Insomnia Café Owned and Operated by: Kelsey Eklund, Spencer Henshaw & Alison Wigglesworth.
Upload
roxana-badicioiuCategory
view
8download
0description

Time Use and Occupational PerformanceAmong Persons with Schizophrenia
Ulrika Bejerholm, Reg. OT, BScMona Eklund, PhD, Reg. OT
ABSTRACT. Schizophrenia is a complex disorder with a heavy impacton daily life. Since the human occupational pattern is a product of per-son-occupation-environment interaction, it is of importance to exploreall these factors to understand the daily occupational pattern among per-sons with schizophrenia. This study aimed to describe the time use of 10persons with schizophrenia, reflecting the participants’ daily occupa-tions, social and geographical environments, and emotional reaction andreflection on their occupational performance. The results showed stag-nation in the participants’ occupational pattern and time use. Most activi-ties were not triggered by a facilitating environment but from within theperson by basic, immediate life needs, or wanting to escape reality. Oc-cupational therapists could assist this group in reshaping the environ-ment and regaining roles that involve interacting with the outside world.[Article copies available for a fee from The Haworth Document Delivery Ser-vice: 1-800-HAWORTH. E-mail address: <[email protected]>Website: <http://www.HaworthPress.com> © 2004 by The Haworth Press, Inc.All rights reserved.]
Ulrika Bejerholm is a doctoral student and Lecturer, and Mona Eklund is AssociateProfessor, Lund University, Department of Clinical Neuroscience, Division of Occu-pational Therapy.
Address correspondence to: Ulrika Bejerholm, Lund University, Department ofClinical Neuroscience, Division of Occupational Therapy, P.O. Box 157, SE-221 00Lund, Sweden (E-mail: [email protected]).
The authors would like to thank the participants and staff of Rundelen, Malmö Psy-chiatry, for their collaboration and hospitality.
Occupational Therapy in Mental Health, Vol. 20(1) 2004http://www.haworthpress.com/web/OTMH
2004 by The Haworth Press, Inc. All rights reserved.Digital Object Identifier: 10.1300/J004v20n01_02 27

KEYWORDS. Time use, occupational performance, occupational pat-tern, schizophrenia, psychiatry
INTRODUCTION
The balance between the different types of occupations that composepeople’s daily lives–in terms of, e.g., work, self-maintenance, and play–has been regarded as vital for adaptation ever since occupational ther-apy was founded (Meyer, 1922/1977). During the past few years thebalance between different types of occupations has gained renewed andincreasing interest, and it has been hypothesized that a balanced patternof occupations may lead to better well-being (Erlandsson & Eklund,2001; Persson, Erlandsson, Eklund, & Iwarsson, 2001). Furthermore,within occupational therapy it has been emphasized that participation inmeaningful occupations stimulates health and well-being (Law et al.,1997; McLaughlin Gray, Kennedy, & Zemke, 1996; McLaughlin Gray,2001; Wilcock, 1995; Wilcock et al., 1998; WHO, 2001). Presumably,if active involvement in occupations has been shown to positively affecthealth and well-being, an imbalance of activities and roles may causeproblems with health and quality of life (Pentland, Harvey, & Walker,1998).
People who develop schizophrenia often fail to accomplish age-re-lated developmental occupations in work, self-maintenance, and play(American Psychiatric Association, 1994). In general, there has beenlimited research into the patterns of occupational performance amongpersons with disabilities (Pentland et al., 1998). Besides, even though itis known that there is a relationship between mental illness and howtime is experienced, there is no specific description of how the mentallyill spend their time (Suto & Frank, 1994; Emerson, Cook, Polatajko, &Segal, 1998), especially not among people with psychotic disorders(Rosenthal & Howe, 1984). Persons with schizophrenia often haveproblems with organising the daily occupations, which results in a cha-otic way of dealing with time (Melges, 1982; Neville, 1980; Neville,Kreisberg & Kielhofner, 1985), and a disharmony between the futureimages, plans of action, and emotions (Melges, 1982). Time appears tostand still, often because of a decreased ability to integrate perceptualinformation (Creek, 1997; Hartocollis, 1975). A volitional problem iscommon in persons with schizophrenia, and a social regression occurswith few roles to fulfil (Creek, 1997), which in turn further decreasesthe possibility of organizing the occupational performance (Neville et
28 OCCUPATIONAL THERAPY IN MENTAL HEALTH

al., 1985). Weeder (1986) showed that compared to a normal popula-tion, participants with schizophrenia spent more time in passive occu-pations, and their social activities were mostly planned and initiatedexternally.
Schizophrenia is a complex disorder where health cannot be under-stood in relation to biological aspects only (Tsang & Pearson, 2000).Since the human occupational pattern is a product of the person-envi-ronment interaction (Dunn, Brown, & McGuigan, 1994; Kielhofner,1995, 1997; McLaughlin Gray, 2001; WHO, 2000; von Bertalanffy,1968; Zemke & Clarke, 1996) it is of importance to explore the contex-tual factors involved in order to understand the complexity of occupa-tion for persons with schizophrenia. This implies a dynamic perspectiveon occupation, and according to Law et al. (1996) occupational perfor-mance is shaped by the occupational, the environmental, and the per-sonal domain. Few studies, however, consider contextual factors fromall domains (Crist, Davis, & Coffin, 2000; Robinson, 1997). For exam-ple, Weeder (1986) did not focus on the environmental domain. Simi-larly, few studies have looked into who mentally ill people typicallyspend their time with. Furthermore, to fully understand the occupa-tional pattern, it is essential to have a time-use perspective when study-ing occupational performance (Creek, 1997; Meyer, 1922/1977). Atime-use perspective deepens the understanding of how persons withschizophrenia go about their daily lives (Suto & Frank, 1994). To have atime-use perspective means reflecting as realistic a picture as possibleof daily occupations (Robinson, 1977; Rosenthal & Howe, 1984; Slagle,1922; Suto & Frank, 1994).
Occupational factors, such as satisfaction with daily occupations in abroad sense, have been shown to be strongly related to quality of lifeand other aspects of well-being among people with schizophrenia(Eklund, Hansson, & Bejerholm, 2001). No empirical studies, however,seem to have addressed what people with severe mental illness reallyspontaneously do in their everyday lives, what occupies their time, whatactivities they experience as satisfying and anxiety-provoking, and inwhat social and geographical environments they perform their daily oc-cupations. Knowing more about their spontaneous patterns of daily occu-pations, and how these occupations are experienced, would be importantknowledge for the planning of care for the severely mentally ill and forassisting them in setting adequate life goals, congruent with their abili-ties, interests, and their environmental context. This was the impetus forthis study, which aims to investigate in depth the occupational perfor-mance in a group of persons with schizophrenia in a time-use perspective.
Ulrika Bejerholm and Mona Eklund 29

