
3 Literature Review
53
Chapter 3 Review of literature CHAPTER-3 REVIEW OF LITERATURE 3.1 Hyperlipidemia Hyperlipidemia refers to elevated levels of lipids and cholesterol in the blood and is also identified as dyslipidemia to describe the manifestations of different disorders of lipoprotein metabolism. Alteration and/or abnormality in the metabolism of lipid and lipoproteins is a very common condition that taken place within general population and it consider as one of the main risk factor in the incidence of cardiovascular disease due to their influence on atherosclerosis .11 Critical Factors that Play Role in Hyperlipidemia Incidence There are several factors which play significant role in the incidence of this medical problem like family history, Chronic diseases (diabetes mellitus, renal failure, nephritic syndrome and hypothyroidism), alcoholism and smoking, obesity and unhealthy diets intake .12 3.1.1 Classifications of Hyperlipidemia Besides the above classifications i.e., primary and secondary hyperlipidemia subtypes, hyperlipidemia also classified according to the type of lipid elevated which is hypercholesterolemia, hypertriglyceridemia or both in combined hyperlipidemia. Department of Pharmacolgy Page 7
-
Upload
bowjanku-amulya-b -
Category
Documents
-
view
30 -
download
0
description
litreature survey
Transcript of 3 Literature Review

Chapter 3 Review of literature
CHAPTER-3
REVIEW OF LITERATURE
3.1 Hyperlipidemia
Hyperlipidemia refers to elevated levels of lipids and cholesterol in the blood
and is also identified as dyslipidemia to describe the manifestations of different
disorders of lipoprotein metabolism. Alteration and/or abnormality in the metabolism of
lipid and lipoproteins is a very common condition that taken place within general
population and it consider as one of the main risk factor in the incidence of
cardiovascular disease due to their influence on atherosclerosis.11
Critical Factors that Play Role in Hyperlipidemia Incidence
There are several factors which play significant role in the incidence of this
medical problem like family history, Chronic diseases (diabetes mellitus, renal failure,
nephritic syndrome and hypothyroidism), alcoholism and smoking, obesity and
unhealthy diets intake.12
3.1.1 Classifications of Hyperlipidemia
Besides the above classifications i.e., primary and secondary hyperlipidemia
subtypes, hyperlipidemia also classified according to the type of lipid elevated which is
hypercholesterolemia, hypertriglyceridemia or both in combined hyperlipidemia.
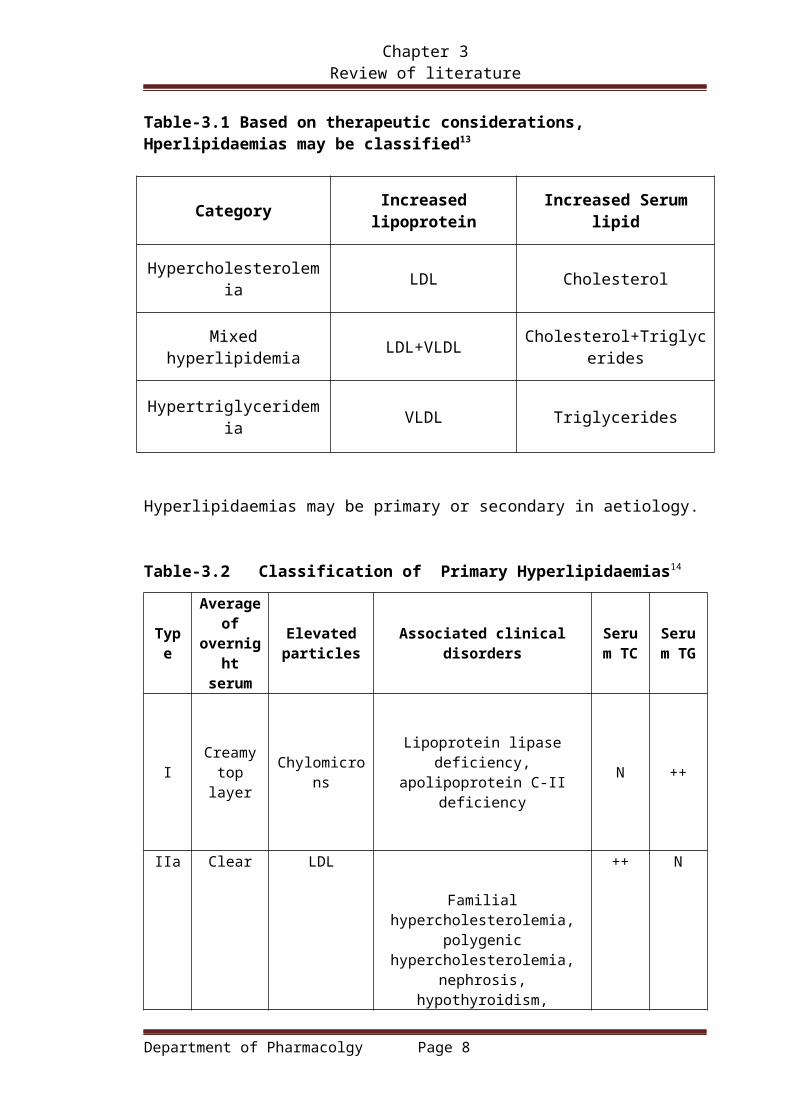
Table-3.1 Based on therapeutic considerations, Hperlipidaemias may be classified13
Category Increased lipoprotein Increased Serum lipid
Hypercholesterolemia LDL Cholesterol
Mixed hyperlipidemia LDL+VLDL Cholesterol+Triglycerides
Hypertriglyceridemia VLDL Triglycerides
Department of Pharmacolgy Page 7
Chapter 3 Review of literature
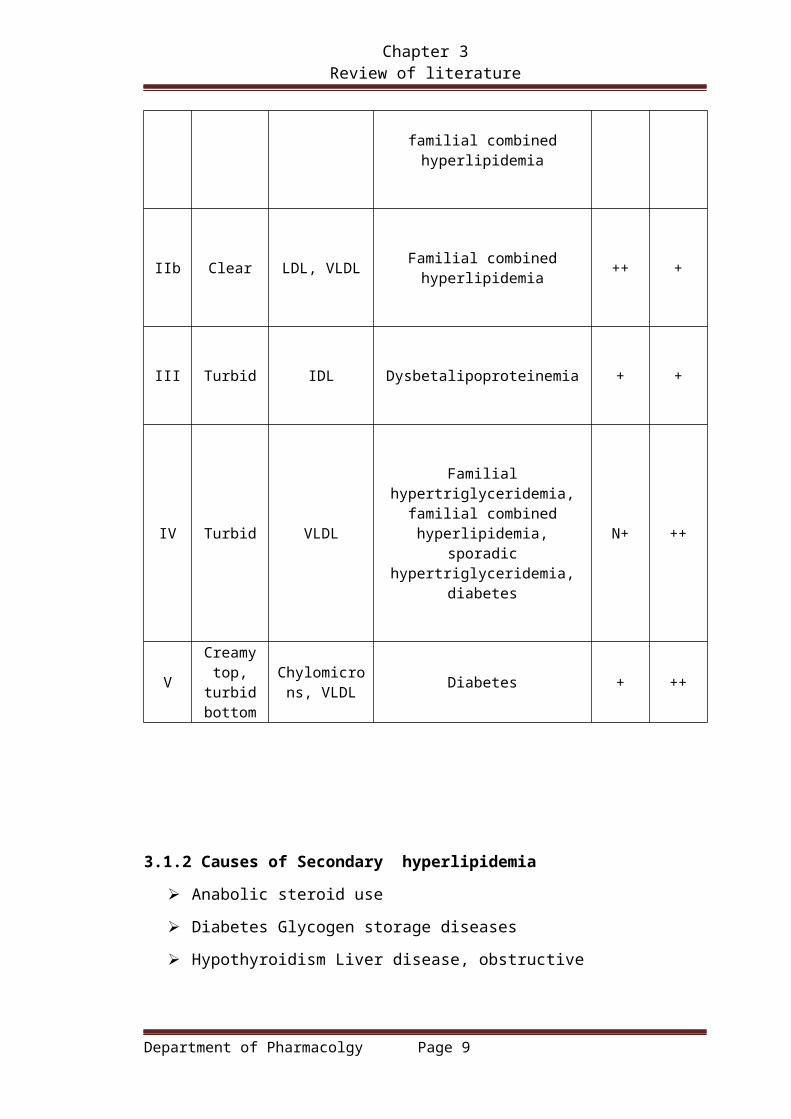
Hyperlipidaemias may be primary or secondary in aetiology.
Table-3.2 Classification of Primary Hyperlipidaemias14
Type
Average of
overnight serum
Elevated particles
Associated clinical disordersSerum
TCSerum
TG
ICreamy top layer
ChylomicronsLipoprotein lipase deficiency, apolipoprotein C-II deficiency
N ++
IIa Clear LDL
Familial hypercholesterolemia, polygenic hypercholesterolemia,
nephrosis, hypothyroidism, familial combined hyperlipidemia
++ N
IIb Clear LDL, VLDL Familial combined hyperlipidemia ++ +
III Turbid IDL Dysbetalipoproteinemia + +
IV Turbid VLDL
Familial hypertriglyceridemia, familial combined hyperlipidemia,
sporadic hypertriglyceridemia, diabetes
N+ ++
VCreamy
top, turbid bottom
Chylomicrons, VLDL
Diabetes + ++
3.1.2 Causes of Secondary hyperlipidemia
Anabolic steroid use
Department of Pharmacolgy Page 8
Chapter 3 Review of literature
Diabetes Glycogen storage diseases
Hypothyroidism Liver disease, obstructive
Medications: corticosteroids, bile acid-binding resins, anticonvulsants,
Certain oral contraceptives, Accutane® (isotretinoin), Depo-provera®
Overweight or obesity
Renal diseases
Therapeutic diet: ketogenic; high carbohydrate
3.2 Lipids
Lipids are a heterogeneous group of compounds, including fats, oils, steroids,
wax and related compounds, which are related more by their physical than by
their chemical properties. Lipids may be regarded as organic substances
relatively insoluble in water, soluble in organic solvents (alcohol, ether etc.)
3.2.1 CLASSIFICATION:16
Lipids are broadly classified into simple, complex and derived, which are
further subdivided into different groups.
1. Simple lipid
2. Compound/complex lipid
Fig-3.1 Classification of lipids
Table 3.3 Etiologies of Hyperlipidemias15
Department of Pharmacolgy Page 9

