
3 ZARXIO PRODUCT ATTRIBUTES 6 Commercial Co … · Part B biosimilar biological product payment and...
6
Important Safety Information CONTRAINDICATIONS • ZARXIO is contraindicated in patients with a history of serious allergic reactions to human granulocyte colony-stimulating factors such as filgrastim or pegfilgrastim products. WARNINGS AND PRECAUTIONS • Splenic rupture, including fatal cases, has been reported following the administration of filgrastim products. Patients who report left upper abdominal or shoulder pain should be evaluated. • Acute respiratory distress syndrome (ARDS) has been reported in patients receiving filgrastim products. Patients who develop fever and lung infiltrates or respiratory distress should be evaluated. Discontinue ZARXIO in patients with ARDS. • Serious allergic reactions, including anaphylaxis, have been reported in patients receiving filgrastim products. The majority of reported events occurred upon initial exposure. Provide symptomatic treatment for allergic reactions. Allergic reactions, including anaphylaxis, in patients receiving filgrastim products can recur within days after the discontinuation of initial anti-allergic treatment. Permanently discontinue ZARXIO in patients with serious allergic reactions. • Sickle cell crisis, in some cases fatal, has been reported with the use of filgrastim products in patients with sickle cell trait or sickle cell disease. Supported by the totality of evidence for biosimilarity and the expertise of Sandoz, a Novartis Division 2,3 • Approved in the US in 2015 • Approved in Europe in 2009 4 • More than 7.5 million patient-exposure days outside of the US 4 • Confirmed biosimilarity to Neupogen ® (filgrastim) 1,4,5 Please see additional Important Safety Information throughout and accompanying full Prescribing Information. ZARXIO is a registered trademark of Novartis AG. Neupogen is a registered trademark of Amgen Inc. ZARXIO shares the following 5 indications with Neupogen ®3,6 • Patients with Cancer Receiving Myelosuppressive Chemotherapy • Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation Chemotherapy • Patients with Cancer Undergoing Bone Marrow Transplantation • Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and Therapy • Patients with Severe Chronic Neutropenia
Transcript of 3 ZARXIO PRODUCT ATTRIBUTES 6 Commercial Co … · Part B biosimilar biological product payment and...

PRODUCT ATTRIBUTES
Identical routes of administration
Identical dosing schedules
Identical dosage strengths
ZARXIO3 Neupogen®
(filgrastim)6
To learn more about enrolling your patients, go to www.sandozonesource.com.
94
1
2
3
4
5
Patients with Cancer Receiving Myelosuppressive Chemotherapy ZARXIO is indicated to decrease the incidence of infection‚ as manifested by febrile neutropenia‚ in patients with nonmyeloid malignancies receiving myelosuppressive anti-cancer drugs associated with a significant incidence of severe neutropenia with fever.
Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation ChemotherapyZARXIO is indicated to reduce the time to neutrophil recovery and the duration of fever, following induction or consolidation chemotherapy treatment of patients with acute myeloid leukemia (AML).
Patients with Cancer Undergoing Bone Marrow TransplantationZARXIO is indicated to reduce the duration of neutropenia and neutropenia-related clinical sequelae‚ e.g., febrile neutropenia, in patients with nonmyeloid malignancies undergoing myeloablative chemotherapy followed by bone marrow transplantation.
Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and TherapyZARXIO is indicated for the mobilization of autologous hematopoietic progenitor cells into the peripheral blood for collection by leukapheresis.
Patients with Severe Chronic NeutropeniaZARXIO is indicated for chronic administration to reduce the incidence and duration of sequelae of neutropenia (e.g., fever, infections, oropharyngeal ulcers) in symptomatic patients with congenital neutropenia, cyclic neutropenia, or idiopathic neutropenia.
ZARXIO® (filgrastim-sndz) Shares the Following 5 Indications With Neupogen® (filgrastim)3,6
Important Safety InformationWARNINGS AND PRECAUTIONS (cont’d)• Thrombocytopenia has been reported in patients receiving filgrastim products.
Monitor platelet counts.
• Leukocytosis:
º Patients with Cancer Receiving Myelosuppressive Chemotherapy: White blood cell counts of 100‚000/mm3 or greater were observed in approximately 2% of patients receiving filgrastim at dosages above 5 mcg/kg/day. In patients with cancer receiving ZARXIO as an adjunct to myelosuppressive chemotherapy‚ to avoid the potential risks of excessive leukocytosis‚ it is recommended that ZARXIO therapy be discontinued if the ANC surpasses 10‚000/mm3 after the chemotherapy-induced ANC nadir has occurred. Monitor CBCs at least twice weekly during therapy.
º Peripheral Blood Progenitor Cell (PBPC) Collection and Therapy: During the period of administration of ZARXIO for PBPC mobilization in patients with cancer, discontinue ZARXIO if the leukocyte count rises to >100,000/mm3.
• Cutaneous vasculitis has been reported in patients treated with filgrastim products. In most cases‚ the severity of cutaneous vasculitis was moderate or severe. Most of the reports involved patients with SCN receiving long-term filgrastim therapy. Hold ZARXIO therapy in patients with cutaneous vasculitis. ZARXIO may be started at a reduced dose when the symptoms resolve and the ANC has decreased.
$0 $10out-of-pocket for fi rst dose or cycle
out-of-pocket forsubsequent doses or cycles
• For eligible commercially insured patients
• No income eligibility requirements
Program Eligibility Requirements:• Maximum benefi t of $10,000 annually
• ZARXIO prescription must be for an approved indication
• This program is not health insurance. This program is for insured patients only; cash-paying or uninsured patients are not eligible
• Patients are not eligible if prescriptions are paid, in whole or in part, by any state or federally funded programs including, but not limited to, Medicare (including Part D, even in the coverage gap), Medicaid, Medigap, VA, DOD, TriCare, private indemnity, HMO insurance plans that reimburse the patient for the entire cost of their prescription drugs, or where prohibited by law
• Co-Pay Program may apply to out-of-pocket expenses that occurred within 120 days prior to the date of the enrollment
• Patients can participate for a maximum of 12 months
• Co-Pay Program may not be combined with any other rebate, coupon, or offer
• Sandoz reserves the right to rescind, revoke, or amend this offer without further notice
Commercial Co-Pay Program forZARXIO® (fi lgrastim-sndz)
Please see Important Safety Information throughoutand accompanying full Prescribing Information.
ZARXIO is a registered trademark of Novartis AG.Sandoz One Source is a trademark of Novartis AG.
Important Safety InformationCONTRAINDICATIONS• ZARXIO is contraindicated in patients with a history of serious allergic reactions to human
granulocyte colony-stimulating factors such as filgrastim or pegfilgrastim products.
WARNINGS AND PRECAUTIONS• Splenic rupture, including fatal cases, has been reported following the administration of
filgrastim products. Patients who report left upper abdominal or shoulder pain shouldbe evaluated.
• Acute respiratory distress syndrome (ARDS) has been reported in patients receiving filgrastim products. Patients who develop fever and lung infiltrates or respiratory distress should be evaluated. Discontinue ZARXIO in patients with ARDS.
