
21 d of normobaric hypoxia and bed rest …abr.ijs.si/upload/1495028428-2017_Strewe et...
10
Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ists20 Download by: [178.172.42.65] Date: 12 April 2017, At: 01:06 Stress The International Journal on the Biology of Stress ISSN: 1025-3890 (Print) 1607-8888 (Online) Journal homepage: http://www.tandfonline.com/loi/ists20 PlanHab study: assessment of psycho- neuroendocrine function in male subjects during 21 d of normobaric hypoxia and bed rest C. Strewe, R. Zeller, M. Feuerecker, M. Hoerl, I. Kumprej, A. Crispin, B. Johannes, T. Debevec, I. Mekjavic, G. Schelling & A. Choukèr To cite this article: C. Strewe, R. Zeller, M. Feuerecker, M. Hoerl, I. Kumprej, A. Crispin, B. Johannes, T. Debevec, I. Mekjavic, G. Schelling & A. Choukèr (2017) PlanHab study: assessment of psycho-neuroendocrine function in male subjects during 21 d of normobaric hypoxia and bed rest, Stress, 20:2, 131-139, DOI: 10.1080/10253890.2017.1292246 To link to this article: http://dx.doi.org/10.1080/10253890.2017.1292246 Accepted author version posted online: 06 Feb 2017. Published online: 05 Mar 2017. Submit your article to this journal Article views: 28 View related articles View Crossmark data
Transcript of 21 d of normobaric hypoxia and bed rest …abr.ijs.si/upload/1495028428-2017_Strewe et...

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ists20
Download by: [178.172.42.65] Date: 12 April 2017, At: 01:06
StressThe International Journal on the Biology of Stress
ISSN: 1025-3890 (Print) 1607-8888 (Online) Journal homepage: http://www.tandfonline.com/loi/ists20
PlanHab study: assessment of psycho-neuroendocrine function in male subjects during21 d of normobaric hypoxia and bed rest
C. Strewe, R. Zeller, M. Feuerecker, M. Hoerl, I. Kumprej, A. Crispin, B.Johannes, T. Debevec, I. Mekjavic, G. Schelling & A. Choukèr
To cite this article: C. Strewe, R. Zeller, M. Feuerecker, M. Hoerl, I. Kumprej, A. Crispin, B.Johannes, T. Debevec, I. Mekjavic, G. Schelling & A. Choukèr (2017) PlanHab study: assessmentof psycho-neuroendocrine function in male subjects during 21 d of normobaric hypoxia and bedrest, Stress, 20:2, 131-139, DOI: 10.1080/10253890.2017.1292246
To link to this article: http://dx.doi.org/10.1080/10253890.2017.1292246
Accepted author version posted online: 06Feb 2017.Published online: 05 Mar 2017.
Submit your article to this journal
Article views: 28
View related articles
View Crossmark data

ORIGINAL RESEARCH REPORT
PlanHab study: assessment of psycho-neuroendocrine function in male subjectsduring 21d of normobaric hypoxia and bed rest
C. Strewea, R. Zellera, M. Feuereckera, M. Hoerla, I. Kumpreja,b, A. Crispinc, B. Johannesd, T. Debevecb,I. Mekjavicb, G. Schellinga and A. Chouk�era
aDepartment of Anaesthesiology, Klinikum Großhadern, University of Munich, Stress and Immunology Lab, Munich, Germany; bDepartment ofAutomation, Biocybernetics and Robotics, Jozef Stefan Institute, Ljubljana, Slovenia; cDepartment of Biometry and Epidemiology, KlinikumGroßhadern, University of Munich, Munich, Germany; dDepartment of Space Physiology, Institute of Aerospace Medicine, German AerospaceCenter (DLR), Cologne, Germany
ABSTRACTImmobilization and hypoxemia are conditions often seen in patients suffering from severe heart insuffi-ciency or primary pulmonary diseases (e.g. fibrosis, emphysema). In future planned long-duration andexploration class space missions (including habitats on the moon and Mars), healthy individuals willencounter such a combination of reduced physical activity and oxygen tension by way of technical rea-sons and the reduced gravitational forces. These overall unconventional extraterrestrial conditions canresult in yet unknown consequences for the regulation of stress-permissive, psycho-neuroendocrineresponses, which warrant appropriate measures in order to mitigate foreseeable risks. The PlanetaryHabitat Simulation Study (PlanHab) investigated these two space-related conditions: bed rest as modelof reduced gravity and normobaric hypoxia, with the aim of examining their influence on psycho-neu-roendocrine responses. We hypothesized that both conditions independently increase measures of psy-chological stress and enhance neuroendocrine markers of stress, and that these effects would beexacerbated by combined treatment. The cross-over study composed of three interventions (NBR, nor-mobaric normoxic horizontal bed rest; HBR, normobaric hypoxic horizontal bed rest; HAMB, normobarichypoxic ambulatory confinement) with 14 male subjects during three sequential campaigns separatedby 4months. The psychological state was determined through three questionnaires and principalneuroendocrine responses were evaluated by measuring cortisol in saliva, catecholamine in urine, andendocannabinoids in blood. The results revealed no effects after 3 weeks of normobaric hypoxia onpsycho-neuroendocrine responses. Conversely, bed rest induced neuroendocrine alterations that werenot influenced by hypoxia.
ARTICLE HISTORYReceived 13 June 2016Revised 1 November 2016Accepted 29 November 2016
KEYWORDSPlanetary habitat; spaceflight; bed rest;microgravity; hypoxia;psycho-neuroendocrineresponse
Introduction
In the hospital setting, hypoxic states and immobilization rep-resent regularly encountered conditions affecting health.However, healthy individuals can be exposed to acute orchronic hypoxia either through sport activities or living athigh altitudes, respectively. Such hypoxic stress has beenshown to have various effects on sleep, neuroendocrine path-ways, respiratory, and psychological functions (Richalet, 2016;Saugy et al., 2016; Zaeh et al., 2016). Persistent immobiliza-tion, in turn, influences bone metabolism, cardiovascularfunctioning, and muscle composition and thus represents astressful pathophysiological state (Arentson-Lantz et al., 2016;Yang et al., 2014).
In space research, the approved study concept of bed rest(Smith et al., 2014; Westby et al., 2016) is an acceptedmethod used in examining effects of immobilization by suit-ably mimicking a microgravity state (Barratt & Pool, 2008).The study conditions can be expanded from orbital (e.g. the
International Space Station) to lunar or Mars exploration classmissions where future manned habitat atmospheres will likelybe hypoxic in order to reduce the biological effects of radi-ation, the risk of fire, and to simplify extravehicular activities.Therefore, both immobilization and hypoxia represent phys-ical stressors of scientific relevance.
