29th European Congress of Pathology (ECP 2017) … · Department of Surgical Pathology Aichi...
45
The Paris System for Reporting Urinary Cytology: The Concept and Management Toyonori Tsuzuki MD, PhD Professor and Chair Department of Surgical Pathology Aichi Medical University Hospital Tuesday, September 5, 2017 29th European Congress of Pathology (ECP 2017) Amsterdam RAI.
Transcript of 29th European Congress of Pathology (ECP 2017) … · Department of Surgical Pathology Aichi...
The Paris System for
Reporting Urinary Cytology:
The Concept and
Management
Toyonori Tsuzuki MD, PhDProfessor and Chair
Department of Surgical Pathology
Aichi Medical University Hospital
Tuesday, September 5, 2017
29th European Congress of Pathology (ECP 2017)
Amsterdam RAI.
The author has no conflict of interest to disclose
with respect to this presentation.
The 29th European Congress of
Pathology
Presenter: Toyonori Tsuzuki
Conflict of Interest (COI)
Department of Surgical Pathology
Aichi Medical University Hospital
Outline of the presentation
• Why to standardize, why Paris?
• What is the guiding principle?
• What are diagnostic categories?
• What are the criteria?
Department of Surgical Pathology
Aichi Medical University Hospital
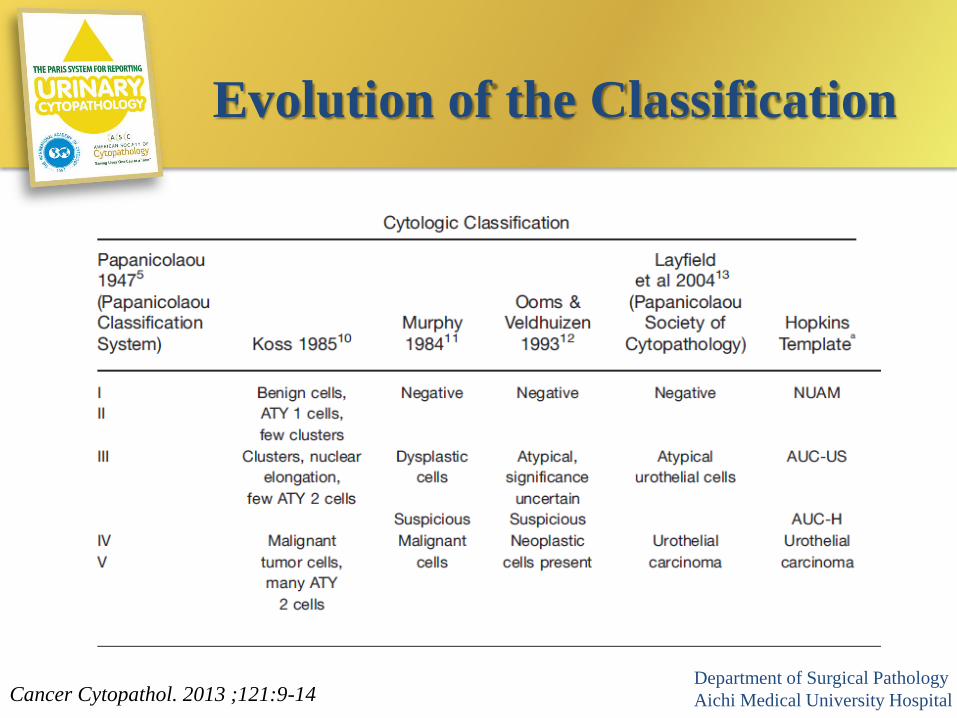
Evolution of the Classification
Cancer Cytopathol. 2013 ;121:9-14Department of Surgical Pathology
Aichi Medical University Hospital
• Reproducibility
• Improvement of communication
• Atypical cells
– Wide intraobserver variability
• Nationally rates of atypical vary among
institutions
– Range from 2% to 30%
Why standardize reporting of
urinary cytology?
Department of Surgical Pathology
Aichi Medical University Hospital
Where did we start?
• 18th International Congress of Cytology, Paris, May, 2013
– Outline of the Paris System for Reporting Urinary
Cytopathology
– Ultimate goal – detection of high grade urothelial carcinoma
(HGUC)