• Serious allergic reactions, including anaphylaxis, have been reported in patients receiving filgrastim products. The majority of reported events occurred upon initial exposure. Provide symptomatic treatment for allergic reactions. Allergic reactions, including anaphylaxis, in patients receiving filgrastim products can recur within days after the discontinuation of initial anti-allergic treatment. Permanently discontinue ZARXIO in patients with serious allergic reactions.
• Sickle cell crisis, in some cases fatal, has been reported with the use of filgrastim products in patients with sickle cell trait or sickle cell disease.
Supported by the totality of evidence for biosimilarityand the expertise of Sandoz, a Novartis Division2,3
• Approved in the US in 2015
• Approved in Europe in 20094
• More than 7.5 million patient-exposure days outside of the US4
• Confirmed biosimilarity to Neupogen® (filgrastim)1,4,5
Please see additional Important Safety Information throughout and accompanying full Prescribing Information.ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.
ZARXIO shares the following 5 indications with Neupogen®3,6
• Patients with Cancer Receiving Myelosuppressive Chemotherapy
• Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation Chemotherapy
• Patients with Cancer Undergoing Bone Marrow Transplantation
• Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and Therapy
• Patients with Severe Chronic Neutropenia
ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.Sandoz One Source is a trademark of Novartis AG.
© 2017 Sandoz Inc., 100 College Road West, Princeton, NJ 08540 All Rights Reserved. S-ZRX-1341272 03/2017
References: 1. FDA approves first biosimilar product Zarxio [press release]. US Food and Drug Administration; March 6, 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm436648.htm. Accessed March 3, 2017.2. Data on file. Sandoz Inc. Princeton, NJ. 3. ZARXIO Prescribing Information. Sandoz Inc. February 2017. 4. US Food and Drug Administration. Christl L. Overview of the regulatory pathway and FDA’s guidance for the development and approval of biosimilar products in the US (approved in European Union under the trade name Zarzio). 5. Blackwell K, Semiglazov V, Krasnozhon D, et al. Comparison of EP2006, a filgrastim biosimilar, to the reference: a phase III, randomized, double-blind clinical study in the prevention of severe neutropenia in patients with breast cancer receiving myelosuppressive chemotherapy. Ann Oncol. 2015;26(9):1948-1953. http://annonc.oxfordjournals.org/content/26/9/1948.full.pdf. Accessed March 3, 2017. 6. Neupogen® Prescribing Information. Amgen Inc. June 2016. 7. US Department of Health and Human Services; Draft guidance. Applications covered by Section 505(b)(2). Washington, DC: US Dept of Health and Human Services; October 1999. 8. US Department of Health and Human Services. Scientific considerations in demonstrating biosimilarity to a reference product. Washington, DC: US Dept of Health and Human Services; April 2015. 9. US Department of Health and Human Services. Draft guidance. Reference product exclusivity for biological products filed under Section 351(a) of the PHS Act. Washington, DC: US Dept of Health and Human Services; August 2014. 10. Affordable Care Act, Title VII, Biologics Price Competition Innovation Act, Subtitle A, Section 7002. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/ucm216146.pdf. Accessed March 3, 2017. 11. Centers for Medicare & Medicaid Services. Part B biosimilar biological product payment and required modifiers. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Part-B-Drugs/McrPartBDrugAvgSalesPrice/Part-B-Biosimilar-Biological-Product-Payment.html. Accessed March 3, 2017.
TRUST the Totality of Evidence for ZARXIO® (filgrastim-sndz) and the Expertise of Sandoz2,3
For the ZARXIO prefilled syringe, direct administration of less than 0.3 mL is not recommended.3
HCPCS code Q5101 Injection, Filgrastim (G-CSF), Biosimilar, 1 microgram11
Effective January 1, 2016, Corresponding Required Modifier when billing Q5101 for Zarxio is ZA-Novartis/Sandoz11
• As commercial and public payer requirements may vary, providers should verify payer-specific coding requirements and may contact Sandoz One SourceTM for additional reimbursement information
Please see Important Safety Information throughoutand accompanying full Prescribing Information.

STATUTE
STATUTE
New DrugNDA 505(b)(1)
Generic DrugANDA 505(j)
Abbreviated NewDrug PathwayNDA 505(b)(2)
Biologic9
BLA 351(a)12-year exclusivity
Biosimilar10
BLA 351(k)(2)(A)
Interchangeable Biosimilar10*BLA 351(k)(2)(B)
1-year exclusivity
Federal Food, Drug,and Cosmetic Act7
Public HealthService Act
APPLICATION
APPLICATION
Biosimilar requirements and ZARXIO
Statutory requirement ZARXIO fulfillment of requirement
Analytical data• Physiochemical and functional analytical data
demonstrated that ZARXIO is highly similar to Neupogen® (filgrastim)2
Animal studies*• Five animal studies confirmed that the
pharmacologic and toxicological profiles of ZARXIO and Neupogen® are similar2
Clinical studies
• Study to evaluate pharmacodynamics, pharmacokinetics, and safety2
• Study to evaluate comparative efficacy and safety of ZARXIO and Neupogen® (the PIONEER study)5
Mechanism of action• The mechanism of action of filgrastim is mediated
by selective binding to the G-CSF receptor and is similar across all labeled indications2,3
Route of administration, dosage form, and strength
• ZARXIO has the same route of administration, dosage form, and strengths as Neupogen®3,6
DE
MO
NS
TRA
TE
HIG
H S
IMIL
AR
ITY
R
EFER
ENCE
SAM
E A
SB
IOLO
GIC
2
Current US Regulatory Approval Pathways for New Drugs, Generics, and Biosimilars7-10
ZARXIO® (filgrastim-sndz), the first FDA-approved biosimilar, was reviewed via the abbreviated pathway under section 351(k) of the PHS Act and was proven highly similar to the reference biologic1,8
ANDA=Abbreviated new drug application; BLA=Biologics license application; NDA=New drug application; PHS=Public Health Service.
*Sandoz did not seek a designation of interchangeability for ZARXIO.
Important Safety InformationWARNINGS AND PRECAUTIONS (cont’d)• Glomerulonephritis has occurred in patients receiving filgrastim products. The diagnoses
were based upon azotemia, hematuria (microscopic and macroscopic), proteinuria, and renal biopsy. Generally, events of glomerulonephritis resolved after dose reduction or discontinuation of filgrastim products. If glomerulonephritis is suspected, evaluate for cause. If causality is likely, consider dose-reduction or interruption of ZARXIO.
• Alveolar hemorrhage manifesting as pulmonary infiltrates and hemoptysis requiring hospitalization have been reported in healthy donors treated with filgrastim products undergoing peripheral blood progenitor cell (PBPC) collection mobilization. Hemoptysis resolved with discontinuation of filgrastim. The use of ZARXIO for PBPC mobilization in healthy donors is not an approved indication.
