3rd Year Med Student Survival Guide · 3rd Year Med Student Survival Guide
42
1 3 rd Year Survival Guide Originally Compiled by
Transcript of 3rd Year Med Student Survival Guide · 3rd Year Med Student Survival Guide
1
3rd Year Survival Guide
Originally Compiled by Class of 2015 Class Officers

2
Table of Contents
You Made it!..................................................................................................................................................4
General Information......................................................................................................................................5Clinical Education Manual.........................................................................................................................................5Didactic Week...........................................................................................................................................................5Shelf Exams..............................................................................................................................................................5Budgeting.................................................................................................................................................................5Information Specific to Each Rotation Site................................................................................................................5Staying Organized.....................................................................................................................................................6
Where to Live................................................................................................................................................7Helpful Websites......................................................................................................................................................7General Advice.........................................................................................................................................................7“EAST” Rotations (Arrowhead, Riverside, etc )..........................................................................................................7“CENTRAL” Rotations (WesternU, Chino, Pomona Valley, etc)...................................................................................7“WEST” Rotations (Downey, Long Beach, LA, etc).....................................................................................................7If Your Rotations are “Spread Out All Over”..............................................................................................................7
DO’S and DONT’S...........................................................................................................................................8DO’S.........................................................................................................................................................................8DON’TS.....................................................................................................................................................................8
More Unsolicited Advice................................................................................................................................9
How to be the Best 3rd Year..........................................................................................................................10
The Essentials...............................................................................................................................................11What to Have in Your White Coat...........................................................................................................................11General Texts/Resources for Rotation.....................................................................................................................11Useful Apps............................................................................................................................................................11Terminology...........................................................................................................................................................11Essential Abbreviations...........................................................................................................................................12
Family Medicine...........................................................................................................................................13Resources for Rotation and Shelf Exam...................................................................................................................13High Yield Topics (Start Looking @ Weekend Before Starting Rotation)...................................................................13Example SOAP Notes for Outpatient medicine........................................................................................................13
Internal Medicine.........................................................................................................................................14Resources for Rotation and Shelf Exam...................................................................................................................14High Yield Topics (Start Looking @ Weekend Before Starting Rotation)...................................................................14Getting the Most Out of Your Rotation....................................................................................................................15Note Examples and Tips..........................................................................................................................................15
H&P/admission............................................................................................................................................................15Progress Note..............................................................................................................................................................15
3
Obstetrics and Gynecology...........................................................................................................................17Resources for Rotation and Studying.......................................................................................................................17High Yield Topics (Start Looking @ Weekend Before Starting Rotation)...................................................................17Getting the Most Out of Your Rotation....................................................................................................................17Tips.........................................................................................................................................................................17Sample Notes.........................................................................................................................................................17
Postpartum..................................................................................................................................................................17OB visit in clinic...........................................................................................................................................................18Other Examples...........................................................................................................................................................18
Pediatrics.....................................................................................................................................................19Resources for Rotation and Shelf Exam...................................................................................................................19High Yield Topics (Start Looking @ Weekend Before Starting Rotation)...................................................................19Getting the Most Out of Your Rotation....................................................................................................................19Miscellaneous/Tips.................................................................................................................................................19Sample Notes.........................................................................................................................................................20
Newborn note.............................................................................................................................................................20Peds note:...................................................................................................................................................................20
Psychiatry....................................................................................................................................................21Resources for Rotation and Studying.......................................................................................................................21High Yield Topics (Start Looking @ Weekend Before Starting Rotation)...................................................................21Getting the Most Out of Your Rotation....................................................................................................................21Sample Notes.........................................................................................................................................................21
OMM...........................................................................................................................................................22Resources for Rotation and Shelf Exam...................................................................................................................22High Yield Topics (Start Looking @ Weekend Before Starting Rotation)...................................................................22Getting the Most Out of Your Rotation....................................................................................................................22
Surgery........................................................................................................................................................23Resources for the Rotation and Studying................................................................................................................23High Yield Topics (Start Looking @ Weekend Before Starting Rotation)...................................................................23Getting the Most Out of Your Rotation....................................................................................................................23Scrub Etiquette.......................................................................................................................................................24Sample Notes.........................................................................................................................................................24
Advice About Level/Step 2...........................................................................................................................25
VSAS and Other 4th Year Relevant Info.........................................................................................................26Checklist.................................................................................................................................................................26
3rd Year........................................................................................................................................................................264th Year.......................................................................................................................................................................27
How to Submit an Elective Request on VSAS...........................................................................................................27Saving your Elective.....................................................................................................................................................27Applying to your Elective.............................................................................................................................................28Check on the status of your elective on VSAS.............................................................................................................28
4
You Made it!
Welcome to your third year of medical school! This year brings a whole new, memorable, rewarding, and challenging journey that is completely unlike the last two years of medical school. Hopefully, you’ve made it through the boards with all of your fingers and toes still attached and you’ve had a chance to recover and get revved up for the coming year! Many career decisions will be made and many opportunities to see and do what brought you to medical school will be presented to you over the course of this year. You will deliver a baby or two, learn how to set up a central line, and comfort a patient at the time when he or she is most alone and afraid. From bringing new life into this world to comforting a patient as they die, this year will be quite memorable.
As amazing and challenging as this journey is, it is not a guided tour. By the end of June, you will appreciate the importance of being a "self-guided learner." No one will tell you exactly what is expected of you during your rotations, what you should study to prepare for daily tasks or for your shelf exams, or what it means to do well during your rotations.
So, this guide was made with the hope that it might help orient you and make this transition a little less scary. In here you will find useful resources, expectations, daily activities, SOAP note examples, and much more. We hope that after reading this document you will feel a little better prepared as you walk into the first day of your next rotation.
Also, remember you Good luck!
Izzy [email protected]
ACKNOWLEDGEMENTS: George Washington University’s Cruising Through 3rd Year AOA Guide to the 3rd Year PCOM 3rd Year Survival Guide University of Pittsburgh School of Medicine University of North Carolina School of Medicine COSGP
5
Note: This guide was adapted from the above resources and suggestions from upperclassmen. It is NOT associated with COMP
General Information
Clinical Education Manual Found on Blackboard (BB), the Clinical Education Manual is your GO TO for anything rotations related. Consider it the syllabus for years III and IV. The rotations office will expect you to abide by the policies stated within, so make sure you read it/skim it over prior to starting rotations. Know what you’re accountable for. Also, start with this manual if you have a question – it contains everything from scheduling electives, to board requirements, time off, VSAS, etc.
Didactic Week Every 3 months you will return to campus for a week of exams covering the rotations you just completed. Schedules will vary, but generally are:
- MON: o AM = Pre-OSCE (similar to a group patient encounter)
PAY ATTENTION to their advice for your OSCEo PM = professional development lectures, Deans Town hall, etc.
