3B New Strategies in Opioid Stewardship Conference Documents... · Naloxone administrations by...
12
1 New Strategies in Opioid Stewardship Friday, September 28 th , 2018 1:30PM – 2:20PM Christina Wiekamp, RN, MS, APRN, CNS, ACHPN Yleana Baggenstos, PharmD, BCPS, CPE JOIN SLIDO.COM WITH #5118 2 INTRO 3 Christina Wiekamp Lana Baggenstos
Transcript of 3B New Strategies in Opioid Stewardship Conference Documents... · Naloxone administrations by...

1
New Strategies in Opioid StewardshipFriday, September 28th, 2018
1:30PM – 2:20PM
Christina Wiekamp, RN, MS, APRN, CNS, ACHPN
Yleana Baggenstos, PharmD, BCPS, CPE
JOIN SLIDO.COM WITH #5118
2
INTRO
3
Christina Wiekamp Lana Baggenstos

2
CONFLICT OF INTEREST DISCLOSURE
Author’s Conflicts of interest:
• Christina, no conflict of interest
• Lana, no conflict of interest
4
LEARNING OBJECTIVES
• Explain how the opioid epidemic has impacted and burdened our healthcare system
• Express how the opioid epidemic led to the demand for pain management services
and stewardship programs
• Evaluate the importance of an opioid stewardship program
• Specify the goals of an opioid stewardship program
• List the components of an opioid stewardship program
• Build an institutional specific opioid stewardship program (OSP)
5
Audience Response Question #1
Do you feel comfortable in initiating or adjusting pain management pharmacotherapy in patients with medical and psychological comorbidities?
• A. Yes
• B. No
6

3
Audience Response Question #2
Are you expected to initiate or adjust pain management pharmacotherapy in patients with medical and psychological comorbidities at your workplace?
• A. Yes
• B. No
7
“Opioid abuse is a serious public health
issue, but PREVENTATIVE ACTIONS,
treatment for addiction, and proper
response to overdoses can help.” –U.S.
Dept of HHS
THE OPIOID EPIDEMIC
8
9

4
10
"the fifth vital sign" by the American Pain Society in 1995
2000, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) introduced new pain management standards
2002 HCAPs
• 2003 landmark study of the impact of acute pain management in the hospitalized patient over a 10 yr period1
– Improvement in pain management has not kept up with other advances inhealthcare
– Reports of “any pain” and “extreme pain” are reported as higher
• 2013 surgical pain congress report4
– Inadequate pain control was the most common reason for readmission aftersame-day surgery
– Surgical pain was the leading driver of surgery patient dissatisfaction
THE PARADOX OF PAIN MANAGEMENTPain continues to be a prevalent problem for medical and surgical patients2,3
11
1. Apfelbaum JL, Chen C, Mehta SS, et al. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be unmanaged. Anesth Analg. 2003;97:534-5402. Helfand M, Freeman M. Assessment and management of acute pain in adult medical inpatients: a systematic review. Pain Med. 2009 Oct;10(7):1183-1199.3. Kohler M, Chiu F, Gelber KM, et al. Pain Manag. 2016 Nov;6(6):591-6024. Joshi G, et al. Defining new directions for more effective management of surgical pain in the United States: Highlights of the inaugural surgical pain congress. The Amer Surg. 2014 Mar;80:219-
228.
THE DEMAND FOR PAIN MANAGEMENT SERVICES
12

5
Hospital Accreditation Standards
• “Consult a pharmacist or pain management expert (when available) when converting from one opioid to another, or
changing the route of administration (from oral to IV or
transdermal).”
• “Create and implement policies and procedures that allow for a second level review by a pain management specialist or
pharmacist of pain management plans that include high-risk
opioids, such as methadone, fentanyl, IV hydromorphone and meperidine.”
13
• Effective January 1, 2018 new and revised pain assessment and management standards will be applicable to all Joint Commission-accredited hospitals
• Opioid Stewardship is a HealthEast organization tactic for 4 out of the 6 JCstandards for pain management
Hospital Accreditation Standards
14
• “If patients do not experience improvement in pain and function at >/= 90 MME/day, or if there are escalating dosage requirements, clinicians should...consider consulting a pain specialist.”
• “For patients agreeing to taper to lower opioid doses as well as for those remaining on high opioid dosages, clinicians should...consider consulting a pain specialist.”
• Because pain management in patients with substance abuse disorder can be complex, clinicians should consider consulting …pain specialists.”
• “Experts noted that naloxone co-prescribing can be facilitated …by collaborative practices models withpharmacists.”
• “Clinicians should check the PDMP for concurrent controlled medications prescribed by other clinicians and should consider involving pharmacists and pain specialists.”
• “In patients with opioid use disorder clinicians should …consider consulting a pain specialist”
Guidelines
15

