
3.basal ganglia kjg
33
BASAL GANGLIA Dr. K.Jaiganesh, MD Professor of Physiology MGMCRI
-
Upload
physiology-mgmcri -
Category
Health & Medicine
-
view
363 -
download
0
Transcript of 3.basal ganglia kjg
BASAL GANGLIA
Dr. K.Jaiganesh, MD
Professor of Physiology
MGMCRI
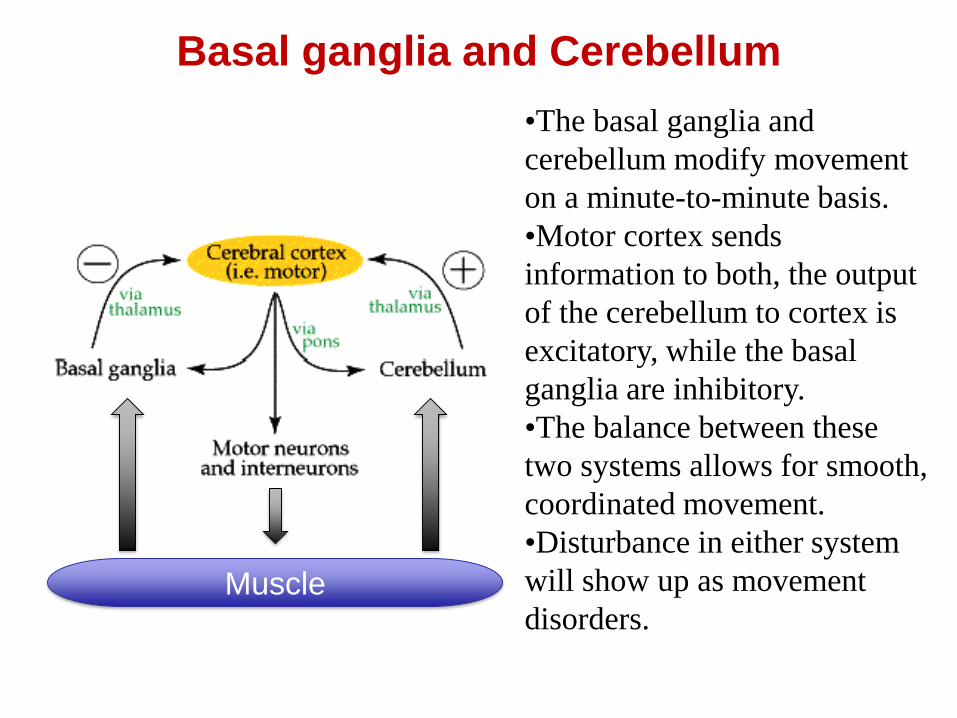
Basal ganglia and Cerebellum
•The basal ganglia and
cerebellum modify movement
on a minute-to-minute basis.
•Motor cortex sends
information to both, the output
of the cerebellum to cortex is
excitatory, while the basal
ganglia are inhibitory.
•The balance between these
two systems allows for smooth,
coordinated movement.
