35020982
9
Effect of Artificial Oxygen Carrier with Chemotherapy on Tumor Hypoxia and Neovascularization Jianqun Han, Minghua Yu, Min Dai, Peilin Cui, Hongwei Li, Jian Zhang, Qian Liu and Ruijuan Xiu Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing, China Abstract: In addition to transfusion alternatives, artificial oxygen carriers are a benefit in ischemia disorders. This study aimed at evaluating the possible effects of PEG- conjugated hemoglobin (PEG-Hb) plus cisplatin on tumor hypoxia and neovasculature. Methods: HeLa cells were injected into submucosa of golden hamster cheek pouch to build tumor model. Animals were randomly assigned to 4 groups (n 10) and treated respectively: group 1, saline; group 2, cisplatin (5mg/kg); group 3, cisplatin (5mg/kg) plus PEG-Hb (0.3g/kg); group 4, cisplatin (5mg/kg) plus PEG-Hb (0.6g/kg). Tumor neovascularization morphological variation and tissue hypoxia were detected by intravital microscopy and immunostaining, respectively. Results: Microvessel tortuos- ity and area capillary density in peritumoral areas were notably depressed in group 4 compared with group 2 (p B0.05). Hypoxia markers pimonidazole and HIF-1a expression were decreased significantly in group 4. Conclusion: PEG-Hb in high concentration can notably improve tumor tissue oxygenation and normalize neovascu- lature; it may be a potential adjuvant to chemotherapy in cancer. Keywords: Oxygen carrier, tumor hypoxia, HIF-1a, angiogenesis, HeLa We thank Prof. T.M.S. Chang, McGill University, Canada, for serious review of this manuscript. This work was supported by Prof. Ruijuan Xiu’s UNESCO Award for Women in Science 2000 and the grant of ‘‘Knowledge Innovation Project,’’ Academy of Science, China (No.KJCX1-SW-07). Address correspondence to Ruijuan Xiu, Institute of Microcirculation, Chinese Academy of Medical Sciences (CAMS) & Peking Union Medical College (PUMC), 5 Dong Dan San Tiao, Beijing, 100005, China. E-mail: [email protected] Artificial Cells, Blood Substitutes, and Biotechnology, 36: 431438, 2008 Copyright # Informa UK Ltd. ISSN: 1073-1199 print / 1532-4184 online DOI: 10.1080/10731190802369789 431
-
Upload
istvan-portoero -
Category
Documents
-
view
12 -
download
2
description
35020983 artif
Transcript of 35020982

Effect of Artificial Oxygen Carrier with
Chemotherapy on Tumor Hypoxia and
Neovascularization
Jianqun Han, Minghua Yu, Min Dai, Peilin Cui,
Hongwei Li, Jian Zhang, Qian Liu and Ruijuan Xiu
Peking Union Medical College and Chinese Academy of Medical Sciences,
Beijing, China
Abstract: In addition to transfusion alternatives, artificial oxygen carriers are a benefit
in ischemia disorders. This study aimed at evaluating the possible effects of PEG-
conjugated hemoglobin (PEG-Hb) plus cisplatin on tumor hypoxia and neovasculature.
Methods: HeLa cells were injected into submucosa of golden hamster cheek pouch to
build tumor model. Animals were randomly assigned to 4 groups (n�10) and treated
respectively: group 1, saline; group 2, cisplatin (5mg/kg); group 3, cisplatin (5mg/kg)
plus PEG-Hb (0.3g/kg); group 4, cisplatin (5mg/kg) plus PEG-Hb (0.6g/kg). Tumor
neovascularization morphological variation and tissue hypoxia were detected by
intravital microscopy and immunostaining, respectively. Results: Microvessel tortuos-
ity and area capillary density in peritumoral areas were notably depressed in group 4
compared with group 2 (pB0.05). Hypoxia markers pimonidazole and HIF-1aexpression were decreased significantly in group 4. Conclusion: PEG-Hb in high
concentration can notably improve tumor tissue oxygenation and normalize neovascu-
lature; it may be a potential adjuvant to chemotherapy in cancer.
Keywords: Oxygen carrier, tumor hypoxia, HIF-1a, angiogenesis, HeLa
We thank Prof. T.M.S. Chang, McGill University, Canada, for serious review of this
manuscript. This work was supported by Prof. Ruijuan Xiu’s UNESCO Award for
Women in Science 2000 and the grant of ‘‘Knowledge Innovation Project,’’ Academy
of Science, China (No.KJCX1-SW-07).
