
2015: Pain Management - A Practical and Functional Approach-Lakkaraju
100
PAIN MANAGEMENT – A PRACTICAL AND FUNCTIONAL APPROACH Ravi Lakkaraju, MD Poway Spine and Pain Poway, CA
-
Upload
sdgwep -
Category
Health & Medicine
-
view
606 -
download
0
Transcript of 2015: Pain Management - A Practical and Functional Approach-Lakkaraju
PAIN MANAGEMENT – A PRACTICAL AND
FUNCTIONAL APPROACHRavi Lakkaraju, MD
Poway Spine and PainPoway, CA
The Phenomenon of Pain The International Association for the
Study of Pain (IASP) defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage”
Pain is the single most common reason for patients to seek medical attention
What is Pain ?
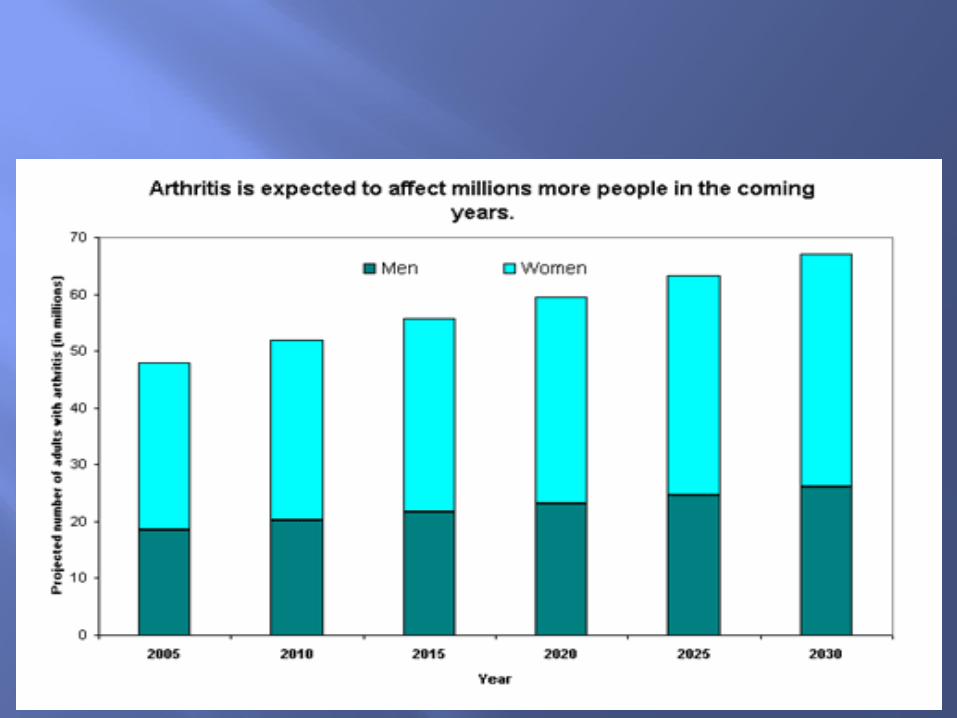
Demographics 2000 – 13.1% of population over 65 2030 – 20% of population over 65
25-50% of community elders suffer chronic pain of some kind
45-50% of Nursing home residents suffer chronic pain
