2nd CUTEHeart Workshop Manuel Gomes Presentation
13
theta.lshtm.ac.uk Non-compliance in randomised controlled trials comparing vascular and endovascular interventions for cardiovascular care 2 nd CUTEHeart Workshop Manuel Gomes April 23, 2016
Transcript of 2nd CUTEHeart Workshop Manuel Gomes Presentation
theta.lshtm.ac.uk
Non-compliance in randomised controlled
trials comparing vascular and endovascular
interventions for cardiovascular care
2nd CUTEHeart Workshop
Manuel Gomes
April 23, 2016

• Non-compliance in RCTs – cardiovascular care
• Defining the question of interest
• Specific challenges in HTA
• Methods for handling non-compliance
• Results from the IMPROVE trial
• Discussion
Overview
theta.lshtm.ac.uk
Non-compliance in RCTs
theta.lshtm.ac.uk
• Patients often do not comply with their randomised treatment:– Switch to other randomised arm (treatment switching)
– Change to non-trial treatment
– Stop receiving treatment altogether
• Reasons– Intervention not suitable (randomisation happens before assessment)
– Patient is responding poorly to their allocated treatment (unethical)
– Patient’s disease progresses and requires alternative treatment
– Clinical expert is more familiar with particular intervention
• Problem– Non-compliance is usually related to individual characteristics and
prognosis, and can lead to misleading inferences.
High levels of non-compliance
in cardiovascular trials
theta.lshtm.ac.uk
• Drug therapies for treating patients with coronary heart disease– Uncertainty about the benefits of statins; perceived adverse effects
• Medication/diet for treating patients with chronic heart failure– Complicated drug regimens; difficulties in changing lifestyle
• Cardiac rehabilitation programmes– Low levels of physical activity; pain/depression/anxiety
• Surgical interventions (emergency setting)– Surgeon’s expertise; other clinical indications

Motivating example
theta.lshtm.ac.uk
IMPROVE trial
• Aim: to compare a preferential endovascular strategy (EVAR) with emergency Open Repair for the management of suspected ruptured abdominal aortic aneurysm (AAA)
• Pragmatic RCT (EVAR: n=316; Open repair: n=297)– Randomisation happens before CT scan
– EVAR to Open Repair switch (42%); e.g. surgeon expertise
– Open Repair to EVAR (12%); e.g. not fit for general anaesthesia
• Cost-effectiveness outcomes (1-year)– Overall mortality (life – years)
– Quality of life (EQ-5D) at 3 and 12 months
– costs
Defining the question
theta.lshtm.ac.uk
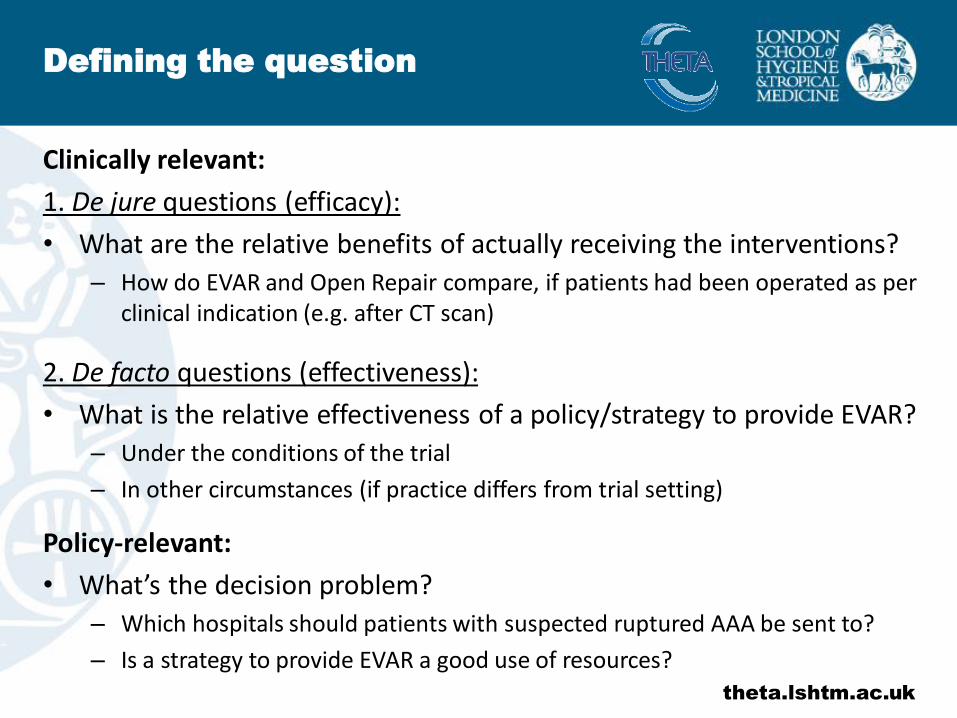
Clinically relevant:
1. De jure questions (efficacy):
• What are the relative benefits of actually receiving the interventions?
