48.full

of 12
-
Upload
hawania-ii -
Category
Documents
-
view
11 -
download
0
description
jurnal paru
Transcript of 48.full
-
Image: Janulla, iStockphoto
Key points
Bronchial thermoplasty, which involves the delivery of radio frequency energy to the airways, is a nonpharmacological intervention developed for the treatment of patients with moderate-to-severe asthma that is poorly controlled despite maximal therapy
Randomised controlled clinical trials of bronchial thermoplasty in patients with moderate and severe asthma have shown modest improvements in asthma quality of life and clinically worthwhile reductions in severe exacerbations and emergency department visits
The treatment involves three bronchoscopy sessions with repeated, precise and carefully recorded activations of a radiofrequency catheter within the medium and large airways
Bronchial thermoplasty causes short-term increases in asthma-related morbidity including increased admissions to hospital for asthma; follow-up data, to date, supports the long-term safety of the procedure
-
How to: Bronchial thermoplastyin asthma
Educational aims
N To provide an overview on how to perform bronchial thermoplasty for thetreatment of asthma
N To summarise the development, mode of action and evidence for theeffectiveness of bronchial thermoplasty as well as its place in the managementof asthma
Summary
Bronchial thermoplasty, which involves the delivery of radio frequency energy tothe airways, is a nonpharmacological intervention developed for the treatment ofmoderate-to-severe asthma. The mode of action of bronchial thermoplasty is notestablished, but could be due to reduction in airway smooth muscle massinduced by thermal energy. Bronchial thermoplasty results in modestimprovements in asthma quality of life questionnaire scores and clinicallyworthwhile reductions in severe exacerbations and emergency department visitsin the year post-treatment, which may persist for up to 5 years.
The procedure involves systematic, controlled heating of the airways usingdedicated radiofrequency equipment during a series of three bronchoscopysessions. Bronchial thermoplasty causes short-term increases in asthma-relatedmorbidity, including hospital admissions. Follow-up data, to date, supports thelong-term safety of the procedure. Bronchial thermoplasty is a novel treatmentoption for selected patients with moderate-to-severe asthma that is poorlycontrolled despite maximal therapy.
HERMES syllabus link:modules B.1.1, D.2.11
Statement of InterestThe authors have allbeen investigators inthe AIR, RISA and AIR 2clinical studies andreceived institutionalfunding for research.N. Thomson hasreceived grants andfees for lectures fromBoston Scientific.
ERS 2014
Breathe | March 2014 | Volume 10 | No 1 49DOI: 10.1183/20734735.007813
Stephen Bicknell,
Rekha Chaudhuri,
Neil C. Thomson
Respiratory Medicine,Gartnavel General Hospital,Glasgow, andInstitute of Infection,Immunity andInflammation, University ofGlasgow, Glasgow, UK
S. Bicknell, RespiratoryMedicine, GartnavelGeneral Hospital, GlasgowG12 OYN, UK
-
BackgroundAsthma is a chronic inflammatory disease ofthe airways that affects over 300 millionpeople worldwide, and over 30 million chil-dren and adults in Europe. Patients with moresevere asthma, which accounts for 510% ofcases, experience considerable morbidity andgenerate high healthcare costs despite cur-rent therapies. Bronchial thermoplasty, whichinvolves the delivery of radio frequency energyto the airways, is a nonpharmacologicalintervention developed for the treatment ofmoderate-to-severe asthma [1]. This articleprovides an overview on how to performbronchial thermoplasty and summarises thedevelopment, mode of action and evidence
for the effectiveness of bronchial thermo-plasty as well as its place in the managementof asthma.
Development and mode of action ofbronchial thermoplasty
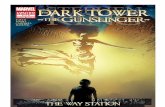
Airway remodelling in asthma includes anincrease in airway smooth muscle mass [2],particularly in severe disease [3], which maycontribute to impaired lung function, airwayhyperresponsiveness and poor symptomcontrol [4, 5]. Bronchial thermoplasty wasdeveloped as a nonpharmacological treat-ment to reduce the amount of airway smoothmuscle by delivering radio frequency energyto the airways with the aim of improvingclinical outcomes in asthma. In support ofthis hypothesis there are data indicating thatbronchial thermoplasty treatment of airways.3 mm diameter, at a temperature of 65uC,reduces smooth muscle mass in experi-mental animals (fig. 1) [6] and in non-asthmatics undergoing lobectomy [7], as wellas preliminary data suggesting that this effectmay also occur in asthma [8]. In addition,bronchial thermoplasty treatment of canineairways decreases airway responsiveness tomethacholine for at least 3 years post-treat-ment and increases airway size measured bycomputed tomography [6, 9, 10].
