37_Minimally Invasive Preparation and Design
11
Minimally Invasive Preparation and Design of a Cantilevered, All-Ceramic, Resin-Bonded, Fixed Partial Denture in the Esthetic Zone: A Case Report and Descriptive Review CHRISTOPHER A. BARWACZ, DDS*, MARCELA HERNANDEZ, DDS, MS † , R. HENRY HUSEMANN, MDT, CDT, TE ‡ ABSTRACT Resin-bonded, fixed partial dentures have the potential to offer a minimally invasive, fixed-prosthetic approach to tooth replacement in patients who may not be candidates for implant therapy. However, traditional preparation protocols often recommend extensive preparation designs on two abutment teeth, thereby potentially compromising the long-term health of the adjacent abutments and often resulting in unilateral debonding of one of the retainers in the long term. In light of advances in high-strength ceramic systems capable of being reliably bonded to tooth structure and offering improved esthetic outcomes, as well as clinical and case-series research demonstrating improved survivability of cantilevered resin-bonded fixed partial dentures, new preparation designs and methodologies can be advocated. The following case report demonstrates the clinical application of sonoabrasion, coupled with a dental operating microscope, to minimally prepare a single abutment for a cantilevered, all-ceramic resin-bonded fixed partial denture. Relevant historic and contemporary literature regarding double versus single-retainer resin-bonded fixed partial dentures are reviewed, as well as clinical conditions that are most favorable for such restorations to have an optimal long-term prognosis. CLINICAL SIGNIFICANCE If appropriate clinical conditions exist, a cantilevered, all-ceramic, resin-bonded, fixed partial denture may be the most conservative means of tooth replacement in a patient who is not a candidate for an endosseous implant. (J Esthet Restor Dent 26:314–323, 2014) INTRODUCTION Implant therapy has the potential to offer patients a predictable, minimally invasive, fixed, and potentially esthetic replacement solution to partial edentulism. However, there are many patients for whom a single-tooth implant may not be the first or optimal choice for tooth replacement yet still seek a fixed replacement strategy. These patients include those who have compromised immune status or other uncontrolled systemic diseases that would negatively impact surgical healing, are pregnant, have incomplete skeletal growth, have insufficient apical root spacing to enable placement of an implant, are heavy tobacco users, or have financial limitations. Patients who fulfill specific clinical criteria can potentially benefit from contemporary minimally invasive adhesive approaches that enable a fixed prosthetic replacement via the use of *Assistant Professor, Craniofacial Clinical Research Center, The University of Iowa College of Dentistry, Iowa City, Iowa † Clinical Associate Professor, Department of Family Dentistry, The University of Iowa College of Dentistry, Iowa City, Iowa ‡ Instructional Resource Associate, Department of Prosthodontics, The University of Iowa College of Dentistry, Iowa City, Iowa CLINICAL ARTICLE DOI 10.1111/jerd.12086 © 2013 Wiley Periodicals, Inc. Vol 26 • No 5 • 314–323 • 2014 Journal of Esthetic and Restorative Dentistry 314
-
Upload
pablo-benitez -
Category
Documents
-
view
225 -
download
1
description
minamente invasivo prepaacion
Transcript of 37_Minimally Invasive Preparation and Design

Minimally Invasive Preparation and Design of aCantilevered, All-Ceramic, Resin-Bonded, Fixed PartialDenture in the Esthetic Zone: A Case Report andDescriptive ReviewCHRISTOPHER A. BARWACZ, DDS*, MARCELA HERNANDEZ, DDS, MS†, R. HENRY HUSEMANN, MDT, CDT, TE‡
ABSTRACT
Resin-bonded, fixed partial dentures have the potential to offer a minimally invasive, fixed-prosthetic approach to toothreplacement in patients who may not be candidates for implant therapy. However, traditional preparation protocolsoften recommend extensive preparation designs on two abutment teeth, thereby potentially compromising thelong-term health of the adjacent abutments and often resulting in unilateral debonding of one of the retainers in thelong term. In light of advances in high-strength ceramic systems capable of being reliably bonded to tooth structureand offering improved esthetic outcomes, as well as clinical and case-series research demonstrating improvedsurvivability of cantilevered resin-bonded fixed partial dentures, new preparation designs and methodologies can beadvocated.The following case report demonstrates the clinical application of sonoabrasion, coupled with a dentaloperating microscope, to minimally prepare a single abutment for a cantilevered, all-ceramic resin-bonded fixed partialdenture. Relevant historic and contemporary literature regarding double versus single-retainer resin-bonded fixedpartial dentures are reviewed, as well as clinical conditions that are most favorable for such restorations to have anoptimal long-term prognosis.
