
2015 RA-UK ASM ABSTRACTS BOOKLET€¦ · 2015 RA-UK ASM . ABSTRACTS BOOKLET. 2 . Benefits of RA-UK...
45
1 2015 RA-UK ASM ABSTRACTS BOOKLET
Transcript of 2015 RA-UK ASM ABSTRACTS BOOKLET€¦ · 2015 RA-UK ASM . ABSTRACTS BOOKLET. 2 . Benefits of RA-UK...
1
2015 RA-UK ASM ABSTRACTS BOOKLET

2
Benefits of RA-UK membership
Joining RA-UK helps to financially support your local society. RA-UK membership confers some additional benefits over and above ESRA membership
You will become a FULL member in YOUR national society RAUK, actively supporting national goals in education and research.
Payment of annual ESRA membership fee by Direct Debit via the RAUK administration (AAGBI)*
15% reduction on all RAUK organised course and Annual Scientific Meeting
Eligibility for small grant awards Free copy of "A Pocket Guide to Ultrasound Guided
Regional Anaesthesia" when you first join * As ESRA is a European society, collection of their fees by Direct Debit is
not available and it requires annual payment by credit card. The AAGBI will
collect both payments and then pay ESRA for you, relieving you of the
inconvenience of having to re-register every year. Please see our Frequently Asked Questions for further information about RA-UK membership and its benefits on www.ra-uk.org .
You cannot join RA-UK (Full member - £25, Trainee member - £10) without ESRA membership ( Full member - €120, Trainee member - €35). ESRA membership includes a subscription to Regional Anaesthesia and Pain Medicine. You may join ESRA without joining RA-UK - to do this please visit the www.esraeurope.org .

3
2015 RA-UK ASM, TOWN HALL, OXFORD
PROGRAMME
Thursday 14 May 2015
AM: Update lectures; PM: Workshop sessions
08:50–09:20 Registration, tea & coffee
09:20–09:30 Welcome
09:30–09:55 Adductor canal block – Truths and myths 2G02, 2G03 Dr Thomas Bendtsen, Denmark
09:55–10:20 Regional anaesthesia in the morbidly obese 1I03, 1D02, 2E01, 2G01, 2G02, 2G03, 2G04, 3A09, 3E00 Prof Rob Raw, USA
10:20–10:45 “RANTS” Regional Anaesthesia Non-Technical Skills 1I03, 3A09 Dr Morné Wolmarans, Norwich
10:45–11:15 Tea & coffee
11:15–11:40 Peripheral nerve catheters: Why do them and how to overcome the
obstacles to placement 1A02, 1D02, 1H02 Dr Brandon Winchester, USA
11:40–12:05 Regional anaesthesia in patients with pre-existing neuropathy – Adapt
or avoid? 1D02, 2G01, 3A09 Dr Philipp Lirk, Netherlands
12:05–12:30 What’s best for breast Dr Amit Pawa, London 2G01, 2G03, 1D02
12:30–13:30 Lunch
13:30–14:30 Workshop session 1 2G03, 3A09
Upper limb
a. Above clavicle
b. Axillary
c. Elbow and forearm
14:30–15:30 Workshop session 2 2G03, 3A09
Lower limb
a. Femoral/saphenous, LCNT and obturator
b. Sciatic parasacral to popliteal
c. Ankle
15:30–16:00 Tea & coffee
4
16:00–17:00 Workshop session 3 2G03, 3A09
Body wall and neuraxis
a. Neuraxial
b. Paravertebral and chest wall (Pecs/
Serratus plane)
c. Abdominal wall
17:00 Close
Friday 15 May 2015
AM and PM: Scientific Programme
08:15–08:50 Registration, tea & coffee
08:50–09:00 Welcome
09:00–09:35 IV lidocaine in major surgery 1A02, 2G02, 3A09 Dr Philipp Lirk, Netherlands
09:35–10:10 Hand surgery using Wide Awake Local Anaesthesia No Tourniquet (WALANT); keeping the anaesthetist involved 1A02, 2G02 Mr Alistair Phillips, Southampton
10:10–10:45 Ultrasound guided approach to the lumbosacral plexus 2G02, 2G03 Dr Thomas
Bendtsen, Denmark
10:45–11:15 Tea & coffee2
11:15–12:00 Liposomal bipivacaine – Holy Grail or money pit 1A02, 1D02, 1H02 Dr Brandon
Winchester, USA
12:00–13:00 DEBATE: ‘This house believes that the use of ultrasound enables the
safe conduct of regional anaesthesia in asleep patients’ 1I03, 1D02, 2E01, 2G01, 2G02, 2G03, 2G04, 3A09, 3E00
Pro: Prof Rob Raw, USA
Con: Dr William Harrop-Griffiths, London
13:00–14:15 Lunch & AGM
14:15–14:45 Nerve injury and nerve repair 2G04, 3A09 Mr Anthony Macquillan, Southampton
14:45–15:35 Bruce Scott lecture: Is intraneural injection so bad and are we just missing the point? 1D02, 1I03, 2E01, 2G01, 2G02, 2G03, 2G04, 3A09, 3E00 Prof Rob Raw, USA
15:35–16:05 Tea & coffee
16:05–17:00 Problem-based discussion with expert panel
17:00 Close

5
3102781 Ask The Patient About Their Awake Elbow, Forearm, Wrist And Hand Surgery An Awake Upper Limb Surgery Survey Asif, Sunita; Russon, Kim Rotherham NHS Foundation Trust Introduction At Rotherham NHS Foundation Trust (RFT), it is routine practice to offer patients the choice to stay awake during upper limb surgery. The surgery is performed using a brachial plexus block instead of general anaesthesia. This technique has many patient and hospital benefits. This survey follows on from an 'Awake shoulder surgery survey (1),' that we presented at the RAUK ASM in 2012, which showed good patient satisfaction with having awake shoulder surgery. This survey aims to explore the patient's experience of staying awake during elbow, forearm, wrist and hand surgery at RFT. Method Adult patients booked for elective upper limb surgery were eligible, provided they spoke english and were able to lie still. Pre operatively, the surgeon discussed the option of awake upper limb surgery with the patient. The RFT 'Brachial plexus block for elbow, forearm, wrist and hand surgery' booklet (2) was provided by nurses in pre-assessment clinic 4-6 weeks pre surgery. On the day of surgery, the Anaesthetist discussed anaesthetic options. If the patient agreed to stay awake, they received the questionnaire and a stamped addressed envelope in which to return the questionnaire following surgery. Oral paracetamol and ibuprofen (sustained release) were administered as premedication. Ultrasound guided brachial plexus nerve block was performed using 0.75% Ropivacaine. Post operatively, patients were given oral analgesia and the RFT 'Looking after your arm and hand after a block' booklet (3). Patients could be treated as daycase provided they met the daycase criteria. Results Between 6th June 2013 and 20th March 2014, 27/39 (69%) patient questionnaires were returned. 2 Consultant Anaesthetists and 3 Surgeons were involved in the cases. Patient demographics: Male 48% (n=13) and Female 52% (n=14). Age Range (years) 43 - 82. Mean Age (years) 63. 67% of patients had hand surgery, 18% wrist surgery, 11% elbow surgery and 4% forearm surgery. Patient responses for 'How soon after your operation did the numbness wear off?' were as follows; 62% next day, 26% night, 4% evening, 4% night/next day and 4% not sure. Patient Questionnaire Responses Yes Mostly No Not sure No comment
Did you receive the booklet* pre surgery? 96% 0 4% 0 0
Was the booklet adequate? 100% 0 0 0 0
Were you comfortable during the nerve block? 85% 15% 0 0 0
Were you comfortable during surgery? 96% 4% 0 0 0
Did the anaesthetist or surgeon give explanations during surgery? 93% 0 7% 0 0
Were the explanations useful? 82% 11% 0 0 7%
After the numbness wore off, was the pain adequately controlled with tablets given? 74% 18% 4% 4% 0
Were you satisfied with your care? 100% 0 0 0 0
Would you have awake surgery again? 100% 0 0 0 0
*RFT Brachial plexus block for elbow, forearm, wrist and hand surgery booklet Conclusion Within our hospital, patients are satisfied with the pre operative information they are receiving. Most patients are comfortable throughout the nerve block and surgery with no conversion to general anaesthesia. Patients reported 100% satisfaction and all would have awake surgery again. We advocate awake upper limb surgery using brachial plexus block as it is a highly successful technique with 100% patient satisfaction and benefits for both patients and the hospital. References
1. Hirst C, Russon K, Shekar M and Maxwell L. Asking the patients about their Awake Shoulder Surgery Survey. RAUK ASM 2012.

6
2. Brachial plexus block for elbow, forearm, wrist and hand surgery. Patient information booklet. Rotherham NHS Foundation Trust
3. Looking after your numb arm and hand after a block. Patient information booklet. Rotherham NHS Foundation Trust.

7
3132947 Formal Assessment Of Patients' Experience Of Audio-visual Distraction When Undergoing Surgery Under Regional Anaesthesia: A Service Evaluation Study Athanassoglou Vassilis; Wallis, Anna; Galitzine, Svetlana; Matthews, James; Pepper, Warwick Oxford University Hospitals NHS Trust Introduction Patient anxiety is common during surgery performed under regional anaesthesia (RA). Intravenous sedation, titrated to patients’ requirements, is therefore widely used. For some patients sedation can be challenging and may lead to complications. In recent years various modalities of audio-visual distraction (AVD), such as music and television and their positive impact on patients’ care have been extensively studied in the setting of surgical procedures (1,2). We set out to conduct a service evaluation of AVD for limb surgery under RA. Methods Multimedia equipment consisting of a Wi-Fi connected tablet device and noise-cancelling headphones has recently become available in our tertiary referral orthopaedic centre and is now offered to patients undergoing limb surgery under RA. Following initial very positive informal patient feedback (3), we initiated a formal assessment of patients' experience with AVD when undergoing surgery under RA. With institutional approval, all patients using AVD were invited to complete a standardised postoperative questionnaire. Results Our care series to date consists of 25 consecutive patients who underwent orthopaedic and/or plastic limb surgery under RA with AVD +/- sedation. Surgical duration varied from around an hour to over nine hours. Nine and 16 patients had upper and lower limb surgery, respectively. Fourteen patients used AVD alone, 11 used AVD in combination with low-dose sedation. All patients reported feeling “very comfortable” or “comfortable”. Twenty one patients rated their experience as “better” than previous GA. All patients were “very satisfied” (24 patients) or “satisfied” (1 patient). All patients stated they would recommend the technique to other patients. Discussion For some patients the only barrier to agreeing to surgery under RA is the anxiety of being “awake” in operating theatre. Intravenous sedation for anxiolysis may lead to complications. The main objective of using AVD is to allay anxiety and decrease the amount of sedation, especially in very anxious and high risk patients. Our care series represents a diverse group of patients. Formal feedback in our group of consecutive patients is very positive. Conclusions We are encouraged by the overwhelmingly positive patient feedback on the use of AVD to facilitate surgery under RA and hope to expand our service to benefit more patients. In an era when not only patient safety and clinical outcomes but also patients’ positive experiences are of paramount importance, AVD is a simple tool to improve experience of appropriately informed patients undergoing suitable procedures under RA. References
1. O’Connor K, Pace N. AVD during spinal anaesthesia for orthopaedic surgery. Journal of Perioperative Practice 2010;20:428-9
2. Sabideen H, Parikh A, Dobbs T, Pay A, Critchley PS. Is there a role for music in reducing anxiety in plastic surgery minor operations? Annals of Royal College Surgeons 2012;94:152-4
3. Athanassoglou V, Galitzine S, Choi D, Matthews J. Patients’ reported experience with novel AVD technique for prolonged upper limb surgery under RA. Regional anesthesia&pain medicine 2014;39:E227