The mode of action of bronchial thermo-plasty remains uncertain and, in particular, itis not clear if a reduction in the amount ofairway smooth muscle accounts for itsefficacy in the treatment of asthma. Severalother mechanisms, either alone or in com-bination, could explain the beneficial effectsof bronchial thermoplasty in the treatment ofasthma. For example, bronchial thermoplastymight alter airway function by reducingcontractility of airway smooth muscle [11] orby stiffening the airway wall [6] or by reducingthe secretion of pro-inflammatory mediatorsfrom airway smooth muscle cells [5]. Inaddition, it is possible that bronchial thermo-plasty might alter airway epithelial, neural orinflammatory cell function. A placebo effectmay also contribute to some of the improve-ments in clinical outcome measures follow-ing bronchial thermoplasty [1215].
Efficacy of bronchial thermoplasty
Evidence for the efficacy of bronchial thermo-plasty in the treatment of asthma is based on
70
80
90
100a)
b)
60
50
40
30
20
10
0
Air
way
res
pons
iven
ess
% d
ecre
ase
in a
irw
ay d
iam
eter
aft
er M
Ch
Untreated control airway
Follow-up time weeks
Treated airway (65C)
200 40
Parenchyma
Parenchyma
8060 100 120 140 180
Control
55C
65C
75C
160
Seromucousgland Seromucous
gland
Ciliatedepithelium
Ciliatedepithelium
ASM
ASM absent
Figure 1Effect of treatment with bronchial thermoplasty at different temperature on airwayresponsiveness to methacholine (MCh) and airway pathology in dogs. a) Airwayresponsiveness (percentage change in diameter after local MCh challenge) in dogstreated with bronchial thermoplasty at 55uC, 65uC and 75uC. b) Histological changes inuntreated control airway and an airway treated with radiofrequency energy at 65uC,12 weeks post-treatment (trichrome stain, original magnification x100). Airway smoothmuscle (ASM) in the untreated airway is unchanged compared to the reduction inairway smooth muscle in the treated airway. Reproduced from [6] with permission fromthe publisher.
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 150
-
the results of three randomised controlledtrials, two of which compared bronchialthermoplasty with usual care [13, 14] andone with a sham procedure [15], plus asystematic review and meta-analysis of thesetrials [16].
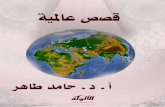
In the Asthma Intervention Research(AIR) trial 112 adults with moderate or severeasthma were randomised to bronchial ther-moplasty treatment or usual care (controlgroup) [13]. Bronchial thermoplasty reducedthe rate of mild exacerbations comparedwith the control group and also resultedin improvements in morning peak expira-tory flow (PEF), Asthma Quality of LifeQuestionnaire (AQLQ) and Asthma ControlQuestionnaire (ACQ) scores at 12 months. Inthe Research in Severe Asthma (RISA) trialthe safety and efficacy of bronchial thermo-plasty was compared to usual care in 34patients with severe asthma, half of whomwere also taking oral prednisolone daily [14].Bronchial thermoplasty resulted in improve-ments in ACQ scores and rescue medicationuse at 52 weeks, and although more subjectsin the bronchial thermoplasty group weanedoff oral corticosteroids the difference was notstatistically significant compared with theusual care group. The AIR2 trial comparedbronchial thermoplasty with a sham proced-ure in 288 adult subjects with severe asthmarandomised to the active procedure in a ratioof two to one [15]. Bronchial thermoplastyresulted in improvements in AQLQ scorecompared with the sham group (1.35 forbronchial thermoplasty versus 1.16 for sham),with 79% of bronchial thermoplasty and 64%of sham participants achieving changes inAQLQ of o0.5 (fig. 2a). In the post-treat-ment period (from the end of the treatmentperiod up to 1 year post-treatment), there wasa 32% reduction in severe exacerbations and84% fewer emergency department visits withbronchial thermoplasty (fig. 2b). A systematicreview and meta-analysis of the three trialsconcluded that bronchial thermoplastyimproves AQLQ scores and PEF [16]. Anobservational follow-up study of 92% ofpatients who completed the AIR2 trialreported that the reduction in the proportionof subjects experiencing severe exacerba-tions and emergency department visits afterbronchial thermoplasty is maintained up to5 years (fig. 3). Severe exacerbations in yearfive after bronchial thermoplasty occurredin 22% of patients, compared with 31% in
year one and 52% in the year prior tothe intervention [17]. Compared with the12 months before bronchial thermoplasty,the average reduction over the 5 years inthe proportion of subjects with emergencydepartment visits for respiratory symptomswas 78%. The decrease in rate of emergencydepartment visits that was achieved afterbronchial thermoplasty in year one wasmaintained out to 5 years [17].