CLINICAL SIGNIFICANCE
If appropriate clinical conditions exist, a cantilevered, all-ceramic, resin-bonded, fixed partial denture may be the mostconservative means of tooth replacement in a patient who is not a candidate for an endosseous implant.(J Esthet Restor Dent 26:314–323, 2014)
INTRODUCTION
Implant therapy has the potential to offer patients apredictable, minimally invasive, fixed, and potentiallyesthetic replacement solution to partial edentulism.However, there are many patients for whom asingle-tooth implant may not be the first or optimalchoice for tooth replacement yet still seek a fixedreplacement strategy. These patients include those who
have compromised immune status or otheruncontrolled systemic diseases that would negativelyimpact surgical healing, are pregnant, have incompleteskeletal growth, have insufficient apical root spacing toenable placement of an implant, are heavy tobaccousers, or have financial limitations. Patients who fulfillspecific clinical criteria can potentially benefit fromcontemporary minimally invasive adhesive approachesthat enable a fixed prosthetic replacement via the use of
*Assistant Professor, Craniofacial Clinical Research Center, The University of Iowa College of Dentistry, Iowa City, Iowa†Clinical Associate Professor, Department of Family Dentistry, The University of Iowa College of Dentistry, Iowa City, Iowa‡Instructional Resource Associate, Department of Prosthodontics, The University of Iowa College of Dentistry, Iowa City, Iowa
CLINICAL ARTICLE
DOI 10.1111/jerd.12086 © 2013 Wiley Periodicals, Inc.Vol 26 • No 5 • 314–323 • 2014 Journal of Esthetic and Restorative Dentistry314

a cantilevered, all-ceramic, resin-bonded, fixed partialdenture (RBFPD).
RBFPDs were first proposed in the early 1970s1 and, inthe intervening 40 years, have continued to evolve theirdesign and luting protocols based on advancements inprosthetic materials and adhesive systems. Howe andDenehy’s2 initial designs of such prostheses advocatedfor the incorporation of perforated metallic retainers tooptimize retention of the adhesive luting agent.Livaditis and Thompson3 subsequently developed amethod for etching nonperforated, nonprecious metalalloy retainers that improved the longevity of theresin-metal retainer bond by protecting the resininterface from abrasion or leakage. To preventpremature failure or unilateral debonding, designs forRBFPDs often promoted mechanical resistance withdesign elements such as rest seats,4 channels and/orslots,5 struts,6 and grooves.7 Such preparation strategies,however, sacrificed additional tooth structure and oftenmoved the preparation into dentin, making such arestoration significantly more invasive andpotentially prone to developing caries if a retainerdebonded.
Since the early to mid 1990s, all-ceramic RBFPDs weresubsequently optimized for the anterior esthetic region,facilitating predictable bonding to tooth structure andenhanced esthetics by eliminating the requirement formetallic retainers that lowered the value of theabutment teeth that supported them.8,9 Initialall-ceramic, two-retainer RBFPDs demonstrated a highincidence of unilateral framework failure because offracture, which left the pontic bonded to a singleretainer in a cantilevered fashion, often for a significantamount of time.10 Rarely were there instances of failureat the ceramic-resin-enamel bond, consistent with invitro studies that demonstrated that resin bondstrengths of such all-ceramic RBFPDs exceededthe fracture strength of the all-ceramicRBFPDs.9,11,12
Concurrent with investigations into all-ceramicRBFPDs, multiple investigators documented theprolonged survival of two-retainer RBFPDs that hadbecome unilaterally debonded and essentially
transformed into cantilevered RBFPDs. Theseinvestigators thus proposed a cantilevered design as ade facto approach in minimizing shear and torquestresses placed on RBFPD frameworks that wasattributed to differential movement of the abutmentsduring function, ascribable to their respectiveperiodontal ligaments.13–18
Subsequent clinical trials and case-series studies haveindependently demonstrated the potential for highsuccess rates not only for metal-ceramic cantileveredRBFPDs16,17,19–23 but additionally for cantileveredall-ceramic RBFPDs of various high-strength ceramicsystems.24–27 Unfortunately, long-term, randomized,prospective, clinical trial data directly comparing theclinical survival and complications associated withmetal-ceramic RBFPDs, as compared with all-ceramicRBFPDs of either design, are absent in the literature.Such data would be valuable to clinicians to offerevidence-based criteria on which to base clinicaltreatment. With regard to all-ceramic RBFPDs, Kernevaluated the long-term survival of both two-retainerand cantilevered anterior RBPFDs, and reported a5-year survival rate of 73.9% in the two-retainer groupand 92.3% in the single-retainer group.26 If unilateralfracture of the two-retainer group was accepted as acriterion for failure, the 5-year survival decreased to67.3%. Emerging data are therefore promising withregard to the potential for cantilevered, all-ceramicRBPFDs to serve as a minimally invasive treatmentmodality for patients who are not candidates for,capable of, or interested in having a single-toothimplant restoration. Often, a treatment strategyincluding cantilevering an all-ceramic RBFPD isoverlooked by clinicians because of lack offamiliarity or comfort with such a treatmentapproach.
