©2015 The Advisory Board Company advisory.com 11 Directions for customizing the slides with...
14
©2015 The Advisory Board Company • advisory.com 1 1 • Directions for customizing the slides with hospital-specific information are included on green boxes throughout the presentation. The green boxes should be deleted before presenting the slides to your target audience. • Alternatively, this presentation can be given without any hospital-specific data by deleting the slides that contain green boxes. • The notes section of each slide contains talking points for presenting each slide and more details about the data they contain. Access this tool: advisory.com/ccc/PerinatalToolkit Source: Crimson Continuum of Care interviews and analysis. Perinatal Patient Safety Briefing Deck To help perinatal patient safety leaders make the case to administrators and physicians for investing in improving perinatal patient safety Purpose This tool consists of a PowerPoint presentation that contains national data about perinatal care variation and complications and the need for perinatal patient safety efforts. It also contains template slides that perinatal patient safety leaders can modify to include hospital-specific outcomes data and program analyses. Overview Tool 3 Notes and Considerations
-
Upload
arline-hudson -
Category
Documents
-
view
215 -
download
1
Transcript of ©2015 The Advisory Board Company advisory.com 11 Directions for customizing the slides with...

©2015 The Advisory Board Company • advisory.com
11
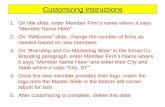
• Directions for customizing the slides with hospital-specific information are included on green boxes throughout the presentation. The green boxes should be deleted before presenting the slides to your target audience.
• Alternatively, this presentation can be given without any hospital-specific data by deleting the slides that contain green boxes.
• The notes section of each slide contains talking points for presenting each slide and more details about the data they contain.
Access this tool: advisory.com/ccc/PerinatalToolkit
Source: Crimson Continuum of Care interviews and analysis.
Perinatal Patient Safety Briefing Deck
To help perinatal patient safety leaders make the case to administrators and physicians for investing in improving perinatal patient safety
Purpose
This tool consists of a PowerPoint presentation that contains national data about perinatal care variation and complications and the need for perinatal patient safety efforts. It also contains template slides that perinatal patient safety leaders can modify to include hospital-specific outcomes data and program analyses.
Overview
Tool 3
Notes and Considerations

Crimson Continuum of Care
Making the Case for Investing in Perinatal Patient Safety

©2015 The Advisory Board Company • advisory.com
3
Source: “National Vital Statistics System Birth Data, 2013,” CDC; Weiss, A, “Overview of Hospital Stays in the US, 2012,” Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality , October 2014; Weiss, A, “Characteristics of Operating Room Procedures in U.S. Hospitals, 2011,” Healthcare Cost and Utilization Project, February 2014; Crimson Continuum of Care interviews and analysis.
Perinatal Care Plays Prominent Role in Hospitals
Babies delivered in the United States annually
3.9MHospital stays related to perinatal care
22%Where cesarean sections rank among operating room procedures in the U.S.
#1U.S. Hospitals’ Perinatal Care Volume
Babies delivered in 2014
###Hospital stays related to perinatal care
##%Number of cesarean sections performed annually
##[NAME OF HOSPITAL] Perinatal Care Volumes
Work with your Crimson Dedicated Advisor to customize this slide with your own data.
Consider adding a slide subtitle summarizing your institution-specific data, such as: Births Account for X% of Stays at [Name of Hospital]

©2015 The Advisory Board Company • advisory.com
4
15%-20%
21%-25%
26%-30%
31%-35%
36%-40%
41%-45%
46%-50%
51%-55%
>55%<15%
Variation Seen Even among Physicians in the Same Hospital
Source: Kozhimannil, KB et al, “Cesarean Delivery Rates Vary Tenfold among US Hospitals; Reducing Variation May Address Quality and Cost Issues,” Health Affairs, 32, no. 3 (2013): 527-535; Crimson Continuum of Care interviews and analysis.
Perinatal Practice Patterns Vary Widely
Department Chair Women’s Health Services
500-bed Hospital in the Midwest
“Initially, our physicians said that the C-section rates varied because of differences in patient population, but then they realized that there were actually differences in how they practiced medicine.”
Distribution of C-Section Rates in US Hospitals, 2009n=593 hospitals with at least 100 births

©2015 The Advisory Board Company • advisory.com
5
Patient Characteristics Explain Only Portion of Variation
Sources: Glance LG, et al, “Rates of Major Obstetrical Complications Vary Almost Fivefold Among US Hospitals,” Health Affairs, 33, no. 8 (2014):1330-1336; Grobman WA, et al, “Can differences in obstetric outcomes be explained by differences in the care provided? The MFMU Network APEX Study,” Am J Obstet Gynecol, 211, no. 147 (2014):e1-16; Crimson Continuum of Care interviews and analysis.
Complication Rates Indicate Room for Improvement
Study authors found that while volume and case mix have some impact on complication rates, they do not explain the full difference. Varying outcomes likely resulted from differences in clinical performance.
Vaginal Deliveries Cesarean Deliveries
22.6 20.9
10.4
4.4
Low Quality Hospitals High Quality Hospitals
Complication Rates At “High” and “Low” Quality Hospitals, 2010
Percent of inter-hospital variation in complication rates that can be explained by patient characteristics, according to another study
20-40%