•Disturbance in either system
will show up as movement
disorders.Muscle
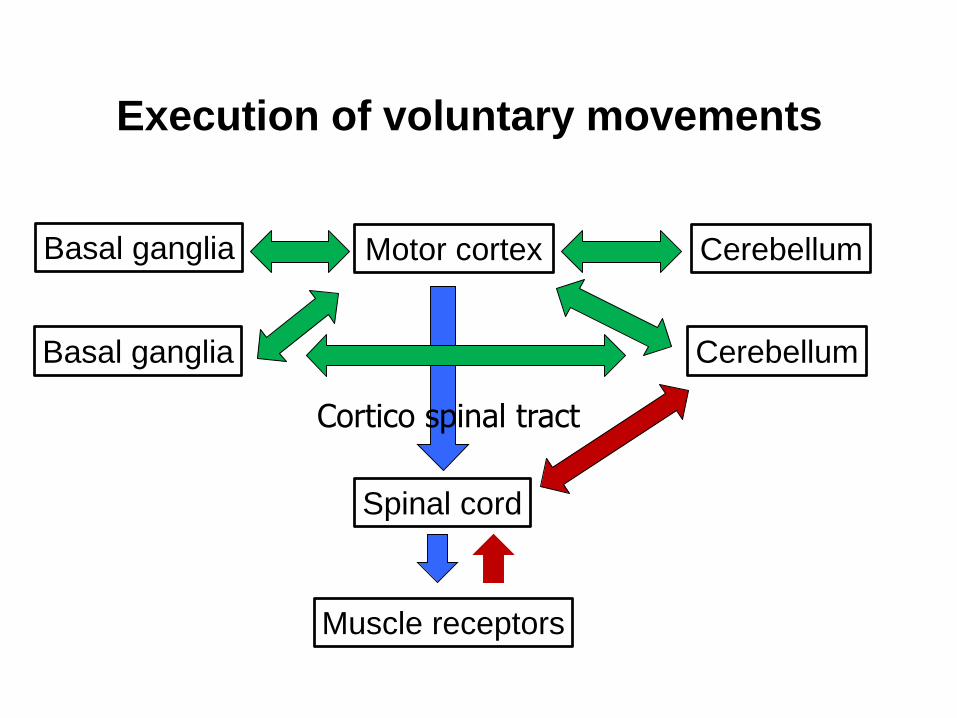
Execution of voluntary movements
Motor cortex
Spinal cord
CerebellumBasal ganglia
CerebellumBasal ganglia
Muscle receptors
Cortico spinal tract
Basal ganglia
• Objectives:
*Structure and Nuclei of Basal Ganglia
*Connections of Basal Ganglia
*Functions of Basal Ganglia
*Disorders of Basal ganglia