8
3131746 The Incidence And Severity Of Acute Kidney Injury Following The Introduction Of Anaesthetic Guidelines For The Peri-operative Management Of Patients Undergoing Primary Total Knee Replacement Beauchamp, Nigel; Akerman, Harry; Onofrei, Mihaela University Hospital Southampton NHS Foundation Trust Introduction In 2013, new anaesthetic guidelines were introduced on the peri-operative management of patients undergoing primary total knee replacement (TKR). The protocol recommends the use of opiate free spinal, peri-operative use of NSAIDs, Gabapentin, oral opiates and local anaesthetic infiltration. It also limits the amount of intra-operative fluid to avoid urinary catheterisation. However, since the introduction of guidelines there has been a perceived increase in the incidence of acute kidney injury (AKI). The aim of this survey is to measure the incidence and severity of AKI before and after the introduction of the peri-operative protocol. Methods We compared two groups of patients who underwent TKR between 1 April and 31 July 2012 (pre-protocol) and 2014 (post-protocol). Serum creatinine levels were recorded pre-operatively and up to 7 days post-operatively. The severity of AKI was assessed according to Kidney Disease Improving Global Outcome (KDIGO) classification: stage 1, serum creatinine 1.5-1.9 times baseline or ≥ 26.5 μmol/l increase; stage 2, serum creatinine 2.0-2.9 times baseline; stage 3, serum creatinine 3.0 times baseline. The change in creatinine was calculated as the difference or ratio between the highest post-operative and the pre-operative values. Results Table 1. Characteristics of 218 patients who underwent TKR Characteristic AKI (n=42), 19.3% No AKI (n=176), 80.7%
Age, mean ± SD 69 ± 9.9 SD 67.4 ± 11.3 SD
Number of patients (%), 2012 24 (21.4%) 88 (78.5%)
Number of patients (%), 2014 18 (17%) 88 (83%)
% return to baseline creatinine, 2012 62.5%
% return to baseline creatinine, 2014 66.6%
In 2012, two patients developed stage 2 AKI versus seven in 2014 and no patients developed stage 3 AKI in 2012 versus two patients in 2014. Nine out of eleven patients who developed stage 2 and 3 AKI were hypertensive treated with ACEi/ARB, two of these nine patients were also diabetic. The mean BMI of patients with stage 2 and 3 AKI was 38.9. The average amount of intra-operative fluid for these patients was 1.4 L. AKI prolonged the median length of stay by one day in both groups (median LOS without AKI: 7 days in 2012 vs 6 days in 2014). Discussion Postoperative AKI is associated with increased morbidity and length of stay. Our survey has its limitations due to the relatively small number of patients studied, however the incidence of AKI in our population is similar with the percentage quoted in other studies. We have seen an increase in the severity of AKI but we can not reliably attribute this change to the new guidelines as causes of AKI are multifactorial. We recommend TKR patients undergo peri-operative renal risk stratification and avoid NSAIDs if the eGFR is <60. We have adopted a more liberal fluid policy in the elderly and hypovolaemic patients. Conclusions Our anaesthetic protocol aims to reduce variations in practice however it needs to be adapted to match individual patient’s needs. References
1. www.kdigo.org/clinical_practice_guidelines/pdf/KDIGO%20AKI%20Guideline.pdf. 2. Sehgal V et al. Predictors of Acute Kidney Injury in Geriatric Patients Undergoing Total Knee
Replacement Surgery. International Journal of Endocrinology and Metabolism 2014; 12(3): e16713.
9
3132138 Repeatability And Reproducibility Of The Measurement Of Shear Wave Speed At Peripheral Nerve Sites Using Acoustic Radiation Force Impulse In Volunteers Belford, Iain1; McLeod, Graeme1; Coyle, Damien1; Yan, Lingxang2; Lockwood, Heather2; Corner, George2; Munirama, Shilpa3 1NHS Tayside;
2University of Dundee;
3Manchester Royal Infirmary
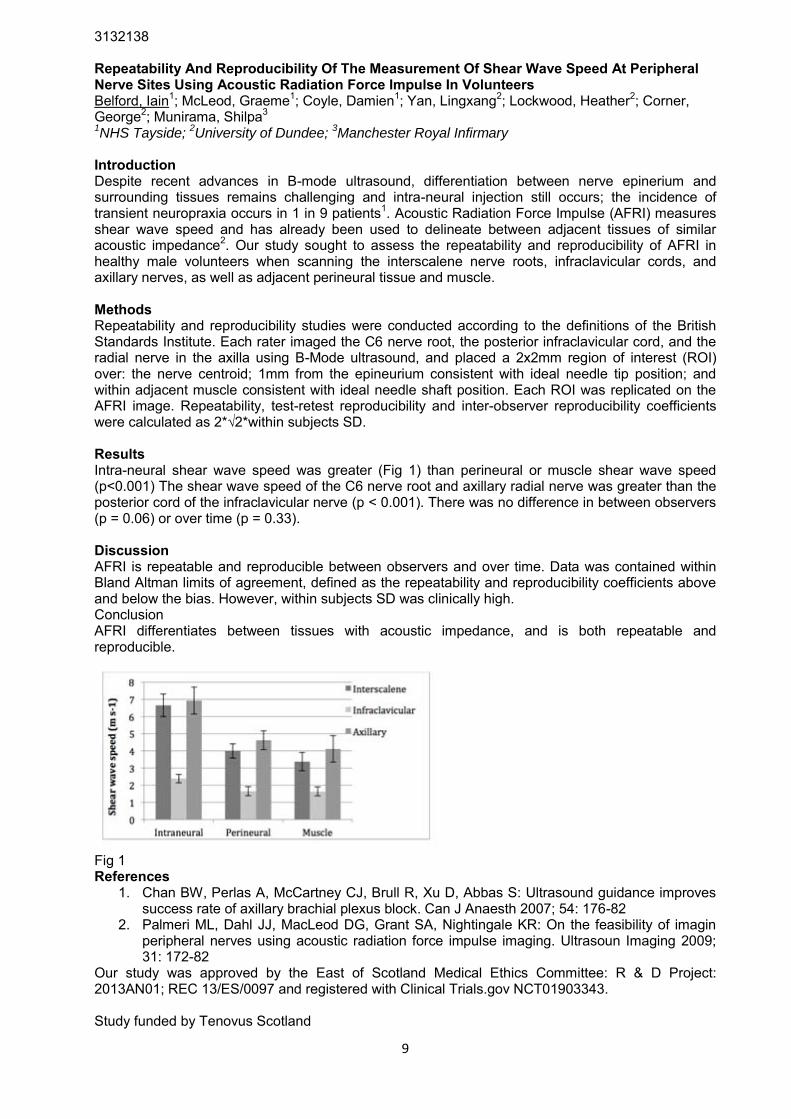
Introduction Despite recent advances in B-mode ultrasound, differentiation between nerve epinerium and surrounding tissues remains challenging and intra-neural injection still occurs; the incidence of transient neuropraxia occurs in 1 in 9 patients1. Acoustic Radiation Force Impulse (AFRI) measures shear wave speed and has already been used to delineate between adjacent tissues of similar acoustic impedance2. Our study sought to assess the repeatability and reproducibility of AFRI in healthy male volunteers when scanning the interscalene nerve roots, infraclavicular cords, and axillary nerves, as well as adjacent perineural tissue and muscle. Methods Repeatability and reproducibility studies were conducted according to the definitions of the British Standards Institute. Each rater imaged the C6 nerve root, the posterior infraclavicular cord, and the radial nerve in the axilla using B-Mode ultrasound, and placed a 2x2mm region of interest (ROI) over: the nerve centroid; 1mm from the epineurium consistent with ideal needle tip position; and within adjacent muscle consistent with ideal needle shaft position. Each ROI was replicated on the AFRI image. Repeatability, test-retest reproducibility and inter-observer reproducibility coefficients were calculated as 2*√2*within subjects SD. Results Intra-neural shear wave speed was greater (Fig 1) than perineural or muscle shear wave speed (p<0.001) The shear wave speed of the C6 nerve root and axillary radial nerve was greater than the posterior cord of the infraclavicular nerve (p < 0.001). There was no difference in between observers (p = 0.06) or over time (p = 0.33). Discussion AFRI is repeatable and reproducible between observers and over time. Data was contained within Bland Altman limits of agreement, defined as the repeatability and reproducibility coefficients above and below the bias. However, within subjects SD was clinically high. Conclusion AFRI differentiates between tissues with acoustic impedance, and is both repeatable and reproducible.
Fig 1 References
1. Chan BW, Perlas A, McCartney CJ, Brull R, Xu D, Abbas S: Ultrasound guidance improves success rate of axillary brachial plexus block. Can J Anaesth 2007; 54: 176-82
2. Palmeri ML, Dahl JJ, MacLeod DG, Grant SA, Nightingale KR: On the feasibility of imagin peripheral nerves using acoustic radiation force impulse imaging. Ultrasoun Imaging 2009; 31: 172-82
Our study was approved by the East of Scotland Medical Ethics Committee: R & D Project: 2013AN01; REC 13/ES/0097 and registered with Clinical Trials.gov NCT01903343. Study funded by Tenovus Scotland

10
3101213 Audit Of Patient Outcomes On Forefoot Surgery Blundell, Michael; Suri Mohanram, Kannan North Tyneside General Hospital Introduction Common forefoot procedures done for hallux vulgus deformity and bunionectomies all recieve regional anaesthesia as part of the anaesthetic and post operative pain management. Then patients may have the operation under GA, mild sedation or awake. The foot is supplied by five nerves (the tibial, superficial and deep peroneal, saphenous and sural nerves). These nerves are blocked either at the ankle, or with a popliteal sciatic +/- saphenous nerve block. Our common practice is to block tibial, superficial and deep peroneal nerves at the ankle. Post-operatively, patients are assessed in recovery, treated as necessary and then discharged from the day unit with take home analgesia. All patients are intended to be day case. This audit was done to look at our anaesthetic outcomes and patient experience for these procedures. Method This is a retrospective audit of 80 cases collected from our block room database. Our standards were from the RCoA audit recipe, aiming for 100% day of surgery discharge and 85% satisfaction with pain management. Results Our cohort consisted of 65 females and 15 males, with 40 patients ASA grade 1, 37 grade 2 and three grade 3. All cases had regional anaesthesia, with 70 ankle blocks and 10 popliteal blocks. 20 cases had a GA(volatile or TCI propofol), the rest were awake or mildly sedated. Post-operatively only 13 cases (16%) had symptoms of pain, 3 of nausea, and none vomited. Of those complaining of pain, 3 had mild (pain score 1-4), 9 had moderate (score 5-7) and one had severe pain (score 8-10). Of the 3 patients with nausea, two had volatile and one had propofol TCI. 76 patients were done as daycase (95%). Of the 4 inpatient cases, 3 were social admissions, 1 was for surgical reasons. We managed to contact 64 patients (80%) after discharge. Of these pateints, 58 (91%) had adequate pain relief, 61 (95%) described their experience as excellent,good or bearble, and 60 (94%) would have a block again and recommend it to a friend. Discussion Following the routine implemention of regional anaesthetic techniques we have achieved high success at maximising day discharge, analgesia, and patient satisfaction. Outcomes could be improved further by optimising block success, avoiding GAs and ensuring patients are discharged home with regular and rescue analgesia. We need to ensure block and analgesia information is given in verbal and written form throughout the patients hospital journey to improve understanding, compliance and experience. Conclusion Regional Anaesthesia is an integral aspect of care for forefoot procedures and contributes to successful daycase surgery, good patient experience and outcomes. References
1. RCoA Raising the standard:a compendium of audit recipes: page 160 and 164

