47286068
7
Click here to load reader
-
Upload
leydavillagrasa -
Category
Health & Medicine
-
view
102 -
download
0
Transcript of 47286068

Nonsteroidal Anti-Inflammatory Drugs, Aspirin, and CognitiveFunction in the Baltimore Longitudinal Study of Aging
Shari R. Waldstein, PhD,�wz Carrington Rice Wendell, MA,�§ Stephen L. Seliger, MD, MS,k
Luigi Ferrucci, MD, PhD,§ E. Jeffrey Metter, MD,§ and Alan B. Zonderman, PhD§
OBJECTIVES: To examine the relations between the useof nonaspirin, nonsteroidal anti-inflammatory drugs(NSAIDs) and aspirin and age-related change in multipledomains of cognitive function in community-dwelling in-dividuals without dementia.
DESIGN: Longitudinal, with measures obtained on one to18 occasions over up to 45 years.
SETTING: General community.
PARTICIPANTS: A volunteer sample of up to 2,300 par-ticipants from the Baltimore Longitudinal Study of Agingfree of diagnosed dementia.
MEASUREMENTS: At each visit, reported NSAID oraspirin use (yes/no) and tests of verbal and visualmemory, attention, perceptuo-motor speed, confrontationnaming, executive function, and mental status.
RESULTS: Mixed-effects regression models revealed thatNSAID use was associated with less prospective decline onthe Blessed Information-Memory-Concentration (I-M-C)Test, a mental status test weighted for memory and con-centration (Po.001), and Part B of the Trail Making Test, atest of perceptuo-motor speed and mental flexibility(Po.05). In contrast, aspirin use was related to greaterprospective decline on the Blessed I-M-C Test (Po.05) andthe Benton Visual Retention Test, a test of visual memory(Po.001).
CONCLUSION: Consistent with studies of incident de-mentia, NSAID users without dementia displayed less pro-spective decline in cognitive function, but on only twocognitive measures. In contrast, aspirin use was associatedwith greater prospective cognitive decline on select mea-sures, potentially reflecting its common use for vascular
disease prophylaxis. Effect sizes were small, callinginto question clinical significance, although overall publichealth significance may be meaningful. J Am Geriatr Soc58:38–43, 2010.
Key words: NSAIDs; aspirin; cognitive function; neuro-psychology
Alzheimer’s disease and vascular dementia commonlyco-occur,1 and inflammatory mechanisms may play a
critical role in the pathogenesis of both diseases.2 Use ofnonsteroidal anti-inflammatory drugs (NSAIDs) other thanaspirin (referred to hereafter as NSAID use) was associatedwith a lower incidence and prevalence of Alzheimer’s dis-ease in a recent meta-analysis of available data.3 All sub-types of NSAIDs appear to confer similar benefit.4 Onestudy concluded that NSAID use conferred protectionagainst Alzheimer’s disease but not vascular dementia.5 As-pirin, which is frequently prescribed for vascular diseaseprophylaxis and has strong anti-inflammatory properties,may also confer protection with respect to Alzheimer’s dis-ease,6–8 although some studies have found no benefit,9–11 orgreater incidence of Alzheimer’s disease12 or vascular de-mentia13 in aspirin users.
Early neuroprotection may be beneficial to both typesof disease pathogenesis, yet little is known about the po-tential cognitive benefit of NSAID or aspirin use by personswithout dementia or on specific domains of cognitive func-tion. In that regard, diminished prospective decline has beenfound in conjunction with NSAID or aspirin use on theShort Portable Mental Status Questionnaire (SPMSQ)Famental status test.14,15 A recent study found a relationshipbetween NSAID use and less prospective decline on adifferent mental status test (the Modified Mini-Mental StateExamination (3MS)) but only when use was begun in mid-life rather than older age.16 Furthermore, this associationwas more pronounced in persons having one or moreapolipoprotein E e4 alleles. Cross-sectional relations
Address correspondence to Shari R. Waldstein, Department of Psychology,University of Maryland, Baltimore County, 1000 Hilltop Circle, Baltimore,MD 21250. E-mail: [email protected]
DOI: 10.1111/j.1532-5415.2009.02618.x
From the �Department of Psychology, University of Maryland, BaltimoreCounty, and Divisions of wGerontology and kNephrology, Department ofMedicine, School of Medicine, University of Maryland, Baltimore, Maryland;zGeriatric Research Education and Clinical Center, Baltimore VeteransAffairs Medical Center, Baltimore, Maryland; and §Intramural ResearchProgram, National Institute on Aging, National Institutes of Health, Balti-more, Maryland.