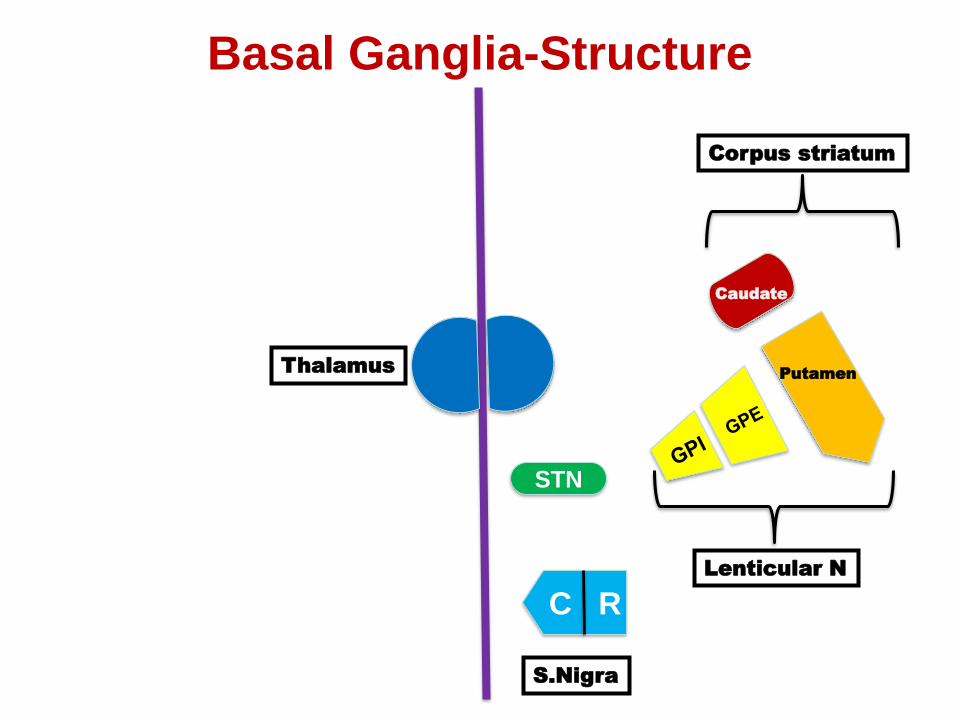
Basal Ganglia-Structure
STN
C R
ThalamusPutamen
Caudate
Corpus striatum
S.Nigra
Lenticular N
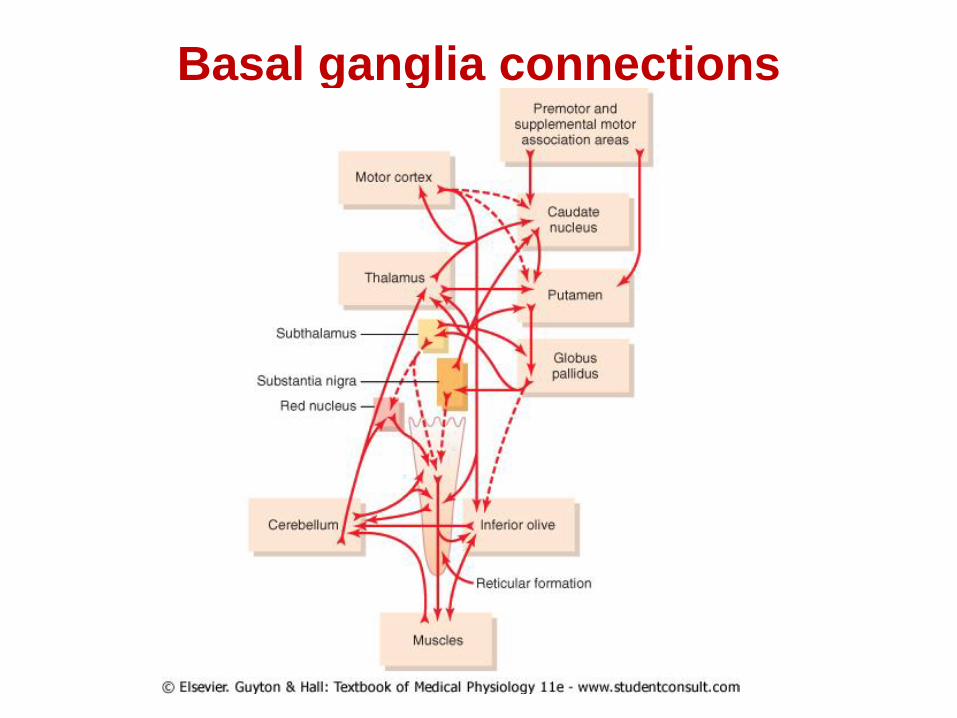
Basal ganglia connections
Connections of Basal Ganglia
• Afferent connections: terminate in (striatum)
Caudate nucleusPutamen
• Cortico striate projections from all parts of the cortex
• Projections from thalamus
• Efferent ( output from Basal Ganglia is from):