In modulating stress responses as well as the attempt tomaintain homeostasis under stress, hormonal systems such asthe hypothalamic–pituitary–adrenocortical axis (HPA) and thecatecholaminergic system play an important role (Hermanet al., 2003; Tsigos & Chrousos, 2002). Additionally, the endo-cannabinoid system (ECS), an evolutionarily old but well-con-served part of the nervous system, regulates central andperipheral physiological functions such as memory and thevegetative state (Atsak et al., 2015). Its endogenous agents,i.e. anandamide or 2-arachidonoylglycerol (2-AG), signalthrough the G-protein-coupled receptor (CB1, CB2) pathway.The ECS is activated by both psychological and physicalinsults (Feuerecker et al., 2012; Hauer et al., 2014).
CONTACT Alexander Chouk�er [email protected] Department of Anaesthesiology, University of Munich, Marchioninistrasse 15,81377 Munich, Germany� 2017 Informa UK Limited, trading as Taylor & Francis Group
STRESS, 2017VOL. 20, NO. 2, 131–139http://dx.doi.org/10.1080/10253890.2017.1292246

The interactions between both systems, the ECS and the HPA,are not completely understood. Previous studies reportedincreased glucocorticoid concentrations following activationwith suppression of the ECS (Hill et al., 2009; Romero et al.,2002). An activated ECS, in turn, reduces HPA activity afterstress exposure and is regulated by the HPA related feedbackmechanisms to restore its baseline activity levels (Wang et al.,2012). Roberts et al. (2014) demonstrated a time-dependentbiphasic interaction of both systems with an early suppressionand a late increase of HPA activity through the ECS.Furthermore, compensation for ECS signaling suppressionseems to display sexual dimorphism in mice yielding differentcoping strategies in females and males, illustrating the sys-tems’ complex and cross-linked nature.
Space flight studies have already demonstrated psycho-logical impairment caused by isolation and confinement(Eksuzian, 1999). Therefore, immobilization and hypoxia mayalso entail relevant psychological alterations, changes seen inmodified functions and interactions of the different physio-logical systems.
As a model for future extraterrestrial habitat design underreduced gravity, the present study hypothesizes that hypoxiaand bed rest can increase psycho-neuroendocrine responseswith compounding effects.
Material and methods
Study design and participants
The Planetary Habitat Simulation Study (PlanHab Study) wascarried out at the Olympic Sport Centre Planica (Ratece,Slovenia), situated at an altitude of 940m from sea level. Thestudy was approved by the Committee for Medical Ethics atthe Ministry for Health of the Republic of Slovenia, respectedthe Declaration of Helsinki and the bed rest protocols wereconducted in accordance with the criteria provided by theEuropean Space Agency (ESA, Standardization of Bed RestStudy Conditions (Version 1.5) (ESTEC contract number 20187/06/NL/VJ) 2009). These guidelines were applied during theselection of participants. Additionally, individuals with recentexposition (< 2months) to altitudes above 2000m and indi-viduals that normally reside at altitudes higher than 500mwere excluded. From the initial pool of 65 healthy male appli-cants, 14 were included in the trial. All subjects gave informedconsent prior to enrolling in the study. Given a cross-overstudy design, the 14 participants (age 26.4 ± 5.2 years); bodymass 75.9 ± 10.6 kg; height 1.80 ± 0.05m; BMI 23.5 ± 2.8 kg/m2
(mean± SD)) were exposed consecutively to all three proto-cols during a total of three campaigns beingperformed between October 2012 and October 2013: normo-baric normoxic horizontal bed rest (NBR: FiO2¼0.209%;PiO2¼133.1±0.3mmHg), normobaric hypoxic horizontal bedrest (HBR: FiO2¼0.141±0.004%; PiO2¼90.0±0.4mmHg; equiva-lent to �4000 m) and normobaric hypoxic ambulatory confine-ment (HAMB: FiO2¼0.141±0.004%; PiO2¼90.0±0.4mmHg).Three participants dropped out before the last campaign due topersonal reasons.
To ensure safety during hypoxic conditions, the partici-pants were provided with portable O2 gas analyzers (RAE
PGM-1100, San Jose, CA) with an alarm triggered at a pre-setO2 level of 13.5%. Details on establishing and maintainingthe designated hypoxic conditions have been reported previ-ously (Debevec et al., 2014).
General environmental conditions in the facility were con-trolled and remained stable during all three campaigns(ambient temperature: 24.4 ± 0.7 �C; relative humidity:53.5 ± 5.4%; ambient pressure: 684± 4mmHg).
Moreover, the participants were subjected to a standar-dized diet that was strictly applied in all three phases of eachcampaign in order to better evaluate individual body com-position, energy expenditure, and water balance. They wereserved five meals a day each day at the same time (breakfast8:00 am; snack 11:00 am; lunch 1:00 pm; snack 4:00 pm; din-ner 7:00 pm).
Each campaign lasted 21 d under applied study conditions(NBR, HBR, and HAMB) preceded by a period of 7 d for base-line data collection (BDC) and followed by a 4-day recoveryperiod during which post-intervention measurements wereobtained (R). In each experimental campaign, two subjectsbegan the designated intervention each day, and in the sameorder in all interventions. The experimental campaigns wereseparated by a 4-month wash-out period.
Blood and saliva collections to measure the endocannabi-noid and cortisol concentrations as well as the paper-formquestionnaires were carried out 2 d before the beginning ofthe intervention period (baseline data collection, BDC), atdays 2, 5, 14, and 21 during the confinement and 2 and/or4 d after the end of confinement (R2/R4). The time points forurine sampling differed only slightly due to organizationalreasons with the baseline data collection at day 1 before thecondition (BDC) and day 4 during the condition. R4 was notquantifiable due to the early departure of subjects at the endof each campaign.
Bed rest and hypoxic ambulatory restrictions
During the three campaigns, two participants wereassigned to share one room with two single beds. Bed restconditions (NBR and HBR) implicated that all daily routines(e.g. showering, toilet, leisure activities) had to be per-formed in the horizontal position and physical activity wasprohibited except for changing of the position in bed fromlateral to supine or prone, and vice versa. Continuousvideo surveillance was used to ensure strict compliancewith these regulations. Additionally, passive stretching by aphysiotherapist and mild medication (paracetamol) againstbed rest induced neck- or backache was provided ondemand.
Participants subjected to HAMB could carry out their nor-mal daily routines and move around in the confined andrestricted hypoxic area (110m2). They participated in dailyexercise sessions (30min twice a day, in the morning andafternoon) performing either stepping, cycling, or dancing asphysical activity similar to their habitual level.
In all three conditions, the circadian rhythm was standar-dized by a clock-regulated wake-up/sleep cycle (wake-up7:00 am; lights off 11:00 pm). Taking naps during day hourswas prohibited.
132 C. STREWE ET AL.

Psychological response
The quantification of each individual’s stress level and theintensity of perceived anxiety was collected by using threedifferent questionnaires completed at several time pointsthroughout the observation period.
1. KAB (short questionnaire on current stress) evaluates thestress level by benchmarking opposing adjectives indicat-ing stress or ease on a Likert scale (Mueller & Basler,1993). It was surveyed twice a day, in the morning andevening.