• Numerous face-to-face meetings among 49 members, 28 from 10
countries including USA, Canada, France, Italy, Japan, Korea,
Luxembourg, Slovenia, Switzerland, and the UK.
Department of Surgical Pathology
Aichi Medical University Hospital
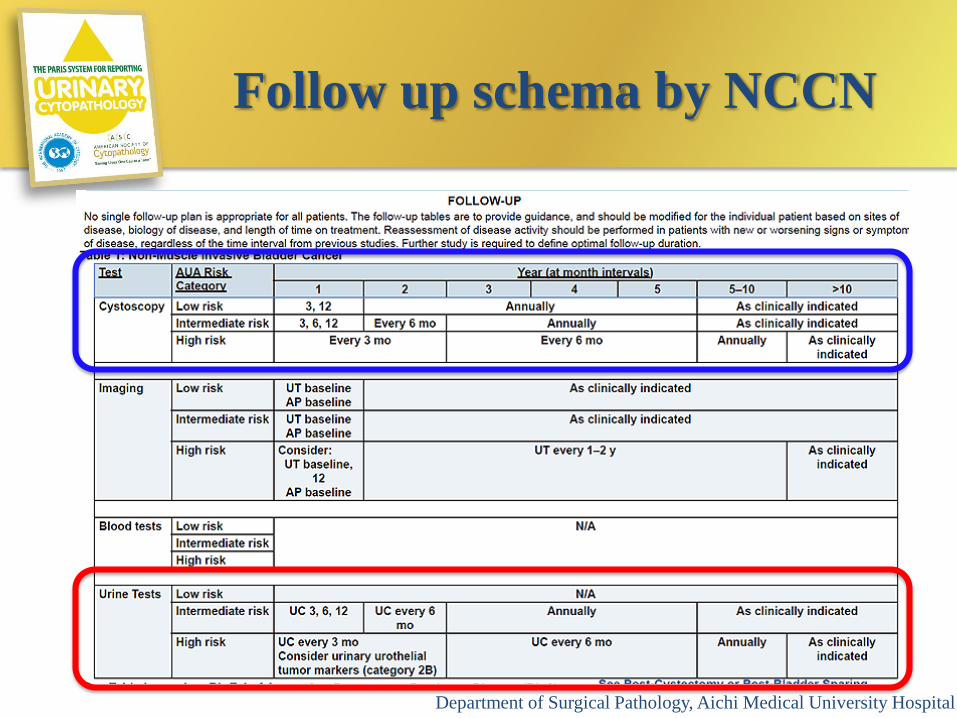
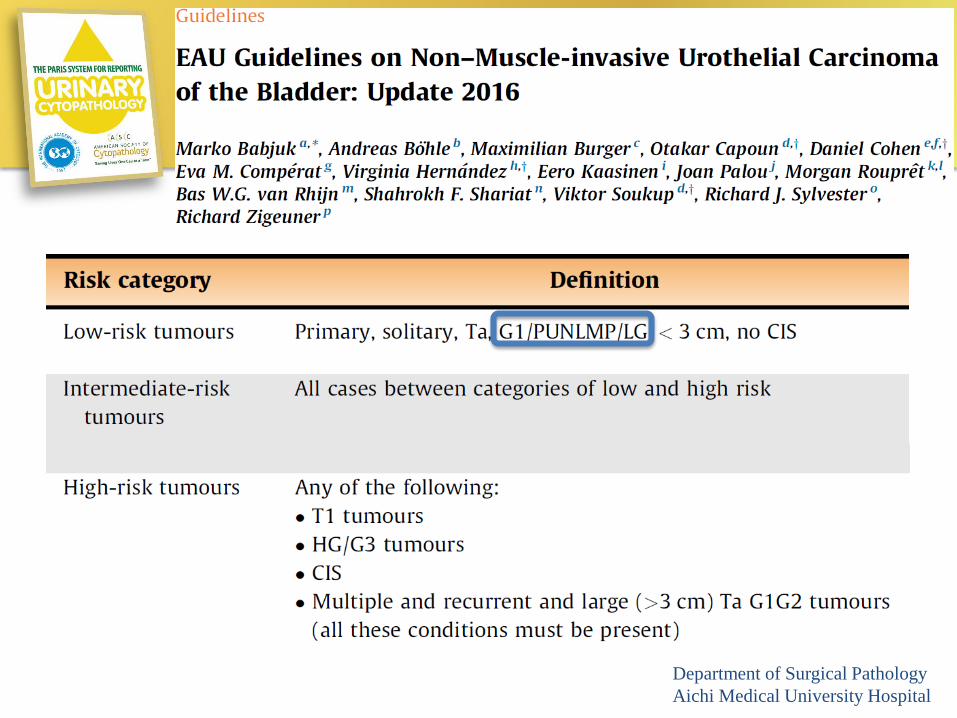
Follow up schema by NCCN
Department of Surgical Pathology, Aichi Medical University Hospital
What is high grade urothelial
carcinoma (HGUC)?
• Life threatened cancer
• Need definitive therapies
• Need strict follow up
• Including urothelial carcinoma in situ
(CIS) and invasive urothelial carcinoma
(with divergent differentiation)
Department of Surgical PathologyAichi Medical University Hospital
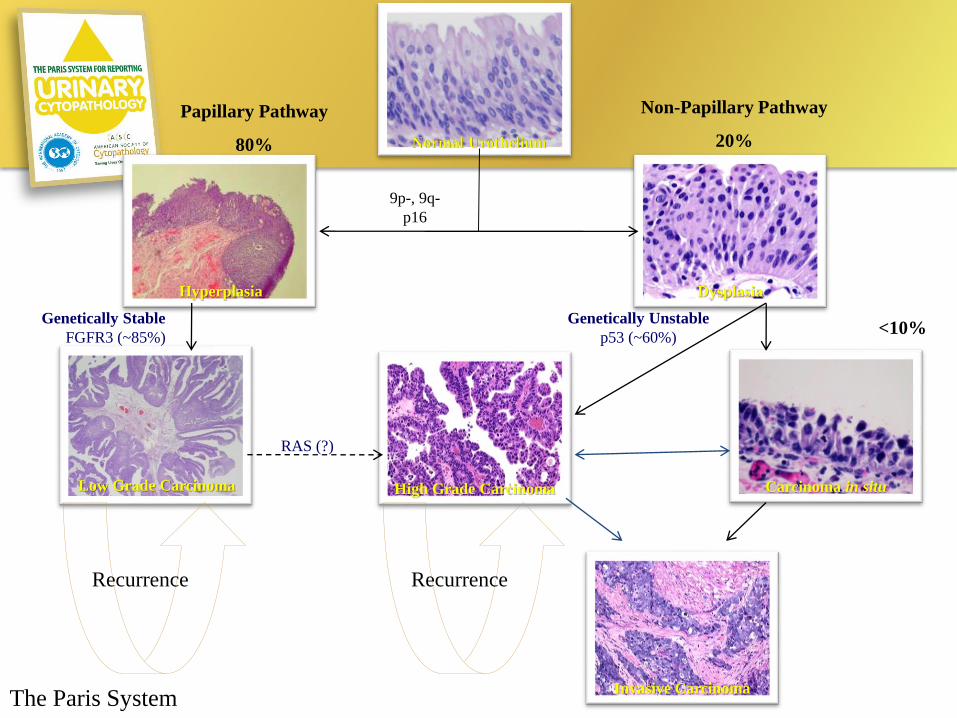
Normal Urothelium
Hyperplasia Dysplasia
Low Grade Carcinoma High Grade Carcinoma Carcinoma in situ
Invasive Carcinoma
Papillary Pathway
80%
Non-Papillary Pathway
20%
9p-, 9q-
p16
Genetically Stable
FGFR3 (~85%)
Genetically Unstable
p53 (~60%)<10%
Recurrence Recurrence
RAS (?)
The Paris System
Chapters in the Book
I. Adequacy
II. Negative for High Grade Urothelial Carcinoma
III. Atypical Urothelial Cells
IV. Suspicious for High Grade Urothelial Carcinoma
V. High Grade Urothelial Carcinoma
VI. Low Grade Urothelial Neoplasm
VII. Other malignancies, both primary and secondary
VIII.Ancillary Studies
IX. Clinical management
X. Preparatory techniques relative to Urinary Tract samples
Department of Surgical Pathology
Aichi Medical University Hospital
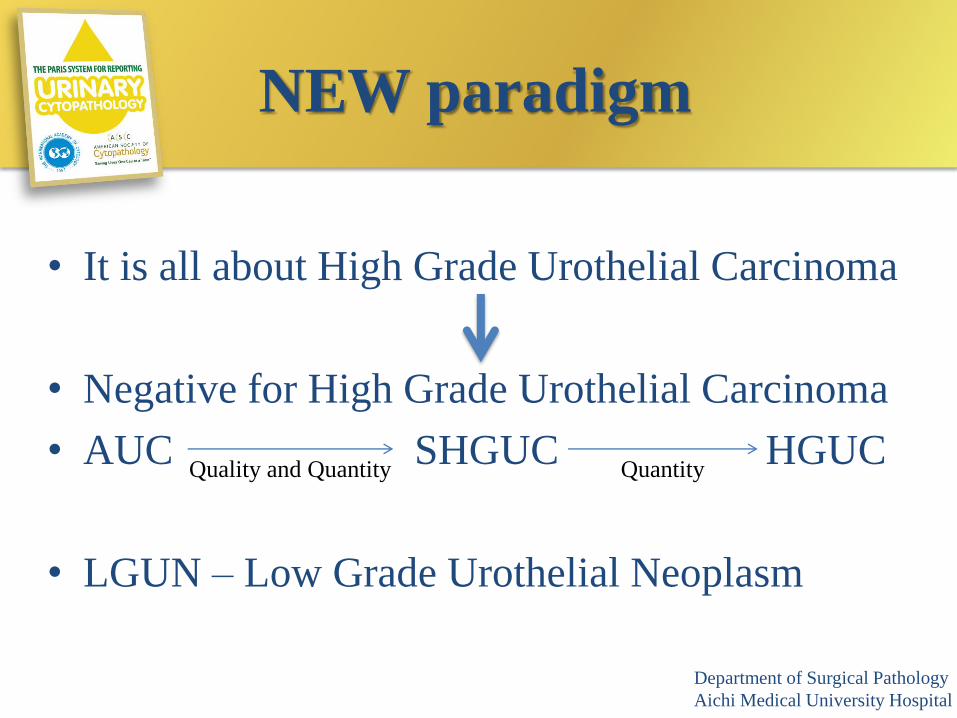
NEW paradigm
• It is all about High Grade Urothelial Carcinoma
• Negative for High Grade Urothelial Carcinoma
• AUC SHGUC HGUC
• LGUN – Low Grade Urothelial Neoplasm
Quality and Quantity Quantity
Department of Surgical Pathology
Aichi Medical University Hospital
Adequacy
Department of Surgical Pathology
Aichi Medical University Hospital
Adequacy
• Most of cytology systems require
minimum cell number.