11
3130979 Setting Up A Multidisciplinary Fascia Iliaca Block Delivery Service In A District General Hospital Carey, Ben; El-Hibri, Fouad; Wingate, Robin; Courtenay-Evans, Nick; Wilson, Helen; Berry, Matt; Foxall, Gillian Royal Surrey County Hospital Introduction Peripheral nerve blockade can be used to augment analgesia in patients with a fractured neck of femur (NOF), reducing opiate requirements in a vulnerable patient group (1,2). A local Fascia Iliaca Block (FIB) service was set up to be provided by Emergency Nurse Practitioners (ENPs) under supervision; or by ED doctors. This was audited to assess service delivery, after which interventions were made with anaesthetic & orthogeriatric input & re-audit was performed. Methods Audits occurred over 6 weeks during April-May 2014 & January-March 2015, with all NOF patients identified. Notes were retrospectively audited for demographics, admission date & time, speciality delivering FIB & any contraindications/complications noted. Patients were excluded if the fracture was not diagnosed in ED. Results
Apr/May 2014 Jan/Mar 2015
Sample Size 41 43
FIB Performed 13 31
Contraindications noted 5 6
FIB
performed/contraindicated 18(43.95%) 37(86.05%)
Average time to FIB 4h* 2h43
Performed by ED - 5; Anaesthetics - 4; Unknown - 2; No medical
notes - 2**
ED - 23; Anaesthetics - 6;
Unknown - 2
*average time was 7h48, one outlier excluded to reduce to 4h **No documentation in medical notes, but documented in nursing notes Both audits had 2 exclusions (1 missed diagnosis & 1 fall on ward for both). Original audit had 5 contraindications (2 refusal, 1 raised INR, 1 too agitated, 1 ‘not indicated’); re-audit had 6 (4 raised INR; 1 ‘too confused to consent’; 1 unable to find medication). No complications were noted. Discussion After service introduction, preliminary audit showed limited uptake & delayed FIB provision. The audit revealed no ENPs performed a FIB; either from a lack of appropriate supervision; or from conflicting time & resource pressures of working in ED. Additionally, it was felt that the number of doctors trained in FIBs was too limited to provide an effective service. After this, service delivery changes were made in December 2014 after liaison between ED, Anaesthetics & Orthogeriatrics including: further training of ED doctors & anaesthetists; raised FIB awareness; & bleep notification to the on-call anaesthetist of a fractured NOF. Re-audit performed after these interventions showed improved performance for both block provision & time to block administration. Documentation in both audits was not always complete, including pre- & post-FIB pain scores & observations post-FIB. As such, it was difficult to fully assess FIB efficacy as analgesia & the lack of observations could imply that monitoring post-FIB is not always occurring. Conclusion Setting up a multidisciplinary FIB service in a busy DGH has been a way of providing analgesia to patients presenting in ED with fractured NOF. The initial audit of the FIB service led to changes & considerable improvements in FIB provision, demonstrated by a re-audit. Further work will now focus on continuing FIB provision, safe delivery, improved documentation & potential use of catheters. References
1. The National Institute for Health and Clinical Excellence. Clinical Guideline 124. The management of hip fracture in adults. 2011. http://www.nice.org.uk/nicemedia/live/13489/54918/54918.pdf (accessed 16/3/15)
2. Foss NB,et al. Anesthesiology 2007;106:773-8
12
3124666 Visualising Needle Nerve Trauma Using High Frequency Ultrasound Chandra, Anu1; Munirama, Shilpa2; Hu, Q1; Felts, Paul1; Eisma, Roos1; Demore, Christine1; McLeod, Graeme3 1University of Dundee;
2Manchester Royal Infitrmary;
3Ninewells Hospital
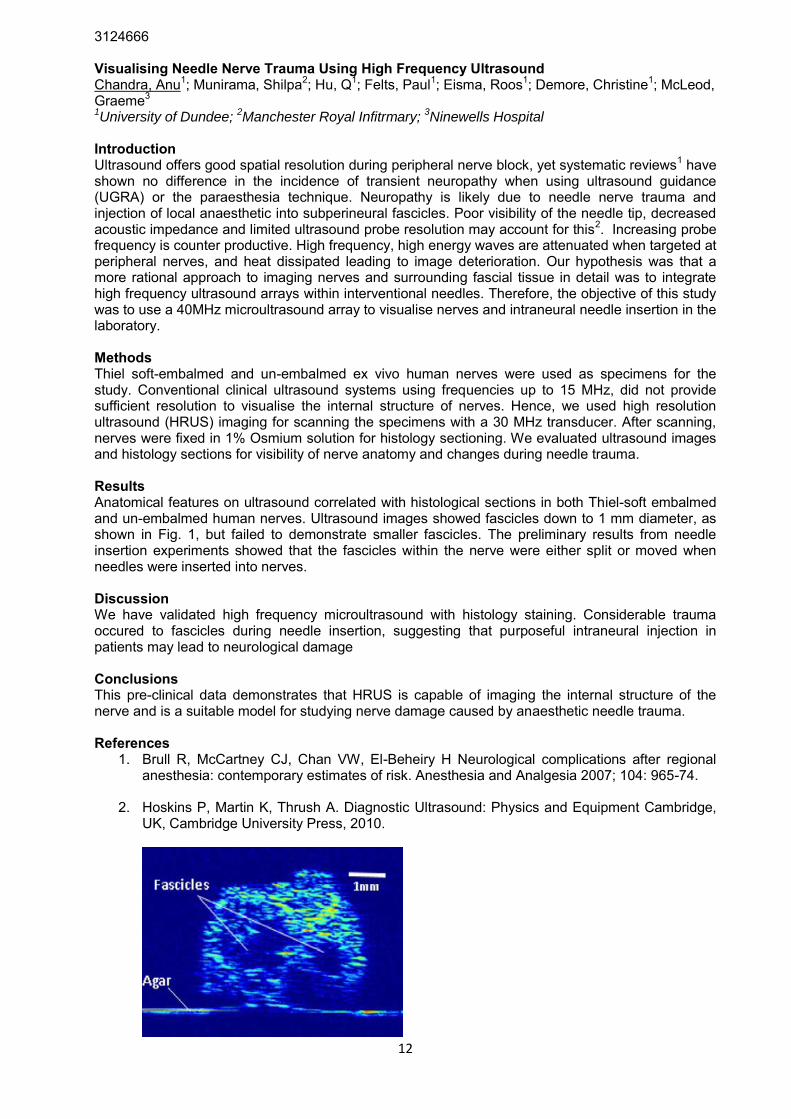
Introduction Ultrasound offers good spatial resolution during peripheral nerve block, yet systematic reviews1 have shown no difference in the incidence of transient neuropathy when using ultrasound guidance (UGRA) or the paraesthesia technique. Neuropathy is likely due to needle nerve trauma and injection of local anaesthetic into subperineural fascicles. Poor visibility of the needle tip, decreased acoustic impedance and limited ultrasound probe resolution may account for this2. Increasing probe frequency is counter productive. High frequency, high energy waves are attenuated when targeted at peripheral nerves, and heat dissipated leading to image deterioration. Our hypothesis was that a more rational approach to imaging nerves and surrounding fascial tissue in detail was to integrate high frequency ultrasound arrays within interventional needles. Therefore, the objective of this study was to use a 40MHz microultrasound array to visualise nerves and intraneural needle insertion in the laboratory. Methods Thiel soft-embalmed and un-embalmed ex vivo human nerves were used as specimens for the study. Conventional clinical ultrasound systems using frequencies up to 15 MHz, did not provide sufficient resolution to visualise the internal structure of nerves. Hence, we used high resolution ultrasound (HRUS) imaging for scanning the specimens with a 30 MHz transducer. After scanning, nerves were fixed in 1% Osmium solution for histology sectioning. We evaluated ultrasound images and histology sections for visibility of nerve anatomy and changes during needle trauma. Results Anatomical features on ultrasound correlated with histological sections in both Thiel-soft embalmed and un-embalmed human nerves. Ultrasound images showed fascicles down to 1 mm diameter, as shown in Fig. 1, but failed to demonstrate smaller fascicles. The preliminary results from needle insertion experiments showed that the fascicles within the nerve were either split or moved when needles were inserted into nerves. Discussion We have validated high frequency microultrasound with histology staining. Considerable trauma occured to fascicles during needle insertion, suggesting that purposeful intraneural injection in patients may lead to neurological damage Conclusions This pre-clinical data demonstrates that HRUS is capable of imaging the internal structure of the nerve and is a suitable model for studying nerve damage caused by anaesthetic needle trauma. References
1. Brull R, McCartney CJ, Chan VW, El-Beheiry H Neurological complications after regional anesthesia: contemporary estimates of risk. Anesthesia and Analgesia 2007; 104: 965-74.
2. Hoskins P, Martin K, Thrush A. Diagnostic Ultrasound: Physics and Equipment Cambridge, UK, Cambridge University Press, 2010.
13
3132581 Echogenic Regional Block Needles -- More Than Just Needle Brightness Cooper, Dawn1; Haslam, Nathaniel2 1Sheffield Hallam Univeristy;
2City Hospitals Sunderland NHS Foundation Trust
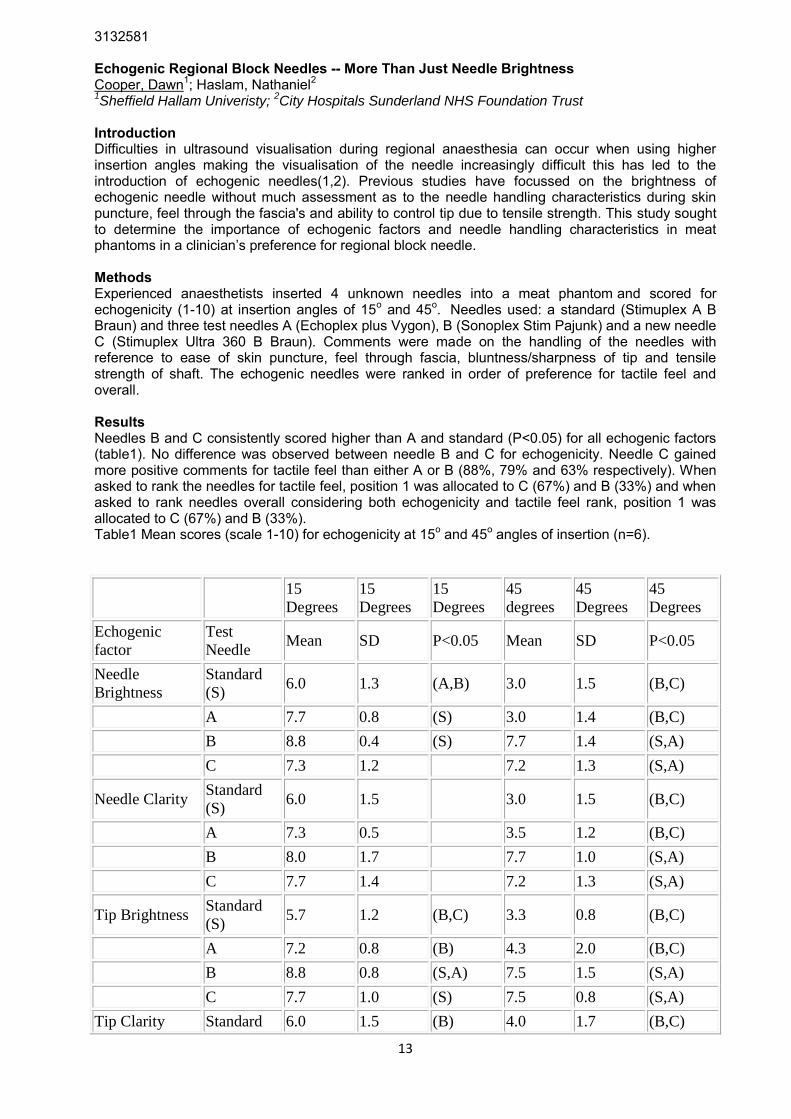
Introduction Difficulties in ultrasound visualisation during regional anaesthesia can occur when using higher insertion angles making the visualisation of the needle increasingly difficult this has led to the introduction of echogenic needles(1,2). Previous studies have focussed on the brightness of echogenic needle without much assessment as to the needle handling characteristics during skin puncture, feel through the fascia's and ability to control tip due to tensile strength. This study sought to determine the importance of echogenic factors and needle handling characteristics in meat phantoms in a clinician’s preference for regional block needle. Methods Experienced anaesthetists inserted 4 unknown needles into a meat phantom and scored for echogenicity (1-10) at insertion angles of 15o and 45o. Needles used: a standard (Stimuplex A B Braun) and three test needles A (Echoplex plus Vygon), B (Sonoplex Stim Pajunk) and a new needle C (Stimuplex Ultra 360 B Braun). Comments were made on the handling of the needles with reference to ease of skin puncture, feel through fascia, bluntness/sharpness of tip and tensile strength of shaft. The echogenic needles were ranked in order of preference for tactile feel and overall. Results Needles B and C consistently scored higher than A and standard (P<0.05) for all echogenic factors (table1). No difference was observed between needle B and C for echogenicity. Needle C gained more positive comments for tactile feel than either A or B (88%, 79% and 63% respectively). When asked to rank the needles for tactile feel, position 1 was allocated to C (67%) and B (33%) and when asked to rank needles overall considering both echogenicity and tactile feel rank, position 1 was allocated to C (67%) and B (33%). Table1 Mean scores (scale 1-10) for echogenicity at 15o and 45o angles of insertion (n=6).
15
Degrees
15
Degrees
15
Degrees
45
degrees
45
Degrees
45
Degrees
Echogenic
factor
Test
Needle Mean SD P<0.05 Mean SD P<0.05
Needle
Brightness
Standard
(S) 6.0 1.3 (A,B) 3.0 1.5 (B,C)
A 7.7 0.8 (S) 3.0 1.4 (B,C)
B 8.8 0.4 (S) 7.7 1.4 (S,A)
C 7.3 1.2
7.2 1.3 (S,A)
Needle Clarity Standard
(S) 6.0 1.5
3.0 1.5 (B,C)
A 7.3 0.5
3.5 1.2 (B,C)
B 8.0 1.7
7.7 1.0 (S,A)
C 7.7 1.4
7.2 1.3 (S,A)
Tip Brightness Standard
(S) 5.7 1.2 (B,C) 3.3 0.8 (B,C)
A 7.2 0.8 (B) 4.3 2.0 (B,C)
B 8.8 0.8 (S,A) 7.5 1.5 (S,A)
C 7.7 1.0 (S) 7.5 0.8 (S,A)
Tip Clarity Standard 6.0 1.5 (B) 4.0 1.7 (B,C)

14
(S)
A 7.0 0.0
4.3 2.0 (B,C)
B 8.5 0.8 (S) 7.5 1.5 (S,A)
C 7.5 0.8
7.2 1.2 (S,A)
Discussion Needles B and C were both significantly more echogenic than standard and A, no difference was observed between B and C. Needle C obtained more positive comments regarding the handling characteristics and ranked highest for tactile feel. In the overall rankings it was needle C which was rated in the top position most frequently. Conclusion This study demonstrates that tactile feel is important in choice of regional block needle. This small scale study requires repeating gaining quantitative data on tactile feel. Acknowledgements. Supplies for this study were provided by B Braun and Sonosite loaned ultrasound machinery. References
1. Chapman, G.A., D. Johnson, and A.R. Bodenham, Visualisation of needle position using ultrasonography. Anaesthesia, 2006. 61(2): p. 148-58.
2. Chin, K.J., et al., Needle visualization in ultrasound-guided regional anesthesia: challenges and solutions. Regional Anesthesia and Pain Medicine, 2008. 33(6): p. 532-44.
Conflicts of Interest D Cooper is also employed as a research analyst by B Braun Medical. None of the other authors have any conflicts to declare.

15
3132570 Starvation For Hand Surgery Under Brachial Plexus Block Czech, Alexander; Al-Sharher, Husham Guy's and St Thomas' Hospitals Introduction Many cases of hand surgery are performed with brachial plexus block as the sole anaesthetic technique. These patients are all routinely fasted, but frequently starved for much longer than the necessary 6 hours for food and 2 hours for water. This prolonged starvation may have significant psychological and physiological consequences on vulnerable patients. Aims Our aim was to explore anaesthetists’ ideas about preoperative fasting for patients undergoing surgery where brachial plexus bock alone is the planned anaesthetic technique. Methods We conducted an anonymous survey of 69 anaesthetists in a London teaching hospital. We enquired about experience in brachial plexus blocks and asked the question: “Do you believe patients should be fasted for hand surgery under brachial plexus block if we are not using sedation?” Results We collected data from 33 consultants and 36 trainees. The most common blocks performed were axillary brachial plexus blocks. Ultrasound was used by 97% of anaesthetists. Overall, 38% of anaesthetists feel patients do not need to be fasted prior to hand surgery under brachial plexus block (24% of consultants and 50% of trainees). In those with over 5yrs experience regional anaesthesia 31% disagreed with fasting patients. In those who performed over 100 brachial plexus blocks 40% disagreed. In those who do a regular list under brachial plexus block 40% disagreed. Of those who agreed with fasting, 49% had experience of converting a block to GA as opposed to 27% of those who disagreed. Discussion Whilst the majority are in favour of fasting patients for hand surgery under brachial plexus block, a significant proportion disagree. This opinion was independent of the level of experience in brachial plexus blockade or being a regular regional anaesthetist. However, more seniority, more years exposure to regional anaesthesia and previous experience converting a block to a GA made people much more likely to agree with the current system of fasting. Frequently cited reasons for starvation are that there should always be a contingency plan in case of inadequate block or patient preference and that there may be a need for intubation in case of emergency such as local anaesthetic toxicity. Conclusions This survey is about a balance of risk and opinion is quite clearly divided. It would be interesting to gauge the opinion of anaesthetists nationwide. Finally, whilst this is food for thought, we should also focus on preventing prolonged starvation beyond the current guidelines. References 1. AAGBI Safety Guideline: Pre-operative assessment and patient preparation - the role of the anaesthetist, January 2010. Association of Anaesthetists of Great Britain and Ireland.

16
3132239 Are Training Opportunities In Performing Thoracic Epidurals Limited? A Trainee's Perspective. Elliott, Sianedd; Lacasia, Carmen University Hospital Aintree Introduction Thoracic epidurals are seen as a core skill that trainees should be able to perform independently by the end of Higher training.1 With centralisation of surgical services and change in practice the opportunity to perform this skill is becoming increasingly limited.2 The Royal College of Anaesthetists estimates that 30 performances of a clinical skill are required to achieve 70-80% of the standard performance of an expert practitioner. Thoracic epidurals are seen as one of the most difficult technical skills for an anaesthetist to master. With decreasing training opportunities it is possible that registrars at the end of their training may have limited ability to perform this skill. A survey was conducted to explore trainee’s perspective on this potential problem. Methods A link to an online survey questionnaire was sent to all 68 higher level and advanced level trainees (ST5-7) in the Mersey Deanery. Respondents were asked to answer questions in relation to adult anaesthetic experience only. Results The response rate was 61% (42/68). Fifty one percent of respondents felt they were competent at performing thoracic epidurals independently. Of the remaining trainees, 21% felt they would be able to perform thoracic epidurals independently before completion of training, whilst 23% felt they would not reach this level. The more senior trainees had a greater confidence at performing thoracic epidurals. Seventy percent of ST7’s responded they were competent at this skill compared to 27% of ST5’s. Only three of the 42 trainees surveyed had performed greater than 20 thoracic epidurals during higher and advanced level training. Discussion The survey results are a cause for concern and identify a training issue. Over a quarter of trainees surveyed feel that they will lack the technical skills to perform a thoracic epidural unaided by the completion of their training. Whether this translates to clinical practice is uncertain but if it does it will have clinical implications. The number of thoracic epidurals performed per trainee is likely to be much lower than counterparts 10-20 years ago, which is a consequence of reduction in training hours as well as centralisation of services. The results of the survey have been disseminated to consultants and college tutors to maximise future learning potential. Conclusion Our survey suggests that current training leaves senior trainee’s feeling underprepared to perform thoracic epidurals independently. The question that may need to be asked in the future is whether the thoracic epidural continues to be a skill performed by all or should it be limited to those with high logbook numbers and regular experience. References
1. Royal College Of Anaesthetists.Curriculum for a CCT in Anaesthetics 2010. 2. Pennefather S, Gilby S, Danecki A, Russell, G. The changing practice of thoracic epidural
analgesia in the United Kingdom: 1997–2004. Anaesthesia 2006;4: 363-369.