JAGS 58:38–43, 2010r 2010, Copyright the AuthorsJournal compilation r 2010, The American Geriatrics Society 0002-8614/10/$15.00

between aspirin and better cognitive function have alsobeen noted.17
The current study examined cross-sectional and longi-tudinal relations between NSAID and aspirin use and cog-nitive function in participants without dementia in theBaltimore Longitudinal Study of Aging (BLSA). A prior re-port from the BLSA noted that the relative risk of Alzhei-mer’s disease in NSAID users was half that of nonusers.11
After exclusion of persons with diagnosed dementia, pro-spective relations were examined between NSAID and as-pirin use and performance on two commonly used mentalstatus tests and on tests reflecting a greater number of do-mains of cognitive function than examined previously (ver-bal and visual memory, attention, perceptuo-motor speed,executive functions, and language).
METHODS
Participants
The BLSA is a prospective study of community-dwellingvolunteers initiated by the National Institute on Aging in1958. Approximately every 2 years, participants visit theGerontology Research Center in Baltimore for medical,psychological, and cognitive testing.18 Beginning in 1986,participants aged 60 and older were administered a more-extensive neuropsychological test battery, so the majority oftests examined herein were available only during visits oc-curring on or after January 1, 1986. Two thousand fivehundred forty-seven BLSA participants (aged 17–102; meanage 52.3 � 17.7) were available for potential inclusion inthe present analyses. Persons with dementia (n 5 247; seeKawas et al.19 for determination of dementia status) at allassessment visits, before and after diagnosis, were excluded.Persons with stroke or renal failure were censored fromthe visit at which diagnosis was recorded. Two thousandthree hundred participants (1,381 men and 919 women)were included in the analyses. Baseline characteristics ofparticipants are presented in Table 1. Because the BLSA usescontinuous enrollment procedures, participants have differ-
ent start times in the project, numbers of visits, and follow-up intervals. The total number of participants according tonumber of visits is listed in Table 2. These participants hadan average of 3.8 � 3.4 (range 1–18) visits, and the averagetime between visits was 3.4 � 1.7 years. Over the course ofthe study, 648 participants died, and 125 formally withdrewfrom the investigation; rate of attrition was therefore33.6%. Institutional Review Board approval was obtainedfrom the Johns Hopkins Bayview Medical Center before2002 and the MedStar Research Institute after 2002. Allparticipants provided written informed consent. The Insti-tutional Review Board of the University of Maryland, Bal-timore County, approved the data analyses.