2. Spielberger State and Trait Anxiety Inventory (STAI) differ-entiates between the perceived anxiety in a specific situ-ation (state anxiety) and the anxiety belonging to one�scharacter (trait anxiety) (Spielberger et al., 1983). Twoparts with 20 questions each rate the answers on a 4-point scale with a global score ranging from 40 to 160.
3. Post-traumatic symptom scale 10 (PTSS-10) is a two parttest investigating feelings associated with anxiety anddepression (e.g. nightmares, pain). Part A asks for theirexistence in the last month and comprises of yes or noanswers. Part B grades 10 negative feelings in the pastfew days on a 7-point scale leading to a minimum scoreof 10 up to a maximum of 70 points in total. Both partswere answered at time points BDC and R4 to cover thebaseline and the interventional period.
Neuroendocrine response
CortisolThe collection of saliva samples twice a day, in the morning(7 am) and evening (8 pm) enabled monitoring of the diurnalrhythm of cortisol. The morning collection took place imme-diately after the subjects awakened from an overnight fast.The evening collection was carried out before dinner.Subjects chewed on a cotton swab for 30–45 s that was sub-sequently stored in a SALIVETTE tube (Sarstedt, N€urnbrecht,Germany) and frozen at �20 �C. An automated immunoassaysystem based on the principle of electrochemiluminescence(Elecsys Cortisol, Roche Diagnostics, Mannheim, Germany)quantified cortisol levels (reference values: morning<0.87lg/dl; evening <0.35lg/dl; the intra-assay CV rangedfrom 1.5 to 5.4% for concentrations from 0.007 to 0.972 lg/dl;and the inter-assay CV ranged from 1.9 to 10.1% for concen-trations from 0.013 to 1.17lg/dl according to the referenceranges of the manufacturer).
CatecholaminesUrine was gathered twice a day at 12 h intervals (daytime:7:00 am to 7:00 pm; nighttime: 7:00 pm to 7:00 am). The vol-ume was measured, a 10ml sample extracted and immedi-ately frozen at �20 �C. From this sample, the catecholaminenorepinephrine was analyzed with high-performance liquidchromatography (Chromosystem, Martinsried, Germany).Finally, the absolute mass of norepinephrine was calculatedwith respect to urine volumes (reference values: norepineph-rine <100 lg/24 h; intra-assay CV <2.7%; inter-assay CV
<4.1% according to the reference ranges of the manufacturerand to values surveyed by the laboratory of clinical chemistry,Ludwig-Maximilians-University, Munich, Germany).
Endocannabinoids (ECs)Sample measurements of EC concentrations of arachidonyle-thanolamide (AEA), 2-arachidonoylglycerol (2-AG), palmitoyle-thanolamin (PEA), oleoylethanolamide (OEA), andstearoylethanolamide (SEA) were taken from lithium-hepari-nized whole blood drawn from fasting subjects in supine pos-ition. Samples were collected according to standard operatingprocedures, collection times were strictly adhered to (7 am asfor morning saliva and nighttime urine collection) and sam-ples were immediately frozen on-site at �80 �C. Prior to thefinal analysis, whole blood samples were thawed, mixed, andvortexed with 20 ll of internal standard (stable isotope-labeled ECs 2-AG-d5, PEA-d4, NADA-d8, AEA-d4, AG-d8(Cayman Europe, Tallinn, Estonia)) as well as 1ml of methyltertiary-butyl ether (MTBE, Sigma-Aldrich, Milano, Italy), andcentrifuged at 13,000�g for 5min. The clear supernatant wastransferred into a clean 1ml polypropylene tube (Sarstedt,Numbrecht, Germany) and evaporated in the Speed Dry/Speed Vac centrifuge (Christ, Osterode am Harz, Germany) for30min at room temperature until drying of the organic phase.Dried organic phases were reconstituted in 80 ll of aceto-nitrile plus 80 ll R1 buffer (5mM ammonium formate(NH4OFo) added to water with 15% methanol) and vortexedfor 30 s. After centrifugation at 13,000� g for 5min, 110ll ofclear solution was transferred to HPLC/MS-MS suitable tubesmade of polypropylene and frozen at �80 �C. Subsequentanalysis and quantification of the ECs were carried out by theHPLC Tandem Mass Spectrometry Technique as described pre-viously (Hauer et al., 2013) at the Institute of Doping Analysisund Sports Biochemistry, Kreischa/Dresden, Germany.
Statistics
Data were analyzed and plotted with SPSS 23.0 (IBM, Armonk,NY) and Sigma Plot 12.5 (Systat Software Inc., San Jose, CA).Outcome variables were tested for deviations from the normaldistribution using Kolmogorov–Smirnov tests followed by aBox–Cox Transformation where deviations were present.Statistical inferences regarding the effects of different condi-tions and time points during the same campaign wereimputed through mixed linear models (LME). We included fixeffects for campaign, sequence of campaigns, potential carry-over from the previous campaign, condition, time within therespective campaign, and the interaction of condition andtime. Random effects were included for subject and carry-overusing a covariance matrix with variance components structure.We regarded p values < .05 as statistically significant.
Results
Psychological responses
KAB (short questionnaire on current stress)The KAB generally displayed relative low-stress levels withscores below 3 in all groups in the morning and evening
STRESS 133
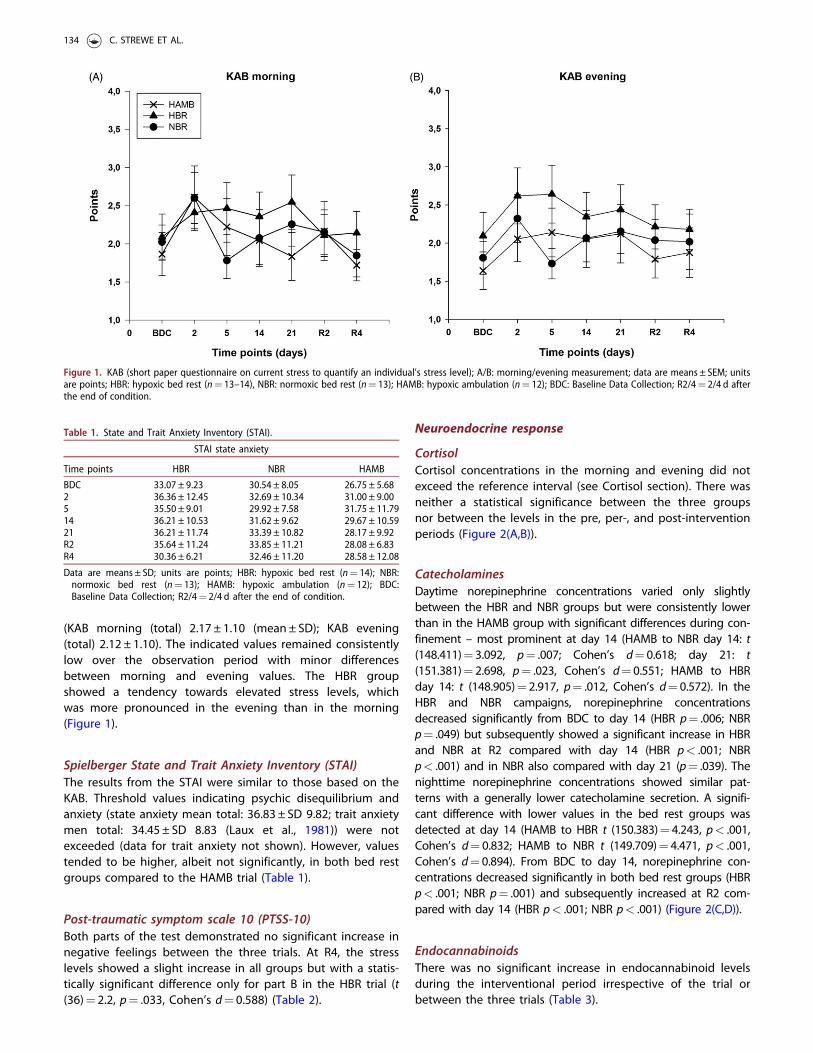
(KAB morning (total) 2.17 ± 1.10 (mean± SD); KAB evening(total) 2.12 ± 1.10). The indicated values remained consistentlylow over the observation period with minor differencesbetween morning and evening values. The HBR groupshowed a tendency towards elevated stress levels, whichwas more pronounced in the evening than in the morning(Figure 1).