METHODS
Selection Procedure
A consecutive sampling method was used in this study. The first 10participants who entered a larger study (Eklund et al., 2001), of whichthe present study is a part, were chosen. The selection criteria for thelarger study, as well as for the present part, were between 20-55 years ofage, and had a diagnosis of schizophrenia based on DSM-IV (AmericanPsychiatric Association, 1994). The participants were registered pa-tients at an outpatient unit in a geographically defined catchment area ina Swedish town and had visited the unit within the past 12 months. Theinitial contact with the participant was taken by the patient’s primarycontact person who asked for his or her consent. The subsequent contactwas maintained by the interviewer, the first author of this study, andtime for an appointment was set. This study was based on informed con-sent, and the project was approved by the Research Ethics Committee,Faculty of Medicine at Lund University.
Participants
Out of the ten participants that were included in this study, eight weremen and two were women. Their age ranged from 20 to 55 years. Fiveparticipants were diagnosed with paranoid schizophrenia. Other sub-groups of schizophrenia represented among the patients were the disor-ganized type, the catatonic type, and schizoaffective disorder. Three ofthe participants had a relationship with a person of the opposite sex, butonly one of them lived with that person. Nine participants lived alone intheir own flats. Three of them had satellite accommodation, whichmeant living near a group home and having the opportunity to contactthe staff there. All participants took medication for their mental disor-ders and none of them worked or had any children.
Instrument and Interview
There is agreement among scientists that a time-use diary is the most ad-equate and valid instrument when collecting reliable data about people’stime use and occupational performance (Creek, 1997; Cynkin & Robinson,1990; Ellegård & Nordell, 1997; Juster & Stafford, 1991; Karlsson,Söderback, Synnerholm, Ekholm, & Bergroth, 1996; Kielhofner, 1995;Robinson, 1997). The instrument in this study was a 24-hour diary.
30 OCCUPATIONAL THERAPY IN MENTAL HEALTH

Twenty-four hours is an appropriate time limit and the 24-hour diaryhas good validity when it is used on a group belonging to the same pop-ulation (Szalai, 1972). The instrument used in this study is based on atime-use diary developed for a study run by Statistics Sweden, investi-gating time use and living conditions among men and women in Swe-den (Statistiska centralbyrån, 1992). The instructions were somewhatmodified because of anticipated difficulties regarding the participants’ability to comprehend complicated information. The participants wereasked to provide a description of their actual time use in the past 24hours. The appointments for the recording of the time-use diary were seton a weekday, except Mondays, implying that all reports concerned in-formation about time use during weekdays. The time-use diary was ad-ministered as a self-report questionnaire. The sheets were divided intofour columns, each with rows representing one-hour intervals. Eachcolumn had a question on top, the first asking what the participant per-formed, the second about geographic environment, the third about so-cial environment, and finally personal comments or reflections aboutthe performance. The time-use diary was completed with a supplemen-tary interview, which was recorded in writing. The interview emanatedfrom the 24-hour diary and served as a complement. It helped the partic-ipant recall what she or he did, for how long, and so on. This served toincreased the validity (Robinson, 1997), since different types of datasources minimize distortion from a single data source or from a biasedresearcher (Knafl & Breitmeyer, 1989; Krefting, 1991). The data col-lection took place at the outpatient clinic, which was familiar to the par-ticipants, and took about 45 minutes.
Data Analysis
To categorize the reported material, a content analysis was used.Content analysis is an unobtrusive method and the observer has no ef-fect upon the material collected (Fox, 1992; Sommer & Sommer, 1991).First, the information from the time-use diary and the supplementary in-terview were integrated and viewed as a single set of information. Dur-ing the course of the content analysis a structure of domains, factors,and categories emerged, related to occupational performance. Theywere, in part, hierarchic, as presented in Table 1.
The domains were derived from theory (Law et al., 1996) and corre-sponded closely to the factors, which were represented by the four col-umns of the 24-hour time-use diary. The only divergence was that thepersonal comments and reflections, which formed one column in the di-
Ulrika Bejerholm and Mona Eklund 31
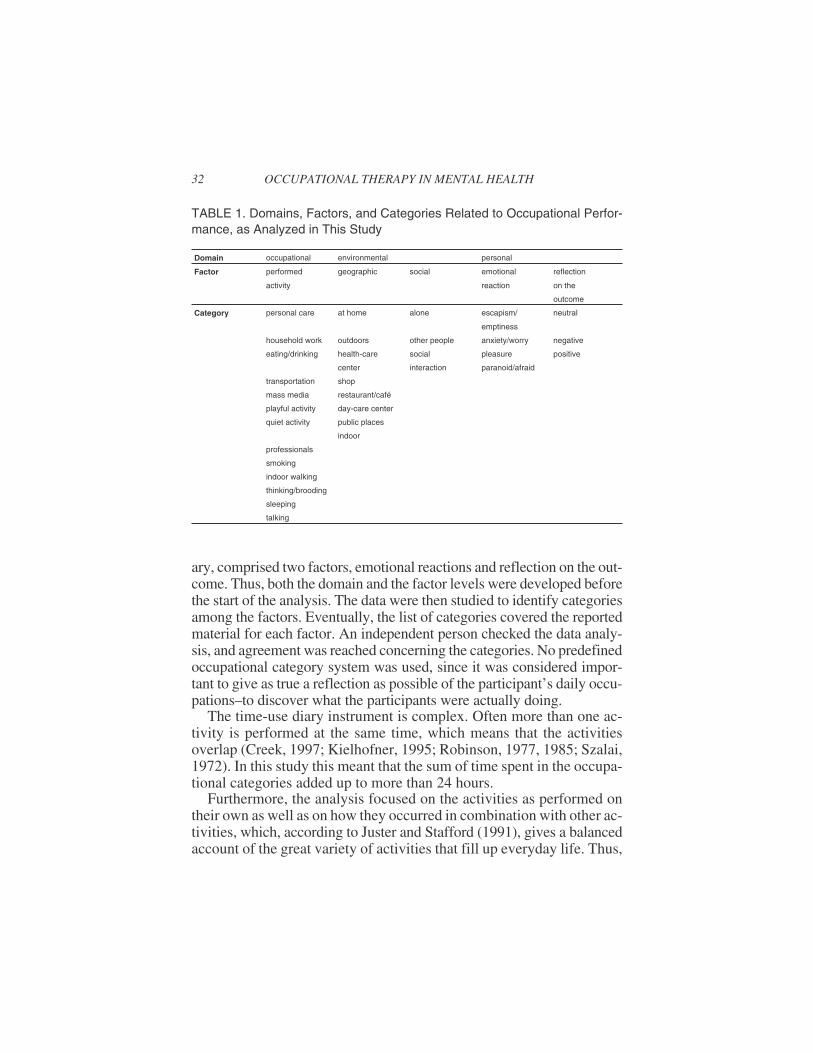
ary, comprised two factors, emotional reactions and reflection on the out-come. Thus, both the domain and the factor levels were developed beforethe start of the analysis. The data were then studied to identify categoriesamong the factors. Eventually, the list of categories covered the reportedmaterial for each factor. An independent person checked the data analy-sis, and agreement was reached concerning the categories. No predefinedoccupational category system was used, since it was considered impor-tant to give as true a reflection as possible of the participant’s daily occu-pations–to discover what the participants were actually doing.
The time-use diary instrument is complex. Often more than one ac-tivity is performed at the same time, which means that the activitiesoverlap (Creek, 1997; Kielhofner, 1995; Robinson, 1977, 1985; Szalai,1972). In this study this meant that the sum of time spent in the occupa-tional categories added up to more than 24 hours.
Furthermore, the analysis focused on the activities as performed ontheir own as well as on how they occurred in combination with other ac-tivities, which, according to Juster and Stafford (1991), gives a balancedaccount of the great variety of activities that fill up everyday life. Thus,
32 OCCUPATIONAL THERAPY IN MENTAL HEALTH
TABLE 1. Domains, Factors, and Categories Related to Occupational Perfor-mance, as Analyzed in This Study
Domain occupational environmental personal
Factor performed geographic social emotional reflection
activity reaction on the
outcome
Category personal care at home alone escapism/ neutral
emptiness
household work outdoors other people anxiety/worry negative
eating/drinking health-care social pleasure positive
center interaction paranoid/afraid
transportation shop
mass media restaurant/café
playful activity day-care center
quiet activity public places
indoor
professionals
smoking
indoor walking
thinking/brooding
sleeping
talking