Address correspondence to Ruijuan Xiu, Institute of Microcirculation, Chinese
Academy of Medical Sciences (CAMS) & Peking Union Medical College (PUMC), 5
Dong Dan San Tiao, Beijing, 100005, China. E-mail: [email protected]
Artificial Cells, Blood Substitutes, and Biotechnology, 36: 431�438, 2008
Copyright # Informa UK Ltd.
ISSN: 1073-1199 print / 1532-4184 online
DOI: 10.1080/10731190802369789
431

INTRODUCTION
It is now accepted that intratumoral hypoixa affects every major aspect of cancer
biology. Severe hypoxia is correlating with progression, angiogenesis, invation,
metastasis, and therapy resistance, etc. [12]. Thus, tumor hypoxia might
represent a novel potential target for therapeutic intervention in solid tumors [9].
A variety of experimental and clinical studies have demonstrated that the
structural and functional abnormalities of the vascular microenvironment such
as tortuosity, dilation, sacculation and permeability are the special character-
istics of cancer newly formed vessels [1,2,6]. The microvascular network
appears highly chaotic [22]; accordingly the irregular and less effective
mircovessels result in a small amount of anticancer drugs reaching the mass and
aggravation of tissue hypoxia. These changes make the situation more
complex. Microcirculation detection is a valuable parameter in the assessment
of the anticancer agent’s action on tumor vessels [16]. Previously we have
utilized a non-invasive computer-assisted intravital microscopy system to
observe and quantitatively analyze the vascular microenvironment repeatedly,
which enabled us to evaluate the influence of the drug on tumor microcircula-
tion [24,25]. So we utilize the model in the artificial oxygen carrier experiment
with emphasis on its possible chemo-sensitization effect in cancer treatment.
The development of an artificial oxygen carrier is associated with the
known and potential infective agents, ambulance service, and the shortage of
donor blood. To date, only nanotechnology based polyhemoglobin (PolyHb)
and conjugated Hb continue to show promise in clinical trials [5]. In addition
to transfusion alternatives, the artificial oxygen carrier is a benefit in ischemia
disorders [3,4,7]. The application of it in tumor tissue hypoxia was carried out
decades ago. Owing to the difference of tested samples and doses, some
controversial data exist, which indicate that there still will be a long way to go.
MATERIALS AND METHODS
Polyethyleneglycol-conjugated Hemoglobin (PEG-Hb)
The PEG-Hb used in this study was a Chinese domestic sample. Its
preparation processes and physiochemical properties belong to the manufac-
turer’s proprietary information and will not be discussed in this paper. The
sample was kept at 48C in the dark until use.
Tumor Cell Line
HeLa cells were obtained from the Cell Bank of the Chinese Academy of Medical
Sciences, Beijing, China, were grown in RPMI-1640 (Gibco, Life Technologies,
432 J. Han et al.

Vienna, Austria) supplemented with 10% heat-inactivated fetal bovine serum
(FBS), 100U/mL penicillin G, 0.1mg/ml streptomycin, termed the growth
medium, and maintained in a humidified atmosphere with 5% CO2 at 378C.
Animal Preparation and Drug Administration
Forty male Syrian hamsters (Mesocricetus auratus), 8 weeks old with an initial
average body weight of 85g, were used throughout the following experiments
performed in compliance with the guidelines of authorities. The tumor model
was built in the cheek pouch of the hamster as we described previously
[24,26]. Briefly, after acclimation, 40 animals were anesthetized with
pentobarbital sodium (30mg/kg b.w. i.p., sigma), and 5�106 HeLa cell
suspension (100mL) was injected into the submucosa cheek pouch of
hamsters. Two days after tumor-cell inoculation, animals all had an observable
tumor xenograft in inoculated point. The animals were then randomly assigned
to 4 groups (n�10) and treated respectively: group 1 was given saline via a
jugular catheter; group 2, cisplatin (5mg/kg in 0.5mL of saline, Mayne Pharma
Pty Ltd, Mulgrave, Australia); group 3, cisplatin (5mg/kg) combined with
PEG-Hb (0.3g/kg); group 4, cisplatin (5mg/kg) combined with PEG-Hb (0.6g/
kg). Five days after tumor-cell inoculation, hamsters in each group received
repeated treatment, respectively.
Intravital Microscopy
The development of the newly formed vessels was observed on days 0, 3, 5,
and 7 after tumor implantation with an intravital microscope (ACM, Zeiss,
Germany). Simultaneously, tumor volume was measured by sliding caliper.