6
MAKING THE CASE
16
OSPEconomic Burden
Economic Burden
HCAHPSHCAHPS
Unmanaged Pain
Unmanaged Pain
Joint Commission
Joint Commission
Opioid Epidemic
Opioid Epidemic
CDC Guidelines
CDC Guidelines
Education Gap
Education Gap
Provider ShortageProvider Shortage
Value of Pharmacy Services
Value of Pharmacy Services
Audience Response Question #3
Do you have an opioid stewardship program at your institution?
• A. Yes
• B. No
17
• 7,500 employees
• 850 physicians
• 100+ primary care providers
• 4 hospitals
– Bethesda: 254 beds
– St. Joseph’s: 401 beds
– St. John’s: 184 beds
– Woodwinds: 86 beds
“To deliver optimal health and well-being for our patients, our communities and ourselves.”
HEALTHEAST CARE SYSTEM
St. Paul, MN
18
St John’s
St Joseph’s
Woodwinds
Bethesda

7
• Pain is common among medical patients
- 43% of medical patients experienced pain
- 12% reported unbearable pain
19
OPIOID STEWARDSHIP – EXTENDING OUR REACH
Helfand M, Freeman M. Assessment and management of acute pain in adult medical inpatients: a systematic review. Pain Med. 2009 Oct;10(7):1183-1199.
• Objective
– Evaluate pharmacist interventions and patient outcomes of a pharmacist-ledoutpatient palliative care practice
• Results (March 2011 – March 2012)
– New consults were referred by an oncologist or hematologist
– 84 new and 135 follow-up visits
– A change in pain medication dose and initiation of a new medication forconstipation and N/V were the most common interventions
– Statistically significant change in pain score was observed at the 3rd visit
Published Opioid Stewardship Programs
Outpatient Palliative Care Practice – University of California
20
Ma J, Tran V, Chan C, et al. Retrospective analysis of pharmacist interventions in an ambulatory palliative care practice. J Oncol Pharm Practice. 2015. DOI:10.1177/1078155215607089.
• Objective
– Described their experience with development of a opioid stewardship pharmacy service implemented in June 2010
• Pharmacist responsibilities- Admission medication reconciliation (PMP), review of pharmacy-generated reports (oral
long-acting opioids, fentanyl formulations, and methadone), monitor high-risk opioid therapy
(high dose IV opioids, multiple pain medications, PCAs, continuous infusions), providing pain management consultations for complex patient cases
• Results (June 2010 – June 2011)
– 2499 patients reviewed (16% of all admissions)
– 1099 (44%) required an intervention related to medication reconciliation, most commonly clarifying the most recent opioid use history (n=945, 86%)
– 154 consultations requested by physicians or pharmacists
Published Opioid Stewardship Programs
Academic Medical Center – University of Minnesota
21
Ghafoor V.Implementation of a pain medication stewardship program.AJHP.Dec 1, 2013:70;2070-75.