- TUE: OSCE dayo 2 patient encounters back to backo Based on the rotations you are coming off
For example, if you came off Orange Block you will do an IM encounter and a Psych encountero Will be on campus for about 2 hourso You will watch the recording of your encounter immediately after and critique it
- WED: Shelf exams x 2 (unless Blue Block, then only OMM)o One in the AM, one in the PM
- THUR: Plenary sessions for upcoming rotations (schedule varies, can be few hrs - all day) - FRI: Plenary sessions for upcoming rotations (schedule varies, can be few hrs - all day)
Shelf ExamsCOMP uses the NBOME “COMAT” exams. Generally, you will take 2 shelf exams/didactic week (except for Blue Block. There is only OMM). The exams are 2.5 hours with 125 questions on the computer. See http://www.nbome.org/comat3.asp?m=can for exam breakdowns, outlines, and free PRACTICE EXAMS.
Budgeting Budget your disbursement for 3rd year to pay for Step 2 Boards (the written exam AND the PE). It’s expensive, ~$1300 for the PE and ~$600 for the written! If you plan to take USMLE Step 2 as well, keep that in mind since that will be another ~$600. See page 25 for more details.
Information Specific to Each Rotation SiteThis Google doc has been created by the class of 2015. It includes tips/tricks, general schedules, and suggestions specific for each rotation site. Please continue to reference and update the document for yourself, your classmates, and the classes beneath you: https://docs.google.com/spreadsheet/ccc?key=0Am04pPlEOo-ydGhCbmxPSWNBV1FsdnFuekQ0VExFclE&usp=sharing
https://docs.google.com/spreadsheet/ccc?key=0Am04pPlEOo-ydGhCbmxPSWNBV1FsdnFuekQ0VExFclE&usp=sharing
6
Staying Organized If you’re into organizing the notes you take on wards, this small (6” x 8”) cheap notebook work GREAT. It works like a three ring binder without the bulky rings (it uses little plastic discs instead). You can scribble whatever you want on the first page and then “re-file” it into a section later. You can buy refillable pages, tabs, dividers, etc. I divided min e up into a section for each rotation (renal, IM, cardio, etc).http://www.staples.com/M-by-Staples-Arc-Customizable-Durable-Poly-Notebook-System-Navy-6-3/product_886235
Another option is to use EverNote. It is a free web-based, computer app, or phone/tablet app. I made similar “Notebooks” in EverNote and transcribed anything learned throughout the day into EverNote. The app syncs between your computer and your phone or tablet so you can have all this information in your pocket as well. https://evernote.com/?var=c

7
Where to Live
Helpful Websites- Airbnb.com - Rotatingroom.com
General Advice- Subletting can be expensive. Use friends/family when you can, or share/swap with classmates. - Be flexible and prepare for the unexpected – sometimes rotations are cancelled/changed at the last minute - Check Blackboard - sometimes there is info on housing under the description of your rotation - Seriously consider your commute time with the stress and physical exhaustion of rotations. If your commute is
long, listen to audio lectures/board prep in the car or wait out traffic at a coffee shop while studying or make that your new gym time
“EAST” Rotations (Arrowhead, Riverside, etc ) - Claremont and Rancho Cucamonga are popular. Traffic is not bad traveling East in the AM - Suggestions: Indian Hills Villas Apartments, Del Mar Apartments in Rancho Cucamonga - Riverside: Private renter Rosalinda ([email protected]) ($400/month) 5 min from RCRMC
“CENTRAL” Rotations (WesternU, Chino, Pomona Valley, etc) - Upland, Claremont areas are popular - Suggestions: College Park, Rancho Monte Vista - If you’re living centrally but have a “West” rotation (RLA, LA), consider getting a room closer to the site. Traffic is
intense traveling West in the AM and East in the PM
“WEST” Rotations (Downey, Long Beach, LA, etc) - Consider living West of your rotations for the sake of traffic - Long beach, Culver City, Playa del Ray, Manhattan Beach, Downtown Pasadena, Westwood/Century City are
popular
If Your Rotations are “Spread Out All Over” - If ½ of your rotations are East and ½ are West, consider living centrally near school. Budget gas accordingly and
try to keep rotations within a 30-mile radius - Reach out to friends/family if you need a month-long stay somewhere
8
DO’S and DONT’S DO’S
DO buy comfortable shoes and keep your professional wardrobe comfortable. Remember sitting for 10 hours straight? You’ll now stand through 8 hour surgeries or through morning rounds after night call
DO recognize the many sources of information in the hospital. The nurses, scrub techs, technicians, cafeteria staff, and others become surprisingly important to your ability to get things done. Be nice to everyone!
DO be respectful, kind and professional with patients. Simple things like knocking before entering and introducing yourself to the patient AND all family members (as well as asking for their names and relation to the patient) go a long way. Look presentable no matter how terrible your night was. Help patients retain some dignity when they’re hospitalized.
Busy residents often perceive students as a group. Making others in your group look good, while sometimes is painful, makes you look good. Work together, divide the work evenly, be fair and flexible with the call schedule. Don't be too worried about the students who are busy brown-nosing. The general consensus is that residents have enough experience to separate sincerity from posturing
DO ask for a Mid-Rotation Evaluation (found on Blackboard). It may be awkward asking a busy resident/attending to fill out a form – if you get shot down, ask for some verbal feedback when they have a moment. Express your interest in improving – it’s a sign of tremendous maturity and few actually do it! Plus, you won’t be surprised if you thought you were getting Honors but end up with a Low Pass. Also, if your preceptor does not add comments on your official end-of-rotation evaluation with your grade, but you do have a signed mid-rotation evaluation, you can have the rotation office add those comments into your MSPE
DO download scutsheets from http://www.medfools.com/downloads.php for Medicine, Peds, and OBGYN. Or keep an index card on each patient with the trend in labs and a list of all meds.
DON’TSDON’T lie. No one ever thinks they will, but it can be tempting to say “lungs clear to auscultation bilaterally” if they were yesterday, or to say H&H is normal if you think you checked the computer and didn’t see any values in the red. It is safer to say “I’m not sure” or “I’ll check”.
DON’T make assumptions about a patient. Always be curious. You are their student doctor and have the right (the responsibility!) to ask “why” to everything. Don’t assume you know why they started drinking again or need dialysis at home. Their answers are often very different than you would expect.
DON’T forget to have fun! Despite the state of constant change, rotations are some of the best times of your whole medical education. Cherish the opportunity to learn. Make mistakes while you’re under close supervision and enjoy learning while you have minimal patient responsibilities. Enjoy yourself!
9
More Unsolicited Advice
It can be stressful dealing with a different rotation site each month. Call ahead and always ask where to report and where to park the 1st day. Ask if there’s a safe place to store your belongings; otherwise, pack as light as possible and plan on carrying everything you bring for the first day.
Instead of asking, “Do you need help?” try “How can I help?” It’s a subtle difference, but it’s easy for a busy intern or resident to brush you off with a quick “no” in response to the first question in addition to interpreting your question as an attitude of disinterest and wanting to leave. Asking the second way (open ended) makes someone think about how you can be useful and that you actually want to be useful. Trust me, it seems like semantics, but it makes a difference.