the time spent in every separate performed activity was analyzed. Simi-larly, in an initial phase of analysis, the occupational performance fac-tors were analyzed separately. In this initial phase, the social andgeographic environment, the emotional response and reflection on theoutcome, were analyzed according to reported time spent within thesefactors. The time use was summed up in minutes and rounded into hourswith one decimal.
The activities, however, were frequently performed simultaneously.Therefore, the analysis also focused on how an activity was combinedwith other activities, and no judgement was made about whether any ofthem was more important than the others. In this second step it was dis-cerned to what extent the activity was performed as a single activity orin combinations.
A third step of the analysis also included the environment in whichthe activity was performed and the personal reflections it gave rise to,giving a multifaceted picture of the actual performance. In this study,such a combination, based either on activity categories only or on acombination of categories from two or more factors, was called a mod-ule. The frequency with which the modules appeared was recorded.
RESULTS
The Occupational Domain: Performed Activities
Table 2 shows the distribution of the different activities for each re-spondent. Among all performed activities sleeping was the category onwhich the participants spent most time. The least time was spent on see-ing a professional from the health care. Everyone spent time on consum-ing mass media, eating and drinking, performing quiet activities, andpersonal care, but to varying extents. With respect to consuming massmedia, five participants alternated between watching television, listeningto the radio, and reading the newspaper. Four participants watched televi-sion only, and one participant only listened to the radio. Having coffeewas the main activity for three of the participants with respect to eatingand drinking. For every participant, more than 1.2 hours was spent in aquiet activity, which means sitting or lying, looking at other people or ob-jects. One participant spent 9.4 hours in this type of activity. Personalcare mostly meant getting dressed or undressed and going to the toilet.
Personal care and household work were activities that were per-formed only for short periods of time. For example, seven out of ten par-
Ulrika Bejerholm and Mona Eklund 33

ticipants reported that they bought microwave dinners and fast food,instead of performing household work themselves. Eight participantssmoked cigarettes for 2.7-13.2 hours. Two participants did not leavetheir homes during the investigated 24 hours. As to transportation, theparticipants mostly walked.
Five participants spent more than 2 hours walking around indoors,and also thinking and brooding was an ingredient in the daily life of fiveparticipants. Playful activities engaged seven participants. Musical in-struments were played by three of them and the other participants didvarious things such as writing philosophical notes, browsing in or read-ing books, and painting in an occupational therapy session. Talkingwith other people was an activity that occurred among seven partici-pants. Most of them small-talked with staff or visitors at day-care cen-ters. Two participants reported having a whole conversation, and inthese cases the interlocutors were employees at a day-care center.
34 OCCUPATIONAL THERAPY IN MENTAL HEALTH
TABLE 2. Each Participant’s Time Spent on Different Activities (24 hr.)
Occupational Domain
Factor
Performed Activity
Participants
Category 1 2 3 4 5 6 7 8 9 10 mdn
sleeping 10 4.8 10.5 8 11 6 7.8 14 9 6.8 8.5
smoking 3.8 7.3 - 5.9 2.7 13.2 - 4.2 6 8.2 5
mass media 2 6.8 2.5 6.4 0.9 3 9.8 1 6.7 7.8 4.7
quiet activity 1.9 1.8 2.2 3.9 5.2 9.4 1.2 5.8 3.5 1.7 2.8
eating/drinking 3 7.7 1.8 4.2 2.3 4.8 1.6 2.8 1 1.6 2.6
talking 5 3.5 2.8 4.7 5.6 - - 1 - 4 3.2
transportation 1.4 1.2 2.2 0.8 1.7 3.2 - 0.8 - 1.8 1.3
indoor walking - 2.8 - 3 - 2 8.2 - 4 - 1
personal care 0.5 1 0.9 1.7 0.2 0.5 1.8 1 2.2 1.8 1
playful activity 0.8 1 2 - 0.9 1.8 6.7 0.2 - - 0.8
household work 0.2 0.2 2.2 0.2 0.2 0.2 2.7 - 1.8 2 0.2
thinking/brooding - - 0.2 3 - 1.8 9.3 - 9 - 0.1
professionals 1.8 1.9 1.2 2.3 - - - - - - 0
Note. Figures in bold show the most common activity for each participant.The figures denote amount of time spent on activities, given that two or more activities can be performed simultaneously.