During preparation and observation, the hamster’s cheek pouch was
continuously superfused with warmed physiological solution composed of
(in mM) 131.9 NaCl, 4.7 KCl, 2.0 CaCl2, 1.2 MgSO4, and 18 NaHCO3, PH
7.4 at 378C, and equilibrated with oxygen-containing gas. Then the recorded
microscopic images were analyzed off-line by a professional staff in a blinded
fashion. A computer-assisted digital image processing system (Institute of
Microcirculation, PUMC&CAMS, China) was used to quantitatively analyze
the changes of the microvessel tortuosity and area functional capillary density.
Detection of Tumor Hypoxia
Animals were sacrificed after a week of respective treatment, intraperitoneally
injected hamsters with pimonidazol hydrochloride (60mg/kg) (Hypoxyprobe-1,
Oxygen Carrier and Tumor Neovasculature 433

Chemicon, USA) 1hr before being sacrificed. A tumor mass of appropriate
size was fixed in neutral-buffered formalin (10%) following paraffin
imbedding. Immunostaining for pimonidazole and HIF-1a was carried out
on contiguous sections using procedures described previously [11,15]. The
primary antibodies were polyclonal anti-HIF-1a (1:25 dilution) from Santa
Cruz Biotechnology (Santa Cruz, CA, USA) and Hypoxyprobe-1Mab1 (1:50
dilution) from Chemicon (California, USA). The resultant immunocomplexes
were detected with horseradish peroxidase-conjugated antirabbit IgG (Santa
Cruz Biotechnology). Eosin (HIF-1a sections) or hematoxlin (pimonidazole
sections) were used as counterstains.
Statistical Analysis
All data were presented as mean9S.E.M. Statistical analysis was performed
using the statistical program SPSS 10.0 for Windows (SPSS Inc., Chicago, IL,
USA) and differences were analyzed by one-way ANOVA. The level of
significance was taken as PB0.05.
RESULTS
1. Tumor Growth and Development of Neovasculature
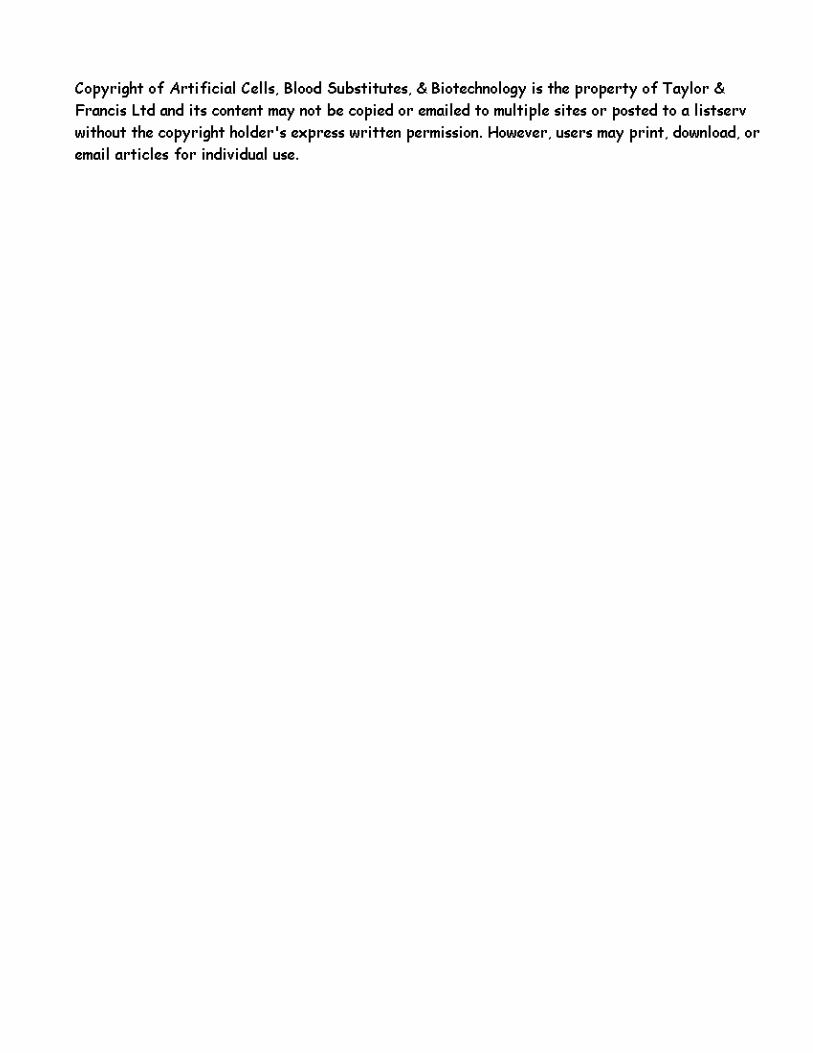
On the 2nd day after implantation, neoplasma were visible in all hamsters;
after respective drugs administration, tumor volume was decreased sharply in
groups 2, 3 and 4 compared with group 1 (PB0.01). There was no significant
difference in tumor volume when cisplatin combined with or without artificial
oxygen carrier in a short time period (Figure 1).