Sandoz: the US Biosimilar Pathway PioneerThe efforts of Sandoz led to the development of the first biosimilar to receive FDA approval. Sandoz selected comprehensive methods to fully characterize and evaluate ZARXIO in order to meet all FDA requirements.1
Important Safety InformationWARNINGS AND PRECAUTIONS (cont’d)• Capillary leak syndrome (CLS) has been reported after G-CSF administration, including
filgrastim products, and is characterized by hypotension, hypoalbuminemia, edema and hemoconcentration. Episodes vary in frequency, severity and may be life-threatening if treatment is delayed. Patients who develop symptoms of capillary leak syndrome should be closely monitored and receive appropriate treatment.
• Confirm the diagnosis of severe chronic neutropenia (SCN) before initiating ZARXIO therapy. Myelodysplastic syndrome (MDS) and acute myelogenous leukemia (AML) have been reported to occur in the natural history of congenital neutropenia without cytokine therapy. Cytogenetic abnormalities, transformation to MDS, and AML have also been observed in patients treated with filgrastim products for SCN. Abnormal cytogenetics and MDS have been associated with the eventual development of myeloid leukemia. The effect of filgrastim products on the development of abnormal cytogenetics and the effect of continued filgrastim administration in patients with abnormal cytogenetics or MDS are unknown. If a patient with SCN develops abnormal cytogenetics or myelodysplasia‚ the risks and benefits of continuing ZARXIO should be carefully considered.
Please see additional Important Safety Information throughout and accompanying full Prescribing Information.ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.
* The use of EU-approved Neupogen® as comparator for the non-clinical development of ZARXIO is considered justified by the high level of similarity between EU-approved and US-licensed Neupogen®.4
3
STATUTE
STATUTE
New DrugNDA 505(b)(1)
Generic DrugANDA 505(j)
Abbreviated NewDrug PathwayNDA 505(b)(2)
Biologic9
BLA 351(a)12-year exclusivity
Biosimilar10
BLA 351(k)(2)(A)
Interchangeable Biosimilar10*BLA 351(k)(2)(B)
1-year exclusivity
Federal Food, Drug,and Cosmetic Act7
Public HealthService Act
APPLICATION
APPLICATION
Biosimilar requirements and ZARXIO
Statutory requirement ZARXIO fulfillment of requirement
Analytical data• Physiochemical and functional analytical data
demonstrated that ZARXIO is highly similar to Neupogen® (filgrastim)2
Animal studies*• Five animal studies confirmed that the
pharmacologic and toxicological profiles of ZARXIO and Neupogen® are similar2
Clinical studies
• Study to evaluate pharmacodynamics, pharmacokinetics, and safety2
• Study to evaluate comparative efficacy and safety of ZARXIO and Neupogen® (the PIONEER study)5
Mechanism of action• The mechanism of action of filgrastim is mediated
by selective binding to the G-CSF receptor and is similar across all labeled indications2,3
Route of administration, dosage form, and strength
• ZARXIO has the same route of administration, dosage form, and strengths as Neupogen®3,6
DE
MO
NS
TRA
TE
HIG
H S
IMIL
AR
ITY
R
EFER
ENCE
SAM
E A
SB
IOLO
GIC
2
Current US Regulatory Approval Pathways for New Drugs, Generics, and Biosimilars7-10
ZARXIO® (filgrastim-sndz), the first FDA-approved biosimilar, was reviewed via the abbreviated pathway under section 351(k) of the PHS Act and was proven highly similar to the reference biologic1,8
ANDA=Abbreviated new drug application; BLA=Biologics license application; NDA=New drug application; PHS=Public Health Service.
*Sandoz did not seek a designation of interchangeability for ZARXIO.
Important Safety InformationWARNINGS AND PRECAUTIONS (cont’d)• Glomerulonephritis has occurred in patients receiving filgrastim products. The diagnoses
were based upon azotemia, hematuria (microscopic and macroscopic), proteinuria, and renal biopsy. Generally, events of glomerulonephritis resolved after dose reduction or discontinuation of filgrastim products. If glomerulonephritis is suspected, evaluate for cause. If causality is likely, consider dose-reduction or interruption of ZARXIO.
• Alveolar hemorrhage manifesting as pulmonary infiltrates and hemoptysis requiring hospitalization have been reported in healthy donors treated with filgrastim products undergoing peripheral blood progenitor cell (PBPC) collection mobilization. Hemoptysis resolved with discontinuation of filgrastim. The use of ZARXIO for PBPC mobilization in healthy donors is not an approved indication.
Sandoz: the US Biosimilar Pathway PioneerThe efforts of Sandoz led to the development of the first biosimilar to receive FDA approval. Sandoz selected comprehensive methods to fully characterize and evaluate ZARXIO in order to meet all FDA requirements.1
Important Safety InformationWARNINGS AND PRECAUTIONS (cont’d)• Capillary leak syndrome (CLS) has been reported after G-CSF administration, including
filgrastim products, and is characterized by hypotension, hypoalbuminemia, edema and hemoconcentration. Episodes vary in frequency, severity and may be life-threatening if treatment is delayed. Patients who develop symptoms of capillary leak syndrome should be closely monitored and receive appropriate treatment.
• Confirm the diagnosis of severe chronic neutropenia (SCN) before initiating ZARXIO therapy. Myelodysplastic syndrome (MDS) and acute myelogenous leukemia (AML) have been reported to occur in the natural history of congenital neutropenia without cytokine therapy. Cytogenetic abnormalities, transformation to MDS, and AML have also been observed in patients treated with filgrastim products for SCN. Abnormal cytogenetics and MDS have been associated with the eventual development of myeloid leukemia. The effect of filgrastim products on the development of abnormal cytogenetics and the effect of continued filgrastim administration in patients with abnormal cytogenetics or MDS are unknown. If a patient with SCN develops abnormal cytogenetics or myelodysplasia‚ the risks and benefits of continuing ZARXIO should be carefully considered.
Please see additional Important Safety Information throughout and accompanying full Prescribing Information.ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.
* The use of EU-approved Neupogen® as comparator for the non-clinical development of ZARXIO is considered justified by the high level of similarity between EU-approved and US-licensed Neupogen®.4
3

PRODUCT ATTRIBUTES
Identical routes of administration
Identical dosing schedules
Identical dosage strengths
ZARXIO3 Neupogen®
(filgrastim)6
To learn more about enrolling your patients, go to www.sandozonesource.com.
94
1
2
3
4
5
Patients with Cancer Receiving Myelosuppressive Chemotherapy ZARXIO is indicated to decrease the incidence of infection‚ as manifested by febrile neutropenia‚ in patients with nonmyeloid malignancies receiving myelosuppressive anti-cancer drugs associated with a significant incidence of severe neutropenia with fever.
Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation ChemotherapyZARXIO is indicated to reduce the time to neutrophil recovery and the duration of fever, following induction or consolidation chemotherapy treatment of patients with acute myeloid leukemia (AML).
Patients with Cancer Undergoing Bone Marrow TransplantationZARXIO is indicated to reduce the duration of neutropenia and neutropenia-related clinical sequelae‚ e.g., febrile neutropenia, in patients with nonmyeloid malignancies undergoing myeloablative chemotherapy followed by bone marrow transplantation.
Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and TherapyZARXIO is indicated for the mobilization of autologous hematopoietic progenitor cells into the peripheral blood for collection by leukapheresis.