Times spent in single and combined activities are shown in Table 3.For example, the categories, personal care, household work, transporta-tion, seeing a professional, and sleeping were activities mostly performedas separate, single activities. Walking indoors and thinking/broodingwere always combined with other categories and eating/drinking, massmedia, playful activities, quiet activities, smoking, and talking weremostly performed in combinations.
To further assess how the performed activities were typically com-bined, the most frequent modules for the whole group were discerned(Table 4). Quiet activity together with smoking was the most commonmodule; it was included in the 49 most frequently occurring modules. In14 instances this module was combined with mass media and in 13cases with eating/drinking.
The Environmental Domain: Geographic and Social Environment
Table 5 shows that, as regards the geographic environment, all par-ticipants spent most of their time in their home environment, from 15 upto 24 hours. Eight participants went outdoors, mostly around the neigh-borhood, going to small shops to buy cigarettes and snacks.
Ulrika Bejerholm and Mona Eklund 35
TABLE 3. Time Spent in Combined and Single Activities, as a Sum for theWhole Group, N = 10 (24 hr.)
Category Single activity Combined activity
personal care 10.6 1
household work 5.7 4
eating/drinking 4 26.8
transportation 1.2 0.1
mass media 8.8 38.1
playful activity 2.4 11
quiet activity 9.1 27.6
professionals 3.9 3.3
smoking 1.8 49.6
indoor walking 19.9
thinking/brooding 23.4
sleeping 87.8
talking 6 17.8
Note. Figures in bold indicate the most frequent mode (single or combined activity).
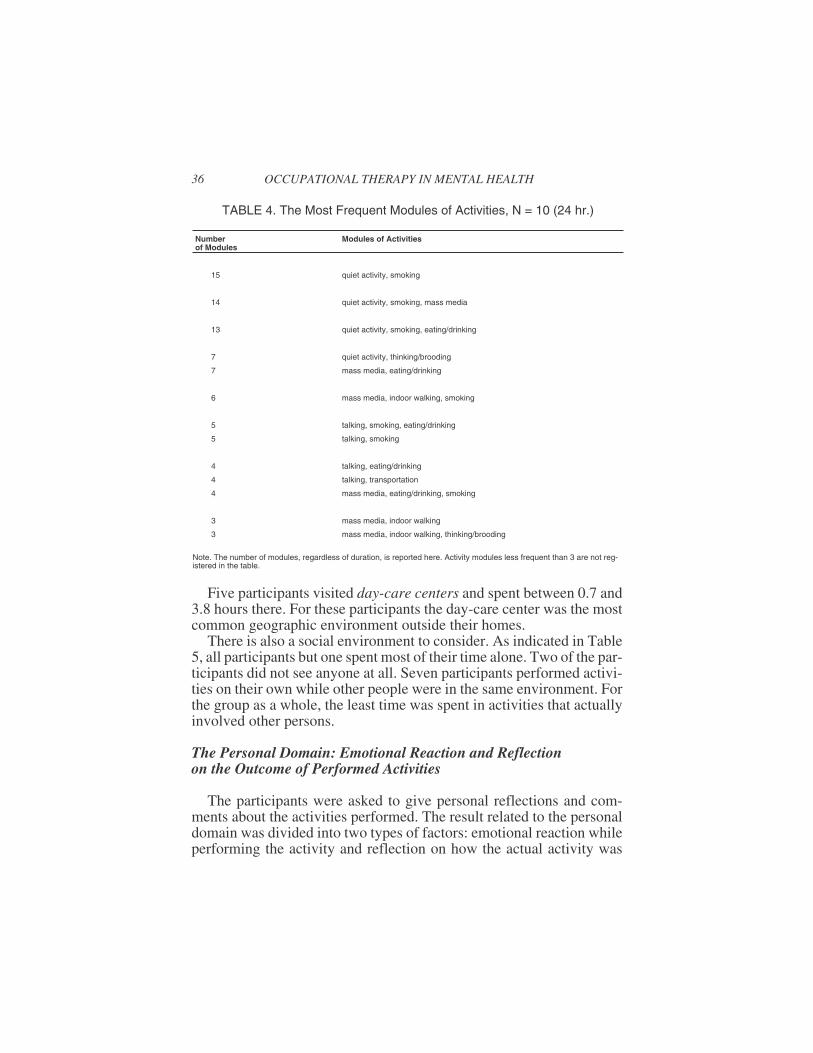
Five participants visited day-care centers and spent between 0.7 and3.8 hours there. For these participants the day-care center was the mostcommon geographic environment outside their homes.
There is also a social environment to consider. As indicated in Table5, all participants but one spent most of their time alone. Two of the par-ticipants did not see anyone at all. Seven participants performed activi-ties on their own while other people were in the same environment. Forthe group as a whole, the least time was spent in activities that actuallyinvolved other persons.
The Personal Domain: Emotional Reaction and Reflectionon the Outcome of Performed Activities
The participants were asked to give personal reflections and com-ments about the activities performed. The result related to the personaldomain was divided into two types of factors: emotional reaction whileperforming the activity and reflection on how the actual activity was
36 OCCUPATIONAL THERAPY IN MENTAL HEALTH
TABLE 4. The Most Frequent Modules of Activities, N = 10 (24 hr.)
Numberof Modules
Modules of Activities
15 quiet activity, smoking
14 quiet activity, smoking, mass media
13 quiet activity, smoking, eating/drinking
7 quiet activity, thinking/brooding
7 mass media, eating/drinking
6 mass media, indoor walking, smoking
5 talking, smoking, eating/drinking
5 talking, smoking
4 talking, eating/drinking
4 talking, transportation
4 mass media, eating/drinking, smoking
3 mass media, indoor walking
3 mass media, indoor walking, thinking/brooding
Note. The number of modules, regardless of duration, is reported here. Activity modules less frequent than 3 are not reg-istered in the table.

