4-Aminopyridine Treatment for Chronic Spinal Cord Injury
10
4-Aminopyridine treatment for chronic spinal cord injury Dr. Young, What is the average dosage required for 4 AP to work? I started a fe w days ago at 10 mg twice a day. I was extremely tired at first and experienced more intense neuropathic (pressure)pain, but I feel ready to increase the dosage. I will wait for my doctor's opinion of course, but I read that one had to take at least 30 mg to get results. Please let me know what you think. I would also like to know if getting deep anal sensations ( I realized I c ould now feel a suppository) means that the drug is working for me? Thanks. gretchen 1 Gretchen, Let me start from the beginning. Until recently, I have been reluctant to post much about 4 -aminopyridine (4-AP) or fampridine for three reasons. First, although the drug can be dispensed by compounding pharmacies, there is limited data concerning the quality a nd shelf-life of the drug. I had heard that some formulations of the drug may lose as much as 10% of its potency per week. Second, Acorda Therapeutics was running two phase 3 clinical trials to assess a new sustained release formulation of the d rug (Fampridine SR). Since I am on the Board of Directors of Acorda Therapeutics, I did not want my comments interpreted by the FDA or others as being for or against compounded formulations. Third, the drug is not innocuous and should not be taken without close supervision by a physician. I was forced to comment when I found out that many are taking the drug with minimal physician supervision. Last year, unfortunately, the two Acorda-run phase 3 clinical trials assessing Fampridine SR in people with chronic spinal cord injury did not meet the effica cy criteria of significantly reducing spasticity in people with chronic spinal cord injury. This failure may have been due to several reasons. First, in theory, only people with demyelinated axons should show improvements in motor and sensory function. The reason why spasticity was chosen as the primary outcome measures of these trials was because phase 2 trials suggested that more people show reduced spasticity. Second, the effective dose of the drug is close to doses that cause unacceptable side effects such as seizures. Therefore, the dose of the drug was kept at a level where no seizures were seen. Third, people recruited into the trials had to have severe spasticity but were allowed to continue taking other anti-spasticity drugs such a s baclofen. It is possible that some people reduced their other anti-spasticity drugs to qualify for the trial. The trials suggested that both the control a nd the treated groups had reduced spasticity. Due to lack of funding for more clinical trials of Fampridine SR in spinal cord injury, Acorda Therapeutics has decided to focus on developing Fampridine SR for multiple sclerosis where a large percentage of patients show improved motor and sensory function on the drug. Once the drug is approved for MS, the company can go back a nd redo clinical trials for spinal cord injury. The company therefore stopped fampridine trials for spinal cord injury. It may be several years before the drug is approved for spinal cord injury. Therefore, I feel that it is appropriate for me to discuss the compounding formulations of 4 -AP and its use in spinal cord injury. Several polls on CareCure suggested that as many as 15% of people with chronic spinal cord injury have tried or are taking 4-AP. Many questions are asked over and over again. Therefore, I will try to answer the most frequently asked questions: What is the difference between immediate-release and time-release formulations of 4-AP? At the present, 4-AP comes from compounding pharmacies in two f ormulations. One is called immediate release or is just the drug mixed with filler and placed in a capsule. This is the most common form of the drug. The other is a
-
Upload
gustavo-cabanas -
Category
Documents
-
view
13 -
download
0
Transcript of 4-Aminopyridine Treatment for Chronic Spinal Cord Injury
4-Aminopyridine treatment for chronic spinal cord injuryDr. Young,
What is the average dosage required for 4 AP to work? I started a few days ago at 10 mg twice a day. I was extremely tired at first and experienced more intense neuropathic (pressure)pain, but I feel ready to increase the dosage. I will wait for my doctor's opinion of course, but I read that one had to take at least 30 mg to get results. Please let me know what you think.
I would also like to know if getting deep anal sensations ( I realized I could now feel a suppository) means that the drug is working for me?
