211.full
3
Case report A case of giant benign localized fibrous tumor of the pleura 1 Mehmet Bic ¸er*, Sadık Yaldız, Soner Gu ¨rsoy, Metin U ¨ lg ˘an Department of Thoracic Surgery, Chest Diseases and Thoracic Surgery Teaching Hospital (Go ¨g ˘u ¨s Hastalıkları ve Cerrahisi Egitim Hastanesi), I ˙ zmir, Turkey Received 15 December 1997; revised version received 28 April 1998; accepted 13 May 1998 Abstract A 60-year-old man had noted exertional dyspnea and left anterior chest pain. A chest roentgenogram showed the presence of a giant mass and computed tomography (CT) of the chest confirmed the mass with an inhomogeneous density in the left hemithorax. A transthoracic TruCut needle biopsy of the mass showed benign fibrous tissue. The patient underwent a thoracotomy. A tumor arose from the visceral pleura of left lower lobe and pedinculated. Size of the tumor was 19 × 18 × 7 cm and weighed 1500 g. It was successfully resected. The pathological diagnosis of the tumor was benign localized fibrous tumor of the pleura. 1998 Elsevier Science B.V. All rights reserved Keywords: Benign mesothelioma; Pleural neoplasms 1. Case report Localized fibrous tumors of the pleura are rare neo- plasms. Previously these tumors have mostly been classified as localized mesotheliomas of the pleura, either benign or malignant [1]. Pleural fibrous tumors are generally malig- nant and are associated with asbestos exposure, but benign tumors do occur. The cell origin of these tumors is a non- committed mesenchymal cell present in the areolar tissue subadjacent to the mesothelial cells of the pleura [1]. We report the case of a patient with localized fibrous tumor of the pleura, which is notable for its rare massive size. A 60-year-old male patient complained of exertional dys- pnea and left-sided chest pain at the time of admission to hospital. PA and lateral chest roentgenograms showed pre- sence of a giant mass and computed tomography (CT) of the chest confirmed the mass to have an inhomogeneous density and irregular central calcification in the left hemithorax (Fig. 1). Hemogram and biochemical findings were normal. At physical examination breath sounds were absent on left lower zone. Bronchoscopy showed extrinsic compression at the level of left lower lobe bronchus. Spirometry showed restrictive pulmonary defect with a vital capacity of 1500 cm 3 . A transthoracic TruCut needle biopsy of the mass showed benign fibrous tissue. Left posterolateral thoracotomy was performed for the resection of the tumor. The tumor was arising from the visceral pleura on a stalk and projected into the pleural space in a pedinculated manner. A thin membranous capsule was present. Size of the tumor was 19 × 18 × 7 cm and weighed 1500 g. On the cut section, the mass was composed of dense, whorled fibrous tissue with irregular central calci- fication. A chest roentgenogram on the tenth postoperative day showed reexpansion of the lung. Pathological diagnosis of the tumor was benign localized fibrous tumor of the pleura (Fig. 2). 2. Discussion Localized benign fibrous tumors of the pleura are approximately one-third of malignant mesothelioma [2]. Unlike malignant form, benign fibrous tumor of the pleura appears to be unrelated to asbestos exposure [3]. There was no asbestos exposure in our case. The localized form of the fibrous tumors are usually considered benign, but malignant cases have been reported [4]. European Journal of Cardio-thoracic Surgery 14 (1998) 211–213 1010-7940/98/$19.00 1998 Elsevier Science B.V. All rights reserved PII S1010-7940(98)00166-3 * Corresponding author. 180/1 Sok. No. 3 A Blok D.1, 35040 Bornova I ˙ zmir, Turkey. Tel.: +90 232 3428299. 1 Presented at the 1st International Congress of Thorax Surgery, Athens, Greece, July 1–8, 1997.