Taken together, these clinical studiessuggest that bronchial thermoplasty treat-ment results in a modest improvement inAQLQ scores and clinically worthwhile reduc-tions in severe exacerbations and emergencydepartment visits in the year after treatmentand also suggest that these benefits maypersist for at least 5 years. However, bron-chial thermoplasty produces no consistentimprovement in forced expiratory volume in1 s (FEV1) or airway responsiveness.
Patient selectionAssessment and management of difficultto control asthma
It is important that patients are assessed at aspecialist asthma clinic prior to considerationfor bronchial thermoplasty. A systematicevaluation should be performed to identifypatients with severe asthma and differentiatefrom those with difficult-to-treat asthma dueto poor adherence, untreated comorbidities,dysfunctional breathing or psychological pro-blems [18, 19]. Once it is established that thepatient has severe refractory asthma and isreceiving maximal therapy, bronchial thermo-plasty is a potential treatment option.
Selection criteria
When selecting patients for this procedurecaution is advised as efficacy and safetyinformation is available only for patientswho satisfied the inclusion criteria for thepivotal clinical trials of the procedure (seethe box Eligibility criteria for bronchial ther-moplasty used in pivotal clinical trials).In patients with severe asthma who falloutside these entry criteria, such as a post-bronchodilator FEV1 ,65% predicted, use oforal corticosteroids in excess of 10 mg perday for asthma or greater than four exacer-bations of asthma in the past year, there islimited information on the safety of bronchialthermoplasty treatment and caution should
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 1 51
-
be exercised in treating such patients. In theRISA study more severe patients, with FEV1 aslow as 55% predicted post-salbutamol andhigher daily doses of oral prednisolone(f30 mg per day), were treated safelyalthough the numbers in this study weresmall (n515) [14].
Patient information about bronchialthermoplasty
The balance of risks and benefits of bronchialthermoplasty treatment should be discussedwith patients being considered for the pro-cedure. Patients should be given writteninformation to take home to read andconsider after a face to face discussion withthe physician. Information sheets for patientsbeing considered for bronchial thermoplastyare available online [23, 24].
Bronchial thermoplastyprocedureThe procedure should be performed atfacilities that are appropriately equipped toperform bronchoscopy and are equipped tohandle respiratory emergencies. Respira-tory physicians undertaking bronchialthermoplasty should be experienced inbronchoscopy. Training is required by themanufacturer and is available in diffe-rent formats: didactic technical reviewof the equipment; bronchial thermoplasty
6.0a)
5.5
5.0
AQ
LQ s
core
Month3 6 9 12
0.9b)
0.5
0.6
0.7
0.8
0.4
0.3
0.2
0.1
0
Even
ts p
er s
ubje
ct y
ear
Severeexacerbations
Unscheduledphysician
office visits
Emergencyroomvisits
Hospitalisations
Average score#
5.80BT(n=173)
Sham(n=95)
5.56
5.40
5.485.49
5.685.715.71
+
Sham
BT
Figure 2a) Total Asthma Quality of Life Questionnaire (AQLQ) score over 12 months after treatment with bronchial thermoplasty (BT) in the per protocolpopulation and b) meanSEM healthcare utilisation events during the post-treatment period. Severe exacerbations were defined as exacerbationsrequiring treatment with systemic corticosteroids or doubling of the inhaled corticosteroids dose. #: Posterior probability of superiority 97.9%;": posterior probability of superiority 95.5%; +: posterior probability of superiority 99.9%. Reproduced from [15] with permission from the publisher.
70a)
60
50
40
30
20
10
0
Subj
ects
with
sev
ere
exac
erba
tions
%
Year post-BT
12monthspre-BT
Averageover 5years
1 32 4 5
1.2b)
1.0
0.8
0.6
0.4
0.2
0
Seve
re e
xace
rbat
ions
per
sub
ject
per
yea
r
Year post-BT
12monthspre-BT
Averageover 5years
1 32 4 5
70c)
60
50
40
30
20
10
0
Subj
ects
with
ED
vis
its %
Year post-BT
12monthspre-BT
Averageover 5years
1 32 4 5
1.2d)
1.0
0.8
0.6
0.4
0.2
0
ED v
isits
per
su
bjec
t per
yea
r
Year post-BT
12monthspre-BT
Averageover 5years
1 32 4 5
Figure 3Severe exacerbations and emergency department (ED) visits in the 5 years afterbronchial thermoplasty (BT). a) Proportion of subjects with severe exacerbations and b)severe exacerbation rates. c) Proportion of subjects with ED visits for respiratorysymptoms and d) ED visit rates. Values are point estimates with 95% confidenceintervals. The 365-day period constituting year 1 began at 6 weeks after the lastbronchial thermoplasty bronchoscopy. Reproduced from [17] with permission from thepublisher.
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 152
-
computer-based simulator learning module;or model-based hands-on technical trainingwith bronchoscopy team.
