2019 QUALITY REPORT - nhsltd.com · PEDIATRIC BRAIN INJURY CONTINUUM Our Brain Injury...
24
2019 QUALITYREPORT
Transcript of 2019 QUALITY REPORT - nhsltd.com · PEDIATRIC BRAIN INJURY CONTINUUM Our Brain Injury...

2019 QUALITY REPORT


3
Nexus Children’s Hospital is accredited by DNV-GL’s NIAHO® and is ISO 9001:2008 certified.
2019 StatisticsNumber of Employees: 134
Number of Licensed Beds: 40
Number of Patients Served: 137
Average Length of Stay (days): 65
TABLE OF CONTENTSWelcome to Nexus Children’s Hospital 4
Mission, Vision & Core Values 4
Physician Leadership 4
Patient Satisfaction 5
Admissions & Discharge Information 5
Infection Control 7
Pediatric Pulmonary Medicine 8
Rehabilitation 9
Pediatric Brain Injury Continuum 10
Patient Story 13
Measurement Outcomes 14
Patient Case Study 16
Disorder of Consciousness Program 17
Patient Case Study 19
Changes Health & Wellness Program 20
Patient Story 22

4
NEXUS HEALTH SYSTEMS CORE VALUES
MISSIONTo return our patients to lives of productivity and meaning.
VISIONTo be recognized as the leader in providing specialized pediatric care and facilitating the transition for children and families from the hospital to home and community.
PHYSICIAN LEADERSHIP & ALLIED HEALTH SPECIALISTSJohn W. Cassidy, MD Chief Medical Officer
Rachel Leppo, PhD Neuro Psychology
Monica LeBrie, PhD, BCBA, LBA Behavioral Psychology
Sheryl Vinci, DMP, APRN, FNP-C Behavioral Nurse Practitioner
Courtney Toomey, MD Physical Medicine and Rehabilitation Director
Sarat Susarla, MD Pulmonology
Pediatrix Hospitalist Group Pediatricians Pediatric Nurse Practitioners Pediatric Intensivist
WELCOMEWelcome to Nexus Children’s Hospital, where we’ve created an environment that feels more like home than a hospital for our young patients and their families.
The multidisciplinary team of medical specialists at Nexus Children’s Hospital has a passion for helping every child who comes
to our facility. Working with an understanding that hospitals can be a scary and overwhelming place for children — and their families — our medical team places as much attention on caring for emotional challenges and educating parents and family members as it does on addressing medical challenges.
While there is no place like home for a child, it is our hope that should you need individualized care for your young loved one or patient, that you turn to Nexus Children’s Hospital.
MARY HARBESON, BSN, MS Chief Executive Officer Nexus Children’s Hospital – Houston

5
PATIENT SATISFACTIONNexus Children’s Hospital prides itself on delivering exceptional care and support to our patients and their families. To develop quality initiatives and ensure needs are met, satisfaction surveys are conducted with each patient and his or her family. Scores are based on a 5-point rating scale.
2019 Patient Satisfaction Score:
4.7TEAM CONFERENCENexus Children’s Hospital offers weekly interdisciplinary team conferences in an effort to better serve the needs of our patients and their families. Individual goals are discussed in conjunction with clinical goals to prepare the patient for an optimal discharge. Our conferences may include members from our medial team, respiratory care, rehabilitation, wound care, infection control, nursing, dietary, and case management.
2019 Nexus Children’s Hospital IP Category Rating
2019 Discharge
53% Home or Self-Care
16% Home with Health
Services
20% Short Term Hospital*
2019 Payor Mix
7% Other
46% Medicaid
47% Commercial Insurance
2019 Admissions
92% Acute Care Hospital
7% Home 1% Other 11% Other
* Sometimes patients leave Nexus Children’s Hospital to stay at an acute hospital in the event they need follow up procedures or evaluation. Patients usually return once treatment is completed.