Internal segment of GLOBUS PALLIDUS
via thalamic fasciculus
Nuclei of Thalamus
Prefrontal and Premotor cortex
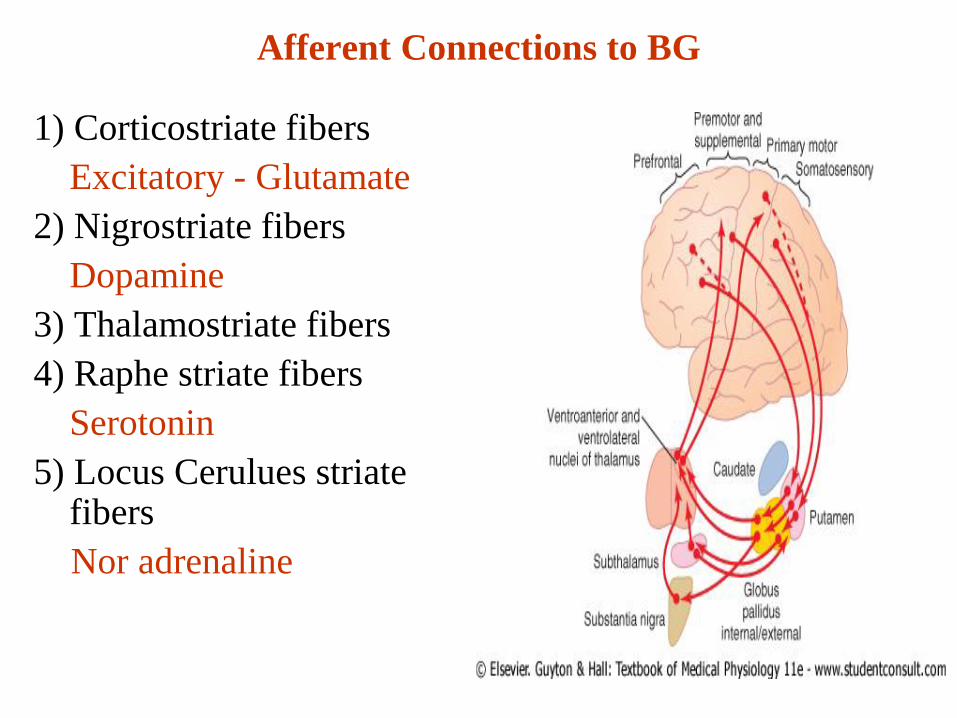
Afferent Connections to BG
1) Corticostriate fibers
Excitatory - Glutamate
2) Nigrostriate fibers
Dopamine
3) Thalamostriate fibers
4) Raphe striate fibers
Serotonin
5) Locus Cerulues striate fibers
Nor adrenaline
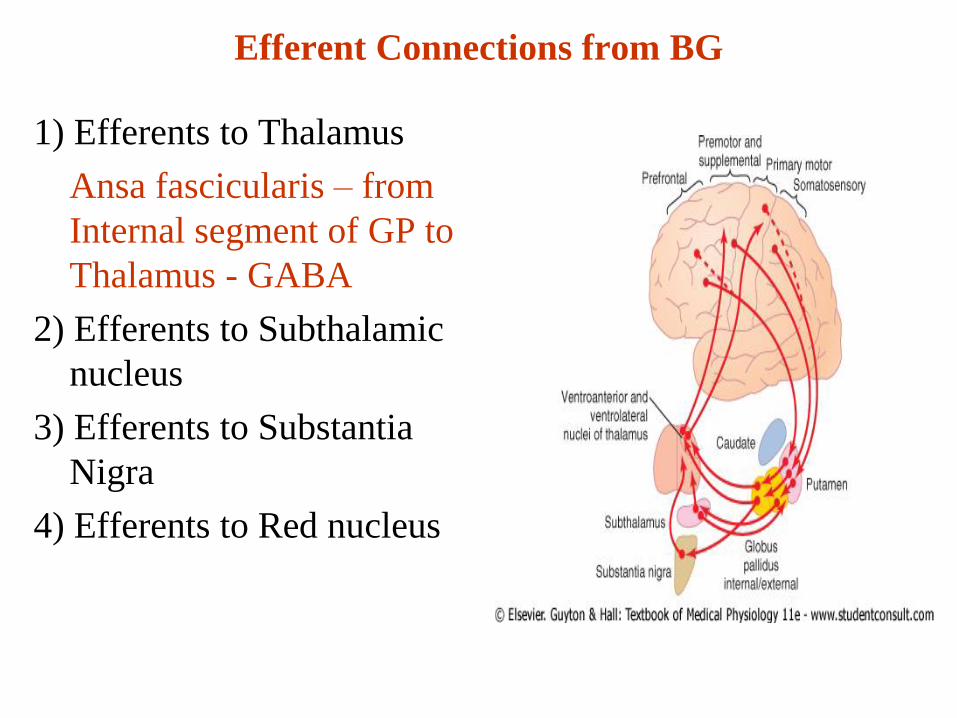
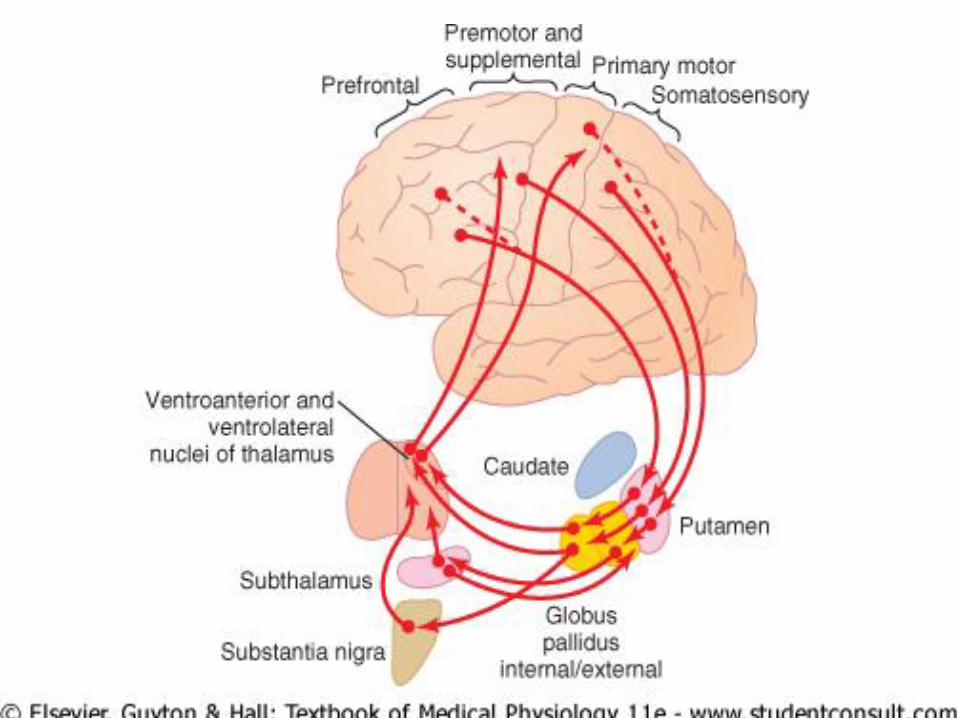