Chapter 3 Review of literature
Phenotype
Elevated
Particles
Major Lipid
Abnormality Frequency Etiology
IChylomicron
TG Very rare
LPLdeficiency, apoC-
II deficiency LPL eg,
systemic
lupuserythematosus
IIA LDL LDL-C Common
FH, FCH,
polygenic
hypercholesterimia
,hypothyroidism,
IB LDL and
VLDLLDL-C, TG Common Similar to type IIA
HLP
III IDL TC, TG Rare
ApoE-2
homozygosity (E-
2/E-2) plus obesity,
diabetes mellitus,
renal disease,
hypothyroidism, or
IV VLDL TG Common
FCH,FH,metabolien
docrine disease,
renal disease, liver
disease, ethanol
use/abuse,
V
Chylomicron
and VLDL TGUncommon
Usually resultsfrom a
combination of any
twoconditions that
cause type IV HLP
1.Simple lipids: These are esters of fattyacids with various alcohols.
Department of Pharmacolgy Page 10

Chapter 3 Review of literature
(a) fats and oils: Esters of fatty acids with glycerol. The difference between fat
and oil is only physical. Thus, oil is a liquid while fat is a solid at room
temperature.
(b) waxes: Esters of fatty acids(usually long chain)with alcohols other than
glycerol. these alcohols may be aliphatic or alicyclic.
2. Compound/Complex lipid: Esters of fatty acids containing groups in addition to
an alcohol
(a) Phospholipids: Lipids containing, in addition to fatty acids and an alcohol, a
phosphoric acid residue.They frequently have nitrogen containing bases and
other substituents.
b) Glycolipids: Lipids containing a fatty acid, sphingosine, carbohydrate and
nitrogenous base. glycerol and phosphate are absent e.g.cerebrosides,
(c)lipoproteins: macromolecular complexes of lipids with protein.
(d) Other complex lipids : Lipids such as sulfolipids, and amino lipids.
3.precursor and derived lipids: these include fatty acids,glycerol, steroids, other
alcohols, fatty aldehydes and ketone bodies, hydrocarbones, lipid-soluble vitamins and
hormones.
Major lipids found in the blood stream are.16
1. Triglycerides
2. Phospholipids
3. Cholesterol
4. Free fatty acid
3.2.2 Triglycerides17
Triglycerides also know as triacylglycerol or triacylglycerides are glycerides
in which the glycerol is esterified with three fatty acids. They are the main
constituents of vegetable oil and animal fats. They play an important role in the
metabolism as energy source. They contain a bit more than twice as much as energy
9k.cal/gm as carbohydrates and proteins. Triglycerides are water insoluble, non-polar
neutral fats. These fats primarily occur in adipocytes of adipose tissue
predominantly found in the subcutaneous layer and in the abdominal cavity, having
specialized storage of TGs.The fat is stored in the form of globules dispersed in
Department of Pharmacolgy Page 11

Chapter 3 Review of literature
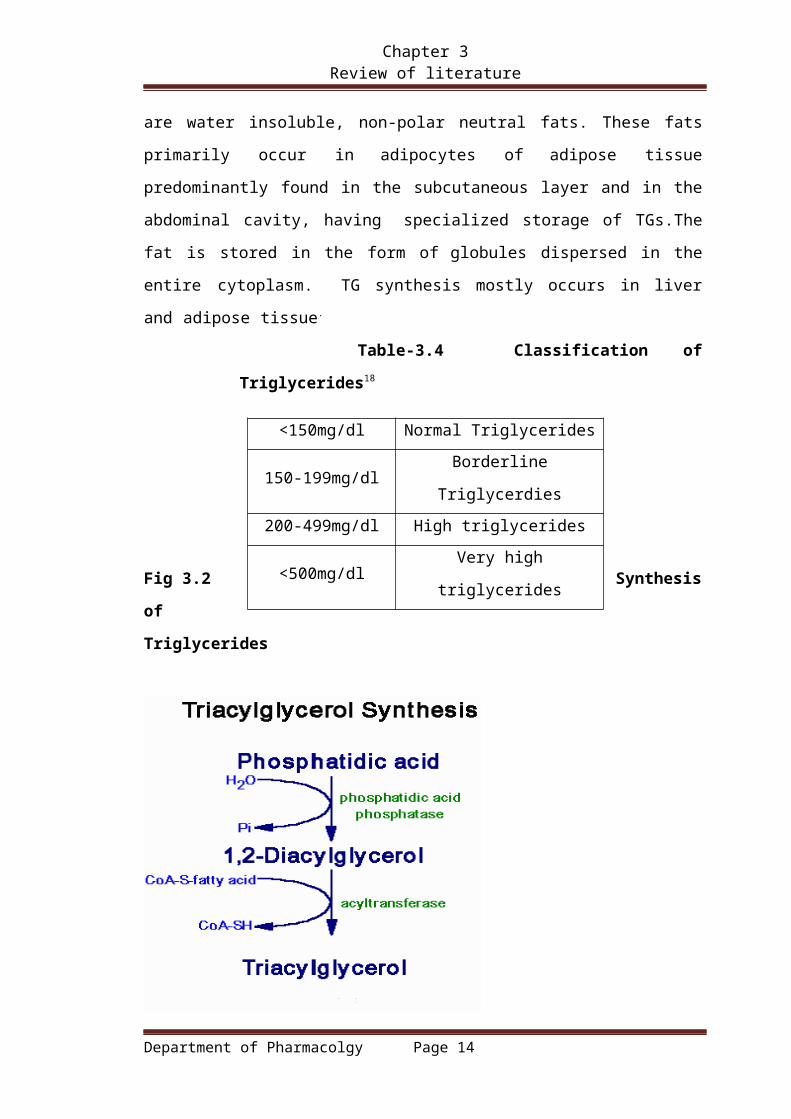
the entire cytoplasm. TG synthesis mostly occurs in liver and adipose tissue.
Table-3.4 Classification of Triglycerides18
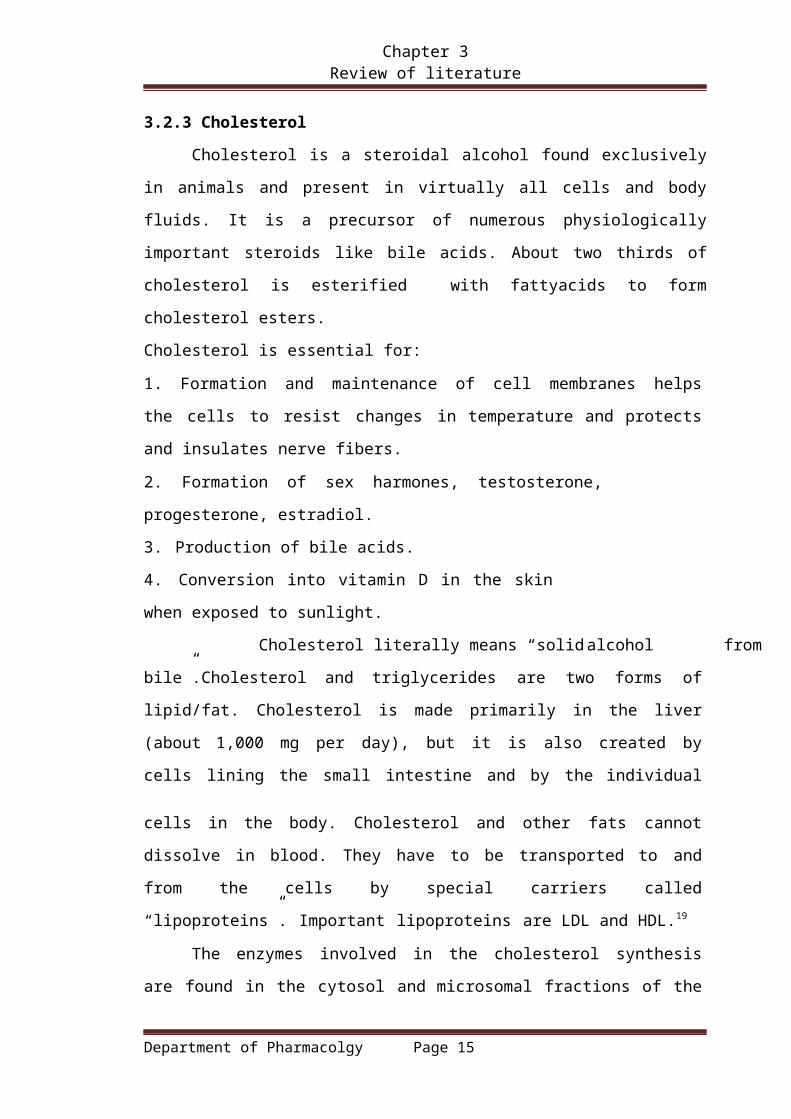
Fig 3.2 Synthesis of Triglycerides
3.2.3 Cholesterol
Cholesterol is a steroidal alcohol found exclusively in animals and present in
virtually all cells and body fluids. It is a precursor of numerous physiologically
important steroids like bile acids. About two thirds of cholesterol is esterified with
fattyacids to form cholesterol esters.
Cholesterol is essential for:
1. Formation and maintenance of cell membranes helps the cells to resist changes
in temperature and protects and insulates nerve fibers.
2. Formation of sex harmones, testosterone, progesterone, estradiol.
3. Production of bile acids.
4. Conversion into vitamin D in the skin when exposed to
sunlight. Cholesterol literally means “solid alcohol from bile”.Cholesterol and
triglycerides are two forms of lipid/fat. Cholesterol is made primarily in the liver
Department of Pharmacolgy Page 12
<150mg/dl Normal Triglycerides
150-199mg/dl Borderline Triglycerdies
200-499mg/dl High triglycerides
<500mg/dl Very high triglycerides

