospheres
Eudragit S MMX technology
5-ASA
5-ASA

Oral Mesalamine for mild-to-moderate UC
R (%)*Response (%)*Study Disease Status Placebo Mesalamine (g)
0.8 1.6 2.4 4.8Schroeder1
(6 weeks)Active 18
(n=38)27
(n=11)74
(n=38)Sninsky2
(6 weeks)Active 23
(n=52)43**
(n=53)49***
(n=53)Hanauer3
(6 months)Maintenance 48
(n=87)63†
(n=90)70††
(n=87)
1Schroeder, et al. N Engl J Med. 1987. 2Sninsky, et al. Ann Internal Med. 1991.
3Hanauer, et al. Ann Internal Med. 1996.
*Response defined as Schroeder: Combined complete and partial response Sninsky: Patients who improved and were in remission Hanauer: Maintenance of remission
**P=0.03, ***P=0.003, †P=0.05, ††P=0.005

1.00
Granulated Mesalamine: ITT PopulationKaplan-Meier Plot of Relapse-Free Duration
Granulated Mesalamine 1.5 g/d
Placebo
ty
0.75
Prob
abili
t
0.25
0.50
p<0.05
Days
0 100 200 300
Lichtenstein, et al. ACG 2008.

Delayed-Release Mesalamine:Dose Response at Week 6
ASCEND II1 ASCEND III2
Trea
tmen
t W
eek
6 (%
)
Mild UC (n=110)
5972P<0.05
60708090
100
66 70P=NS
Trea
tmen
t W
eek
6 (%
)Moderate UC (n= 772)
60708090
100
Moderate UC (n= 254)
3340P=NS
Patie
nts
With
TSu
cces
s at
W
2.4 g/day 4.8 g/day D l d R l M l i *
0102030405060
* Asacol®
Patie
nts
With
TSu
cces
s at
W
2.4 g/day 4.8 g/day D l d R l M l i *
0102030405060
Delayed-Release Mesalamine*
2. Sandborn WJ et al. DDW 2008.
Delayed-Release Mesalamine*
1. Hanauer SB et al. Am J Gastroenterol. 2005;100:2478.

Kamm et al1
Dose Response at Week 8: Delayed Release Mesalamine in Mild to Moderate UC
100 Kamm et al1
Lichtenstein et al2
s in
Clin
ical
En
dosc
opic
n at
Wee
k 8
(%)
41 41P=0.01* P=0.007*
405060708090
100
* P-values represent active treatment vs. placebo† Lialda™
2.4 g/day
Patie
ntan
d E
Rem
issi
on
Placebo
22
4.8 g/day
13
3429
P<0.001* P=0.009*
010203040
1. Kamm MA et al. Gastroenterology. 2007;132:66. 2. Lichtenstein GR et al. Clin Gastroenterol Hepatol.2007;5:95.
Delayed Release Mesalamine†

Treatment of Distal UC: Oral and Topical Mesalamine Therapy
100 Oral (2.4 g/d)Rectal (4 g/d)Combined
*
port
ing
edin
g (%
)
100
60
80
Patie
nts
Rep
No
Rec
tal B
lee
40
20
6 Weeks0
*P<0.002 vs oral alone, P=0.04 vs topical alone.
Adapted from Safdi M et al. Am J Gastroenterol. 1997;92:1867.

Mesalamine 4 g total PO
Extensive Mild/Moderate UC: Oral and Rectal Mesalamine Therapy
89
62
nts
(%)
Mesalamine 4 g total PO (in divided doses; 2 g BID) + mesalamine enema 1 g HS (N=71)
P=NS
P=0.0008
Mesalamine 4 g total PO (in divided doses; 2 g BID) + placebo enema HS (N=56)
60708090
100
44
34
No.
of P
atie
n P=NS
102030405060
Remission Improvement
Week 4
Marteau P et al. Gut. 2005;54:960.
0