17
3131135 Educational Regional Anaesthesia Block Videos: A Different Concept Jegendirabose, Parthipan; Ibrahim, Mark; Pawa, Amit Guys and St Thomas Hospital Introduction Benefits of regional anaesthesia include reduced postoperative pain, early mobilisation and shorter hospital stay (1)(2). The practice of peripheral nerve block requires a sound anatomical and sonoanatomical knowledge as well as the practical skills. Therein lies the challenge when teaching blocks to novice trainee. Visual aids have always been a valuable tool to employ for training (1). Our aim was to produce a free, easily accessible series of block videos with relevant anatomy, sonoanatomy and scanning tips to site the blocks. Method We made a series of short regional anaesthesia block videos to demonstrate relevant anatomy, sonoanatomy scanning tips and actual block. All material on the videos were originally produced and edited by the authors. These videos can be easily accessed via the LSORA Youtube channel. Furthermore, we presented our PECS II block video at our local clinical governance meeting. Attendees were surveyed to ascertain whether or not the video enhanced their understanding of anatomy and sonanatomy pertinent to the block. Results To date, we have published five short regional anaesthesia block videos and have had a total of 7000 views. We surveyed 28 attendees at our local clinical governance meeting, 68% consultants and 32% trainees. Eighty nine percent of the attendees had never performed this block. Our survey demonstrated a 65% and 43% improvement in identification of the anatomy and sonoanatomy respectively after watching the video for the first time. 96% of the attendees rated the educational content of the video to be above average and also 96% felt that they had gained anatomical knowledge. Discussion The limitations of the many teaching tools available such as cadaver workshops, three-dimensional videoclips, ultrasound guidance and acoustic assist devices are accessibility and cost (1). The use of video in medical education has been found to support and enhance learning and offer greater flexibility compared to traditional methods (3). Furthermore, research has shown that incorporating images into educational process increases learning retention (3). Conclusion The practice of regional anaesthesia is multi-faceted, and anatomical knowledge is crucial in reducing complications and improving the quality of the block. Our education block videos are a promising teaching tool for anatomy and sonoanatomy, and are beneficial to both the trainee as well as the trainer. Whilst the videos are not meant to replace the traditional hands-on approach to training, they serve to equip the viewer with the fundamental knowledge to execute the block safely. References
1. Broking K, Waurick R. How to teach regional anesthesia. Current Opinion in Anaesthesiol 2006; 19: 526–30
2. Adhikary S D, Hadzic A, and McQuillan P M. Simulator for teaching hand–eye coordination during ultrasound-guided regional anaesthesia British Journal of Anaesthesia. 2013 111: 844-845
3. Hurtubise L, Martin B, Gilliland A, Mahan J. To play or not to play: leveraging video in medical education. Journal of Graduate Medical Education. 2013 Mar;5(1):13-8

18
3132548 How Much Is Enough Information? Documentation Of Consent For Regional Anaesthesia In A District General Hospital's Theatres. Knowles, Tim1; Talwar, Vasundhara2; Ali, Leena2; Richards, Julia2 1Imperial College Healthcare NHS Trust;
2London North West Healthcare NHS Trust
Introduction Informed consent is a cornerstone of medical practice. The recent landmark Supreme Court decision sets a new standard for consent and patients are now the arbiters in deciding whether risks and alternatives have been adequately communicated (1). We audited the documentation of consent for elective neuraxial blockade. Methods We retrospectively audited anaesthetic charts for the period September-October 2014. Using a combination of existing publications from the Association of Anaesthetists of Great Britain and Ireland (AAGBI) and Royal College of Anaesthetists (RCOA) we created an audit standard for the documentation of consent process for neuraxial blocks. Results Our preliminary data indicates wide variation in individual practice concerning the documentation of risks, benefits and alternatives to regional anaesthesia within our unit. The percentage of operators documenting the specified “common side effects” (2) were as follows; headache 67%, hypotension 33%, urinary retention 17% and pain on injection 17%. The documentation rate for the listed “rare complication” (2) of nerve damage was better with 83% of operators documenting this risk as being discussed. A lower proportion (33%) documented the concept of permanent vs. partial nerve damage and a lower number still (17%) quoted a probability for nerve damage that was reflective of the incidence in the National Audit of Major Complications of Central Neuraxial Block (NAP3). Failure of the technique was quoted as being a risk by 50% of operators. We inferred this to be an indicator of alternatives being discussed, as documentation of risks of general anesthesia were invariably included. There was an apparent absence of written documentation of the proposed benefits of regional anaesthesia. Discussion There are several useful publications (3), providing guidance on the key principles of consent for regional anesthesia, but there is no agreed national standard to guide the specific consent process for neuraxial blocks. As the risks are similar for the majority of elective patients, we are in the process of developing a local protocol to standardise consent within our unit. This should serve as a guide to facilitate discussion with patients who may benefit from a regional technique and ensure adequate contemporaneous documentation of the conversation. Conclusion The update of UK law regarding consent gives a renewed cause to scrutinise and improve our approach to consent for anaesthesia. A National care bundle for regional anaesthesia was one of the recommendations of the NAP3 audit and incorporating a formalised consent process within this may prove helpful. References
1. Sokol DK. Update on the UK law on consent. BMJ. 2015 Mar 16;350:h1481. 2. Your spinal anaesthetic [Internet]. [cited 2015 Mar 26]. Available from:
http://www.rcoa.ac.uk/document-store/your-spinal-anaesthetic 3. Patient consent for peripheral nerve blocks [Internet]. [cited 2015 Mar 26]. Available from:
http://www.ra-uk.org/index.php/guidelines-standards/5-detail/255-patient-consent-for-peripheral-nerve-blocks
19
3131617 Anatomical Variation Of The Phrenic Nerve: An Anatomic And Ultrasonographic Study Lockwood, Heather1; Lamb, Claire1; McLeod, Graeme2 1University of Dundee;
2Ninewells Hospital
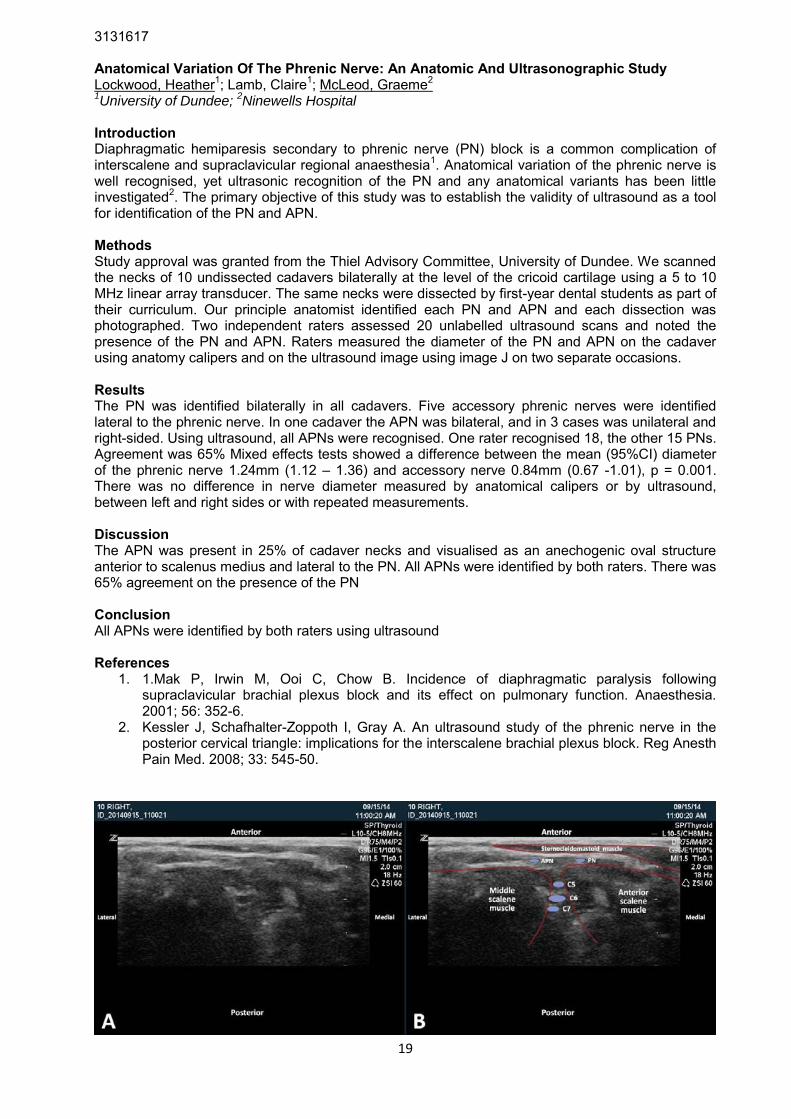
Introduction Diaphragmatic hemiparesis secondary to phrenic nerve (PN) block is a common complication of interscalene and supraclavicular regional anaesthesia1. Anatomical variation of the phrenic nerve is well recognised, yet ultrasonic recognition of the PN and any anatomical variants has been little investigated2. The primary objective of this study was to establish the validity of ultrasound as a tool for identification of the PN and APN. Methods Study approval was granted from the Thiel Advisory Committee, University of Dundee. We scanned the necks of 10 undissected cadavers bilaterally at the level of the cricoid cartilage using a 5 to 10 MHz linear array transducer. The same necks were dissected by first-year dental students as part of their curriculum. Our principle anatomist identified each PN and APN and each dissection was photographed. Two independent raters assessed 20 unlabelled ultrasound scans and noted the presence of the PN and APN. Raters measured the diameter of the PN and APN on the cadaver using anatomy calipers and on the ultrasound image using image J on two separate occasions. Results The PN was identified bilaterally in all cadavers. Five accessory phrenic nerves were identified lateral to the phrenic nerve. In one cadaver the APN was bilateral, and in 3 cases was unilateral and right-sided. Using ultrasound, all APNs were recognised. One rater recognised 18, the other 15 PNs. Agreement was 65% Mixed effects tests showed a difference between the mean (95%CI) diameter of the phrenic nerve 1.24mm (1.12 – 1.36) and accessory nerve 0.84mm (0.67 -1.01), p = 0.001. There was no difference in nerve diameter measured by anatomical calipers or by ultrasound, between left and right sides or with repeated measurements. Discussion The APN was present in 25% of cadaver necks and visualised as an anechogenic oval structure anterior to scalenus medius and lateral to the PN. All APNs were identified by both raters. There was 65% agreement on the presence of the PN Conclusion All APNs were identified by both raters using ultrasound References
1. 1.Mak P, Irwin M, Ooi C, Chow B. Incidence of diaphragmatic paralysis following supraclavicular brachial plexus block and its effect on pulmonary function. Anaesthesia. 2001; 56: 352-6.
2. Kessler J, Schafhalter-Zoppoth I, Gray A. An ultrasound study of the phrenic nerve in the posterior cervical triangle: implications for the interscalene brachial plexus block. Reg Anesth Pain Med. 2008; 33: 545-50.
20
3128316 Enhanced Needle Guidance In Regional Anaesthesia Through Ultrasonic Actuation Of A Standard Needle McLeod, Graeme1; Sadiq, Muhammad2 1Nine wells Hospital & University of Dundee School of Medicine;
2University of Dundee
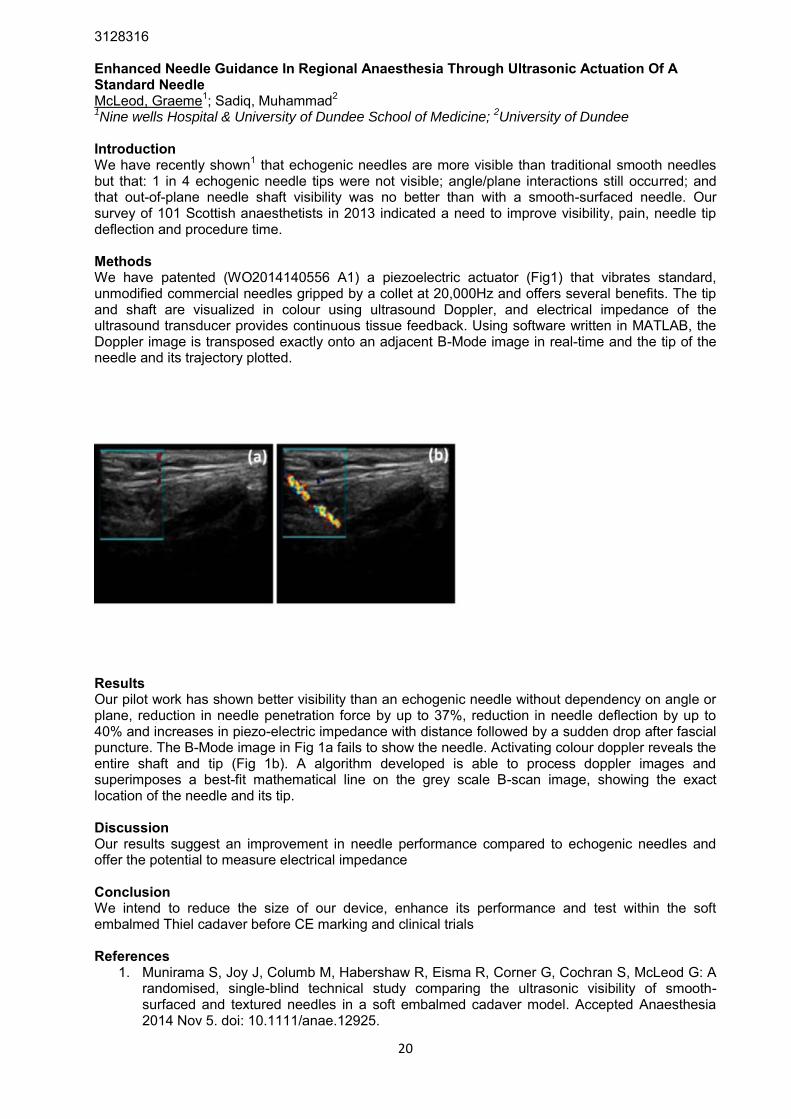
Introduction We have recently shown1 that echogenic needles are more visible than traditional smooth needles but that: 1 in 4 echogenic needle tips were not visible; angle/plane interactions still occurred; and that out-of-plane needle shaft visibility was no better than with a smooth-surfaced needle. Our survey of 101 Scottish anaesthetists in 2013 indicated a need to improve visibility, pain, needle tip deflection and procedure time. Methods We have patented (WO2014140556 A1) a piezoelectric actuator (Fig1) that vibrates standard, unmodified commercial needles gripped by a collet at 20,000Hz and offers several benefits. The tip and shaft are visualized in colour using ultrasound Doppler, and electrical impedance of the ultrasound transducer provides continuous tissue feedback. Using software written in MATLAB, the Doppler image is transposed exactly onto an adjacent B-Mode image in real-time and the tip of the needle and its trajectory plotted.
Results Our pilot work has shown better visibility than an echogenic needle without dependency on angle or plane, reduction in needle penetration force by up to 37%, reduction in needle deflection by up to 40% and increases in piezo-electric impedance with distance followed by a sudden drop after fascial puncture. The B-Mode image in Fig 1a fails to show the needle. Activating colour doppler reveals the entire shaft and tip (Fig 1b). A algorithm developed is able to process doppler images and superimposes a best-fit mathematical line on the grey scale B-scan image, showing the exact location of the needle and its tip. Discussion Our results suggest an improvement in needle performance compared to echogenic needles and offer the potential to measure electrical impedance Conclusion We intend to reduce the size of our device, enhance its performance and test within the soft embalmed Thiel cadaver before CE marking and clinical trials References
1. Munirama S, Joy J, Columb M, Habershaw R, Eisma R, Corner G, Cochran S, McLeod G: A randomised, single-blind technical study comparing the ultrasonic visibility of smooth-surfaced and textured needles in a soft embalmed cadaver model. Accepted Anaesthesia 2014 Nov 5. doi: 10.1111/anae.12925.
21
3132775 A Comparison Of The Shamrock Lumbar Plexus Block With The Posterior TAP And Quadratus Lumborum II Block - Spread Of Injectate In The Soft Embalmed Thiel Cadaver Carline, Lydia1; Lamb, Claire1; McLeod, Graeme2 1University of Dundee;
2Ninewells Hospital
Introduction Several posterior abdominal wall blocks have been proposed in order to provide thoracolumbar anaesthesia. The posterior Transversus Abdominal Plane (TAP) block1, described as an injection of local anaesthetic injected through the angle of Petit, the quadratus lumborum I and II blocks2 and the Shamrock3 lumbar plexus block have all been described. Spread to nerve roots has been proposed as a mechanism of action. However, no study has been undertaken in order to compare the spread of these blocks in cadavers. Therefore our objective was to evaluate the spread of dye when administered as a 20ml volume when conducting a posterior TAP block, Quadratus lumborum II block and Shamrock block in the soft embalmed Thiel cadaver. Methods This study was conducted in the Centre for Anatomy and Human Identification (CAHiD, Universioty of Dundee Thiel cadavers retain life-like flexibility, with realistic tissue planes, and are suitable for long-term use. We conducted 10 ultrasound guided nerve blocks (UGRA) on the left and right sides of 5 soft embalmed Thiel cadavers. In all we administered 4 Shamrock blocks, 3 posterior TAP blocks and 3 Quadratus lumborum II blocks. A 20ml mixture of diluted latex and ink was injected, then the lumbar region dissected 48 hours later in order to observe spread along tissue planes and into nerve roots. Results We successfully performed UGRA and obtained images of muscle, bowel, bone and lumbar nerve plexus as well as clear dynamic flow of fluid during injection. All posterior TAP blocks and quadratus II blocks were associated with superficial spread of dye within the TAP plane. All shamrock blocks spread consistently to the L1 and L3 nerve roots. Discussion We have shown that Shamrock blocks but not posterior TAP blocks or Quadratus Lumborum II blocks are associated with nerve root spread. Conclusion Our pilot data suggest there is a need for a comprehensive anatomical and clinical comparison of these nerve blocks. References
1. Carney J, Finnerty O, Rauf J, Bergin D, Laffey JG, Mc Donnell JG. Studies on the spread of local anaesthetic solution in transversus abdominis plane blocks. Anaesthesia 2011; 66: 1023-30
2. BlancoR, McDonnellJG Optimal point of injection: The quadratus lumborum type I and II blocks Br J Anaesth 2013; 68 (correspondence) 3. Sauter AR, Ullensvang K, Bendtsen TF, Borglum J. The ‘Shamrock Method’ a new and promising technique for ultrasound-guided lumbar plexus block. Br J Anaesth 2013 e-letter (http://www.bja.oxfordjournals.org/forum/topic/brjana_el%3B9814)
22
3124682 A Systematic Review And Meta-analysis Of Ultrasound Versus Electrical Stimulation For Peripheral Nerve Location And Blockade Munirama, Shilpa1; McLeod, Graeme2 1Manchester Royal Infirmary;
2Ninewells Hospital
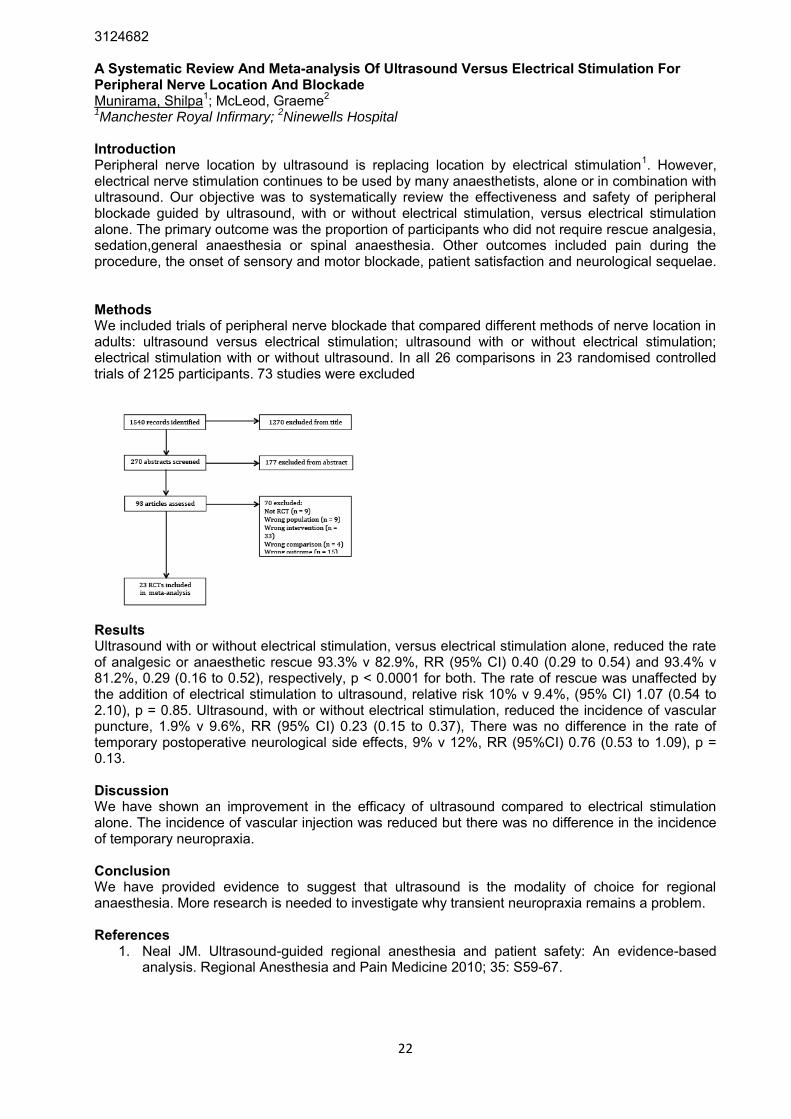
Introduction Peripheral nerve location by ultrasound is replacing location by electrical stimulation1. However, electrical nerve stimulation continues to be used by many anaesthetists, alone or in combination with ultrasound. Our objective was to systematically review the effectiveness and safety of peripheral blockade guided by ultrasound, with or without electrical stimulation, versus electrical stimulation alone. The primary outcome was the proportion of participants who did not require rescue analgesia, sedation,general anaesthesia or spinal anaesthesia. Other outcomes included pain during the procedure, the onset of sensory and motor blockade, patient satisfaction and neurological sequelae. Methods We included trials of peripheral nerve blockade that compared different methods of nerve location in adults: ultrasound versus electrical stimulation; ultrasound with or without electrical stimulation; electrical stimulation with or without ultrasound. In all 26 comparisons in 23 randomised controlled trials of 2125 participants. 73 studies were excluded
Results Ultrasound with or without electrical stimulation, versus electrical stimulation alone, reduced the rate of analgesic or anaesthetic rescue 93.3% v 82.9%, RR (95% CI) 0.40 (0.29 to 0.54) and 93.4% v 81.2%, 0.29 (0.16 to 0.52), respectively, p < 0.0001 for both. The rate of rescue was unaffected by the addition of electrical stimulation to ultrasound, relative risk 10% v 9.4%, (95% CI) 1.07 (0.54 to 2.10), p = 0.85. Ultrasound, with or without electrical stimulation, reduced the incidence of vascular puncture, 1.9% v 9.6%, RR (95% CI) 0.23 (0.15 to 0.37), There was no difference in the rate of temporary postoperative neurological side effects, 9% v 12%, RR (95%CI) 0.76 (0.53 to 1.09), p = 0.13. Discussion We have shown an improvement in the efficacy of ultrasound compared to electrical stimulation alone. The incidence of vascular injection was reduced but there was no difference in the incidence of temporary neuropraxia. Conclusion We have provided evidence to suggest that ultrasound is the modality of choice for regional anaesthesia. More research is needed to investigate why transient neuropraxia remains a problem. References
1. Neal JM. Ultrasound-guided regional anesthesia and patient safety: An evidence-based analysis. Regional Anesthesia and Pain Medicine 2010; 35: S59-67.