Chapter 3 Review of literature
(about 1,000 mg per day), but it is also created by cells lining the small intestine
and by the individual cells in the body. Cholesterol and other fats cannot dissolve in
blood. They have to be transported to and from the cells by special carriers called
“lipoproteins”. Important lipoproteins are LDL and HDL.19
The enzymes involved in the cholesterol synthesis are found in the cytosol
and microsomal fractions of the cell. Acetate to acetyl Co A provides all the carbon
atoms in the cholesterol. Cholesterol synthesis takes place in 5 stages, which
includes synthesis of HMG CO A, formation of mevalonate (6c), production of
isoprenoid units (5c), synthesis of squalene (30c) and conversion of squalene to
cholesterol (27c).
Cholesterol biosynthesis is controlled by the rate-limiting enzyme HMG
CoA reductase, at the beginning of the pathway, which is found in association with
endoplasmic reticulum and subjected to different metabolic controls like feed back control,
hormonal regulation, inhibition by drugs and inhibition by bile acids.
Table -3.5 Desirable levels of cholesterol
3.2.4 FATTY ACIDS
These are straight-chain carbon compounds of varying lengths. They
may be saturated, containing no double bonds, monounsaturated, with one
double bond, or polyunsaturated, with more than one double bond Fatty
acids can esterify with glycerol to form triglycerides or be non-esterified
(NEFAs) or free. Plasma NEFAs liberated from adipose tissue by lipase
activity are transported to the liver and muscle mainly bound to albumin. The
NEFAs provide a significant proportion of the energy requirements of the
body.20
The fatty acids in the body are mostly oxidized by beta-oxidation which
takes place in 3 stages i.e. activation of fatty acids occurring in the cytosol, transport
of FAs into mitochondria and beta-oxidation in the mitochondrial matrix.
Department of Pharmacolgy Page 13
<200 Desirable
200-239 Boderline high
>240 High
Chapter 3 Review of literature
The dietary carbohydrates and amino acids, when consumed in excess
are converted to FAs and stored as TGs. It occurs predominantly in liver, kidney,
adipose tissue and lactating mammary glands. The enzymes required for fatty acid
synthesis are present in the cytosomal fraction of the cell. Acetyl CoA is the
source of carbon atoms, NADPH provides the reducing equivalent and ATP
supplies energy for fatty acid formation. The synthesis occurs in 3-stages
including production of acetyl CoA and NADPH, conversion of acetyl CoA to
malonyl CoA, reactions of FA synthase complex.
Fig-3.3 Synthesis of cholesterol
3.2.5 PHOSPHOLIPIDS:
Phospholipids are triglycerides that are covalently bonded to a phosphate group
by an ester linkage. The diglyceride is composed of a glycerol backbone that has
esterified to two fattyacids.The hydrocarbon chains are hydrophobic (FAs), the
charges on the phosphate and group make that portion of molecule hydropyllic.The
result is an amphophilic molecule.There are two classes of phospholipids, which
include sphingomyelins where sphingosine as the alcohol and
glycerphospholipids/phosphoglycerides. glycerol is the alcohol.
Department of Pharmacolgy Page 14
Chapter 3 Review of literature
Phospholipids perform important functions including regulating membrane
permeability and in maintaining electron transport chain in mitochondria. Due to
their amphophilic nature, they can combine with polar and non-polar compounds in
the cell. They serve as a precursor for synthesis of eicosanoids, participate in the
reverse cholesterol transport and thus help in the removal of cholesterol from the
body.
They are synthesized from phosphatidic acid and 1, 2-diacyl glycerol, which
are also intermediates in the production of triglycerides. Phospholipid synthesis,
occurs in the endoplasmic reticulum. Lecithin, cephalin, phosphotidyl serine,
phosphotidylinostol, phosphotidylglycerol, are important phospholipids. Phospholipids
are degraded by phospholipases, which cleave the phosphodiester bonds. E.g.:
Phospholipase A1, A3, phospholipase C and phospholipase .
Fig-3.4 Synthesis of phospholipids
Department of Pharmacolgy Page 15
Chapter 3 Review of literature
3.3 LIPPROTEINS
Lipoproteins are the “packages” in which cholesterol and triglycerides (lipids)
are transport through out the body by combining with proteins. Lipoproteins
contain cholesterol, phospholipids and triglycerides at the core and an outer layer of
protein called “apolipoproteins/apoproteins”. The lipid constituents are water
insoluble and apoproteins are water soluble.21
Dependining upon their lipid carrying capacity Lipoproteins are classified
into clases
1. Chylomicrons
2. LDL (Low-density lipoproteins)
3. VLDL (very low-density lipoproteins)
Department of Pharmacolgy Page 16

Chapter 3 Review of literature
4. IDL (Intermediate density lipoproteins)
5. HDL (High-density lipoprotein)
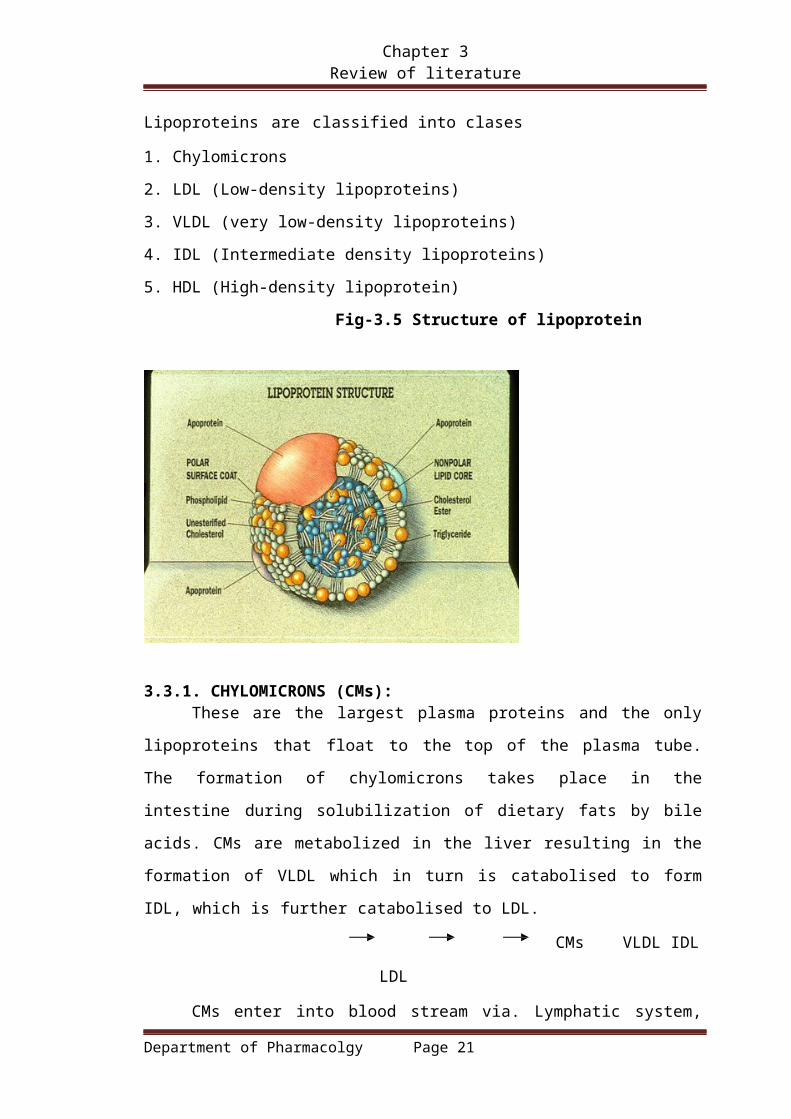
Fig-3.5 Structure of lipoprotein
3.3.1. CHYLOMICRONS (CMs):These are the largest plasma proteins and the only lipoproteins that float to
the top of the plasma tube. The formation of chylomicrons takes place in the
intestine during solubilization of dietary fats by bile acids. CMs are metabolized in the
liver resulting in the formation of VLDL which in turn is catabolised to form IDL,
which is further catabolised to LDL.
CMs VLDL IDL LDL
CMs enter into blood stream via. Lymphatic system, where they acquire apo
c-II and apoE from plasma HDL. The apoC II in CMs activates LPL in the
presence of phospholipids. This LPL removes fatty acids of CMs from triglycerides.
A progressive decrease in particle diameter occurs as triglycerides in the core are
depleted and small apoproteins are transported to HDL. The resultant CM remnants
are taken up by receptor-mediated endocytosis, as into hepatocytes. The
concentration of CMs can be controlled only by reducing dietary fat consumption.
There is no current therapeutic approach that will enhance CM catabolism except
for insulin replacement in patients with type–I diabetis. CMs function to deliver
dietary TGs to adipose tissue and muscle and dietary cholesterol
to liver.
Department of Pharmacolgy Page 17

Chapter 3 Review of literature
Fig-3.6 Chylomcron structure
3.3.2. VERY LOW DENSITY LIPOPROTEINS (VLDLs):VLDLs are the next in size to CMs, which are responsible to carry
endogenous TGs from the liver into the blood stream to other parts. They contain
TGs, cholesterol esters, phospholipids and apoproteins. Like nascent CMs, newly
released VLDL acquires apo C and apo E from circulating HDLs.
Lipoprotein lipase (LPL) located on capillary endothelial cell surface
catalyses the release of fatty acids portion of VLDL to adipose tissue and muscle in
the same way as CMs. The action of LPL converts VLDL to intermediate density
lipoproteins (IDLs), also termed as VLDL remnants. The further losses of TGs in
IDLs by hepatic glyceride hydrolase lipase results in the generation of LDL. The
apo Cs are converted to HDLs.
Apo E plays an important role in the metabolism of TG rich
lipoproteins CMs, CM remnants, VLDL and IDL and has number of functions
related to the binding and uptake of plasma proteins. In transgenic mice, over
expression of apo E by macrophages inhibits hypercholesterolemia-induced
atherosclerosis.22
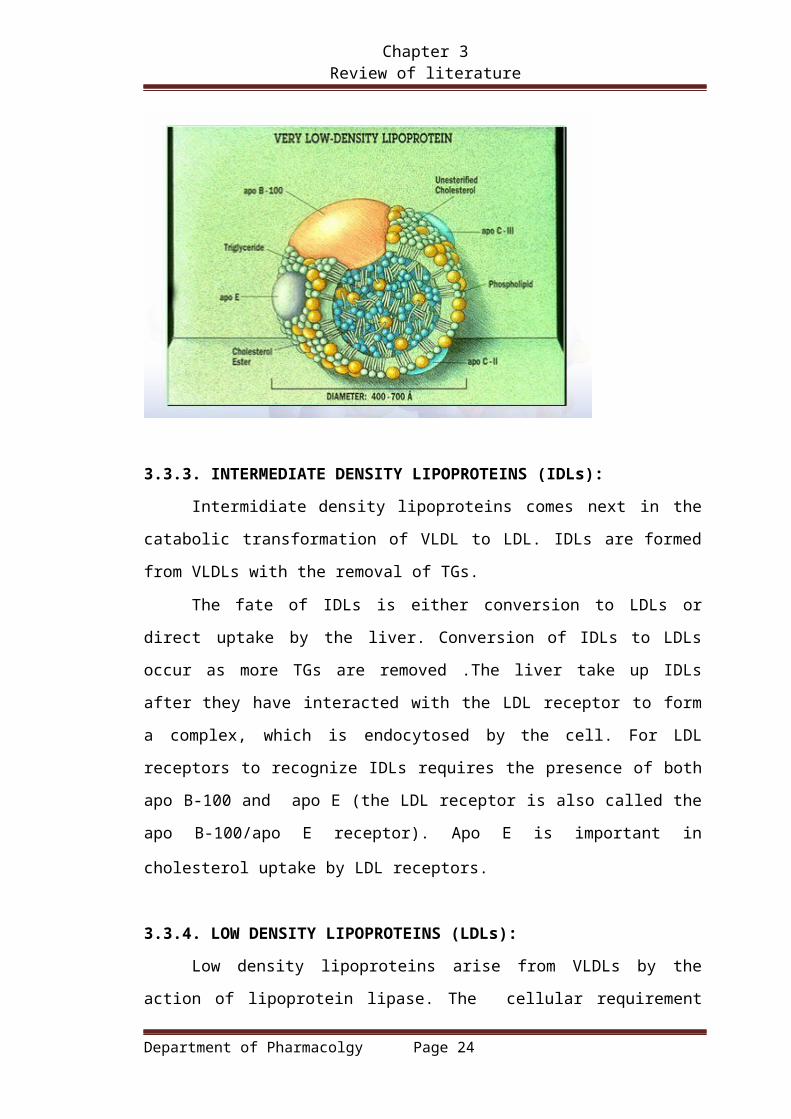
Fig-3.7 Very low density lipoprotein
Department of Pharmacolgy Page 18