Efferent Connections from BG
1) Efferents to Thalamus
Ansa fascicularis – from
Internal segment of GP to
Thalamus - GABA
2) Efferents to Subthalamic
nucleus
3) Efferents to Substantia
Nigra
4) Efferents to Red nucleus
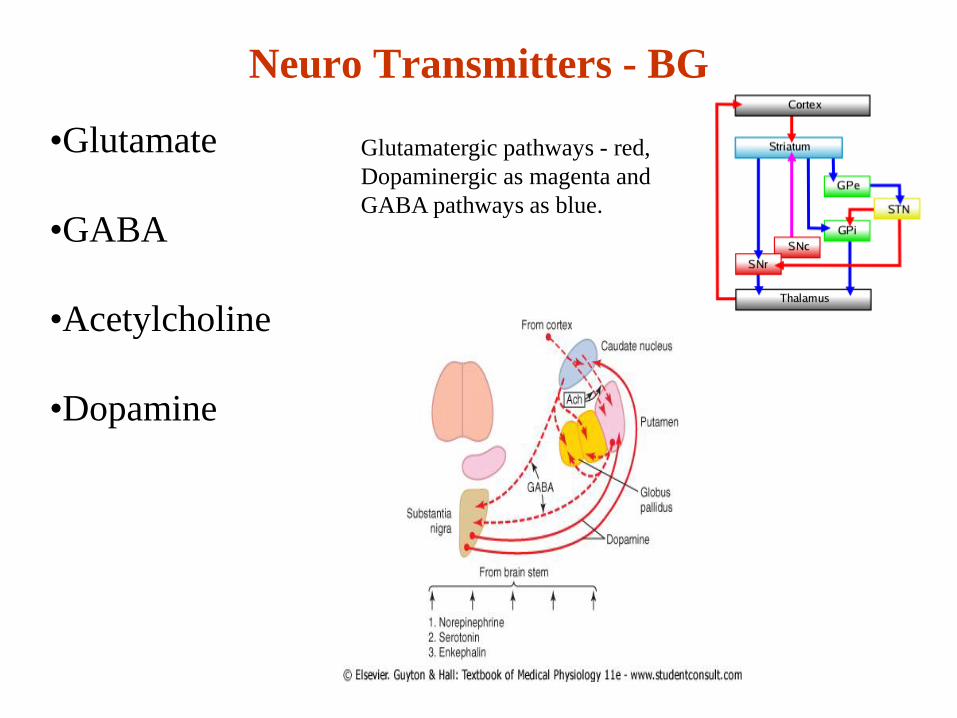
Neuro Transmitters - BG
•Glutamate
•GABA
•Acetylcholine
•Dopamine
Glutamatergic pathways - red,
Dopaminergic as magenta and
GABA pathways as blue.