The following case report documents the use ofminimally invasive diamond oscillating instrumentation,with the aid of a dental operating microscope, toprepare and restore a congenitally missing maxillarylateral incisor using a cantilevered, all-ceramic RBFPDfabricated from lithium disilicate (IPS e.max Press,Ivoclar Vivadent, Amherst, NY, USA) in a patient whowas not a candidate for implant therapy.
RESIN-BONDED FIXED PARTIAL DENTURE Barwacz et al.
© 2013 Wiley Periodicals, Inc. DOI 10.1111/jerd.12086 Journal of Esthetic and Restorative Dentistry Vol 26 • No 5 • 314–323 • 2014 315

Case Report
A 17-year-old healthy male was referred to the authors’intramural practice at The University of Iowa, Collegeof Dentistry for evaluation and replacement of themaxillary left lateral incisor (#10), which wascongenitally missing (Figure 1). The patient had recentlycompleted comprehensive orthodontics that includedspace preparation of #10 for an eventual single-toothimplant (Figure 2). However, the patient had yet tocomplete skeletal growth and was nearing departure forpost-secondary education, therefore precluding implanttherapy. The patient expressed desire for a fixedrestoration for the time period leading up to asingle-tooth implant; therefore, the establishedtreatment plan called for an RBFPD as a long-termprovisional restoration. Such a strategy enabled thepatient to complete skeletal growth and to decide uponan optimal time to pursue implant therapy based on thepatient’s biological, personal, and financialcircumstances. Additionally, the prosthesis providedlong-term orthodontic stability of the adjacentabutments that was critical to future implant therapysuccess. The patient was informed of the alveolar boneand soft-tissue deficiency at site #10 and was offered asubepithelial connective-tissue graft prior to restorationfabrication to aid in esthetic integration of the RBFPD.
FIGURE 2. Periapical radiograph at conclusion ofcomprehensive orthodontic treatment to provide space for afuture endosseous implant after completion of skeletal growth.
A B
FIGURE 1. A, Frontal view of initial clinical presentation demonstrating asymmetry of the maxillary central incisors and thecongenitally missing maxillary left lateral incisor. B, Lateral view of initial clinical presentation demonstrating inadequate residualridge volume and soft-tissue texture apical to site #10.
RESIN-BONDED FIXED PARTIAL DENTURE Barwacz et al.
DOI 10.1111/jerd.12086 © 2013 Wiley Periodicals, Inc.Vol 26 • No 5 • 314–323 • 2014 Journal of Esthetic and Restorative Dentistry316

The patient declined this option and preferred todefer this treatment until implant therapy couldcommence.
Clinical evaluation of the patient’s maxillary anteriorsegment revealed asymmetry of the central incisorsalignment and length, with #9 presenting 0.7 mmshorter in length and 0.5 mm lingual displacementcompared with #8. The patient requested that thecentral incisors display symmetry of length andprominence, and an additive direct compositerestoration for #9 was included in the treatment plan.The teeth adjacent to site #10 revealed intact,noncarious, virgin teeth (Figure 3A). Additionally,occlusal analysis revealed a slight anterior open bite,and an end–end canine relationship on the patient’s leftside (Figure 3B). The occlusal scheme, combined with adesire by the patient for a minimally invasive yetdurable fixed restoration, resulted in a scenario optimalfor a cantilevered RBFPD. The patient was informedthat minimal preparation would be necessary and thatupon eventual commencement of implant therapy,the connector could be sectioned, and theremaining porcelain wing left bonded to thecingulum of #11.
