4 Rheumatoid Arthriis 2010
30
Rheumatoid Arthritis (RA) • A chronic, systemic disease characterized by inflammation of connective tissue in the synovial joints • Typically have periods of remission and exacerbation
-
Upload
northtec -
Category
Health & Medicine
-
view
239 -
download
0
description
pathophysiology
Transcript of 4 Rheumatoid Arthriis 2010

Rheumatoid Arthritis (RA)
• A chronic, systemic disease characterized by inflammation of connective tissue in the synovial joints
• Typically have periods of remission and exacerbation

Rheumatoid Arthritis (RA)
• Affects all ethnic groups• Can occur at any time of life• Incidence ↑ with age• Women are affected 2-3 times
more frequently then men• Smoking appears to be a link

Etiology and Pathophysiology
• Cause of RA is unknown• No infectious agent has been
cultured from blood and synovial tissue or fluid
• Autoimmune etiology is currently the most widely accepted

Etiology and Pathophysiology
• Autoimmunity – Changes begin when a susceptible
host experiences an initial immune response to an antigen
– Antigen triggers the formation of an abnormal immunoglobulin G (IgG)

Etiology and Pathophysiology
• Autoimmunity – RA is characterized by the presence of
autoantibodies (rheumatoid factor [RF])– RF and IgG form immune complexes
that initially deposit on synovial membranes or superficial articular cartilage in the joints
– An inflammatory response results

Etiology and Pathophysiology
• Autoimmunity – Joint changes from chronic
inflammation begin when the hypertrophied synovial membrane invades the surrounding • Cartilage• Ligaments• Tendons• Joint capsule

Etiology and Pathophysiology
• Autoimmunity – Pannus (a proliferation of synovial tissue) forms
within the joint– Eventually covers and erodes the entire surface
of the articular cartilage– Pannus scars and shortens supporting structures
• Tendons• Ligaments
– Causing joint laxity, subluxation, and contracture

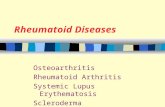
A. Synovial swelling & fluid accululation
B. Pannus, eroded articular cartilage & joint space narrowing

Joint space narrowing and osteophytes

Etiology and Pathophysiology
• Genetic factors– Genetic predisposition appears to be
important in the development of RA– Strongest evidence for a familial
influence is the ↑ occurrence of certain human leukocyte antigens (HLA)

Clinical Manifestations Joints
• Onset of RA is typically insidious• Nonspecific manifestations may
precede the onset of arthritic complaints– Fatigue– Anorexia– Weight loss– Generalized stiffness

Clinical Manifestations Joints
• Stiffness becomes more localized in the following weeks to months
• Some patients report a history of precipitating stressful events– Research has been unable to
correlate such events directly with the onset of RA

Clinical Manifestations Joints
• Specific joint involvement – Pain– Stiffness– Limitation of motion– Signs of inflammation
• Heat• Swelling• Tenderness

Clinical Manifestations Joints
• Joint symptoms occur symmetrically and frequently– Small joints of the hands and feet– Larger peripheral joints
• Wrists, elbows, shoulders, knees, hips, ankles, and jaw
– Cervical spine

Clinical Manifestations Joints
• Often experience joint stiffness after periods of inactivity
• Morning stiffness may last from 60 minutes to several hours or more
• Joints become tender, painful, and warm to the touch

Clinical Manifestations Joints
• Joint pain– ↑ with motion – Varies in intensity– May not be proportional to the
degree of inflammation – Tenosynovitis
• Difficult for patients to grasp objects

Clinical Manifestations Joints
• Inflammation and fibrosis of the joint capsule and supporting structures may lead to deformity and disability
• Subluxation– Atrophy of muscles and destruction of
tendons around the joint cause one articular surface to slip past the other

Early Rheumatoid Athritis

Advanced Rheumatoid Athritis

Deformities of RA
Fig. 63-4

Clinical Manifestations Extraarticular Manifestations
• RA can affect nearly every system of the body
• Three most common – Rheumatoid nodules – Sjögren syndrome– Felty syndrome

Extraarticular Manifestations of RA
Fig. 63-5

Rheumatoid Nodules• Develop in 25% of all patients with RA• Usually have high titers of RF• Appear as firm, nontender,
granuloma-type masses • Usually over the extensor surfaces of
joints such as fingers and elbows

Rheumatoid Nodules• Nodules at the base of the spine
and back of the head are common in older adults
• Develop insidiously • Can persist or regress
spontaneously• Usually not removed

Rheumatoid Nodules

Rheumatoid Nodules - elbow

Rheumatoid Nodules

Complications • Flexion contractures and hand
deformities – Cause diminished grasp strength – Affect the patient’s ability to perform
self-care tasks

Complications • Cataract development and loss of
vision possible from scleral nodules
• Rheumatoid nodules can ulcerate, similar to pressure ulcers
• Hoarseness from nodules on the vocal cords

Complications • Bone destruction from nodules in
the vertebral bodies• Cardiopulmonary effects later in
the disease– Pleurisy, pleural effusion, pericarditis,
pericardial effusion, cardiomyopathy
• Carpal tunnel syndrome