• Minimum requirement for voided urine is
needed.
• What is “unsatisfactory” in voided urine?
• Which is better urine volume or cell
number?Department of Surgical Pathology
Aichi Medical University Hospital
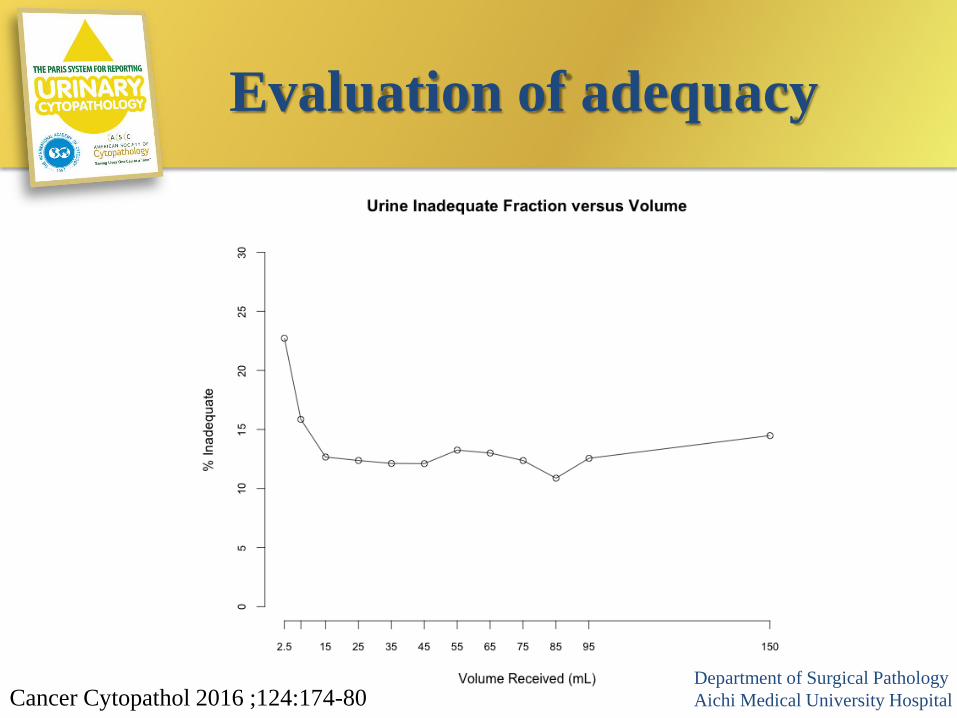
Evaluation of adequacy
Cancer Cytopathol 2016 ;124:174-80Department of Surgical Pathology
Aichi Medical University Hospital
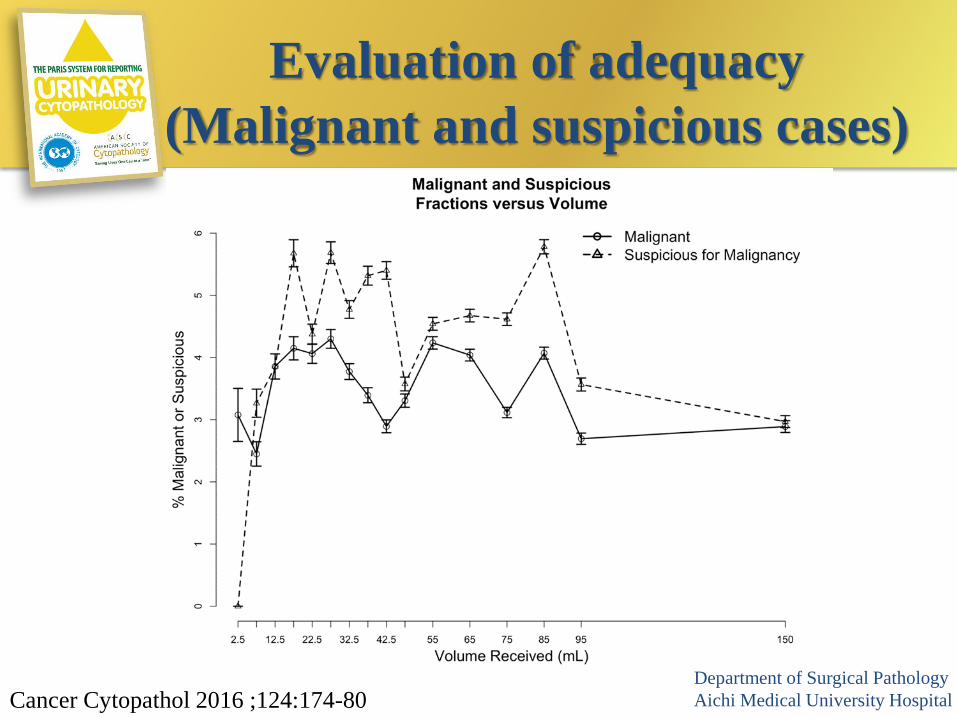
Evaluation of adequacy
(Malignant and suspicious cases)
Cancer Cytopathol 2016 ;124:174-80Department of Surgical Pathology
Aichi Medical University Hospital
TPS requires ”30ml”,
at least.
Adequacy
Department of Surgical Pathology
Aichi Medical University Hospital

Negative for HGUC
• Negative for High Grade Urothelial Carcinoma
– This diagnostic category will include cases where “low
grade urothelial carcinoma can not be excluded”
• If there is a cause for “atypia” i.e. urolithiasis,
treatment related changes etc. – it is negative!