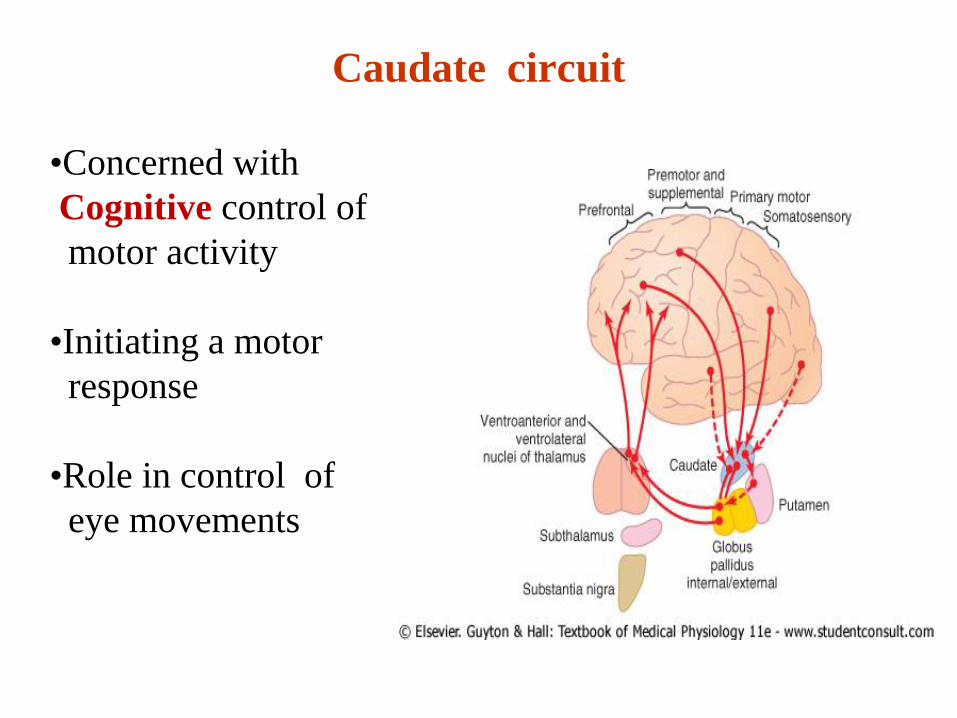
Caudate circuit
•Concerned with
Cognitive control of
motor activity
•Initiating a motor
response
•Role in control of
eye movements
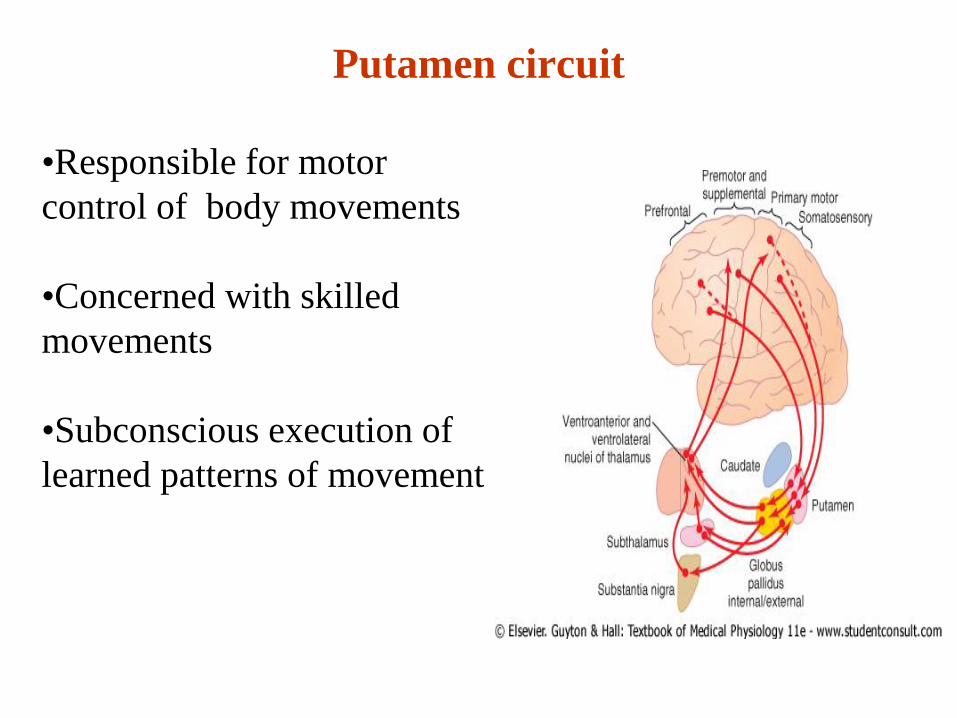
Putamen circuit
•Responsible for motor
control of body movements
•Concerned with skilled
movements
•Subconscious execution of
learned patterns of movement
Sub thalamic N of Luys – Function
• Controls posture of limbs
• Controls position & movement at shoulder & pelvic
girdles
• Effect of lesion
Hemiballismus: violent flinging movements of the
arm & leg on one side on attempting to make a
movement
Functions of basal ganglia
1. Control of voluntary motor activity
2. Control of reflex muscular activity
3. Control of muscle tone
4. Role in arousal mechanism
Functions of basal ganglia
• Control of voluntary motor activity
– Planning and Programming of movements –
Cognitive process – Caudate circuit
– Timing and scaling of movement: caudate circuit -
Lesion leads to Akinesia and Micrographia
– Production of automatic associated movements
• Swinging of arms while walking
– Subconscious execution of movements
– Prevents oscillations and after discharges in motor
system
Functions of basal ganglia
1. Control of Reflex muscular activity
– Has inhibitory effect on spinal reflexes