Spielberger State and Trait Anxiety Inventory (STAI)The results from the STAI were similar to those based on theKAB. Threshold values indicating psychic disequilibrium andanxiety (state anxiety mean total: 36.83 ± SD 9.82; trait anxietymen total: 34.45 ± SD 8.83 (Laux et al., 1981)) were notexceeded (data for trait anxiety not shown). However, valuestended to be higher, albeit not significantly, in both bed restgroups compared to the HAMB trial (Table 1).
Post-traumatic symptom scale 10 (PTSS-10)Both parts of the test demonstrated no significant increase innegative feelings between the three trials. At R4, the stresslevels showed a slight increase in all groups but with a statis-tically significant difference only for part B in the HBR trial (t(36)¼ 2.2, p¼ .033, Cohen’s d¼ 0.588) (Table 2).
Neuroendocrine response
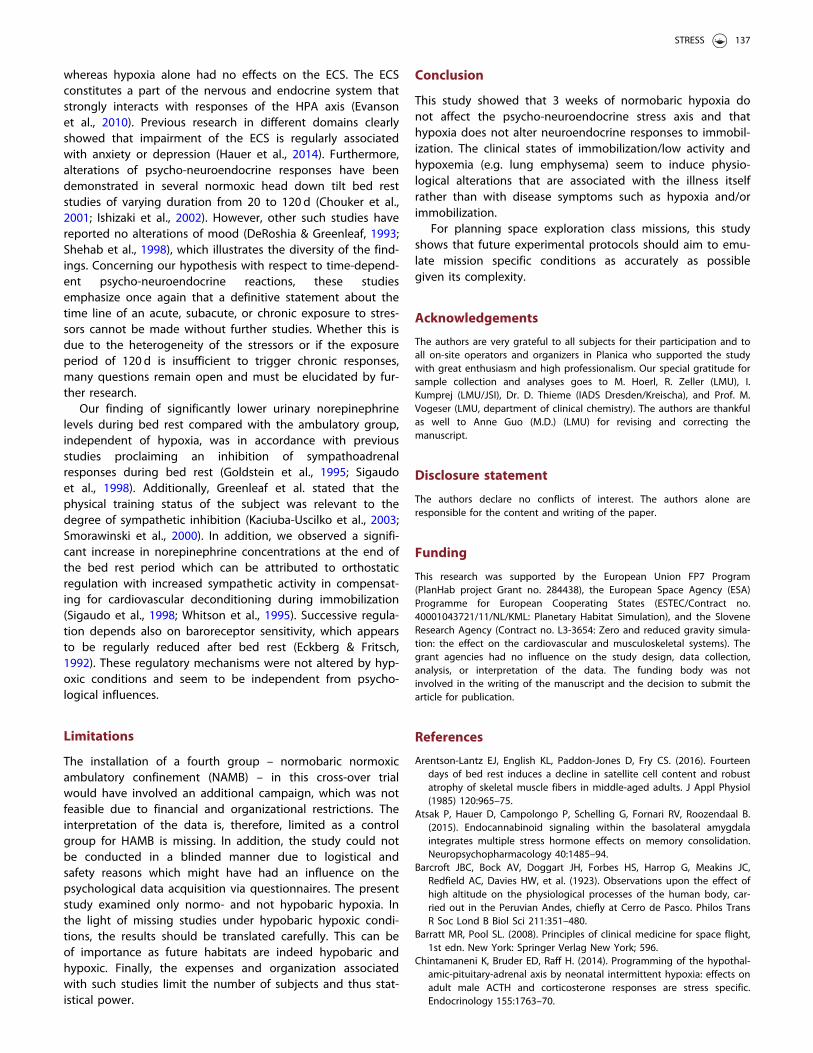
CortisolCortisol concentrations in the morning and evening did notexceed the reference interval (see Cortisol section). There wasneither a statistical significance between the three groupsnor between the levels in the pre, per-, and post-interventionperiods (Figure 2(A,B)).
CatecholaminesDaytime norepinephrine concentrations varied only slightlybetween the HBR and NBR groups but were consistently lowerthan in the HAMB group with significant differences during con-finement – most prominent at day 14 (HAMB to NBR day 14: t(148.411)¼ 3.092, p¼ .007; Cohen’s d¼ 0.618; day 21: t(151.381)¼ 2.698, p¼ .023, Cohen’s d¼ 0.551; HAMB to HBRday 14: t (148.905)¼ 2.917, p¼ .012, Cohen’s d¼ 0.572). In theHBR and NBR campaigns, norepinephrine concentrationsdecreased significantly from BDC to day 14 (HBR p¼ .006; NBRp¼ .049) but subsequently showed a significant increase in HBRand NBR at R2 compared with day 14 (HBR p< .001; NBRp< .001) and in NBR also compared with day 21 (p¼ .039). Thenighttime norepinephrine concentrations showed similar pat-terns with a generally lower catecholamine secretion. A signifi-cant difference with lower values in the bed rest groups wasdetected at day 14 (HAMB to HBR t (150.383)¼ 4.243, p< .001,Cohen’s d¼ 0.832; HAMB to NBR t (149.709)¼ 4.471, p< .001,Cohen’s d¼ 0.894). From BDC to day 14, norepinephrine con-centrations decreased significantly in both bed rest groups (HBRp< .001; NBR p¼ .001) and subsequently increased at R2 com-pared with day 14 (HBR p< .001; NBR p< .001) (Figure 2(C,D)).