Meta-Analysis of Mesalamine* (4 g/day) in Active Crohn’s Disease
0 0
40
-30
-20
-10
0
m B
asel
ine
Sco
re
30
-20
-10
0
P=0.7 P=0.05
P=0.04
80
-70
-60
-50
-40
Cha
nge
From
in C
DA
I
P=0.005
P=0.7
P=0.05
P=0.04
60
-50
-40
-30
P=0.005
*Controlled-release capsules Hanauer S et al. Clin Gastroenterol Hepatol. 2004;2:379.
Mesalamine* 4 g Placebo
Crohn’s In=155
Crohn’s IIn=150
Crohn’s IIIn=310
Overalln=615
Mesalamine* 4 g minus placebo
Crohn’s In=155
Crohn’s IIn=150
Crohn’s IIIn=310
Overalln=615
-80 -60

Mesalamine Maintenance ofRemission in Crohn’s Disease
Study Year Pts (n)
McLeod 1995 163Brignola 1995 87Sutherland 1997 66Overall 411
Thomson 1990 248Prantera 1992 125
Caprilli 1994 95
Brignola 1992 44Gendre 1993 161Bresci 1994 66Thomson 1995 286Arber 1995 59Modigliani 1996 85Sutherland 1997 180De Franchis 1997 117
Favors Treatment Favors ControlRisk Difference 95% CI
Overall 1,371De Franchis 1997 117
-0.5 0.50.40.30.20.10.0-0.1-0.2-0.3-0.4
Adapted from Cammà C et al. Gastroenterology. 1997;113:1465-1473 with permission from American Gastroenterological Association.

Does It Matter Which Aminosalicylate Is Used?
• D li t f di• Deliver to area of disease• Insurance and adherence issues• Don’t settle for less than remission!• Rationale that delivery system may make a difference,
but untested/unprovenbut u tested/u p o e• Oral aminosalicylates share more than
they differ– Pharmacokinetics– Clinical efficacy– Adverse events
• Different for prodrugs– Sulfapyridine– Looser stools
• Monitor renal function for all

Corticosteroid Therapy in IBDEff ti i UC d CD• Effective in UC and CD
• The need (or choice) of steroids is a prognostic marker
– May represent a “tipping point” needing other therapies for maintenancetherapies for maintenance
– Have an exit strategy!• Systemic corticosteroids demonstrate
substantial toxicity at higher doses and for longer periods of timelonger periods of time
• The development of non-systemic steroid formulations provide benefit with less toxicity