Neuropsychological Tests
Highly trained psychometricians administered standardneuropsychological tests at each BLSA visit.20 The num-bers that follow each test indicate respective sample sizesbecause of test-specific missing data associated with vari-ability of the neuropsychological battery during differentepochs of the BLSA, as well as scheduling constraints. TheDigits Forward (n 5 1,394) and Backward (n 5 1,397) por-tions of the Wechsler Adult Intelligence ScaleFRevised as-sessed attention and concentration. The California VerbalLearning Test (CVLT) (n 5 1,313) measured verbal learningand memory (learning slope, short and long free recall). TheCVLT learning slope quantifies rate of learning by estimat-ing the slope of item acquisition over the five learning trials,with positive slopes indicating a benefit of additional learn-ing trials. The Benton Visual Retention Test (n 5 2,300)evaluated visual memory. The Trail Making Test Parts A(n 5 1,004) and B (n 5 987) assessed attention, perceptuo-motor speed, visuomotor scanning, and mental flexibility(an executive function). Letter Fluency (n 5 1,008) and
Table 1. Characteristics of Study Sample at FirstAssessment
Characteristic Value
Age, mean � SD (range) 50.6 � 17.4 (17–96)
Education, years, mean � SD (range) 16.6 � 2.7 (4–24)
Male, % 60.0
White, % 82.9
Hypertension, % 36.7
Cardiovascular disease,� % 11.8
Diabetes mellitus, % 3.9
Inflammatory disease,w % 22.5
NSAID use, % 16.2
Aspirin use, % 11.1
Concurrent NSAID and aspirin use, % 3.9
�Chronic cerebrovascular disease, coronary artery disease, and peripheral
arterial disease, coded as a time-dependent binary variable.wOsteoarthritis, rheumatoid arthritis, and rheumatism, coded as a time-
dependent binary variable.
SD 5 standard deviation; NSAID 5 nonsteroidal anti-inflammatory drug.
Table 2. Sample Size According to Number of BaltimoreLongitudinal Study of Aging Visits: Available Data for thePresent Data Analyses
Number of
Visits n (%)
1 2,300 (100.0)
2 1,548 (67.3)
3 1,123 (48.8)
4 885 (38.5)
5 691 (30.0)
6 541 (23.5)
7 433 (18.8)
8 348 (15.1)
9 279 (12.1)
10 199 (8.7)
11 155 (6.7)
12 105 (4.6)
13 70 (3.0)
14 42 (1.8)
15 21 (0.9)
16 10 (0.4)
17 4 (0.2)
18 2 (0.09)
NSAIDS, ASPIRIN, AND COGNITIVE FUNCTION 39JAGS JANUARY 2010–VOL. 58, NO. 1

Category Fluency (1,002) examined phonetic and semanticassociation fluency, respectively, and executive function.The Boston Naming Test (n 5 847) assessed confrontationnaming (word finding). The Mini-Mental State Examination(MMSE) (n 5 1,018) and the Blessed Information-Memory-Concentration (I-M-C) Test (n 5 1,810) are mental statustests.
NSAID and Aspirin Use
Use of NSAIDs and aspirin was self-reported as yes or noat each BLSAvisit and coded as a binary, fully time-dependentvariable. Quantity and frequency measures were notobtained.
Covariates
Age and education were assessed in years. A cardiovascularcomorbidity indicator variable (absent vs present) reflectedhistory of chronic cerebrovascular disease, coronary arterydisease, and peripheral arterial disease and was codedas a time-dependent binary variable. Diagnosed diabetesmellitus was coded as a time-dependent binary variable. Aninflammatory disease index included osteoarthritis, rheu-matoid arthritis, and rheumatismFconditions for whichregular NSAID use might be indicatedFcoded as a time-dependent binary variable. Hypertension was defined time-dependently as having systolic blood pressure (SBP) of 140mmHg or higher, diastolic blood pressure (DBP) of90mmHg or higher, or self-reported antihypertensive med-ication use. Resting brachial systolic SBP and DBP valueswere obtained three times bilaterally with participants inthe seated position after a 5-minute resting period. SBP andDBP were defined by Korotkoff phases I and V, respectively.
Data Analyses
Mixed-effects regression analyses were conducted to ex-amine longitudinal relations between NSAID and aspirinuse (included in the same models) and cognitive function.Mixed-effects models are the preferred method of analyzingdata with different numbers of repeated outcome measure-ments that are obtained at nonuniform intervals.21,22 Thesemodels examine the unique effects of individual predictorsadjusted for all other predictors in the model, include fixedand random effects, account for the correlation betweenrepeated measurements on the same participant, and areunaffected by randomly missing data. Because concurrentmeasures of NSAID and aspirin use and cognitive functionwere available at all visits, results of the present mixed-effects regression indicate age-related change in cognitiveperformance as a function of concurrently reported NSAIDor aspirin use (and all relevant covariates).