Equipment
The Alair bronchial thermoplasty system(Boston Scientific, Natick, MA, USA) com-prises an Alair radiofrequency controller, an
Alair catheter with an expandable electrodearray (fig. 4), a patient return electrode and asuitable flexible bronchoscope.
The Alair controller contains a radio-frequency generator and additional elementswhich regulate the energy applied to theairways to allow effective treatment withoutunwanted tissue damage. The controller isactivated by a footswitch which triggers atimed period of radiofrequency energy deliv-ered via the Alair catheter.
The Alair catheter is a single use catheterwhich is connected to the controller via anintegral electrical cable. The catheter has abasket electrode at its distal end which can beprogressively expanded and retracted by ahandle-grip control. The catheter has mark-ings at 5 mm intervals to facilitate endobron-chial spacing of treatment activations.
The patient return electrode completesthe electrical circuit. A CE-marked gel typeelectrode for adult use is suitable.
Treatment requires a radiofrequency com-patible flexible bronchoscope with an inser-tion diameter of 4.95.3 mm and a workingchannel of at least 2 mm. Larger broncho-scopes are less suitable because of reducedflexibility and reduced access to the smaller,distal airways.
Contraindications for bronchialthermoplasty
Patients with the following conditionsshould not receive bronchial thermoplastytreatment [22]:
N Presence of a pacemaker, internal defi-brillator or other implantable electronicdevice
N Known sensitivity to medications re-quired to perform bronchoscopy,including lignocaine, atropine andbenzodiazepines
N Patients previously treated with bronchialthermoplasty should not beretreated inthe same area(s), as no clinical data isavailable studying the safety and/oreffectiveness of repeat treatments
Eligibility criteria for bronchial thermoplasty used in pivotal clinical trials
N Adult aged 1865 yearsN Asthma requiring regular maintenance medication that includes inhaled corticosteroids (.1000 mg beclometasone
per day or equivalent) and long-acting b2-agonists, with or without other asthma medications; oral corticosteroids ata dosage f10 mg per day
N AQLQ score [20] of 6.25 or lessN Non-smoker for o1 year or greater (if a former smoker, ,10 pack-years total smoking history)N Post-bronchodilator FEV1 o 65% predictedN Not excessively using their short-acting bronchodilator (in excess of 12 puffs per day within 48 h of bronchoscopy,
excluding prophylactic use for exercise)N None of the following within the past 12 months:o4 lower respiratory tract infections;o4 oral corticosteroid pulses for asthma exacerbation;o3 hospitalisations for respiratory symptoms
N No history of intubation for asthma or intensive care unit admission for asthma within the prior 24 monthsN No evidence of other respiratory diseases including emphysema, vocal cord dysfunction, mechanical upper airway
obstruction, cystic fibrosis or uncontrolled obstructive sleep apnoeaN No conditions associated with increased risk for adverse events associated with bronchoscopy or anaesthesia, such
as pregnancy, insulin dependent diabetes, epilepsy or other significant comorbidities (e.g. uncontrolled coronaryartery disease, acute or chronic renal failure and uncontrolled hypertension)
N Patient considered suitable for bronchoscopy
Data from [21].
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 1 53
-
Pre-procedure patient preparation
Oral corticosteroids: administer prophylacticprednisolone or equivalent at a dose of 50 mgper day for the 3 days before the procedure,the day of the procedure and the day afterthe procedure to minimise post-procedureinflammation. This is the dose used in theclinical trials. Locally we use 40 or 50 mgprednisolone depending on the asthmaseverity and body weight, for 2 days prior tothe procedure, the day of the bronchialthermoplasty and 2 days after the procedure.We provide patients with a further 5-dayssupply of prednisolone and advise them touse it only in the event of significant worseningof asthma symptoms post-procedure.
Pre-procedure spirometry: on the dayof procedure, perform a post-bronchodilatorFEV1 to assess the patients stability pre- andpost-procedure. Pre-procedure FEV1 valueshould beo85% of the patients recent valuewhen stable.
As with other bronchoscopy procedures,patients should stop taking anticoagulants,antiplatelet agents, aspirin and non-steroidalanti-inflammatory drugs before the procedurewith physician guidance.