performed, the outcome (Table 6). The feeling of escapism and empti-ness, expressed as “I escape from reality” or “I feel empty,” was anemotional reaction that nine of the participants experienced. Five out ofthese participants reported that this was the most common emotional re-action, and one participant spent as much as 17.6 hours feeling empty,wanting to escape the situation (Table 6). The second most commoncategory for the group as a whole was anxiety and worry. Statementslike “I get restless and worried” and “I feel anxious” were common amongeight participants. Seven participants experienced pleasure, expressedin statements like “at ease,” “excited,” “feeling pleasure,” and for twoof them this state of mind was the most common emotion. Five partici-pants reported paranoiac reactions and being afraid. Usual commentswere “afraid that people are talking about me,” “watching me though Iwas alone” and “I was scared.”
Ulrika Bejerholm and Mona Eklund 37
TABLE 5. Time Use in Relation to Factors in the Environmental Domain, N = 10(24 hr.)
Environmentaldomain
Range (h) Mdn(h)
Factor
Geographic
environment
Category
at home 15-24 19.2
outdoors 0-3.1 1.7
day-care center 0-3.8 0.4
health-care center 0-1.5 0
shop 0-1 0.2
restaurant/café 0-1 0
public places indoors 0-0.5 0
Factor
Social
environment
Category
alone 9.5-24 17.4
other people* 0-11.3 3.2
others involved** 0-8.1 2.8
*Other people in the environment while performing the activity**Others involved in the actual performance

A neutral statement, like “it was okay,” “a habit,” “as usual,” abouthow the activity was performed was the most common reflection on theoutcome among every participant but one. Eight participants reportednegative reflections regarding the outcomes on at least one performedactivity. “I couldn’t concentrate,” “it had no meaning” and “it was toodifficult” were comments that occurred. Five participants were positiveabout how they performed their activities some time during the day.Comments like “it was meaningful,” “I was confident,” and “I could con-centrate” were reported. The amount of time the participants reportedspending on activities that resulted in each type of reflection on the out-come is shown in Table 6.
Occupational Performance as Indicated by Different Modulesof Occupational Performance Factors
Table 7 shows occupational performance modules, as composed bythe performance factors in this study: performed activities, the geo-graphic and social environment, emotional reaction, and reflections onthe outcome. Out of a total of 50 occupational performance modules,
38 OCCUPATIONAL THERAPY IN MENTAL HEALTH
TABLE 6. Time Use in Relation to Factors in the Personal Domain, N = 10 (24 hr.)
Personaldomain
Range(h) Mdn(h)
Factor
Emotional
reaction
Category
escapism/emptiness 0-17.6 4.5
anxiety/worry 0-10.8 1.5
pleasure 0-7.7 1.2
paranoid/afraid 0-1 0.2
Factor
Reflection on
the outcome
Category
neutral 1.1-13.8 5
negative 0-4.8 1.4
positive 0-4 0

Table 7 shows the 14 most common modules, performed by four ormore participants.
All participants but one reported the following module: a combina-tion of performing personal care, being alone, at home, and feeling neu-tral as to how the activity was performed. The second most commonmodule involved consuming mass media and smoking, combined withbeing alone, at home, with negative reflections on the performance, andthey all felt worried and anxious. As many as seven participants werepositive about the outcome and experienced pleasure while performinga playful activity alone at home at least once during the 24-hour period.
Further modules of occupational performance factors clearly demonstratethat most of them included being at home and alone, while the personal ex-perience varied. With the exception of transportation, lonely occupationswere exclusively performed at home. Neutral reflections were predomi-nant in these modules, but the combination of negative reflections and thefeeling of worry and anxiety were also common. Most modules that in-volved transportation involved feelings of paranoia and fear.
When others were included in the occupational performance at homeor in service settings, talking was the most common activity. Another
Ulrika Bejerholm and Mona Eklund 39
TABLE 7. The Most Common Combinations of Occupational PerformanceFactors, N = 10 (24 hr.)
Number ofparticipants
Performedactivities
Geographicenvironment
Emotional reaction,refl. on the outcome
9 personal care home neutral
8 mass media + smoking home negative, worry/anxiety
7 playful activity home positive, pleasure
7 eating/drinking home neutral
6 quiet activity home escapism/emptiness
6 quiet activity home worry/anxiety
6 sleeping home neutral
6 transportation outdoors paranoid/afraid, worry
6 eating/drinking day-care centre neutral
4 mass media + smoking + home worry/anxiety
indoor walking
4 quiet activity day-care centre neutral
4 talking home negative, worry/anxiety
4 talking + eating/drinking + home positive
smoking + mass media
Note: Combinations that are performed alone are in normal type. Combinations that are performed when other people are inthe environment are in italics. Combinations that are performed while interacting socially are in bold letters.

social aspect, that people were present in the environment but not in-volved in the activity, was combined with either eating/drinking orquiet activity. These activities took place at a day-care center and weretypically perceived as neutral. The module that included quiet activity,consuming mass media, eating/drinking, and smoking was performedboth at home and at a health-care center. The only difference betweenthese environmental contexts was that the health-care center triggered anegative reflection and feelings of anxiety, while the home environmentwas perceived as positive.
DISCUSSION
As little is known about the daily occupations of persons with schizo-phrenia, this study aimed to reflect as original a picture as possible. Theleast time was spent in habitual and playful activities, and in accordancewith Weeder’s study (1986), passive activities were predominant. Thepassive lifestyle is characteristic of persons with schizophrenia (Weeder,1986; Suto & Frank, 1994), compared to the general population, whereas little as 5% is spent on passive activities (Juster & Stafford, 1991).
According to Bonder (1997), the way in which social interaction isexperienced has to do with the perception of where the control of eventsrests. Persons with schizophrenia have been shown not to experiencecontrol when social activities were externally initiated (Weeder, 1986).Perhaps some of the social activities performed by the participants inthe present study, such as performing quiet activities while other peoplewere in the environment, made the participants feel in control since theactivity was not externally initiated. Perhaps they preferred a less activesocial role, where they could study and observe their environment attheir own pace, interacting socially according to their own capabilityand keeping in control. The present study, like Weeder’s (1986), clearlyshowed how much importance, perhaps too much importance, profes-sionals and different social activity centers place on the need for awhole conversation to take place. The staff’s empathetic qualities–be-ing interested and understanding, listening to and respecting the pa-tients (Björkman, Hansson Svensson, & Berglund, 1995)–are qualitiesin the social environment that might be essential for persons withschizophrenia, for communicating with others.
This study clearly demonstrated that the participants’ occupationalpattern was characterized by passivity and a low level of structure andorganization. Smoking clearly worked as a behavioral filler for most of
40 OCCUPATIONAL THERAPY IN MENTAL HEALTH