– Maintains posture
2. Control of muscle tone
– Through reticular formation –In BG lesion –rigidity occurs
3. Role in arousal mechanism
– Through its connections with reticular formation
4. Role in emotions and Learning
Disorders of Basal ganglia
Hypokinetic disorders (Lesion in Loop I)
Parkinsonism
Hyperkinetic disorders (Lesion in Loop II)
1. Athetosis
2. Ballismus
3. Chorea
4. Torsion spasm
Parkinsonism
• Described by James Parkinson in 1817 &
termed Paralysis agitans because of the
symptoms of weakness of muscle power
&tremor. Also known as Shaking palsy
Parkinsonism- Etiology
1. Infection - viral encephalitis
2. Degenerative - both due to aging & genetic predisposition
3. Drug induced parkinsonism
a) Phenothiazine group of drugs which Block Dopamine D2
Receptors eg.Chlorpromazine &promethazine
b) Reserpine which depletes Dopamine & prevents storage of
dopamine in nerve terminals
4. Ischemia- atherosclerotic
5. Toxin -- MPTP : 1 Methyl 4 Phenyl 1256 Tetra
hydropyridine that prevents synthesis of Dopamine
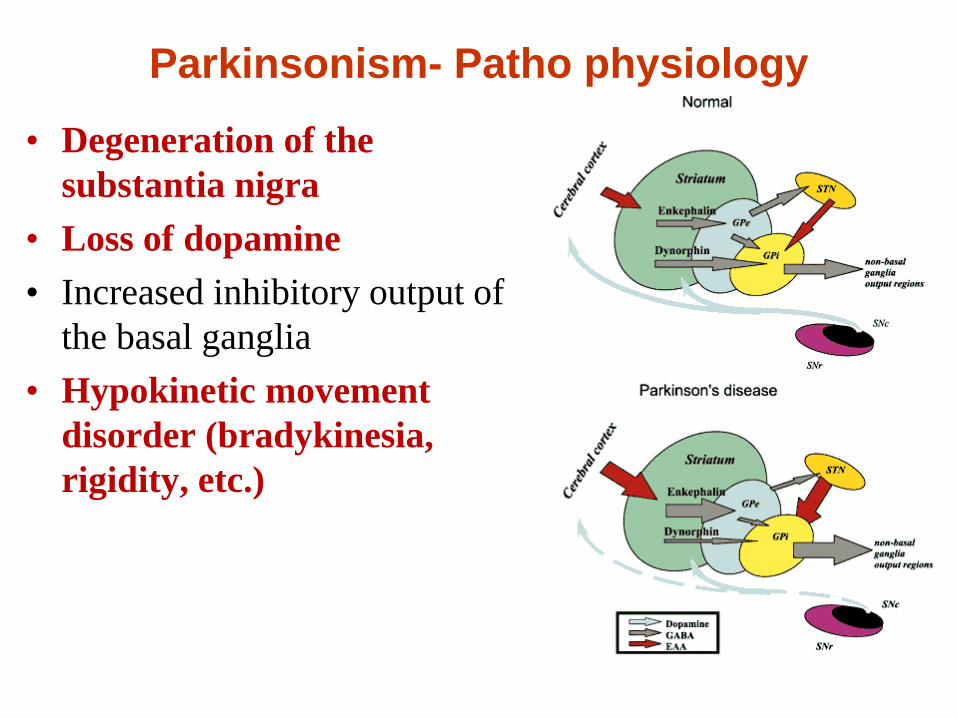
Parkinsonism- Patho physiology
• Degeneration of the
substantia nigra
• Loss of dopamine
• Increased inhibitory output of
the basal ganglia
• Hypokinetic movement
disorder (bradykinesia,
rigidity, etc.)