Chapter 3 Review of literature
3.3.3. INTERMEDIATE DENSITY LIPOPROTEINS (IDLs):
Intermidiate density lipoproteins comes next in the catabolic transformation
of VLDL to LDL. IDLs are formed from VLDLs with the removal of TGs.
The fate of IDLs is either conversion to LDLs or direct uptake by the
liver. Conversion of IDLs to LDLs occur as more TGs are removed .The liver take up
IDLs after they have interacted with the LDL receptor to form a complex, which is
endocytosed by the cell. For LDL receptors to recognize IDLs requires the presence
of both apo B-100 and apo E (the LDL receptor is also called the apo B-100/apo E
receptor). Apo E is important in cholesterol uptake by LDL receptors.
3.3.4. LOW DENSITY LIPOPROTEINS (LDLs):
Low density lipoproteins arise from VLDLs by the action of lipoprotein lipase.
The cellular requirement for cholesterol as a membrane component is satisfied by
CMs and LDLs. LDLs is the primary plasma carriers of cholesterol for delivery to all
tissues .It contain 60-70% total cholesterol.
The apoprotein of LDL is apoB-100.LDLs is taken up by cells via. LDL
receptor- mediated endocytosis, as described above for IDL uptake. The uptake of
LDLs occurs predominantly in liver 75%,adrenals and adipose tissue. As with IDLs,
the interaction of LDL with LDL-receptors requires the presence of apo B-100.The
endocytosed membrane vesicles endosomes fuse with lysosomes, in which the
apoprotein are degraded and the cholesterol esters hydrolyzed to yield free
Department of Pharmacolgy Page 19

Chapter 3 Review of literature
cholesterol. The cholesterol is then incorporated into the plasma membranes as
necessary. Excess intracellular cholesterol is re-esterified by acyl -Co A-cholesterol
acyl transferase ACAT, for intracellular storage.23
Insulin and Tri-iodothyronine( T3) increases the binding of LDL to liver
cells, where as glucocorticoids has opposite effect. The precise mechanism for this
effect in not clear but may be mediated through the regulation of apoB degradation.
The effects of insulin and T3 on hepatic LDL binding may explain the
hypercholesterolemia and increased risk of atherosclerosis that have been shown to
be associated with uncontrolled diabetes or hypothyroidism.
An abnormal form of LDL, identified as “lipoprotein-x Lp-x” predominates in
the circulation of patients suffering cholestatic liver disease. In this case,there is an
elevation in the level of circulating free cholesterol and phospholipids. LDL often
called as “bad” cholesterol because LDL easily adheres to the wall of arteries, which
leads to initiation of atherogenic process.24
3.3.5 High density lipoproteins(HDL-C)
High density lipoprotein is the smallest lipoprotein. It contains 20-30% of
person’s total cholesterol. HDL is often called “good cholesterol” which finds and
removes, stuck LDL at the apo B and E receptors of peripheral cells and brings them
back to the liver, where they get discarded. HDLs are synthesized in the liver and
small intestine, as primarily protein rich disc shaped particles. The newly formed
HDLs are devoid of any cholesterol and cholesterol esters.
The primary apoproteins of HDL are apoA-1, apoC-1, apoC-11and apo E.
Infact, the major function of HDL is to act as circulating stores of apoC-1, apoC-11
and apoE. HDLs are converted into spherical lipoproteins particles through
accumulation of cholesterylesters. The accumulation converts HDLs to HDL2 and
HDL3. Any free cholesterol present in CM remnant and VLDLremnants can be
esterified through the action of Lecithin cholesterol acyl transferase(LCAT). LCAT is
synthesized in liver and so named because it transfers a fattyacid from the C-2
position of lecithin to the C-3OH of cholesterol, generating a cholesteryl ester and
lysolecithin. The activity of LCAT requires interaction with apoA-1, which is found on
the surface of HDLs.25
Cholesterol rich HDLs return to liver, where they are endocytosed. Hepatic
Department of Pharmacolgy Page 20
Chapter 3 Review of literature
uptake of HDLs or reverse cholesterol transport may be mediated through an HDL-
specific apoA1receptor or through lipid-lipid interactions.HDLs also get cholesterol
from macrophages by the same way. HDLs also acquire cholesterol by extracting it
from cell surface membranes,which lead to lowering of intracellular cholesterol,
since the cholesterol stored within cells as cholesteryl esters will be mobilized to
replace the cholesterol removed from the plasma membrane.
The cholesterol esters of HDLs can also be transferred to VLDLs and
LDLs through the action of HDL-associated enzyme, cholesterol ester transfer
protein CETP. This has the added effect of allowing the excess cellular cholesterol to
be returned to the liver through the LDL-receptor pathway as well as the HDL-receptor
pathway.
3.3.6 [LP (a)]-
[Lp(a)] consists of an LDL-like particle and the specific apolipoprotein(a)
[apo(a)], which is covalently bound to the apoB of the LDL like particle. Lp(a)
accumulates in the vessel wall and inhibits binding of Plasminogen (PLG) to
the cell surface, reducing plasmin generation which increases clotting. This
inhibition of PLG by Lp(a) also promotes proliferation of smooth muscle cells
causing generation of clots and atherosclerosis.
Fig-3.8 Transport of lipoproteins
Department of Pharmacolgy Page 21

Chapter 3 Review of literature
Lipoprotein particles are produced by hepatocytes (liver cells) and enterocytes from
TAG, cholesterol, apolipoproteins, and phospholipids. The hydrophobic TAG and
cholesteryl esters make up the central part, whilst apolipoprotein strands, cholesterol
molecules and phospholipids are located in the outer shells.
Although LDL cholesterol (LDL-C) is associated with an increased risk of coronary
heart disease, other lipoproteins and their constituents, apolipoproteins, may play an
important role in atherosclerosis. Elevated levels of apolipoprotein (apo) B, a
constituent of atherogenic lipoproteins, and reduced levels of apo A-I, a component of
anti-atherogenic HDL, are associated with increased cardiac events. Apo B, apo A-I and
the apo B/apo A-I ratio have been reported as better predictors of cardiovascular events
than LDL-C and they even retain their predictive power in patients receiving lipid-
modifying therapy. Measurement of these apolipoproteins could improve
cardiovascular risk prediction.
Apolipoproteins are protein components found on the outside of the lipoprotein,
which emulsify the lipoprotein particle to make it more stable in aqueous solution for
carriage in plasma. They also interact with cellular receptors that determine how and
where lipoprotein particles are metabolised. Each lipoprotein particle has a specific set
of apolipoproteins. Apolipoproteins are important because they control lipoprotein
metabolism. Apolipoprotein and LDL receptor genes have been identified, sequenced
and mapped to chromosomes. Apolipoprotein disorders are known to lead to defects of
lipid metabolism
The important apolipoproteins are:
ApoA - present in HDLs. The binding of ApoA-I to cellular receptors
mediates the efflux of cholesterol from peripheral cells, and the influx of
cholesterol into hepatocytes.
ApoB - encourages cellular uptake of LDL. ApoB-100 is derived from liver
and forms part of LDL. ApoB-48 is derived from the gut and is found in
chylomicrons.
ApoC - synthesised in the liver and is a peripheral activator of lipoprotein
lipase (LPL). It is transferred between lipoproteins
ApoE - stabilises VLDL for cellular uptake.
Apo(a) - links with aAoB-100 to oxidise LDL, giving Lp(a) lipoprotein
particles.
Department of Pharmacolgy Page 22