EndocannabinoidsThere was no significant increase in endocannabinoid levelsduring the interventional period irrespective of the trial orbetween the three trials (Table 3).
Figure 1. KAB (short paper questionnaire on current stress to quantify an individual’s stress level); A/B: morning/evening measurement; data are means ± SEM; unitsare points; HBR: hypoxic bed rest (n¼ 13–14), NBR: normoxic bed rest (n¼ 13); HAMB: hypoxic ambulation (n¼ 12); BDC: Baseline Data Collection; R2/4¼ 2/4 d afterthe end of condition.
Table 1. State and Trait Anxiety Inventory (STAI).
STAI state anxiety
Time points HBR NBR HAMB
BDC 33.07 ± 9.23 30.54 ± 8.05 26.75 ± 5.682 36.36 ± 12.45 32.69 ± 10.34 31.00 ± 9.005 35.50 ± 9.01 29.92 ± 7.58 31.75 ± 11.7914 36.21 ± 10.53 31.62 ± 9.62 29.67 ± 10.5921 36.21 ± 11.74 33.39 ± 10.82 28.17 ± 9.92R2 35.64 ± 11.24 33.85 ± 11.21 28.08 ± 6.83R4 30.36 ± 6.21 32.46 ± 11.20 28.58 ± 12.08
Data are means ± SD; units are points; HBR: hypoxic bed rest (n¼ 14); NBR:normoxic bed rest (n¼ 13); HAMB: hypoxic ambulation (n¼ 12); BDC:Baseline Data Collection; R2/4¼ 2/4 d after the end of condition.
134 C. STREWE ET AL.

Table 2. Post-traumatic symptom scale (PTSS-10) Part A/B.
PTSS-10 Part A
HBR NBR
Time points Pain Troubles of breathing Nightmares Anxiety/panic Pain Troubles of breathing Nightmares Anxiety/panic
BDC 1 0 2 0 1 2 1 0R4 3 1 4 3 1 1 3 1
HAMB
Pain Troubles of breathing Nightmares Anxiety/panic
BDC 1 0 1 1R4 3 2 2 2
PTSS-10 Part B
HBR NBR HAMB
BDC 15.50 ± 3.82 14.77 ± 4.57 15.33 ± 2.74R4 �18.71 ± 7.62 16.54 ± 7.40 16.17 ± 4.91
Data are means ± SD; units are points; HBR: hypoxic bed rest (n¼ 14); NBR: normoxic bed rest (n¼ 13); HAMB: hypoxic ambulation (n¼ 12); BDC: Baseline DataCollection; R4¼ 4 d after the end of condition. �Significant difference between R4 and BDC in HBR (p< .05).
Figure 2. Cortisol in saliva; norepinephrine in urine; A/B: cortisol morning/evening (HBR: n¼ 14; NBR: n¼ 12–13; HAMB: n¼ 12); C/D: norepinephrine day/night(HBR: n¼ 10–14; NBR: n¼ 8–13; HAMB: n¼ 12); data are means ± SEM; units are lg/dl (cortisol) or lg/12 h (norepinephrine); HBR: hypoxic bed rest; NBR: normoxicbed rest; HAMB: hypoxic ambulation; BDC: Baseline Data Collection; R2¼ 2 d after the end of condition; norepinephrine daytime: # significant difference betweenHAMB and NBR; � significant difference between HAMB and HBR; l significant difference BDC to day 14 in HBR/NBR;þ significant difference R2 to day 14 in HBR/NBR; � significant difference R2 to day 21 in NBR; norepinephrine nighttime: # significant difference between HAMB and NBR; � significant difference betweenHAMB and HBR;þ significant difference R2/BDC to day 14 in HBR/NBR.
STRESS 135

Discussion
The present study demonstrates that 3 weeks of normobarichypoxia evoke no significant stress response, neither on thepsychological nor on hormone levels. However, bed rest, anindependent factor to hypoxia, induces a significantly differ-ent stress response, with lower norepinephrine concentra-tions during confinement (day 14) compared with HAMB.Furthermore, in both bed rest groups, norepinephrine con-centrations significantly decreased from BDC to day 14 andincreased again at R2.
We aimed to assess whether hypoxia alone, or in combin-ation with bed rest, induces psycho-neuroendocrineresponses, since it is well established that hypoxia affectsphysiological responses and neuropsychological capacities(Barcroft et al., 1923; de Aquino Lemos et al., 2012). Weanticipated a hypoxia-triggered exacerbated stress responsewith higher levels of psychological stress and a subsequentlyincreased neuroendocrine response, with both supposedlyalready increased by immobilization alone. It is well docu-mented that hypoxia leads to specific reactions of differentneuroendocrine systems essential to the maintenance ofadequate physiological responses (King et al., 2015; Wenzelet al., 2013). Most studies investigating the influence of hyp-oxia on the HPA axis and the ECS are carried out in animalfetus/neonates (Newby et al., 2015) demonstrating a dysregu-lation of the HPA axis with subsequent negative effects onendocrine activity and behavior (Chintamaneni et al., 2014).Furthermore, studies investigating effects of hypoxia in ani-mals aimed to define the threshold level of hypoxia thatclearly invoked physiological effects (King et al., 2015; Smithet al., 1995). The applied hypoxic levels ranged from 18 to3% FiO2 and most of the effects were recorded at levels ofFiO2�12%. In contrast to previous studies, the aim of thistrial was not to define threshold values in humans but toidentify the consequences of a fixed and likely applicable O2
content for manned space habitats. We focused on identify-ing the consequences of normobaric hypoxia at 14% and itsimpact on human physiology.
Previous studies carried out with human subjects surveyedphysiological reactions predominantly under the influence of
hypobaric hypoxia (Feuerecker et al., 2014) or normobaric/hyperbaric hyperoxia (Mazdeh et al., 2015; Strewe et al.,2015). Millet et al. (2012) argue that hypobaric comparedwith normobaric hypoxia induces different physiologicalresponses concerning factors such as ventilation (Savoureyet al., 2003) or fluid balance (Loeppky et al., 2005) whereasMounier et al. (Mounier & Brugniaux, 2012) refuted thishypothesis. With no clear answer to the question to date anda lack of comparable data, exploration of these results tohealthy humans or to a clinical setting (immobilized patientswith (normobaric) hypoxemic diseases (i.e. emphysema, fibro-sis)) would not be prudent.
The PlanHab project has enabled us to investigate healthyhumans precisely in such conditions for the first time: undernormobaric hypoxia and concomitant immobilization withhighly standardized conditions for 3 weeks.