8
• Pharmacist responsibilities- Opioid stewardship: review of pharmacy-generated reports (patients at high-risk for
oversedation, inadequate analgesia, continuous infusions, PCAs, fentanyl patches, and methadone), and medication recommendations
- Pain Management Consultations placed by providers
- Post-discharge phone calls to patients
• Results (October 2013 – June 2014)
– 1,355 interventions (81% consultations, 19% stewardship)
– $1.6 million in estimated indirect cost avoidance ($400k from stewardship interventions)
– 59% reduction in opioid related RRT calls and Code Blues
– > 50% reduction in use of 2-4 mg IV hydromorphone dose vials
– 19% reduction in fentanyl patches
– Increase in patient satisfaction scores related to pain management
Published Opioid Stewardship Programs
Community Hospital – Kaweah Delta Medical Center, California
22
Poirier R, Brown C, Garcia, Y. Implementation of a Pharmacy Directed Pain Management Service in the Inpatient Setting. Poster presented at: ASHP Midyear Clinical Meeting; Dec 7,2014; Anaheim, CA.
• Optimize pain management pharmacotherapy
– Pharmacy generated report that identifies patients are using > 6 prn opioid doses in 24 hours
• Minimize opioid associated adverse events and cost- Pharmacy generated report that identifies patients that are receiving high-risk
opioid therapy
- Epic generated patient list that ranks hospitalized patients who have received anopioid in the last 24 hours at risk for opioid induced respiratory depression
• Quality and safety improvement- Ongoing review of naloxone events/IV opioid usage/ prescribing
patterns/documentation compliance
- Findings have warranted order set reviews, practice improvements, epic prescribing thresholds, and directed education
• Enhance patient experience
OPIOID STEWARDSHIP GOALS
23
METRICS
• % of recommendations accepted
• # interventions
• Decrease hospital induced naloxone events
• Decrease in IV opioid utilization
• Decrease # of opioids prescribed
• Improve RN documentation compliance with PCA policy
24

9
• Retrospective review/activities
– Naloxone use
– Evaluate provider prescriber patterns with goal to reduce prescribing
– Decrease IV opioid utilization, optimize use of orals when appropriate
• Prospective review/activities
– Medication profile review by decentral pharmacists• Computer generated report of pain scores > 6 in the last 16 hours for opportunity to
optimize use of PRN medications (opioid and/or opioid-sparing) for uncontrolled pain
• Determine if there is a need for a Pain Team Consult
– Pilot by clinical pharmacy pain specialists on Pain Team for daily reviewof all patients meeting select criteria to reduce risk
SUMMARY OF OPIOID STEWARDSHIP IMPROVEMENT WORK
25
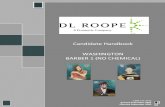
Naloxone administrations by hospital: 2017 & 2016
Naloxone administrations by patient location: 2017 & 2016
Retrospective Review: Naloxone Use
26
18
275
216
72
33
58
276
257
102
00
50
100
150
200
250
300
Bethesda St. John's St.Joseph's
Woodwinds Unknown
Nu
mb
er
of
Doses
Doses Per Hospital
2017
2016
279
42
91
135
338
7196
188
0
50
100
150
200
250
300
350
400
ED ICU OR Other PatientCare Areas
Doses in Different Patient Care Areas
• ConclusionsSimilar use in 2016 and 2017; however 3 interventions were implemented from2016 review by 2017
– Documentation for indication of naloxone use in MAR
– Opioid Stewardship Pilot Program implemented 8/1/2017
– Provider, RN, and Pharmacist education completed
• Goals for 2018
– Assess compliance rate with MAR documentation re: indication ofnaloxone use
– Assess order sets that contain both opioids and benzodiazepines and consider adjustment
– Ongoing opioid stewardship pilot
Next Steps: Naloxone Use
Naloxone Use Summary for 2017
27