Chapter 3 Review of literature
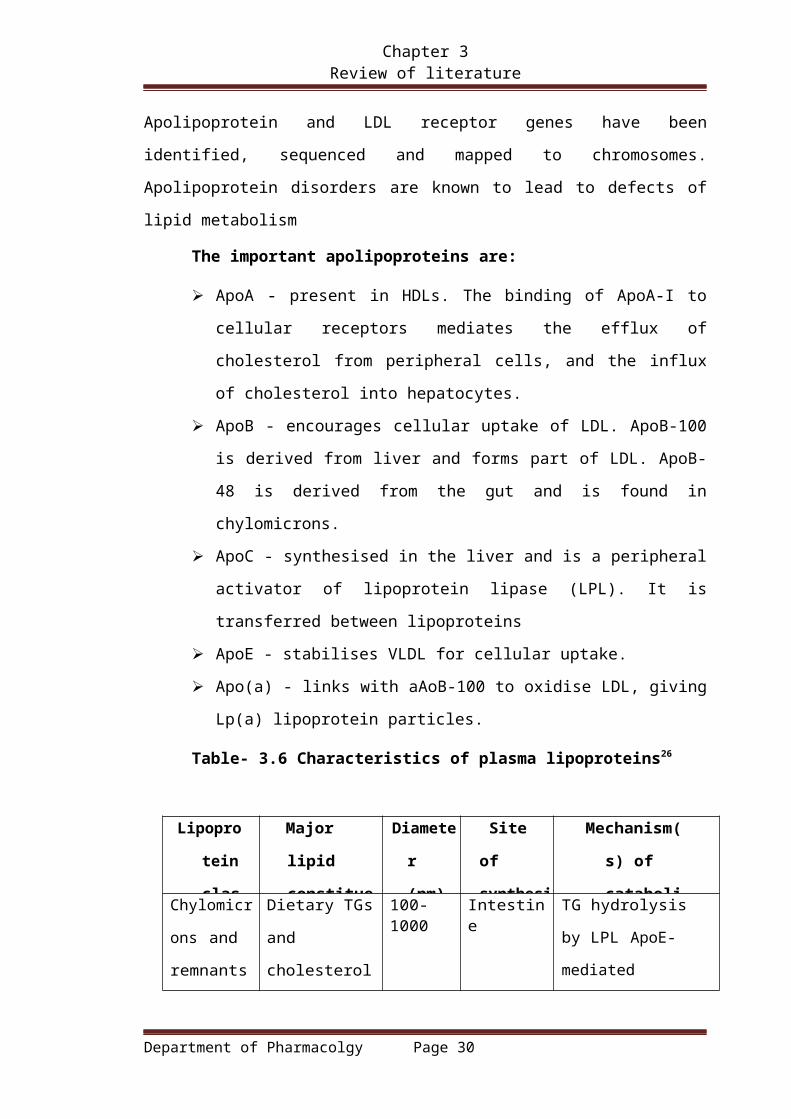
Table- 3.6 Characteristics of plasma lipoproteins26
Lipoprote
in
class
Major lipid
constituent
Diameter
(nm)
Site of
synthesis
Mechanism(s)
of
catabolism
Chylomicrons
and remnants
Dietary TGs and
cholesterol
100-1000 Intestine TG hydrolysis by LPL
ApoE-mediated
remnant uptake by liver
VLDL Endogenous or
hepatic TGs
30–80 Liver TG hydrolysis by LPL
IDL Cholesteryl
esters and
"endogenous"
TGs
25–50 Product of
VLDL
Catabolism
50% converted to
LDL mediated by
HDL, 50% apoE-
mediated uptake by
liverLDL Cholesteryl esters 18–28 Product of
VLDL
Catabolism
ApoB-100-mediated
uptake by LDL
receptor (~75% in
liver)HDL Phospholipids,
cholesteryl esters
5–15 Intestine,
liver, plasma
Transfer of cholesteryl
ester to VLDL and
LDL Uptake of HDL
cholesterol by
hepatocytes
Department of Pharmacolgy Page 23
Chapter 3 Review of literature
3.4 Pathway for lipid transport
Each class of lipoprotein has a specific role in lipid transport, and there
are different pathways for exogenous and for endogenous lipids. The pathways are
distinguished by the main apoproteins that are ligands for the key receptors27.
3.4.1.Exogenous Pathway (From ingested food to intestine to peripheral cells and
Liver):
In the exogenous pathway, cholesterol and TGs absorbed from the ileum are
transported as chylomicrons, in lymph and then blood, to capillaries in muscle and
adipose tissue. Here, TG are hydrolysed by LPL, and the tissues take up the
resulting FFA and glycerol. The chylomicron remnants, still containing their full
complement of cholesteryl esters, pass to the liver, bind to receptors on
hepatocytes and undergo endocytosis. Cholesterol liberated in hepatocytes is
stored, oxidised to bile acids, secreted unaltered in bile, or can enter the endogenous
pathway.
3.4.2 Endogenous Pathway (From liver to peripheral tissues):
In the endogenous pathway cholesterol and newly synthesised TGs are
transported from the liver as VLDL to muscle and adipose tissue, where TG is
hydrolysed to fatty acids and glycerol these enter the tissues. During this process,
the lipoprotein particles become smaller but retain a full complement of
cholesterylesters. Consequently,they increase in density to IDL cholesterol and
ultimately become LDL particles.
Cells take up LDL by endocytosis via LDL receptors. Cholesterol can
return to plasma from the tissues in HDL particles. Cholesterol is esterified with
long-chain fatty acids in HDL particles and the resulting cholesteryl esters are
transferred to VLDL or LDL particles by a transfer protein present in the plasma
known as CETP. Lp(a) contains a unique [apo(a)], with structural similarities to
PLG. Lp(a) competes with and inhibits the binding of PLG to its receptors on
the endothelial cell. PLG is normally the substrate for PLG activator, which is
secreted by and bound to endothelial cells, generating the fibrinolytic enzyme
plasmin.
Department of Pharmacolgy Page 24

Chapter 3 Review of literature
Reverse Cholesterol Transport
Reverse cholesterol transport refers to the process by which cholesterol is removed
from the tissues and returned to the liver. HDL is the key lipoprotein involved in
reverse cholesterol transport and the transfer of cholesteryl esters between lipoproteins.
The smallest and most dense lipoprotein particle is HDL. HDL is formed through a
maturation process where nascent HDL is secreted by the liver and intestine and
proceeds through a series of conversions (known as the "HDL cycle") to attract
cholesterol from cell membranes and free cholesterol to the core of the HDL particle,
although the exact mechanism for this not yet clear. It has been suggested that the
action of cholesteryl ester transfer protein transforms HDL into a TAG-rich particle that
interacts with hepatic-triglyceride lipase. Cholesterol ester-rich HDL may also be taken
up directly by the receptors in the liver. Another mechanism may be that cholesterol
esters are delivered directly to the liver for uptake without catabolism of the HDL
cholesterol particle.
Fig 3.9 Exogenous and Endogenous pathway for lipid Transport in Liver
Department of Pharmacolgy Page 25
Chapter 3 Review of literature
Table-3.7 Enzymes of importance in lipid transport & metabolism28
Enzymes Functions
Lipoprotein lipase
Hydrolysis of TG rich particles
some phospholipase activity activated
by APO C-II
Hepatic lipase
Hydrolysis of Tri-, Di- and mono acyl-
glycerol’s, acyl-CoA thioester and
phospholipids conversion of HDL2 to
HDL1 activated by apoA- II
Pancreatic lipase
Hydrolysis of FAs at positions 1 and
3 of emulsified TGs in the intestine.
Lecithin cholesterol Acyl
transferase LCAT
Catalysis of lecithin with cholesterol to
give lysolecithin and cholesteryl ester
activated by apo A-I and apo c -I.
Pancreatic cholsterolesterase Esterification of cholesterol in the
intestinal lumen
Acyl co A-cholesterol acyl
transferase ACAT
Esterification of cholesterol with in the cells
Cholesterol ester transfer protein CETP
Transfers esterified cholesterol from
HDLs to VLDLs and LDLs.
HMG Co A reductase Rate limiting enzyme of cholesterol synthesis
Department of Pharmacolgy Page 26