Get comfortable being uncomfortable. You won’t always know the answer while are on rounds, or what to say to a dying patient who breaks down in front of you. Learn how to stay calm, remember to be “present”, and keep your chin up when the unexpected arises. The earlier you can accept that you can’t possibly know everything, the more you’ll learn and grow. Often times attendings are asking you questions to gauge how much you know and where the attending needs to fill in the gaps. So don’t take it personally. Have a thick skin.
Recognize the tremendous amount of independent learning third year demands. There are no more PowerPoints to memorize, “test challenges”, or multiple choice answers on the wards. You will have some attendings who will provide guidance and others who will make it seem like you’re treading water alone. Take ownership of your education. This new “freedom” will feel overwhelming, but remember everyone is in the same boat. Try to actively learn 3 things every day.
You will never have enough time to do all the things you want to accomplish for each rotation. Take advantage of down time while on call, breaks between lectures, and especially any outpatient months to read, read, and read some more! Accept that you may never have more than 15 minutes in a row to do productive work (hard for those of us who need 4 hour blocks to study). You won’t be able to look up everything you didn’t understand every day. So pick 1 thing that is pertinent to your patient that you didn’t understand and really study that. Know that one topic very well.
The key to being a good physician is knowing what you don’t know. Look things up! Don’t be afraid to ask questions. Find the appropriate time to ask thoughtful questions (while a patient is crashing or the attending is deep in concentration in the OR…this is NOT the time). Asking may seem intimidating, but if you don’t understand the plan speak up. You’ll get much more out of the discussion and will avoid getting caught nodding in blank agreement if someone asks you a question. More importantly, it’s a waste of your time if you pretend to know what’s happening. You can probably get through almost every rotation nodding your head – so it’s critical you take ownership of your education and remain proactive
Know your patients! Be the expert. Know their medical history, when/why they had surgeries, their medications, labs, as well as everything that’s happened to them while they’re in the hospital. This can be challenging, as the resident is called when things change, not you. Check with the resident before you present to make sure you’re up to speed. Try to present from memory, but have your notes in hand in case you need them. Memorizing is impressive, but having to scramble for a lab value tucked away in your pocket is not.
Know your patient’s disease. If they present with rule out endocarditis, know Duke’s criteria. If they present with pneumonia and happen to have SLE, know the criteria for lupus

10
How to be the Best 3rd Year
Be on time. Be present. Be available. This seems basic and common sense, but you will be surprised. Get there early if you are chronically known as the late person in the group. If other students or residents are presenting or talking about patients, pay attention. There is something to be learned ALWAYS. A lab value or test result may slip through the cracks, but you might have heard it in a conversation. So be a team player and help the group out in those situations.
Be enthusiastic and interested. Even if you aren’t interested in the specialty there is something to be learned in every experience you have. If you aren’t interested in surgery, fine. Have a goal that month to improve on your communication skills with nurses or refining the length of your case presentation. Every rotation has something to offer you. It is your job to figure out what that is.
Become a master presenter of a history and physical. This is what will set you apart as a new 3rd year apart from the rest. Be organized and keep everything in its proper section. Some attendings are told about the RIME (Reporter, Interpreter, Manager, Educator) learning model for students on clerkships. You should move from a Reporter to an Interpreter by the end of third year. If you can become a manager (developing a solid plan) or an educator that would be awesome, but be sure to master the Reporter and Interpreter role first.
Attend all lectures (AM reports, noon conferences, tumor boards, journal clubs). Attend and stay engaged.
If a volunteer is needed, be the volunteer. If they need someone to cover a call shift, if there is a consult, a new admission, volunteer. Don’t be begrudging about offering to be the volunteer. Be earnestly interested in volunteering otherwise don’t do it. This is about being a team player not about outshining your teammates.
NEVER ask to go home or leave early. Apathy about being there is very annoying to everyone else who is there. So if you don’t want to be there keep it to yourself. If you are just sitting there with nothing to do ask you attending, resident or intern how you can help them get whatever it is they are working on done.
Offer to write notes. Not only will you get more out of the experience, but it will help the team get work done.
Spend extra time with your patients ensuring they understand what was just explained. This will go a long way with the patients and their families. It won’t go unnoticed either by the nurses, residents, and attendings. This significantly increases patient satisfaction and also helps with compliance which are aspects that hospitals are graded on now.
11
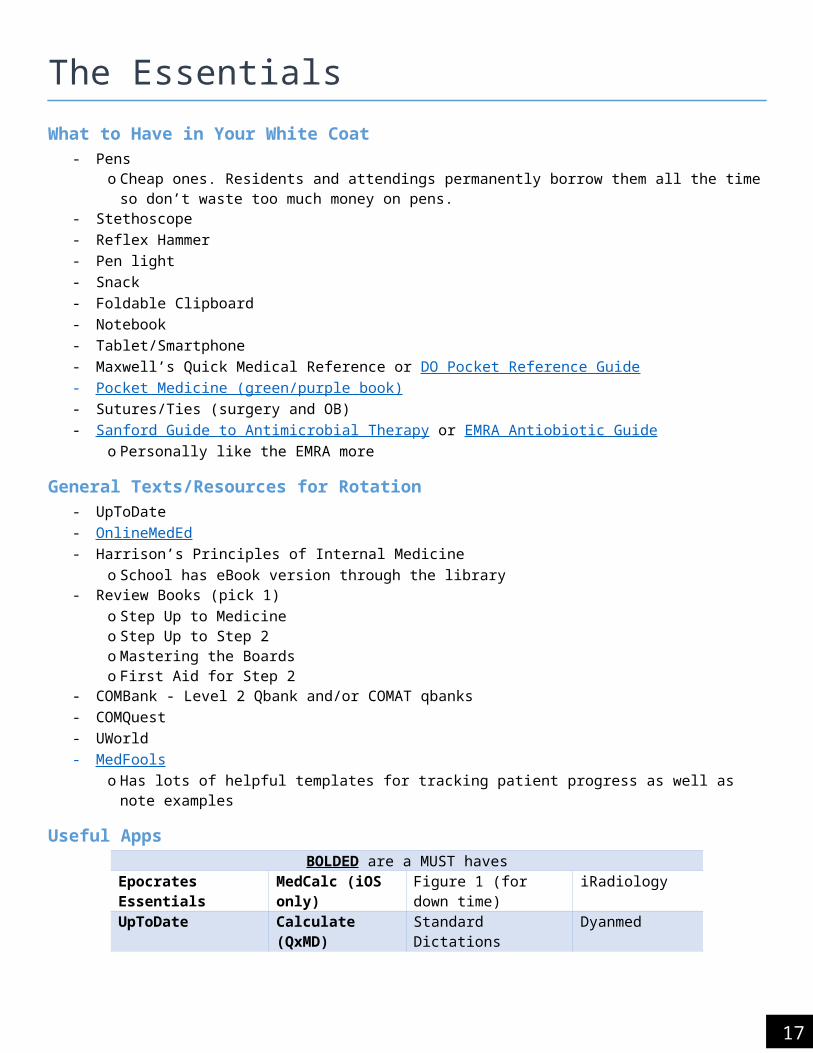
The EssentialsWhat to Have in Your White Coat
- Pens o Cheap ones. Residents and attendings permanently borrow them all the time so don’t waste too much