6

7
INFECTION CONTROL Hand Hygiene
Nexus Children’s Hospital follows the Centers for Disease Control (CDC) Guidelines for hand hygiene in health care settings. Performing hand hygiene can decrease the amount of bacterial burden on the hands and is the number one way to prevent the spread of infections.
Central Line, Catheter & Ventilator Management
A central line is a catheter (tube) that doctors often place in a large vein in the neck, chest, or groin to give medication or fluids or to collect blood for medical tests. Central lines are different from IVs because these lines access a major vein that is close to the heart and may remain in place for weeks or months. Central lines also have greater potential to cause serious infections.
Central-Line Associated Bloodstream Infection (CLABSI) A CLABSI is a serious infection that occurs when germs (usually bacteria or viruses) enter the bloodstream through the central line. Health care providers must follow a strict protocol when inserting a central line, as well as use stringent infection control practices each time they check the line or change the dressing.
Nexus Children’s Hospital 2019 CLABSI Per 1,000 Line Days
Catheter-Associated Urinary Tract Infection (CAUTI) A urinary tract infection (UTI) is an infection involving any part of the urinary system, including the urethra, bladder, ureters, and kidneys. Many UTIs acquired in the hospital are associated with a urinary catheter, a tube inserted into the bladder through the urethra to drain urine. The most important risk factor for developing a CAUTI is prolonged use of the urinary catheter. Therefore, catheters should only be used for appropriate indications and should be removed as soon as they are no longer needed.
Nexus Children’s Hospital 2019 CAUTI Per 1,000 Foley/Indwelling Catheter Days
Ventilator-Associated Pneumonia (VAP) VAP is a lung infection that develops in a person who is on a ventilator, a machine that is used to help a patient breathe through a tube placed in a patient’s mouth or nose, or through a tracheostomy in the front of the neck. An infection may occur if germs enter through the tube and get into the patient’s lungs. The CDC provides guidelines and tools to the healthcare community to help end VAP, resources to help the public understand these infections, and take measures to safeguard their own health when possible.
Nexus Children’s Hospital 2019 VAP Per 1,000 Ventilator Days
GOAL < .8
Per the CDC, all hospitals should strive to have zero CAUTI incidences.
Per the CDC, all hospitals should strive to have zero VAP incidences.
Per the CDC, all hospitals should strive to have zero CLABSI incidences.

8
PEDIATRIC PULMONARY MEDICINEAt Nexus Children’s Hospital, we offer a Pediatric Pulmonary Medicine Program for children who are chronically ill, physically fragile, or traumatically injured. Our program provides care to children who require short-term tracheostomy/ventilator management, as well as those with long-term tracheostomy/ventilator dependencies who will return home.
Patients are placed on a portable ventilator and may receive therapies in one of our facility’s living or therapy areas. As our children improve, they may receive Bi-level Positive Airway Pressure (BiPAP) or Continuous Positive Airway Pressure (CPAP) as other forms of ventilation.
Our program is overseen by a pediatric pulmonologist who works closely with on-site therapists. This program is staffed 24 hours a day by a licensed respiratory therapist.
Number of Trach & Vent Days in 2019
Jan Feb Mar April May June July Aug Sept Oct Nov Dec
Trach Days 53 98 144 91 115 104 113 178 155 150 177 201
Vent Days 31 55 31 31 16 17 82 89 76 37 94 110
Vent Patients/Month
1 3 1 1 1 1 5 3 3 3 5 7
of patients with wean orders were successfully weaned off the ventilator while admitted to Nexus Children’s Hospital.
of patients successfully decannulated 86%

9
REHABILITATION The unique licensing of our facility enables our rehabilitation team to develop individualized treatment plans that meet the specific needs of each child. This means that we are able to provide an acute rehabilitation level of care (15 hours per week) for those children who are ready for intensive inpatient rehabilitation. Conversely, we are also able to provide a lower intensity intervention for those children with significant physical or medical limitation who are not yet able to tolerate acute rehabilitation programming.
Nexus Children’s Hospital has devoted itself to implementing evidence-based assessment tools and interventions in a concerted effort to enhance the competency our staff, collect meaningful outcome data, and increase the efficiency of our care delivery. We also utilize a number of discipline and disability specific assessment tools to closely monitor a patient’s rate of recovery throughout the course of their admission. The patient’s physician determines frequency and duration of treatment with input from our physical therapists.
100% of our rehab staff is WeeFIM-II certified. WeeFIM is a measurement tool used to evaluate functional improvement in activities of daily living.
Physical Therapy
Our Physical Therapy treatment focuses on the mobility of the child through direct one-on-one therapy and parent/caregiver education for carryover between therapy sessions. Patients undergo a comprehensive assessment prior to beginning therapy to determine a treatment plan based on their unique needs. Progress is monitored and goals are updated and modified as needed.
Occupational Therapy
Concentrating on functional independence in areas of daily living and progression of age-appropriate developmental skills in a child’s home, community, and school environments, patients in this program undergo a comprehensive assessment prior to beginning therapy to determine a treatment plan based on their unique needs.
Speech & Language Therapy
Speech Language Pathology services address swallowing disorders in children as well as cognitive communication and social communication deficits that limit age appropriate interaction for home or school. The program utilizes formal assessments, behavioral observations, parental reports, medical history, and background information about the child to determine the severity of the speech and/or language problem and/or swallowing deficits.
Our speech-language pathologists establish appropriate goals, then design and implement individualized treatment plans. The child’s response and progress is carefully monitored on an ongoing basis with timely and appropriate modifications as needed.