Chapter 3 Review of literature
3.5 HYPERLIPIDAEMIA AS A RISK FACTOR FOR CHD
From available epidemiological and scientific data, dyslipidaemia has been
identified as one of the main risk factors for CHD. Specific lipid abnormalities
implicated are :
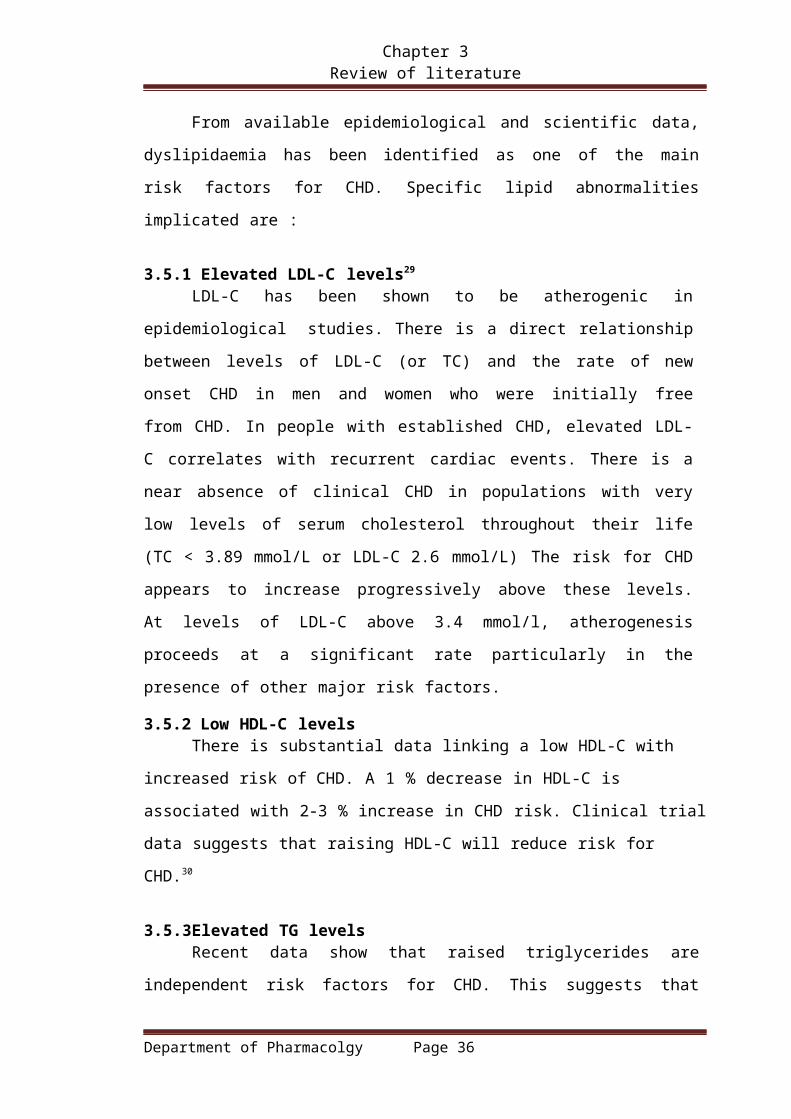
3.5.1 Elevated LDL-C levels29
LDL-C has been shown to be atherogenic in epidemiological studies. There
is a direct relationship between levels of LDL-C (or TC) and the rate of new
onset CHD in men and women who were initially free from CHD. In people
with established CHD, elevated LDL-C correlates with recurrent cardiac events.
There is a near absence of clinical CHD in populations with very low levels of
serum cholesterol throughout their life (TC < 3.89 mmol/L or LDL-C 2.6 mmol/L)
The risk for CHD appears to increase progressively above these levels. At levels
of LDL-C above 3.4 mmol/l, atherogenesis proceeds at a significant rate
particularly in the presence of other major risk factors.
3.5.2 Low HDL-C levelsThere is substantial data linking a low HDL-C with increased risk of CHD. A 1
% decrease in HDL-C is associated with 2-3 % increase in CHD risk. Clinical trial
data suggests that raising HDL-C will reduce risk for CHD.30
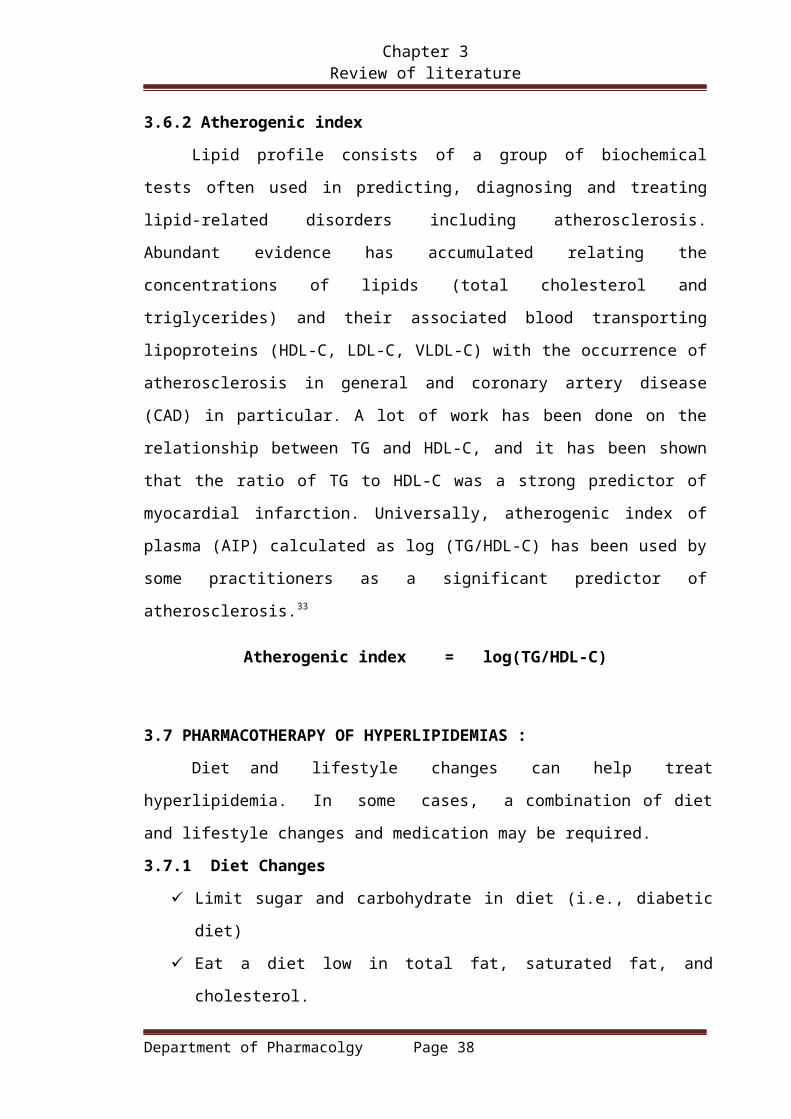
3.5.3Elevated TG levelsRecent data show that raised triglycerides are independent risk factors for
CHD. This suggests that some TG-rich lipoproteins are atherogenic. Weight
reduction and drug therapies reduce remnant lipoproteins (fibrates, nicotinic acidand
statins) and are accompanied by reduced risk for CHD .31
3.6 Atherosclerosis
The word atherosclerosis is derived from greek words Athero(gruel or paste)
and sclerosis(hardness). Atherosclerosis maybe defined as degenerative changes in
intima of medium and large arteries. The degeneration includes accumulation of lipis,
complex carbohydrates, blood and blood products, cellular waste products and is
accompanied by formation of fibrous tissue and calcium deposits in intima of blood
vessels.
3.6.1 Role of lipids in atherogenic process32
Framingham et al and from other studies demonstrate that risk of developing
Department of Pharmacolgy Page 27

Chapter 3 Review of literature
cardiovascular disease is related to degree of TC and LDL elevation in graded and
continous fashion. There is an evidence implicating role of hypercholesterolemia in
atherogenic process is that dominant lipids in atheromatus plaques are cholesterol and
cholesterol esters. Genetic defects in lipoprotein uptake and lipoprotein metabolism
that cause hypolipoprotenemia are associated with accelerated atherosclerosis.
Lowering serum cholesterol by diet or drugs slows the rate of progression of
atherosclerosis, causes regression of some plaques and reduces risk of cardiovascular
diseases.
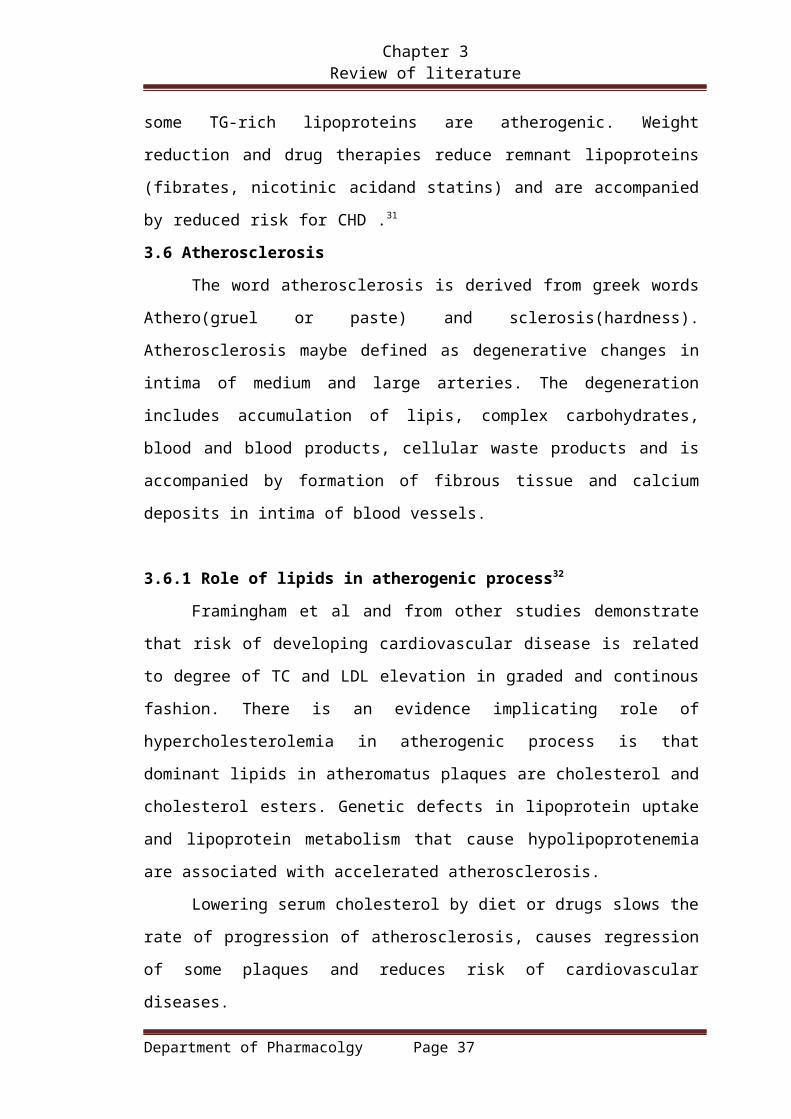
3.6.2 Atherogenic index
Lipid profile consists of a group of biochemical tests often used in predicting,
diagnosing and treating lipid-related disorders including atherosclerosis. Abundant
evidence has accumulated relating the concentrations of lipids (total cholesterol and
triglycerides) and their associated blood transporting lipoproteins (HDL-C, LDL-C,
VLDL-C) with the occurrence of atherosclerosis in general and coronary artery disease
(CAD) in particular. A lot of work has been done on the relationship between TG and
HDL-C, and it has been shown that the ratio of TG to HDL-C was a strong predictor of
myocardial infarction. Universally, atherogenic index of plasma (AIP) calculated as log
(TG/HDL-C) has been used by some practitioners as a significant predictor of
atherosclerosis.33
Atherogenic index = log(TG/HDL-C)
3.7 PHARMACOTHERAPY OF HYPERLIPIDEMIAS :
Diet and lifestyle changes can help treat hyperlipidemia. In some cases,
a combination of diet and lifestyle changes and medication may be required.
3.7.1 Diet Changes
Limit sugar and carbohydrate in diet (i.e., diabetic diet)
Eat a diet low in total fat, saturated fat, and cholesterol.
Reduce or eliminate the amount of alcohol drink.
Increase consumption of high-fiber foods such as fruits, vegetables, beans,
and whole grains.
3.7.2 Lifestyle Changes34
Obtain and maintain optimal body weight.
Smoking cessation
Department of Pharmacolgy Page 28