– How do EVAR and Open Repair compare, if patients had been operated as per clinical indication (e.g. after CT scan)
2. De facto questions (effectiveness):
• What is the relative effectiveness of a policy/strategy to provide EVAR?
– Under the conditions of the trial
– In other circumstances (if practice differs from trial setting)
Policy-relevant:
• What’s the decision problem?
– Which hospitals should patients with suspected ruptured AAA be sent to?
– Is a strategy to provide EVAR a good use of resources?

HTA-specific challenges
theta.lshtm.ac.uk
• Decision makers require an assessment of the relative effectiveness and cost-effectiveness over a long-period of time– Clinically-relevant outcomes such as progression-free survival raise less
concerns about non-compliance, but are insufficient for decision making
• Levels of non-compliance may not be representative of those seen in practice
• Differences in costs often depend on intervention receipt, not on the intention to receive treatment– Drug trial: expensive drug is prescribed but may not always be taken
• Added complexity for analysis– E.g. correlations between the multiple outcomes
theta.lshtm.ac.uk
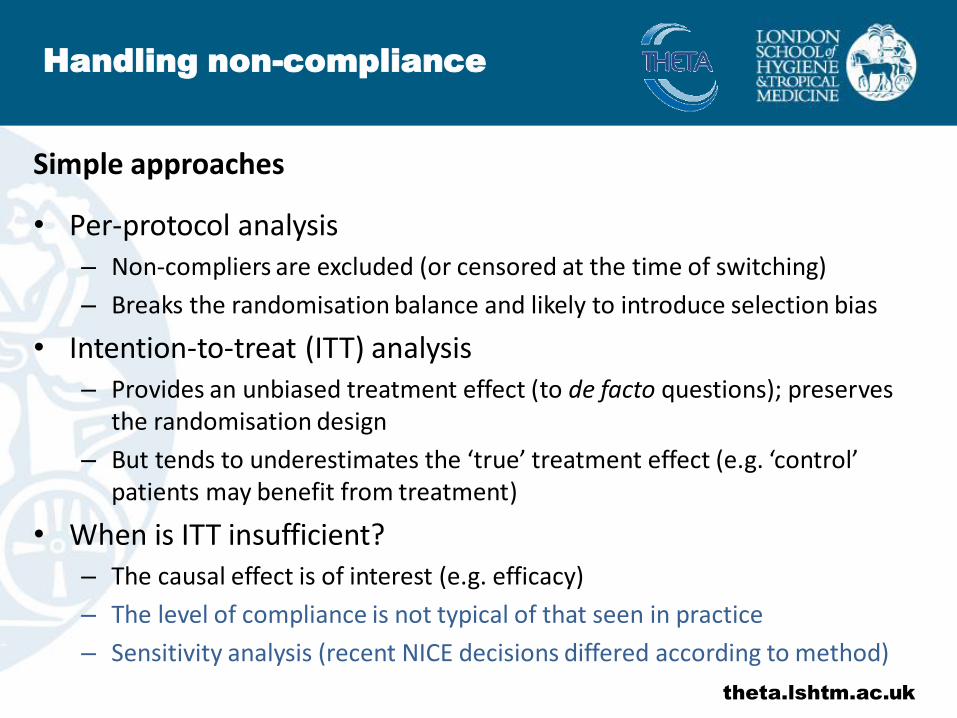
Simple approaches
• Per-protocol analysis– Non-compliers are excluded (or censored at the time of switching)
– Breaks the randomisation balance and likely to introduce selection bias
• Intention-to-treat (ITT) analysis– Provides an unbiased treatment effect (to de facto questions); preserves
the randomisation design