The preparation of abutment #11 was facilitated by useof a dental operating microscope (OPMI pico, CarlZeiss Meditec AG, Jena, Germany) and an oscillating
handpiece (KaVo SONICflex LUX 2003/L, KaVoDental, Charlotte, NC, USA) with a hemisphericalmicrotip (microtip no. 33, KaVo SONICflex) and amodified-shoulder sonic tip (SF847KR.000.016, KometUSA, Rock Hill, SC, USA) (Figure 4) under rubber damisolation. Simultaneously, a direct composite restorationinvolving the facial and incisal surfaces of #9 wascarried out using shades B1B (Filtek Supreme Ultra, 3MESPE, St. Paul, MN, USA), BL2 and MW (EsteliteOmega, Tokoyama Dental America, Encitas, CA, USA)using a layering technique. The final preparation
FIGURE 4. Diamond oscillating tips (left: hemisphericalmicro-tip no. 33, KaVo Dental; right: modified-shoulder sonictip SF847KR.000.016, Komet) used for micropreparation ofabutment tooth #11.
A B
FIGURE 3. A, Preoperative palatal view of maxillary anterior dentition. B,View of centric occlusion (note the minimaloverbite/overjet, allowing for minimal forces to be placed on the retainer wing, connector, and cantilevered pontic of the all-ceramicresin-bonded, fixed partial denture).
RESIN-BONDED FIXED PARTIAL DENTURE Barwacz et al.
© 2013 Wiley Periodicals, Inc. DOI 10.1111/jerd.12086 Journal of Esthetic and Restorative Dentistry Vol 26 • No 5 • 314–323 • 2014 317

dimensions on the retainer #11 were 5.2 mm in width,6.0 mm in height, and 0.5 mm in depth, and werelimited to enamel throughout the preparationdimensions (Figure 5).
A mounted master cast of the clinical situation wasprovided to the ceramist (Figure 6A), and acantilevered, all-ceramic (IPS e.max Press, IvoclarVivadent) RBFPD was fabricated using a BL3 ingot
A B
FIGURE 5. A, Palatal view of maxillary anterior dentition after preparation completion. B, Direct view of abutment preparation,the dimensions of the preparation were 6.0 mm (height) × 5.2 mm (width) × 0.5 mm (depth) and were limited to enamel throughout.
A
C
B
FIGURE 6. A, Master cast provided to ceramist. B, Completed cantilevered, all-ceramic resin-bonded, fixed partial denture(RBFPD) (IPS e.max press). C, Cantilevered, all-ceramic RBFPD seated on master cast.
RESIN-BONDED FIXED PARTIAL DENTURE Barwacz et al.
DOI 10.1111/jerd.12086 © 2013 Wiley Periodicals, Inc.Vol 26 • No 5 • 314–323 • 2014 Journal of Esthetic and Restorative Dentistry318
(Figure 6B). Upon cutback, Opal Effect 3 powder wasapplied from the incisofacial third to the cervical thirdof the pontic, and T blue and T clear were layered inthe incisal third to adequately mimic incisal effects. Therestoration was glazed and subsequently mechanicallyglazed with rubber wheels and polishing compound tomatch the luster of the adjacent teeth. The adaptationand fit of the restoration were verified on the mastercast (Figure 6C).
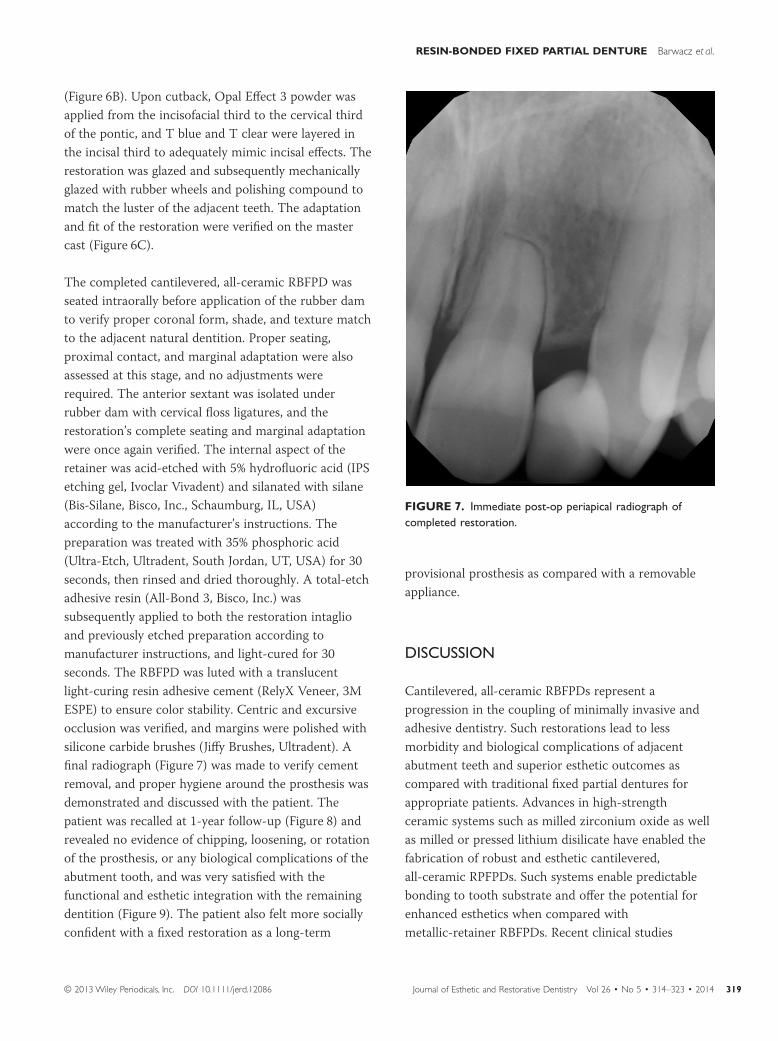