10
PEDIATRIC BRAIN INJURY CONTINUUM Our Brain Injury Rehabilitation Continuum of Care Program is designed for any patient who has experienced a traumatic or acquired brain injury. As children progress through the stages of brain injury recovery, they may require a broad range of specialized services to meet their individual needs. As a result, many children will receive a combination of services provided in each of the following inpatient programs: Brain Injury Responsiveness, Brain Injury Rehabilitation, and Home and School Re-Entry.
Our program is designed for any patient who has experienced an injury to the central nervous system (CNS) including:
Traumatic Brain Injuries
» Motor vehicle/ATV accident
» Gunshot wound/penetration wound
Acquired Brain Injuries
» Cardiac arrest
» Stroke
» Neoplasms/brain tumor
» Encephalitis
» Meningitis
» Falls
» Non-accidental head trauma
» Drug overdose/poisoning
» Drowning/asphyxia
» Prematurity
» Epilepsy
Brain Injury Responsiveness Program
Designed for children and adolescents who continue to exhibit altered arousal and/or limited ability to interact with their environment and are not yet or inconsistently following commands (Unresponsive Wakefulness Syndrome/Minimally Conscious State).
» Determine the level of consciousness and monitor using evidence-based measures
» Evaluate for barriers to recovery of consciousness
» Normalize sleep wake cycle
» Improve alertness during the day
» Initiate sensory stimulation treatments
» Initiate a medically appropriate rehabilitation program
Brain Injury Rehabilitation Program
» Designed for recovery from acute confusion and/or post-traumatic amnesia (PTA) and beyond
» Provide orienting information to promote increased environmental awareness
» Creation of a “Memory Log”
» Management of behavioral agitation
» Intensive multidisciplinary rehabilitation

11

12
Home and School Re-Entry Program
Designed to support children and their families as they navigate the transition from hospital back into their home, school, and community environments.
» Neuropsychological evaluation during admission
» Enrollment in home-bound educational services while hospitalized (when appropriate)
» Work with families and schools to develop an individualized plan for academic re-entry
» Provide families with information about special education supports through school
» Support family in identifying and scheduling relevant follow-up and outpatient appointments
» Coordination with insurance to obtain necessary discharge prescriptions and home equipment
Continuous Goals Throughout the Brain Injury Continuum of Care Programs
» Inclusion of rehabilitation and child life services
» Receipt of neuropsychological services
» Respiratory therapy, tracheostomy, and ventilator management
» Optimization of medication and respiratory needs
» Prevention of secondary complications
» Trial for assistive technology for communication
» Determine long-term care needs (e.g., school and home plans post discharge)
» Education, training, and support for families and caregivers
» Spasticity management

13
PATIENT STORYPatient: Bryan Iverson
Bryan Iverson was a healthy, 15-year-old up until he was found unconscious at the gym. Doctors at an El Paso, Texas emergency room first thought he was dehydrated, but after he stopped breathing and had a seizure, they knew something more was wrong. A CT scan confirmed he had a severe brain bleed.
Surviving multiple surgeries, Bryan had a tracheostomy, was put on a ventilator and had G-tube placed to help his body recover. He was in a coma over the course of three weeks before he finally woke up. His family recalls Bryan being sedated and neurostorming, a typical response for severely brain injured individuals. But because his vitals were stable and his brain pressure was under control, his doctors said he was ready for rehabilitation at Nexus Children’s Hospital.
Once Bryan arrived at Nexus Children’s Hospital, Bryan started making improvements right away. His sister, Michelle Mendez, explained, “My mother went with Bryan and I would video call them every day. I literally saw improvements each day after he started rehabilitation. The therapies he performed really helped him.”
Rita Guillory, Respiratory Manager at Nexus Children’s Hospital said, “Bryan was fortunate to have a family that supported and encouraged him to participate in all aspects of his care. Although he admitted with a stable trach, Bryan faced challenges in managing his secretions. To help him maintain a good airway clearance, he worked through aggressive pulmonary therapy using cough assist, breathing treatments, and vest therapy. He always challenged himself to do more and more each day.”
Michelle explained, “The first hospitals we were at gave us worst case scenarios, so we were ready for the worst, and didn’t expect him to get off the ventilator or trach but look at him now! When he came home, he was off everything and all his medications. He’s doing so well and is really looking forward to starting school again.”
It was a miracle when Bryan woke up!
We tell him we like him better now, but really, we’re just happy that he’s made the progress he needed to and that he’s home.
Michelle Mendez Patient’s Sister