money on pens.- Stethoscope- Reflex Hammer- Pen light- Snack- Foldable Clipboard- Notebook- Tablet/Smartphone- Maxwell’s Quick Medical Reference or DO Pocket Reference Guide- Pocket Medicine (green/purple book) - Sutures/Ties (surgery and OB)- Sanford Guide to Antimicrobial Therapy or EMRA Antiobiotic Guide
o Personally like the EMRA more
General Texts/Resources for Rotation- UpToDate- OnlineMedEd - Harrison’s Principles of Internal Medicine
o School has eBook version through the library- Review Books (pick 1)
o Step Up to Medicineo Step Up to Step 2o Mastering the Boardso First Aid for Step 2
- COMBank - Level 2 Qbank and/or COMAT qbanks- COMQuest- UWorld- MedFools
o Has lots of helpful templates for tracking patient progress as well as note examples
Useful AppsBOLDED are a MUST haves
Epocrates Essentials MedCalc (iOS only) Figure 1 (for down time) iRadiologyUpToDate Calculate (QxMD) Standard Dictations DyanmedMedscape AHRQ ePSS Micromedex Diagnosaurus DDxOb (Pregnancy) Wheel
Terminology- AM Report - A case presentation done by a student, resident or attending @ 7AM in the trailer (except for
Friday)- “Running the List” - You sit with your team and discuss all your patients including pre-rounding info (see below)
if in the AM or events of the day including labs, tests, procedures if done at the end of the day. So know

12
everything you can about your patients before this happens. Doesn’t always happen, but be ready. Happens on surgery and IM
- Pre-rounds - Look at AM labs, AM vitals, nursing notes from overnight, and last progress note (if the pt wasn’t yours) before you meet with the team first thing. If you can see the patient before running the list, that is ideal. Make sure to read the H&P if you don’t know it. Print a patient summary if you want. Attempt developing an A/P.
- Rounds - You go from patient to patient and present to your attending and then do a PE with your attending- M&M - Morbidity and Mortality lecture is when a resident presents a case where something went wrong and
there is something to be learned from it- Grand Rounds - Occur once a week. Each service will have one during the month. It is an opportunity for each
service to teach everyone about a certain topic.
Essential Abbreviations
13
Family MedicineResources for Rotation and Shelf Exam
- UpToDate – invaluable for the latest information and treatment guidelines for most diseases This resource is especially useful for topic presentations to faculty
- Rapid Interpretation of EKGs (Dubin)- Step Up to Medicine - Ambulatory section- Case Files: Family Medicine- COMBank Family Medicine COMAT QBank
High Yield Topics (Start Looking @ Weekend Before Starting Rotation)- Review performing a full physical exam
o Look up Stanford 25- Review common medications for:
o Diabetes mellituso HTNo Hyperlipidemiao Asthmao COPDo Anxietyo Depression
- Review the following topics:o USPSTF guidelines for screening exams (e.g., colonoscopy, mammogram, DEXA, etc.)o Immunization schedule for both children and adultso Routine prenatal careo Routine well child checko Developmental milestones
Example SOAP Notes for Outpatient medicine- UNC Chapel Hill (Outpatient Medicine Templates and Examples) -
14
Internal MedicineResources for Rotation and Shelf Exam
- Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (purple/green book…purple is newer)
- UpToDate – invaluable for the latest information and treatment guidelines for most diseases. This resource is especially useful for topic presentations to faculty.
- Rapid Interpretation of EKGs (Dubin)- Onlinemeded.org - Pick one review book
o Mastering the Boardso Step Up to Medicineo First Aid for the Medicine Clerkshipo IM Essentials (condensed version of MKSAP for students by ACP)o Pretest Internal Medicine - Good question book to use if you use it with another question book like
MKSAP. Alone, the questions are too easy compared to the actual shelf exam and do not cover enough material.
o Blueprints: Medicine - Some people used this as their primary source of info. Use when pressed for time.
High Yield Topics (Start Looking @ Weekend Before Starting Rotation)- Review performing a full physical exam
o Look up Stanford 25o Review the osteopathic hospital and post-op screening exams
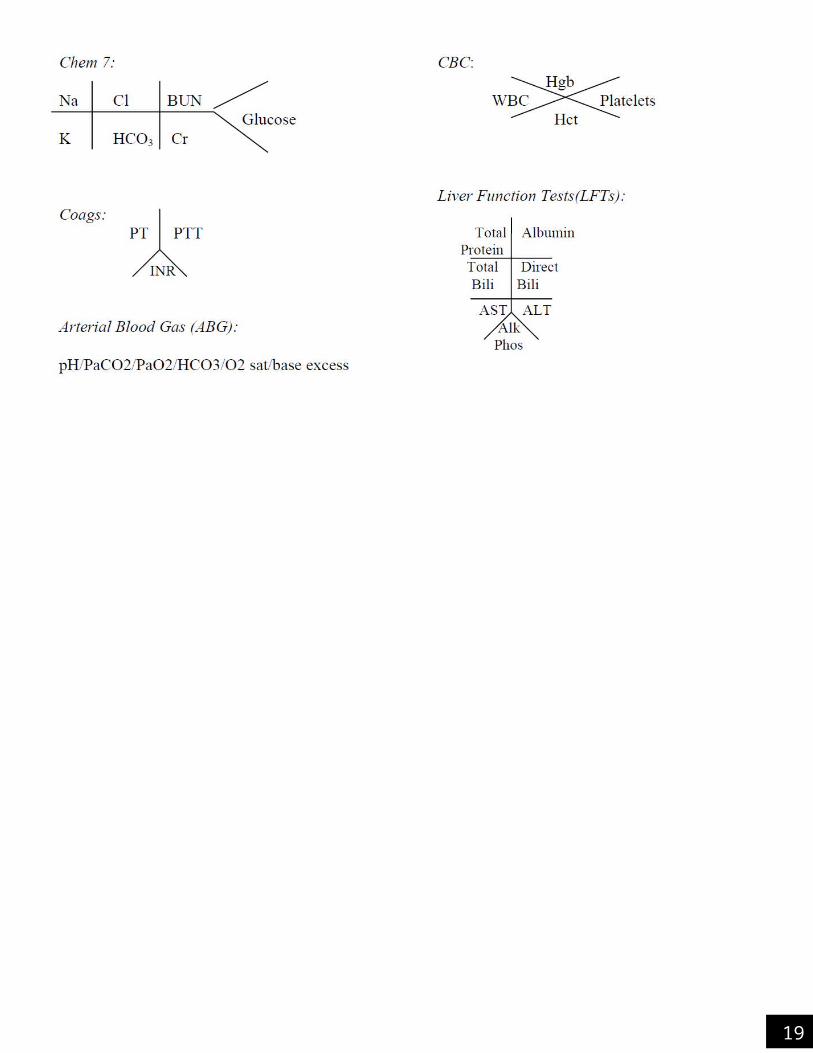
- Get used to the short hands for CBC, CMP, and LFTs (see above in Essentials)- Review common inpatient problems:
o SIRS/sepsis/severe sepsis/septic shock/SOFA criteriao How to correct electrolyte disturbances (e.g., how many mEq raise K)o Duke criteriao What a therapeutic INR iso Antibiotic prophylaxis in COPD exacerbationo CHADS2-VASC scoreo DKAo Types of pneumonia (community-acquired vs….)o CHF exacerbationo COPD exacerbationo EKG Guide o CXR Guide
- Start to familiarize yourself with what murmurs and abnormal lung sounds sound like- Have RED and black pens in your coat pocket
o Red is for your To Do list for the day (e.g., MRI results, repeat Hgb, etc)
15
Getting the Most Out of Your Rotation- Be inquisitive- Volunteer for everything- Look things up as you go- Take time with your patients. It isn’t a race
Note Examples and Tips- Tips
o Write out current meds on the left margin of your note (for your reference during your presentation)o Make sure to include what day of antibiotics they are on in your plan, if they are on antibiotics. E.g., on
day 4 of 10 of vancomycin.o Don’t forget to sign your noteo Read other notes on that patient or that day so that you get an idea of what to writeo Your note should always be the longest in relation to interns, residents, and attendings
H&P/admission- Think full H and P from ECM. The more info you get, the better- Don’t forget to ask about code status - Take your time. You’re going to feel rushed, but you have the excuse of being a student so exploit that. Toward
the end of your rotation, these should get faster. At the same time, don’t abuse the privilege of taking your time.