Corticosteroid Therapy
St d Di St id/ D R (%)*Study Disease State
Steroid/ Dose Response (%)*
Steroid PlaceboTruelove1
(6 weeks)Active Cortisone ≥
100 mg69
(n=109)41
(n=101)
Lennard-Jones2
(6 months)
Maintenance Prednisone 15 mg
38 (n=34)
40 (n=35)
Truelove3
(5 days)Severely
activePrednisolone
60 mg73 N/A
(5 days) active 60 mg (Total n=49)
1Truelove, et al. Br Med J. 1955;2:1041.2Lennard-Jones, et al. Lancet. 1965;1:188.
3Truelove, et al. Lancet. 1974;1:1067.
*Response defined as Truelove: Patients who improved and were in remission Lennard-Jones: Maintenance of remissionTruelove: Patients in remission
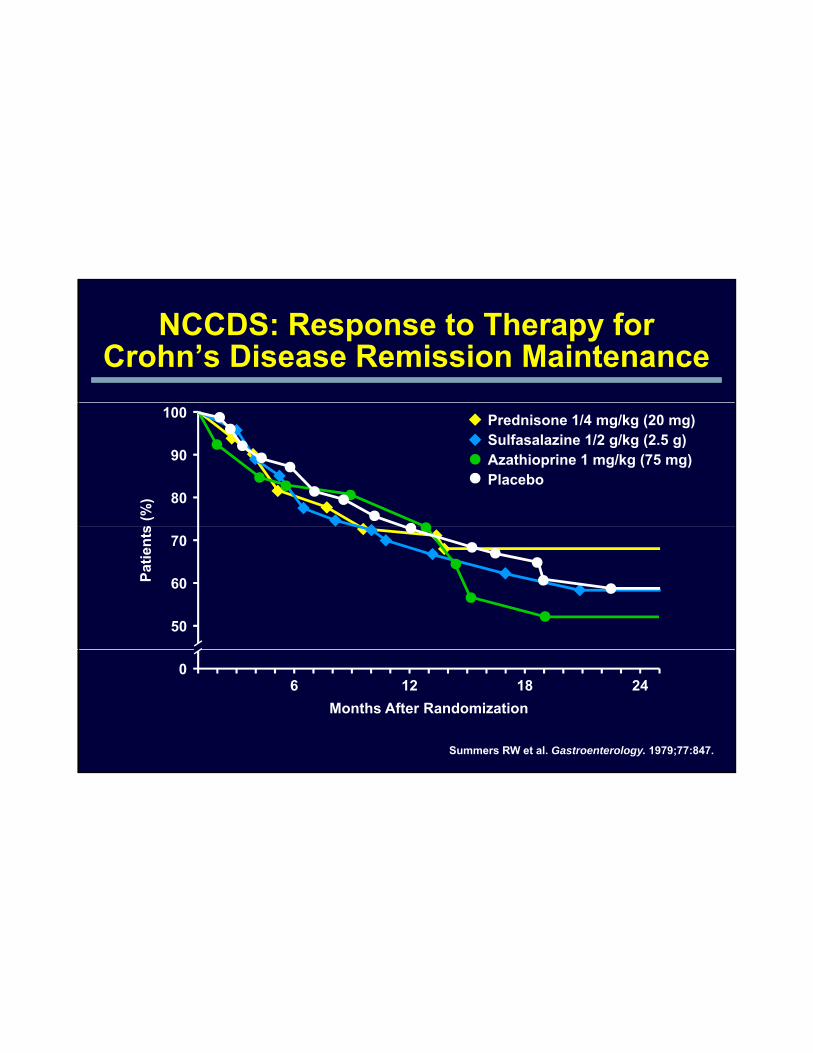
NCCDS: Response to Therapy for Crohn’s Disease Remission Maintenance
100
90
80
Prednisone 1/4 mg/kg (20 mg)
Placebo
Sulfasalazine 1/2 g/kg (2.5 g)Azathioprine 1 mg/kg (75 mg)
70
50
60
0
Months After Randomization2418126
Summers RW et al. Gastroenterology. 1979;77:847.

Corticosteroids: Short- and Long-Term Efficacy in UC
1-Month Outcomes*(n=63)
Complete Remission
54%(n=34)
Partial Remission
30%(n=19)
No Response 16%
(n=10)
1-YearOutcomes
Steroid Dependent
Prolonged Response Surgery
( ) ( )
*30 days after initiating corticosteroid therapy Faubion W, et al. Gastroenterology. 2001;121:255.
Outcomes(n=63)
Dependent22%
(n=14)
Response49%
(n=31)
29%(n=18)

Corticosteroids: Short- and Long-Term Efficacy in Crohn’s Disease
30-DayResponses(n=74)
None 16% (n=12)
Complete 58%(n=43)
Partial26%(n=19)
1-YearResponses
Prolonged response
Steroid dependent Surgery
38%
Faubion WA Jr. et al. Gastroenterology. 2001;121:255.
Responses(n=74)*
*1 patient lost to follow-up
p28%(n=21)
p32%(n=24)
38%(n=28)

Mortality Associated with Current and Recent Corticosteroid Use – Adjusted HR (95% CI)
2.813
4
5
atio
2.49
1
2
3
Haz
ard
Ra
Lewis JD, et al. Am J Gastroenterol. 2008;103:1428-1435.
0 95% CI: (2.26-3.5) 95% CI: (1.65-3.75)
Recent Use of Corticosteroids
Current Use of Corticosteroids

Oral Budesonide: Efficacy as Maintenance Therapy
Prob
abili
tyss
ion
Budesonide 6 mgBudesonide 3 mgPlacebo
1.00.9
0.70.8
0.6
Cum
ulat
ive
Pof
Rem
is
0.4
0.2
0.5
0.3
0.10.0
Time (Days)
300100 2000
Adapted from Greenberg GR et al. Gastroenterology. 1996;110:45-51 with permission from American Gastroenterological Association.