14
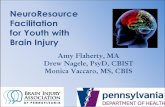
Figures 1-2: Average Total WeeFIM-II Score for Children Diagnosed with Traumatic Brain Injury (fig. 1) and Diagnosed with Non-Traumatic Brain Injury (fig.2). The Reported National Average is That of Similar Facilities Types (w1140).
fig.1 & fig.2 Nexus Children’s Hospital Outcomes Compared to Published National Statistics
Nexus Children’s Hospital WeeFIM Total National WeeFIM Total
Traumatic Brain Injury Non-Traumatic Brain Injury
MEASUREMENT OUTCOMES Nexus Children’s Hospital outperforms national averages.
Nexus Children’s Hospital outperformed the national average for patients with traumatic brain injuries (TBIs).

15
Functional Recovery as Assessed by the WeeFIM-II
Sample characteristics for the WeeFIM-II.
Analyses presented only children with severe non-penetrating, traumatic brain injury (Glasgow Coma Scale [GCS] score between 3 and 8) were included in the analyses below (n = 10).
Ages ranged from 8-21 | 80% male
Figures 3-6: Change in WeeFIM Ratings from Admission to Discharge as assessed by Wilcoxon Signed Ranks Test for dependent, non-normally distributed, ordinal data. *p > .05
fig.4 Average Change in WeeFIM
0
1
2
3
4
5
0
1
2
3
4
5
fig.5 WeeFIM-II Mobility Admission Discharge
Admission Discharge
0
1
2
3
4
5
0
1
2
3
4
5fig.6 WeeFIM- II Cognition Admission Discharge
fig.3 WeeFIM-II Self-Care Admission Discharge 0
WeeFIM Score Range:
Self-Care 8-56 Cognition 5-35
Mobility 5-35 Total Score 18-126

16
72 1093 61ADMISSION0
5
10
15
20
0
20
40
60
80
100
PATIENT CASE STUDY Background Data with Patient with Traumatic Brain Injury
Age: 16-year-old female
Injury Severity: Severe traumatic brain injury (initial GCS of 6, imaging showing subarachnoid hemorrhages and diffuse axonal injury) and polytrauma. She required ventilator support and had limited success with daily weaning trials.
LOS: 172 days
Comorbidities: None
Admission Summary:
» Presentation consistent with a disorder of consciousness (e.g., no purposeful movements, disrupted sleep/wake cycles), vent-dependent, and g-tube dependent
» Hospital stay was complicated by fevers, infection requiring antibiotics, mild colonic ileus, and a seizure-like event
Discharge Summary: Functional gains included de-cannulation, advancement to regular diet, and emergence from a DOC. She was able to ambulate, but required assistance for some ADLs. Targeted neuropsychological evaluation showed a significant change in her overall cognitive skills, with specific deficits in language and memory. Recommendations included close supervision for safety, accommodations in the school setting, and evaluation through vocational rehabilitation.
fig. 10 Average Change in WeeFIM Admission Discharge
WeeFIM Score Range:
Self-Care 8-56 Cognition 5-35
Mobility 5-35 Total Score 18-126
fig. 9 Disorder of Consciousness Trajectory
72 1093 61ADMISSION0
5
10
15
20
0
20
40
60
80
100
Total Score
Weeks
Wessex Head Injury Matrix JFK Coma Recovery Scale
FOUR Coma Scale Coma Near Coma Scale
Figure 10: Change in WeeFIM Ratings from Admission to Discharge.