23
3127514 BLOC MANIAC - A Novel Aide-Memoir For Regional Anaesthesia Documentation Murphy, Stephen; Chandra, Manik Leeds Teaching Hospitals Trust Introduction Peripheral nerve block documentation is highly variable. Currently no standard exists concerning what information should be documented on the anaesthesia record in the patient notes. Serious complications as a result of peripheral nerve blocks are thankfully rare, but with the expansion of ultrasound guided regional anaesthesia in recent years and increasing medical litigation, the requirement for thorough documentation has never been clearer. A previous casenote analysis conducted by ourselves in a different institution demonstrated this high degree of variability and, in many cases, a lack of information that we felt should be essential for the documentation of most blocks.1 We sought to create a brief, transferrable and memorable mnemonic to help remember the key points to note regarding each block procedure on the anaesthesia record. Methods As part of a previous project1, we had consulted a local medicolegal representative and several Consultant Anaesthetists with an interest in Regional Anaesthesia regarding what information should be documented for each nerve block. We used these discussions to formulate a list that was thorough and robust yet maintaining practicality and brevity. In order to create a clinically practical and usable tool we developed this list into a mnemonic. Results The mnemonic created is BLOC MANIAC: B:Block - name of block L:Laterality or level - side (left/right), level of central neuraxial block O:Operator - name of person performing the block C:Consciousness - awake/anaesthetised/sedated/regional M:Method - US Guided (including needle plane technique), Nerve Stimulation or landmark A:Asepsis - precautions taken N:Needle - type/gauge/length of needle used I:Injectate - anaesthetic mix used (including additives) A:Asymptomatic/appearances - absence of symptoms on injection, ease of injection,post injection ultrasound appearances C:Comments/complications - quality of block, other Discussion We believe that BLOC MANIAC is an effective aide memoir for peripheral nerve block documentation that is memorable, easy to apply and improves current standards of documentation. It may be of particular benefit to trainees or less frequent practitioners in regional anaesthesia in maintaining a robust and consistent quality of block recording. This mnemonic can also be applied effectively to the documentation of central neuraxial blocks. References
1. Murphy S., Chandra M., Wilson-Baig N. Design and implementation of a sticker to improve documentation of peripheral nerve blocks - a Quality Improvement Project [Abstract]. Regional Anaesthesia and Pain Medicine. Sep-Oct 2014; 39(5) Suppl 1. pE255

24
3129953 How Low Can We Go? The Accuracy Of B-Mode Ultrasound And Strain Elastography In The Recognition Of Femoral And Interscalene Test Doses In The Soft Embalmed Thiel Cadaver Model Mustafa, Ayman1; Seeley, Jonathan1; Eisma, Roos2; McLeod, Graeme3; Corner, George2; Munirama, Shilpa4 1Ninewells Hospital;
2University of Dundee;
3Ninewells Hospital & University of Dundee;
4Manchester
Royal Infirmary Introduction Hydrolocation is a recognised means of detecting needle tip position during ultrasound guided regional anaesthesia. Hydrolocation volumes vary between 0.5ml and 1ml in order to minimize neural damage in the event of accidental subperineural injection. However, 1 in 6 intraneural injections may be missed1 2, and a need arises to accurately recognize small volume test doses. Therefore the objective of our study was to assess the accuracy of fusion elastography compared to B-Mode ultrasound as rated post-procedure by anaesthetic trainees when injecting 0.25ml, 0.5ml and 1ml test doses during interscalene and femoral nerve blocks in the soft embalmed Thiel cadaver. Methods An expert regional anaesthetist conducted 60 ultrasound guided femoral and interscalene nerve blocks. Two raters independently measured the cross-sectional area and brightness of nerves and fluid spread using during B-Mode ultrasound and fusion elastography using ImageJ. We also conducted a mixed regression analysis of area and brightness using cadaver, injection side, injection sequence, type of block volume and imaging (nerve, hydrolocation, and fusion elastogram) as covariates. Trainees assessed both images for perineural, intraneural and inadvertent spread and number of hydrolocation areas and we compared their results to experts. We used a MRMC - ROC mixed effects regression model for analysis Results We recorded 58 blocks. In all fusion images we visualised a white strain pattern. Term-by-term hypothesis test showed that fusion elastograms were larger and brighter than hydrolocation test doses and nerves on B-Mode ultrasound. Nerve block (p = 0.72), sequence (p = 0.15), cadaver (p = 0.63), or side of injection (p = 0.48) had no effect on area, brightness or their product. The product of area and brightness on the fusion elastograms was 15 times greater than B-Mode hydrolocation (Fig 1) using 0.5ml volumes. Discussion Fusion elastography detects test doses better than B-Mode ultrasound, independently of cadaver, injection side, injection sequence, or type of block. Conclusion Small volume fusion elastography is 15 times more sensitive than B-Mode ultrasound References
1. Liu SS, YaDeau JT, Shaw PM, Wilfred S, Shetty T, Gordon M: Incidence of unintentional intraneural injection and postoperative neurological complications with ultrasound-guided interscalene and supraclavicular nerve blocks. Anaesthesia 2011; 66: 168-74
2. Hara K, Sakura S, Yokokawa N, Tadenuma S: Incidence and effects of unintentional intraneural injection during ultrasound-guided subgluteal sciatic nerve block. Reg Anesth Pain Med 2012; 37: 289-93

25
3132178 Ultrasound Guided Posterior Capsular Infiltration Of Local Anaesthetic As Part Of An Enhanced Recovery Programme For Total Knee Arthroplasty. Nalawade, Vaishali; Skalska-Lis, Barbara; Haslam, Nathaniel Sunderland Royal Hospital Introduction The optimal technique for total knee arthroplasty (TKA) should support early mobilisation by combining good pain relief whilst minimising side effects such as nausea, drowsiness and muscle weakness.1 When compared to popliteal sciatic block, posterior capsular infiltration (PCI) blocks only the terminal branches innervating the posterior knee joint, and may be superior in terms of post-operative ambulation.2 The aim of our audit was to ensure that we are providing good analgesia, early mobilisation and a short length of hospital stay (LOHS) by including ultrasound guided PCI as part of our TKA enhanced recovery programme (ERP). Methods: The audit was approved by the hospital audit committee. The Sunderland ERP for TKA includes spinal anaesthesia (0.5% levobupivacaine) in conjunction with ultrasound guided femoral nerve block and PCI (0.25% levobupivacaine 20 mls each site). We prospectively collected data using a standard proforma for patients undergoing TKA during the period 08/14 – 01/15. Outcome measures were: maximum and minimum pain scores (day 0-2), LOHS, opioid consumption and time to independent mobilisation. Patients were asked to rate pain assessment at discharge on a scale of 1 (excellent) to 4 (very unsatisfactory). Data were compared with a previous audit where popliteal sciatic blocks, rather than PCI were performed. Results The following table demonstrates the mean pain scores, morphine dose and LOHS.
Femoral block + Popliteal
sciatic block
Femoral block + Posterior capsular
infiltration (PCI)
Number of Patients 30 42
Day 0 Mean Pain Score:
Lowest 0.4 0.0
Day 0 Mean Pain Score:
Highest 3.4 5.7
Day 1 Mean Pain Score:
Lowest 0.4 0.4
Day 1 Mean Pain Score:
Highest 3.5 5.8
Day 2 Mean Pain Score:
Lowest 0.1 0.5
Day 2 Mean Pain Score:
Highest 2.9 5.0
Mean Morphine Dose
(mg) 25.1 (PCA)
6.7 Oromorph (PRN) + Morphine
Sulphate BD
Mean LOHS (days)
[median] 4.06 [4] 3.59 [2]
Mean time for independently mobilisation was day one. Mean and median pain assessment scores at discharge were 1.4 and 1 respectively. Discussion Pre-operative PCI under ultrasound guidance has significant, theoretical advantages over blind surgical infiltration. It allows correct identification of the required local anaesthetic plane, avoids vascular structures and allows adjustment of needle position to avoid local anaesthetic spread around major nerves (and hence the motor block).
26
Conclusion: The above data suggest that, in conjunction with a femoral nerve block, PCI provides good post-operative analgesia, allows early mobilisation and facilitates an early discharge from hospital (median day 2). There was a clinically significant reduction in LOHS compared to previous patients who had received a popliteal sciatic block (median discharge day 4). References
1. Fischer HBJ, Simanski CJP, Sharp C et al. A procedure-specific systematic review and consensus recommendations for postoperative analgesia following total knee arthroplasty. Anaesthesia 2008;63: 1105-1123.
2. Gi E, Yamauchi M, Yamakage M, et al. Effects of local infiltration analgesia for posterior knee pain after total knee arthroplasty: comparison with sciatic nerve block. J Anesth. 2014 Feb 16