Department of Surgical PathologyAichi Medical University
Various conditions:
Negative for HGUC
• Benign urothelial and squamous cells
• Reactive urothelial cells
• Polyoma Viral Cytopathic Effect: Decoy cells
• Benign Urothelial Tissue Fragments (BUTF)
• Post-therapy effect
• Changes associated with lithsiasis
Department of Surgical PathologyAichi Medical University
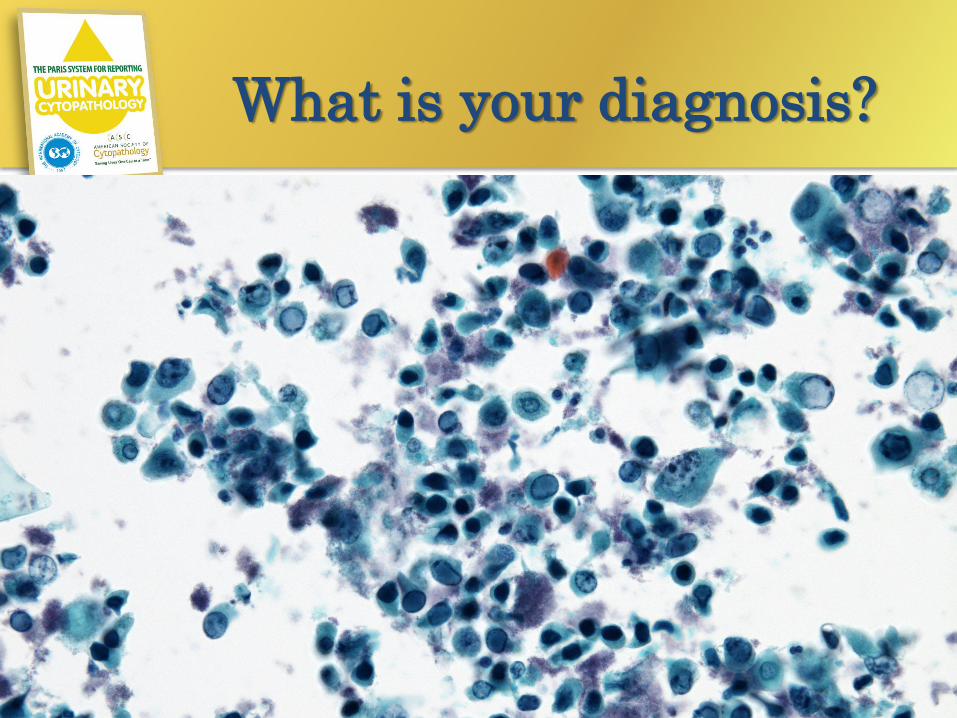
What is your diagnosis?
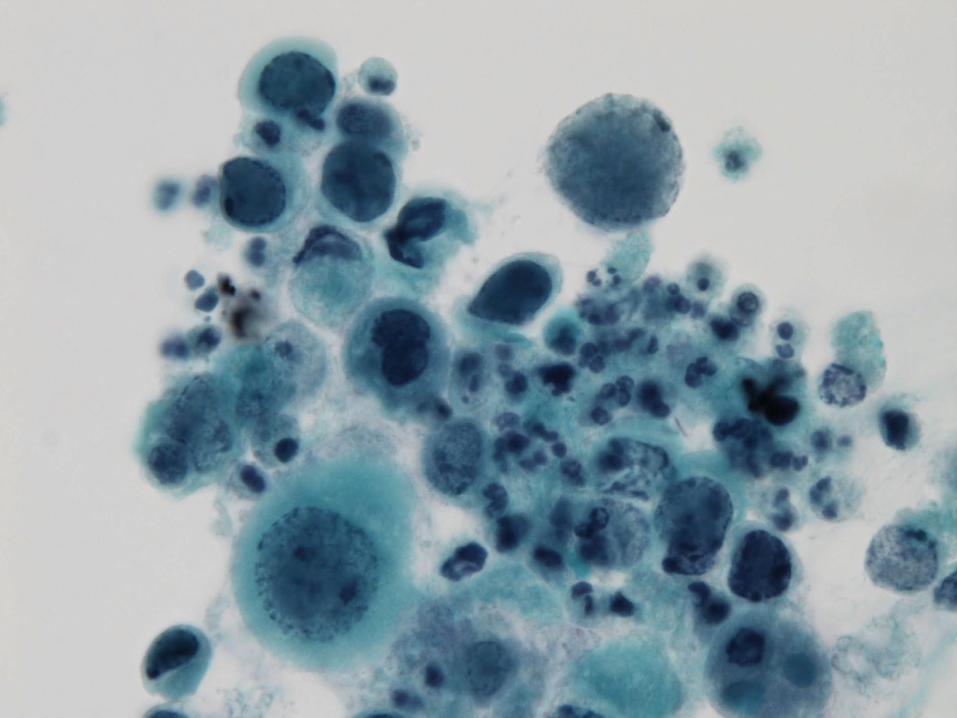
What is your diagnosis?
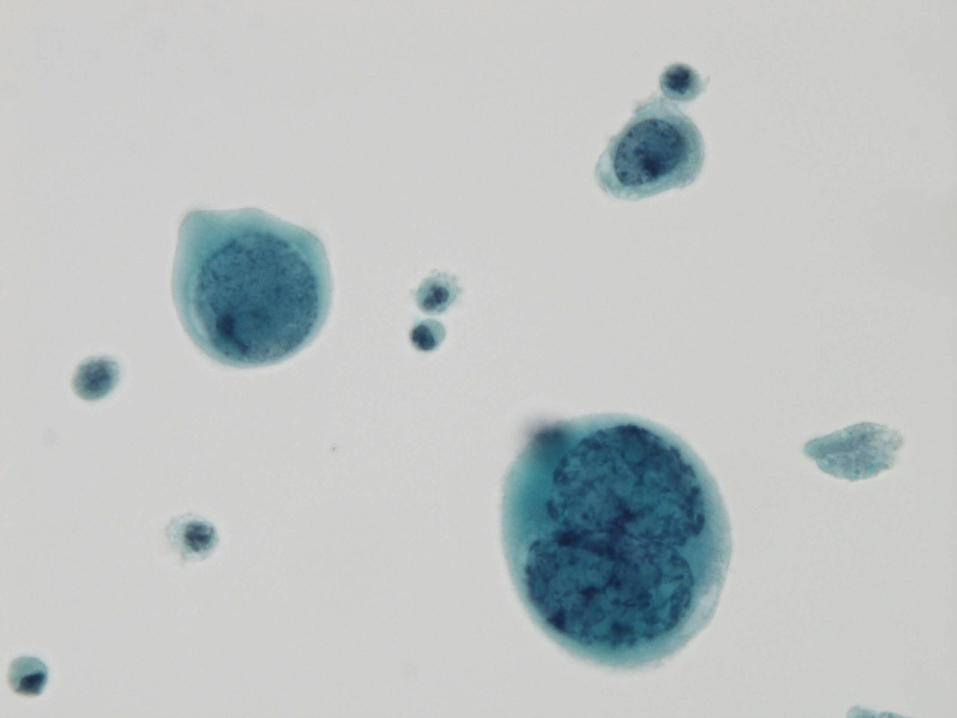
Decoy cells!