– But tends to underestimates the ‘true’ treatment effect (e.g. ‘control’ patients may benefit from treatment)
• When is ITT insufficient?– The causal effect is of interest (e.g. efficacy)
– The level of compliance is not typical of that seen in practice
– Sensitivity analysis (recent NICE decisions differed according to method)
Handling non-compliance
theta.lshtm.ac.uk
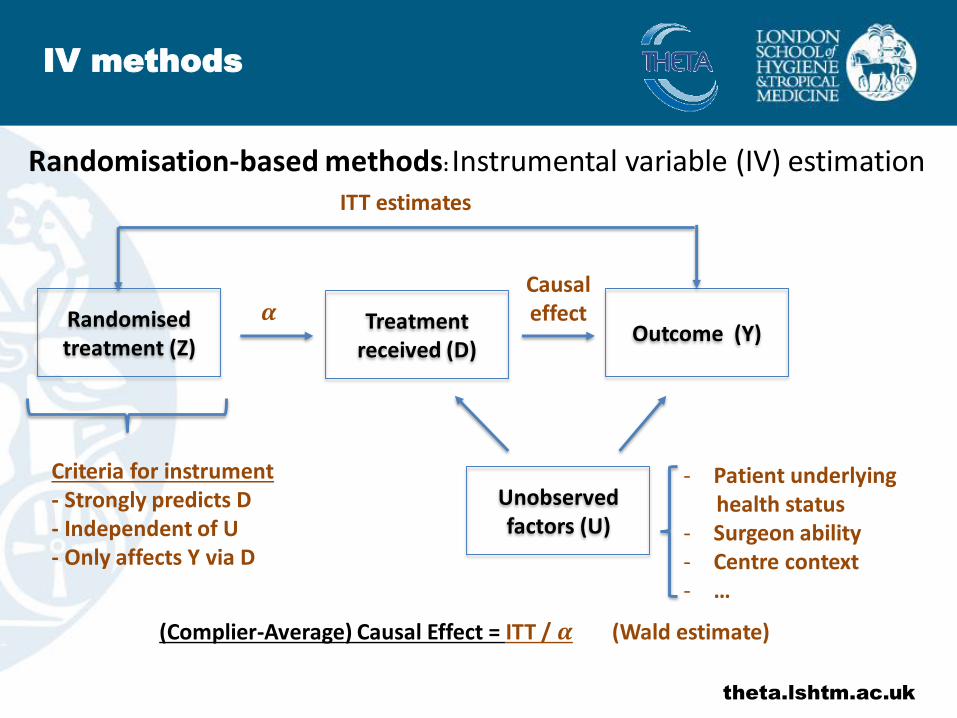
Randomisation-based methods: Instrumental variable (IV) estimation
Randomised treatment (Z)
Outcome (Y)Treatment
received (D)
Unobserved factors (U)
ITT estimates
- Patient underlying health status
- Surgeon ability- Centre context- …
Causal effect
Criteria for instrument- Strongly predicts D- Independent of U- Only affects Y via D
(Complier-Average) Causal Effect = ITT / 𝜶 (Wald estimate)
𝜶
IV methods

theta.lshtm.ac.uk
Continuous outcomes (e.g. quality of life, costs)
- 2-stage methods (2SLS)- Stage 1: Regress D on Z
- Stage 2: Regress Y on the predicted D (Variance needs to be corrected)
- Likelihood-based methods (LIML, full-Bayesian analysis)- Joint estimation of the outcome and treatment models
- Usually assumes multivariate Normality
- Semi-parametric approaches (GMM, G-estimation)- Relaxes assumptions about error distribution and model specification
IV methods

theta.lshtm.ac.uk
Limitations
- Survival outcomes (e.g. overall survival)
- Cox regression could be used (stage 2), but resulting estimates may differ from population-average hazard difference (marginal ≠ conditional effect)