Patients with Severe Chronic NeutropeniaZARXIO is indicated for chronic administration to reduce the incidence and duration of sequelae of neutropenia (e.g., fever, infections, oropharyngeal ulcers) in symptomatic patients with congenital neutropenia, cyclic neutropenia, or idiopathic neutropenia.
ZARXIO® (filgrastim-sndz) Shares the Following 5 Indications With Neupogen® (filgrastim)3,6
Important Safety InformationWARNINGS AND PRECAUTIONS (cont’d)• Thrombocytopenia has been reported in patients receiving filgrastim products.
Monitor platelet counts.
• Leukocytosis:
º Patients with Cancer Receiving Myelosuppressive Chemotherapy: White blood cell counts of 100‚000/mm3 or greater were observed in approximately 2% of patients receiving filgrastim at dosages above 5 mcg/kg/day. In patients with cancer receiving ZARXIO as an adjunct to myelosuppressive chemotherapy‚ to avoid the potential risks of excessive leukocytosis‚ it is recommended that ZARXIO therapy be discontinued if the ANC surpasses 10‚000/mm3 after the chemotherapy-induced ANC nadir has occurred. Monitor CBCs at least twice weekly during therapy.
º Peripheral Blood Progenitor Cell (PBPC) Collection and Therapy: During the period of administration of ZARXIO for PBPC mobilization in patients with cancer, discontinue ZARXIO if the leukocyte count rises to >100,000/mm3.
• Cutaneous vasculitis has been reported in patients treated with filgrastim products. In most cases‚ the severity of cutaneous vasculitis was moderate or severe. Most of the reports involved patients with SCN receiving long-term filgrastim therapy. Hold ZARXIO therapy in patients with cutaneous vasculitis. ZARXIO may be started at a reduced dose when the symptoms resolve and the ANC has decreased.
$0 $10out-of-pocket for fi rst dose or cycle
out-of-pocket forsubsequent doses or cycles
• For eligible commercially insured patients
• No income eligibility requirements
Program Eligibility Requirements:• Maximum benefi t of $10,000 annually
• ZARXIO prescription must be for an approved indication
• This program is not health insurance. This program is for insured patients only; cash-paying or uninsured patients are not eligible
• Patients are not eligible if prescriptions are paid, in whole or in part, by any state or federally funded programs including, but not limited to, Medicare (including Part D, even in the coverage gap), Medicaid, Medigap, VA, DOD, TriCare, private indemnity, HMO insurance plans that reimburse the patient for the entire cost of their prescription drugs, or where prohibited by law
• Co-Pay Program may apply to out-of-pocket expenses that occurred within 120 days prior to the date of the enrollment
• Patients can participate for a maximum of 12 months
• Co-Pay Program may not be combined with any other rebate, coupon, or offer
• Sandoz reserves the right to rescind, revoke, or amend this offer without further notice
Commercial Co-Pay Program forZARXIO® (fi lgrastim-sndz)
Please see Important Safety Information throughoutand accompanying full Prescribing Information.
ZARXIO is a registered trademark of Novartis AG.Sandoz One Source is a trademark of Novartis AG.
Important Safety InformationCONTRAINDICATIONS• ZARXIO is contraindicated in patients with a history of serious allergic reactions to human
granulocyte colony-stimulating factors such as filgrastim or pegfilgrastim products.
WARNINGS AND PRECAUTIONS• Splenic rupture, including fatal cases, has been reported following the administration of
filgrastim products. Patients who report left upper abdominal or shoulder pain shouldbe evaluated.
• Acute respiratory distress syndrome (ARDS) has been reported in patients receiving filgrastim products. Patients who develop fever and lung infiltrates or respiratory distress should be evaluated. Discontinue ZARXIO in patients with ARDS.
• Serious allergic reactions, including anaphylaxis, have been reported in patients receiving filgrastim products. The majority of reported events occurred upon initial exposure. Provide symptomatic treatment for allergic reactions. Allergic reactions, including anaphylaxis, in patients receiving filgrastim products can recur within days after the discontinuation of initial anti-allergic treatment. Permanently discontinue ZARXIO in patients with serious allergic reactions.
• Sickle cell crisis, in some cases fatal, has been reported with the use of filgrastim products in patients with sickle cell trait or sickle cell disease.
Supported by the totality of evidence for biosimilarityand the expertise of Sandoz, a Novartis Division2,3
• Approved in the US in 2015
• Approved in Europe in 20094
• More than 7.5 million patient-exposure days outside of the US4
• Confirmed biosimilarity to Neupogen® (filgrastim)1,4,5
Please see additional Important Safety Information throughout and accompanying full Prescribing Information.ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.
ZARXIO shares the following 5 indications with Neupogen®3,6
• Patients with Cancer Receiving Myelosuppressive Chemotherapy
• Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation Chemotherapy
• Patients with Cancer Undergoing Bone Marrow Transplantation
• Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and Therapy
• Patients with Severe Chronic Neutropenia
ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.Sandoz One Source is a trademark of Novartis AG.
© 2017 Sandoz Inc., 100 College Road West, Princeton, NJ 08540 All Rights Reserved. S-ZRX-1341272 03/2017
References: 1. FDA approves first biosimilar product Zarxio [press release]. US Food and Drug Administration; March 6, 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm436648.htm. Accessed March 3, 2017.2. Data on file. Sandoz Inc. Princeton, NJ. 3. ZARXIO Prescribing Information. Sandoz Inc. February 2017. 4. US Food and Drug Administration. Christl L. Overview of the regulatory pathway and FDA’s guidance for the development and approval of biosimilar products in the US (approved in European Union under the trade name Zarzio). 5. Blackwell K, Semiglazov V, Krasnozhon D, et al. Comparison of EP2006, a filgrastim biosimilar, to the reference: a phase III, randomized, double-blind clinical study in the prevention of severe neutropenia in patients with breast cancer receiving myelosuppressive chemotherapy. Ann Oncol. 2015;26(9):1948-1953. http://annonc.oxfordjournals.org/content/26/9/1948.full.pdf. Accessed March 3, 2017. 6. Neupogen® Prescribing Information. Amgen Inc. June 2016. 7. US Department of Health and Human Services; Draft guidance. Applications covered by Section 505(b)(2). Washington, DC: US Dept of Health and Human Services; October 1999. 8. US Department of Health and Human Services. Scientific considerations in demonstrating biosimilarity to a reference product. Washington, DC: US Dept of Health and Human Services; April 2015. 9. US Department of Health and Human Services. Draft guidance. Reference product exclusivity for biological products filed under Section 351(a) of the PHS Act. Washington, DC: US Dept of Health and Human Services; August 2014. 10. Affordable Care Act, Title VII, Biologics Price Competition Innovation Act, Subtitle A, Section 7002. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/ucm216146.pdf. Accessed March 3, 2017. 11. Centers for Medicare & Medicaid Services. Part B biosimilar biological product payment and required modifiers. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Part-B-Drugs/McrPartBDrugAvgSalesPrice/Part-B-Biosimilar-Biological-Product-Payment.html. Accessed March 3, 2017.