17
DISORDER OF CONSCIOUSNESS PROGRAMDepending on the severity of an injury, an individual can experience impaired consciousness resulting in confusion and disorientation, as well as more acute disorders of consciousness (DOC) including coma, persistent vegetative state (PVS), and minimally conscious state (MCS).
Nexus Children’s Hospital offers a holistic program that combines a variety of specialties, including neuropsychology, neuropharmacology, physical, occupational, and speech therapy, to help improve the wakefulness of patients.
Patients are monitored using the Wessex Head Injury Matrix, JFK Coma Recovery Scale, FOUR coma scale, and Rappaport – Coma/Near Coma Scale to capture glimpses of changes in patient responsiveness.
Wessex Head Injury Matrix assesses a range of behavior from lower level responses (e.g., eyes open) to remembering events across a 24-hour period. Number given reflects the highest order behavior demonstrated (e.g., chooses an object when requested).
JFK Coma Recovery Scale assesses levels of responsivity to sensory stimuli (e.g., auditory, tactile, visual), ability to follow commands, use of objects, and reliability of communicative responses (e.g., affirmative gestures, verbal yes/no). When a patient demonstrates functional object use and consistent communicative responses, they have emerged from a DOC.
FOUR Coma Scale assesses eye and motor responses, brainstem reflexes, and respiration pattern. Higher scores mean improved responsivity.
Coma/Near Coma Scale assesses responses to multiple sensory modalities (e.g., vision, hearing, smell, tactile), pain, and responsivity to simple commands. Higher score indicates consistent responses and emerging responsivity to simple commands.
The majority of patients in the program emerged from a DOC. However, all of these patients had very severe injuries, and many would not have otherwise received the level of rehabilitation care to help them continue to progress because their early trajectories showed minimal changes in their levels of responsiveness. Nexus Children’s Hospital’s DOC program gives this group of patients a chance to show their potential and prevent secondary complications as their level of responsiveness improves.
2019 Statistics for Patients with with Acquired Brain Injury**
patients who left without contractures
of patients successfully decannulated*50%
*6 of the 8 patients had tracheostomies. ** Only three patients presented with acquired brain injuries of this severity. Of note, one of these patients was described as having severe irreversible cerebral dysfunction and another had a severe anoxic injury due to a near drowning. These two patients did not emerge from a disorder of consciousness. However, the third patient did emerge from a DOC.

18
2019 Statistics for Patients with Traumatic Brain Injury*
Patients who emerged from DOC during admission (%) 88%
Patients who emerged from DOC in <1 month 25%
Patients who emerged from DOC in 2 months 12.5%
Patients who emerged from DOC in 3 months 25%
Patients who emerged from DOC in > 3 months 12.5%
Patients able to complete neuropsychological testing prior to discharge 37.5%
*Due to differences in developmental expectations and lack of clinically validated measures for assessing disorders of consciousness in children under the age of three, two children under three were excluded from this analysis.
Gender (male) 63%
Gender (female) 37%
Non-penetrating head injury 88%
Penetrating head injury 13%

19
2 3 41ADMISSION
0
3
6
9
12
15
PATIENT CASE STUDY Background Data with Patient with Acquired Brain Injury
Age: 5-year-old male
Injury Severity: New onset right sided hemiplegia, right-sided partial gaze palsy, right sided facial droop, bulbar dysfunction, and potential seizure. He was also had associated aphasia and encephalopathy. Neuroimaging significant for diffusion restriction throughout the left hemisphere and subtle cortical edema in the right hemisphere. His EEG noted left hemispheric cerebral dysfunction superimoposed on diffuse encephalopathy of non-specific etiology, with no noted seizures. Genetic panels noted a gene associated with alternating hemiplegia of childhood.
LOS: 35 days
Comorbidities: Speech delay and autism
Admission Summary:
» Presentation consistent with a disorder of consciousness (e.g., no purposeful movements, disrupted sleep/wake cycles)
» He had alternating right to left hemiplegia, spasticity in both ankles with clonus, and poor head and trunk control
» He was g-tube dependent, dependent for all transfers and ADLs, and poor secretion managment
Discharge Summary: Functional gains included emergence from a disorder of consciousness (i.e., appropriate vocalizations, following one step commands, improvements in sleep/wake cycle), ability to assist with some ADLs (i.e., pulling up his pants when dressing), and maintaining head and trunk control when ambulating. He was also beginning to improve in his managment of his oral secretions. Recommendations included ongoing outpatient therapies and home nursing care.
fig. 12 Average Change in WeeFIM Admission Discharge
WeeFIM Score Range:
Self-Care 8-56 Cognition 5-35
Mobility 5-35 Total Score 18-126
fig. 11 Disorder of Consciousness Trajectory
2 3 41ADMISSION
0
3
6
9
12
15
010203040
Total Score
Weeks
Wessex Head Injury Matrix JFK Coma Recovery Scale
FOUR Coma Scale Coma Near Coma Scale
Figure 12: Change in WeeFIM Ratings from Admission to Discharge.