Chapter 3 Review of literature
Exercise regularly.
Get your doctor's okay before starting exercise, because people with
hyperlipidemia may already have hardening of the arteries or heart disease,
which increase the risk of a heart attack or death while exercising.
3.7.3 Medications:When dietary therapy and exercise cannot reduce triglyceride
levels to normal values, medication should be considered.
3.8. Drugs used in Hyperlipidemia
The five major pharmacological classes of drugs routinely used in the
treatment are
1. Statins
2. Fibrates
3. Bile acid sequestrants
4. Cholesterol absorption inhibitors
5. Nicotinic acid derivatives
Although many efficacious lipid-lowering drugs exist, none is effective for all
lipoprotein disorders and all such agents are associated with some adverse effects.
Diet should be continued to achieve the full potential of the drug regimen.
3.8.1 Statins (3-hydroxy-3-methylglutaryl-coenzymeA(HMG-CoA)reductase
inhibitors):
These compounds are structural analogs of HMG-CoA and are the most
effective and best-tolerated agents for treating hyperlipidemia. Lovastatin,
atorvastatin, fluvastatin, pravastatin, simvastatin, and rosuvastatin belong to this
class.36
Mechanism of Action: Statins affect blood cholesterol levels by inhibiting hepatic
cholesterol synthesis by reducing the conversion of HMG-CoA to mevalonate. Statins
inhibit an early and rate-limiting step in cholesterol biosynthesis, which results in
increased expression of the LDL receptor gene. In response to the reduced free
cholesterol content within hepatocytes, membrane-bound Sterol Regulatory Element-
Binding Proteins (SREBPs) are cleaved by a protease and translocated to the nucleus.
The transcription factors then bind the sterol-responsive element of the LDL receptor
Department of Pharmacolgy Page 29
Chapter 3 Review of literature
gene, enhancing transcription and increasing the synthesis of LDL receptors.
Degradation of LDL receptors also is reduced. The greater number of LDL receptors
on the surface of hepatocytes results in increased removal of LDL from the blood,
thereby lowering LDL levels.
Adverse Effects: Major adverse effect associated with statin use is myopathy but
the risk of myopathy and rhabdomyolysis increases in proportion to plasma statin
concentrations.
3.8.2 Fibric acid derivatives
These cause a marked reduction in circulating VLDL, and hence TG, with a
modest reduction in LDL and an approximately 10% increase in HDL. Benzafibrate,
ciprofibrate, g em f i b r o z i l , fenofibrate come under this class.
Mechanism of Action: T hey are agonists for a subset of lipid-controlled gene
regulatory element, Peroxisome proliferator-activated receptors (PPARα), which are
members of the superfamily of nuclear receptors, the main effects are to increase
transcription of the genes for lipoprotein lipase, apolipoproteinA1 and A5. They
increase hepatic LDL uptake.
Adverse Effects: Myositis is unusual but can be severe, with myoglobinuria and
acute renal failure.37
3.8.3 Bile acid sequestrants
Cholestyramine and colestipol are among the oldest of the hypolipidemic
drugs, and they are probably the safest, since they are not absorbed from the intestine.
Mechanism of Action: The bile-acid sequestrants are highly positively charged and
bind negatively charged bile acids. Because of their large size, the resins are not
absorbed, and the bound bile acids are excreted in the stool. Since over 95% of bile
acids are normally reabsorbed, interruption of this process depletes the pool of bile
acids and hepatic bileacid synthesis increases. As a result, hepatic cholesterol
content declines, stimulating the production of LDL receptors. The increase in hepatic
LDL receptors increases LDL clearance and lowers LDL levels.38
Adverse effects: A s resins are not absorbed, systemic toxicity is low but
gastrointestinal symptoms-especially diarrhoea are common and dose-related.
Department of Pharmacolgy Page 30

Chapter 3 Review of literature
3.8.4 Cholesterol absorption inhibitors: It is one of a group of azetidinone
cholesterol absorption inhibitors, and is indicated as an adjunct to diet
and statins in hypercholesterolaemia.39
Mechanism of Action: Ezetimibe inhibits a specific transport process in jejunal
enterocytes, which take up cholesterol from the lumen.
Adverse effects: Ezetimibe is generally well tolerated but can cause diarrhoea,
abdominal pain, headache, rash and angio-oedema.
3.8.5 Niacin (Nicotinic Acid) derivatives :
It affects virtually all lipid parameters. Niacin decreases VLDL and LDL
levels and Lp(a). It often increases HDL levels significantly. It is given adjunct
to a statin and diet in dyslipidemia or when a statin is contraindicated.
Mechanism of Action: In adipose tissue, niacin inhibits the lipolysis of TGs by
hormone sensitive lipase, which reduces transport of FFA to the liver and
decreases hepatic triglyceride synthesis.
Table-3.8 Classification of antihyperlipidemic drugs39
Drug Class Lipid Effects Side Effects Contraindications
HMG-CoAreductase Inhibitors (statins)
LDL-C - 18-55%HDL-C - 5-15%TG - 7-30%
-Myopathy-Increased liver enzymes
Absolute: -Active or chronic liver disease Relative: -Concomitant use of certain drugs*
Fibric-Acid Derivatives (Fibrates)
LDL-C - 5-20% HDL-C - 10-35% TG - 20-50%
-Dyspepsia-Gallstones-Myopathy
Absolute: -Severe hepatic disease-Severe renal disease
Department of Pharmacolgy Page 31

Chapter 3 Review of literature
Bile-Acid Sequestrants (Resins)
LDL-C - 15-30% HDL-C - 3-5%
-GIT distress-Constipation-**Decreased absorption of certain
drugs63,64,65,66
Absolute: -Dysbeta- lipoproteinemia-Tg > 4.5 mmol/l Relative: Tg > 2.3 mmol/l
Nicotinic Acid (Niacin)
LDL-C - 5-25 HDL-C - 15-35% TG - 20-50%
-Flushing-Hyperglycemia-Hyperuricemia (or gout)-Upper-GIT distress-Hepatotoxicity
Absolute: -Chronic-liver disease-Severe Gout Relative: -Diabetes (high doses only )-Hyperuricemia-Peptic-Ulcer Disease
Cholesterol Absorption Inhibitors ***
LDL-C - 18-25% HDL-C - 3-5% TG - 8-14%
-Headache-Abdominal pain-Diarrhea
3.8.6 Role of plant sterols in controlling cholesterol
Phytosterols (referred to as plant sterol and stanol esters) are a group of
naturally occurring compounds found in plant cell membranes. While cholesterol is
sterol of mammalian cells, phytosterols are sterols produced by plants. Plant sterols are
similar to their structure to cholesterol they posses ethyl or methyl group in their side
chain. plant derived sterols have been showed to decrease cholesterol for more than
fifty years. plant sterols have now become a part of public health strategy along with
normal medication. Due to structural similarity to cholesterol plant sterol impair
intestinal absorbtion of cholesterol. The ability of plant sterols to displace cholesterol
from micelles in small intestine is one mechanism of action of plant sterols. It appears
that esterification of sterol increases their solubility in fat and their in lowering LDL-
Cholesterol.
The useage of plant sterols has been recommended by both American heart
association and National cholesterol education program panel as adjuvant in lowering
lipid levels.40Plant sterols and stanols are substances that occur naturally in small
amounts in many grains, vegetables, fruits, legumes, nuts, and seeds. Since they have
powerful cholesterol-lowering properties, manufacturers have started adding them to
foods. You can now get stanols or sterols in margarine spreads, orange juice, cereals,
Department of Pharmacolgy Page 32

Chapter 3 Review of literature
and even granola bars. As part of a heart-healthy eating plan, consuming phytosterols in
recommended quantities has been shown to lower total cholesterol up to 10 percent and
LDL or “bad” cholesterol up to 14 percent. This reduction is in addition to other
cholesterol-lowering strategies you may have initiated, such as eating more heart
healthy or taking a cholesterol-lowering statin. The effectiveness of phytosterols is so
strong that The National Cholesterol Education Program recommends people with high
cholesterol consume 2 grams of phytosterols each day.
The Food and Drug Administration (FDA) has even approved a health claim on
phytosterols, which states: “Foods containing at least 0.65 gram per serving of
vegetable oil plant sterol esters, eaten twice a day with meals for a daily total intake of
at least 1.3 grams, as part of a diet low in saturated fat and cholesterol, may reduce the
risk of heart disease.”
Table-3.9 Screening models for Antihyperlipidemic agents
S.no Model Mechanism
1. Diet
a)Atherogenic41
b)Cafeteria
Higher availability of Acetyl co-A
stimulates cholesterogenesis synthesis.
2. Triton43 Increasing hepatic cholesterol synthesis
and by decreasing cholesterol excretion
3. Carbohydrates42 A hypertriglyceridemic effect is seen due
to hepatic overproduction of VLDL and
induction of lipogenic enzymes via dietary
sucrose
4 Alcohol Generate free radicals which induce
oxidative stress that have potential to raise
blood cholesterol and triglycerides.
5 Isoproterenol44 By increasing lipid peroxidation induced
free radicals that causes cholesterol
synthesis
6 Genetic models
a)Monosodium
MSG reported to produce lesions of
arcurate nucleus in h followed by
Department of Pharmacolgy Page 33

Chapter 3 Review of literature
glutamate(MSG)45
b)Hereditary
hypercholesterolemia in rats
and rabbits
hypoplastic-hypertri=ophic obesity.
b)By decreasing rate of catabolism of
chylomicrons and LDL.
7 Iron rich diet and copper
deficiency46
Copper deficiency results in inadequate
antioxidant mechanism that results in liver
iron retension.This in combination of diet
results in generation of free radicals that
leads to increased cholesterol synthesis.
8 Polaxomer-407 induced47 By inhibition of lipoprotein lipase
9 Intravenous lipid tolerance
test43
Drugs possessing lipolytic activity can be
determined
10 Influence on lipoprotein
lipase43
Inhibition of lipoprotein lipase decrease
degradation of lipids
11 Diabetic models48
a)Alloxan induced
b)Streptozocin induced
By selective degradation of beta cells
inhibit insulin secretion that alters
carbohydrate,lipid metabolism
3.9 Experimental models of hyperlipidemia
3.9.1 High fat diet induced hyperlipidemia41
Principle-
The model is based on fact that high fat diet causes Higher availability of
Acetyl co-A stimulates cholesterogenesis synthesis.
Procedure -
In rats hyperlipidemia can be induced by daily oral administration of fat diet
containing 2%cholesterol, 2%cholic acid, choline chloride suspended in peanut oil
for a period of 26 days. Test compounds and standard drug administered after
induction or may be administered simultaneously. High fat diet causes increased
lipid profile. The cholesterol, triglycerides, HDL-C, LDL-C,VLDL-C are compared
with positive control to asses antihyperlipidemic activity.
3.9.2 TritonX-100 induced hyperlipidemia43
Principle-
Department of Pharmacolgy Page 34