©2015 The Advisory Board Company • advisory.com
6
Substantial Cost Opportunity with Standardizing Perinatal Care
Source: Elixhauser A, Wier LM, “Complicating Conditions of Pregnancy and Childbirth, 2008,” AHRQ Healthcare Cost and Utilization Project Statistical Brief #113 (2011); Podulka J et al, “Hospitalizations Related to Childbirth, 2008,” AHRQ Healthcare Cost and Utilization Project Statistical Brief #110 (2011); Crimson Continuum of Care data, interviews and analysis.
The Impact of Reducing Variation in Complications
Average annual per-hospital cost opportunity of reducing physician outliers for vaginal and cesarean deliveries
$1.2M
Maternal admissions with complications are more costly than stays without complications
1.3x
Average total hospital costs associated with maternity complications, nationwide
5%
4.5
3.1
Increase of 1.4 days to average LOS
Complications Increase Length of Stay for C-Sections

©2015 The Advisory Board Company • advisory.com
7
Crimson Data Identifies Areas for Improvement
Source: Crimson Continuum of Care.
Taking a Look at [Hospital’s] Performance
Measure Number of Cases
Hospital Rate/1000
Cohort Average Rate /1000
Performance
Birth Trauma Rate – Injury to Neonate (PSI 17)
3/524 5.73 3.60 Below Average
Obstetric Trauma Rate – Vaginal Delivery With Instrument (PSI 18)
0/24 0 118.81 Above Average
Obstetric Trauma Rate – Vaginal Delivery Without Instrument (PSI 19)
9/289 31.14 18.67 Below Average
Cesarean Delivery Rate (IQI 21)
173/459 37.69 33.68 Below Average
Vaginal Birth After Cesarean Rate, Uncomplicated (IQI 22)
13/109 11.93 13.46 In-line with Average
This table contains sample data. Work with your DA to customize this slide with data from your own institution by selecting appropriate metrics and filling out table with institution- and cohort-specific data.

©2015 The Advisory Board Company • advisory.com
8
Sentinel Events Often Preventable, Feed High Liability Costs
Sources:Bacak SJ et al (editors), “State Mortality Review: Accomplishments of Nine States,” Center for Disease Control and Prevention, 2006, https://www.cdph.ca.gov/data/statistics/Documents/MO-CDC-ReportAccomplishments9States.pdf ; Greve, P. “Labor Pains: Liability Trends in Obstetrics,” Medical Liability Monitor, 2009, http://www.scpcf.com/pdf/mlm_laborpains08_09.pdf; “Report: 2015 Hospital and Physician Professional Liability Benchmark Analysis,” AON Thought Leadership, http://www.aon.com/risk-services/thought-leadership/2015-report-hospital-professional-liability-overview.jsp ; “Obstetrics,” CRICO, https://www.rmf.harvard.edu/Clinician-Resources/Specialty-Reference-Tag/Obstetrics ; Crimson Continuum of Care interviews and analysis.
Also Need to Improve OB Emergency Response
CDC State Maternal Mortality Review Committee
“Although maternal mortality is a relatively rare event in the United States, each year an estimated 1,000 American women die of pregnancy-related complications such as hemorrhage, embolisms, and hypertension. These deaths are devastating to these women’s families, and they have a profound impact on health care providers and communities.About half of these deaths are believed to be preventable.”
Ranking of OB/Gyn among all specialties in claims paid out from 1985-2007 (more than $3B in total)
1st
Projected loss per birth for hospital obstetrics claims in 2015
$163
OB malpractice cases involving high-severity injuries, including maternal and infant deaths
52%

©2015 The Advisory Board Company • advisory.com
9
Organizational Structures Play a Role in Facilitating Patient Safety
Source: The Joint Commission Office of Quality and Patient Safety, “Sentinel Event Data: Root Causes by Event Type, 2004-2014,” The Joint Commission, http://www.jointcommission.org/assets/1/18/Root_Causes_by_Event_Type_2004-2014.pdf ; Crimson Continuum of Care interviews and analysis.
Systemic Factors Often Underlie Poor Outcomes
39%
41%
48%
52%
63%
68%
70%
79%
Neonatal Events Maternal Events
Most Common Root Causes for Sentinel Events Reviewed by TJC, 2004-2014
Human Factors(staffing, education)
Communication(among providers, with patient)
Assessment(clinical assessment, care decisions)
Leadership(organizational structures, culture)