the participants, similar to what was found in a study by Ziedonis andGeorge (1997). What does it mean to have no temporal framework, butto be predominantly passive and to have no time-bound activities? Forpersons with schizophrenia, having a job is often associated with abetter quality of life (Eklund et al., 2001). Still, individuals with mentalhealth problems have been shown to derive less enjoyment, compe-tence, and importance from work than working individuals withoutmental health problems (Crist et al., 2000). In relation to this result, thefinding of a strong relationship between daily occupations in a broadsense and quality of life (Eklund et al., 2001) seems even more impor-tant to acknowledge. It remains to be determined, however, what posi-tive effects account for the more favorable quality of life that comesalong with performing daily activities (Priebe, Warner, Hubschmid, &Eckle, 1998), knowledge related to occupational health that is of specialinterest to occupational therapists.
According to Strong et al. (1999), the quality of a person’s experienceis determined by the outcome of the person-environment-occupationtransaction. It is, therefore, important to understand how different occu-pational performance factors contribute to a more or less effective perfor-mance (Bonder, 1997). The environmental factors are a hindrance or ahelp to people wishing to get involved in activities (Corcoran & Gitlin,1997; Neville et al., 1985). In the present study, the environment did notseem to provide many external cues that triggered any internal pro-cesses or led to interaction. It is as if the activities were performed in avacuum, and in some ways they resembled the institutionalized livingconditions and the passive occupational situation in a hospital ward.Hocking (1997) says that situations like these decrease the opportuni-ties to develop. Arranging and reshaping the environment would mostlikely shape opportunities for promoting occupational performanceamong the participants. This would form an important strategy for occu-pational therapists in their work with this group of clients, diminishingthe gap between the clients’ adaptive capacity and the environmental de-mands (Schkade & Schultz, 1997). As mentioned above, most activitiesreported in this study were not triggered by a facilitating environmentbut rather from within the person, by basic, immediate life needs, a wishfor satisfaction, or wanting to escape reality. This is in line with whatwas found by Suto and Frank (1994), that a person with schizophreniahas this preference for immediate and proximal goal setting. Also, theneutral reflections about the performance of these activities tell us thatthey were neither very meaningful and inspiring nor negative to per-form. It was as if nothing really got hold of the participants, inspiring
Ulrika Bejerholm and Mona Eklund 41

them to interact and seek new challenges. This implies that few activitieswere performed because they were, as Lobo (1998) put it, pleasurableand pursued for their own rewards. Still, persons with schizophrenia doexperience enjoyment (Emerson, Cook, Polatajko, & Segal, 1998).Winnicott (1981) stressed that playful and creative activities promote ahealthy development and a sense of doing. Such self-rewarding activitiescould be introduced as therapy and serve as a basis for a positive spiral ofactivities and development. The participants in this study spent little timeperforming these personally satisfying activities. Clark (1997), however,argued that a small amount of time engaged in these activities may be farmore determinant of health and well-being than more time spent on mini-mally to moderately satisfying activities. Therefore, it could be suggestedthat occupational therapy for persons with schizophrenia should rein-force and extend the duration of these activities.
If anything, the participants in this study had low time pressure, whichis often associated with the lowest levels of mental health (Lobo, 1998;Zuzanek, 1998). Homeless people in a similar situation said that therewas no such thing as time, because the activities they performed meantliving outside society (Robinson, 1997). According to Suto and Frank(1994), the occupational therapist should have an important role in deter-mining who might benefit from a more passive lifestyle, a safe haven.Should it then be a main purpose to help persons back to a technocratic,economy-controlled society, that is hard to relate to even for personswithout disabilities? It might be a better solution to aim for activities andenvironments that, according to Clark (1997), are related to an original,more natural way of being. Still, the activities should have features thatare similar to the society in general, since it is important for this group ofpeople not to form a subculture and remain in a chronically disabled situ-ation. To meet the lack of engagement in activity that was indicated inthis study, structured time-limited activity programs might serve as a trig-ger to overcome lack of personal initiative to engage in daily occupations.
This study did not consider gender differences in relation to time useand occupational performance. There might be differences in howwomen and men with schizophrenia use their time, and a study of gen-der differences in this respect seems warranted.
There is probably no methodology by which the actual dynamics be-tween occupational, environmental, and personal factors could be fullycaught and revealed. In the present study, however, the way in whichoccupational performance factors were combined was studied to in-crease an understanding of the dynamics. Also, the time-use diary em-
42 OCCUPATIONAL THERAPY IN MENTAL HEALTH

ployed is considered to come close enough, giving a realistic picture ofongoing lives (Robinson, 1985; Szalai, 1972). Still, the time-use diaryand the supplementary interview could only reflect certain facets ofwhat went on in the participants’ daily occupational repertoire. Whetheror not a person with schizophrenia is capable of reliably filling in theself-report instrument and participating in the supplementary interviewis a relevant issue to discuss. Cognitive impairments (Spaulding et al.,1999), flattening of affect, and a feeling of alienation (Gerhardsson &Jonsson, 1996) may influence the ability to identify recent experiences ofeveryday life by means of a questionnaire. Clinical experiences, how-ever, have indicated that a time-use diary and a supplementary interviewconstitute an appropriate and useful method when assessing occupationalperformance among persons with schizophrenia. The time-use diaryseemed to provide a temporal order, the natural logic in which activitiesare performed helped the participants to remember. Since little timepassed between the actual performance and the recording of the experi-ence, the occupational performance was still fresh in mind. In addition,the bias effect in the exaggeration of socially acceptable activities isalso likely to be minimized (Robinson, 1977). The fact that this study isbased on reports from a singular weekday may be seen as a limitation.In this study, however, it is not the individual perspective on time useand occupational performance that is in the center of attention. Rather,the focus is on persons belonging to the one and same population, shar-ing common features and patterns. When a group perspective is appliedon time use, a 24-hour diary is normally used (Szalai,1972).
In conclusion, the participants performed most activities alone intheir home environment. Few occupational situations worked as a rou-tine, providing a structure in terms of familiarity of habits. Apart fromthese few habitual activities and the playful activities reported, the par-ticipants did not really seem to interact with the environment; they wererather observing or escaping from it. Furthermore, many activities wereaccompanied with a feeling of emptiness and neutral reflection over theoccupational outcome. These results converge into a picture of stagna-tion and emptiness permeating the participants’ occupational patternand time use. From an occupational therapy point of view it wouldprobably be important to help reshape the environment and help regainroles that involve interacting with the outside world.
Ulrika Bejerholm and Mona Eklund 43