Progress Note- HPI: 1 liner of what brought them to the hospital and why the patient was admitted. Then follow that with their
subjective complaints and anything reported from the nurses. If pt is intubated, then put sedated and intubated for subjective complaints.
- Meds: Only new meds or changes since last time you rounded with attending- Surgery/Procedures: Only anything done since last rounds with attending (include outcome, complications)- PE: DON’T FORGET VITALS AND I/Os. Want 24hr Tmax
Make sure to ID all lines that are in the patient and comment on them appropriately in your note. An attending or resident WILL ask you about this. Be able to differentiate between a PICC or peripheral IV.
- Imaging & Labs- A/P: Justify everything. These should be really long.- Example:
o HPI: Hospital day 3. 57 yo woman with h/o MVR presented to the ED with acute RUQ abd pain and was admitted for acute cholecystitis. Patient had cholecystectomy yesterday and is in moderate pain, but is controlled with PO pain meds. Tolerating clear liquid diet. Denies N/V, fevers, chills. She is ambulating without problem. No overnight events to report.
o Meds: Ancef 1g IV (Day 2); Norco 5/325mg PO (took 4 times)o PE: BP 122/80 HR 85 RR 16 Tmax 99.8 O2Sat 99% RA
Gen: NAD. Conversant with full sentences. A&Ox4HEENT: Sclera anicteric b/l. Conjunctiva pink b/l. Oral mucosa moistNeck: No JVD presentCV: RRR. S1 and S2 appreciated. Holosystolic murmur heard best at the base. Radial pulses and dorsalis pedis pulses +2/4 b/lLungs: CTAB.Abd: Bandages clean and dry. Bowel sounds appreciated in four quadrants. Abd is soft, nondistended, and not tender to palpation.Ext: No peripheral edema b/l. LE warm to touch b/l. PIV in left forearm and dorsal side of right hand.
o WBC: 12.2; Hgb: 13.1; Hct: 40.0; Plt: 220; Tbili 2.2; Dbili 0.9o A/P:

16
1) Acute cholecystitis s/p laparoscopic cholecystectomy POD #1: Symptoms improving. WBC stable. Tbili is still elevated. Advance diet today since patient is tolerating PO. Continue PO pain meds. Plan to d/c home tomorrow as long as Tbili continues to downtrend. Surgery is following patient.2) MVR: stable and asymptomatic. Will continue home meds3) DVT prophylaxis: Continue to encourage patient to ambulate at least 4 times a day.4) Full code status
17
Obstetrics and GynecologyResources for Rotation and Studying
- Essentials of OB-GYN (Hacker and Moore) - Gold standard for the rotation- Blueprints in OB-GYN - Brief review of major topics. Good reference- UpToDate - First Aid for the Obstetrics and Gynecology Clerkship - Blueprints Q&A Step 2 Obstetrics & Gynecology – hidden gem! Can be finished in about two days- Onlinemeded.org
High Yield Topics (Start Looking @ Weekend Before Starting Rotation)- Read up on the following:
o Abnormal bleedingo Pap smear screening guidelineso Contraception (types and mechanism of action)o Fetal Heart Tracingso Routine Prenatal Screening/Labs o STIso Recommendations for mammography screeningo Gyn terminology (menarche, menopause, menorrhagia….)o Menstrual cycleo Layers of abdominal wallo Leopold maneuver (helpful for finding fetal heart tones with Doppler)
Getting the Most Out of Your Rotation- If going to the OR, read up on the surgery you are walking into. It is more meaningful and you are able to ask
more pointed questions.- Ask for sutures and practice tying 1 handed knots with your non-dominant hand, instrument ties, and 2 handed
knots if things are slow.
Tips- When presenting, don’t say 26-year-old G2P1 female… It’s implied she is a female. She’s pregnant.- Always have a chaperone when doing a pelvic, breast, or rectal exam, regardless of your gender.
Sample Notes
Postpartum- HPI should include:
o Ageo G/P status (if the G’s and P’s don’t match, make sure you know why)o Weeks gestationo Route of delivery (if c-section, what was the reason...repeat, fetal distress, etc)o Breast or bottle feedingo Vaginal bleeding (lochia): like a period, heavier, lighter, spottingo Pain: is it improving and what is it being controlled by (motrin, percocet)