The completed cantilevered, all-ceramic RBFPD wasseated intraorally before application of the rubber damto verify proper coronal form, shade, and texture matchto the adjacent natural dentition. Proper seating,proximal contact, and marginal adaptation were alsoassessed at this stage, and no adjustments wererequired. The anterior sextant was isolated underrubber dam with cervical floss ligatures, and therestoration’s complete seating and marginal adaptationwere once again verified. The internal aspect of theretainer was acid-etched with 5% hydrofluoric acid (IPSetching gel, Ivoclar Vivadent) and silanated with silane(Bis-Silane, Bisco, Inc., Schaumburg, IL, USA)according to the manufacturer’s instructions. Thepreparation was treated with 35% phosphoric acid(Ultra-Etch, Ultradent, South Jordan, UT, USA) for 30seconds, then rinsed and dried thoroughly. A total-etchadhesive resin (All-Bond 3, Bisco, Inc.) wassubsequently applied to both the restoration intaglioand previously etched preparation according tomanufacturer instructions, and light-cured for 30seconds. The RBFPD was luted with a translucentlight-curing resin adhesive cement (RelyX Veneer, 3MESPE) to ensure color stability. Centric and excursiveocclusion was verified, and margins were polished withsilicone carbide brushes (Jiffy Brushes, Ultradent). Afinal radiograph (Figure 7) was made to verify cementremoval, and proper hygiene around the prosthesis wasdemonstrated and discussed with the patient. Thepatient was recalled at 1-year follow-up (Figure 8) andrevealed no evidence of chipping, loosening, or rotationof the prosthesis, or any biological complications of theabutment tooth, and was very satisfied with thefunctional and esthetic integration with the remainingdentition (Figure 9). The patient also felt more sociallyconfident with a fixed restoration as a long-term
provisional prosthesis as compared with a removableappliance.
DISCUSSION
Cantilevered, all-ceramic RBFPDs represent aprogression in the coupling of minimally invasive andadhesive dentistry. Such restorations lead to lessmorbidity and biological complications of adjacentabutment teeth and superior esthetic outcomes ascompared with traditional fixed partial dentures forappropriate patients. Advances in high-strengthceramic systems such as milled zirconium oxide as wellas milled or pressed lithium disilicate have enabled thefabrication of robust and esthetic cantilevered,all-ceramic RPFPDs. Such systems enable predictablebonding to tooth substrate and offer the potential forenhanced esthetics when compared withmetallic-retainer RBFPDs. Recent clinical studies
FIGURE 7. Immediate post-op periapical radiograph ofcompleted restoration.
RESIN-BONDED FIXED PARTIAL DENTURE Barwacz et al.
© 2013 Wiley Periodicals, Inc. DOI 10.1111/jerd.12086 Journal of Esthetic and Restorative Dentistry Vol 26 • No 5 • 314–323 • 2014 319

A
C
B
D
FIGURE 8. Clinical views of completed case at 1 year post-insertion (note gingival health apical to the pontic and connector):A, frontal view; B, lateral view; C, palatal view; D, incisal view.
A B
FIGURE 9. A, Centric retracted view. B, Smile photograph demonstrating acceptable esthetic integration with the remainingdentition.
RESIN-BONDED FIXED PARTIAL DENTURE Barwacz et al.
