

3 dimensions of care for diabetes June 2015
43
3 D imensions of care F or D iabetes (3DFD) Dr Carol Gayle, Consultant Diabetologist Dr Anne M. Doherty Consultant Liaison Psychiatrist 18 th June 2015 1
-
Upload
nhs-improving-quality -
Category
Healthcare
-
view
185 -
download
3
Transcript of 3 dimensions of care for diabetes June 2015

3 Dimensions of care For Diabetes (3DFD)
Dr Carol Gayle, Consultant DiabetologistDr Anne M. Doherty Consultant Liaison Psychiatrist
18th June 2015
1

Dissemination

The cost of diabetes to the NHS

Depression is associated with all stages of diabetes
odds ratio 1.37-1.60
Pre-diabetes: Mezuk Diabetes Care 2008; Kan Diabetes Care 2012 Diabetes: Anderson et al Diabetes Care 2001 Glycaemic control: Lustman et al Diabetes Care 2000Complications: de Groot et al Psychosom Med 2001 Mortality: Ismail et al Diabetes Care 2007; Winkley Diabetologia 2011
odds ratio 2.1
effect size 0.17
odds ratio 3.1
hazards ratio 2.0-5.0
pre-diabetes diabetes suboptimal glycaemic control
complications mortality
4
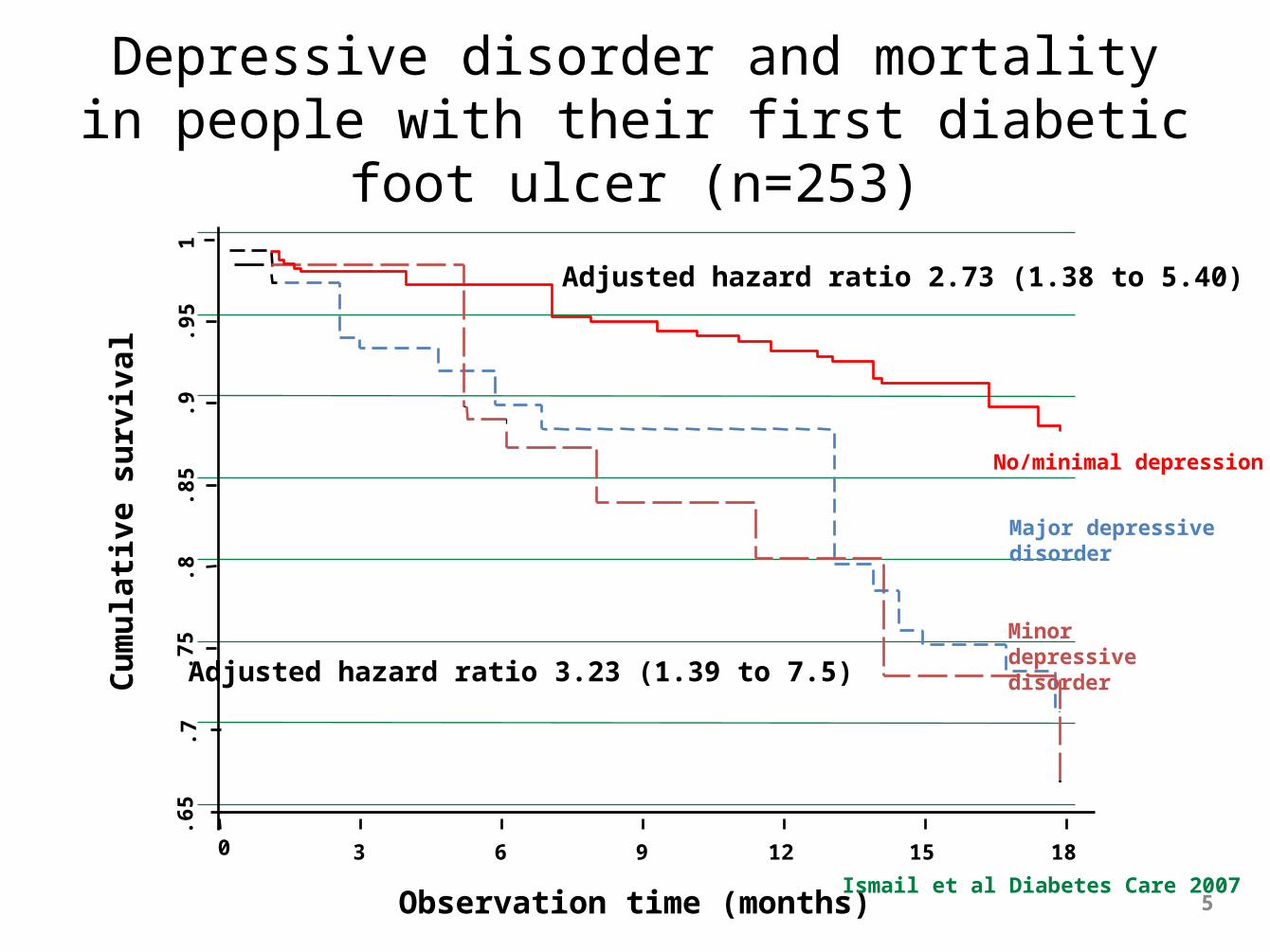
Depressive disorder and mortality in people with their first diabetic foot ulcer (n=253)
.65
.7.7
5.8
.85
.9.9
51
3 6 9 12 15 18
Observation time (months)
Major depressive disorder
Minor depressive disorder
No/minimal depression
Ismail et al Diabetes Care 2007
Adjusted hazard ratio 3.23 (1.39 to 7.5)
Adjusted hazard ratio 2.73 (1.38 to 5.40)
Cu
mu
lati
ve s
urv
ival
5
0