Department of Surgical PathologyAichi Medical University
Clinical history
• Patient: 50 years, Male
• The patient received chemotherapy for
malignant lymphoma.
• During his chemotherapy, microhematuria
was pointed out.
• A urine cytology test were performed
Department of Surgical PathologyAichi Medical University
Are decoy cells
diagnosed correctly?
• BK virus infection in urinary tract is well-known in immunocompromised patients.
• Decoy cell is BK virus infected epithelial cell.
• TPS recommend to diagnose decoy cell as negative, not atypical.
• However, decoy cells might be diagnosed as “HGUC” in some case .
Department of Surgical PathologyAichi Medical University
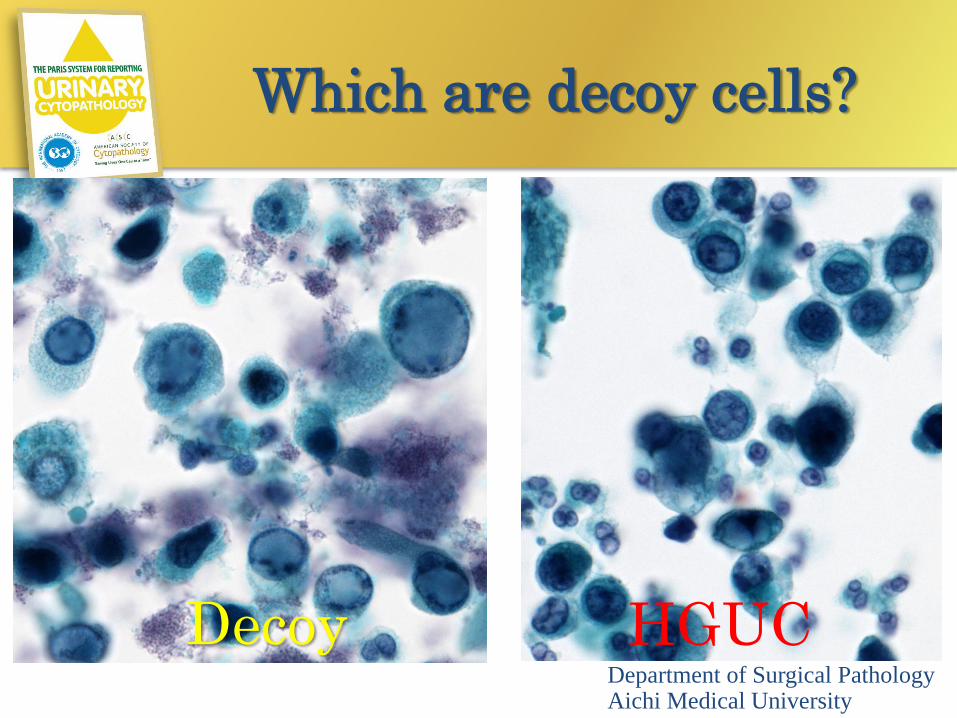
Which are decoy cells?
Decoy HGUCDepartment of Surgical PathologyAichi Medical University
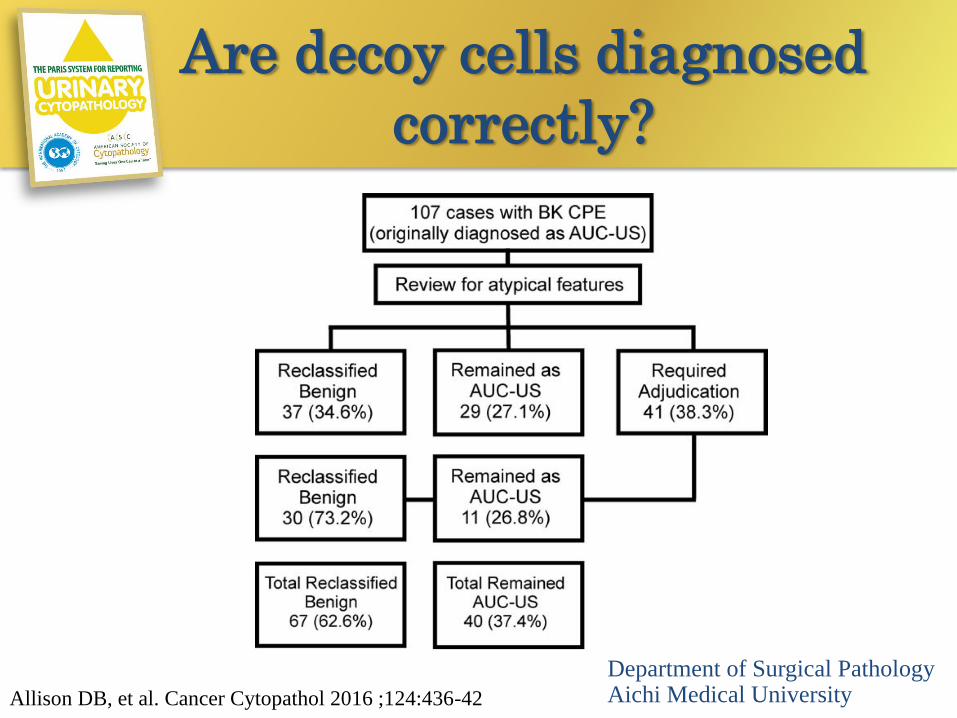
Are decoy cells diagnosed
correctly?
Department of Surgical PathologyAichi Medical UniversityAllison DB, et al. Cancer Cytopathol 2016 ;124:436-42
• N/C ratio
• Hyperchromasia
• Plumped chromatin
• Nuclear membrane contour
• Size DOESN’T matter!