Chapter 3 Review of literature
The model is based on fact that triton,non ionic surfactant (iso octyl
polyoxyethylene phenol/Tyloxipal) to rats results in biphasic elevation of lipid
levels.
Procedure-
Phase I- It is is thought to be due to increased hepatic synthesis of cholesterol
which reaches to elevated lipid levels at end of 48hr through the ability to interfere
with uptake of lipids by tissues.
Phase II- In this phase the elevated lipid levels reach maximum by end of 72hrs
due decreased cholesterol secretion. Drugs that can alter cholesterol excretion can be
assessed. The biphasic nature of Triton induced hyperlipidemia is helpfull in
understanding mode of action of antihyperlipidemic drugs.
3.9.3 Fructose indued hyperlipidemia42
Principle –
The model is based on fact that dietary fructose causes hepatic overproduction
of VLDL and induction of lipogenic enzymes.
Procedure-
Carbohydrate, fructose plays an important role in pathogenesis of experimental
hypertriglyceridemia and hyperinsulinemia. Adverse effect of fructose on
insulin sensitivity in rats is well established. In rats hypertriglyceridemia can be
induced by administering fructose(60%) for 30 days. Test drug and standard
drugs administerd simultaneously or after induction for 2 weeks. Later lipid
profile of all animals measured and compared with positive control.
3.9.4 Intravenous lipid tolerance test in rats50,51
Purpose and rationale
Intravenous injection of a lipid emulsion results in an increase of triglycerides in
serum. The lipolytic activity an be determined by measuring lipid elimination.
procedure
Male Wistar rats weighing 200–240 g are treated daily with various doses of the
test compound or the vehicle over a period of 5 days. On the fifth day, two
hours after the last administration of the test compound, the animals are
anesthetized with 125 mg/kg sodium hexobarbital i.p. Then they are injected
intravenously with 2 ml/kg of a 10% lipid emulsion (Intralipid® Vitrum,
Hausmann AG, St. Gallen, Switzerland). Prior to the injection and 10, 20, 30,
Department of Pharmacolgy Page 35
Chapter 3 Review of literature
and 40 min thereafter blood is withdrawn by retroorbital puncture for
determination of triglycerides.
Table-3.10 Medicinal plants having Antihyperlipidemic activity52
Plant Family Part Mechanism
Corriandrum sativum Umbelliferae Leaves,seeds
By decreasing update
and increasing break
down of lipid
Trichilia connaroides Meliaceae LeavesBy interfering with
cholesterol biosynthesis
Curcuma longa Zinziberaceae TuberBy increasing
cholesterol catabolism
Nardostachys
jatamansiValerianaceae Whole plant
By increasing
cholesterol catabolism
Achyranthus aspera Amaranthaceae Aerial parts
By rapid excretion of
bile acids causing low
absorption of cholesterol
Cassia tora Caesalpinaceae seedsBy inhibitinf Acetyl co-
A activity.
Phaseolus
aconitifoliusLeguminosae Seeds
By increasing LDL
catabolism and
decresing LDL synthesis
Allium sativum Liliaceae BulbsBy enhancing
cholesterol degradation
Enicostemma littorale Gentianaceae Whole plantBy inhibiting HMGCoA
activity
Pterocarpus
marsupiumFabaceae Heart wood Not known
Trigonellafoenum
graecumFabaceae Seeds Not known
Phyllanthus niruri Euphorbiaceae Whole plant By enhancing LCAT
Department of Pharmacolgy Page 36
Chapter 3 Review of literature
activity
Paeonia lactiflora Ranunculaceae Roots Not known
Glycine tomentella Leguminosaes Roots Not known
3.10 Plant profile
Botanical name : Glycosmis pentaphylla
Taxonomical classification
Kingdom : Plantae
Order : Sapindales
Family : Rutaceae
Subfamily : Aurantioideae
Genus : Glycosmis
Species : Glycosmis pentaphylla
Synonyms : Glycosmis arborea
3.9.1 Vernacular names in India53
English : Orange berry
Hindi : Ban nimbu
Sanskrit : Asvasakhotha
Oriya : Gonjipandu
Telugu : Sirna tulasi
sTamil : Konchi
Malayalam : Kurumpannal
3.9.2 Common names in other countries53
Chinese : Shi ling ju.
Department of Pharmacolgy Page 37
Chapter 3 Review of literature
English : Gin berry
French : Glycosmisier de Cochinchine
3.9.3 Geographical distribution
Glycosmis pentaphylla(Rutaceae) is a medium annual shrub native to tropical Asia and
distributed in the tropical and subtropical regions.
Fig- 3.10 Glycosmis pentaphylla palnt
Department of Pharmacolgy Page 38
Chapter 3 Review of literature
Fig –3.11 Glycosmis pentaphylla stem
Morphological characteristics
Glycosmis pentaphylla is a shrub growing 1 to 5 meters high. Leaves usually have 3 to
5 pinnately arranged leaflets, though these are sometimes reduced to one or two, all
forms being often found on the same plant. Leaflets are oblong-lanceolate to lanceolate,
5 to 18 centimeters long, and 2 to 7 centimeters wide. Flowers are small, white, about 6
millimeters in diameter, borne in axillary, solitary or paired, interrupted, narrow,
cymose panicles which are 5 centimeters long or less. Fruit is fleshy, pink or reddish,
rounded, 1 centimeter in diameter, and contains a single nearly spherical seed which is
about 4 millimeters in diameter. Mesocarp is fleshy and sweet.
3.9.4 CHEMICAL CONSTITUENTS54 :
Leaves : Contains quinolone alkaloid-glycolone.
Flowers: Contains alkaloids and an amide, alkaloids-arborine, arborinine,
skimmianine, glycorine, glycosmicine benzamide-2-methylamino. Also contains
carbazole alkaloid-mupamine
Roots: Contains Dictamine, γ-fagarine, skimmianine, β-sitosterol, coumarin,
stigmasterol, myricylalcohol, base glyborine, triterpenes-arborinolA,arborinolB,
arborine, arborinine,carbazolealkaloid- Glycozolinol,Glycozolicine,3-formylcarbazole
Department of Pharmacolgy Page 39

Chapter 3 Review of literature
and glycosinine,glycozolidol.Root bark contains Acridone alkaloids-Noracronycine, de-
methylacronycine and e-N-methylnoracronycine.
3.9.5 Traditional uses:54
The plant is used in indigenous medicine for cough, rheumatism, anaemia and
jaundice.
The juice of the leaves ,which is bitter, is used in fever, liver complaints and as
vermifuge.
A paste of the leaves with ginger is applied in eczema and skin infections.
A decoction of the root is given for facial inflammations.
3.9.6 LITERATURE REVIEW OF ACTIVITIES DONE ON PLANT
1. Wang J, DiY, Yang X, Li S, Wang Y , Hao X, in 2006 reported ,
Hydroquinone diglycoside acyl esters from the stems of Glycosmis pentaphylla .
Four hydroquinone diglycoside acyl esters, glypentosides A–C (1–3) and
seguinoside F (4), were isolated from the stems of Glycosmis pentaphylla.56
2. Pacher T, Bacher M , Hofer O , Greger H , in 2001 reported, Stress induced
carbazole phytoalexins in Glycosmis species . Induced formation of a series of
carbazole alkaloids was observed in leaves of Glycosmis parviflora and
G.pentaphylla after wounding, UV-irradiation, and particularly after inoculation
with the fungus Botrytis cinerea. Detailed experiments with marked infection areas
confirmed the restricted accumulation of carbazole derivatives which could not be
detected in non-infected areas of the same leaf.57
3. Quader MA., Nutan MTH , Rashid MA , in 1999 reported , Antitumor
alkaloid from Glycosmis pentaphylla . Arborinine, an acridone alkaloid obtained
from Glycosmis pentaphylla, exhibited significant inhibition of crown gall tumors
produced by Agrobacterium tumefaciens in a potato disc bioassay58.
Department of Pharmacolgy Page 40
Chapter 3 Review of literature
4. Muthukrishnan J, Seifert K, Hoffmann KH , Lorenz MW,in 1999 reported,
Inhibition of juvenile hormone biosynthesis in Gryllus bimaculatus by Glycosmis
pentaphylla leaf compounds. The EtOAc fraction of Glycosmis pentaphylla leaf
extract inhibits the juvenile hormone III-biosynthesis in vitro of corpora allata
from 3 day old females of the field cricket Gryllus bimaculatus. The bioactive
compound which is responsible for this activity was identified as the quinazolone
alkaloid arborine. This alkaloid showed also a larvicidal activity against the
mosquito Culex quinquefasciatus59
5. Bhattacharyya P, Chowdhury BK, in 1985 reported ,Glycolone, a quinolone
alkaloid from Glycosmis pentaphylla Glycolone, a quinolone alkaloid has been
isolated from the leaves of Glycosmis pentaphylla. The structure of the compound
has been established as 4,8-dimethoxy-3-(3-methyl but-2-enyl)-2-quinolone from
physical and chemical evidences.60
6. Bhattacharyya P, Chakrabartty PK , Chowdhury BK ,in 1985 reported,
Glycozolidol, an antibacterial carbazole alkaloid from Glycosmis pentaphylla.
Glycozolidol, a new carbazole alkaloid, has been isolated from the roots of
Glycosmis pentaphylla. Its structure has been established as 6-hydroxy-2-methoxy-
3-methylcarbazole on the basis of physical and chemical evidence. The compound
has been found to be active at some Gram-positive and Gram-negative bacteria.61
7. Mukherjee S, Mukherjee M, Ganguly SN , in 1983 reported , Glycozolinine, a
carbazole derivative from Glycosmis pentaphylla. A new carbazole derivative,
glycozolinine, was isolated from the seeds of Glycosmis pentaphylla. From
physical and chemical evidence its structure is 6-hydroxy-3-methylcarbazole.61
8. N. Jaya Raju et al. studied hepatoprotective activity of glycosmis pentaphylla
roots against ccl4– induced acute liver injury in rats. Golugu and Gongipadu
(Telugu) of ethyl acetate and methanolic extracts (100, 200 and 400 mg/kg) was
prepared and tested for its hepatoprotective effect against carbon tetrachloride
induced in rats. Treatment with ethyl acetate extract of Glycosmis pentaphylla
(Rutaceae) roots has brought back the altered levels of biochemical markers to the
near normal levels in the dose dependent manner. This was evident from
Department of Pharmacolgy Page 41
Chapter 3 Review of literature
significant reduction in serum enzyme, SGOT, SGPT, ALP and Total bilirubin
Sand both the extracts were recorded with significant hepatoprotective activity62
9. Ramesh petchi r et al. studied anti-diabetic and anti-arthritic potential of
Glycosmis pentaphylla stem bark in fca induced arthritis and streptozotocin
induced diabetic rats. Graded doses of the ethonolic extract of Glycosmis
pentaphylla were administered to experimental arthriticand diabetic rats for
21days.Significant reductions in fasting blood glucose levels and inflammation
were observed in the respective diabetic and arthritic animals.63
Department of Pharmacolgy Page 42


