©2015 The Advisory Board Company • advisory.com
10
Move Follows Risk Reduction Goal Set by Liability Insurer
Source: Pettker CM et al., “A Comprehensive Obstetric Patient Safety Program Reduces Liability Claims and Payments,” Am J Obstet Gynecol, 211, no. 4(2014):319-325, http://www.ajog.org/article/S0002-9378(14)00434-7/pdf; Pettker CM et al., “Impact of a Comprehensive Patient Safety Strategy on Obstetric Adverse Events,” Am J Obstet Gynecol , 200 (2009):492e1-492e8; Crimson Continuum of Care interviews and analysis.
Implementing a Comprehensive OB Safety Program
Key Components of Yale-New Haven Hospital’s Obstetric Patient Safety Program
Standardized guidelines for high-risk patient care practices
Required electronic fetal monitoring interpretation certification
Program evaluation, including an outside expert review and safety attitudes survey
Obstetric patient safety nurse and obstetric hospitalists
Obstetric patient safety committee, with anonymous event reporting
Obstetric team training
Case in Brief: Yale-New Haven Hospital
• 1,500-bed academic medical center in New Haven, CT
• Roughly 5,000 deliveries annually
• Developed and implemented a comprehensive obstetrics patient safety program, in collaboration with its malpractice liability carrier, to improve care quality and reduce liability costs
• Introduced nine interventions over a four-year timespan
• Results show reductions in both adverse outcomes and liability claims and payments

©2015 The Advisory Board Company • advisory.com
11
Also Cut Liability Claims and Payments
1) Mean quarterly rate of deliveries with at least one adverse outcome from the adverse outcome index (includes blood transfusion, maternal death, maternal ICU admission, maternal return to OR or L&D, uterine rupture, third- or fourth-degree laceration, Apgar score <7 at 5 min, fetal traumatic birth injury, intrapartum or neonatal death > 2500 g, or unexpected admission to neonatal ICU > 2500 g and for > 24 hours).
2) 1998-20023) 2003-2007
OB Patient Safety Program Reduced Complications
Total Liability Payments per 1,000 Deliveries
Prior to patient safety program2$2.2M
$123K After patient safety program3
2.9%
2.1%
Adverse Outcome Rates1 Improved Across Implementation Period
Source: Pettker CM et al., “A Comprehensive Obstetric Patient Safety Program Reduces Liability Claims and Payments,” Am J Obstet Gynecol, 211, no. 4(2014):319-325; Pettker CM et al., “Impact of a Comprehensive Patient Safety Strategy on Obstetric Adverse Events,” Am J Obstet Gynecol , 200 (2009):492e1-492e8; Crimson Continuum of Care interviews and analysis.
First Half Second Half

©2015 The Advisory Board Company • advisory.com
12
Best Practices from Leaders in the Field
Source: Crimson Continuum of Care interviews and analysis.
Nine Elements of a Perinatal Patient Safety Program
Laying the Foundation
1. Assessment of Potential Perinatal Patient Safety Problems
2. Administrative, Physician Support of Patient Safety Efforts
Building Infrastructure
3. Perinatal Patient Safety Nurse
4. Perinatal Patient Safety Committee
5. Process for Standardizing Care Protocols
6. 24x7 Physician Coverage of Labor & Delivery Unit
Strengthening Provider and Staff Training
7. Established Team Communication Framework
8. Electronic Fetal Monitoring Training
9. Multidisciplinary Emergency Drills

©2015 The Advisory Board Company • advisory.com
13
1. Perinatal Patient Safety Problem Identification
2. Administrative, Physician Support of Patient Safety Efforts
3. Perinatal Patient Safety Nurse
4. Perinatal Patient Safety Committee
5. Multidisciplinary Team Focused on Standardizing Perinatal Care Protocols
6. 24x7 Physician Coverage of L&D Unit
7. Common Team Communication Framework
8. Electronic Fetal Monitoring Training
9. Multidisciplinary Emergency Drills
How Does [Hospital Name] Compare?
Copy, paste, and delete the Harvey Balls on the right side of the slide to indicate which components of a best practice patient safety program your hospital has fully implemented, partially implemented, or not yet implemented.
Evaluating Our Current Perinatal Patient Safety Program

©2015 The Advisory Board Company • advisory.com
14
Initial Steps Toward Improving Perinatal Patient Safety
Where Do We Start? Modify the suggested next steps below to customize this slide for your institution.
Suggested Next Steps
1. Designate a clinical and administrative leader for perinatal patient safety
2. Work with IT and department leadership to review current outcomes data and clinical processes to identify the highest-need perinatal patient safety problems
3. Present information about perinatal patient safety trends at labor & delivery department meeting to inform providers and staff of new initiative and identify those who may be interested in contributing