To maximize the unique information provided by eachneuropsychological test, separate regression models wereconstructed for each test as a dependent measure. Age andyears of education were treated as continuous covariates,and sex and all comorbidity indexes were treated as cate-gorical covariates. Other than sex, all covariates weretreated as time-varying. Age was modeled as a randomeffect to index time.21 All main effects and two-way inter-actions of NSAIDs or aspirin with age were entered intoeach model.
Statistical analyses were conducted using SAS version9.1 (SAS Institute, Inc., Cary, NC). Significant main effectsof NSAID or aspirin use indicate that the cognitive outcome(collapsed across all available testing sessions) is associatedwith overall differences in usage patterns regardless of lon-gitudinal change. The interaction term of NSAID (or aspi-rin) use and age indicates longitudinal change in cognitiveoutcome associated with NSAID or aspirin use. The latterreflects age-related differences in cognitive decline as afunction of prospectively assessed NSAID or aspirin use.Graphs were created to visualize the significant longitudinalrelations using the prototypical values of the predictors as afunction of age.21 Each graph depicts the predicted changesin the cognitive outcome over time using all of the infor-mation in the analyses regardless of the number of repeatedassessments. Because the primary focus was on age-relatedchange, each graph shows change in a cognitive test per-formance as a function of age.
RESULTS
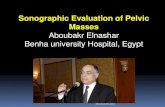
Significant main effects of NSAID and aspirin use and theirinteractions with age are depicted in Table 3. Significantinteraction between NSAID use and age (indicating changeover time) was found for the Blessed I-M-C Test and TrailMaking Part B such that NSAID use was associated withless decline in performance over time (Figure 1). Significantmain effects of NSAID use (that were not qualified by an ageinteraction) were noted for the Benton Visual RetentionTest, the Boston Naming Test, the CVLT’s learning slopeand short and long free recall, and Digits Backward. Withthe exception of the Boston Naming Test, NSAID use wasassociated with better test performance across all testingsessions.
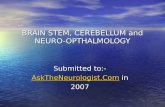
Significant interactions between aspirin use and agewere noted for the Blessed I-M-C Test and the Benton Vi-sual Retention Test (Figure 2), although aspirin was asso-ciated with a steeper gradient of cognitive decline on thesetests. Significant main effects of aspirin use (that were notqualified by an age interaction) were noted for the BentonVisual Retention Test, the CVLT’s learning slope and shortfree recall, and the MMSE and indicated better averagelevels of function for aspirin users.
DISCUSSION
Knowledge of longitudinal trajectories in cognitive perfor-mance associated with NSAID or aspirin use in personswithout dementia is minimal, and few studies have exam-ined cross-sectional and prospective relations. Further, mostprior studies used only mental status tests to index cognitivefunction. Accordingly, the present study examined cross-sectional and longitudinal relations between NSAID andaspirin use and performance on tests reflecting multipledomains of cognitive function in persons without dementia.Results indicated that, with increasing age, NSAID use wasassociated with less prospective decline on the BlessedI-M-C Test, a mental status test weighted for memory andconcentration, and Part B of the Trail Making Test, a test ofperceptuo-motor speed and mental flexibility (an executivefunction). In contrast, aspirin use was associated withgreater prospective decline on the Blessed I-M-C Test andthe Benton Visual Retention Test, a test of visual memory.
40 WALDSTEIN ET AL. JANUARY 2010–VOL. 58, NO. 1 JAGS

As illustrated in Figures 1 and 2, effect size magnitudes wereparticularly small for the longitudinal associations betweenNSAID and aspirin use and rate of change in cognitive per-formance over time. Clinical significance of these findingson an individual level is therefore questioned, althoughoverall public health significance may be meaningful.