20
CHANGES HEALTH & WELLNESS PROGRAMOur inpatient weight loss program for children ages 3 to 21 years old is the only inpatient program in the United States that also specifically addresses the needs of children with Prader-Willi Syndrome (PWS). Our strategies include a safe, structured environment for children with established weight control problems who have found traditional outpatient programs unsuccessful.
Our expert team addresses the individual’s medical and behavioral needs including issues characteristic of persons with PWS. The team members who support our patients and direct our evidenced based programs include psychiatry, neuropsychology, behavioral psychology, behavioral nurse practitioners, pediatricians, physical medicine and rehabilitation, nursing, registered dietician, pulmonology, respiratory therapy, recreational therapy, and physical, occupational, and speech therapies.
Nexus Children’s Hospital is dedicated to seeing each patient reach his or her health goal and maintain that goal after discharge from the program.
Program Goals
» Decrease BMI
» Resolve weight-related conditions
» Develop strategies to manage behavior
» Decrease unstructured time
» Develop coping skills for at home, school, or in the community
» Improve overall quality of life
» Decrease burden of care

21
PROGRAM PROGRESS 2019
was the Shortest and Longest Length of Stay (varied by patient)
4 49 WEEKS
Total Pounds Lost918.6
100% of Patients Saw at Least BMI
Decrease 17.2%
Avg. BMI Decrease7.9

22
PATIENT STORYPatient: Christopher Hernandez
Christopher Hernandez was diagnosed with Prader-Willi Syndrome (PWS) at five years old. His mother, Joanne, explained there were few places she could turn to for help or support. It wasn’t until he was six that she found the program for children with PWS at Nexus Children’s Hospital. After spending three months with Christopher in the program, Joanne and her son returned home to Chicago to try and make day-to-day life work.
Individuals with PWS lack the internal restraints that most people develop as they mature. Joanne explained her son was motivated by food, and because he didn’t have the coping skills to deal with not having that desire met immediately, he would become angry. She explained, “When Christopher turned nine, it was like a switch went off. All of the behaviors involved with someone with PWS that I read and heard about seemed to turn on at once. His aggression made it difficult for me as his mother and sole caregiver to manage him as well as my other children, husband, house, and everything else.”
Joanne took Christopher to a hospital in Chicago where he saw nearly 15 specialists, but nothing worked. Many places turned her away because they weren’t equipped to work with him, while others simply wouldn’t prescribe certain medications that were known to help individuals with PWS. Inpatient psychiatric therapy also wasn’t successful since Christopher took away bad ideas from other kids.
As his aggression increased and he gained weight — up to 318 pounds at this time — Joanne felt backed into a corner. Now 11 years old, he needed help and Joanne was desperate to find a resource — but her options were limited. Hearing that Nexus Children’s Hospital reopened their program, she knew that was the place for Christopher.
“Since we’d been at Nexus before, we were anticipating similar feedback about Christopher’s progress,” Joanne said. “To my surprise, he was doing better than expected and I was getting good reports. He lost weight and was working with a teacher. He also participated in different activities.”
Joanne also explained that she and her husband realized they wouldn’t be able to capture what Nexus could give him, saying: “The boundaries, food security, routine, psychiatric medicine and support — all of that helped him get better and be happier. We feared bringing Christopher home would ruin all the progress he had at Nexus, so we concluded that a residential program would be best for him. That would enable him to live a more normal life and he’s worked hard and deserves that.”
As far as Christopher’s time at Nexus Children’s Hospital, he lost over 120 pounds and was able to celebrate with a special party.
He was doing better than expected and I was getting good reports. He lost weight and was working with a teacher. He also participated in different activities.
Joanne Hernandez Patient’s Mother

23

2929 Woodland Park Drive | Houston, Texas 77082 | 281.293.7774
nexuscontinuum.com
NEXUS SPECIALTY HOSPITAL
NEXUS NEURORECOVERY CENTER
NEXUS CHILDREN’S HOSPITAL
COLLEGESTATION
LUFKIN
CLEAR LAKE
SUGARLAND
TEXASMEDICALCENTER
KATY
CONROE
Tomball • 21 milesKingwood • 28 milesTexas Medical Center • 41 milesSugar Land • 55 miles
Clear Lake • 57.9 milesBeaumont • 97 milesLufkin • 106 miles
DISTANCES FROM COMMON LOCATIONS