10
Prospective Review: Recipe for Success
28
• DETERMINED BY THE MEDS OR PATIENTS YOU CHOOSE TO REVIEW
• SCREEN PATIENTS FOR OPIOID THERAPY PROBLEMS
OBTAIN COMPUTER GENERATED REPORTS
OBTAIN COMPUTER GENERATED REPORTS
•MED REC, DDI, ALLERGIES, PMH, PSH, HPI, I/O’S, CURRENT MEDICATION,OVERSEDATION RISK, COMORBIDITIES, AGE, PAIN SCORE
COMPREHENSIVE MEDICATION REVIEW
COMPREHENSIVE MEDICATION REVIEW
• OPIOID AND NON-OPIOID RECOMMENDATIONS, BOWEL MEDS, OR LAB MONITORING• RECOMMEND CONSULTATION (CHEMICAL DEPENDENCY, PSYCHIATRY, PSYCHOLOGY, ACUPUNCTURE, PM&R, ANESTHSIOLOGY, ORTHO, NEURO, PALLIATIVE CARE, HOSPICE)
• PATIENT COUNSELING
COMMUNICATE RECOMMENDATIONS
COMMUNICATE RECOMMENDATIONS
•OFFER TO WRITE THE ORDERS IF APPROVEDMODIFY ORDERSMODIFY ORDERS
•PROGRESS NOTE
•COMPUTERIZED INTERVENTION TRACKING SYSTEM OR EXCEL DATABASE (HIPAA COMPLIANT)
DOCUMENT INTERVENTIONS
DOCUMENT INTERVENTIONS
•UNTIL DISCHARGE PLAN ESTABLISHED OR AS DETERMINED BY TEAMMONITORMONITOR
•ASSESS SAFETY EVENTS, PRESRIBING PATTERNS, SATISFACTION, AND COSTREPORT OUTCOMESREPORT OUTCOMES
1. http://www.ajhp.org/content/ajhp/70/23/2070.full.pdf
2. The Joint Commission. Safe Use of Opioids in Hospitals. Sentinel Event Alert. 2012;49.
• “When I completed the specific opioids report for OS on 5/11, I noticed he was on same long acting and high dose short acting opioids at home, even though he came in with respiratory failure. I left sticky note to decrease long acting and short acting, but pt was discharged the next am. He came right back in for severe SOB, and the same provider who discharged him consulted our team the day after. The pain team did end up decreasing the opioids and patient improved.
• The win here is that the Hospitalist may order a consult more readily when they see our opioid stewardship notes for more complex cases,and maybe realize this patient would have been better served with a consult from the beginning of his first hospital visit. The hospitalized ordered a consult when he came back in, and another new consult from the day after, for a chronic opioid tolerant patient.”
Case Studies
29
• ML 78 yo female, admitted 01/12/18 for community-acquired pneumonia with symptoms of dyspnea on O2 as well as AKI
• PMH includes chronic back pain, DM2, GERD, HTN and pancreatitis.
• Med Rec recorded pt taking morphine sulfate controlled-release (MS Contin)15 mgtid, and MS Contin 60 mg bid. RPh noted that the pt ran out of her morphine day prior to admission and that her last refill was 3 months ago for a 30 day supply.
• Both medications were ordered however provider ended up d/c’ing MSER 15 mgTID and continued MSER 60 mg BID with oxy IR 5-10 mg q4h prn d/t AKI
• Pt unable to wean off O2, drowsy
• Days later pt seen giving MSER to husband
• O/S pharmacist reviews case and left recommendations to resident that patient has not filled this in 3 months and diversion witnessed
• Opioids d/c’d and APAP scheduled, patient able to wean off O2
Case Studies
30

11
Strengths of an OSP
� Simplicity and adaptability� Use of existing infrastructure (i.e. decentralized pharmacists)
� Impact on quality patient care� Individualized treatment of patients
� Medication safety� Closer review of patients deemed high risk for respiratory depression or receiving high-risk
opioid therapy
� Enhanced patient satisfaction
� Indirect cost avoidance data supporting pharmacist interventions
Challenges and barriers
� Not all patients in pain or experiencing adverse events are on high risk opioid therapy or deemed high risk for respiratory
depression
� Pain services are usually only available during business
hours leaving evening and overnight requests to be
addressed the following day
� Indirect cost savings makes it difficult to proactively budget
for additional positions to manage increased referrals and requests for policy revision and education
� Estimating the time required for services
Challenges and barriers
� Identification of patients at risk for poorly managed pain and timely communication with anticipated members of team
� Early patient education reviewing goals and setting expectations
� Timely follow-up with PCP or pain management provider

12
Summary
• Over-reliance on opioid-based therapies has led to significant adverse events and nationwide epidemic of opioidmisuse and diversion
• Societal and economic costs of pain are substantial
• Opioid stewardship programs can help direct and monitor analgesic pharmacotherapy
• Opioid stewardship and pain management programs have demonstrated the ability to improve opioid prescribing, avoidcosts associated with opioid adverse effects, improve pain control and increase patient satisfaction
• Stewardship programs help ensure the safe use of opioids and improve patient care through proactively mitigatingopioid associated adverse events
• Patient experience, MD/RN satisfaction, education, intervention documentation, and cost-avoidance tracking are important to the sustainability of opioid stewardship programs
Questions ?