The results of the present study do not align with previousfindings (Keramidas et al., 2016; Stavrou et al., 2015), whichmay partly be explained by different methodologies.Specifically, the duration of exposure to the stressors and theexperimental set-up as well as questionnaire methods dif-fered. In contrast to our results, a former study of hypoxicbed rest of only 10 d demonstrated negative effects on moodwith amelioration when omitting immobilization (Stavrouet al., 2015). Thus, an acute, short-term exposure of 10 dseems to generate a negative psychic response whereas asubacute influence of 3 weeks as in our actual study evokesan inert response. This may reflect a state of adaptation andhabituation over time. Hence, two questions arise: Whichtime frame represents a chronic, long-term exposure? Wouldthis adaptation process sustain chronic exposure or nega-tively exaggerate the stressors’ impact, subsequently leadingto negative physiological reactions?
Another recent report also stated negative emotions undersevere hypoxia (Keramidas et al., 2016) but the experimentalset-up differed from that of our study. The results wereobtained following incremental exercise until exhaustion,thus preventing a direct comparison.
Feuerecker et al. (2012) found that the activation of theECS through exercise was further enhanced by hypoxia,
Table 3. Endocannabinoid concentrations in blood.
2-AG AEA OEA
Time points HBR NBR HAMB HBR NBR HAMB HBR NBR HAMB
BDC 7.6 ± 6.1 8.1 ± 6.1 7.0 ± 8.3 0.1 ± 0.1 0.1 ± 0.1 0.1 ± 0.1 0.6 ± 0.3 0.8 ± 0.6 0.6 ± 0.52 8.4 ± 10.6 5.6 ± 5.3 6.2 ± 6.2 0.1 ± 0.2 0.1 ± 0.1 0.1 ± 0.1 0.8 ± 1.0 0.5 ± 0.3 0.5 ± 0.45 14.1 ± 18.9 8.2 ± 8.2 7.8 ± 8.8 0.2 ± 0.2 0.1 ± 0.1 0.1 ± 0.1 1.0 ± 1.0 0.7 ± 0.6 0.7 ± 0.814 9.3 ± 14.1 6.4 ± 4.4 12.1 ± 27.2 0.1 ± 0.1 0.1 ± 0.1 0.1 ± 0.2 0.6 ± 0.6 0.4 ± 0.2 0.7 ± 1.221 9.1 ± 7.5 11.5 ± 11.1 10.0 ± 7.9 0.1 ± 0.1 0.1 ± 0.1 0.2 ± 0.1 0.7 ± 0.6 0.8 ± 0.9 0.9 ± 0.8R2 7.4 ± 6.8 6.7 ± 4.9 9.4 ± 7.9 0.1 ± 0.1 0.1 ± 0.1 0.1 ± 0.1 0.6 ± 0.5 2.0 ± 5.5 0.6 ± 0.5
PEA SEA
HBR NBR HAMB HBR NBR HAMB
BDC 1.0 ± 0.4 1.1 ± 0.7 1.1 ± 0.7 0.4 ± 0.2 0.4 ± 0.2 0.4 ± 0.32 1.0 ± 0.7 0.7 ± 0.4 0.9 ± 0.5 0.4 ± 0.2 0.3 ± 0.2 0.3 ± 0.25 1.2 ± 0.7 0.9 ± 0.7 1.1 ± 0.7 0.5 ± 0.2 0.4 ± 0.2 0.4 ± 0.214 0.8 ± 0.4 0.7 ± 0.2 1.1 ± 1.6 0.3 ± 0.1 0.3 ± 0.1 0.5 ± 0.921 0.9 ± 0.6 1.3 ± 1.4 1.1 ± 0.7 0.4 ± 0.2 0.3 ± 0.2 0.4 ± 0.2R2 0.9 ± 0.6 0.9 ± 0.7 1.0 ± 0.6 0.4 ± 0.2 0.4 ± 0.3 0.4 ± 0.2
2-AG: 2-arachidonoylglycerol; AEA: arachidonoylethanolamide; OEA: oleoylethanolamide; PEA: palmitoylethanolamin; SEA: stearoylethanolamide; data aremeans ± SD; units are ng/ml; HBR: hypoxic bed rest (n¼ 14); NBR: normoxic bed rest (n¼ 13); HAMB: hypoxic ambulation (n¼ 11-12); BDC: Baseline DataCollection; R2¼ 2 d after the end of condition.
136 C. STREWE ET AL.
whereas hypoxia alone had no effects on the ECS. The ECSconstitutes a part of the nervous and endocrine system thatstrongly interacts with responses of the HPA axis (Evansonet al., 2010). Previous research in different domains clearlyshowed that impairment of the ECS is regularly associatedwith anxiety or depression (Hauer et al., 2014). Furthermore,alterations of psycho-neuroendocrine responses have beendemonstrated in several normoxic head down tilt bed reststudies of varying duration from 20 to 120 d (Chouker et al.,2001; Ishizaki et al., 2002). However, other such studies havereported no alterations of mood (DeRoshia & Greenleaf, 1993;Shehab et al., 1998), which illustrates the diversity of the find-ings. Concerning our hypothesis with respect to time-depend-ent psycho-neuroendocrine reactions, these studiesemphasize once again that a definitive statement about thetime line of an acute, subacute, or chronic exposure to stres-sors cannot be made without further studies. Whether this isdue to the heterogeneity of the stressors or if the exposureperiod of 120 d is insufficient to trigger chronic responses,many questions remain open and must be elucidated by fur-ther research.
Our finding of significantly lower urinary norepinephrinelevels during bed rest compared with the ambulatory group,independent of hypoxia, was in accordance with previousstudies proclaiming an inhibition of sympathoadrenalresponses during bed rest (Goldstein et al., 1995; Sigaudoet al., 1998). Additionally, Greenleaf et al. stated that thephysical training status of the subject was relevant to thedegree of sympathetic inhibition (Kaciuba-Uscilko et al., 2003;Smorawinski et al., 2000). In addition, we observed a signifi-cant increase in norepinephrine concentrations at the end ofthe bed rest period which can be attributed to orthostaticregulation with increased sympathetic activity in compensat-ing for cardiovascular deconditioning during immobilization(Sigaudo et al., 1998; Whitson et al., 1995). Successive regula-tion depends also on baroreceptor sensitivity, which appearsto be regularly reduced after bed rest (Eckberg & Fritsch,1992). These regulatory mechanisms were not altered by hyp-oxic conditions and seem to be independent from psycho-logical influences.
Limitations
The installation of a fourth group – normobaric normoxicambulatory confinement (NAMB) – in this cross-over trialwould have involved an additional campaign, which was notfeasible due to financial and organizational restrictions. Theinterpretation of the data is, therefore, limited as a controlgroup for HAMB is missing. In addition, the study could notbe conducted in a blinded manner due to logistical andsafety reasons which might have had an influence on thepsychological data acquisition via questionnaires. The presentstudy examined only normo- and not hypobaric hypoxia. Inthe light of missing studies under hypobaric hypoxic condi-tions, the results should be translated carefully. This can beof importance as future habitats are indeed hypobaric andhypoxic. Finally, the expenses and organization associatedwith such studies limit the number of subjects and thus stat-istical power.