DOI 10.1111/jerd.12086 © 2013 Wiley Periodicals, Inc.Vol 26 • No 5 • 314–323 • 2014 Journal of Esthetic and Restorative Dentistry320

utilizing these ceramic materials for cantileveredRBFPDs have demonstrated promising results in the 3-to 5-year follow-up timeframe.
Sasse and colleagues reported a randomized, clinicaltrial evaluating 30 patients restored with cantilevered,all-ceramic RBFPDs fabricated with zirconium oxideretainers and frameworks with two adhesive systems.27
The study demonstrated a 3-year survival rate of 93.1%,if debonding was considered as a technical failure, and100% survival if only the final loss of the RBFPD,notwithstanding rebonded RBFPDs, was a criterion forsuccess. The investigators reported two debondingevents in this cohort that were attributable to traumaticevents (hits/pushes on chin and/or teeth). A secondcase-series study evaluated the clinical outcomes ofcantilevered, all-ceramic RBFPDs fabricated with IPSe.max Press for tooth replacement in the anteriormaxilla and mandible.25 A total of 35 patients (17maxillary sites, 18 mandibular sites) were treated andrecalled for a mean of 64.57 months (range 35–69months). The study reported no incidences ofprosthesis debonding, no postoperative sensitivity orrecurrent caries, or any prosthesis chipping orfracturing. Excellent 3- to 5-year survival outcomes incontrolled studies as well as successful documentedcase reports28,29 of cantilevered, all-ceramic RBFPDs areencouraging to practitioners who are presented withpatients who may desire a fixed restoration in ananterior, bounded edentulous site either as a long-termprovisional restoration or an alternative definitiverestoration to a single-tooth implant.
Two factors are of critical importance when evaluatingif a patient is a good candidate for a cantilevered,all-ceramic RBFPD. The first contributing factor toevaluate is the patient’s occlusion. It is the authors’experience that patients who present with mutuallyprotected occlusion including canine or group functiontend to have more successful outcomes withcantilevered RBFPDs. Prioritization of minimizinglateral and protrusive forces on the cantilevered ponticis of utmost concern for this restoration design.Patients who possess minimal vertical space because ofa deep overbite or supraeruption of opposing teethmake poor candidates for this treatment approach.
Such situations limit the height and width (and hencestrength) that can be established for the connectorregion of the all-ceramic prosthesis,30 as well as placethe restoration under greater stress in excursivemovements because of steeper inclines that must beovercome for the patient to function. The secondcritical factor to evaluate is the tooth that requiresreplacement. Hussey and Linden16 reported thatsignificant differences exist in the performance ofcantilevered RBFPDs based on the teeth that they werereplacing. In their study, cantilevered RBFPDs replacingmaxillary central incisors and canines had a tenfoldhigher failure rate, when compared with maxillarylateral incisors and premolars, as well as mandibularincisor and premolar teeth. Therefore, in addition toocclusion, the candidate tooth for replacement mustalso be taken into account by the clinician whenassessing the potential success of a cantilevered,all-ceramic RBFPD. It is of interest to note that Sun andcolleagues.25 did not include central incisors or caninesin their case-series study that reported 100% success.
The clinical case presented here was optimized not onlyby accounting for factors present clinically, such as ananterior open bite, anterior disclusion, and groupfunction in lateral excursive movements, but also by themicropreparation methodologies employed.Sonoabrasion via the use of oscillating diamond-coatedtips, as well as enhanced visualization of the field via adental operating microscope, allowed the authors a highdegree of control and accuracy while preparing thecanine abutment. Such sonoabrasive preparationmethodologies have been demonstrated to result in lesstooth substance loss after preparation as compared withtraditional rotary instrumentation31 and havetraditionally been proposed for Class II cavity lesionpreparation32,33 or finishing of prosthetic margins priorto prosthetic final impressions.34 To the authors’knowledge, this is the first report of oscillatinginstrumentation being employed for the preparation ofan abutment for a cantilevered, all-ceramic RBFPD.
When appropriate clinical conditions are present,cantilevered, all-ceramic RBFPDs are more conservativein nature, require less time for the clinician to prepareand impress, and are less burdensome to deliver than
RESIN-BONDED FIXED PARTIAL DENTURE Barwacz et al.