Thanks.
gretchen 1Gretchen,
Let me start from the beginning. Until recently, I have been reluctant to post much about 4-aminopyridine (4-AP) or fampridine for three reasons. First, although the drug can be dispensed by compounding pharmacies, there is limited data concerning the quality and shelf-life of the drug. I had heard that some formulations of the drug may lose as much as 10% of its potency per week. Second, Acorda Therapeutics was running two phase 3 clinical trials to assess a new sustained release formulation of the drug (Fampridine SR). Since I am on the Board of Directors of Acorda Therapeutics, I did not want my comments interpreted by the FDA or others as being for or against compounded formulations. Third, the drug is not innocuous and should not be taken without close supervision by a physician. I was forced to comment when I found out that many are taking the drug with minimal physician supervision.
Last year, unfortunately, the two Acorda-run phase 3 clinical trials assessing Fampridine SR in people with chronic spinal cord injury did not meet the efficacy criteria of significantly reducing spasticity in people with chronic spinal cord injury. This failure may have been due to several reasons. First, in theory, only people with demyelinated axons should show improvements in motor and sensory function. The reason why spasticity was chosen as the primary outcome measures of these trials was because phase 2 trials suggested that more people show reduced spasticity. Second, the effective dose of the drug is close to doses that cause unacceptable side effects such as seizures. Therefore, the dose of the drug was kept at a level where no seizures were seen. Third, people recruited into the trials had to have severe spasticity but were allowed to continue taking other anti-spasticity drugs such as baclofen. It is possible that some people reduced their other anti-spasticity drugs to qualify for the trial. The trials suggested that both the control and the treated groups had reduced spasticity.
Due to lack of funding for more clinical trials of Fampridine SR in spinal cord injury, Acorda Therapeutics has decided to focus on developing Fampridine SR for multiple sclerosis where a large percentage of patients show improved motor and sensory function on the drug. Once the drug is approved for MS, the company can go back and redo clinical trials for spinal cord injury. The company therefore stopped fampridine trials for spinal cord injury. It may be several years before the drug is approved for spinal cord injury. Therefore, I feel that it is appropriate for me to discuss the compounding formulations of 4-AP and its use in spinal cord injury. Several polls on CareCure suggested that as many as 15% of people with chronic spinal cord injury have tried or are taking 4-AP. Many questions are asked over and over again. Therefore, I will try to answer the most frequently asked questions:
What is the difference between immediate-release and time-release formulations of 4-AP?At the present, 4-AP comes from compounding pharmacies in two formulations. One is called immediate release or is just the drug mixed with filler and placed in a capsule. This is the most common form of the drug. The other is a time-release formulation where the drug dissolves slower. The immediate release formulation causes a rapid rise of the blood drug levels within about half an hour and then falls gradually to about half of its level within 6 hours. To maintain the level, one has to take a capsule every 5-6 hours. Little is known about the time-release capsule from compounding pharmacies. Acorda Therapeutics has developed and is testing a sustained release (SR) formulation with a half-time of about 12 hours, allowing higher doses of the drug to be taken every 12 hours.
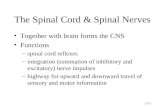
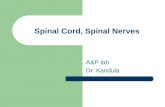
How does 4-AP work?4-AP blocks the fast voltage-sensitive potassium channel on neurons and other excitable tissues such as the heart and muscle. This has two effects on the nervous system. First, the potassium channel is responsible for shortening the duration of action potentials (the signals that axons conduct). Blocking the potassium channel increases duration of the action potentials and allows the signals to conduct through demyelinated areas. Second, the duration of the action potential determines the amount of neurotransmitters released by the axons. Thus, 4-AP not only increases the reliability of action potentials but strengthens their effects when they get through. In recommended doses, it primarily affects demyelinated axons and has relatively little effect on normally myelinated axons. At higher doses, however, it begins to affect normal axons and neurons, as well as heart, muscle, and other excitable tissues of the body. The effect of 4-AP goes away when the drug level drop below certain levels.