Conclusion
This study showed that 3 weeks of normobaric hypoxia donot affect the psycho-neuroendocrine stress axis and thathypoxia does not alter neuroendocrine responses to immobil-ization. The clinical states of immobilization/low activity andhypoxemia (e.g. lung emphysema) seem to induce physio-logical alterations that are associated with the illness itselfrather than with disease symptoms such as hypoxia and/orimmobilization.
For planning space exploration class missions, this studyshows that future experimental protocols should aim to emu-late mission specific conditions as accurately as possiblegiven its complexity.
Acknowledgements
The authors are very grateful to all subjects for their participation and toall on-site operators and organizers in Planica who supported the studywith great enthusiasm and high professionalism. Our special gratitude forsample collection and analyses goes to M. Hoerl, R. Zeller (LMU), I.Kumprej (LMU/JSI), Dr. D. Thieme (IADS Dresden/Kreischa), and Prof. M.Vogeser (LMU, department of clinical chemistry). The authors are thankfulas well to Anne Guo (M.D.) (LMU) for revising and correcting themanuscript.
Disclosure statement
The authors declare no conflicts of interest. The authors alone areresponsible for the content and writing of the paper.
Funding
This research was supported by the European Union FP7 Program(PlanHab project Grant no. 284438), the European Space Agency (ESA)Programme for European Cooperating States (ESTEC/Contract no.40001043721/11/NL/KML: Planetary Habitat Simulation), and the SloveneResearch Agency (Contract no. L3-3654: Zero and reduced gravity simula-tion: the effect on the cardiovascular and musculoskeletal systems). Thegrant agencies had no influence on the study design, data collection,analysis, or interpretation of the data. The funding body was notinvolved in the writing of the manuscript and the decision to submit thearticle for publication.
References
Arentson-Lantz EJ, English KL, Paddon-Jones D, Fry CS. (2016). Fourteendays of bed rest induces a decline in satellite cell content and robustatrophy of skeletal muscle fibers in middle-aged adults. J Appl Physiol(1985) 120:965–75.
Atsak P, Hauer D, Campolongo P, Schelling G, Fornari RV, Roozendaal B.(2015). Endocannabinoid signaling within the basolateral amygdalaintegrates multiple stress hormone effects on memory consolidation.Neuropsychopharmacology 40:1485–94.
Barcroft JBC, Bock AV, Doggart JH, Forbes HS, Harrop G, Meakins JC,Redfield AC, Davies HW, et al. (1923). Observations upon the effect ofhigh altitude on the physiological processes of the human body, car-ried out in the Peruvian Andes, chiefly at Cerro de Pasco. Philos TransR Soc Lond B Biol Sci 211:351–480.
Barratt MR, Pool SL. (2008). Principles of clinical medicine for space flight,1st edn. New York: Springer Verlag New York; 596.
Chintamaneni K, Bruder ED, Raff H. (2014). Programming of the hypothal-amic-pituitary-adrenal axis by neonatal intermittent hypoxia: effects onadult male ACTH and corticosterone responses are stress specific.Endocrinology 155:1763–70.
STRESS 137

Chouker A, Thiel M, Baranov V, Meshkov D, Kotov A, Peter K, Messmer K,Christ F. (2001). Simulated microgravity, psychic stress, and immunecells in men: observations during 120-day 6 degrees HDT. J ApplPhysiol 90:1736–43.
de Aquino Lemos V, Antunes HK, dos Santos RV, Lira FS, Tufik S, deMello MT. (2012). High altitude exposure impairs sleep patterns,mood, and cognitive functions. Psychophysiology 49:1298–306.
Debevec T, Bali TC, Simpson EJ, Macdonald IA, Eiken O, Mekjavic IB.(2014). Separate and combined effects of 21-day bed rest and hypoxicconfinement on body composition. Eur J Appl Physiol 114:2411–25.
DeRoshia CW, Greenleaf JE. (1993). Performance and mood-state parame-ters during 30-day 6 degrees head-down bed rest with exercise train-ing. Aviat Space Environ Med 64:522–7.
Eckberg DL, Fritsch JM. (1992). Influence of ten-day head-down bedreston human carotid baroreceptor-cardiac reflex function. Acta PhysiolScand Suppl 604:69–76.
Eksuzian DJ. (1999). Psychological and behavioral health issues of long-duration space missions. Life Support Biosph Sci 6:35–8.
Evanson NK, Tasker JG, Hill MN, Hillard CJ, Herman JP. (2010). Fast feed-back inhibition of the HPA axis by glucocorticoids is mediated byendocannabinoid signaling. Endocrinology 151:4811–19.
Feuerecker M, Crucian B, Salam AP, Rybka A, Kaufmann I, Moreels M,Quintens R, et al. (2014). Early adaption to the antarctic environmentat dome C: consequences on stress-sensitive innate immune functions.High Alt Med Biol 15:341–8.
Feuerecker M, Hauer D, Toth R, Demetz F, Holzl J, Thiel M, Kaufmann I,et al. (2012). Effects of exercise stress on the endocannabinoid systemin humans under field conditions. Eur J Appl Physiol 112:2777–81.
Goldstein DS, Vernikos J, Holmes C, Convertino VA. (1995).Catecholaminergic effects of prolonged head-down bed rest. J ApplPhysiol 78:1023–9.
Hauer D, Kaufmann I, Strewe C, Briegel I, Campolongo P, Schelling G.(2014). The role of glucocorticoids, catecholamines and endocannabi-noids in the development of traumatic memories and posttraumaticstress symptoms in survivors of critical illness. Neurobiol Learn Mem112:68–74.
Hauer D, Schelling G, Gola H, Campolongo P, Morath J, Roozendaal B,Hamuni G, et al. (2013). Plasma concentrations of endocannabinoidsand related primary fatty acid amides in patients with post-traumaticstress disorder. PLoS One 8:e62741.
Herman JP, Figueiredo H, Mueller NK, Ulrich-Lai Y, Ostrander MM, ChoiDC, Cullinan WE. (2003). Central mechanisms of stress integration: hier-archical circuitry controlling hypothalamo-pituitary–adrenocorticalresponsiveness. Front Neuroendocrinol 24:151–80.
Hill MN, McLaughlin RJ, Morrish AC, Viau V, Floresco SB, Hillard CJ,Gorzalka BB. (2009). Suppression of amygdalar endocannabinoid sig-naling by stress contributes to activation of the hypothalamic–pituitar-y–adrenal axis. Neuropsychopharmacology 34:2733–45.
Ishizaki Y, Ishizaki T, Fukuoka H, Kim CS, Fujita M, Maegawa Y, Fujioka H,et al. (2002). Changes in mood status and neurotic levels during a 20-day bed rest. Acta Astronaut 50:453–9.
Kaciuba-Uscilko H, Smorawinski J, Nazar K, Adrian J, Greenleaf JE. (2003).Catecholamine responses to environmental stressors in trained anduntrained men after 3-day bed rest. Aviat Space Environ Med74:928–36.