Compared with contralateral normal cheek pouch mucosa microvessels,
chaotic and heterogeneous microvasculature was presented in tumor side
characterized by dilation, tortuosity, sacculation and permeability profiles.
Quantitatively evaluation neoplasma neovascular network revealed that
increasing microvessel tortuosity and area capillary density were obvious in
peritumoral areas after tumor cell inoculation in group 1. However, these
changes were notably depressed after cisplatin combined with or without the
oxygen carrier. The interesting thing is that group 4, combined with a higher
dose of oxygen carrier, had a further inhibiting effect on these changes
compared with group 2 (cisplatin alone) on the fifth day (tortuosity) and fifth
and seventh day (capillary density), respectively (Figure 2 and 3). But in
group 3, combined with a low dose of oxygen carrier, this effect was not
significant.
434 J. Han et al.
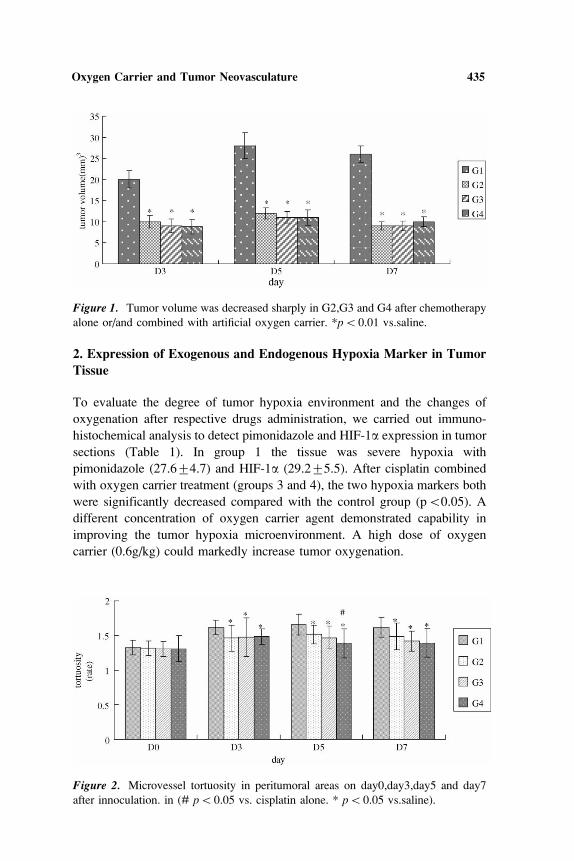
2. Expression of Exogenous and Endogenous Hypoxia Marker in Tumor
Tissue
To evaluate the degree of tumor hypoxia environment and the changes of
oxygenation after respective drugs administration, we carried out immuno-
histochemical analysis to detect pimonidazole and HIF-1a expression in tumor
sections (Table 1). In group 1 the tissue was severe hypoxia with
pimonidazole (27.694.7) and HIF-1a (29.295.5). After cisplatin combined
with oxygen carrier treatment (groups 3 and 4), the two hypoxia markers both
were significantly decreased compared with the control group (pB0.05). A
different concentration of oxygen carrier agent demonstrated capability in
improving the tumor hypoxia microenvironment. A high dose of oxygen
carrier (0.6g/kg) could markedly increase tumor oxygenation.
Figure 1. Tumor volume was decreased sharply in G2,G3 and G4 after chemotherapy
alone or/and combined with artificial oxygen carrier. *pB0.01 vs.saline.
Figure 2. Microvessel tortuosity in peritumoral areas on day0,day3,day5 and day7
after innoculation. in (# pB0.05 vs. cisplatin alone. * pB0.05 vs.saline).