REFERENCES
American Psychiatric Association. (1994). Diagnostic and statistical manual of mentaldisorders, DSM IV (4th ed.). Washington, DC: Author.
Björkman, T., Hansson, L., Svensson, B., & Berglund, I. (1995). What is important inpsychiatric outpatient care? Quality of care from a patient’s perspective. Interna-tional Journal for Quality in Health Care, 7, 355-362.
Bonder, R. (1997). Coping with psychological and emotional challenges. In C. Christiansen &C. Baum (Eds.), Occupational therapy: Enabling function and well-being (2nd ed.).Thorofare, NJ: Slack.
Christiansen, C., & Baum, C. (1997). Occupational therapy: Enabling function andwell-being (2nd ed.). Thorofare, NJ: Slack.
Clark, F. (1997). Reflections on the human as an occupational being: Biological need,tempo and temporality. Journal of Occupational Science: Australia, 4, 86-92.
Corcoran, M., & Gitlin, L. (1997). The role of the physical environment in occupa-tional performance. In C. Christiansen & C. Baum (Eds.), Occupational therapy:Enabling function and well-being (2nd ed.). Thorofare, NJ: Slack.
Creek, J. (Ed.) (1997). Occupational therapy and mental health (2nd ed.). London:Churchill Livingstone.
Crist, P., Davis, C., & Coffin, P. (2000). The effects of employment and mental healthstatus on the balance of work, play/leisure, self-care, and rest. Occupational Ther-apy in Mental Health, 15, 27-42.
Cynkin, S., & Robinson, A.M. (1990). Occupational therapy and activities health:Toward health through activities. Boston/London/Toronto: Little Brown and Co.
Dunn, W., Brown, C., & McGuigan, A. (1994). The ecology of human performance: Aframework for considering the effect of context. American Journal of OccupationalTherapy, 48, 595-607.
Eklund, M., Hansson, L., & Bejerholm, U. (2001). Relationships between occupa-tional factors and health-related variables among people with schizophrenia. SocialPsychiatry and Psychiatric Epidemiology, 3, 79-85.
Ellegård, K., & Nordell, K. (1997). Att byta vanmakt mot egenmakt. [To change power-lessness into power of self]. Stockholm: Johansson & Skyttmo Förlag AB.
Emerson, H., Cook, J., Polatajko, H., & Segal, R. (1998). Enjoyment experiences asdescribed by persons with schizophrenia: A qualitative study. Canadian Journal ofOccupational Therapy, 4, 183-192.
Erlandsson, L-K., & Eklund, M. (2001). Describing patterns of daily occupations–Amethodological study comparing data from four different methods. ScandinavianJournal of Occupational Therapy, 8, 31-39.
Fox, D.J. (1992). Fundamentals of research nursing (4th ed.). Norwalk, CT:Appleton-Century-Croft.
Gerhardsson, C., & Jonsson, H. (1996). Experience of therapeutic occupations inschizophrenic participants: Clinical observations organised in terms of the flow the-ory. Scandinavian Journal of Occupational Therapy, 3, 149-155.
Hartocollis, P. (1975). Time and affect in psychopathology. Journal of American Psy-choanalysis Association, 23, 383-395.
44 OCCUPATIONAL THERAPY IN MENTAL HEALTH

Hocking, C. (1997). Person-object interaction model: Understanding the use of every-day objects. Journal of Occupational Science, 4, 27-35.
Juster, F.T., & Stafford, F.P. (1991). The allocation of time: Empirical findings, be-havioural models, and problems of measurements. Journal of Economic Literature,24, 471-522.
Karlsson, E., Söderback, I., Synnerholm, M., Ekholm, J., & Bergroth, A. (1996).Självskattad tidsanvändning under arbete och sjukfrånvaro [Self-assessed time useduring work and sick leave]. (Rapport nr 3) Östersund, Sweden: Centrum försocialförsäkringsforskning.
Kielhofner, G. (1995). A model of human occupation (2nd ed.). Baltimore: Williams &Wilkins.
Kielhofner, G. (1997). Conceptual foundations of occupational therapy (2nd ed.).Philadelphia: F. A. Davis.
Knafl, K., & Breitmayer, B. J. (1989). Triangulation in qualitative research: Issues ofconceptual clarity and purpose. In J. Morse (Ed.), Qualitative nursing research: Acontemporary dialogue. Rockville, MD: Aspen.
Krefting, L. (1991) Rigor in qualitative research: The assessment of trustworthiness.American Journal of Occupational Therapy, 45, 214-222.
Law, M., Cooper, B.A., Stewart, D., Letts, L., Rigby, P., & Strong, S. (1997). Theoreti-cal contexts for the practice of occupational therapy. In C. Christiansen & C. Baum(Eds.) Occupational therapy: Enabling function and well-being (2nd ed.).Thorofare, NJ: Slack.
Law, M., Cooper, B.A., Strong, S., Stewart, D., Rigby, P., & Letts, L. (1996). The per-son-environment-occupation model: A transactive approach to occupational per-formance. Canadian Journal of Occupational Therapy, 63, 9-23.
Lobo, F. (1998). Social transformation and the changing work-leisure relationship inthe late 1990s. Journal of Occupational Science, 5, 147-154.
McLaughlin Gray, J. (2001). Discussion of the ICIDH-2 in relation to occupationaltherapy and occupational science. Scandinavian Journal of Occupational Therapy,8, 19-30.
McLaughlin Gray, J., Kennedy, B. L. & Zemke, R. (1996). Dynamic systems theory:An overview. In R. Zemke & F. Clarke (Eds.) Occupational Science. The evolvingdiscipline. Philadelphia: F. A. Davis.
Melges, F.T. (1982). Time and the inner future. New York: John Wiley & Sons.Meyer, A. (1922/1977). The philosophy of occupational therapy. American Journal of
Occupational Therapy, 31, 639-642.Neville, A. (1980). Temporal adaption: Application with short-term psychiatric patients.
American Journal of Occupational Therapy, 34, 328-331.Neville, A., Kreisberg, A., & Kielhofner, G. (1985). Temporal dysfunction in schizo-
phrenia. Occupational Therapy in Mental Health, 5, 1-19.Pentland, W., Harvey, A.S., & Walker, J. (1998). The relationship between time use
and health and well-being in men with spinal cord injury. Journal of OccupationalScience, 5, 14-25.
Persson, D., Erlandsson, L-K., Eklund, M., & Iwarsson, S. (2001). Value dimensions,meaning, and complexity in human occupation–A tentative structure for analysis.Scandinavian Journal of Occupational Therapy, 8, 7-18.
Ulrika Bejerholm and Mona Eklund 45