Parkinsonism- Patho physiology
• Decrease dopamine leads to imbalance in ratio of
cholinergic transmission & dopaminergic effect
• Nigrostriatal dopamine inhibits acetylcholine
secreting corticostriatal neurones; in absence of
dopaminergic inhibition there is increased cholinergic
transmission effects
Parkinsonism- Features
1. Rigidity
2. Akinesia
3. Tremor
4. Festinent gait
PARK - RAT- REST
Parkinsonism-Rigidity
• Rigidity may be cogwheel type of Rigidity or Plastic type or Lead pipe rigidity
1.COG WHEEL: intermittent change in tone to
passive movement of joint.
2.LEAD PIPE: Continuous resistance
Parkinsonism-Akinesia
• Poverty of movement seen as defects in fine
movement & speech
• Mask like face
• Difficulty in Initiating movement
• Micrographia: handwritten letters are small in
size & become progressively smaller
Parkinsonism-Resting Tremor
• Coarse Tremor at rest disappears during movement
• Fingers- Pill rolling movement
• Tremor disappears during movement
• Absent in sleep
• Tremor due to loss of inhibition of thalamus & relieved by lesion of VA&VL of thalamus
Parkinsonism- Festinant gait
• Festinant Gait : consists of short rapid
shuffling steps leaning forward as though to
catch centre of gravity
• Lack of associated movements such as
swinging of the arms
• Severe stage- retropulsion & propulsion ie.
Inability to stop
Parkinsonism-Treatment
1) L-DOPA because Dopamine does not cross the Blood-brain
barrier along with Carbidopa which inhibits extracerebral
DOPA decarboxylase to prevent formation of Dopamine in
circulation.
2) BROMOCRIPTINE- Dopamine Agonist
3) DEPRENYL- MAO inhibitor
4) ANTICHOLINERGICS which block action of
ACETYLCHOLINE leading to restoration of Ach/ dopamine
ratio
5) SURGERY: VA& VL OF THALAMUS -Electrocoagulation
relieves tremor.Globus pallidus externa lesions relieves
akinesia & rigidity &tremor
6) Transplantation of fetal neurons (dopaminergic)
Chorea
• Effects of Lesion of Caudate nucleus
• Involuntary semipurposive, Jerky, Dance Like movements of the Hands & Fingers
• Cause : Loss of GABAergic neurons action
• Types: – Sydenham Chorea (post Streptococcal infection sequelae)
– Senile chorea
– Huntington’s Chorea: Involuntary movement with dementia
Huntington’s disease
• Inherited as Autosomal Dominant
• Abnormal gene locus near end of short arm of
chromosome 4
• Hyperkinetic symptoms of choreiform
movements that gradually increase to
incapacitate the patient
• DEMENTIA is because of loss of Cholinergic
neurons
Athetosis
• Athetosis- Slow writhing purposeless movements of
the limbs &neck
• Lesion in Putamen
Other lesions of basal ganglia
• Hemiballismus: Due to destruction of
subthalamic nucleus. Flailing movements of
one arm and leg.
• Wilson’s Disease – Hepato Lenticular
degeneration – Copper toxicity.
• Kernicterus – Rh incompatibility.
Probable questions
• Essay
Describe the functional anatomy and connections
of Basal Ganglia . Enumerate the functions of
Basal ganglia . List the disorders of Basal ganglia.
• Short question:
Parkinsonism


