Researchers have shown how an experimental drug might restore the function of nerves damaged in spinal cord injuries by preventing short circuits caused when tiny "potassium channels" in the fibers are exposed by trauma. The compound also might be developed as a treatment for multiple sclerosis. This diagram illustrates how the drug functions as a "channel blocker," meaning it permits the conduction of signals even though the protective myelin insulation has been damaged.Credit: Purdue University, Department of Basic Medical Sciences
Will 4-AP help me?It is difficult to predict whether 4-AP will have an effect on a given person. If the person does not have demyelinated axons crossing the injury site, 4-AP should not improve motor or sensory function. Only about a third of people with spinal cord injury have demyelinated axons as a cause of their neurological loss. In people who do have demyelinated axons crossing the injury site, it should strengthen motor and sensory function. In addition, 4-AP reduces spasticity without weakening muscles. Other anti-spasticity drugs such as baclofen reduce spasticity but at the same time will weaken voluntarily muscle activation. 4-AP may also reduce neuropathic pain but this effect is mixed because 4-AP increases pain sensations. Some people who have taken 4-AP have discovered that they have pain that is masked by their spinal cord injury. Because different people have different populations of demyelinated axons, the degree of improvement and type function vary considerably from person to person.
What bad effects do 4-AP have?In general, 4-AP increases excitability of the nervous system. Side-effects of the drug include insomnia, nervousness, tingling, increased blood pressure and heart rate, and trembling. Also, at doses of greater than 10 mg, 4-AP may cause seizures in susceptible people. The side effects depend on peak blood drug levels. The immediate release formulation results in peak blood levels within 30 minutes and gradually decline to half that level in about 6 hours. The drug is cleared by the kidney and blood levels of the drug can be abnormally elevated if a person has renal problems (such as kidney damage or infection). The side effects are most prominent when a person starts taking the drug but they diminish after several days while the improvement in conduction remains. In very high overdoses, 4-AP can provoke overwhelming excitation of the nervous system, including status epilepticus (continuous seizures), life-threatening hypertension, cardiac arrythmias, and hyperthermia.
I hope that this is helpful.
Wise.Fampridine (4-AP)Trauma, ischemia, and inflammation demyelinate the spinal cord. 4-aminopyridine (4-AP or fampridine) blocks potassium channels on demyelinated axons, improves conduction, and increases neurotransmitter release [49]. In 1981, Bostock, et al. [50] reported that 4-AP improves conduction in demyelinated axons and Zangger, et al. [51] showed that it also facilitates L-DOPA induced spinal locomotor rhythms in spinal-injured animals. In 1986, Eliasson, et al. [52] showed that 4-AP restores conduction in heat-injured nerve and spinal roots in animals. In 1987, Bowe, et al. [53] confirmed that 4-AP improves conduction in demyelinated axons and Blight & Gruner [54] found that 4-AP improved vestibulospinal free fall responses in spinal-injured cats. In 1989, Blight et al. studied the effects of 4-AP in dogs [55] and proposed clinical trials of 4-AP in spinal cord injury.In 1993, Hansebout, et al. [56] did the a double-blind, crossover trial of 4-AP in eight patients, finding the drug improved motor and sensory function. Hayes, et al. [57] confirmed the 4-AP effects on function [58] and motor evoked potentials [59] in patients with spinal cord injury. In 1997, Segal & Brunnemann [60] found that 4-AP improves pulmonary function in quadriplegic humans with chronic spinal cord injury [60]. In 1997, Acorda Therapeutics licensed the use patent for 4-AP treatment of spinal cord injury. In 1998, Potter, et al. [61] did a randomized crossover trial of a sustained release 4-AP (Fampridine SR) made by Elan. In 1999, Acorda partnered with Elan to develop Fampridine SR, including preclinical studies [62, 63], studies