Despite the paucity of longitudinal findings, there werea multitude of cross-sectional associations between NSAIDor aspirin use and cognitive performance. Specifically,NSAID use was related to better average levels of perfor-mance across all testing sessions on measures of verbal andvisual learning and memory, as well as concentration (orworking memory), yet diminished confrontation naming.Use of aspirin was also related to better average perfor-mance across testing sessions on measures of verbal andvisual learning and memory and global mental status. It isunclear whether this apparent benefit is attributable tomedication use per se or other characteristics of the indi-viduals who choose to take these medications over time.
Prior prospective investigations have been mixed withrespect to the positive, negative, or neutral relation betweenaspirin and cognitive function,6–11 and a greater incidenceof Alzheimer’s disease or vascular dementia was noted in
two studies.12,13 In that regard, it may be important to re-call that aspirin is frequently prescribed to people withexisting vascular disease. Thus, a decline in cognitive per-formance in aspirin users may be attributable, in part, to theneurobiological effects of cardiovascular disease or its riskfactors23 that may ultimately influence the development ofvascular dementia and Alzheimer’s disease.1 Despite thefact that hypertension and other cardiovascular disease di-agnoses were adjusted for in the present data analyses, re-sidual confounding is possible because of potentialdifferences in severity of extent of vascular disease betweenthose with and without aspirin use even in those with car-diovascular disease according to the indicator variable. Itwould also be important to conduct a standard assessmentof subclinical cardiovascular disease to more fully evaluatethis possibility. In addition, select individuals are ‘‘aspirinresistant’’ and thus may not benefit from its use with respectto clinical outcomes,24 with a concomitant lack of protec-tion against disease-related cognitive decline. That aspirinuse was related to greater decline on the Benton Visual Re-tention Test may be of interest because performance on thistest has been shown to predict Alzheimer’s disease up to 10years before its diagnosis in the BLSA.25,26
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Ble
ssed
Men
tal
Sta
tus
Err
ors
50 60 70 80 90Age
No NSAIDNSAID
No NSAIDNSAID
30
50
70
90
110
130
150
Trai
ls B
50 60 70 80 90Age
Figure 1. Longitudinal change in performance on the Blessed Information-Memory-Concentration Test and Part B of the TrailMaking Test as a function of nonsteroidal anti-inflammatory drug (NSAID) use. Because age was modeled as a random effect in thedata analyses, this figure displays change in cognitive performance over time (as individuals grew older during the course of the study)as a function of concurrently assessed NSAID use. Higher scores on each test indicate poorer performance.
Table 3. Mixed-Effects Regression Models Predicting Neuropsychological Test Performance from NonsteroidalAnti-Inflammatory Drug (NSAID) Use, Aspirin Use, and Covariates: Significant Main and Interactive Effects of NSAIDor Aspirin Use
Neuropsychological Test
B (Standard Error)
NSAID Use Aspirin Use NSAID Use � Age Aspirin Use � Age
Blessed Information-Memory-Concentration Test (n 5 1,810) 0.611� (0.163) � 0.422� (0.175) � 0.011� (0.003) 0.006� (0.003)
Benton Visual Retention Test (n 5 2,300) � 0.150� (0.069) � 2.02� (0.315) F 0.030� (0.005)
Boston Naming Test (n 5 847) � 0.290� (0.144) 0.017 (0.131) F F
California Verbal Learning Text
Learning Slope (n 5 1,313) 0.090� (0.020) 0.071� (0.019) F F
Free Recall Short Delay (n 5 1,313) 0.242� (0.093) 0.199� (0.090) F F
Free Recall Long Delay (n 5 1,313) 0.259� (0.094) 0.154 (0.091) F F
Digits Backward (n 5 1,397) 0.255� (0.073) 0.003 (0.070) F F
Mini-Mental State Examination (n 5 1,018) � 0.011 (0.053) 0.096� (0.049) F F
Trail Making Test Part B (n 5 987) 22.2 (11.8) � 1.33 (1.22) � 0.319� (0.163) F
Note: Coefficients associated with main effects of NSAID or aspirin use indicate the magnitude and direction of the relationship between the variables;
coefficients associated with the interaction terms are not directly interpretable and are clarified in Figures 1 and 2.�Po.05.