© 2013 Wiley Periodicals, Inc. DOI 10.1111/jerd.12086 Journal of Esthetic and Restorative Dentistry Vol 26 • No 5 • 314–323 • 2014 321
conventional double-retainer, all-ceramic RBFPDs. Forpatients with limited financial means, laboratory costswill also be less as compared with conventionaldouble-retainer RBFPDs. Additionally, there issignificantly less potential for developing recurrentcaries on a partially debonded retainer wing for acantilevered prosthesis, as such an event willimmediately lead to loss of the prosthesis, promptingthe patient to return to the practitioner for rebondingor repair.
In conclusion, the cantilevered, all-ceramic RBFPD is auniquely positioned prosthesis that can serve as either aminimally invasive definitive prosthesis for patients whoare not candidates for implant therapy, or as along-term fixed provisional prosthesis for the patientwho may desire to pursue implant therapy at a latertime, should skeletal growth, health, or finances be ofconcern. In order to obtain data that could potentiallyvalidate the treatment strategy employed in this casereport, future case-series, or more ideally, randomized,clinical trial studies including larger populations withlonger follow-up periods (greater than 5 years) arewarranted. Given that health care is increasinglymoving toward minimally invasive approaches whensurgical intervention is deemed necessary,35,36 it seemsnatural that such trends are increasingly beingseen in private and academic dentistry,37 wheresurgical procedures are completed and/or taughtroutinely.
DISCLOSURE
The authors declare no potential conflicts of interestwith respect to the authorship and/or publication ofthis article.
REFERENCES
1. Rochette AL. Attachment of a splint to enamel of loweranterior teeth. J Prosthet Dent 1973;30:418–23.
2. Howe DF, Denehy GE. Anterior fixed partial denturesutilizing the acid-etch technique and a cast metalframework. J Prosthet Dent 1977;37:28–31.
3. Livaditis GJ, Thompson VP. Etched castings: an improvedretentive mechanism for resin-bonded retainers.J Prosthet Dent 1982;47:52–8.
4. Barrack G, Bretz WA. A long-term prospective study ofthe etched-cast restoration. Int J Prosthodont1993;6:428–34.
5. Rammelsberg P, Pospiech P, Gernet W. Clinical factorsaffecting adhesive fixed partial dentures: a 6-year study.J Prosthet Dent 1993;70:300–7.
6. Kilpatrick NM, Wassell RW. The use of cantilevered,adhesively retained bridges with enhanced rigidity.Br Dent J 1994;176:13–6.
7. Simon JF, Gartrell RG, Grogono A. Improved retention ofacid-etched fixed partial dentures: a longitudinal study.J Prosthet Dent 1992;68:611–5.
8. Kern M, Knode H, Strubb JR. The all-porcelain,resin-bonded bridge. Quintessence Int 1991;22:257–62.
9. Kern M, Douglas WH, Fechtig T, et al. Fracture strengthof all-porcelain, resin-bonded bridges after testing in anartificial oral environment. J Dent 1993;21:117–21.
10. Kern M, Strub JR. Bonding to alumina ceramic inrestorative dentistry: clinical results over up to 5 years.J Dent 1998;26:245–9.
11. Kern M, Fechtig T, Strub JR. Influence of water storageand thermal cycling on the fracture strength ofall-porcelain, resin-bonded fixed partial dentures.J Prosthet Dent 1994;71:251–6.
12. Koutayas SO, Kern M, Ferraresso F, Strub JR. Influence ofdesign and mode of loading on the fracture strength ofall-ceramic resin-bonded fixed partial dentures: an invitro study in a dual-axis chewing simulator. J ProsthetDent 2000;83:540–7.
13. Hussey DL, Pagni C, Linden GJ. Performance of 400adhesive bridges fitted in a restorative dentistrydepartment. J Dent 1991;19:221–5.
14. Dunne SM, Millar BJ. A longitudinal study of the clinicalperformance of resin bonded bridges and splints. Br DentJ 1993;174:405–11.
15. Gilmour AS, Ali A. Clinical performance of resin-retainedfixed partial dentures bonded with a chemically activeluting cement. J Prosthet Dent 1995;73:569–73.
16. Hussey DL, Linden GJ. The clinical performance ofcantilevered resin-bonded bridgework. J Dent1996;24:251–6.
17. Briggs P, Dunne S, Bishop K. The single unit, singleretainer, cantilever resin-bonded bridge. Br Dent J1996;181:373–9.
18. Kern M, Glaser R. Cantilevered all-ceramic, resin-bondedfixed partial dentures: a new treatment modality. J EsthetDent 1997;9:255–64.
19. Botelho MG, Nor LC, Kwong HW, Kuen BS. Two-unitcantilevered resin-bonded fixed partial dentures—a
RESIN-BONDED FIXED PARTIAL DENTURE Barwacz et al.