to assess pharmacokinetics of intravenous [64], intrathecal [65], oral [66] 4AP in humans and animals [67].In 2001, van der Bruggen, et al. [68] found that 4-AP (0.5 mg/kg) did not improve neurological function of 20 patients with chronic incomplete spinal cord injury. However, 4-AP improved motor evoked potentials patients with chronic spinal cord injury [69] and Grijalva, et al. [70] randomized 27 patients to 4-AP or placebo, and found that 30 mg/day 4AP for 12 weeks improved neurological function in 69% compared to 46% on placebo. In 2004, Deforge, et al. [71] found no difference between 4-AP (40 mg/day) or placebo in 15 people who were walking after spinal cord injury.From 2005 to 2007, after a phase 2 [72], more pharmacokinetics [73, 74] and safety trials [75], Acorda did two large randomized placebo-controlled phase 3 trials involving over 800 patients with chronic spinal cord injury to assess Fampridine SR effects on spasticity. Both trials [not yet published] showed no significant difference between Fampridine SR and placebo. However, Acorda also did two phase 3 clinical trials that showed that Fampridine SR significantly improves walking performance in multiple sclerosis (MS).In summary, over a decade of clinical trials yielded promising and conflicting results concerning 4-AP effects on chronic spinal cord injury. The trials surprisingly revealed that people with spinal cord injury are susceptible to placebo. Over 40% of patients responded to placebo and perhaps half of the patients responded to 4-AP. Until better outcome measures can be found, it may be better to choose a condition that is more responsive to 4-AP and go back later to demonstrate efficacy for spinal cord injury.49. transmission in excitatory and inhibitory synapses in the spinal cord. Brain Res 136: 387-92.50. transmission in excitatory and inhibitory synapses in the spinal cord. Brain Res 136: 387-92.51. Bostock H, Sears TA and Sherratt RM (1981). The effects of 4-aminopyridine and tetraethylammonium ions on normal and demyelinated mammalian nerve fibres. J Physiol 313: 301-15.52. Zangger P (1981). The effect of 4-aminopyridine on the spinal locomotor rhythm induced by L-DOPA. Brain Res 215: 211-23.53. Eliasson SG, Monafo WW and Meyr D (1986). Potassium ion channel blockade restores conduction in heat-injured nerve and spinal nerve roots. Exp Neurol 93: 128-37.54. Bowe CM, Kocsis JD, Targ EF and Waxman SG (1987). Physiological effects of 4-aminopyridine on demyelinated mammalian motor and sensory fibers. Ann Neurol 22: 264-8.55. Blight AR and Gruner JA (1987). Augmentation by 4-aminopyridine of vestibulospinal free fall responses in chronic spinal-injured cats. J Neurol Sci 82: 145-59. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=283130756. Blight AR, Toombs JP, Bauer MS and Widmer WR (1991). The effects of 4-aminopyridine on neurological deficits in chronic cases of traumatic spinal cord injury in dogs: a phase I clinical trial. J Neurotrauma 8: 103-19. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=187013457. Hansebout RR, Blight AR, Fawcett S and Reddy K (1993). 4-Aminopyridine in chronic spinal cord injury: a controlled, double-blind, crossover study in eight patients. J Neurotrauma 10: 1-18. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=832072858. Hayes KC, Blight AR, Potter PJ, Allatt RD, Hsieh JT, Wolfe DL, Lam S and Hamilton JT (1993). Preclinical trial of 4-aminopyridine in patients with chronic spinal cord injury. Paraplegia 31: 216-24. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=849303659. Hayes KC, Potter PJ, Wolfe DL, Hsieh JT, Delaney GA and Blight AR (1994). 4-Aminopyridine-sensitive neurologic deficits in patients with spinal cord injury. J Neurotrauma 11: 433-46. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=783728360. Qiao J, Hayes KC, Hsieh JT, Potter PJ and Delaney GA (1997). Effects of 4-aminopyridine on motor evoked potentials in patients with spinal cord injury. J Neurotrauma 14: 135-49. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=910493161. Segal JL and Brunnemann SR (1997). 4-Aminopyridine improves pulmonary function in quadriplegic humans with longstanding spinal cord injury. Pharmacotherapy 17: 415-23. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=916554562. Potter PJ, Hayes KC, Hsieh JT, Delaney GA and Segal JL (1998). Sustained improvements in neurological function in spinal cord injured patients treated with oral 4-aminopyridine: three cases. Spinal Cord 36: 147-55. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=955401263. Shi R and Blight AR (1997). Differential effects of low and high concentrations of 4-aminopyridine on axonal conduction in normal and injured spinal cord. Neuroscience 77: 553-62. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=947241164. Shi R, Kelly TM and Blight AR (1997). Conduction block in acute and chronic spinal cord injury: different dose-response characteristics for reversal by 4-aminopyridine. Exp Neurol 148: 495-501. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=941782865. Donovan WH, Halter JA, Graves DE, Blight AR, Calvillo O, McCann MT, Sherwood AM, Castillo T, Parsons KC and Strayer JR (2000). Intravenous infusion of 4-AP in chronic spinal cord injured subjects. Spinal Cord 38: 7-15. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1076219266. Halter JA, Blight AR, Donovan WH and Calvillo O (2000). Intrathecal administration of 4-aminopyridine in chronic spinal injured patients. Spinal Cord 38: 728-32. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1117537267. Segal JL, Hayes KC, Brunnemann SR, Hsieh JT, Potter PJ, Pathak MS, Tierney DS and Mason D (2000). Absorption characteristics of sustained-release 4-aminopyridine (fampridine SR) in patients with chronic spinal cord injury. J Clin Pharmacol 40: 402-9. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1076116868. Hayes KC, Potter PJ, Hsieh JT, Katz MA, Blight AR and Cohen R (2004). Pharmacokinetics and safety of multiple oral doses of sustained-release 4-aminopyridine (Fampridine-SR) in subjects with chronic, incomplete spinal cord injury. Arch Phys Med Rehabil 85: 29-34. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1497096469. van der Bruggen MA, Huisman HB, Beckerman H, Bertelsmann FW, Polman CH and Lankhorst GJ (2001). Randomized trial of 4-aminopyridine in patients with chronic incomplete spinal cord injury. J Neurol 248: 665-71. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1156989470. Wolfe DL, Hayes KC, Hsieh JT and Potter PJ (2001). Effects of 4-aminopyridine on motor evoked potentials in patients with spinal cord injury: a double-blinded, placebo-controlled crossover trial. J Neurotrauma 18: 757-71. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1152698271. Grijalva I, Guizar-Sahagun G, Castaneda-Hernandez G, Mino D, Maldonado-Julian H, Vidal-Cantu G, Ibarra A, Serra O, Salgado-Ceballos H and Arenas-Hernandez R (2003). Efficacy and safety of 4-aminopyridine in patients with long-term spinal cord injury: a randomized, double-blind, placebo-controlled trial. Pharmacotherapy 23: 823-34. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1288509572. DeForge D, Nymark J, Lemaire E, Gardner S, Hunt M, Martel L, Curran D and Barbeau H (2004). Effect of 4-aminopyridine on gait in ambulatory spinal cord injuries: a double-blind, placebo-controlled, crossover trial. Spinal Cord 42: 674-85. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1535667673. Cardenas DD, Ditunno J, Graziani V, Jackson AB, Lammertse D, Potter P, Sipski M, Cohen R and Blight AR (2007). Phase 2 trial of sustained-release fampridine in chronic spinal cord injury. Spinal Cord 45: 158-68. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1677303774. Hayes KC, Katz MA, Devane JG, Hsieh JT, Wolfe DL, Potter PJ and Blight AR (2003). Pharmacokinetics of an immediate-release oral formulation of Fampridine (4-aminopyridine) in normal subjects and patients with spinal cord injury. J Clin Pharmacol 43: 379-85. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1272345875. Hayes KC, Potter PJ, Hansebout RR, Bugaresti JM, Hsieh JT, Nicosia S, Katz MA, Blight AR and Cohen R (2003). Pharmacokinetic studies of single and multiple oral doses of fampridine-SR (sustained-release 4-aminopyridine) in patients with chronic spinal cord injury. Clin Neuropharmacol 26: 185-92. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=12897638Bostock H, Sears TA and Sherratt RM (1981). The effects of 4-aminopyridine and tetraethylammonium ions on normal and demyelinated mammalian nerve fibres. J Physiol 313: 301-15.1. Zangger P (1981). The effect of 4-aminopyridine on the spinal locomotor rhythm induced by L-DOPA. Brain Res 215: 211-23.2. Eliasson SG, Monafo WW and Meyr D (1986). Potassium ion channel blockade restores conduction in heat-injured nerve and spinal nerve roots. Exp Neurol 93: 128-37.3. Bowe CM, Kocsis JD, Targ EF and Waxman SG (1987). Physiological effects of 4-aminopyridine on demyelinated mammalian motor and sensory fibers. Ann Neurol 22: 264-8.4. Blight AR and Gruner JA (1987). Augmentation by 4-aminopyridine of vestibulospinal free fall responses in chronic spinal-injured cats. J Neurol Sci 82: 145-59. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=28313075. Blight AR, Toombs JP, Bauer MS and Widmer WR (1991). The effects of 4-aminopyridine on neurological deficits in chronic cases of traumatic spinal cord injury in dogs: a phase I clinical trial. J Neurotrauma 8: 103-19. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=18701346. Hansebout RR, Blight AR, Fawcett S and Reddy K (1993). 4-Aminopyridine in chronic spinal cord injury: a controlled, double-blind, crossover study in eight patients. J Neurotrauma 10: 1-18. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=83207287. Hayes KC, Blight AR, Potter PJ, Allatt RD, Hsieh JT, Wolfe DL, Lam S and Hamilton JT (1993). Preclinical trial of 4-aminopyridine in patients with chronic spinal cord injury. Paraplegia 31: 216-24. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=84930368. Hayes KC, Potter PJ, Wolfe DL, Hsieh JT, Delaney GA and Blight AR (1994). 4-Aminopyridine-sensitive neurologic deficits in patients with spinal cord injury. J Neurotrauma 11: 433-46. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=78372839. Qiao J, Hayes KC, Hsieh JT, Potter PJ and Delaney GA (1997). Effects of 4-aminopyridine on motor evoked potentials in patients with spinal cord injury. J Neurotrauma 14: 135-49. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=910493110. Segal JL and Brunnemann SR (1997). 4-Aminopyridine improves pulmonary function in quadriplegic humans with longstanding spinal cord injury. Pharmacotherapy 17: 415-23. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=916554511. Potter PJ, Hayes KC, Hsieh JT, Delaney GA and Segal JL (1998). Sustained improvements in neurological function in spinal cord injured patients treated with oral 4-aminopyridine: three cases. Spinal Cord 36: 147-55. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=955401212. Shi R and Blight AR (1997). Differential effects of low and high concentrations of 4-aminopyridine on axonal conduction in normal and injured spinal cord. Neuroscience 77: 553-62. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=947241113. Shi R, Kelly TM and Blight AR (1997). Conduction block in acute and chronic spinal cord injury: different dose-response characteristics for reversal by 4-aminopyridine. Exp Neurol 148: 495-501. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=941782814. Donovan WH, Halter JA, Graves DE, Blight AR, Calvillo O, McCann MT, Sherwood AM, Castillo T, Parsons KC and Strayer JR (2000). Intravenous infusion of 4-AP in chronic spinal cord injured subjects. Spinal Cord 38: 7-15. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1076219215. Halter JA, Blight AR, Donovan WH and Calvillo O (2000). Intrathecal administration of 4-aminopyridine in chronic spinal injured patients. Spinal Cord 38: 728-32. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1117537216. Segal JL, Hayes KC, Brunnemann SR, Hsieh JT, Potter PJ, Pathak MS, Tierney DS and Mason D (2000). Absorption characteristics of sustained-release 4-aminopyridine (fampridine SR) in patients with chronic spinal cord injury. J Clin Pharmacol 40: 402-9. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1076116817. Hayes KC, Potter PJ, Hsieh JT, Katz MA, Blight AR and Cohen R (2004). Pharmacokinetics and safety of multiple oral doses of sustained-release 4-aminopyridine (Fampridine-SR) in subjects with chronic, incomplete spinal cord injury. Arch Phys Med Rehabil 85: 29-34. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1497096418. van der Bruggen MA, Huisman HB, Beckerman H, Bertelsmann FW, Polman CH and Lankhorst GJ (2001). Randomized trial of 4-aminopyridine in patients with chronic incomplete spinal cord injury. J Neurol 248: 665-71. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1156989419. Wolfe DL, Hayes KC, Hsieh JT and Potter PJ (2001). Effects of 4-aminopyridine on motor evoked potentials in patients with spinal cord injury: a double-blinded, placebo-controlled crossover trial. J Neurotrauma 18: 757-71. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1152698220. Grijalva I, Guizar-Sahagun G, Castaneda-Hernandez G, Mino D, Maldonado-Julian H, Vidal-Cantu G, Ibarra A, Serra O, Salgado-Ceballos H and Arenas-Hernandez R (2003). Efficacy and safety of 4-aminopyridine in patients with long-term spinal cord injury: a randomized, double-blind, placebo-controlled trial. Pharmacotherapy 23: 823-34. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1288509521. DeForge D, Nymark J, Lemaire E, Gardner S, Hunt M, Martel L, Curran D and Barbeau H (2004). Effect of 4-aminopyridine on gait in ambulatory spinal cord injuries: a double-blind, placebo-controlled, crossover trial. Spinal Cord 42: 674-85. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1535667622. Cardenas DD, Ditunno J, Graziani V, Jackson AB, Lammertse D, Potter P, Sipski M, Cohen R and Blight AR (2007). Phase 2 trial of sustained-release fampridine in chronic spinal cord injury. Spinal Cord 45: 158-68. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1677303723. Hayes KC, Katz MA, Devane JG, Hsieh JT, Wolfe DL, Potter PJ and Blight AR (2003). Pharmacokinetics of an immediate-release oral formulation of Fampridine (4-aminopyridine) in normal subjects and patients with spinal cord injury. J Clin Pharmacol 43: 379-85. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1272345824. Hayes KC, Potter PJ, Hansebout RR, Bugaresti JM, Hsieh JT, Nicosia S, Katz MA, Blight AR and Cohen R (2003). Pharmacokinetic studies of single and multiple oral doses of fampridine-SR (sustained-release 4-aminopyridine) in patients with chronic spinal cord injury. Clin Neuropharmacol 26: 185-92. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=12897638
Dr. Young is the Richard H. Shindell Chair in Neuroscience, Distinguished Professor of Cell Biology & Neuroscience, and Founding Director of the W. M. Keck Center for Collaborative Neuroscience at Rutgers University. He is CEO of ChinaSCINet, a non-profit company that organizes spinal cord injury (SCI) clinical trials in China. Since 2012, he serves as Global Medical Director (non-paid) for Stemcyte. He helped found Acorda Therapeutics, served on its Board of Directors for 16 years, and continues to advise the company.
The CareCure Community. In 2001, Dr. Young established the CareCure Community (http://carecure.org), a large and active SCI community web site with >100,000 members, >200,000 unique visitors/month, and >2 million page views/month.
SCI Clinical Trials. Dr. Young helped organize the first randomized SCI clinical trials in 1979-2007, i.e. NASCIS I, II, and III that established the safety and efficacy of high-dose methylprednisolone treatment of SCI. In 2004, Dr. Young established and leads the ChinaSCINet to test therapies in China, Hong Kong, and Taiwan. He also organizes trials in India, Norway, and the United States.
Multicenter Animal Spinal Cord Injury Study. In 1987, Dr. Young helped developed the Impactor rat SCI model, received an NIH multicenter grant in 1993 to validate the model. Many researchers use the model to test therapies.
Acorda Therapeutics. In 1995, Dr. Young helped found the Acorda and served on its Board of Directors for 16 years. A public company (ACOR), Acorda develops therapies for SCI, multiple sclerosis, and related conditions.
Neurotrauma Society. In 1989 and 1991, Dr. Young founded the National (USA) and International Neurotrauma Societies for scientists and clinicians studying brain and spinal cord injury. In 1984, Dr. Young founded and served as Editor-in-Chief of Central Nervous System Trauma, renamed Journal of Neurotrauma in 1990, from 1984-1991.
Especialidades: Spinal cord injury Stem cell therapies Umbilical cord blood Regenerative therapies