Pain Chronic pain effects approx. 100 million
Americans
Roughly cost $635 billions annually
Incidence greater than Diabetes, heart disease and cancer combined.
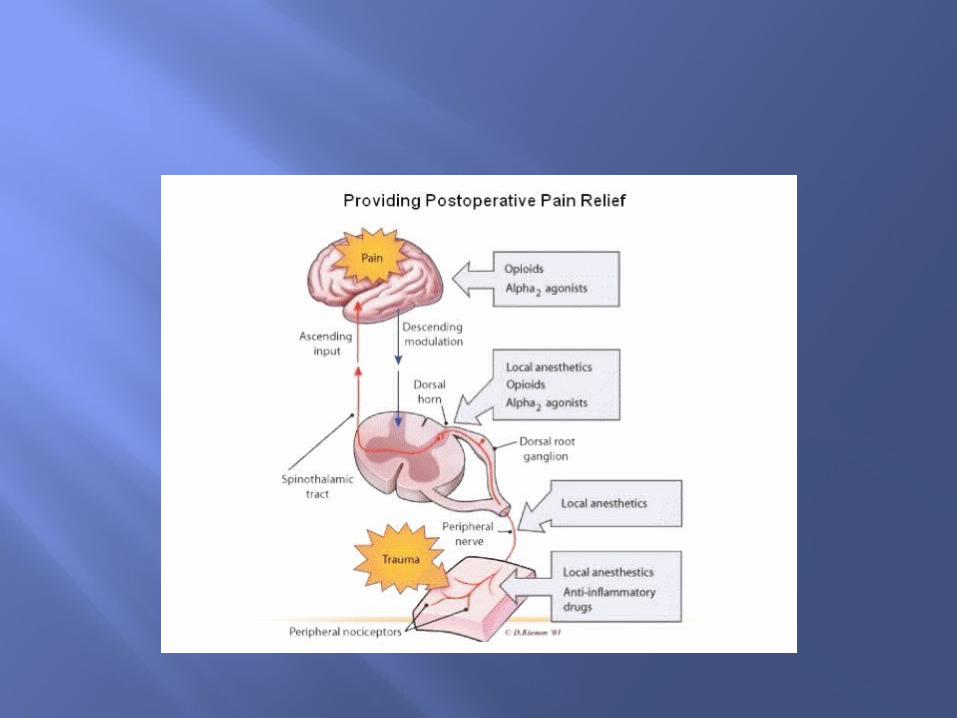
Peripheral Injury - sensitization of nociceptors - Nerve damage - Release of sensitizing humoral
mediators
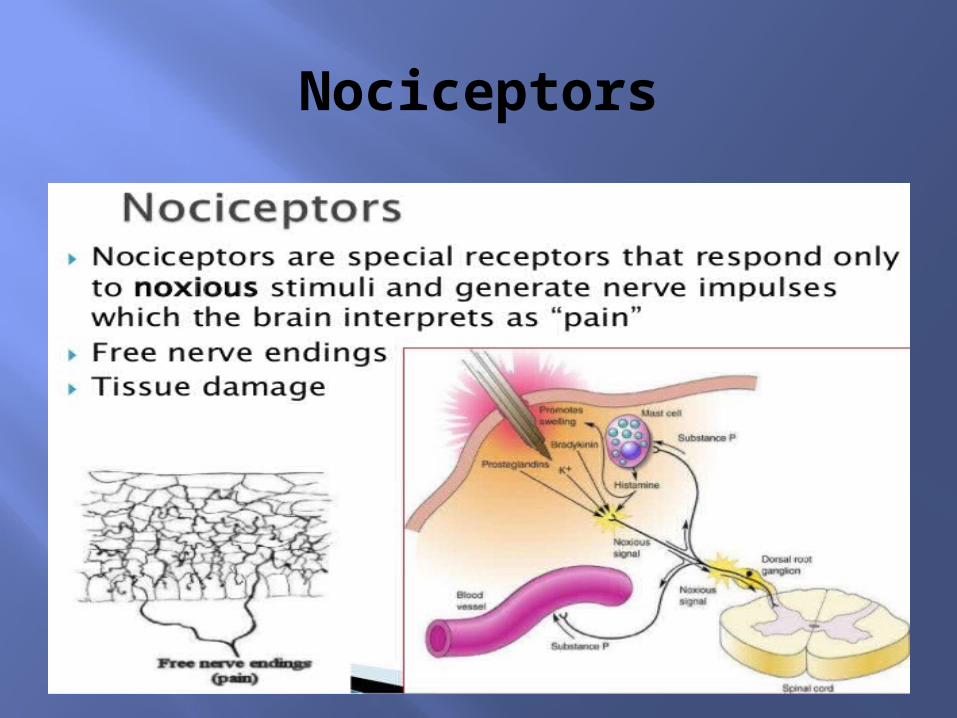
Nociceptors
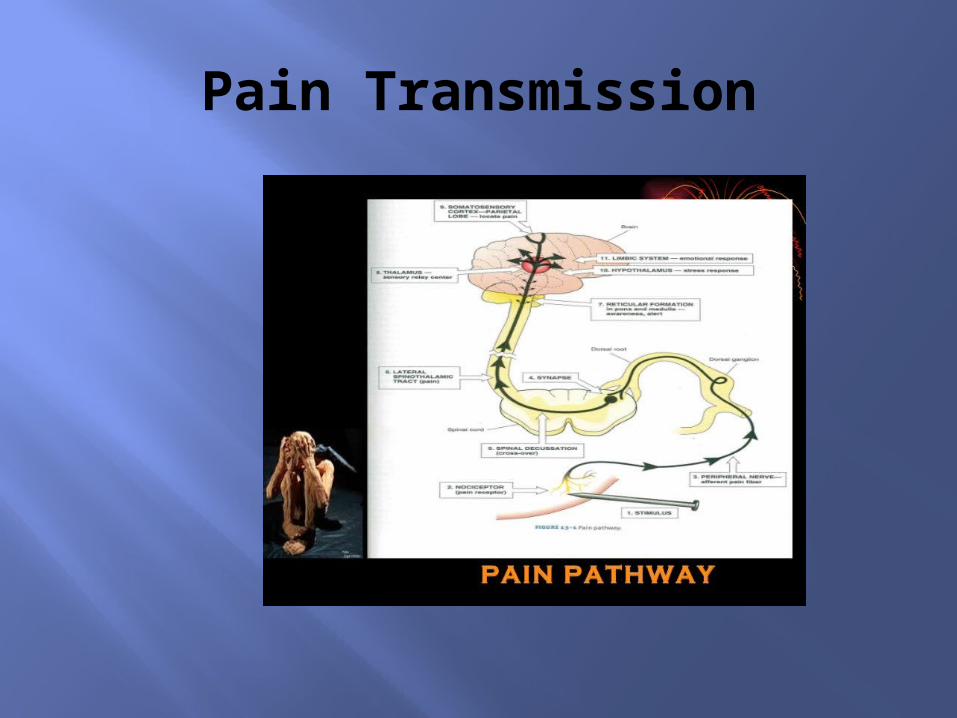
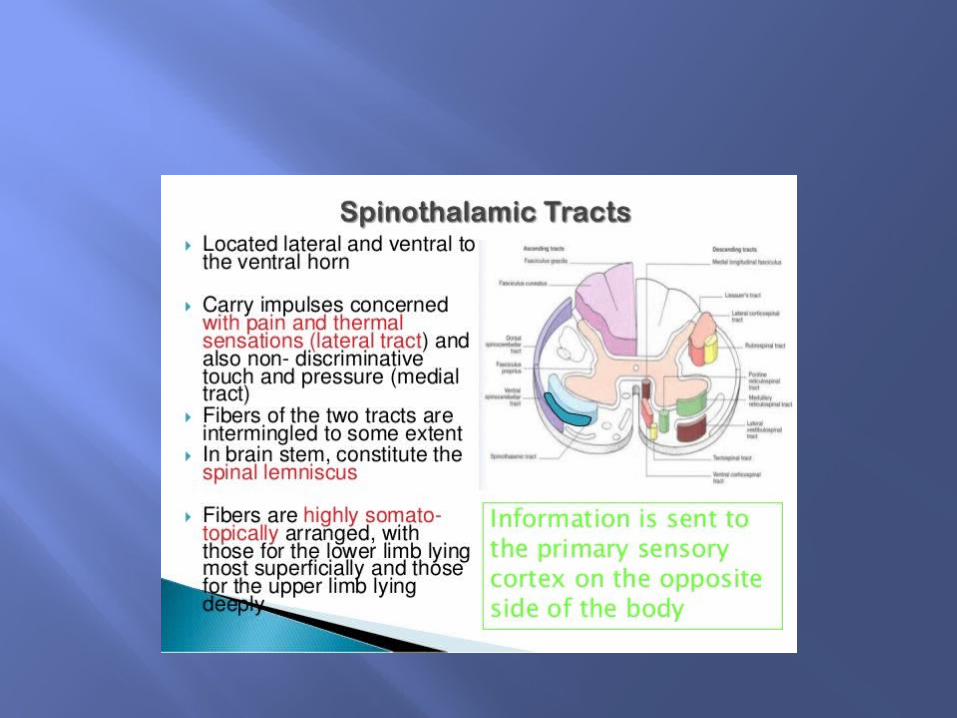