The Item of Morphological
Criteria in TPS
Department of Surgical PathologyAichi Medical University
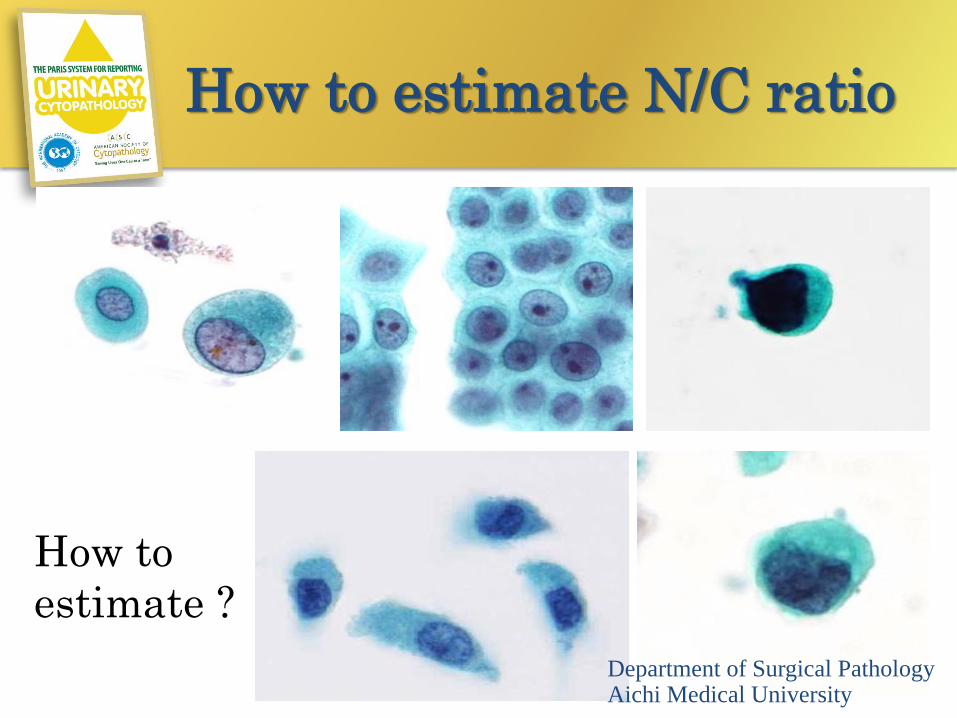
How to estimate N/C ratio
Department of Surgical PathologyAichi Medical University
How to
estimate ?

N/C ratio =b/a
b
aa
b
ba
ab
a bDepartment of Surgical PathologyAichi Medical University
Do you
always
calculate?
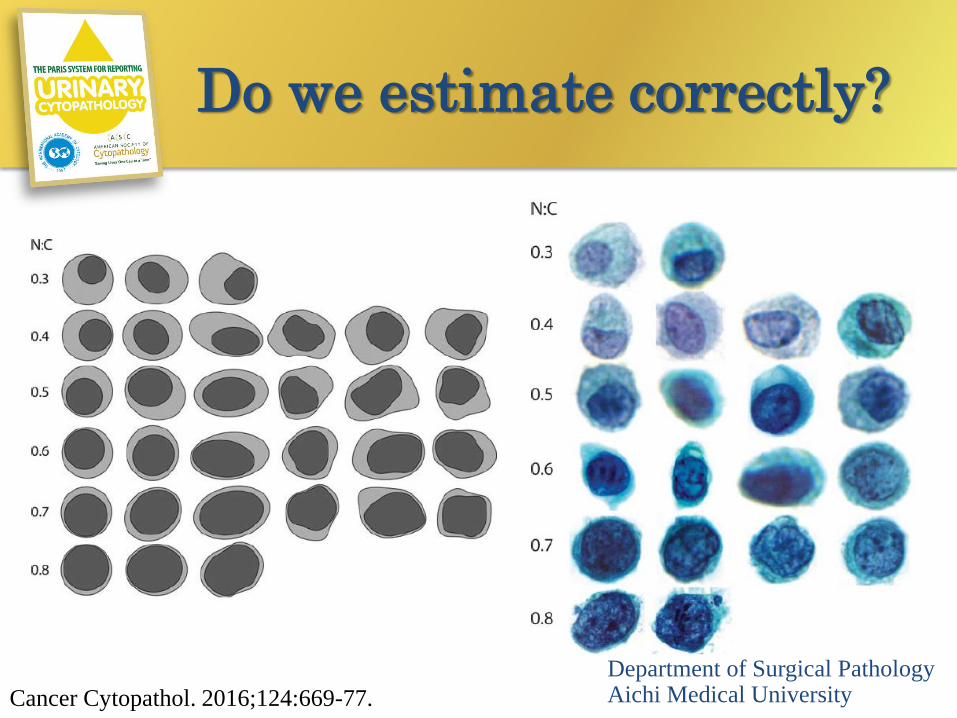
Do we estimate correctly?
Department of Surgical PathologyAichi Medical UniversityCancer Cytopathol. 2016;124:669-77.
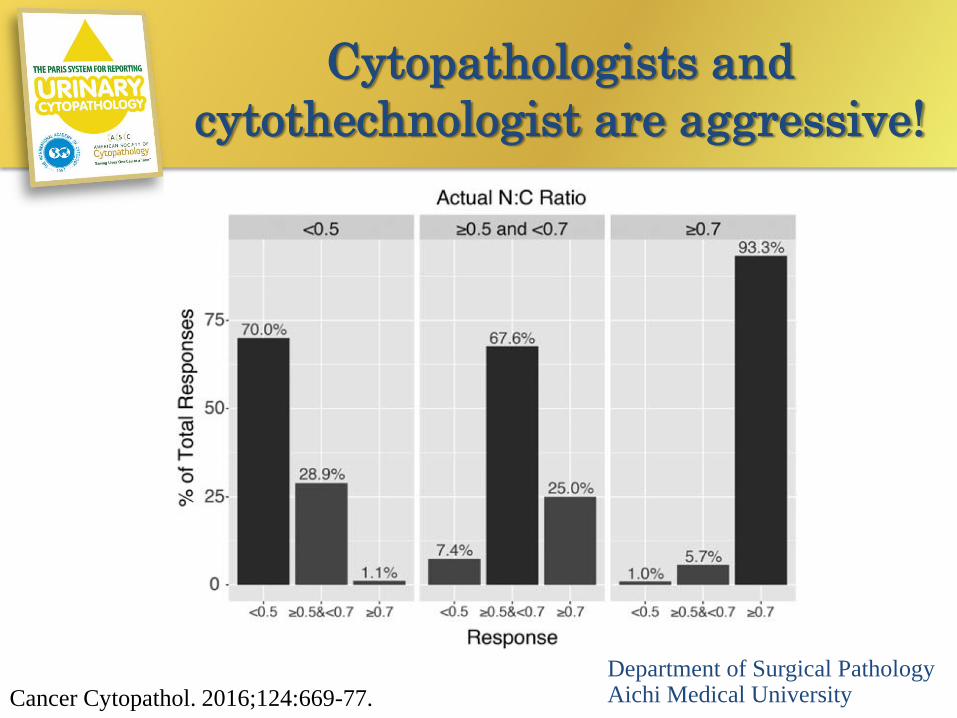
Cytopathologists and
cytothechnologist are aggressive!
Department of Surgical PathologyAichi Medical UniversityCancer Cytopathol. 2016;124:669-77.
• N/C ratio of 0.5 - 0.7
• Nuclear hyperchromasia, mild -
moderate
• Irregular granular chromatin
• Irregular nuclear membranes:
shapes and thickness
• Degenerated cells of uncertain atypia
The criteria of AUC
Department of Surgical PathologyAichi Medical University
• N/C ratio of at least 0.7
• Marked hyperchromasia
• Markedly clumped chromatin
• Deformed nuclear membranes
• Cells of HGUC but only 5-10 of them
• Size DOESN’T matter!