Other psychiatric conditions

STEP 1: All known and suspected presentations of depression
STEP 2: Persistent subthreshold depressive symptoms; mild to moderate depression
STEP 3: Persistent subthreshold depressive symptoms or mild to moderate depression with inadequate response to initial interventions; moderate and severe depression
STEP 4: Severe and complex1 depression; risk to life; severe self-neglect
Low-intensity psychosocial interventions, psychological interventions, medication and referral for further assessment and interventions
Medication, high-intensity psychological interventions, combined treatments, collaborative care2, and referral for further assessment and interventions
Medication, high-intensity psychological interventions, electroconvulsive therapy, crisis service, combined treatments, multiprofessional and inpatient care
Focus of the intervention
Nature of the intervention
Assessment, support, psycho-education, active monitoring and referral for further assessment and interventions
NICE stepped-care model

2013 estimated prevalence of diabetes by local authority
•2030 estimate of diabetes, assuming obesity continues to rise at the current rate
Contains Ordnance Survey data © Crown copyright and database right 2013•Source: Diabetes Prevalence Model for local authorities in England

2013 estimated prevalence of diabetes by local authority
•2030 estimate of diabetes, assuming obesity continues to rise at the current rate
Contains Ordnance Survey data © Crown copyright and database right 2013•Source: Diabetes Prevalence Model for local authorities in England

Social problems

Standards

Psychological care
Diabetes care
Social care
Parallel versus integrated services
Diabetes care
Psychological care
Social care

NHS London Regional Innovation Fund 2010
First round 117 applications = £30m
Final shortlist 17 applications = £5m
3DFD £125k =largest award

3DFD: PrinciplesA Blank Canvas
Inclusivity
Diabetes care
Psychological care
Social care
Integrated Care
3DFD- a few minor road blocks.....