NSAIDS, ASPIRIN, AND COGNITIVE FUNCTION 41JAGS JANUARY 2010–VOL. 58, NO. 1

Other prior studies of NSAID and aspirin use haveemployed a variety of mental status tests that screen fordementia. The findings of the current study are partiallyconsistent with those noted in prior epidemiological inves-tigations in which lesser decline on the SPMSQ or 3MS wasfound in NSAID users.14,16 In the present investigation,NSAID use was associated with less decline on the BlessedI-M-C Test, a screening measure that is more heavilyweighted toward assessment of memory and concentrationthan the SPMSQ (or 3MS) and that may be a more sensitivescreening measure for cognitive difficulties. Performance onPart B of the Trail Making Test, a measure that requiresperceptuo-motor speed and mental flexibility (or set shift-ing), a component of executive functioning, also benefited.Thus, future longitudinal work might include a broaderassessment of executive functions that are weakly (or not)represented on most cognitive screening measures.
These findings may, in part, reflect that the BlessedI-M-C Test and Benton Visual Retention Test were the twomeasures available for the greatest number of BLSA par-ticipants, although this concern does not relate to the TrailMaking Test. Nevertheless, it is striking that neither NSAIDnor aspirin use conferred protection against prospectivedecline on any other clinical neuropsychological or mentalstatus measure. The preponderance of the findings suggestthat NSAID and aspirin use are associated with greater av-erage levels of performance on multiple measures of learn-ing, memory, and verbal fluency across all testing sessions.Prior cross-sectional findings have revealed weak relationsbetween aspirin use and better word recall and word flu-ency17 and relations between NSAID use and better con-centration,27 although fewer tests of cognitive functionwere employed in these investigations. The cross-sectionalfindings here and elsewhere raise the question of whetherNSAID or aspirin use confers habitual neuroprotection orwhether persons taking these medications differ from thosewho do not on other dimensions that may protect the brainand cognitive function. Discussed extensively elsewhere,there are several plausible biological mechanisms wherebyNSAID and aspirin use may preserve cognitive func-tion,28,29 including lower production of cytokines, lessplatelet aggregation (and therefore less beta-amyloid), thescavenging of free radicals, less endothelial damage, andvasodilatation.
Strengths of this investigation include the greatestnumber of repeated, concurrent assessments of NSAID or
aspirin use and cognitive function available to date. Use ofan extensive neuropsychological test battery is also an ad-vantage. Limitations to this investigation include the use ofa highly educated and predominantly white conveniencesample that limits the study’s generalizability. Another lim-itation is the binary assessment of NSAID and aspirin userather than measurement of quantity and frequency or useof pharmacy records, although prior work has suggested noincremental benefit of larger dosage.5,27 Thus, even habit-ual, low-level use may confer benefit.
In sum, NSAID users displayed less prospective declineon a mental status measure weighted for memory and con-centration and a test of perceptuo-motor speed and mentalflexibility. Thus, only select protection against cognitivedecline was apparent in the present sample without demen-tiaFan understudied group in the literature. In contrast,aspirin use was associated with greater prospective cogni-tive decline on the mental status measure described aboveand a visual memory test, potentially reflecting its commonuse for vascular disease prophylaxis. It is therefore possiblethat inception of aspirin use must precede even subclinicalvascular disease to confer the greatest benefit. Further un-derstanding of the longitudinal trajectories of cognitivefunction associated with NSAID and aspirin use may pro-vide optimal information regarding potential maintenanceof cognitive function, or attenuation of decline, with aging.
ACKNOWLEDGMENTS
Conflict of Interest: The editor in chief has reviewed theconflict of interest checklist provided by the authors and hasdetermined that the authors have no financial or any otherkind of personal conflicts with this paper.