The criteria of SHGUC
Department of Surgical PathologyAichi Medical University
• N/C ratio at least 0.7
• Very hyperchromatic nuclei
• Grossly clumped chromatin
• Irregular nuclear contour
• Eccentric nuclei
• At least 10 cells
The criteria of HGUC
Department of Surgical PathologyAichi Medical University

Hyperchromasia, Clumped chromatin, Deformed nuclear membranes
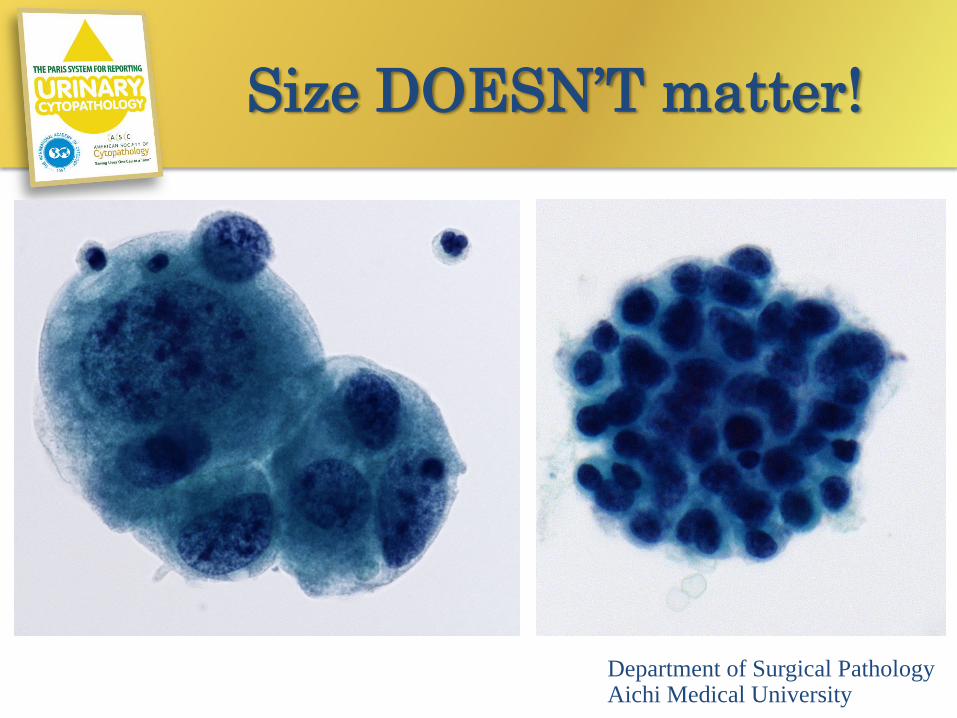
Size DOESN’T matter!
Department of Surgical PathologyAichi Medical University
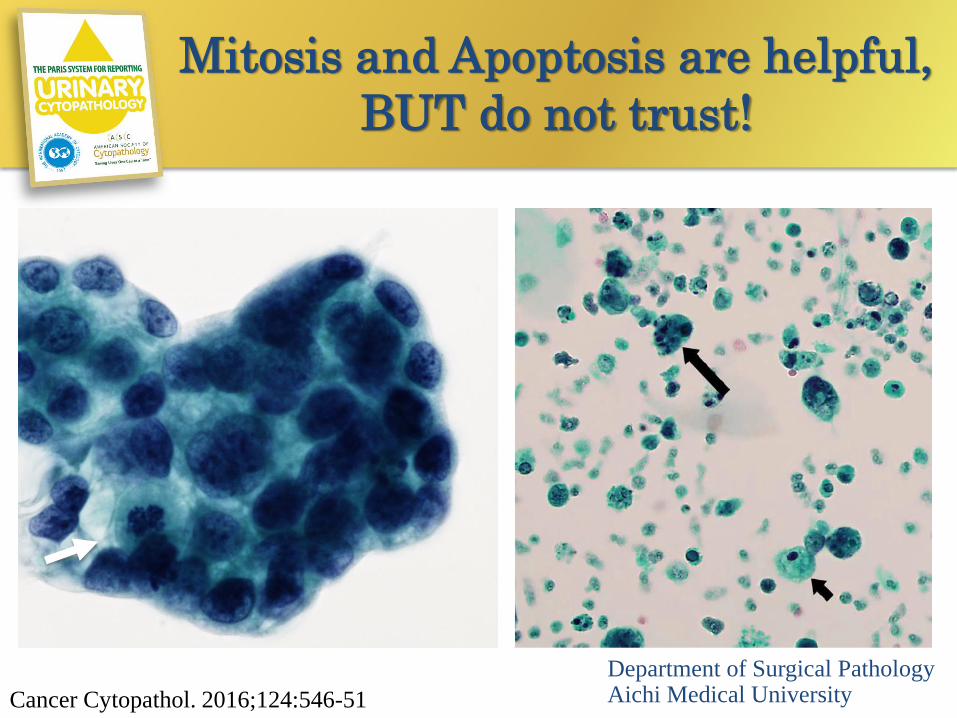
Mitosis and Apoptosis are helpful,
BUT do not trust!
Department of Surgical PathologyAichi Medical UniversityCancer Cytopathol. 2016;124:546-51
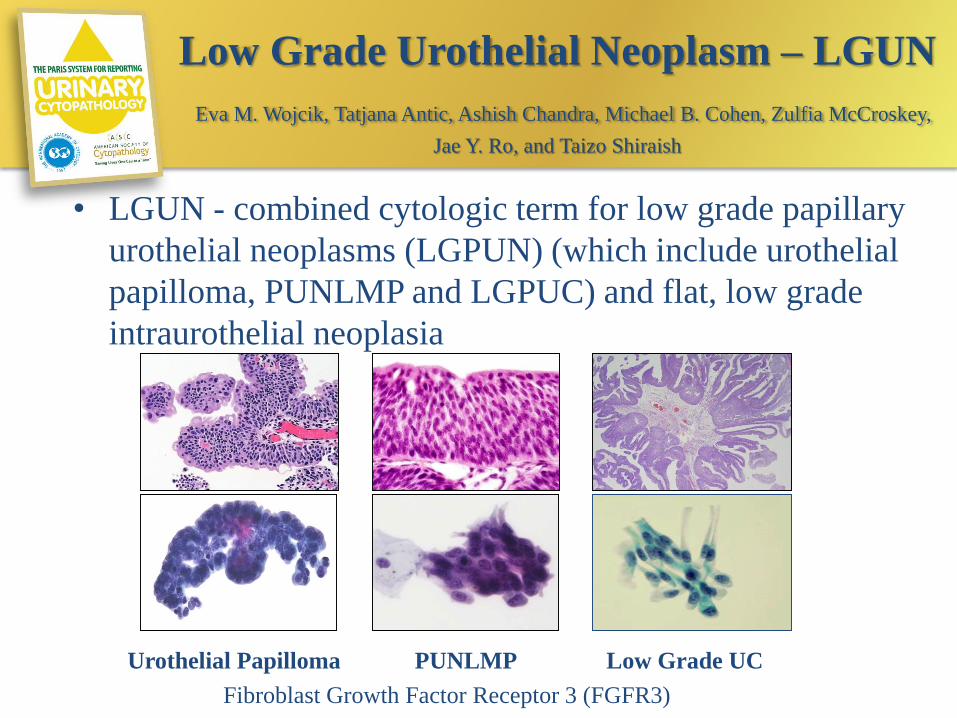
Low Grade Urothelial Neoplasm – LGUN
Eva M. Wojcik, Tatjana Antic, Ashish Chandra, Michael B. Cohen, Zulfia McCroskey,
Jae Y. Ro, and Taizo Shiraish
• LGUN - combined cytologic term for low grade papillary
urothelial neoplasms (LGPUN) (which include urothelial
papilloma, PUNLMP and LGPUC) and flat, low grade
intraurothelial neoplasia
Urothelial Papilloma PUNLMP Low Grade UC
Fibroblast Growth Factor Receptor 3 (FGFR3)
Why we avoid LGUC
• Almost impossible to diagnose without a
mini-biopsy with fibrovascular core
• Cytologically normal nuclei
• Is it truly a carcinoma?