Oxygen Carrier and Tumor Neovasculature 435

DISCUSSION
More attention has recently focused on tumor hypoxia in tumor treatment.
Severe hypoxia is correlating with progression, angiogenesis, metastasis and
therapy resistance. Previous studies documented that in hypoxia condition
tumor cells were susceptible to chemoresistance, with the possible reasons
including poor drug distribution, quiencent tumor cell existence, acquired drug
resistance feature, and loss of apoptotic potential [23,27]. Many attempts have
been performed based on these experimental and preclinical observations
targeting tumor hypoxia.
Artificial oxygen carrier is a perfect mediator in oxygen transmission and
offloading. One type of oxygen carrier perfluorocarbon (PFC) emulsions plus
carbogen breathing have definite adjuvant effects in radiotherapy as well as
chemotherapy in tumor treatment [13,20,21]. Teicher further explored
hemoglobin preparation on the response of tumor models to radiotherapy
and chemotherapy [17�19]. Contrary data have also been reported [10,14].
Figure 3. Microvessel area capillary density in peritumoral areas on day0,day3,day5
and day7 after respective treatment. (# pB0.05 vs. cisplatin alone. * pB0.05
vs.saline).
Table 1. Pimonidazole and HIF-1a expression in neoplasma (mean9S.E.M.)
Group Number Pimonidazole% HIF-1a%
group 1 10 27.694.7 29.295.5
group 2 10 22.593.8 24.196.4
group 3 10 20.594.1* 22.594.7*
group 4 10 14.893.2* # 17.895.3* #
% percentage of tumor area staining positive for HIF-1aimmunoreactivity or pimoni-
dazole binding. * pB0.05 vs.saline # pB0.05 vs. cisplatin alone. group 1 saline; group
2 cisplatin alone; group 3 cisplatin with PEG-Hb (0.3g/kg); group4 cisplatin with PEG-
Hb(0.6/kg).
436 J. Han et al.

The reported results indicate the oxygen carrier’s adjuvant effect in tumor
therapy may depend on the tested sample type and dose. In this experiment,
we have designed two different concentration samples to test the possible
effect of PEG-Hb on chemo-sensitization. Although the low concentration of
PEG-Hb had some influence, it was not a statistical significance. Herein, PEG-
Hb had notable influence on tumor neovasculature and tissue oxygenation
induced by PEG-Hb in high concentration; this effect was based on lable
tumor hypoxia and microvessels morphological observations.
As we mentioned above, tumor neovascularization has its special
charicteristics. In our established tumor model chaotic and heterogeneous
microvasculature was presented. A similar phenomenon existed in Gim-
brone’s tumor model [8]. Tissue hypoxia induce angiogenesis; conversely, the
irregular and less effective microvessels result in a small amount of anticancer
drugs reaching the mass and aggravation of tissue hypoxia. Therefore, these
changes make the situation more complex. Microcirculation detection is a
valuable parameter in assessing the anticancer agent’s action on tumor vessels
[16]. Previously, we have utilized a non-invasive computer-assisted intravital
microscopy system to observe and quantitatively analyze the vascular
microenvironment repeatedly, which enables us to evaluate the influence of
the drug on tumor microcirculation [24,25]. Herein, we also measured the
tumor volume. PEG-Hb had no marked effect on it compared with cisplatin
alone. It might be due to the relatively short period of drug administration. We
have tested PEG-Hb in another tumor model on BALB/C nude mice with
conventional therapy time and a better effect on tumor volume was observed
(in press), whereas the microvessels structure normalization was obvious. We
are the first to show a direct relationship of oxygen carrier to tumor
neovascularization, although this study has some shortcomings.
In summary, tumor angiogenesis can be directly observed in our tumor
model, which is a non-invasive ideal platform to quantitatively analyze the
microvasculature repeatedly and assess the drugs’ action on it. PEG-Hb in
high concentration can notably improve tumor tissue oxygenation and
normalize neovasculature. It is indicated that the evaluated artificial oxygen
carrier (PEG-Hb) may be a potential adjuvant to chemotherapy in cancer.
REFERENCES
1. Bullitt, E., Lin, N. U., Ewend, M. G., Zeng, D., Winer, E. P., Carey, L. A., Smith,
J. K. (2006). Med Image Comput Comput Assist Interv Int Conf Med ImageComput Comput Assist Interv 9:561�568.
2. Bullitt, E., Lin, N. U., Smith, J. K., Zeng, D., Winer, E. P., Carey, L. A., Lin, W.,
Ewend, M. G. (2007). Radiology 245:824�830.