27
3131952 Dose, Volume, Timing And Toxicity Of Local Anaesthetics In Upper Limb Surgery: Data From A Local Audit Namih, Miriam; Robertson, Fiona; Chavan, Shivanand University Hospital Birmingham Introduction Local anaesthetic systemic toxicity carries significant morbidity and mortality. Traditionally, dosing is calculated according to patient weight. Site of anaesthetic injection, volume of drug and timescale of infiltration can also affect systemic absorption of the anaesthetic.1 We audited our local anaesthetic doses in regional blockade (axillary and forearm) to establish whether we dose patients appropriately according to weight. Methods Data collection was prospective random sampling for a period of one month in a regional hand centre. The operator of the regional block completed the data collection form immediately after the block. The information was cross-referenced with electronic patient records. Data included patient age, weight, block site, start and end times of regional block, volume and type of local anaesthetic used, any additional block (‘top-up’) required and presence of any patient symptoms (self reported). Results Data was collected for 50 patients. The age range was 16-87 years (median 35yr) with a weight range of 50-117kg (median 80kg). The primary block site was axillary in 47 patients and forearm in 3 patients. All patients received a mixture of 2% lignocaine with 1 in 200,000 adrenaline and 0.75% ropivacaine. No adverse effects were recorded. Of the axillary blocks: the range of procedure duration was 4-25 minutes (median 10mins). Local anaesthetic volume ranged between 20-34mls (median 28ml). 31% and 19% of patients had more than the recommended mg/kg dose of 2% lignocaine and 0.75% ropivacaine infiltrated respectively, which equated to approximately 6mls of volume. Five patients (10.6%) required an additional nerve block causing total dose to exceed the recommended dose in these patients. This ‘top up’ occurred 35-55mins (median 45min) after the start of the axillary block. Discussion Despite an increased dose in mg/kg of local anaesthetic in almost a third of patients, no significant systemic effects were noted. This may have been due to the adrenaline present in the local anaesthetic mix used, extra care with needle placement or injection technique. Conclusions Data on appropriate local anaesthetic dosing for weight is extrapolated from animal and pharmacological studies.2 However many factors can affect the pharmacokinetic and pharmacodynamics properties of local anaesthetics, including patient age and comorbidities, site of injection and use of additional drugs.1 This small dataset has shown that a larger dose of local anaesthetic has been administered without significant systemic toxicity. References
1. Neal J, Bernards C et al., ASRA Practice Advisory on Local Anesthetic Systemic Toxicity. Regional Anaesthesia and Pain Medicine 2010; 35(2):152-61
2. Mather L, Copeland S et al., Acute toxicity of Local Anaesthetics: Underlying Pharmacokinetic and Pharmacodynamic Concepts Regional Anaesthesia and Pain medicine 2005; 30(6): 553-566

28
3127532 The Impact Of Anaesthetic Management On Postoperative Outcomes In Unicompartmental Knee Arthroplasty Parker, Jacqui1; Crowley, Mark2; Kang, Sujin3; Marfin, Alex2; Price, Andrew2 1John Radcliffe Hospital,;
2Nuffield Orthopaedic Centre, Oxford;
3Nuffield Department of
Orthopaedics, Rheumatology and Musculoskeletal Sciences Introduction The Oxford enhanced recovery pathway (OERP) for anaesthetic/perioperative management of joint arthroplasties has been introduced into our institution. We aimed to evaluate postoperative outcomes for patients managed according to the OERP for unicompartmental knee arthroplasty (UKA) and to benchmark these outcomes against a pre-existing accepted practice. Methods We conducted a retrospective study of medical records of patients undergoing UKA from May 2012-April 2014 under 2 specified teams. Group 1 (G1) were managed according to the OERP with plain spinal anaesthesia (SA) and pre-emptive analgesia (gabapentin/diclofenac). Group 2 (G2) underwent general anaesthesia (GA) and single shot femoral nerve block (FNB) either with 20mls 0.375% bupivacaine (Bu) or 20mls 1% prilocaine (Pr). All patients received paracetamol and ropivacaine periarticular infiltration. Inclusion/exclusion criteria were applied. Our primary outcome was length of hospital stay (LOS). Secondary outcomes were 4hr & 24hr pain scores (PS) and 48hr opioid consumption (OC). Multivariate logistic regression analysis or analysis of covariance (ANCOVA) models were performed as appropriate. Results 89 patients were included, 37 in G1 and 52 in G2 (23 Bu, 29 Pr). Two patients were excluded due to chronic opioid use. LOS results are shown in Figure 1. In the multivariate ANCOVA model, group was not a significant factor for LOS (P=0.23). However, on further analysis of FNB type, the mean LOS was significantly shorter for G1 than G2Bu (P=0.04), but there was no significant difference between G1 and G2Pr (P=0.81). Group was not a significant factor for 4hr PS (P=0.38) but 24hr PS were significantly higher in G1 compared with G2 (P<0.001) and also when compared to each sub group (G2Bu P= 0.002, G2Pr P<0.001). Mean OC in G1 was very significantly higher than G2 (146.9mg v 58.1mg P<0.001) and also when compared to each subgroup (G2Bu P<0.001, G2Pr P<0.001).
Discussion

29
Results suggest that in our institution, the introduction of SA into the OERP does not shorten LOS for UKA when compared to pre-existing practice of GA/FNB. SA was also associated with a significantly inferior analgesic profile, indicated by higher 24 hour PS/OC. It is evident, however, that the use of bupivacaine FNB may prolong LOS by up to 18 hrs, when compared to SA, which is likely to represent an extra overnight stay. No such disadvantages were demonstrated for the use of prilocaine FNB, and this group maintained the superior analgesic profile associated with use of FNB.1,2
Conclusion The combination of GA and short acting FNB may be a superior technique to spinal anaesthesia for enhanced recovery pathways for UKA. References
1. Sahin L, Korkmaz HF, Sahin M et al. Ultrasound-guided single femoral nerve block provides effective analgesia after total knee arthroplasty up to 48 hours. Agri Dergisi 2014; 26/3: 113-8
2. McNamee DA, Convery PN, Milligan KR. Total knee replacement: a comparison of ropivacaine and bupivacaine in combined femoral and sciatic block. Acta Anaesthesiologica Scandinavica 2001; 45/4: 477-81

30
3128081 Comparison Of Bupivacaine Versus Prilocaine For Femoral Nerve Block On Postoperative Outcomes For Unicompartmental Knee Arthroplasty Parker, Jacqui1; Crowley, Mark2; Kang, Sujin3; Marfin, Alex2; Price, Andrew2 1John Radcliffe Hospital,;
2Nuffield Orthopaedic Centre, Oxford;
3Nuffield Department of
Orthopaedics, Rheumatology and Musculoskeletal Sciences Introduction The use of femoral nerve block (FNB) for knee arthroplasty raises concerns over delayed functional recovery and longer hospital stay. Shorter duration local anaesthetics (LA) may therefore be desirable although a shorter analgesic effect may itself be detrimental to recovery. We aimed to compare the effect of bupivacaine versus prilocaine for FNB on postoperative outcomes for patients undergoing unicompartmental knee arthroplasty (UKA). Methods We conducted a retrospective study of medical records of patients undergoing UKA by a specific team from May 2012-April 2014. All patients underwent general anaesthesia, with fentanyl/propofol induction and isoflurane maintenance, and received a single shot FNB with either 20mls 0.375% bupivacaine (Group 1) or 20mls 1% prilocaine (Group 2). All patients received ropivacaine periarticular infiltration and paracetamol/ dexamethasone. Inclusion/exclusion criteria were applied. Our primary outcome was length of hospital stay (LOS). Secondary outcomes were 4hr & 24hr pain scores (PS) and 48hr opioid consumption (OC). Multivariate logistic regression analysis or analysis of covariance (ANCOVA) models were performed, as appropriate. Results 52 patients were included, 23 in Group 1 and 29 in Group 2. One patient was excluded due to chronic opioid use. LOS results are shown in Figure 1. After age, gender, ASA and Group were fitted in the multivariate ANCOVA model, mean LOS in Group 1 was longer than in Group 2 but the difference did not reach statistical significance (P=0.09). For secondary outcomes, group was not a significant factor for 4hr PS (P=0.95), 24hr PS (P=0.36) or mean OC (57.3mg Group 1 vs 67.4mg Group 2, P=0.41).
Discussion Although the difference in LOS between the two groups did not quite reach statistical significance (P=0.09), the results do imply clinical significance. The use of prilocaine FNB may shorten LOS by

31
up to 17 hours when compared to bupivacaine, which may represent one less overnight stay and thus significantly reduce financial costs. The absence of any significant difference in analgesic outcomes between the two groups (PS/OC) suggests that the benefits of prilocaine are not associated, or outweighed, by an inferior analgesic profile. Evidence is surprisingly sparse for comparing the use of different types of LAs for peripheral nerve blocks and higher power studies are needed.1,2
Conclusion The preferred choice of local anaesthetic for peripheral nerve blocks is highly variable and depends on the type of surgery and predicted postoperative course. However, for UKA, prilocaine may be desirable for minimising hospital stay yet still providing adequate postoperative analgesia. References
1. Saritas A, Sabuncu C. Comparison of clinical effects of prilocaine, dexamethasone added to prilocaine and levobupivacaine on brachial plexus block. Journal of the Pakistan Medical Association. 2014: 64/4; 433-6.
2. Theodosiadis P, Sachinis N, Goroszeniuk T et al. Ropivacaine versus bupivacaine for 3-in-1 block during total knee arthroplasty. Journal of Orthopaedic Surgery. 2013: 21/3; 300-4.

32
3132736 Performing Regional Blocks For Limb Surgery Before Or After General Anaesthesia: A Follow-up Survey Of Anaesthetists' Beliefs And Practice In The Oxford Region Pepper, Warwick; Parker, Jacqui; Galitzine, Svetlana; Popat, Mansukh Oxford University Hospitals Introduction Regional anaesthetic techniques are used frequently in combination with general anaesthesia. Debate remains whether there is a safety advantage in performing blocks in an awake patient versus after induction of general anaesthesia (GA). We surveyed anaesthetists within our region to determine their beliefs and clinical practice on this topic as a follow-up to a previous survey from 2008. Method We conducted an on-line survey of 373 anaesthetists in our region to assess beliefs and clinical practice regarding the timing of regional anaesthesia in adult patients undergoing limb surgery, when combined with GA. We compared the results to our previous survey from 2008. Results Of the 153 respondents (41% response rate), 81 (53%) performed regional blocks regularly (at least 1/week). Over 75% of anaesthetists believed that it was safer to perform central neuraxial blocks (CNB) prior to the induction of GA, while around 25% had no preference. Proximal upper limb blocks were believed to be safer in awake patients in excess of 55% of respondents, equivocal in 40% and safer if performed asleep in less than 5%. Clinical practice mirrored this belief with around 60% of proximal upper limb blocks being performed awake. Lower limb blocks were believed to be safer in awake patients in around 22% of respondents, equivocal in 63%, and safer if performed asleep in 15%. Clinical practice mirrored the beliefs with 80% of lower limb blocks being performed asleep. Discussion Central neuraxial blocks were believed to be safer if performed awake in 75%, marking a modest relaxation that awake performance is safer from 2008 (82%). In practice though, over 85% of respondents perform CNBs before GA, which mirrors findings from 2008 (83%). Proximal upper limb blocks were believed to be safer when performed awake by the majority of respondents while lower limb blocks were perceived to have equivocal safety when awake or asleep, and were performed under general anaesthesia predominantly. This trend is consistent with findings from 2008 with a modest percentage increase in both the belief that all peripheral nerve blocks are safer if performed awake and in actual clinical practice. Whether this represents an increasing awareness of block complications combined with increased technical skills and confidence in performing blocks on awake patients, remains to be established. Conclusion Beliefs and practices in our region of regional block timing have changed marginally since 2008. There has been an increasing trend of perceived safety in performance on awake patients and this has translated into a moderate increase in blocks being performed prior to general anaesthesia. References
1. N. M. Feeley, M. T. Popat, S. V. Rutter. Regional Anaesthesia for Limb Surgery: A Review of Anaesthetists' Beliefs and Practice in the Oxford Region. Anaesthesia 2008; 63: 621-625