The procedure should be postponed if anyof the following conditions apply [21]:
N Prescribed prednisolone was not taken onthe days before bronchoscopy
N Arterial oxygen saturation measured bypulse oximetry ,90% on room air
N Increase in asthma symptoms in last 48 hrequiring .4 puffs per day on average ofrescue bronchodilator over pretreatmentusage
N Asthma exacerbation or changing dose ofsystemic corticosteroids for asthma in thepast 14 days
N Active respiratory infection or active aller-gic sinusitis
N Any other reason for clinical instability
Bronchoscopic procedure
Bronchial thermoplasty can be delivered byoutpatient flexible bronchoscopy under con-scious sedation. However, the procedure ismore protracted and more technicallydemanding than routine bronchoscopy andmany other interventional bronchoscopy tech-niques [25, 26]. The combination of atechnically challenging procedure applied toasthmatic subjects with capacity for abruptalterations in airway conditions must beaddressed by a clinical team with expertisein complex bronchoscopy and regular experi-ence of severe asthma. Delivery of bronchialthermoplasty involves close cooperationbetween the bronchoscope operator and thecatheter operator and these two individualsshould have practiced the manoeuvresinvolved together, prior to the procedure.
Following a format established in theprincipal clinical trials, patients receive treat-ment over three bronchoscopy sessionsspaced at approximately 1 month intervals,one for each lower lobe and one for bothupper lobes (fig. 5). The right middle lobe hasnot been treated because of theoreticalconcerns about causing stenosis of therelatively long middle lobe bronchus leadingto middle-lobe syndrome. Patients should beeducated with regard to the practicalities ofthe procedure to reduce anxiety and facilitatecooperation.
The bronchoscopy must be performed ina facility equipped to deal with medicalemergencies including potential treatment-related complications such as pneumothoraxand haemoptysis. Before starting thebronchoscopy procedure the team checkscorrect assembly of the Alair system, includ-ing correct placement of the patient returnelectrode. The Alair catheter is checked withparticular regard to smooth and symmetricaldeployment of the catheter array and if thedeployment is not satisfactory another cath-eter is chosen. Nebulised salbutamol isadministered prior to bronchoscopy. In ourpractice, patients are given an anti-secretory
Figure 4Alair system for bronchial thermoplasty: catheter andradiofrequency controller. Image courtesy of BostonScientific Corporation.
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 154
-
agent, such as glycopyrrolate or atropine, andare sedated, usually with a combination of ashort-acting benzodiazepine (such as mid-azolam) and an opiate (such as alfentanil).Administration of effective topical anaesthe-sia before and during the bronchoscopy is ofcritical importance due to the significantmechanical and thermal irritation inherentto the procedure. As the procedures aresignificantly longer than standard diagnosticbronchoscopy, it is usually necessary to givefurther aliquots of sedation during thetreatment. It is important the cumulativetreatment is documented accurately and thatclinical governance is in place with regard tocomplexities of these procedures.
The bronchoscope can be inserted viathe nose or mouth with the patient ina recumbent or semi-recumbent positionaccording to the teams usual practice.
The area to be treated is first inspected toplan the sequence of treatment. The approachshould be systematic to avoid missing orretreating bronchi, with consideration given totreating the most accessible bronchi first. Thisallows maximum coverage of the airways inthe event of mucosal oedema occurring whenmanipulating the catheter into less accessiblebronchi. If mucosal oedema does start to limitaccess to the airways the authors find that thiscan be reduced by the application of smallaliquots of dilute adrenaline (1:10 000, i.e.0.1mg?mL-1).
Following treatment planning, the bron-choscope is placed in the distal aspect of theairway being treated and the Alair catheter isadvanced under visual guidance (fig. 6). Theelectrode array is then expanded to makecontact with the airway wall, and the foots-witch is depressed to deliver radiofrequencyenergy for 10 s. If electrode contact isinadequate the unit will alarm and abort thetreatment. The system is only activated whenthe electrode array is within vision andthroughout the procedure care must be takento avoid damage to the distal airways. Caremust be taken to avoid over-expansion of thecatheter array which tends to invert theelectrodes, progressive but gentle squeezingof the catheter handle until the electrodes arejust touching the airway wall is most effective.After activation of the catheter the operatorrelaxes the handle, collapsing the electrodesslightly away from the airway wall and thebronchoscope operator then moves thebronchoscope and catheter 5 mm proximally.
This sequence is repeated until the full lengthof each airway has been treated. The sites ofthe various activations are recorded on asuitable airway map. An experienced teamwill typically complete each treatment sessionin ,45 min.
At the start of the second and thirdprocedures, the airways treated in the pre-vious procedure are carefully inspected forpersisting inflammation or infection and ifthis were present, delay of treatment shouldbe considered.
Post-procedure
It is recommended that patients should becarefully monitored and discharged only afterthey are deemed to be stable, and haveadequate lung function, mental status andare able to take liquids adequately. Patientsare rarely required to stay overnight.
Recommended post-procedure assess-ments: 1) 4 h recovery/monitoring periodfollowing each procedure; and 2) spirometry,breath sounds and vital signs (heart rate,blood pressure, temperature, respiratory rate,pulse oximetry) prior to discharge. Criteria fordischarge include a post-bronchodilator FEV1within 80% of the pre-procedure value andthat the patient is feeling well.