3 Dimensions of Care For Diabetes- Innovation

Challenges and Opportunities 'Where ignorance is bliss, 'tis folly to be wise’

• debt management• housing support• occupational rehabilitation• literacy• advocacy
• medication support• biomedical monitoring• diabetes education• technology• complications
• increased self efficacy towards diabetes
• patient reported outcomes • patient led case meetings
• diagnostic assessment• risk management• psychotropic medications • brief psychological
treatments
The model

Integrated across the sectors
Diabetes care
Psychological care
Social care
Patient


3DFD- Current Service

Challenges and Opportunities - current service

3DFD characteristics Year 1
Oct 2012-2013
n=306
Year 2
Oct 2013-2014
n=255
Total
Oct 2012-2014
n=561
Age, mean (SD) 47 (14.8) 50 (15.1) 48 (14.9)
Gender n, (%) Male 121(39.4) 110 (43.3) 231 (41.2)
Female 181 (60.6) 144 (56.7) 325 (58.8)
Diagnosis n, (%) Type 1 89 (28.9) 60 (23.6) 149 (26.6)
Type 2 218 (71.1) 194 (76.4) 412 (73.4)
Ethnic group n, (%)
Caucasian 76 (24.7) 81 (31.9) 157 (28.0)
African/Caribbean 98 (31.9) 88 (34.6) 186 (33.2)
Other 133 (43.2) 88 (33.5) 218 (38.8)
HbA1cmean (SD)
% (DCCT) 10.7 (1.9) 11.6 (2.1) 11.1 (2.0)
mmol/mol (IFCC) 93 (10) 103 (11) 98 (10)

3DFD characteristics Year 1
Oct 2012-2013
n=306
Year 2
Oct 2013-2014
n=255
Total
Oct 2012-2014
n=561
Age, mean (SD) 47 (14.8) 50 (15.1) 48 (14.9)
Gender n, (%) Male 121(39.4) 110 (43.3) 231 (41.2)
Female 181 (60.6) 144 (56.7) 325 (58.8)
Diagnosis n, (%) Type 1 89 (28.9) 60 (23.6) 149 (26.6)
Type 2 218 (71.1) 194 (76.4) 412 (73.4)
Ethnic group n, (%)
Caucasian 76 (24.7) 81 (31.9) 157 (28.0)
African/Caribbean 98 (31.9) 88 (34.6) 186 (33.2)
Other 133 (43.2) 88 (33.5) 218 (38.8)
HbA1cmean (SD)
% (DCCT) 10.7 (1.9) 11.6 (2.1) 11.1 (2.0)
mmol/mol (IFCC) 93 (10) 103 (11) 98 (10)

3DFD characteristics Year 1
Oct 2012-2013
n=306
Year 2
Oct 2013-2014
n=255
Total
Oct 2012-2014
n=561
Age, mean (SD) 47 (14.8) 50 (15.1) 48 (14.9)
Gender n, (%) Male 121(39.4) 110 (43.3) 231 (41.2)
Female 181 (60.6) 144 (56.7) 325 (58.8)
Diagnosis n, (%) Type 1 89 (28.9) 60 (23.6) 149 (26.6)
Type 2 218 (71.1) 194 (76.4) 412 (73.4)
Ethnic group n, (%)
Caucasian 76 (24.7) 81 (31.9) 157 (28.0)
African/Caribbean 98 (31.9) 88 (34.6) 186 (33.2)
Other 133 (43.2) 88 (33.5) 218 (38.8)
HbA1cmean (SD)
% (DCCT) 10.7 (1.9) 11.6 (2.1) 11.1 (2.0)
mmol/mol (IFCC) 93 (10) 103 (11) 98 (10)