• More common than HGUC
• BUT, not life threatening
Department of Surgical PathologyAichi Medical University

LGUN

LGUN
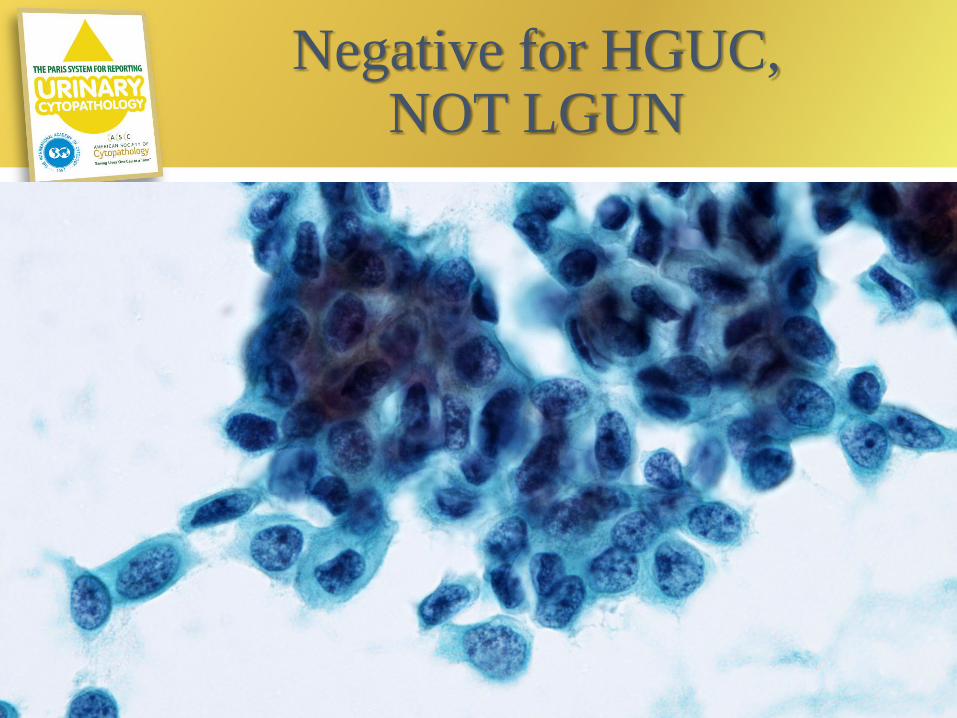
Negative for HGUC, NOT LGUN
Summary
• The aim of TPS is standardization of criteria
and reporting.
• The main focus of TPS is detecting HGUC.
• Adequacy is important.
• Pitfall
– Decoy cell and other causes
• The presence of fibrovascular core is required
to diagnose LGUN.
Department of Surgical PathologyAichi Medical University
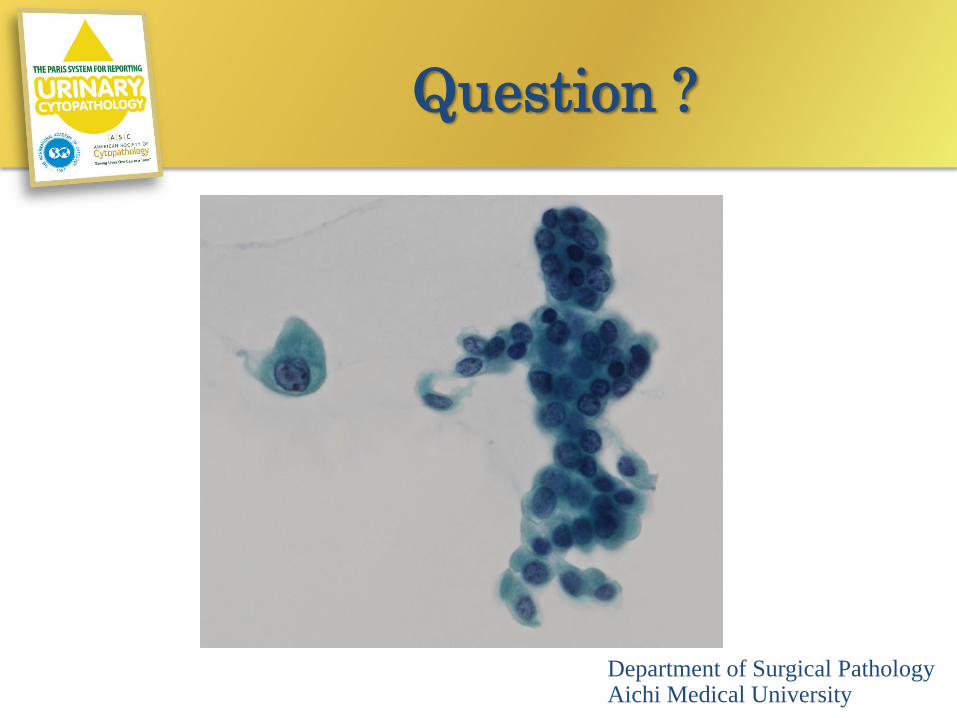
Question ?
Department of Surgical PathologyAichi Medical University


![Future of Toxicologic Pathology in the Post-Genomic Era · The 29th Annual Meeting of the Japanese Society of Toxicologic Pathology January 31st [Thursday] - February 1st [Friday]](https://static.fdocuments.us/doc/165x107/5b4306687f8b9af5798bad86/future-of-toxicologic-pathology-in-the-post-genomic-the-29th-annual-meeting.jpg)