TRUST the Totality of Evidence for ZARXIO® (filgrastim-sndz) and the Expertise of Sandoz2,3
For the ZARXIO prefilled syringe, direct administration of less than 0.3 mL is not recommended.3
HCPCS code Q5101 Injection, Filgrastim (G-CSF), Biosimilar, 1 microgram11
Effective January 1, 2016, Corresponding Required Modifier when billing Q5101 for Zarxio is ZA-Novartis/Sandoz11
• As commercial and public payer requirements may vary, providers should verify payer-specific coding requirements and may contact Sandoz One SourceTM for additional reimbursement information
Please see Important Safety Information throughoutand accompanying full Prescribing Information.
Not actual size.
Please see additional Important Safety Information throughout and accompanying full Prescribing Information.ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.UltraSafe Passive is a registered trademark of Safety Syringes, Inc.
ZARXIO is available with a BD UltraSafe Passive® Needle Guard that provides one-handed passive activation.3
ZARXIO is administered by subcutaneous injection, short intravenous infusion(15 to 30 minutes)‚ or continuous intravenous infusion.3
You should not inject a dose of ZARXIO less than 0.3 mL (180 mcg) from a ZARXIO prefilled syringe. A dose less than 0.3 mL cannot be accurately measured using the ZARXIO prefilled syringe3
Important Safety InformationWARNINGS AND PRECAUTIONS (cont’d)• The possibility that ZARXIO acts as a growth factor for any tumor type cannot be
excluded. The safety of filgrastim products in chronic myeloid leukemia (CML) and myelodysplasia has not been established. When ZARXIO is used to mobilize PBPC‚ tumor cells may be released from the marrow and subsequently collected in the leukapheresis product. Available data is limited and inconclusive.
• The safety and efficacy of ZARXIO given simultaneously with cytotoxic chemotherapy have not been established. Do not use ZARXIO in the period 24 hours before through 24 hours after the administration of cytotoxic chemotherapy. The safety and efficacy of ZARXIO have not been evaluated in patients receiving concurrent radiation therapy. Avoid the simultaneous use of ZARXIO with chemotherapy and radiation therapy.
• Increased hematopoietic activity of the bone marrow in response to growth factor therapy has been associated with transient positive bone-imaging changes on nuclear imaging.
Identical Dosing Schedule and Route of Administration to Neupogen®3,6
Dilution for IV Administration3
• If required for IV administration, ZARXIO may be diluted in 5% Dextrose Injection, USP to concentrations of 5 mcg/mL–15 mcg/mL
— ZARXIO diluted to concentrations of 5 mcg/mL–15 mcg/mL should be protected from adsorption to plastic materials by addition of Albumin (Human) to a final concentration of 2 mg/mL
— When diluted in 5% Dextrose Injection, USP, or 5% Dextrose plus Albumin (Human)‚ ZARXIO is compatible with glass, polyvinylchloride, polyolefin, and polypropylene
• Do not dilute with saline at any time, because the product may precipitate
• Diluted ZARXIO solution can be stored at room temperature for up to 24 hours (this time period includes the duration of the infusion)
5
Important Safety InformationADVERSE REACTIONSMost common adverse reactions in patients:
• With nonmyeloid malignancies receiving myelosuppressive anti-cancer drugs (≥ 5% difference in incidence compared to placebo) are thrombocytopenia, nausea, pyrexia, chest pain, pain, fatigue, back pain, arthralgia, bone pain, pain in extremity, dizziness, cough, dyspnea, rash, blood lactate dehydrogenase increased and blood alkaline phosphatase increased
• With AML (≥ 2% difference in incidence) are epistaxis, back pain, pain in extremity, erythema, and rash maculo-papular
• With nonmyeloid malignancies undergoing myeloablative chemotherapy followed by BMT (≥ 5% difference in incidence) are rash and hypersensitivity
• Undergoing peripheral blood progenitor cell mobilization and collection (≥ 5% incidence) are bone pain, pyrexia, blood alkaline phosphatase increased and headache
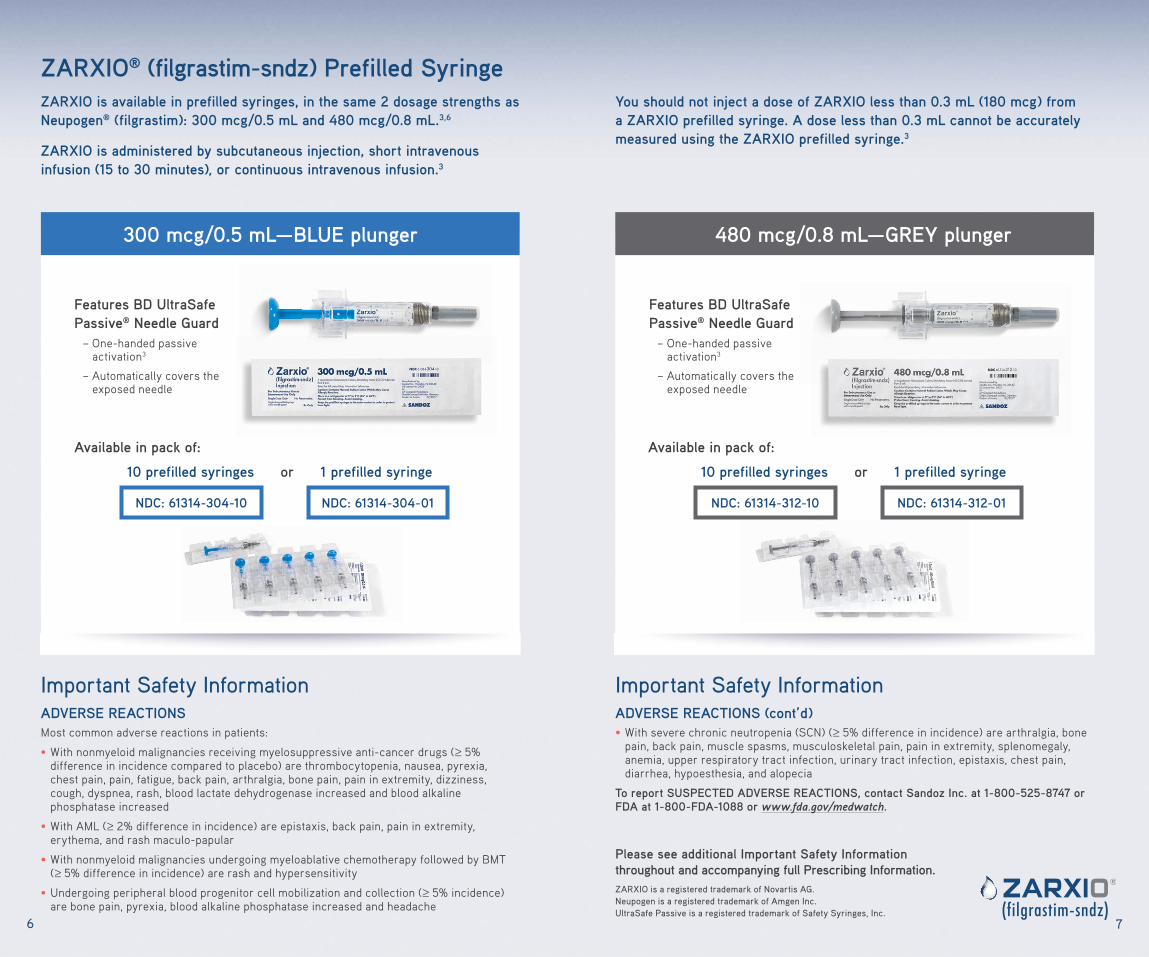
ZARXIO® (filgrastim-sndz) Prefilled SyringeZARXIO is available in prefilled syringes, in the same 2 dosage strengths as Neupogen® (filgrastim): 300 mcg/0.5 mL and 480 mcg/0.8 mL.3,6
ZARXIO is administered by subcutaneous injection, short intravenous infusion (15 to 30 minutes)‚ or continuous intravenous infusion.3
300 mcg/0.5 mL—BLUE plunger
Available in pack of:
10 prefilled syringes or 1 prefilled syringe
NDC: 61314-304-01NDC: 61314-304-10
Features BD UltraSafe Passive® Needle Guard
– One-handed passive activation3
– Automatically covers the exposed needle
6
Please see additional Important Safety Information throughout and accompanying full Prescribing Information.ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.UltraSafe Passive is a registered trademark of Safety Syringes, Inc.