33
3132284 Awake Hand Surgery - A Patient Satisfaction Survey Pothireddy, Rama; Holgate, Carol; Moll, Timothy Sheffield Teaching Hospitals NHS Foundation Trust Introduction As a tertiary referral centre we have a dedicated hand unit with two hand surgery theatres operating five days a week. The majority of the operations are day surgery procedures performed under regional anaesthesia. With a view to improve anaesthetic care, we designed a survey1,2 to gauge how satisfied are our patients with their experience of awake hand surgery and post-operative analgesia. Methods The survey was approved by the Trust's clinical effectiveness unit. Patients were recruited on the day of their surgery, informed consent was obtained and were given a choice between email or telephone survey. Recruited patients were contacted a week after their surgery. The questions aimed to establish their satisfaction with the pre-operative information they had received about regional anaesthesia, the severity of pain or discomfort while performing the block and during the operation, satisfaction with the overall care they received from their anaesthetist and quality of post-operative analgesia. We also included "friends and family test" in the survey. Results: 60 patients who had elective hand surgery using regional anaesthesia participated in the survey. 26 patients responded by email and 34 by telephone. 47 patients(78%) had axillary brachial plexus block, 11(18%) had supraclavicular block and only 2(3%) had infraclavicular block. Over 95% of patients were satisfied with the preoperative information and the overall care they received from their anaesthetist. 88% of patients claimed to have no pain during the operation with 7% saying they had mild discomfort. Over 80% of patients said they had either no pain or mild pain during block performance. 12% of patients were not satisfied with the post-operative analgesia they received. 22% of patients said they had moderate to severe discomfort due to having a numb arm. 90% of patients were happy to have regional anaesthesia in future if needed and about 92% were happy to recommend this to their friends and family.
Conclusions The overwhelming majority of patients were satisfied with the care they received for hand surgery under regional anaesthesia, would be willing to have again and recommend it to their friends and family. However there is still room for improvement. Respondents who scored moderate to severe pain during injection were, unsurprisingly less likely to be willing to have regional anaesthesia again. Improved patient-anaesthetist rapport, judicious sedation and modification of injection technique might address this issue. Areas identified for improvement included quality of post-operative analgesia and avoidance of prolonged motor block by appropriate choice of local anaesthetic. References
1. Irinfield CM, Barrington MJ. Are patients satisfied after peripheral nerve blockade? Results from International Registry of Regional Anaesthesia. Regional Anesthesia and Pain Medicine. 2014 Jan-Feb; 39(1):48-55
2. Montenegro A, Pourtales MC. Assessment of patient satisfaction after regional anaesthesia in two instituitions. Ann Fr Anesth Reanim 2006 Jul;25(7):687-95
34
3131666 Observational Study Of Noninvasive Cardiac Output Monitoring Using Pulse Wave Transit Time In Conscious Patients Under Regional Anaesthesia Ramachandran, Rajasekar; Balaji, Packianathasamy; Hammond Jones, Anne-Mair Hull Royal Infirmary, Hull Introduction Estimated continuous cardiac output [esCCO by Nihon Kohden monitor] provides noninvasive method of cardiac output measurements. It derives cardiac output using new technology PWTT (Pulse Wave Transit Time) obtained from plethysmographic wave and ECG. PWTT principle has never been used previously to monitor cardiac output in awake patients under regional anaesthesia. Methods This is an observational study conducted at women and children’s hospital, Hull Royal Infirmary, UK. Ethics committee and local R&D approval was obtained for this trial. All parturients scheduled for elective caesarean section were seen at pre-assessment clinic and informed about this trial. Participating patients were consented for this trial according to EU Directive guidelines. Women with BMI above 40, Pre-existing or pregnancy induced hypertension, diabetes mellitus, cardiovascular or cerebrovascular disease, placenta accreta, less than 37 weeks and who required translator were excluded. All recruited patients had standard Philips monitor cuff attached to left arm and Nihon-Kohden monitor cuff in right arm to measure Cardiac output (CO) and Stroke volume (SV). All recruited patients received spinal anaesthesia with 0.5% Bupivacaine heavy and diamorphine (total upto 3.0ml volume). If any patient had a drop in BP by 25% from baseline, intermittent boluses of Phenylephrine (80µg) was given to restore NIBP. Both monitors measured NIBP every minute before delivery of baby and every 2.5 minutes after delivery. Heart rate and pulse oximetry were measured continuously. Additionally, Nihon-Kohden monitor measured CO and SV. Results 45 Patients were successfully recruited for the study. Out of 45 patients, 14 patients did not require phenylephrine boluses to maintain NIBP above 75% baseline. 16 patients had interference in cardiac output and stroke volume monitoring. Calibration took 6.82±5.75 minutes to provide CO and SV measurement after disturbance. 2 patients had repeat disturbance during the procedure which affected the continuous CO measurement. Discussion As this machine depends upon the ECG and Saturation reading to calculate the Cardiac output, even minor disturbance like chest movements or finger movements affects the CO, SV values. With the available measurement, 14 patients (33%) did not need phenylephrine boluses. This monitor might be helpful for continuous measurements of CO and SV in awake patients but further comparative studies are required for its reliability in high risk patients. References
1. Anne Doherty 1, Yayoi Ohashi 2, Kristi Downey 3, Jose CA Carvalho - Non-Invasive monitoring based on bioreactance reveals significant haemodynamic instability during elective Caesarean section delivery under spinal anaesthesia: Revista Brasileira de Anestesiologia Vol. 61, No 3, May-June, 2011
2. S. Armstrong, R. Fernando, M. Columb - Minimally- and non-invasive assessment of maternal cardiac output: go with the flow! International Journal of Obstetric Aanasethesia 2011; 20: 330-340

35
3101579 NICE & Comfortable: Fascia-iliaca Blocks In Fractured Neck Of Femurs R. Shah1, E. Wild, J. Thomas, A. Cohen1 1. Barnet General Hospital, London, UK. Central Thames School of Anaesthesia Introduction Approximately 75,000 fractured neck of femurs (NOFs) occur each year. Patients are in severe pain upon arrival to hospital. NICE hip fracture guidelines recommend analgesia with paracetamol and opioids, with addition of a fascia-iliaca block (FIB) if pain persists [1]. We investigated whether these guidelines were being followed at Barnet General Hospital. Methods We performed a prospective audit between March and July 2014, divided into two parts. We questioned orthopaedic and A&E trainees on their knowledge of NICE hip fracture guidelines, and how to perform FIBs. We then audited 105 patients with fractured NOFs over 5-months. We expected 100% of patients to have received analgesia with paracetamol, systemic opioids, and FIB if clinically indicated. We analysed the results and introduced interventions, which included educating staff on how to perform FIBs, and design of a ‘Pain management in fractured NOFs’ poster. After a period of 6-weeks, we completed the audit cycle by re-assessing knowledge amongst the trainees to explore whether our interventions had improved awareness of NICE guidelines and use of FIBs within our hospital. Results We audited 40 trainees in orthopaedics and A&E. Following questioning, 18 (45%) trainees were aware of NICE guidelines on analgesia in hip fractures, and 9 (23%) trainees felt competent to perform a FIB without direct supervision. We audited a total of 105 patients with fractured NOFs, which included 63 in the pre- and 42 in the post-intervention cohort. In the pre-intervention cohort, 63 (100%) patients received pre-operative paracetamol and morphine. Four (6%) patients received fascia-iliaca block, despite 51 (81%) patients remaining in pain pre-operatively. Following our interventions, we re-audited practice in 42 patients and found 28 (67%) of patients received fascia-iliaca blocks, with an overall reduction in pre-operative pain scores. Discussion This audit revealed that our hospital failed to address pre-operative pain in fractured NOFs. Many trainees felt inexperienced to perform fascia-iliaca blocks confidently. By raising awareness of NICE guidelines on hip fractures, improving assessment of pain, and organising a practical workshop, we promoted use of FIBs with confidence, and significantly reduced pre-operative pain. Promoting NICE guidelines and educating trainees to perform a simple, yet effective procedure can provide significant pain relief and reduce opioid-related side effects in fractured NOF patients. References
1. Hip Fracture: The management of hip fracture in adults. NICE clinical guideline 124. Issued June 2011.

36
3101648 Inadvertent Wrong-side Wrong-Block: Are We Stopping Before Blocking? Shah, Raj Royal Free Hospital NHS Trust Introduction Inadvertent wrong-sided nerve blocks can result in serious consequences. These include complications from the unnecessary block itself, such as nerve injury and local anaesthetic toxicity, and can even result in the surgical team performing a wrong-site surgery.The National Patient Safety Agency (NPSA) describe a ‘Never Event’ as a serious, largely avoidable patient safety incident that should not occur if appropriate preventative measures have been implemented [1]. Whilst inadvertent wrong-sided nerve blocks are not defined as a ‘Never Event’, they are understandably unacceptable, and preventative measures are required to reduce their incidence.Several important factors have been identified, contributing toward the performance of the wrong-sided nerve block. The ‘Safety Anaesthesia Liason Group’, together with the Royal College of Anaesthetists, has introduced a ‘Stop Before You Block’ guideline, highlighting important steps which should be carried out prior to insertion of a nerve block [2]. We investigated whether these guidelines were being followed at Moorfield’s Eye Hospital. Methods We performed a prospective audit between December 2014 and February 2015. We questioned anaesthetists at Moorfield’s Eye Hospital on knowledge of the ‘Stop Before You Block’ campaign, using a questionnaire proforma. We expected 100% of anaesthetists to be aware of these guidelines, particularly the steps that should be carried out prior to performing regional techniques for ophthalmic procedures.We analysed the results and introduced interventions, which included design of a modified ‘Stop Before You Block’ poster, and a personalised sticker for record in the patient anaesthetic notes. After a period of 6-weeks, we completed the audit cycle by re-assessing knowledge amongst the anaesthetic department to explore whether these interventions had improved awareness of the guidelines and safe implementation of regional nerve blocks. Results We audited 26 anaesthetists within our department. Following questioning, 14 (54%) anaesthetists were aware of the ‘Stop Before You Block’ campaign, with only 5 (19%) anaesthetists aware of the exact steps that should be conducted prior to insertion of a nerve block. Following our interventions, we re-audited practice and found 26 (100%) of anaesthetists were aware and compliant with the ‘Stop Before You Block’ guidelines. Discussion This audit revealed that specific recall of factors contributing toward a wrong-side nerve block was poor amongst anaesthetists within our department. In addition, the precise steps that have been proposed and recommended by the SALG’s campaign were not being complied wi References
1. National Patient Safety Agency. Never Events; Framework: Update for 2010/2011. Mar 2010. Available from: http://www.nrls.npsa.nhs.uk/resources/?entryid45=68518
2. Safe anaesthesia Liaison Group. Wrong Site Blocks During Surgery . Nov 2011. Available from: http://www.aagbi.org/foundation/safety/SALG_statement_WSB_10_11_10.pdf
37
3125767 'Improvement In Quality Of Pain Relief Following Emergency Laparotomy. Do Rectus Sheath Catheters Have A Place?' Skalska-Lis, Barbara; Nalawade, Vaishali; Cope, Sean Sunderland Royal Hospital Introduction Pain relief following emergency laparotomy can be challenging. Effective analgesia is crucial in enhanced recovery. Morphine Patient Controlled Analgesia (MPCA) is used following emergency laparotomy but is associated with nausea, respiratory depression, post-op delirium and ileus. Safe regional anaesthesia could provide opiate sparing effects. Epidural analgesia can improve postoperative outcome, however they are contraindicated in sepsis and coagulopathy. Rectus sheath catheters (RSC) are an alternative where pain relief is required for a midline incision (T6-T11). Catheters can be inserted by either the surgeon at the end of the procedure under direct vision or after surgery by the anaesthetist under USS guidance. Methods A retrospective case series was carried out on 40 patients who underwent emergency midline laparotomies in 2014. Required data was collected from patient case notes. Patients were excluded if the medical records were incomplete or they received single shot regional anaesthesia in the perioperative period. Patients were divided into two groups: RSC group and PCA only group. Data was collected from anaesthetic, NEWS, PCA charts and inpatient clinical records. Results There were 17 patients in RSC group and 10 patients in PCA only group. Mean pain scores were identical between both groups in recovery, Day 1 and Day 2 post-op. Morphine requirements are demonstrated in the table below.
Recovery Day 1 post op Day 2 post op Total
RSC 8mg 47mg 32mg 140mg
PCA only 11mg 86mg 58mg 210mg
Our practice Initial bolus of 20 mls of 0.25% levobupivacaine bilaterally following insertion followed by a continuous infusion of ropivacaine 0.2% at the rate 5 mls/h bilaterally via two elastomeric pumps. Discussion National Emergency Laparotomy Audit (NELA) suggested effective pain management could improve outcomes for elderly high risk surgical patients. We audited our practice as a quality improvement measure looking to improve pain relief following emergency laparotomy. Conclusion Our case series analysis showed that USS placed Rectus Sheath Catheters are a reliable and safe adjunct to providing post-operative pain relief following emergency laparotomy. They offer a significant morphine sparing effect of up to 30%. With a decrease in morphine consumption it is therefore expected there would be a decrease in side effects associated with morphine use while still providing equally effective analgesia. RSCs can be placed at the end of surgery, as a rescue technique in recovery or prior to extubation on the intensive care unit. Although a continuous infusion technique is standard practice at our hospital, an intermittent bolus technique is a possible and effective alternative but requires regular top-ups and is labour intensive. References
1. Wilkinson KM, Krige A. Rectus Sheath Catheters after emergency laparotomy: A case report. National Acute Pain Symposium. 2014.
2. Wilkinson KM, Krige A. Thoracic Epidural analgesia versus Rectus Sheath Catheters for open midline incisions in major abdominal surgery within an enhanced recovery programme (TERSC). Trials journal 2014. 15-400.
3. Aung E, Fluri P. Introduction of continuous regional analgesia via wound catheters in a peripheral hospital. The New Zealand Medical Journal 2010. 123:1324.

38
3132089 Documentation Of Peripheral Nerve Blocks Tanna, Shamil; Wibberley, Helen; Kale, Vijay; Patel, Dilip Royal Free Hospital Introduction Medical record keeping is an essential part of modern day medicine. It facilitates communication, allows effective and safe continuity of care and is a vital medico-legal record. Both the use of peripheral nerve blocks (PNB) and the variety in techniques to provide anaesthesia & analgesia is increasing, which can lead to the increased possibility of errors and complications. Although documentation is recommended by various bodies, there is a lack of structure as to what is required for PNB’s (1). Methods A sample size of 37 patients receiving a PNB were collected over a 2 week period between 17/11/2014 and 01/12/2014. Data was retrospectively collected from anaesthetic records. Compliance with standards collated from a peer review journal was assessed (2). These included consent (including benefits and risks), name and grade of operator, name of block, site, laterality, site checked, patient conscious level, asepsis (Including details), method of localisation, needle details, injectate details, negative aspiration and ease of injection. Following the initial audit, a label was introduced which listed these standards to allow easy documentation. The documentation of PNBs was re-audited with a sample size of 31 patients collected over a 2 week period between 09/03/2015 and 23/03/2015. Results Standards
Percentage Compliance
Pre- Audit
[n=37]
Post Audit (post label)
[n=31]
Yes No Yes No
Consent 78% 22% 70% 30%
Benefits 0% 100% 3% 97%
Risks 35% 65% 39% 61%
Label Used N/A N/A 54% 46%
Name / Grade of Operator (esp. when 2
anaesthetists) 57% 43% 81% 19%
Name of Block 100% 0% 100% 0%
Side / Laterality 86% 14% 90% 10%
Site Checked (from WHO checklist) 81% 19% 71% 29%
Mention of Awake/Sedation/GA 59% 41% 71% 29%
Asepsis observed 89% 11% 97% 3%
Asepsis details 30% 70% 84% 16%
Method of Nerve Localisation 100% 0% 100% 0%
Needle details 54% 46% 94% 6%
Injectate details 97% 3% 100% 0%
Negative aspiration 30% 70% 65% 35%
Ease of Injection 43% 57% 71% 29%
Discussion Although consent for PNB is often documented, there is no documentation of benefits and limited documentation of risk. Studies have shown that anaesthetists routinely underestimate and fail to