description
teori
Transcript of 211.full
-
Case report
A case of giant benign localized fibrous tumor of the pleura1
Mehmet Bicer*, Sadk Yaldz, Soner Gursoy, Metin U lganDepartment of Thoracic Surgery, Chest Diseases and Thoracic Surgery Teaching Hospital
(Gogus Hastalklar ve Cerrahisi Egitim Hastanesi), Izmir, Turkey
Received 15 December 1997; revised version received 28 April 1998; accepted 13 May 1998
Abstract
A 60-year-old man had noted exertional dyspnea and left anterior chest pain. A chest roentgenogram showed the presence of a giant massand computed tomography (CT) of the chest confirmed the mass with an inhomogeneous density in the left hemithorax. A transthoracicTruCut needle biopsy of the mass showed benign fibrous tissue. The patient underwent a thoracotomy. A tumor arose from the visceralpleura of left lower lobe and pedinculated. Size of the tumor was 19 18 7 cm and weighed 1500 g. It was successfully resected. Thepathological diagnosis of the tumor was benign localized fibrous tumor of the pleura. 1998 Elsevier Science B.V. All rights reserved
Keywords: Benign mesothelioma; Pleural neoplasms
1. Case report
Localized fibrous tumors of the pleura are rare neo-plasms. Previously these tumors have mostly been classifiedas localized mesotheliomas of the pleura, either benign ormalignant [1]. Pleural fibrous tumors are generally malig-nant and are associated with asbestos exposure, but benigntumors do occur. The cell origin of these tumors is a non-committed mesenchymal cell present in the areolar tissuesubadjacent to the mesothelial cells of the pleura [1]. Wereport the case of a patient with localized fibrous tumor ofthe pleura, which is notable for its rare massive size.
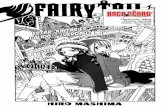
A 60-year-old male patient complained of exertional dys-pnea and left-sided chest pain at the time of admission tohospital. PA and lateral chest roentgenograms showed pre-sence of a giant mass and computed tomography (CT) of thechest confirmed the mass to have an inhomogeneous densityand irregular central calcification in the left hemithorax(Fig. 1). Hemogram and biochemical findings were normal.At physical examination breath sounds were absent on leftlower zone. Bronchoscopy showed extrinsic compression at
the level of left lower lobe bronchus. Spirometry showedrestrictive pulmonary defect with a vital capacity of 1500cm3. A transthoracic TruCut needle biopsy of the massshowed benign fibrous tissue.
Left posterolateral thoracotomy was performed for theresection of the tumor. The tumor was arising from thevisceral pleura on a stalk and projected into the pleuralspace in a pedinculated manner. A thin membranous capsulewas present. Size of the tumor was 19 18 7 cm andweighed 1500 g. On the cut section, the mass was composedof dense, whorled fibrous tissue with irregular central calci-fication. A chest roentgenogram on the tenth postoperativeday showed reexpansion of the lung. Pathological diagnosisof the tumor was benign localized fibrous tumor of thepleura (Fig. 2).
2. Discussion
Localized benign fibrous tumors of the pleura areapproximately one-third of malignant mesothelioma [2].Unlike malignant form, benign fibrous tumor of the pleuraappears to be unrelated to asbestos exposure [3]. There wasno asbestos exposure in our case. The localized form of thefibrous tumors are usually considered benign, but malignantcases have been reported [4].
European Journal of Cardio-thoracic Surgery 14 (1998) 211213
1010-7940/98/$19.00 1998 Elsevier Science B.V. All rights reservedPII S1010-7940(98)00166-3
* Corresponding author. 180/1 Sok. No. 3 A Blok D.1, 35040 BornovaIzmir, Turkey. Tel.: +90 232 3428299.
1 Presented at the 1st International Congress of Thorax Surgery, Athens,Greece, July 18, 1997.
-
Many patients with localized fibrous tumors are asympto-matic; cough, chest pain, and dyspnea occur occasionally,especially with larger tumors [4]. It has slightly higher inci-dence in females than males. The peak incidence is in thesixth and seventh decades of life [5].