Priebe, S., Warner, R., Hubschmid, T., & Eckle, I. (1998). Employment, attitudes to-ward work, and quality of life among people with schizophrenia in three countries.Schizophrenia Bulletin, 24, 469-477.
Robinson, J.P. (1977). How Americans use time. New York: Praeger Publishers.Robinson, J.P. (1985). The validity and reliability of diaries versus alternative time use
measures. In F.T. Juster & F.P. Stafford (Eds.) Time, goods, and well-being. Uni-versity of Michigan: Institute for Social Research.
Robinson, J. P. (1997). Time for life. University Park: The Pennsylvania State Univer-sity Press.
Rosenthal, L., & Howe, M. (1984). Activity patterns and leisure concepts: A compari-son of temporal adaptation among day versus night shift workers. OccupationalTherapy in Mental Health, 4, 59-78.
Schkade, J.K., & Schultz, S. (1997). Adaptation. In C. Christiansen & C. Baum (Eds.)Occupational therapy: Enabling function and well-being (2nd ed.). Thorofare, NJ:Slack.
Slagle, E.C. (1922). Training aides for mental patients. Archives of Occupational Ther-apy, 1, 11-16.
Sommer, B., & Sommer, R. (1991). A practical guide to behavioural research. Toolsand techniques (3rd ed.). Oxford: Oxford University Press.
Spaulding, W., Fleming, S., Reed, D., Sullivan, M., Storzbach, D., & Lam, M. (1999).Cognitive functioning in schizophrenia: Implications for psychiatric rehabilitation.Schizophrenia Bulletin, 25, 275-289.
Statistiska centralbyrån (SCB). (1992). I tid och otid 1990/1991 Levnadsförhållanden.Rapport 79. Stockholm.
Strong, S., Rigby, P., Stewart, D., Law, M., Letts, L., & Cooper, B. (1999). Applicationof the person-environment-occupation model: A practical tool. Canadian Journalof Occupational Therapy, 63, 122-133.
Suto, M., & Frank, G. (1994). Future time perspective and daily occupations of personswith chronic schizophrenia in a board and care home. American Journal of Occupa-tional Therapy, 48, 7-18.
Szalai, A. (1972). The use of time. Daily activities of urban and suburban populationsin twelve countries. Paris: Mouton & Co.
Tsang, H., & Pearson. (2000). Reliability and validity of a simple measure for assess-ing the social skills of people with schizophrenia necessary for seeking and securinga job. Canadian Journal of Occupational Therapy, 67, 250-259.
von Bertalanffy, L.M. (1968). General systems theory: Foundations, development,and applications. New York: Brazillier.
Weeder, T.C. (1986). Comparison of temporal patterns and meaningfulness of thedaily activities of schizophrenic and normal adults. Occupational Therapy in Men-tal Health, 6, 27-48.
Wilcock, A. (1995). The occupational brain: A theory of human nature. Journal ofOccupational Science: Australia, 2, 68-73.
Wilcock, A., van der Arend, H., Darling, K., Scholz, J., Sidall, R., Snigg, C., &Stephens, J. (1998). An exploratory study of people’s perceptions and experiencesof wellbeing. British Journal of Occupational Therapy, 61, 75-82.
Winnicott, D.W. (1981). Playing and reality. London: Tavistock.
46 OCCUPATIONAL THERAPY IN MENTAL HEALTH

World Health Organization (2001). International classification of functioning, disabil-ity and health. Geneva: World Health Organization.
Zemke, R., & Clarke, F. (1996). Occupational Science. The evolving discipline. Phila-delphia: F. A. Davis.
Ziedonis, D. M., & George, T. P. (1997). Schizophrenia and nicotine use: Report of apilot smoking cessation program and review of neurobiological and clinical issues.Schizophrenia Bulletin, 23, 247-254.
Zuzanek, J. (1998). Time use, time pressure, personal stress, mental health, and life sat-isfaction from a life cycle perspective. Journal of Occupational Science, 5, 26-39.
RECEIVED: 07/16/02REVISED: 10/14/02
ACCEPTED: 12/02/02
Ulrika Bejerholm and Mona Eklund 47
For FACULTY/PROFESSIONALS with journal subscriptionrecommendation authority for their institutional library . . .
Please send me a complimentary sample of this journal:
(please write complete journal title here–do not leave blank)
If you have read a reprint or photocopy of this article, would you like tomake sure that your library also subscribes to this journal? If you havethe authority to recommend subscriptions to your library, we will send youa free complete (print edition) sample copy for review with your librarian.
1. Fill out the form below and make sure that you type or write out clearly both the nameof the journal and your own name and address. Or send your request via e-mail [email protected] including in the subject line “Sample Copy Request”and the title of this journal.
2. Make sure to include your name and complete postal mailing address as well as yourinstitutional/agency library name in the text of your e-mail.
[Please note: we cannot mail specific journal samples, such as the issue in which a specific article appears.Sample issues are provided with the hope that you might review a possible subscription/e-subscription withyour institution's librarian. There is no charge for an institution/campus-wide electronic subscriptionconcurrent with the archival print edition subscription.]
I will show this journal to our institutional or agency library for a possible subscription.Institution/Agency Library: ______________________________________________
Name: _____________________________________________________________
Institution: __________________________________________________________
Address: ___________________________________________________________
City: ____________________Return to: Sample Copy Department,The Haworth Press, Inc.,
10 Alice Street, Binghamton, NY 13904-1580
State: __________ Zip: ____________________