This research was supported in part by the IntramuralResearch Program of the National Institutes of Health,National Institute on Aging.
Author’s Contributions: The authors of this manuscriptcontributed in the following ways that meet authorshipcriteria. Dr. Waldstein was responsible for conceptualiza-tion of the research question, analysis and interpretationof the data, drafting the article, and revising it withcoauthor input. Ms. Wendell conducted the data analysesand was involved in conceptualization of the research ques-tion, data interpretation, drafting a portion of the article,and making critical revision of the manuscript. Dr. Seligerwas involved in data analysis and interpretation and critical
23456789
10
BV
RT
Err
ors
50 60 70 80 90Age
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Ble
ssed
Men
tal
Sta
tus
Err
ors
50 60 70 80 90Age
No aspirinAspirin
No aspirinAspirin
Figure 2. Longitudinal change in performance on the Blessed Information-Memory-Concentration Test and the Benton Visual Re-tention Test (BVRT) as a function of aspirin use. Because age was modeled as a random effect in the data analyses, this figure displayschange in cognitive performance over time (as individuals grow older during the course of the study) as a function of concurrentlyassessed aspirin use. Higher scores on each test indicate poorer performance.
42 WALDSTEIN ET AL. JANUARY 2010–VOL. 58, NO. 1 JAGS

revision of the manuscript. Drs. Ferrucci and Metter wereinvolved in data interpretation and critical revision of themanuscript. Dr. Zonderman was involved in conceptual-ization of the research question, analysis and interpretationof the data, and critical revision of the manuscript.
Sponsor’s Role: None.
REFERENCES
1. Langa KM, Foster NL, Larson EB. Mixed dementia: Emerging concepts and
therapeutic implications. JAMA 2004;292:2901–2908.
2. Peila R, Launer LJ. Inflammation and dementia: Epidemiologic evidence. Acta
Neurol Scand 2006;114:102–106.
3. Szekely CA, Thorne JE, Zandi PP et al. Nonsteroidal anti-inflammatory drugs
for the prevention of Alzheimer’s disease: A systematic review. Neuroepide-
miology 2004;23:159–169.
4. Szekely CA, Green RC, Breitner JCS et al. No advantage of AB42-lowering
NSAIDs for prevention of Alzheimer dementia in six pooled cohort studies.
Neurology 2008;70:2291–2298.
5. In’T Veld BA, Ruitenberg A, Hofman A et al. Nonsteroidal anti-inflammatory
drugs and the risk of Alzheimer’s disease. NEJM 2001;345:1515–1521.
6. Anthony JC, Breitner JCS, Zandi PP et al. Reduced prevalence of AD in users of
NSAIDs and H2 receptor antagonists. The Cache County Study. Neurology
2000;54:2066–2071.
7. Zandi PP, Anthony JC, Hayden KM et al. Reduced incidence of AD with
NSAID but not H2 receptor antagonists. Neurology 2002;59:880–886.
8. Nilsson SE, Johansson B, Takkinen S et al. Does aspirin protect against
Alzheimer’s dementia? A study in a Swedish population-based sample aged
�80 years. Eur J Clin Pharmacol 2003;59:313–319.
9. Henderson AS, Jorm AF, Christensen H et al. Aspirin, anti-inflammatory drugs
and risk of dementia. Int J Geriatr Psychiatry 1997;12:926–930.
10. Kang JH, Cook N, Manson J et al. Low does aspirin and cognitive function in
the women’s health study cognitive cohort. BMJ 2007;334:987.
11. Stewart WF, Kawas C, Corrada M et al. Risk of Alzheimer’s disease and du-
ration of NSAID use. Neurology 1997;48:626–632.
12. Cornelius C, Fastbom J, Winblad B et al. Aspirin, NSAIDs, risk of dementia,
and influence of the apolipoprotein E epsilon 4 allele in an elderly population.
Neuroepidemiology 2004;23:135–143.