1. Has she been walking?2. Is she eating and drinking without problem?
- PE should include at least:

18
o Check vitals (looking for tachycardia. sign of too much blood loss)o Palpate the fundus (should be very firm and below the umbilicus)o Check incision if had c-sectiono Palpate the legs (looking for symmetrically warm, any edema, and pulses)o Check if IV is still ino Check if repeat H/H were done after deliver (look at change)
- A/P should include what postpartum day (PPD) or post-op day (POD) it is
OB visit in clinic- HPI should include:
o Ageo G/P status (if the G’s and P’s don’t match, make sure you know why)o Weeks gestationo Any vaginal bleeding, cramping, contractions, headache, change in vaginal discharge, LE edema (if present,
does it go away)o Fetal movement (if >34 weeks, are they doing kick counts)o If GDM or DM, do they have their sugar log (look at it)o Any other complaints
- PE should include:o Measure fundus (20 weeks = level of umbilicus)o Use doppler to look for fetal heart tones (hard to do if <15 weeks. Still try. Don’t try <12 weeks. Too hard
and will freak out mom)o Inspect and palpate LE
- A/P can include things to remind you what is due at the next visit (i.e., if seeing a woman @ 34 weeks, you can write GBS and Tdap will be given at next visit)
Other Examples- http://www.stritch.luc.edu/lumen/MedEd/obgyne/tools.pdf
19
PediatricsResources for Rotation and Shelf Exam
- UpToDate- Nelson's Essentials of Pediatrics- 5 Minute Pediatric Consult- Harriet Lane Handbook- http://pediatrics.aappublications.org/ - Blueprints in Pediatrics- Case Files: Pediatrics- Onlinemeded.org
High Yield Topics (Start Looking @ Weekend Before Starting Rotation)- Immunization schedule- Developmental milestones- Anticipatory guidance- Rashes- Fever of unknown origin- Antibiotics use in peds- Hyperbilirubinemia- Community acquired pneumonia (IDSA has a free PDF)- Acute Otitis Media (AOM)- Respiratory Syncytial Virus (RSV)- Management/evaluation of first febrile UTI- GBS prophylaxis guidelines- Complications of common newborn issues
o LGAo Pretermo Hep B status unknown or positive
Getting the Most Out of Your Rotation- Be proactive, don’t be afraid to ask to do something- Use this rotation to work on your Spanish, if you have any. Any effort is appreciated.- Ask questions
Miscellaneous/Tips- Children are not little adults, so don’t treat them that way.- How to calculate fluids in pediatrics - based on the patient's weight maintenance:
o *4-2-1 rule*o 4cc/kg/hr for the first 10 kg in weight PLUSo 2cc/kg/hr for the second 10 kg in weight PLUSo 1cc/kg/hr for each additional kg in weight
- If a child is dehydrated (or is NPO, or is minimally PO) you will need to give maintenance PLUS some extra depending on their condition or the extent of dehydration - ask your resident. There is some discrepancy on which fluids to use, so check with your attending for what they prefer. In general over 20 kg maintenance fluids use D5 1/2NS and under 20 kg use D51/4NS. For resuscitation always use NS!!!o Breast milk/formula has 20 kcal/oz or 0.67kcal/cc.
20
Sample Notes
Newborn note- Mother’s age and G/P status- Gestational age- vaginal delivery or c-section when (date and time) with how long membranes were ruptured in hours- Mom’s GBS, HIV, Syphilis, Hep B, blood type and Rh status- Breast or formula feeding and how often- Meconium birth? only comment if yes- 1 and 5 min Apgars- Peed and/or pooped overnight?- any complaints from parents- PE should include the following (good overview video: https://www.youtube.com/watch?v=787D5wz1Fpk):
o gestational age assessment (Ballard Score)o general appearanceo skin (normal newborn exanthems, look up)o HEENT (caput, cephalohematoma, molding, red reflex, nares, feel/look at palate)o necko chest and breasts (fractured clavicle, maternal hormonal effect)o heart (murmur evaluation)o lungso abdomen (including umbilical cord)o genitalia (in males, check that both testes are in scrotum)o femoral pulseso hips (Ortolani and Barlow maneuvers)o neuro (activity, tone, primitive reflexes, sacral lesions)o extremities (Erb’s and Klumpke’s palsy)
- Exampleo HPI: Baby Boy Brown was born at 39+3 weeks by NSVD to a 27yo G3P2012 mom with prenatal labs O+, Ab
-, HBsAg-, VDRL non-reactive, GC/CT - , HIV -. Pregnancy was complicated by PIH, treated with Mag. ROM was 7 hours prior to delivery with clear fluid. Nuchal cord x 1 was present. Apgars were 7 and 9. Baby has been doing well since birth, breastfed x3, stool x 1 and void x 1, VSS. Mom states that feedings are going well, but she complains of sore nipples.
o PE: wt: 3578 g (-2% BW), length: 19.5in, Tmax: 98.8, HR 145, RR 48gen: well appearing, NL tone/color/activity, crying with examskin: no jaundice, + red macules with central papules scattered on chest and legsHEENT: normocephalic, + fluctuant area over R parietal bone, does not cross sutures, + RR B eyes, ears NL set/shape, palate intact, tongue WNLneck: WNL, clavicles intact Blungs: clear B, - G/F/RCV: RRR without m, femoral pulses +2 Babd: soft, non-distended, liver palpable, umbilical stump intact/clampedgenitalia: NL male with testes descended Bext: hips stable B, all WNLneuro: NL suck, grasp, Moro reflexes
Peds note: - similar to adult note with H&P- Include developmental status and birth history
21
PsychiatryResources for Rotation and Studying
- DSM 5 – not necessary as physical copy unless interested in psych. Just have an online reference- First Aid for Psychiatry - Case Files: Psychiatry- Blueprints Psychiatry- UpToDate- Onlinemeded.org
High Yield Topics (Start Looking @ Weekend Before Starting Rotation)- Mini-mental Status Exam- Familiarize yourself with the criteria for:
o Acute Stress Disorder vs. PTSDo Anorexia nervosa vs. body dysmorphic disorder vs. bulimiao Brief Psychotic disorder, Psychosis, Delusional disordero General Anxiety Disorder vs. Panic Disorder, OCDo Schizophrenia and diseases on the spectrumo Bipolar disorder and mania o Major Depressive Disordero Substance abuse/dependence
- Review drug class pharmacology for:o Typical antipsychoticso Atypical antipsychoticso SSRIso SNRIso Atypical antidepressantso Anxiolytics
Getting the Most Out of Your Rotation- Ask your attending if they prefer DSM IV or DSM 5. Don’t forget axes if you are using DSM IV.- Guys, ask if you should or should not wear a tie (for safety reasons)- Know when a patient needs restraints, both chemical and physical- Use good judgment and trust your gut. If you feel unsafe with a patient, ask for a chaperone- Spend extra time with your patients. Your attendings usually don’t have as much time as you do to talk to the
patients. Try to gather other pertinent information from your patient.
Sample Noteshttps://www.med.unc.edu/psyclerk/resources/soap-notes

22
OMMOf all the rotations, OMM might be the most variable site to site. Some rotations will be primary care/family medicine with OMT mixed in, while others might be strictly OMT. Good news - 2 years of OMM at WesternU prepares students well for this rotation.
Resources for Rotation and Shelf Exam- School OMM Manual - School Cranial Manual - OMT Review (Savarese) - COMBANK/COMQUEST Qbank
High Yield Topics (Start Looking @ Weekend Before Starting Rotation)- Review some OMM basics
o Type I vs. type 2 diagnoseso Guidelines of 3, etc.o Mechanism of action of modalities
- Review the OMM screening exams- Practice! Diagnose and treat anyone and everyone. Refresh your palpation skills
Getting the Most Out of Your Rotation- Take your time with diagnosing and treatment of somatic dysfunction.- Explain what you’re doing to your patients. Educate your patients about their treatments and provide
anticipatory guidance (you might have some residual soreness after ME, to drink plenty of water, etc.) - If you don’t know what you’re feeling, ASK your attending. This goes for cranial as well - Practice makes perfect!