Important Safety InformationADVERSE REACTIONS (cont’d)• With severe chronic neutropenia (SCN) (≥ 5% difference in incidence) are arthralgia, bone
pain, back pain, muscle spasms, musculoskeletal pain, pain in extremity, splenomegaly, anemia, upper respiratory tract infection, urinary tract infection, epistaxis, chest pain, diarrhea, hypoesthesia, and alopecia
To report SUSPECTED ADVERSE REACTIONS, contact Sandoz Inc. at 1-800-525-8747 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
You should not inject a dose of ZARXIO less than 0.3 mL (180 mcg) from a ZARXIO prefilled syringe. A dose less than 0.3 mL cannot be accurately measured using the ZARXIO prefilled syringe.3
480 mcg/0.8 mL—GREY plunger
NDC: 61314-312-01NDC: 61314-312-10
Features BD UltraSafe Passive® Needle Guard
– One-handed passive activation3
– Automatically covers the exposed needle
Available in pack of:
10 prefilled syringes or 1 prefilled syringe
7

PRODUCT ATTRIBUTES
Identical routes of administration
Identical dosing schedules
Identical dosage strengths
ZARXIO3 Neupogen®
(filgrastim)6
To learn more about enrolling your patients, go to www.sandozonesource.com.
94
1
2
3
4
5
Patients with Cancer Receiving Myelosuppressive Chemotherapy ZARXIO is indicated to decrease the incidence of infection‚ as manifested by febrile neutropenia‚ in patients with nonmyeloid malignancies receiving myelosuppressive anti-cancer drugs associated with a significant incidence of severe neutropenia with fever.
Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation ChemotherapyZARXIO is indicated to reduce the time to neutrophil recovery and the duration of fever, following induction or consolidation chemotherapy treatment of patients with acute myeloid leukemia (AML).
Patients with Cancer Undergoing Bone Marrow TransplantationZARXIO is indicated to reduce the duration of neutropenia and neutropenia-related clinical sequelae‚ e.g., febrile neutropenia, in patients with nonmyeloid malignancies undergoing myeloablative chemotherapy followed by bone marrow transplantation.
Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and TherapyZARXIO is indicated for the mobilization of autologous hematopoietic progenitor cells into the peripheral blood for collection by leukapheresis.
Patients with Severe Chronic NeutropeniaZARXIO is indicated for chronic administration to reduce the incidence and duration of sequelae of neutropenia (e.g., fever, infections, oropharyngeal ulcers) in symptomatic patients with congenital neutropenia, cyclic neutropenia, or idiopathic neutropenia.
ZARXIO® (filgrastim-sndz) Shares the Following 5 Indications With Neupogen® (filgrastim)3,6
Important Safety InformationWARNINGS AND PRECAUTIONS (cont’d)• Thrombocytopenia has been reported in patients receiving filgrastim products.
Monitor platelet counts.
• Leukocytosis:
º Patients with Cancer Receiving Myelosuppressive Chemotherapy: White blood cell counts of 100‚000/mm3 or greater were observed in approximately 2% of patients receiving filgrastim at dosages above 5 mcg/kg/day. In patients with cancer receiving ZARXIO as an adjunct to myelosuppressive chemotherapy‚ to avoid the potential risks of excessive leukocytosis‚ it is recommended that ZARXIO therapy be discontinued if the ANC surpasses 10‚000/mm3 after the chemotherapy-induced ANC nadir has occurred. Monitor CBCs at least twice weekly during therapy.
º Peripheral Blood Progenitor Cell (PBPC) Collection and Therapy: During the period of administration of ZARXIO for PBPC mobilization in patients with cancer, discontinue ZARXIO if the leukocyte count rises to >100,000/mm3.
• Cutaneous vasculitis has been reported in patients treated with filgrastim products. In most cases‚ the severity of cutaneous vasculitis was moderate or severe. Most of the reports involved patients with SCN receiving long-term filgrastim therapy. Hold ZARXIO therapy in patients with cutaneous vasculitis. ZARXIO may be started at a reduced dose when the symptoms resolve and the ANC has decreased.
$0 $10out-of-pocket for fi rst dose or cycle
out-of-pocket forsubsequent doses or cycles
• For eligible commercially insured patients
• No income eligibility requirements
Program Eligibility Requirements:• Maximum benefi t of $10,000 annually
• ZARXIO prescription must be for an approved indication
• This program is not health insurance. This program is for insured patients only; cash-paying or uninsured patients are not eligible
• Patients are not eligible if prescriptions are paid, in whole or in part, by any state or federally funded programs including, but not limited to, Medicare (including Part D, even in the coverage gap), Medicaid, Medigap, VA, DOD, TriCare, private indemnity, HMO insurance plans that reimburse the patient for the entire cost of their prescription drugs, or where prohibited by law
• Co-Pay Program may apply to out-of-pocket expenses that occurred within 120 days prior to the date of the enrollment
• Patients can participate for a maximum of 12 months
• Co-Pay Program may not be combined with any other rebate, coupon, or offer
• Sandoz reserves the right to rescind, revoke, or amend this offer without further notice
Commercial Co-Pay Program forZARXIO® (fi lgrastim-sndz)
Please see Important Safety Information throughoutand accompanying full Prescribing Information.
ZARXIO is a registered trademark of Novartis AG.Sandoz One Source is a trademark of Novartis AG.
Important Safety InformationCONTRAINDICATIONS• ZARXIO is contraindicated in patients with a history of serious allergic reactions to human
granulocyte colony-stimulating factors such as filgrastim or pegfilgrastim products.
WARNINGS AND PRECAUTIONS• Splenic rupture, including fatal cases, has been reported following the administration of
filgrastim products. Patients who report left upper abdominal or shoulder pain shouldbe evaluated.
• Acute respiratory distress syndrome (ARDS) has been reported in patients receiving filgrastim products. Patients who develop fever and lung infiltrates or respiratory distress should be evaluated. Discontinue ZARXIO in patients with ARDS.