3. Burkhoff, D., Lefer, D. J. (2005). Am Heart J 149:573�579.
Oxygen Carrier and Tumor Neovasculature 437

4. Caswell, J. E., Strange, M. B., Rimmer, D. M., 3rd, Gibson, M. F., Cole, P., Lefer,
D. J. (2005). Am J Physiol Heart Circ Physiol 288:H1796�1801.
5. Chang, T. M. (2006). Trends Biotechnol 24:372�377.
6. De Felice, C., Latini, G., Bianciardi, G., Parrini, S., Fadda, G. M., Marini, M.,
Laurini, R. N., Kopotic, R. J. (2003). Gut 52:1764�1767.
7. George, I., Yi, G. H., Schulman, A. R., Morrow, B. T., Cheng, Y., Gu, A., Zhang,
G., Oz, M. C., Burkhoff, D., Wang, J. (2006). Am J Physiol Heart Circ Physiol291:H1126�1137.
8. Gimbrone, M. A., Jr. Gullino, P. M. (1976). Cancer Res 36:2611�2620.
9. Gordan, J. D., Simon, M. C. (2007). Curr Opin Genet Dev 17:71�77.
10. Gottschalk, A., Raabe, A., Hommel, M., Rempf, C., Freitag, M., Standl, T. (2005).
Artif Cells Blood Substit Immobil Biotechnol 33:379�389.
11. Jankovic, B., Aquino-Parsons, C., Raleigh, J. A., Stanbridge, E. J., Durand, R. E.,
Banath, J. P., MacPhail, S. H., Olive, P. L. (2006). Cytometry B Clin Cytom70:45�55.
12. Kim, J. W., Gao, P., Dang, C. V. (2007). Cancer Metastasis Rev 26:291�298.
13. Martin, D. F., Kimler, B. F., Evans, R. G., Morantz, R. A. and Vats, T. S. (1988).
NCI Monogr. 119�122.
14. Raabe, A., Gottschalk, A., Hommel, M., Dubben, H. H., Strandl, T. (2005).
Strahlenther Onkol 181:730�737.
15. Raleigh, J. A., Calkins-Adams, D. P., Rinker, L. H., Ballenger, C. A., Weissler
M. C., Fowler, W. C., Jr., Novotny, D. B., Varia, M. A. (1998). Cancer Res 58:
3765�3768.
16. Read, T. A., Farhadi, M., Bjerkvig, R., Olsen, B. R., Rokstad, A. M., Huszthy
P. C., Vajkoczy, P. (2001). Cancer Res 61:6830�6837.
17. Teicher, B. A., Dupuis, N. P., Emi, Y., Ikebe, M., Kakeji, Y., Menon, K. (1995).
In Vivo 9:11�18.
18. Teicher, B. A., Holden, S. A., Ara, G., Herman, T. S., Hopkins, R. E., Menon, K.
(1992). Biomater Artif Cells Immobilization Biotechnol 20:657�660.
19. Teicher, B. A., Holden, S. A., Menon, K., Hopkins, R. E., Gawryl, M. S. (1993).
Cancer Chemother Pharmacol 33:57�62.
20. Teicher, B. A., Lazo, J. S., Merrill, W. W., Filderman, A. E., Rose, C. M. (1986).
Cancer Chemother Pharmacol 18:213�218.
21. Teicher, B. A., McIntosh-Lowe, N. L., Rose, C. M. (1988). Biomater Artif CellsArtif Organs 16:533�546.
22. Vicaut, E. (2001). Therapie 56:483�494.
23. Wartenberg, M., Ling, F. C., Muschen, M., Klein, F., Acker, H., Gassmann, M.,
Petrat, K., Putz, V., Hescheler, J., Sauer, H. (2003). Faseb J 17:503�505.
24. Xiu, R. J., Duan, C. G., Mu, G. F. (1987). Zhonghua Zhong Liu Za Zhi 9:95�98.
25. Xiu, R. J., Duan, C. G., Mu, G. F. (1988). Proc Chin Acad Med Sci Peking UnionMed Coll 3:26�32.
26. Yu, M., Han, J., Cui, P., Dai, M., Li, H., Zhang, J., Xiu, R. (2008). Cancer Sci99:391�397.
27. Zhang, W., Zhang, H. (2006). J Huazhong Univ Sci Technolog Med Sci 26:
520�523.
438 J. Han et al.