These tumors appear as encapsulated, firm and lobulatedmasses with a characteristic whorled appearance on cut sur-face. Watts et al. reported a giant benign mesothelioma
which was 1460 g [6]. In our case the tumor was also ashuge as the tumor Watts et al. reported, 1500 g. Briselli et al.reported that the small tumors were usually nodular withinthe lung and the large tumors tended to be pedinculatedwithin the pleural cavity, arising from the parietal pleura[5]. A giant tumor arose from the visceral pleura in our case.
Diagnosis is difficult in these tumors. The nature of thesolitary lesion is established most often at the time of thor-
Fig. 1. Computed tomography of the chest shows the mass with an inhomogeneous density and irregular central calcification in the left hemithorax.
Fig. 2. Benign fibrous pleural tumor. Short spindle cells are poorly oriented within a fibrous stroma. (Hematoxylin and eosin stain; original magnification 400).
212 M. Bicer et al. / European Journal of Cardio-thoracic Surgery 14 (1998) 211213
-
acotomy and subsequent histologic examination [1]. When atumor is very large, however, the site of origin is frequentlydifficult or impossible to establish on conventional roent-genograms and even on CT [7]. As a result of this, we triedto diagnose the mass with thoracic CT and abdominal CT.Although it is not recommended, we performed transthor-acic TruCut needle biopsy but it was not sufficient for pre-cise diagnosis.
Infrequently a pleural effusion may be present. Englandet al. reported that 8% of 138 patients had a pleural effusion[8]. We have demonstrated sanguineous pleural effusion atthe time of operation.
Treatments of benign fibrous tumors of the pleura consistof adequate local excision. Great care must be taken at thetime of operation because of the highly vascular pedicle [6].Although histologically benign, Briselli et al. reported thatthe mortality rate is about 12% owing to operative mortality,with removal or compression of mediastinal structures lead-ing to fatal cardiopulmonary complications [5]. Periodiclong-term follow-up is necessary with these tumors. Fivein 78 cases which were diagnosed to be benign histologi-cally at operation, had recurrence later in Japan [9]. After 2years follow-up, our patient is healthy and has no sign ofrecurrence.
References
[1] Shields TW. Localized fibrous tumor of the pleura. In: Shields TW,ed. General thoracic surgery. Malvern: Williams and Wilkins, 1994:722730.
[2] Albelda SM, Sterman DH, Litzky LA. Malignant mesothelioma andother primary pleural tumors. In: Fishman AP, Elias JA, Fishman JA,Grippi MA, Kaiser LR, Senior RM, eds. Fishmans pulmonarydiseases and disorders. New York: McGraw-Hill, 1998:14531466.
[3] Antman KH. Clinical presentation and natural history of benign andmalignant mesothelioma. Semin Oncol 1989;8:313320.
[4] Okike N, Bernatz PE, Woolner LB. Localized mesothelioma of thepleura: benign and malignant variants. J Thorac Cardiovasc Surg1978;75:363372.
[5] Briselli M, Mark EJ, Dickersin GR. Solitary fibrous tumors of thepleura: eight new cases and review of 360 cases in the literature.Cancer 1981;47:26782689.
[6] Watts DM, Jones GP, Bowman GA, Olsen DJ. Giant benignmesothelioma. Ann Thorac Surg 1989;48:590591.
[7] Fraser RS, Pare JAP, Fraser RG, Pare PD, ed. Synopsis of diseases ofthe chest. Philadelphia: WB Saunders, 1994:868895.
[8] England DM, Hochholzer L, McCarthy MJ. Localized benign andmalignant fibrous tumors of the pleura: a clinicopathologic review of223 cases. Am J Surg Pathol 1989;13:640644.
[9] Hatta T, Ohyabu H, Kurisu S, Tachibana S, Kita Y, Oki K, Okada M,Uematsu M, Matsuda S, Eno K. A case of localized pleural meso-thelioma. Kyobu Geka 1991;44 (4):344346.
213M. Bicer et al. / European Journal of Cardio-thoracic Surgery 14 (1998) 211213