3DFD characteristics Year 1
Oct 2012-2013
n=306
Year 2
Oct 2013-2014
n=255
Total
Oct 2012-2014
n=561
Age, mean (SD) 47 (14.8) 50 (15.1) 48 (14.9)
Gender n, (%) Male 121(39.4) 110 (43.3) 231 (41.2)
Female 181 (60.6) 144 (56.7) 325 (58.8)
Diagnosis n, (%) Type 1 89 (28.9) 60 (23.6) 149 (26.6)
Type 2 218 (71.1) 194 (76.4) 412 (73.4)
Ethnic group n, (%)
Caucasian 76 (24.7) 81 (31.9) 157 (28.0)
African/Caribbean 98 (31.9) 88 (34.6) 186 (33.2)
Other 133 (43.2) 88 (33.5) 218 (38.8)
HbA1cmean (SD)
% (DCCT) 10.7 (1.9) 11.6 (2.1) 11.1 (2.0)
mmol/mol (IFCC) 93 (10) 103 (11) 98 (10)

Quantitative outcomesPre 3DFD Post 3DFD Change score p-value
Mean HbA1c, mmol/mol (SD)** 102 (22) 84 (22) -18 (17) <0.001
Mean Patient Health Questionnaire-9 depression score (SD)** 8.8 (6.5) 6.4 (5.8) -2.4 (2.2) 0.021
Mean General Anxiety Scale-7 score (SD)** 8.9 (5.3) 4.9 (5.3) -4.0 (3.5) <0.001
Mean Diabetes Distress Scale (SD)** 47.3 (17.1) 36.0 (15.4) -11.3 (19.1) 0.01
Mean Outcomes Star score (SD)** 55.9 (11.5) 61.6 (14.9) +5.7 (9.1) 0.003
** Service for first 6-12 months (n=198)

Pre 3DFD Post 3DFD Change score p-value
Mean (SD) DCCT % (n=185) 11.3 (2.1) 10 .0 (2.0) 1.5 (1.6) <0.001
Mean (SD) IFCC HbA1c mmol/mol (n=185) 100 (23) 83 (22) 16 (17) <0.001
3DFD outcomes – HbA1c
98
87
82 82
70
75
80
85
90
95
100
Baseline 6 months 1 year 2 years
HbA1c, mmol/mol
Time
Maintenance of HbA1c

Psychiatric morbidity

Support worker assisting patient with type 2 diabetes with accommodation

Social Needs

Qualitative: Focus group (ThinkPublic)
“All of the patients we interviewed spoke extremely positively about their experiences of 3DFD and the difference the service had made to their lives. Patients identified a number of positive characteristics about the service:
– Optional and flexible nature of the service– Caring attitude of staff.– Self-directed nature of support– Reliability – Professionalism and communication

Patient testimonial
My name is Rochelle, I am a single parent with two children. I had difficulties controlling my diabetes. I became very depressed. 3DFD has managed to help me to overcome my fears of dealing with diabetes. I now use my insulins better.....Rochelle:(T1DM) HbA1c 15.2 to 8.7%
My name is Rochelle, I am a single parent with two children. I had difficulties controlling my diabetes. I became very depressed. 3DFD has managed to help me to overcome my fears of dealing with diabetes. I now use my insulins better.....Rochelle:(T1DM) HbA1c 15.2 to 8.7%

Cost benefit analysis
3DFD net saving £33K/borough/year/ 100 patients

Main 3DFD outcomes - economic
Pre 3DFD Post 3DFD Change score p-value
No of admissions to A&E/previous year (n=119) 141 77 -64 <0.001
No of bed days/previous year (n=119) 381 300 -81 0.08
No of recurrent admissions (days)/previous year (n=119) 10 (73) 4 (14) -6 (-59) 0.012

Quality in Care Awards 2011
BMJ Awards 2014Diabetes Team of the Year
Mary McKinnon Lecture DUK 2015
NHS Innovation Challenge Prize 2015

Impact & Dissemination
Other Services Hillingdon
Oxford Hull
Service commissioned by Lambeth and Southwark CCGs from 2014

Would this work in other setting?

Regional Innovation Fund

NEXT WEBINAR:
Managing Demand and Capacity in Mental Health Settings
Friday 26th June, 12.30 – 13.30
Invitations to follow shortly

Thank you!
A link to this webinar will be sent out to you shortly along with a link to the slides which will be made available through Slideshare.


