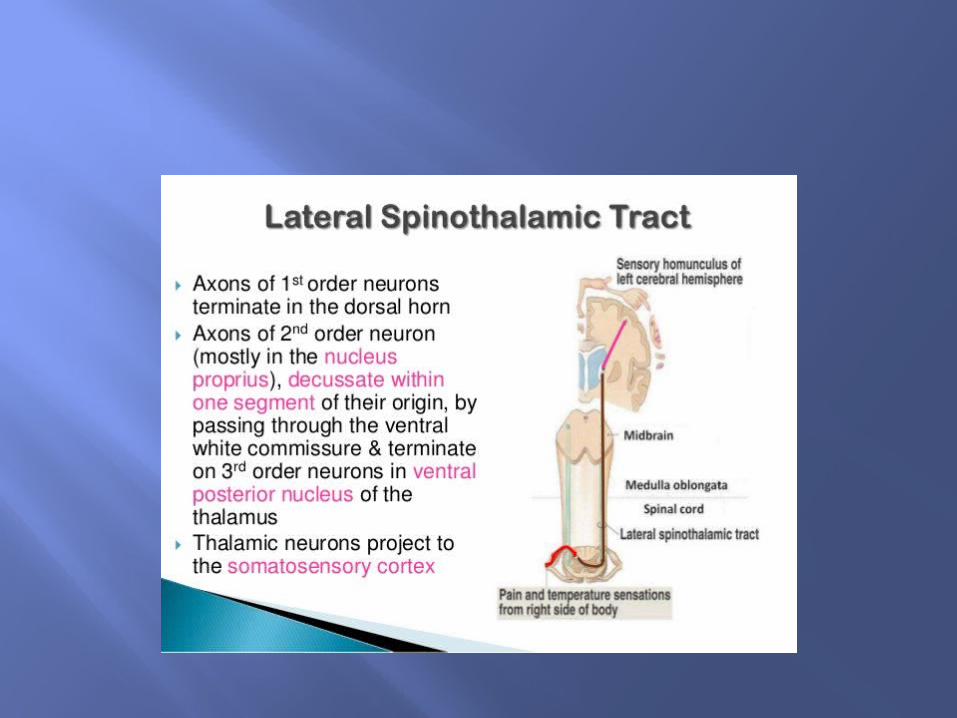
Pain Transmission
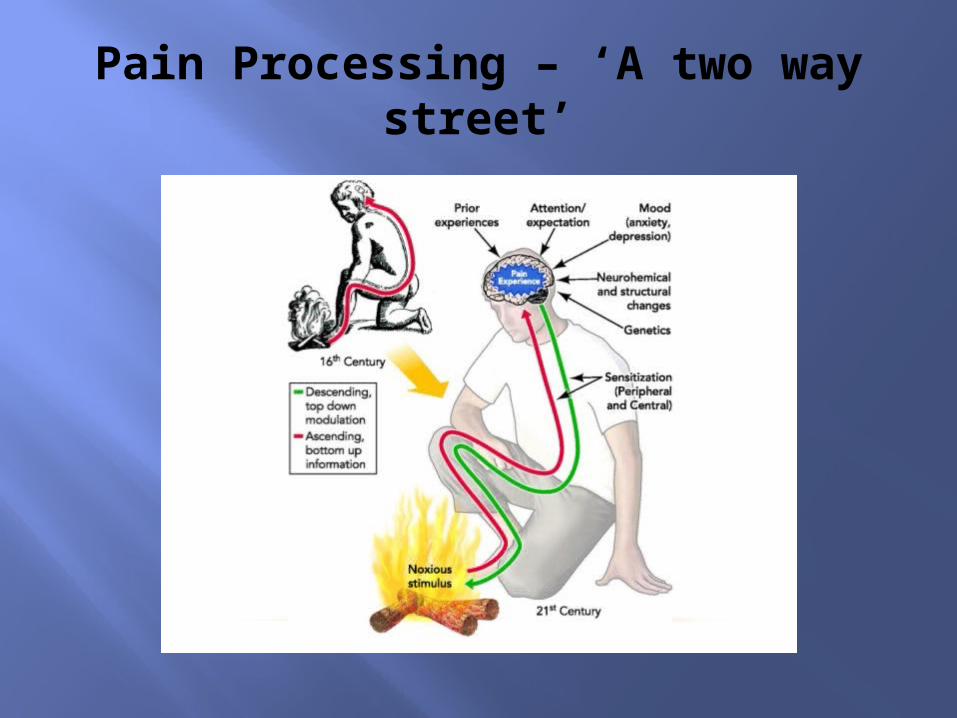
Pain Processing – ‘A two way street’
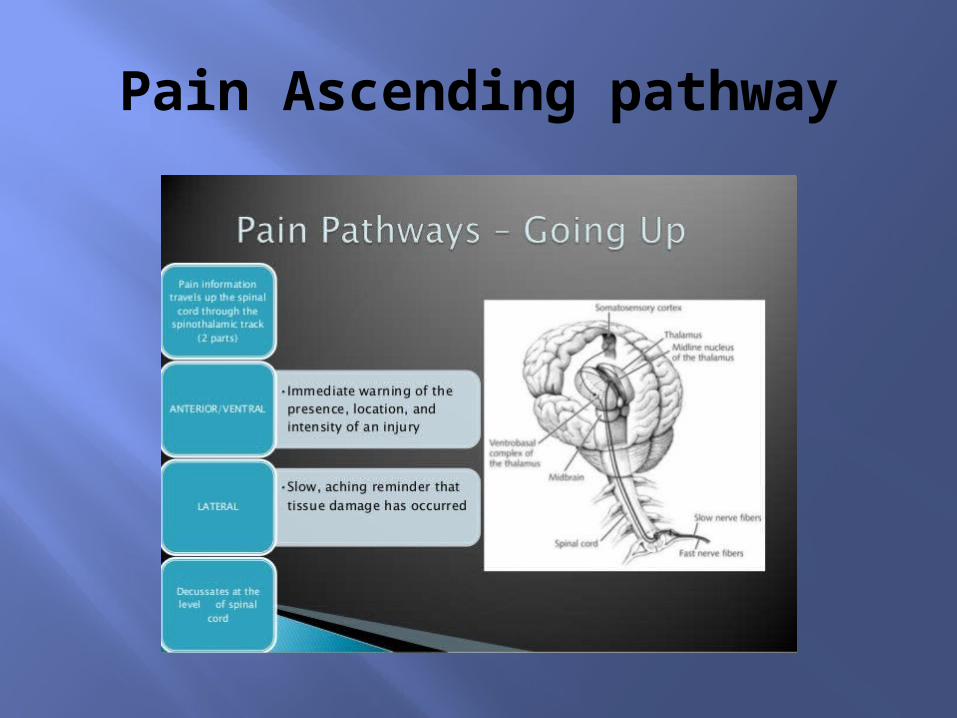
Pain Ascending pathway
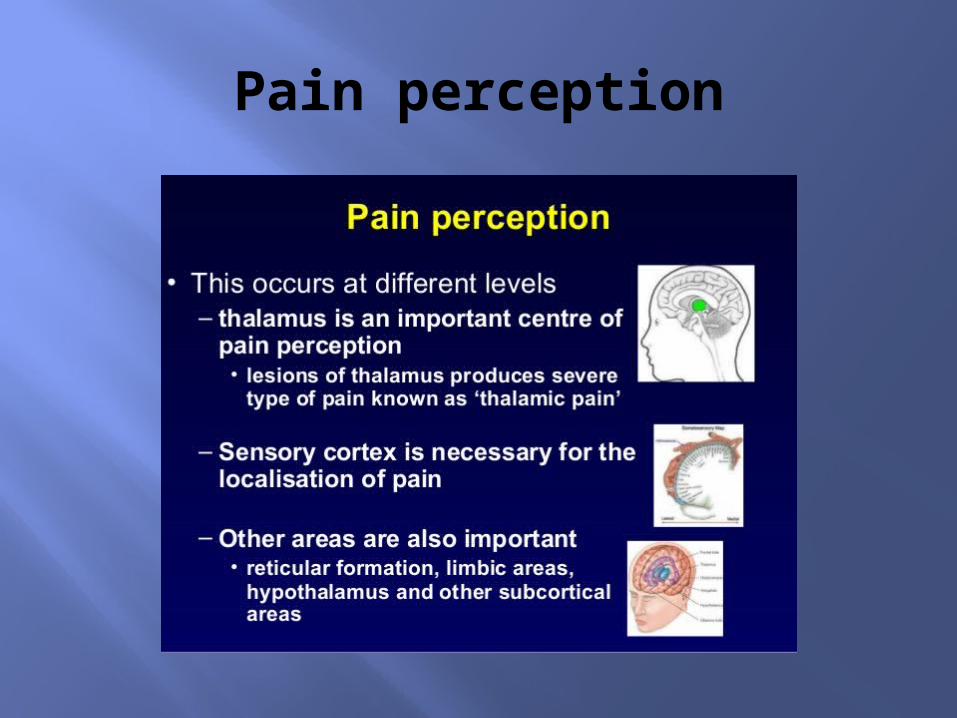
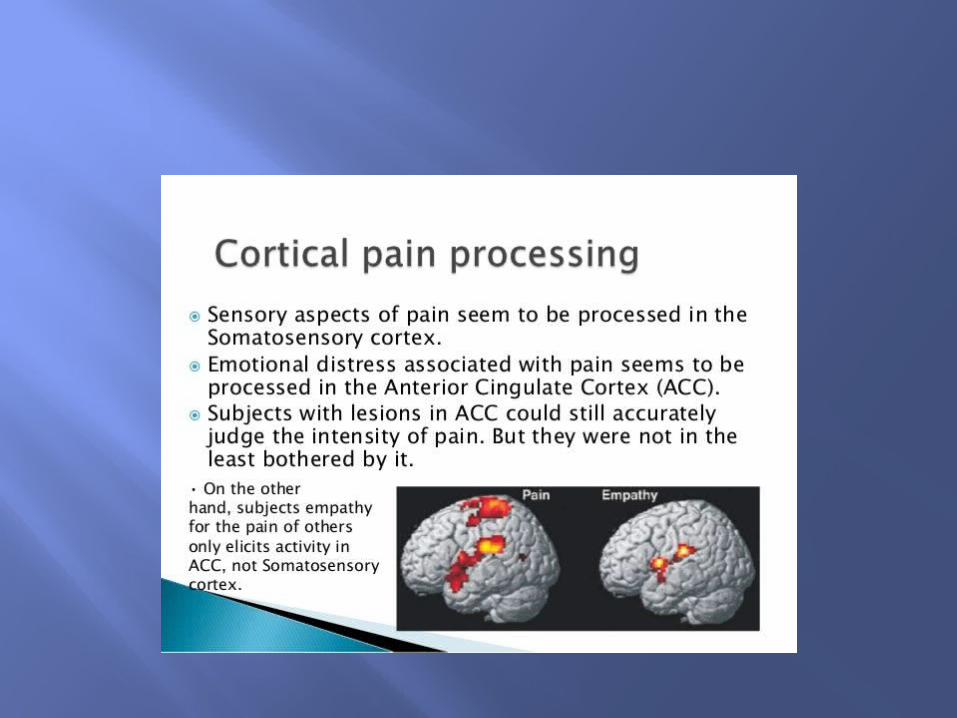
Pain perception
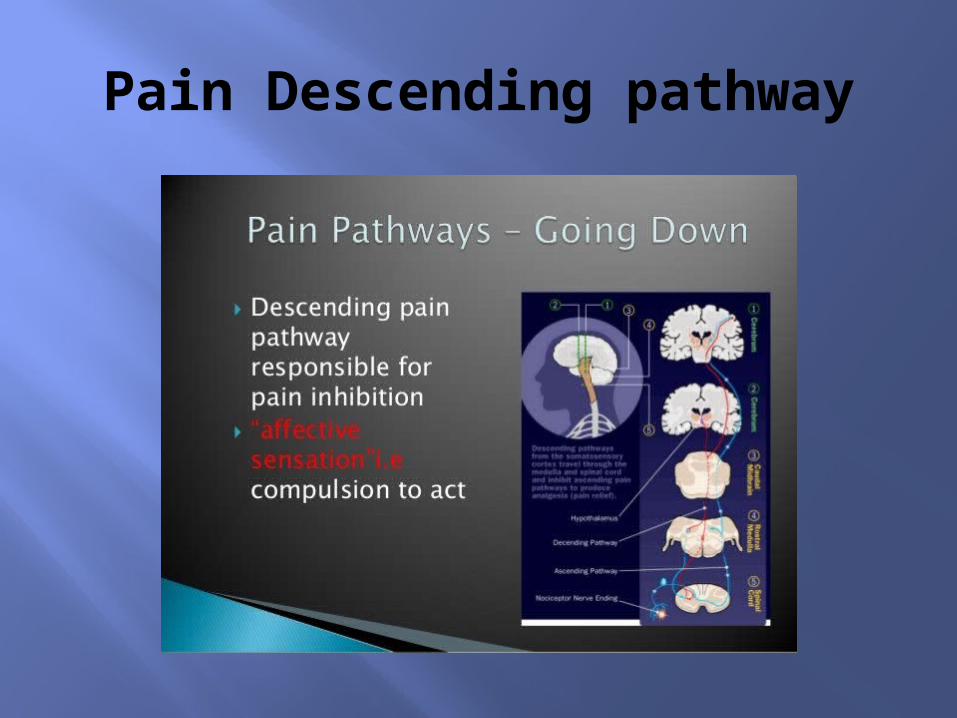
Pain Descending pathway
Nociception In some conditions, nociception due to