Keramidas ME, Stavrou NA, Kounalakis SN, Eiken O, Mekjavic IB. (2016).Severe hypoxia during incremental exercise to exhaustion provokesnegative post-exercise affects. Physiol Behav 156:171–6.
King TL, Ruyle BC, Kline DD, Heesch CM, Hasser EM. (2015).Catecholaminergic neurons projecting to the paraventricular nucleusof the hypothalamus are essential for cardiorespiratory adjustments tohypoxia. Am J Physiol Regul Integr Comp Physiol 309:R721–31.
Laux L, Glanzmann P, Schaffner P, Spielberger C. (1981). Das State-Trait-Angst-Inventar, STAI. 1. Aufl. Beltz, Weinheim
Loeppky JA, Roach RC, Maes D, Hinghofer-Szalkay H, Roessler A, Gates L,Fletcher ER, Icenogle MV. (2005). Role of hypobaria in fluid balanceresponse to hypoxia. High Alt Med Biol 6:60–71.
Mazdeh M, Taher A, Torabian S, Seifirad S. (2015). Effects of normobarichyperoxia in severe acute stroke: a randomized controlled clinical trialstudy. Acta Med Iran 53:676–80.
Millet GP, Faiss R, Pialoux V. (2012). Point: hypobaric hypoxia induces dif-ferent physiological responses from normobaric hypoxia. J ApplPhysiol (1985) 112:1783–4.
Mounier R, Brugniaux JV. (2012). Counterpoint: hypobaric hypoxia doesnot induce different responses from normobaric hypoxia. J ApplPhysiol (1985) 112:1784–6.
Mueller B, Basler HD. (1993). Kurzfragebogen zur aktuellenBeanspruchung (KAB). Weinheim: Belz, Germany.
Newby EA, Myers DA, Ducsay CA. (2015). Fetal endocrine and metabolicadaptations to hypoxia: the role of the hypothalamic–pituitary–adrenalaxis. Am J Physiol Endocrinol Metab 309:E429–39.
Richalet JP. (2016). Physiological and clinical implications of adrenergicpathways at high altitude. Adv Exp Med Biol 903:343–56.
Roberts CJ, Stuhr KL, Hutz MJ, Raff H, Hillard CJ. (2014). Endocannabinoidsignaling in hypothalamic–pituitary–adrenocortical axis recovery fol-lowing stress: effects of indirect agonists and comparison of male andfemale mice. Pharmacol Biochem Behav 117:17–24.
Romero EM, Fernandez B, Sagredo O, Gomez N, Uriguen L, Guaza C, DeMiguel R, et al. (2002). Antinociceptive, behavioural and neuroendo-crine effects of CP 55,940 in young rats. Brain Res Dev Brain Res136:85–92.
Saugy JJ, Schmitt L, Fallet S, Faiss R, Vesin JM, Bertschi M, Heinzer R, MilletGP. (2016). Sleep disordered breathing during live high-train low in nor-mobaric versus hypobaric hypoxia. High Alt Med Biol 17:233–8.
Savourey G, Launay JC, Besnard Y, Guinet A, Travers S. (2003). Normo-and hypobaric hypoxia: are there any physiological differences? Eur JAppl Physiol 89:122–6.
Shehab RL, Schlegel RE, Schiflett SG, Eddy DR. (1998). The NASAPerformance Assessment Workstation: cognitive performance duringhead-down bed rest. Acta Astronaut 43:223–33.
Sigaudo D, Fortrat JO, Allevard AM, Maillet A, Cottet-Emard JM,Vouillarmet A, Hughson RL, et al. (1998). Changes in the sympatheticnervous system induced by 42 days of head-down bed rest. Am JPhysiol 274:H1875–84.
Smith DW, Buller KM, Day TA. (1995). Role of ventrolateral medulla cat-echolamine cells in hypothalamic neuroendocrine cell responses tosystemic hypoxia. J Neurosci 15:7979–88.
Smith SM, Castaneda-Sceppa C, O'Brien KO, Abrams SA, Gillman P, BrooksNE, Cloutier GJ, et al. (2014). Calcium kinetics during bed rest withartificial gravity and exercise countermeasures. Osteoporos Int25:2237–44.
Smorawinski J, Kaciuba-Uscilko H, Nazar K, Kubala P, Kaminska E, ZiembaAW, Adrian J, Greenleaf JE. (2000). Effects of three-day bed rest onmetabolic, hormonal and circulatory responses to an oral glucose loadin endurance or strength trained athletes and untrained subjects. JPhysiol Pharmacol 51:279–89.
Spielberger CD, Gorssuch RL, Lushene PR, Vagg PR, Jacobs GA. (1983).Manual for the state-trait anxiety inventory. Palo Alto, CA: ConsultingPsychologists Press, Inc.
Stavrou NA, McDonnell AC, Eiken O, Mekjavic IB. (2015). Psychologicalstrain: examining the effect of hypoxic bedrest and confinement.Physiol Behav 139:497–504.
Strewe C, Crucian BE, Sams CF, Feuerecker B, Stowe RP, Chouker A,Feuerecker M. (2015). Hyperbaric hyperoxia alters innate immune func-tional properties during NASA Extreme Environment MissionOperation (NEEMO). Brain Behav Immun 50:52–7.
Tsigos C, Chrousos GP. (2002). Hypothalamic-pituitary-adrenal axis, neuro-endocrine factors and stress. J Psychosom Res 53:865–71.
Wang M, Hill MN, Zhang L, Gorzalka BB, Hillard CJ, Alger BE. (2012).Acute restraint stress enhances hippocampal endocannabinoid func-tion via glucocorticoid receptor activation. J Psychopharmacol (Oxford)26:56–70.
Wenzel D, Matthey M, Bindila L, Lerner R, Lutz B, Zimmer A, FleischmannBK. (2013). Endocannabinoid anandamide mediates hypoxic pulmon-ary vasoconstriction. Proc Natl Acad Sci U S A 110:18710–15.
Westby CM, Martin DS, Lee SM, Stenger MB, Platts SH. (2016). Left ven-tricular remodeling during and after 60 days of sedentary head-downbed rest. J Appl Physiol (1985) 120:956–64.
Whitson PA, Charles JB, Williams WJ, Cintron NM. (1995). Changes in sym-pathoadrenal response to standing in humans after spaceflight. J ApplPhysiol 79:428–33.
138 C. STREWE ET AL.

Yang C, Chen J, Wu F, Li J, Liang P, Zhang H, Wang H, et al. (2014).Effects of 60-day head-down bed rest on osteocalcin, glycolipidmetabolism and their association with or without resistance training.Clin Endocrinol (Oxf) 81:671–8.
Zaeh S, Miele CH, Putcha N, Gilman RH, Miranda JJ, Bernabe-Ortiz A, WiseRA, Checkley W. (2016). Chronic respiratory disease and high altitudeare associated with depressive symptoms in four diverse settings. Int JTuberc Lung Dis 20:1263–9.
STRESS 139


