39
discuss the risks of RA. Therefore informed consent allows informed decisions and helps to protect against litigation (3). Our audit shows that there is reduced documentation of needle type and ease of injection. There is data lacking on the likelihood of PNB exhibiting nerve injury, however type of needle and ease of injection is linked and therefore documentation of these details are essential. Following the implementation of the label it can be seen that there is a significant improvement in all aspects of required standards, bar consent, particularly conscious level, details of asepsis and needle details. Of those 16 PNBs documented using a label there was 100% compliance with most standards, except consent (including benefits and risks) and negative aspiration. Thus the use of a label may allow standardised and easy documentation. Conclusion Detailed documentation is essential to allow accurate communication. Although documentation of consent is present, there is limited documentation of benefits or risks. Use of a standardised label may help to bring uniformity and allow accurate and easy documentation. References
1. Royal College of Anaesthetists, The Association of Anaesthetists of Great Britain and Ireland. The Good Anaesthetist: Standards of Practice for Career Grade Anaesthetists [Internet]. 2010.
2. Gerancher JC. Viscusi ER. et al. Development of a Standardized Peripheral Nerve Block Procedure Note Form. Regional Anaesthesia and Pain Medicine. 2005; 30(1): 67-71.
3. Sardesi A, French J, Pawa A. Patient consent for peripheral nerve blocks [Internet]. RA-UK; 2015.
40
3128436 Post Operative Complications Increasing Length Of Stay In Elective Total Hip Replacement Patients: A Single Centre Report Varadan, Rama1; Balaji, Packianathaswamy1; Bowden, Rachel2; Symes, Tom1 1Hull Royal Infirmary;
2Northern General Hospital
Introduction Enhanced recovery programmes have been implemented in many UK centres with a view to reduce hospital inpatient stay post operatively, reducing the length of hospital stay for hip and knee Arthroplasties, with elective total hip replacement surgery patients averaging 4.6 days1.We have implemented ERAS pathway in July 2011 but would like to identify any perioperative factors like bleeding, hypotension etc delaying the discharge of elective primary total hip replacements (THR). Methods After obtaining Trust Clinical Governance approval, we collected Data from 83 consecutive ASA I-III patients who had elective primary THR for 9 weeks. We correlated the length of stay with anaesthetic technique, blood pressure, haemoglobin (intra/post-operative), and any post-operative complications. Results Patients ranged between 41 and 85 years with few having multiple co-morbidities; previous MI, CVA, hypertension, angina. Hypotension and dizziness were present in 22% of study population associated with either a drop in BP/haemoglobin concentration or both in those patients. The length of hospital stay was significantly affected by hypotension and syncope post op (P<0.05), however the mode of anesthesia delaying the length of stay remains inconclusive. Conclusions Post-operative complications have significant impact on the length of stay in elective THR patients, particularly when multiple co-morbidities are combined with perioperative hypotension or a drop in hemoglobin postoperatively. Most patients had a 50% reduction in pre op systolic BP intra-operatively, regardless of anaesthetic technique which delayed the recovery. We advocate the pre-operative optimisation of patients and ensure adequate fluid resuscitation and/or transfusion post surgery in the recovery room. References
1. 1.Benson R.,Drew J.et al,A waiting list to go home:an analysis of delayed discharges from surgical beds,Annals of Royal College of Surgeons England 2006; 88: 650--652
2. 2.Husted H.,Holm G.et al, Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: Fast Track experience in 712 patients, Acta Orthopaedica, 2008; 79: 168--173
3. 3.Husted H., Lunn T.et al, Why still in hospital after fast track hip and knee arthroplasty? Acta Orthopaedica 2011; 82: 679--684

41
3132936 Elvis Presley "Saves The Day" In A High-risk Anxious Patient Undergoing Prolonged Orthoplastic Surgery Under Epidural Anaesthesia And Sedation: Crucial Impact Of Audio-visual Distraction. Wallis, Anna; Athanassoglou, Vassilis; Galitzine, Svetlana Oxford University Hospitals NHS Trust Introduction In our experience epidural anaesthesia and sedation (EA+Sed) for lower limb free tissue transfer (LLFTT) offers many benefits over conventional general anaesthesia (GA), including avoiding possible respiratory complications of prolonged GA (1). Sedation, titrated to patients’ requirements to ensure comfort and reduce anxiety, can be challenging. We present a case when music as a modality of audio-visual distraction (AVD) became crucial in management of a respiratory compromised patient. Case Report A 54 year old man presented for excision of osteomyelitis and LLFTT. He had BMI of 30 and sleep apnoea habitus, history of heavy smoking, excessive alcohol intake and degenerative cervical disc disease with upper limb paraesthesiae. He had 19 previous GAs and was very anxious. He reluctantly agreed to EA with moderate to deep sedation. Management Once effective EA was established, sedation was provided with propofol TCI and aliquots of fentanyl and midazolam but proved difficult. He seemed to settle on deeper levels of TCI with added ketamine (“Ketofol”), with adequate saturation, albeit intermittent snoring. However, arterial blood gas (ABG) at this stage revealed acute respiratory acidosis: pH 7.185, pCO₂ 10.2 kPa, pO₂ 15.6 kPa and normal BE. The options were between intubation and mechanical ventilation or alternative anxiolysis. On lightening sedation, the patient was offered music and requested Elvis Presley, whose album was, fortunately, previously downloaded on our recently acquired AVD kit (a tablet and noise-cancelling headphones). Listening to his favourite music at preferred volume allowed surgery to proceed with a 9.5hr procedure with propofol TCI maintenance at 0.2µg/ml. Outcome Subsequent ABG showed rapid reversal of the acidosis. The patient was physiologically stable throughout, with ABGs before and after flap revascularization, and at the end of surgery: pO2 22.5/22.8/23.1 kPa, pH 7.38/7.37/7.45, pCO₂ 5.7/6.0/4.8 kPa and BE 0.4/1.3/1.8, respectively. There were no complications and the flap outcome was good. On formal assessment he reported being “very satisfied” with the anaesthetic and found it a “better experience” than his previous GAs. Discussion In our centre we are performing service evaluation of AVD as an adjunct to RA. Music of patients' choice played at patients’ preferred volume is known to have a positive impact during minor procedures (2). This is the first use of AVD for prolonged EA+Sed for LLFTT surgery. Conclusions This case demonstrated the challenges of deep sedation and the crucial positive impact of AVD in a respiratory compromised anxious patient undergoing prolonged orthoplastic surgery under EA+Sed. References
1. Galitzine S, Wallis A, Ramsden A, Cogswell L, McNally M. Central neuraxial anaesthesia and sedation for prolonged orthoplastic lower limb surgery requiring free tissue transfer: a seven year experience. Regional Anaesthesia and Pain Medicine 2014; 39(5) Supp 1: E245.
2. Kim YK, Kim SM, Myoung H. Musical intervention reduces patients’ anxiety in surgical extraction of an impacted mandibular third molar. Journal of Oral Maxillofacial Surgery 2011; 69: 1036–45.

42
3132525 Interscalene Block In The Obese Patient: A Tempting Prospect But Is It Doomed To Failure? Comparison Of Techniques And Success Between Obese And Non-Obese Patients. Watkinson, Clare; Blundell, Mike Northumbria Healthcare NHS Foundation Trust Objectives To compare outcomes in obese patients following interscalene block (ISB) compared with those with body mass index (BMI) less than 30kg.m2. Introduction The AAGBI guideline ‘Peri-Operative Management of the Morbidly Obese Patient’1 suggests ‘the use of regional anaesthesia in the morbidly obese patient and the avoidance of general anaesthesia to be a tempting prospect’, but suggests attempts at successfully achieving this may be ‘doomed to failure due to the size of the patient’. Standards for post-operative pain relief were taken from the RCOA compendious of audit recipes. Standards audited against were 85% reporting no pain or mild pain after discharge (with medication), and > 85% satisfied with the management of their pain while at home2. Methods Block room data from Northumbria Hospitals was collected over a two-year period. All patients who had undergone an ISB were included in the analysis. Those with BMI greater than 30kg.m2 were compared with those with BMI of less than 30kg.m2. Data was collected on the purpose of the block (analgesia or anaesthesia), method of block insertion (US or landmark technique), anaesthetic technique, pain scores post operatively and patient satisfaction. Results Data was available for 329 patients undergoing ISB, of these 33% were obese, and 5% morbidly obese (BMI>40). The majority of blocks were performed as analgesic blocks, however 19% were performed for anaesthesia. Seventy-five percent of patients were discharged on the day of surgery. All blocks were performed under ultrasound (US) guidance. 82% of blocks in obese patients were described as perfect intraoperatively by the anaesthetist, compared with 88% in those with BMI <30kg.m2. In recovery, 86% of obese patients had a pain score of zero, compared with 90% with BMI <30kg.m2. The percentage of obese patients describing severe post-operative pain was less than those with BMI<30kg.m2, however in both groups pain scores increased as the block wore off. Of the obese cohort, 89% described their overall experience as good or excellent, with only 2% describing it as awful. Conclusion Results are comparable in obese and non-obese patients. In both groups there was a low incidence of severe pain in the day of the block, but this increased on the first night and the following day, suggesting a potential deficit in provision of additional analgesia. The majority of patients were positive about their overall experience. References
1. AAGBI Peri-Operative Management of the Morbidly Obese Patient. June 2007. 2. Royal College of Anaesthetists. Raising the Standard: a compendium of audit recipes. 3rd
Edition 2012
43
3132248 'Breakfast Block' Creating A Royal College Of Anaesthetists Approved Regional Anaesthesia Course Successfully Providing Teaching To Consultants And Trainees In A District General Hospital Wingate, Robin; Foxall, Gillian Royal Surrey County Hospital Introduction Recently more weight has been given to ultrasound guided regional anaesthesia (USGRA) by the Royal College of Anaesthetists (RCOA) for certificate of completion of training1 2. Regional anaesthesia (RA) is relevant to a consultant anaesthetist’s ‘whole practice’ as stipulated by the RCOA continuing professional development (CPD) matrix for revalidation3. Providing RA teaching for anaesthetists is a challenge with pressures of reduced hours (EWTD) and study leave/budgets. There has therefore been departmental interest in opportunities to improve USGRA knowledge and skills by both consultants & trainees. We set up an early morning USGRA course covering multiple RA topics to fulfil this need. Methods We compiled a schedule of 12 topics incorporating the RCOA matrix for revalidation, 6 CPD points were successfully applied for. The title ‘Breakfast Block’ was created reflecting that sessions took place in the morning prior to anaesthetic reviews, in addition breakfast was provided to encourage attendance! Presentations were compiled & presented by the Regional Fellow in Anaesthesia & included a slideshow presentation & demonstration of sonoanatomy by live ultrasound scanning on a model via a projector (Fig 1). Presentations covered anatomy relevant to specific blocks, block technique and recent evidence in RA. For every session feedback & a register were taken.

44
Results Sessions were well attended & feedback improved throughout the course. Topics presented included: Basic physics of ultrasound, upper & lower limb, neuraxial and trunk blocks. Sessions lasted 30 min. Feedback was reviewed closely, a resultant change was to move the tutorial location to a more spacious area, feedback improved following this. Mean attendees for each session was 16. Average scores: content relevance 4.6/5.0, faculty presentation skills 4.8/5.0, venue/equipment 4.3/5.0. Discussion We successfully created a series of presentations with live demonstrations on USGRA in our department. An interest in RA & a desire for anaesthetists to improve their knowledge was reflected by the high attendance level. CPD points gained by course attendance have aided revalidation and completion of trainee regional modules. Conclusions Making time for departmental teaching is becoming increasingly difficult in modern, time-pressured NHS Trusts. There is however a demand within anaesthetic departments for both consultants and trainees to improve their knowledge and skills in USGRA for both training & revalidation purposes. We found presenting a series of early morning teaching sessions prior to anaesthetic pre-assessments to be an effective way to fulfil this requirement. References
1. Intermediate http://www.rcoa.ac.uk/system/files/TRG-CCT-ANNEXC_0.pdf 2. Higher http://www.rcoa.ac.uk/system/files/TRG-CCT-ANNEXD_0.pdf 3. Consultant http://www.rcoa.ac.uk/system/files/CPD-MATRIX-2013_2.pdf

45
3120035 Does Fusion Elastography Improve The Diagnosis Of Intraneural And Extra Neural Median Nerve Injection When Assessed By Anaesthesia Trainees? Zealley, Katherine1; Celnik, Daniel1; Corner, George2; McLeod, Graeme1; Munirama, Shilpa3 1NHS Tayside;
2University of Dundee;
3Manchester Royal Infirmary
Introduction Nerve injection during regional anaesthesia still occurs. Our recent systematic review and meta analysis has shown no difference in the rate of post operative transient neurological side effects, 8% vs 10.4%, RR (95% CI) 0.76 (0.53-1.09), p=0.13 when ultrasound and peripheral nerve stimulation are used1. Neuropraxia secondary to regional anaesthesia is attributed to accidental intrafascicular injection. A recent editorial recommended that local anaesthetic be injected without direct needle-to-nerve contact2. However, in practice, anaesthetists are poor at detecting intraneural injection. In studies examining post-procedure regional anaesthesia videos3, 1 in 6 nerve blocks performed by trainee anaesthetists, and thought to be extraneural, were later diagnosed as intraneural by experts. This equates to a false negative rate = 17% for diagnosis of extraneural/intraneural injection and sensitivity = 83%. Methods We wished to determine whether fusing elastography to a B-Mode image improved the diagnostic ability of anaesthesia trainees to diagnose intraneural median nerve injection when viewing post-procedure videos within the soft embalmed Thiel human cadaver. Intraneural injection was defined by consensus of two experts who were also aware of nerve area and brightness measured using ImageJ (NLM, Washington DC). Trainees viewed forty, 12 second videos, without repeat, using three ultrasound modalities: (1) B-Mode; (2) the combination of B-Mode and elastography presented as two adjacent images; and one week later (3) fusion images of B-Mode and elastography and (4) repeated B-Mode videos. Each trainee decided if each block was intraneural or extraneural and rated each decision with low, moderate or high degree of confidence. Our primary end point was the AUC of the multiple reader, multiple case, receiver operator characteristic (MRMC-ROC) curve (http:perception.radiology. uiowa.edu). Results Area and brightness measurements from 160 videos showed that intraneural injection diagnosed by experts was associated with: (1) an increase in the cross sectional nerve area (mm2) of the median nerve on B-mode images [intraneural 23.8 mm2 (95%CI: 20.7 - 27.4), extraneural 17.5 mm2 (95%CI: 15.0 - 20.3), difference 6.3, p=0.018; (2) a decrease in the cross sectional area of the elastogram [intraneural 42.1 mm2 (95%CI: 36.6 - 48.4); extraneural 68.0 mm2 (95%CI: 58.6 - 78.3), difference 25.9, p<0.001]; and (3) an increase in the brightness of the nerve on the fusion image [Intraneural 120.3 (95%CI: 108.9 - 133.0); extraneural 82.3 (95%CI: 73.7 - 90.9) difference 38.0, p<0.001)]. Conclusion We conclude that fusion elastography is associated with improved diagnosis of intraneural and extraneural injection.
B Mode
B Mode and
Elastography
Fusion
Elastography B Mode Retest
Sensitivity 69% (61% -
69%) 60% (51% - 68%) 86% (79% - 94%)
77% (68% -
86%)
ROC AUC 0.64 (0.56 - 0.71) 0.55 (0.45 - 0.64) 0.79 (0.71 - 0.87) 0.69 (0.60 - 0.78)
References 1. Munirama S, McLeod G. A systematic review and meta-analysis of ultrasound versus electrical stimulation for peripheral nerve location and blockade - accepted Anaesthesia 2015 2. Abdallah FW, Chan V . Anesth Analg. 2014; 108: 504-6 3. Liu SS, YaDeau JT, Shaw PM et al. Anaesthesia. 2011; 66: 168-74








![[ASM] Lab1](https://static.fdocuments.us/doc/165x107/588121881a28abb9388b706b/asm-lab1.jpg)





![[ASM] Lab2](https://static.fdocuments.us/doc/165x107/588121881a28abb9388b7069/asm-lab2.jpg)