tissue damage may occur, but the patient may not perceive, or feel it i.e., diabetic peripheral neuropathy
Conversely, the patient may perceive severe pain with no demonstrable evidence of tissue damage i.e., trigeminal neuralgia
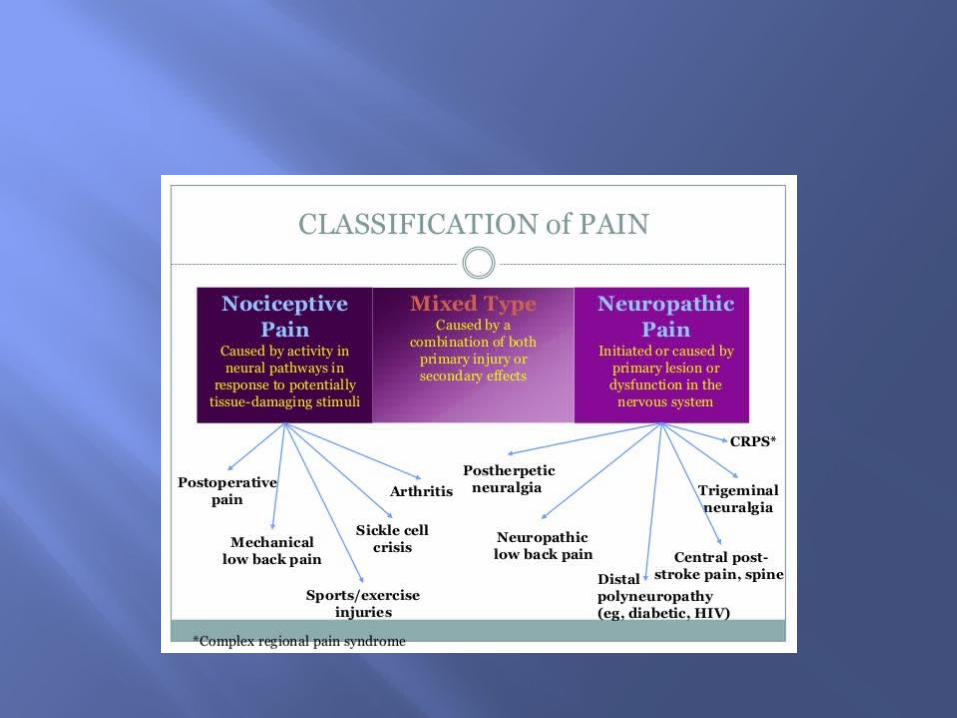
Pain classifications Nociceptive – somatic (superficial, deep)
and Visceral.
Neuropathic – painful mononeuropathies, polyneuropathies, Deafferentation pain, sympathetically maintained pain, central pain.