- Rank-preserving structural failure time models: use randomisation to estimate counterfactual survival times, but assumes common treatment effect
- Multiple switches– Marginal Structural models: Compliers are re-weighted by the inverse of the
probability of being censored (switch treatment) at each time point
– Rely on the ‘no unobserved confounding’ assumption; i.e. non-compliance is independent of unobserved factors
- Clustered designs (e.g. cluster trials)- In principle, hierarchical approaches (ML) can be used, but properties unknown
IV methods
IMPROVE trial results
theta.lshtm.ac.uk
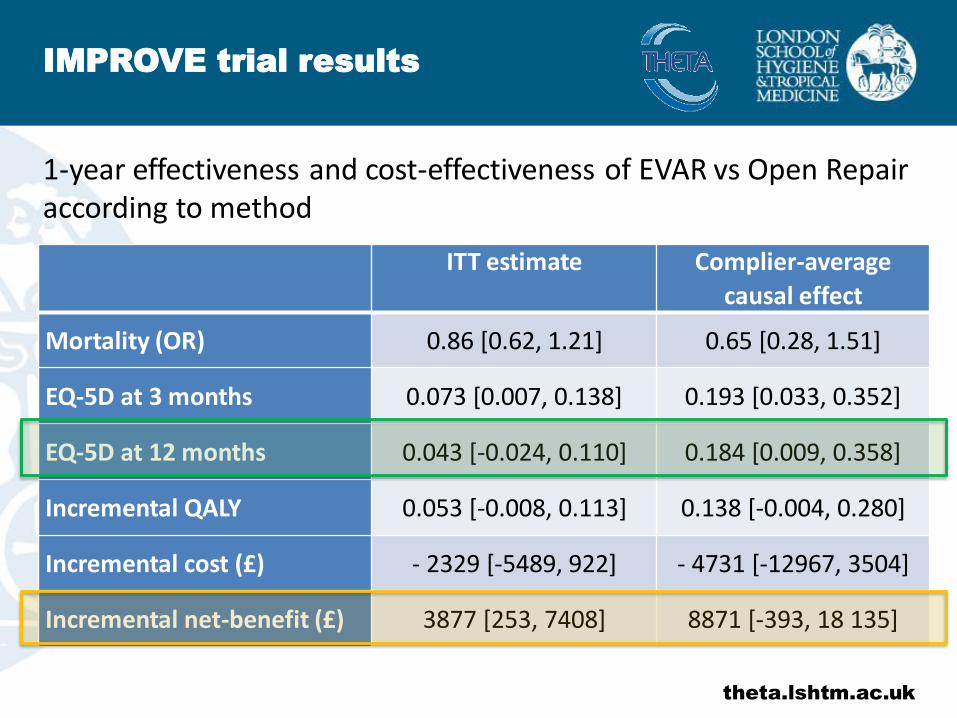
1-year effectiveness and cost-effectiveness of EVAR vs Open Repair according to method
ITT estimate Complier-average
causal effect
Mortality (OR) 0.86 [0.62, 1.21] 0.65 [0.28, 1.51]
EQ-5D at 3 months 0.073 [0.007, 0.138] 0.193 [0.033, 0.352]
EQ-5D at 12 months 0.043 [-0.024, 0.110] 0.184 [0.009, 0.358]
Incremental QALY 0.053 [-0.008, 0.113] 0.138 [-0.004, 0.280]
Incremental cost (£) - 2329 [-5489, 922] - 4731 [-12967, 3504]
Incremental net-benefit (£) 3877 [253, 7408] 8871 [-393, 18 135]
• Non-compliance is a major issue in clinical trials of cardiovascular interventions
• Defining the question beforehand is crucial (does ITT answer it?)
• HTA raises additional challenges for design/methods of analysis
• IV methods promising - randomisation is a valid instrument
• Consider sensitivity analysis to departures from identifying assumptions
Discussion
theta.lshtm.ac.uk