Figure 5Map of the large airways used to record the number of activations undertaken in eachsegment during each bronchial thermoplasty procedure. Image courtesy of BostonScientific Corporation.
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 1 55
-
Short-term adverse effects ofbronchial thermoplastyBronchial thermoplasty is associated with ashort-term increase in asthma-related mor-bidity, including increased hospital admis-sion for asthma [1315]. The main adverseeffects in the treatment phase are wheeze,cough, chest discomfort, night awakeningand discoloured sputum with most adverseevents occurring in the first day after broncho-scopy and resolving within a week. In the AIRstudy there were more hospitalisations in thebronchial thermoplasty group in the treatmentphase of the study (six hospitalisations in foursubjects) compared with the control group[13]. The RISA trial of patients with severeasthma reported seven hospitalisations forrespiratory symptoms in four subjects in thebronchial thermoplasty group during thetreatment period, five for asthma and two forpartial lobar collapse, compared with noadmission to hospital in this period for thecontrol group [14]. In the pivotal AIR2 studyduring the treatment period 16 subjects(8.4%) required 19 hospitalisations in thebronchial thermoplasty group compared withtwo subjects (2.0%) in the sham group [15].
Other commonly reported side-effects wereincreased upper respiratory tract infection,headache and dyspepsia. Details of adverseevents that occurred more commonly in thethermoplasty treated group compared to thesham treated group are presented in table 1.
Long-term safetyThe long-term safety of bronchial thermo-plasty up to 5 years post-procedure has been
completed in patients with moderate-to-severe asthma included in the three rando-mised controlled trials and in those recruitedto an observational trial in patients with mildasthma (table 1). The rate of respiratoryadverse events was unchanged in years twoto five following bronchial thermoplasty in theAIR trial [27], RISA trial [28] and AIR2 trial [17].Lung function was stable and there was noincrease in hospital admissions or emergencydepartment visits for respiratory symptomsbetween years one and five (fig. 3). Inaddition, computed tomography scans takenat baseline and annually for 5 years afterbronchial thermoplasty showed no clinicallysignificant changes in the airways such as
Catheter placeddistally in airway,electrode arrayexpanded andcontroller activated
Electrode arraypartially collapsedand moved 5 mmproximal to previousactivation
Electrode array expanded and adjacent but notoverlapping activation completed
Electrode array partially collapsedand moved 5 mmproximal to previous activation
Electrode arrayexpanded and adjacent but not overlapping activation completed
Figure 6Bronchial thermoplasty procedure. Image courtesy of Boston Scientific Corporation.
Advice to the patient post-procedure
N Reminder to take prophylactic predniso-lone as planned
N Caution the patient about the potentialadverse events that they might experi-ence including haemoptysis, fever, coughand worsening of asthma symptoms
N Patients should be advised on appropriateemergency plans if they experience any ofthese adverse events, or asthma symp-toms that are not controlled by theirmedications
N Contact patient via phone calls to assesspost-procedure status
N Clinic visit after 2 weeks to assess clinicalstability and schedule subsequentbronchial thermoplasty procedures asappropriate
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 156
-
bronchiectasis, parenchymal fibrosis or air-way stenosis [17].
Place of bronchial thermoplastyin the management of asthmaBronchial thermoplasty is licensed for thetreatment of asthma in Europe, the USA and
many other counties worldwide. For example,in 2010 the US Food and DrugAdministration approved bronchial thermo-plasty for the treatment of severe persistentasthma in patients aged o18 years whoseasthma is not well controlled with inhaledcorticosteroids and long-acting b-agonists,the current standard of care treatment for
Table 1. Adverse effects of bronchial thermoplasty (BT)#
Treatment period" Post-treatment period+
BT group Sham group BT group Sham group
Subjects n 190 96 187 96
Average duration of period days 84 322
Worsening of asthma 52 39 27 43
Upper respiratory tract infection 20 11 30 26
Wheezing 15 6 4 3
Chest pain 14 13 3 1
Headaches 14 9 5 3
Dyspnoea 11 6 2 1
Chest discomfort 9 10 2 1
Lower respiratory tract infection 8 2 3 6
Nasopharyngitis 5 7 11 5
Atelectasis 5 0 0 0
Bronchitis 4 2 7 5
Anxiety 4 0 1 2
Dyspepsia 4 2 2 4
Haemoptysis 3 0 1 2
Acute sinusitis 3 2 4 8
Rhinitis 2 0 4 6
Influenza 4 2 4 12
Pyrexia 4 2 0 1
Hypertension 3 2 3 3
Urinary tract infection 1 1 3 1
Data are presented as %, unless otherwise stated. #: adverse events .3% frequency that were higher in the BT group compared with the sham treatedgroup; ": the period from first treatment to 6 weeks after last treatment; +: the period from 6 weeks post-treatment to 12 months after last treatment.Data from [21].