Mixed
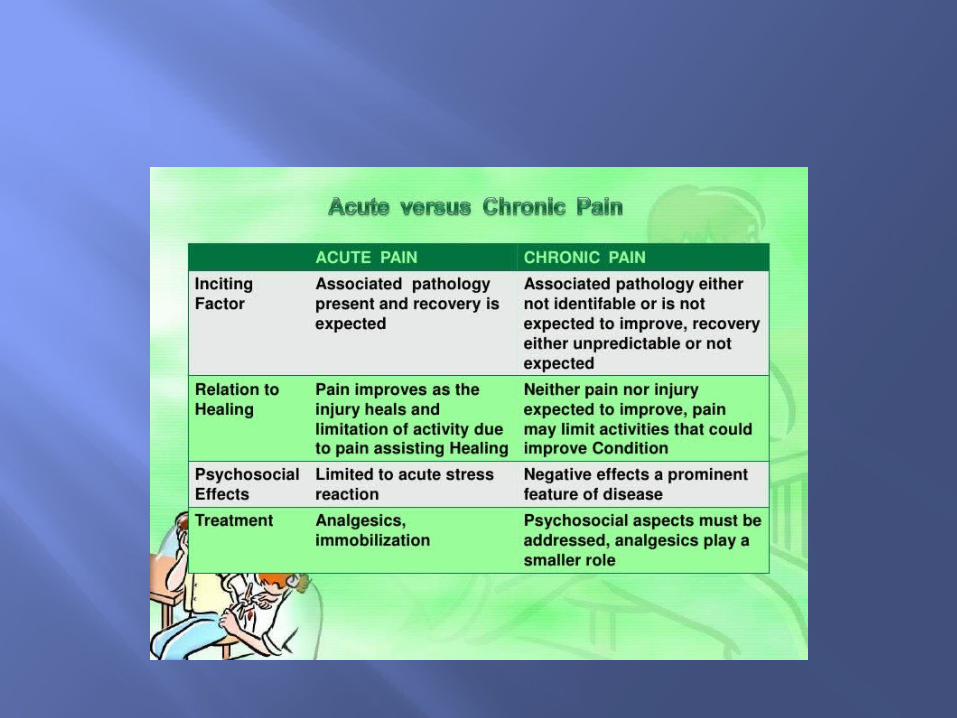
Pain Types Acute pain Chronic pain Cancer pain Chronic non-cancer pain (CNCP) CPS (chronic pain syndrome)
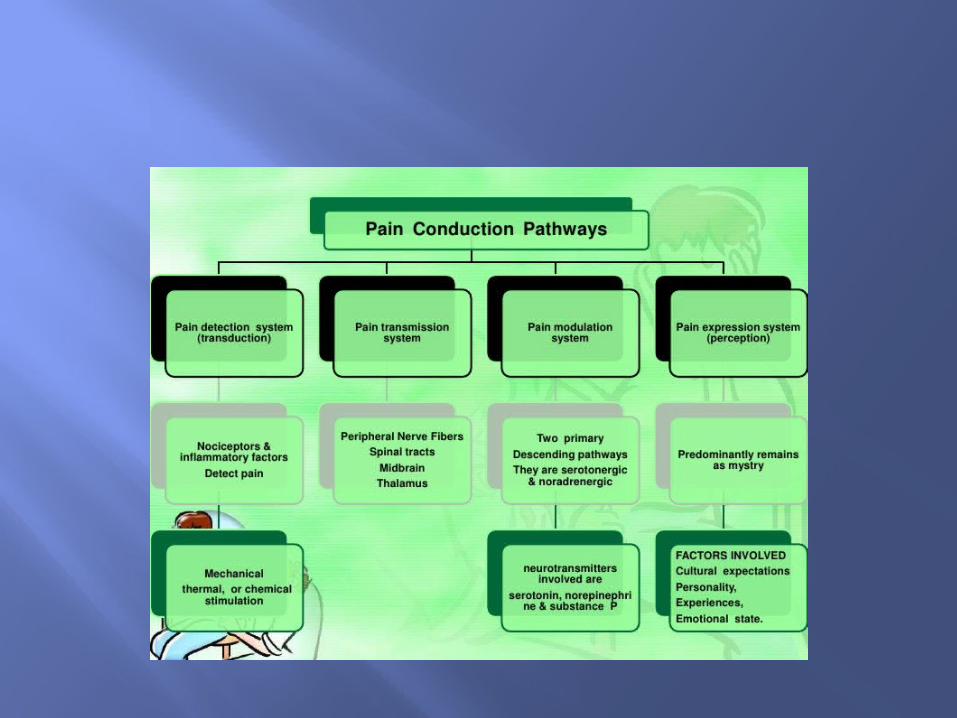
Basic Steps of Pain Transmission
4 Basic Steps: Transduction Transmission Modulation Perception
Transduction The process by which afferent nerve endings
participate in translating noxious stimuli (e.g., a pinprick) into nociceptive impulses
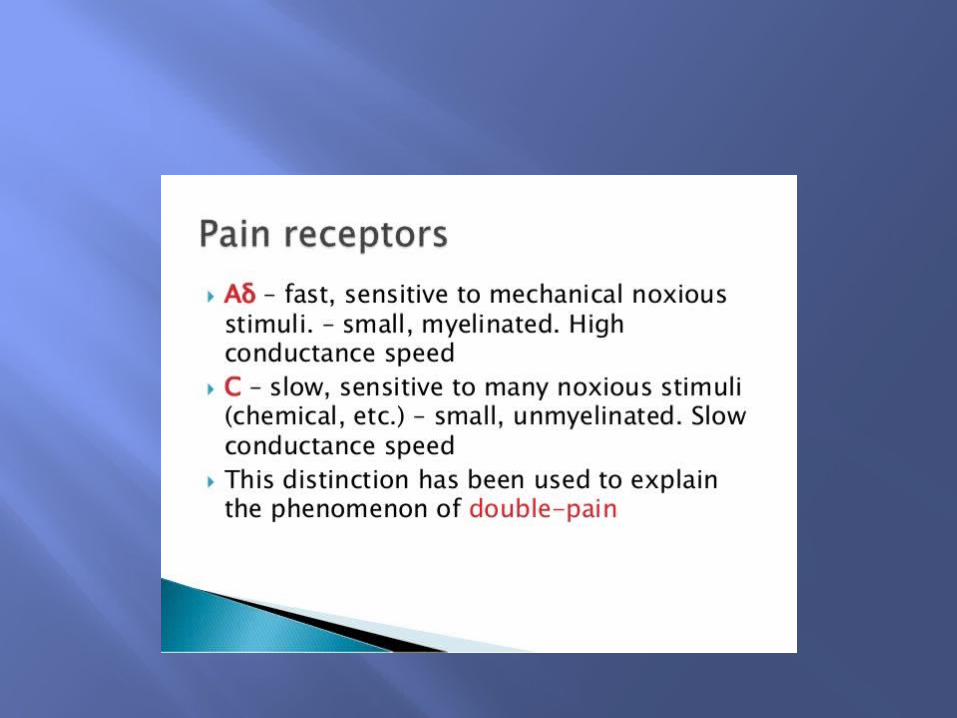
Noxious stimulation is first carried by the faster A-delta fibers and then by the slower C fibers
Local injury can cause nociceptors to become hypersensitive to noxious stimuli, thereby creating a condition called sensitization
Transmission• The process by which impulses