Antibiotic Therapy in IBD• Less rigorously studied• Less rigorously studied• Crohn’s disease:
– Infectious complications– Peri-anal disease– Crohn’s colitis– Crohn s colitis – Prevention of post-op recurrence – Small bowel bacterial overgrowth
• Ulcerative colitis:– No convincing evidence of primary efficacyg p y y– Prophylaxis when on cyclosporine therapy
• Pouchitis

Therapy of Active Crohn’s Disease150150 p= 05
AI
AI 5050
100100
150150PlaceboMetronidazolep=NS
p=.005
p=.05
Cha
nge
in C
DA
Cha
nge
in C
DA
--5050
00
No difference in clinical remission rates.No difference in clinical remission rates.Sutherland L, et al. Sutherland L, et al. Gut.Gut. 1991;32(9):10711991;32(9):1071--1075.1075.
CC
--100100Small intestineSmall intestinen=24n=24
Small/LargeSmall/Largeintestineintestinen=31n=31
Large intestineLarge intestinen=8n=8

Antibiotics in Active CD
emis
sion
(%)
40
50
60
70
0
Patie
nts
in R
e
10
20
30
0Metro + Ciprovs Me-Pred1
Ciprovs Mesalamine3*
Metrovs SASP2
1. Prantera C et al. Am J Gastroenterol. 1996;91:328.2. Ursing B et al. Gastroenterology. 1982;83:550.
3. Colombel JF et al. Am J Gastroenterol. 1999;94:674.Metro, metronidazole; Me-Pred, methylprednisolone;Cipro, ciprofloxacin; SASP, sulfasalazine
*Mesalamine controlled-release capsules

Ornidazole Post-op Prophylaxisin Crohn’s Disease
p=0.09
p=0 02 p=NSp=S54%
48%45%
79%
59%60
80
100OrnidazolePlacebo
rren
ce
p=.046
p=.036
p= 002p=.1
p=.27
p=0.02
p=<0.044
p=NS35%
27%
8%
34%
%45%37%
0
20
40
% o
f Rec
ur p=.002
N=800
3 Months 12 Months 12 Months 24 Months 36 Months
Endoscopic Clinical
Rutgeerts P, et al. Gastroenterology. 2005 Apr;128(4):856-61.

Antibiotics in Pouchitis
• Uncontrolled trials:• Uncontrolled trials: – Oral metronidazole or ciprofloxacin: 96% response1
– Local metronidazole (40-160 mg/d per rectum): 11/11 patients responded2
– Oral rifaximin (1 g BID) + ciprofloxacin (500 mg bid): 86% f 386% improvement in refractory disease3
• Controlled trial: metronidazole (400 mg PO TID):↓ stool frequency, no change endoscopy4
1. Hurst RD, et al. Arch Surg. 1996;131:497-500.2. Nygaard K, et al. Scand J Gastroenterol. 1994;29:462-467.3. Gionchetti P, et al. Gastroenterology. 1997;119:A981.4. Madden MV, et al. Dig Dis Sci. 1994;39:1193-1196.

Conclusions: 5-ASA, Steroids and Antibiotics in IBD
• 5 ASA th i ff ti f i d ti d• 5-ASA therapy is effective for induction and maintenance of UC, limited in CD
– Topical therapy is effective for distal and additive in extensive UC.– There does not appear to be a dose-response for oral 5-ASA in UC.– Simplified dosing regimens and delivery systems have provided
many options for patients and providers.y p p p• Corticosteroids remain effective induction agents in
UC and CD– Should be considered markers of disease prognosis and paired
with effective maintenance strategies.– Limited by toxicity- non-systemic steroids provide new options.
B d t tibi ti h i t t l i• Broad-spectrum antibiotics have an important role in infectious complications of IBD and for pouchitis
– Despite interest in the “infectious cause of IBD” this remains elusive.