• Serious allergic reactions, including anaphylaxis, have been reported in patients receiving filgrastim products. The majority of reported events occurred upon initial exposure. Provide symptomatic treatment for allergic reactions. Allergic reactions, including anaphylaxis, in patients receiving filgrastim products can recur within days after the discontinuation of initial anti-allergic treatment. Permanently discontinue ZARXIO in patients with serious allergic reactions.
• Sickle cell crisis, in some cases fatal, has been reported with the use of filgrastim products in patients with sickle cell trait or sickle cell disease.
Supported by the totality of evidence for biosimilarityand the expertise of Sandoz, a Novartis Division2,3
• Approved in the US in 2015
• Approved in Europe in 20094
• More than 7.5 million patient-exposure days outside of the US4
• Confirmed biosimilarity to Neupogen® (filgrastim)1,4,5
Please see additional Important Safety Information throughout and accompanying full Prescribing Information.ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.
ZARXIO shares the following 5 indications with Neupogen®3,6
• Patients with Cancer Receiving Myelosuppressive Chemotherapy
• Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation Chemotherapy
• Patients with Cancer Undergoing Bone Marrow Transplantation
• Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and Therapy
• Patients with Severe Chronic Neutropenia
ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.Sandoz One Source is a trademark of Novartis AG.
© 2017 Sandoz Inc., 100 College Road West, Princeton, NJ 08540 All Rights Reserved. S-ZRX-1341272 03/2017
References: 1. FDA approves first biosimilar product Zarxio [press release]. US Food and Drug Administration; March 6, 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm436648.htm. Accessed March 3, 2017.2. Data on file. Sandoz Inc. Princeton, NJ. 3. ZARXIO Prescribing Information. Sandoz Inc. February 2017. 4. US Food and Drug Administration. Christl L. Overview of the regulatory pathway and FDA’s guidance for the development and approval of biosimilar products in the US (approved in European Union under the trade name Zarzio). 5. Blackwell K, Semiglazov V, Krasnozhon D, et al. Comparison of EP2006, a filgrastim biosimilar, to the reference: a phase III, randomized, double-blind clinical study in the prevention of severe neutropenia in patients with breast cancer receiving myelosuppressive chemotherapy. Ann Oncol. 2015;26(9):1948-1953. http://annonc.oxfordjournals.org/content/26/9/1948.full.pdf. Accessed March 3, 2017. 6. Neupogen® Prescribing Information. Amgen Inc. June 2016. 7. US Department of Health and Human Services; Draft guidance. Applications covered by Section 505(b)(2). Washington, DC: US Dept of Health and Human Services; October 1999. 8. US Department of Health and Human Services. Scientific considerations in demonstrating biosimilarity to a reference product. Washington, DC: US Dept of Health and Human Services; April 2015. 9. US Department of Health and Human Services. Draft guidance. Reference product exclusivity for biological products filed under Section 351(a) of the PHS Act. Washington, DC: US Dept of Health and Human Services; August 2014. 10. Affordable Care Act, Title VII, Biologics Price Competition Innovation Act, Subtitle A, Section 7002. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/ucm216146.pdf. Accessed March 3, 2017. 11. Centers for Medicare & Medicaid Services. Part B biosimilar biological product payment and required modifiers. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Part-B-Drugs/McrPartBDrugAvgSalesPrice/Part-B-Biosimilar-Biological-Product-Payment.html. Accessed March 3, 2017.
TRUST the Totality of Evidence for ZARXIO® (filgrastim-sndz) and the Expertise of Sandoz2,3
For the ZARXIO prefilled syringe, direct administration of less than 0.3 mL is not recommended.3
HCPCS code Q5101 Injection, Filgrastim (G-CSF), Biosimilar, 1 microgram11
Effective January 1, 2016, Corresponding Required Modifier when billing Q5101 for Zarxio is ZA-Novartis/Sandoz11
• As commercial and public payer requirements may vary, providers should verify payer-specific coding requirements and may contact Sandoz One SourceTM for additional reimbursement information
Please see Important Safety Information throughoutand accompanying full Prescribing Information.
Patient Support ServicesSandoz One Source is a comprehensive program designed to simplify and support patient access. Sandoz One Source offers a variety of customized services for patients, including:
• General payer policy information
• Comprehensive insurance verifi cations
• Claims tracking
• Alternate coverage options
• Commercial Co-Pay Program
• Billing and coding
• Prior authorization information
• Denials/Appeals
• External resources information
• Patient Assistance Program (PAP) requests
CONTACT SANDOZ ONE SOURCE
Please see Co-Pay Program eligibility requirements on right.
8
PO Box 220188 Charlotte, NC28222-0188
Address
www.sandozonesource.com
Online
1-844-726-3695
FaxPhone
1-844-SANDOZ1(1-844-726-3691)
M-F 9AM to 8PM ET

PRODUCT ATTRIBUTES
Identical routes of administration
Identical dosing schedules
Identical dosage strengths
ZARXIO3 Neupogen®
(filgrastim)6
To learn more about enrolling your patients, go to www.sandozonesource.com.
94
1
2
3
4
5
Patients with Cancer Receiving Myelosuppressive Chemotherapy ZARXIO is indicated to decrease the incidence of infection‚ as manifested by febrile neutropenia‚ in patients with nonmyeloid malignancies receiving myelosuppressive anti-cancer drugs associated with a significant incidence of severe neutropenia with fever.
Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation ChemotherapyZARXIO is indicated to reduce the time to neutrophil recovery and the duration of fever, following induction or consolidation chemotherapy treatment of patients with acute myeloid leukemia (AML).
Patients with Cancer Undergoing Bone Marrow TransplantationZARXIO is indicated to reduce the duration of neutropenia and neutropenia-related clinical sequelae‚ e.g., febrile neutropenia, in patients with nonmyeloid malignancies undergoing myeloablative chemotherapy followed by bone marrow transplantation.
Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and TherapyZARXIO is indicated for the mobilization of autologous hematopoietic progenitor cells into the peripheral blood for collection by leukapheresis.
Patients with Severe Chronic NeutropeniaZARXIO is indicated for chronic administration to reduce the incidence and duration of sequelae of neutropenia (e.g., fever, infections, oropharyngeal ulcers) in symptomatic patients with congenital neutropenia, cyclic neutropenia, or idiopathic neutropenia.
ZARXIO® (filgrastim-sndz) Shares the Following 5 Indications With Neupogen® (filgrastim)3,6
Important Safety InformationWARNINGS AND PRECAUTIONS (cont’d)• Thrombocytopenia has been reported in patients receiving filgrastim products.
Monitor platelet counts.
• Leukocytosis:
º Patients with Cancer Receiving Myelosuppressive Chemotherapy: White blood cell counts of 100‚000/mm3 or greater were observed in approximately 2% of patients receiving filgrastim at dosages above 5 mcg/kg/day. In patients with cancer receiving ZARXIO as an adjunct to myelosuppressive chemotherapy‚ to avoid the potential risks of excessive leukocytosis‚ it is recommended that ZARXIO therapy be discontinued if the ANC surpasses 10‚000/mm3 after the chemotherapy-induced ANC nadir has occurred. Monitor CBCs at least twice weekly during therapy.