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 1 57
-
these patients [22]. In the European Union,the Alair bronchial thermoplasty system has aCE mark for the treatment of asthma inpatients aged o18 years.
The Global Initiative for Asthma guide-lines consensus recommendation is thatbronchial thermoplasty is now a possibleoption in some countries for adults withuncontrolled asthma despite maximal therapyand review by an asthma specialist [29]. Therecommendation adds that longer-term safetyfollow-up of larger numbers of active andcontrol patients is required to assess effec-tiveness and that caution should be exercised
in patient selection for the procedure [29].The British Thoracic Society guideline foradvanced diagnostic and therapeutic flexiblebronchoscopy in adults recommends bron-chial thermoplasty as a possible treatmentoption in selected patients with severeasthma already on maximal therapy, althoughits place in management remains to beestablished (Grade A) [30].
ConclusionBronchial thermoplasty, which involves thedelivery of radio frequency energy to theairways, is a nonpharmacological interventiondeveloped for the treatment of uncontrolledmoderate-to-severe asthma. Bronchial ther-moplasty reduces airway smooth musclemass in experimental animals and produceslong-lasting decreases in airway responsive-ness to methacholine. The mode of action ofbronchial thermoplasty in the treatment ofasthma is not established. Randomisedcontrolled clinical trials of bronchial thermo-plasty in patients with moderate and severeasthma have shown modest improvementsin asthma quality of life and clinically im-portant reductions in severe exacerbationsand emergency room visits. The procedureinvolves a systematic approach requiring exper-tise in complex bronchoscopic interventionalprocedures.
Bronchial thermoplasty is associated withshort-term increases in asthma-related mor-bidity including increased hospitalisations forasthma. 5-year follow-up of patients recruitedto randomised clinical trials of bronchialthermoplasty have reported no increase inrespiratory-related adverse effects. Bronchialthermoplasty is a treatment option forpatients with moderate-to-severe asthmawho have poorly controlled disease despitemaximal therapy.
References
1. Thomson NC, Bicknell S, Chaudhuri R. Bronchialthermoplasty for severe asthma. Curr Opin AllergyClin Immunol 2012; 12: 241248.
2. James AL, Elliot JG, Jones RL, et al. Airway smoothmuscle hypertrophy and hyperplasia in asthma.Am J Respir Crit Care Med 2012; 185: 10581064.
3. Pepe C, Foley S, Shannon J, et al. Differences inairway remodeling between subjects with severe and
moderate asthma. J Allergy Clin Immunol 2005; 116:544549.
4. Solway J, Irvin CG. Airway smooth muscle as a targetfor asthma therapy. N Engl J Med 2007; 356:13671369.
5. Zuyderduyn S, Sukkar MB, Fust A, et al. Treatingasthma means treating airway smooth muscle cells.Eur Respir J 2008; 32: 265274.
Future directions
N Longer term follow-up of treatedpatients is recommended. In the UK, allpatients undergoing bronchialthermoplasty have demographic andprocedure details recorded in the BritishThoracic Society Difficult AsthmaRegistry.
N Studies to date have been unable toidentify factors that predict a therapeuticresponse to bronchial thermoplasty. Aprospective observational study ofbaseline clinical, physiological,biological and imaging predictors ofresponse to bronchial thermoplasty inpatients with severe refractory asthma isunderway, with the aim of recruiting 190subjects [31].
N Future studies need to determine themechanisms accounting for thebeneficial clinical response to bronchialthermoplasty, the long-term effects after5 years, and the feasibility of repeatingthe procedure after 10 years or when theeffect wanes in a patient who respondsinitially.
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 158
-
6. Danek CJ, Lombard CM, Dungworth DL, et al.Reduction in airway hyperresponsiveness to meth-acholine by the application of RF energy in dogs.J Appl Physiol 2004; 97: 19461953.
7. Miller JD, Cox G, Vincic L, et al. A prospectivefeasibility study of bronchial thermoplasty in thehuman airway. Chest 2005; 127: 19992006.
8. Gordon IO, Husain AN, Charbeneau J, et al.Endobronchial biopsy: a guide for asthma therapyselection in the era of bronchial thermoplasty.J Asthma 2013; 50: 634641.
9. Brown RH, Wizeman W, Danek C, et al. In vivoevaluation of the effectiveness of bronchial thermo-plasty with computed tomography. J Appl Physiol2005; 98: 16031606.
10. Brown RH, Wizeman W, Danek C, et al. Effect ofbronchial thermoplasty on airway distensibility. EurRespir J 2005; 26: 277282.