23
SurgeryResources for the Rotation and Studying
- Dr. Pestana’s Surgery Notes - Either get the PDF or the physical book. Do all the questions. Gold for shelf exam.- Surgical Recall by Lorne H. BlackBourne – Some students love this, some hate it. It is a quick reference guide for
most surgeries with key points you might be questioned on- Essentials of General Surgery by Lawrence- Netter's- Atlas of General Surgery by Sabiston- COMBank COMAT Qbank
High Yield Topics (Start Looking @ Weekend Before Starting Rotation)- Review suturing videos on YouTube. Know 1 handed and 2 handed knot at least:
o https://www.youtube.com/watch?v=HTxT60u2Lj0 (1 handed)o https://www.youtube.com/watch?v=_lvQ2YJ0RjQ
- Review different suture types and their uses (vicryl, monocryl, silk, etc.) - You can also get a knot tying kit for free from Ethicon
o http://www.ethicon.com/healthcare-professionals/education/student-knot-tying-kit - Know how to scrub in. Practice scrubbing once before if you can
o https://www.youtube.com/watch?v=QvRk5ZE7iRg - Learn the names of the common surgical instruments
o http://www.surgical-instrument-pictures.com/instrument-index.html - Layers of the abdomen
Getting the Most Out of Your Rotation- Read about your cases before you go into the surgeries.- Make sure to read the H&P, at the very least, for every case you are scrubbing in on.- There may be a lot of standing around during some surgeries, but be ready to help out with the scissors,
suctioning, or holding the retractor and be alert in case they do need your help.- KNOW YOUR ANATOMY. You don’t need to know all the details of a given surgical procedure, but be familiar
with the anatomy involved in each case that you scrub on.- Be proactive and ask the intern to show you how to do basic procedures, such as starting IV's, drawing blood,
removing chest tubes, etc.- Know everything about your patients. Often patients are admitted the day of surgery, so you don’t have time to
interview them at length before the OR, but you have plenty of time to do so after their operation. Also, know their x-ray and pathology results BEFORE the intern or residents does (i.e., don’t wait for the results in the computer) and make sure to tell the intern and residents the results, otherwise, they will simply look up the results themselves and won’t realize that you had gone out of your way to obtain them.
- Have fun, learn, challenge yourself, and remember the 4 rules of surgery, “1. Eat when you can, 2. Sleep when you can, 3. Never ever mess with the pancreas." 4. No major changes after 4PM.
- There is a fine line between asking too many questions at wrong times/getting in the way/annoying the docs and being a good student with well-timed questions. This line varies site to site, surgeon to surgeon. Find this line early on (from the resident or RN) and shy just on the side of good student; if you step over the line the first few days, don’t worry. By the time you figure it out, they will only remember the good days.
- Unless your attending tells you not to, listen to everyone’s heart, lungs, and abdomen. Even if it’s an office follow up for a leg amputation. It takes 20 seconds and you look thorough.

24
Scrub Etiquette- BEFORE YOU SCRUB:
o Check to make sure the scrub nurse has your gloves and gown in the ORo If not, get your size and bring them in. Offer to open them (sterily) if the nurse is already scrubbed in o Write your name on the OR white board so the team knows who you are/can document your name in
their records - Depending on your site, a good general rule is to scrub in ahead of your attending/resident; once they arrive, the
scrub nurse will tend to him/her and their needs - you’ll be left dripping/waiting to be dressed - Scrub for just a little longer than your resident/attending, but do not hold them up - Get to know the scrub nurses’ names and KILL THEM WITH KINDNESS. They can be invaluable teammates or
make your month very difficult- Do NOT touch anything blue if you’re not sterile. Be aware of your entire body and where things are at all times- Do NOT get in anybody’s way at the OR table - MAKE FRIENDS WITH THE SCRUB NURSE - MAKE FRIENDS WITH THE SCRUB NURSE
Sample Notes- Surgery Progress Note
o HPI should include: POD #, surgery, indication, IV/PO pain meds and how they are doing addressing pain, flatus/BM since last rounds, urine output, are they tolerating PO intake if they’re eating, and any other complaints they may have. Ask about fevers, chills, SOB, CP, urinary problems, leg pain…(think possible postop fever potentials)
o PE: don’t forget vitals including Tmax and I/Os. Should include at minimum General, heart, lungs, abdomen, wound, and extremities.
o Labso Imaging since surgeryo A/P: #1 should be what you did surgery for. Include all problems you are actively managing and then if
there are other services on board and they are managing other problems, you can include those problems in your note and your plan with be per hospitalist/cardiologist/whoever
o Example:HPI: 50yo mann s/p open colostomy takedown with primary anastomosis and ventral hernia repair, POD#6. Feels well. Tolerating full liquid diet without N, V. BM x2 last night. JP drain removed yesterday. Denies abd pain, SOB, CP, leg pain.Meds: Percocet 5/325mg PO 1-2 tabs Q4 PRN (took x5 yesterday)PE: Tmax 99.4 HR 72 RR 18 BP 138/74 O2Sat 96% RAI/O 2240 / 2800Gen: sitting comfortably at edge of bedCV: RRR. No murmursAbd: mildly distended. bowel sounds present x 4 quadrants. Serous discharge on bandage. Outlines was drawn yesterday. The discharge does not extend beyond outline. No TTP. Ext: IV in right forearm. LE warm to touch b/l. no TTP b/lSkin: Blood blister present 4 inches lateral to inferior incision on the right. Two small blisters at anterior axillary line on left at inferior edge of incision.
- Other Exampleso https://med.uth.edu/graymatter/surgery-notes/ o https://smhs.gwu.edu/surgeryclerkship/resources/notes
25
Advice About Level/Step 2- Level 2 consists of 2 parts:
o COMLEX CE (Cognitive Evaluation) or USMLE CK (Clinical Knowledge). This is the multiple choice exam similar to Step 1, taken at a Prometrics Test Center
o COMLEX PE (Performance Evaluation) or USMLE CS (Clinical Skills). This is the exam in Philadelphia OR Chicago. By and large DO students do NOT take the USMLE version, even those who take multiple level USMLE exams
- Most choose to take the CE/CK towards the very end of 3rd year/beginning of 4th year – the earlier the better. You want to get the exam out of the way by the end of the first rotation of 4th year so you can focus on auditions
o Generally, rotations 2nd through 4th or 5th rotations are auditions o Schedule an easy rotation for the first month of 4th year to study, OR… o Consider taking an independent study rotation. Talk to upperclassmen in your specialty and/or your
academic advisor about this decision o Check the Clinical Education Manual for COMP’s deadlines for each exam. They insist you take and pass
all of your OSCEs and Shelf Exams before sitting for Level 2 exams.