DOI 10.1111/jerd.12086 © 2013 Wiley Periodicals, Inc.Vol 26 • No 5 • 314–323 • 2014 Journal of Esthetic and Restorative Dentistry322

retrospective, preliminary clinical investigation. Int JProsthodont 2000;13:25–8.
20. Botelho MG, Chan AW, Yiu EY, Tse ET. Longevity oftwo-unit cantilevered resin-bonded fixed partial dentures.Am J Dent 2002;15:295–9.
21. Chan AW, Barnes IE. A prospective study of cantileverresin-bonded bridges: an initial report. Aust Dent J2000;45:31–6.
22. Rashid SA, Al-Wahadni AM, Hussey DL. The periodontalresponse to cantilevered resin-bonded bridgework. J OralRehabil 1999;26:912–7.
23. Lam WY, Botelho MG, McGrath CP. Longevity ofimplant crowns and 2-unit cantilevered resin-bondedbridges. Clin Oral Implants Res 2012;24:1369–74.
24. Kern M, Sasse M. Ten-year survival of anteriorall-ceramic resin-bonded fixed dental prostheses. J AdhesDent 2011;13:407–10.
25. Sun Q, Chen L, Tian L, Xu B. Single-tooth replacement inthe anterior arch by means of a cantilevered IPS e.maxPress veneer-retained fixed partial denture: caseseries of 35 patients. Int J Prosthodont 2013;26:181–7.
26. Kern M. Clinical long-term survival of two-retainer andsingle-retainer all-ceramic resin-bonded fixed partialdentures. Quintessence Int 2005;36:141–7.
27. Sasse M, Eschbach S, Kern M. Randomized clinical trialon single retainer all-ceramic resin-bonded fixed partialdentures: influence of the bonding system after up to 55months. J Dent 2012;40:783–6.
28. Stumpel LJ 3rd, Haechler WH. The all-ceramic cantileverbridge: a variation on a theme. Compend Contin EducDent 2001;22:45–50. 52; quiz 54.
29. Foitzik M, Lennon AM, Attin T. Successful use of asingle-retainer all-ceramic resin-bonded fixed partial
denture for replacement of a maxillary canine: a clinicalreport. Quintessence Int 2007;38:241–6.
30. Wolfart S, Bohlsen F, Wegner SM, Kern M. A preliminaryprospective evaluation of all-ceramic crown-retained andinlay-retained fixed partial dentures. Int J Prosthodont2005;18:497–505.
31. Hugo B, Stassinakis A, Hofmann N. Comparison ofdifferent cavity preparation techniques and designs forprimary treatment of proximal carious lesions. DtschZahnärtzl Z 1998;53:441–7.
32. Hugo B, Stassinakis A. Preparation and restoration ofsmall interproximal carious lesions with sonicinstruments. Pract Periodontics Aesthet Dent1998;10:353–9, quiz 360.
33. Wicht MJ, Haak R, Fritz UB, Noack MJ. Primarypreparation of class II cavities with oscillating systems.Am J Dent 2002;15:21–5.
34. Massironi D. Optimizing the prosthetic margin withsonic instrumentation. Dent Today 2011;30:154–5.
35. Silvennoinen M, Mecklin JP, Saariluoma P, Antikainen T.Expertise and skill in minimally invasive surgery. Scand JSurg 2009;98:209–13.
36. Mack MJ. Minimally invasive and robotic surgery. JAMA2001;285:568–72.
37. Kaidonis J, Skinner V, Lekkas D, et al. Reorientatingdental curricula to reflect a minimally invasive dentistryapproach for patient-centred management. Aust Dent J2013;58(Suppl 1):70–5.
Reprint requests: Christopher A. Barwacz, DDS,The University of Iowa,
College of Dentistry, Craniofacial Clinical Research Center, W425 Dental
Science Building, Iowa City, IA 52242-1010, USA;Tel.: 319-384-3002;
Fax: 31-9353-5375; email: [email protected]
RESIN-BONDED FIXED PARTIAL DENTURE Barwacz et al.
© 2013 Wiley Periodicals, Inc. DOI 10.1111/jerd.12086 Journal of Esthetic and Restorative Dentistry Vol 26 • No 5 • 314–323 • 2014 323

Copyright of Journal of Esthetic & Restorative Dentistry is the property of Wiley-Blackwelland its content may not be copied or emailed to multiple sites or posted to a listserv withoutthe copyright holder's express written permission. However, users may print, download, oremail articles for individual use.