are sent to the dorsal horn of the spinal cord and the brain
• Noxious stimulation is first carried by the faster A-delta fibers and then by the slower C fibers
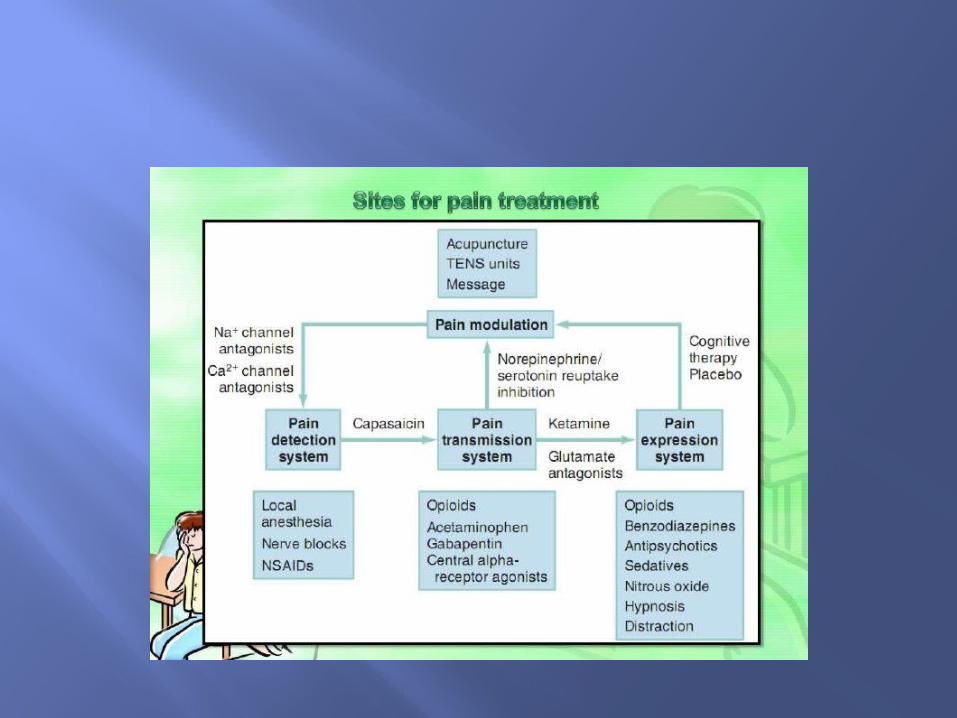
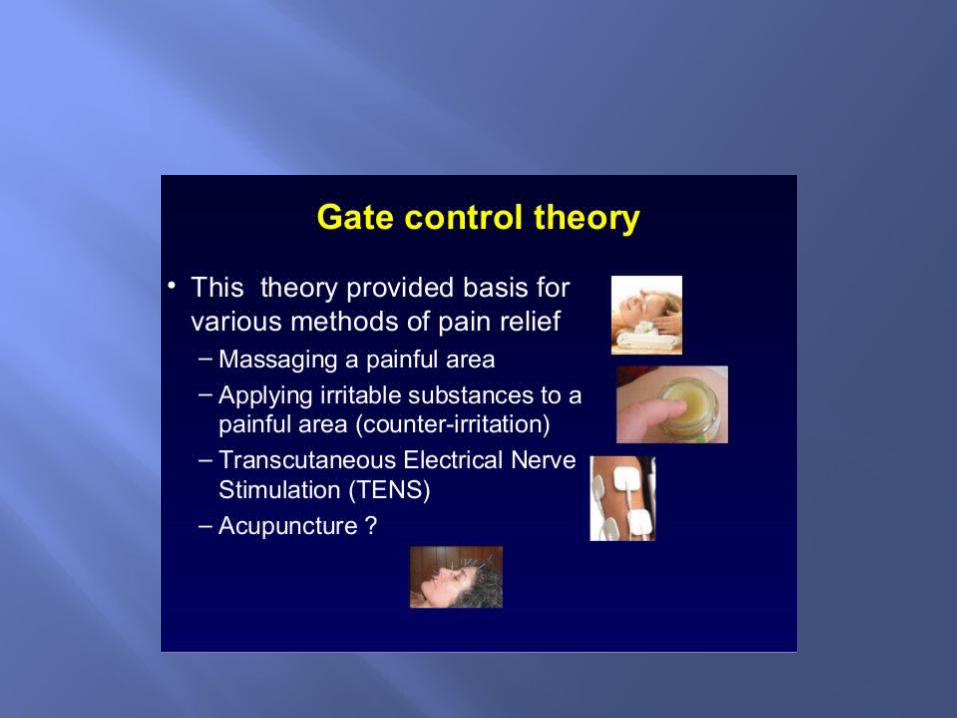
Modulation• The process of dampening or amplifying
pain-related neural signals • A variety of modalities can modulate
these pathways”, including:• Systemic or neuro-axial injection of opioids• Electric stimulation, TENS, Acupuncture,
Massage.• TCA’S, AED’s• Stress, Anxiety• Depression
Perception Refers to the subjective experience of
pain
Results from the interaction of transduction, transmission, modulation
Dependent on the psychological aspects of the individual
Mechanisms of Abnormal Pain
Neuropathic pain is pain due to damaged or dysfunctional nerves The pathophysiology of neuropathic pain can