º Peripheral Blood Progenitor Cell (PBPC) Collection and Therapy: During the period of administration of ZARXIO for PBPC mobilization in patients with cancer, discontinue ZARXIO if the leukocyte count rises to >100,000/mm3.
• Cutaneous vasculitis has been reported in patients treated with filgrastim products. In most cases‚ the severity of cutaneous vasculitis was moderate or severe. Most of the reports involved patients with SCN receiving long-term filgrastim therapy. Hold ZARXIO therapy in patients with cutaneous vasculitis. ZARXIO may be started at a reduced dose when the symptoms resolve and the ANC has decreased.
$0 $10out-of-pocket for fi rst dose or cycle
out-of-pocket forsubsequent doses or cycles
• For eligible commercially insured patients
• No income eligibility requirements
Program Eligibility Requirements:• Maximum benefi t of $10,000 annually
• ZARXIO prescription must be for an approved indication
• This program is not health insurance. This program is for insured patients only; cash-paying or uninsured patients are not eligible
• Patients are not eligible if prescriptions are paid, in whole or in part, by any state or federally funded programs including, but not limited to, Medicare (including Part D, even in the coverage gap), Medicaid, Medigap, VA, DOD, TriCare, private indemnity, HMO insurance plans that reimburse the patient for the entire cost of their prescription drugs, or where prohibited by law
• Co-Pay Program may apply to out-of-pocket expenses that occurred within 120 days prior to the date of the enrollment
• Patients can participate for a maximum of 12 months
• Co-Pay Program may not be combined with any other rebate, coupon, or offer
• Sandoz reserves the right to rescind, revoke, or amend this offer without further notice
Commercial Co-Pay Program forZARXIO® (fi lgrastim-sndz)
Please see Important Safety Information throughoutand accompanying full Prescribing Information.
ZARXIO is a registered trademark of Novartis AG.Sandoz One Source is a trademark of Novartis AG.
Important Safety InformationCONTRAINDICATIONS• ZARXIO is contraindicated in patients with a history of serious allergic reactions to human
granulocyte colony-stimulating factors such as filgrastim or pegfilgrastim products.
WARNINGS AND PRECAUTIONS• Splenic rupture, including fatal cases, has been reported following the administration of
filgrastim products. Patients who report left upper abdominal or shoulder pain shouldbe evaluated.
• Acute respiratory distress syndrome (ARDS) has been reported in patients receiving filgrastim products. Patients who develop fever and lung infiltrates or respiratory distress should be evaluated. Discontinue ZARXIO in patients with ARDS.
• Serious allergic reactions, including anaphylaxis, have been reported in patients receiving filgrastim products. The majority of reported events occurred upon initial exposure. Provide symptomatic treatment for allergic reactions. Allergic reactions, including anaphylaxis, in patients receiving filgrastim products can recur within days after the discontinuation of initial anti-allergic treatment. Permanently discontinue ZARXIO in patients with serious allergic reactions.
• Sickle cell crisis, in some cases fatal, has been reported with the use of filgrastim products in patients with sickle cell trait or sickle cell disease.
Supported by the totality of evidence for biosimilarityand the expertise of Sandoz, a Novartis Division2,3
• Approved in the US in 2015
• Approved in Europe in 20094
• More than 7.5 million patient-exposure days outside of the US4
• Confirmed biosimilarity to Neupogen® (filgrastim)1,4,5
Please see additional Important Safety Information throughout and accompanying full Prescribing Information.ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.
ZARXIO shares the following 5 indications with Neupogen®3,6
• Patients with Cancer Receiving Myelosuppressive Chemotherapy
• Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation Chemotherapy
• Patients with Cancer Undergoing Bone Marrow Transplantation
• Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and Therapy
• Patients with Severe Chronic Neutropenia
ZARXIO is a registered trademark of Novartis AG.Neupogen is a registered trademark of Amgen Inc.Sandoz One Source is a trademark of Novartis AG.
© 2017 Sandoz Inc., 100 College Road West, Princeton, NJ 08540 All Rights Reserved. S-ZRX-1341272 03/2017
References: 1. FDA approves first biosimilar product Zarxio [press release]. US Food and Drug Administration; March 6, 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm436648.htm. Accessed March 3, 2017.2. Data on file. Sandoz Inc. Princeton, NJ. 3. ZARXIO Prescribing Information. Sandoz Inc. February 2017. 4. US Food and Drug Administration. Christl L. Overview of the regulatory pathway and FDA’s guidance for the development and approval of biosimilar products in the US (approved in European Union under the trade name Zarzio). 5. Blackwell K, Semiglazov V, Krasnozhon D, et al. Comparison of EP2006, a filgrastim biosimilar, to the reference: a phase III, randomized, double-blind clinical study in the prevention of severe neutropenia in patients with breast cancer receiving myelosuppressive chemotherapy. Ann Oncol. 2015;26(9):1948-1953. http://annonc.oxfordjournals.org/content/26/9/1948.full.pdf. Accessed March 3, 2017. 6. Neupogen® Prescribing Information. Amgen Inc. June 2016. 7. US Department of Health and Human Services; Draft guidance. Applications covered by Section 505(b)(2). Washington, DC: US Dept of Health and Human Services; October 1999. 8. US Department of Health and Human Services. Scientific considerations in demonstrating biosimilarity to a reference product. Washington, DC: US Dept of Health and Human Services; April 2015. 9. US Department of Health and Human Services. Draft guidance. Reference product exclusivity for biological products filed under Section 351(a) of the PHS Act. Washington, DC: US Dept of Health and Human Services; August 2014. 10. Affordable Care Act, Title VII, Biologics Price Competition Innovation Act, Subtitle A, Section 7002. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/ucm216146.pdf. Accessed March 3, 2017. 11. Centers for Medicare & Medicaid Services. Part B biosimilar biological product payment and required modifiers. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Part-B-Drugs/McrPartBDrugAvgSalesPrice/Part-B-Biosimilar-Biological-Product-Payment.html. Accessed March 3, 2017.
TRUST the Totality of Evidence for ZARXIO® (filgrastim-sndz) and the Expertise of Sandoz2,3
For the ZARXIO prefilled syringe, direct administration of less than 0.3 mL is not recommended.3
HCPCS code Q5101 Injection, Filgrastim (G-CSF), Biosimilar, 1 microgram11
Effective January 1, 2016, Corresponding Required Modifier when billing Q5101 for Zarxio is ZA-Novartis/Sandoz11
• As commercial and public payer requirements may vary, providers should verify payer-specific coding requirements and may contact Sandoz One SourceTM for additional reimbursement information
Please see Important Safety Information throughoutand accompanying full Prescribing Information.
![HIGHLIGHTS OF PRESCRIBING INFORMATION These …Recommend stopping ZARXIO if the ANC increases beyond 10‚000/mm 3 [see Warnings and Precautions (5.10)]. Administer ZARXIO at least](https://static.fdocuments.us/doc/165x107/5e421cabb275d37aa00d8d49/highlights-of-prescribing-information-these-recommend-stopping-zarxio-if-the-anc.jpg)

