11. Dyrda P, Tazzeo T, DoHarris L, et al. Acute responseof airway muscle to extreme temperature includesdisruption of actin-myosin interaction. Am J RespirCell Mol Biol 2011; 44: 213221.
12. Wechsler ME, Kelley JM, Boyd IOE, et al. Activealbuterol or placebo, sham acupuncture, or nointervention in asthma. N Engl J Med 2011; 365:119126.
13. Cox G, Thomson NC, Rubin AS, et al. Asthma controlduring the year after bronchial thermoplasty.N Engl J Med 2007; 356: 13271337.
14. Pavord ID, Cox G, Thomson NC, et al. Safety andefficacy of bronchial thermoplasty in symptomatic,severe asthma. Am J Respir Crit Care Med 2007; 176:11851191.
15. Castro M, Rubin AS, Laviolette M, et al. Effectivenessand safety of bronchial thermoplasty in the treatmentof severe asthma: a multicenter, randomized, double-blind, sham-controlled clinical trial. Am J Respir CritCare Med 2010; 181: 116124.
16. Wu Q, Xing Y, Zhou X, et al. Meta-analysis of theefficacy and safety of bronchial thermoplasty inpatients with moderate-to-severe persistent asthma.J Int Med Res 2011; 39: 1022.
17. Wechsler ME, Laviolette M, Rubin AS, et al. Bronchialthermoplasty: long-term safety and effectiveness inpatients with severe persistent asthma. J AllergyClinical Immunol 2013; 132: 12951302.
18. Heaney LG, Brightling CE, Menzies-Gow A, et al.Refractory asthma in the UK: cross-sectional findingsfrom a UK multicentre registry. Thorax 2010; 65:787794.
19. Bel EH, Sousa A, Fleming L, et al. Diagnosis anddefinition of severe refractory asthma: an inter-national consensus statement from the InnovativeMedicine Initiative (IMI). Thorax 2011; 66: 910917.
20. Juniper EF, Guyatt GH, Willan A, et al. Determining aminimal important change in a disease-specific qualityof life questionnaire. J Clin Epidemiol 1994; 47: 8187.
21. Boston Scientific. Alair Bronchial ThermoplastySystem. www.btforasthma.com Date last accessed:November 26, 2013.
22. U.S. Food and Drug Administration. Asthmatx, Inc.Alair Bronchial Thermoplasty System - P080032.2010. www.fda.gov/medicaldevices/productsandmedicalprocedures/deviceapprovalsandclearances/recently-approveddevices/ucm212594.htm Date last accessed:November 26, 2013. Date last updated: September 9,2013.
23. Boston Scientific. Is Severe Asthma Controlling YourLife? A patient Guide to Bronchial Thermoplasty.Boston Scientific, 2011. www.btforasthma.com/wp-content/uploads/2013/03/BT-Patient-Guide_English.pdf Date last accessed: November 26, 2013.
24. National Institute for Clinical Excellence.Understanding NICE Guidance. Information forPeople who use NHS Services. Treating SevereAsthma Using Heat Energy to Reduce AirwayNarrowing. NHS, 2012. www.nice.org.uk/nicemedia/live/12774/57934/57934.pdf Date last accessed:November 26, 2013. Date last updated: January 2012.
25. Mayse ML, Laviolette M, Rubin AS, et al. Clinicalpearls for bronchial thermoplasty. J Bronchol 2007;14: 115123.
26. Duhamel DR, Hales JB. Bronchial thermoplasty: anovel therapeutic approach to severe asthma. J VisExp 2010; 45: e2428.
27. Thomson NC, Rubin AS, Niven RM, et al. Long-term(5 year) safety of bronchial thermoplasty: AsthmaIntervention Research (AIR) trial. BMC Pulm Med2011; 11: 8.
28. Pavord ID. 5-year safety of bronchial thermoplastydemonstrated in patients with severe refractoryasthma: Research in Severe Asthma (RISA) Trial.Am J Respir Crit Care Med 2011; 183: A6382.
29. Global Initiative for Asthma (GINA). Global Strategyfor Asthma Management and Prevention. GINA,2012. http://www.ginasthma.org/documents/4 Datelast accessed: November 26, 2013. Date last updated:December, 2012.
30. Du Rand IA, Barber PV, Goldring J, et al. BritishThoracic Society guideline for advanced diagnosticand therapeutic flexible bronchoscopy in adults.Thorax 2011; 66: Suppl. 3, iii1iii21.
31. Castro M. A Prospective Observational Study ofBiopredictors of Bronchial Thermoplasty Response inPatients With Severe Refractory Asthma (BTR Study).http://clinicaltrials.gov/show/NCT01185275 Date lastaccessed: November 26, 2013. Date last updated:December 19, 2012.
Bronchial thermoplasty
Breathe | March 2014 | Volume 10 | No 1 59