13. Hebert R, Lindsay J, Verreault R et al. Vascular dementia: Incidence and
risk factors in the Canadian Study of Health and Aging. Stroke 2000;31:
1487–1493.
14. Rozzini R, Ferrucci L, Losonczy K et al. Protective effect of chronic NSAID use
on cognitive decline in older persons. J Am Geriatr Soc 1996; 44:1025–1029.
15. Sturmer T, Glynn RJ, Field TS et al. Aspirin use and cognitive function in the
elderly. Am J Epidemiol 1996;143:683–691.
16. Hayden KM, Zandi PP, Khachaturian AS et al. Does NSAID use modify cog-
nitive trajectories in the elderly? The Cache County Study. Neurology
2007;69:275–282.
17. Peacock JM, Folsom AR, Knopman DS et al. Association of nonsteroidal anti-
inflammatory drugs and aspirin with cognitive performance in middle-aged
adults. Neuroepidemiology 1999;18:134–143.
18. Shock N, Greulich RC, Andres R et al. Normal Human Aging: The Baltimore
Longitudinal Study of Aging. Washington, DC: U.S. Government Printing
Office, 1984.
19. Kawas C, Gray S, Brookmeyer R et al. Age-specific incidence rates of Alzhei-
mer’s disease: The Baltimore Longitudinal Study of Aging. Neurology
2000;54:
2072–2077.
20. Lezak MD, Howieson DB, Loring DW. Neuropsychological Assessment, 4th
Ed. New York: Oxford University Press, 2004.
21. Singer JD, Willett JB. Applied Longitudinal Data Analysis: Modeling Change
and Event Occurrence. New York: Oxford University Press, 2003.
22. Gueorguieva R, Krystal JH. Move over ANOVA. Progress in analyzing re-
peated-measure data and its reflection in papers published in the Archives of
General Psychiatry. Arch Gen Psychiatry 2004;61:310–317.
23. Waldstein SR, Elias MF, (eds). Neuropsychology of Cardiovascular Disease.
Mahwah, NJ: Lawrence Erlbaum Associates, 2001.
24. Krasopoulus G, Brister SJ, Beattie WS et al. Aspirin ‘‘resistance’’ and risk of
cardiovascular morbidity: Systematic review and meta-analysis. BMJ
2008;336:195–198.
25. Zonderman AB, Giambra LM, Arenberg D et al. Changes in immediate
visual memory predict cognitive impairment. Arch Clin Neuropsychol 1995;
10:111–123.
26. Kawas CH, Corrada MM, Brookmeyer R et al. Visual memory predicts Alz-
heimer’s disease more than a decade before diagnosis. Neurology 2003;60:
1089–1093.
27. Hanlon JT, Schmader KE, Landerman LR et al. Relation of prescription non-
steroidal anti-inflammatory drug use to cognitive function among community-
dwelling elderly. Ann Epidemiol 1997;7:87–94.
28. Launer LJ. Nonsteroidal anti-inflammatory drug use and the risk for Alzhei-
mer’s disease. Drugs 2003;63:731–739.
29. Broe GA, Grayson DA, Creasey HM et al. Anti-inflammatory drugs protect
against Alzheimer’s disease at low doses. Arch Neurol 2000;57:1586–1591.
SUPPORTING INFORMATION
Additional Supporting Information may be found in theonline version of this article:
Table S1. Coefficients and Standard Errors fromMixed-effects Regression Models Predicting Neuropsycho-logical Test Performance from NSAIDS Use, Aspirin Use,and Covariates.
Please note: Wiley-Blackwell is not responsible for thecontent or functionality of any supporting materials sup-plied by the authors. Any queries (other than missing ma-terial) should be directed to the corresponding author forthe article.
NSAIDS, ASPIRIN, AND COGNITIVE FUNCTION 43JAGS JANUARY 2010–VOL. 58, NO. 1

Copyright of Journal of the American Geriatrics Society is the property of Blackwell Publishing Limited and its
content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.