- Schedule EARLY – mark your calendar for DECEMBER of third year to start checking available dates for the PE. Don’t wait for school to remind you about scheduling (it’ll be too late!) The exam fills up EARLY and it’s best to get it over with so you can have a complete application for residency. Although some programs may not require that you show proof of passing when you apply, it’s always better to have a complete application. August/September is prime time for the PE
o Remember it takes 1 full day to travel to Philly; see Clinical Education Manual for the amount of time you’re allowed off from rotation (usually 3 days total)
- Use your disbursement from third year to pay for the written exam AND the PE. It’s expensive! Budget accordingly. The 4th year disbursement budgets some cash for travel expenses to Philly
- Some students take a full month off to study, some take 2 weeks, and others no time at allo A general rule is that you will need to devote about ½ the amount of time you needed for Level 1o Realize that it is more mentally challenging to sit and study for 15 hours/day like you did for Level 1;
devoting a full month can be challenging for some.
QBANKS REVIEW BOOKS REVIEW COURSESCOMQuest Step Up to Step 2 KaplanCOMBank Step Up to Medicine Doctors In TrainingUSMLE World Mastering the Boards Boards Boot CampKaplan Qbank First Aid for Step 2
- Note that for Step 2 there isn’t an obvious “Gold Standard” for studying like First Aid was for Step 1. Browse a couple comprehensive review books and choose the one with the layout you like best

26
VSAS and Other 4th Year Relevant InfoMade by Maggie Pham, Class of 2015 and the COMP Office of Career and Professional Development
Checklist3rd YearJuly August
- Save the pdf of your USMLE Step I and COMLEX Level I board scoreso Scores are available to view only for a set period of time. After that window passes, you must pay a fee
(~$70) to get a copy of your scores. VSAS does not care if it is an official or unofficial copy
November- Receive email from VSAS with access code and instructions to register (use your AAMC account info the account
you used for MCATs)- Fill out and submit your VSAS application (general info, dates of core rotation completion)- Start working on your CV
November February- Meet with a member from the Office of Career and Professional Development to go over your CV- Get a professional headshot taken- Visit VSAS and browse different electives, institutions, available dates, timelines, elective requirements- Upload necessary documents depending on host institution requirements (copy of USMLE/COMLEX scores,
photo, letter of intent, copy of health insurance card, etc.)- Transcript: Order through BanWeb and send to VSAS (instructions here)- Download and complete required Immunization Forms (each institution may have its own) may need a
signature from health care provider (Can be Eileen Cotter or PCP)- Contact Employee Health Coordinator Eileen Cotter ([email protected]) to request copies of
immunizations, TB tests- Update your annual TB test (PCC pharmacy $20) get a copy for yourself- Get your flu shot get a copy for yourself
February throughout 4th year- Apply to electives (instructions below)- Register for MyERAS with AAMC ID or account using your ERAS Token (sent to your email)
March-May - Begin researching ACGME or AOA residency programs. (AMA's FREIDA Online and Osteopathic Opportunities)- Write your personal statement. Have advisor, 3 family members/friends, and the Office of Career and
Professional Development- Begin working on your Unique Characteristics with Office of Career and Professional Development- Begin submitting LOR Requests through ERAS. Make sure to follow-up with letter writers.
June - Obtain your ERAS Token from the Registrar- Register for the AOA Match at (https://natmatch.com/aoairp)- Register for Match programs (SF Match, urology, or military), if applicable- MSPE Panel Opens - Upload your MSPE UC to the MSPE Panel (https://jprod.westernu.edu/mspe/login.jsp)- Department Chairs Letter (if required), contact the proper department chair for this letter
27
4th Year July
- ERAS opens - begin entering application information- MSPE Panel Closes for staff review & corrections – end of July- AOA Match Opens – begin submitting applications
August - AOA interviews begin – keep track of every offer- Begin preparing for residency interviews - MSPE Panel Re-Opens for Final Review & Acceptance – mid-August- Schedule a mock interview with Interviewstream and with your advisor (if able)
September - MSPE Panel Closes – MSPE’s forwarded to the Registrar for ERAS- ACGME Opens – submit your applications - National Resident Matching Program® (NRMP)- Email Career Development your interview invitation tally for assessment
October-December- ERAS Opens – All MSPE’s released- Follow up on Residency Programs you haven’t heard from – December- ACGME Interview season begins – keep track and log your preferences for Rank Order List
January - AOA Rank Order List Opens – submit & certify list (first week of January)- ACGME Rank Order List Opens – submit & certify (second to third week of January)- Begin entering your Rank Order List for the NRMP match.
February - AOA Match Results- AOA Scramble- ACGME Rank Order List – closes
March - ACGME SOAP – 3rd week of March- ACGME Match Day – TBD- Attend Match Day Celebration & Reading
April-June - Sign the contract with your residency program- Graduate and prepare to begin residency. Congratulations!
How to Submit an Elective Request on VSASSaving your Elective
- Go to https://services.aamc.org/20/vsas/ and logon with your AAMC ID and password.- Click on the Electives tab.- Search by state, specialty, institution, etc. Check the box “available to DO students”.- Click on the Elective of your choosing. Select your preferred dates (or enter your own) and click save.- Click on the Electives tab again. You will see your newly saved elective in the large window.
28
Applying to your Elective- Click on the Electives tab. You will see all your saved electives in the large window.- Click the checkbox next to the elective you want to apply to.- Click on Apply to Selected Electives at the bottom.- Select the appropriate responses to the questions (“How many elective experiences would you like to be
assigned at this host institution?” “In obtaining elective experiences at this institution, which of the following is most important to you.”) Click next.
- Assign the necessary documents to the institution. To review what is required, go back to the institution’s main page.
- Review the total cost. $15 per new application to a new institution. This is a fee for using the VSAS service. If you have already paid the fee and are applying to a different elective/dates the fee should be $0. Keep in mind there may be additional fees the institution may charge you upon approval of rotation.
- Click next to review. Click Submit. Your rotation will now appear under the Pending tab. It will have the status of “Pending home institution release”.
- You MUST submit an OTRS ticket to have WesternU Release your Application to VSAS
Check on the status of your elective on VSAS- Click on the Tracking Tab.- Click on Pending Apps.- If WesternU has already released your application, the status will now read “Pending Host Institution Review”.
You should also receive an email confirmation of this update.- Check periodically. An email should be sent to you once a decision (approval or denial) has been made.- If you are approved for a rotation, login to VSAS under the Pending Apps, and click on the “accept” or “decline”
button. Keep in mind there is a deadline to accept or decline an offer.- You MUST then submit an OTRS ticket to inform the rotations department that you have been accepted for that
rotation. Make sure it is VSAS CONFIRMATION/DENIAL (see picture below)
29
For more extensive and helpful online tutorials, go to: https://www.aamc.org/students/medstudents/vsas/vsas_resources/46300/students_resources.html