have both peripheral and central mechanisms
it is doubtful that a single mechanism can account for all cases
The end result is pain that is experienced without evidence of noxious stimulus
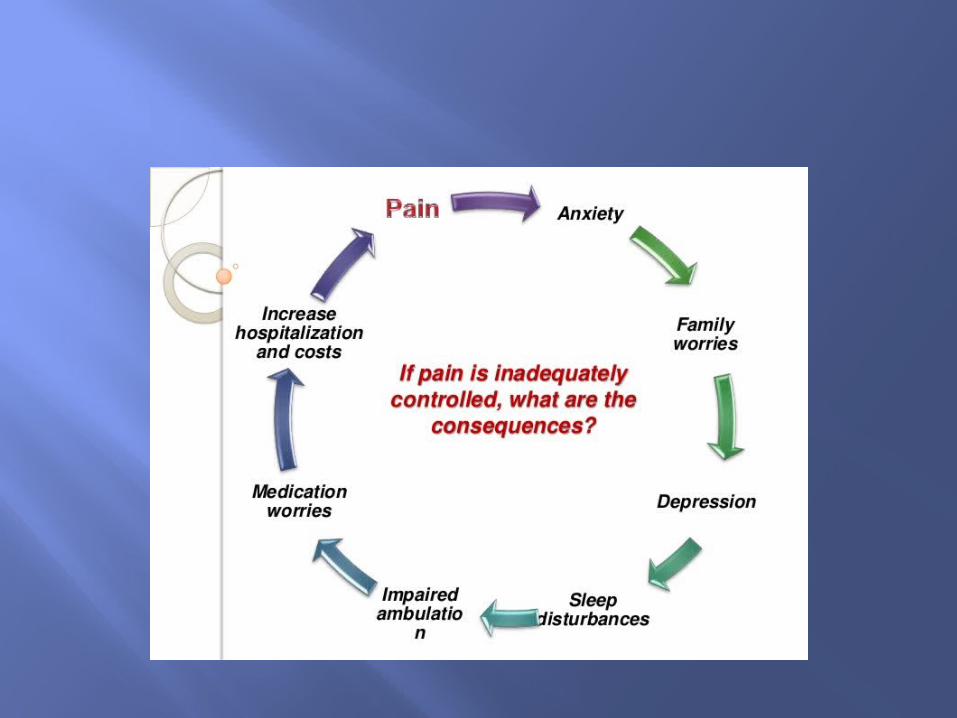
Clinical consequences - Enhanced pain intensity - Enlargement of pain areas - Widespread hyperalgesia - Enhanced disability
Central Hypersensitivity - sensitization of central neural structures
- Dysfunction of endogenous pain modulation
Measuring Central Hypersensitivity
- Psychophysical Assessments - Objective Assessments - Measuring spread of pain and referred
pain areas - Measurement of endogenous
modulation - Measurement of Temporal Summation
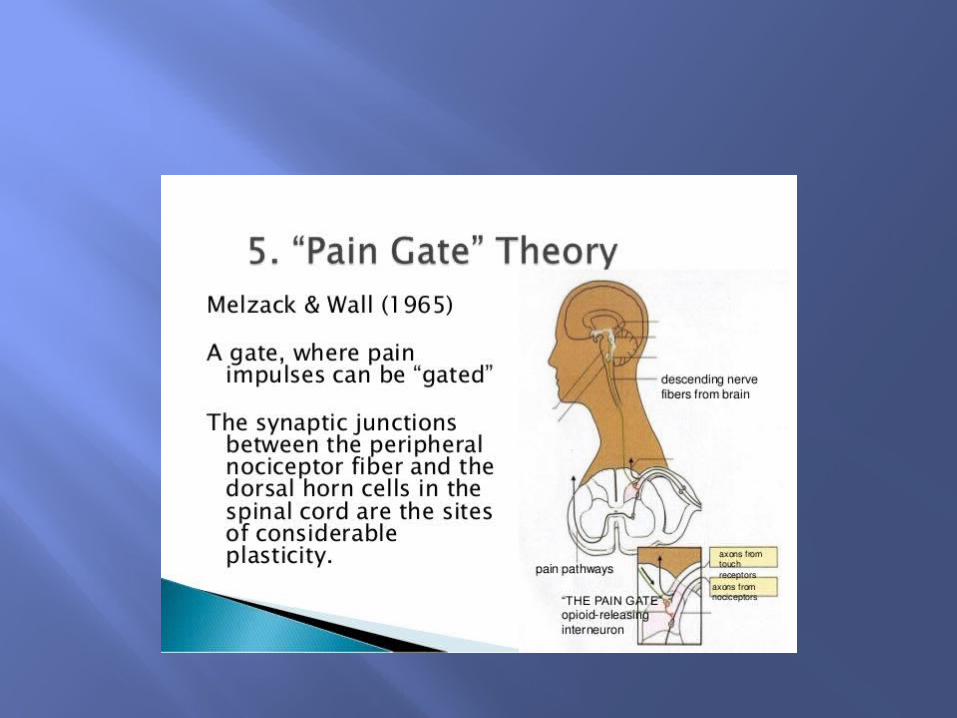
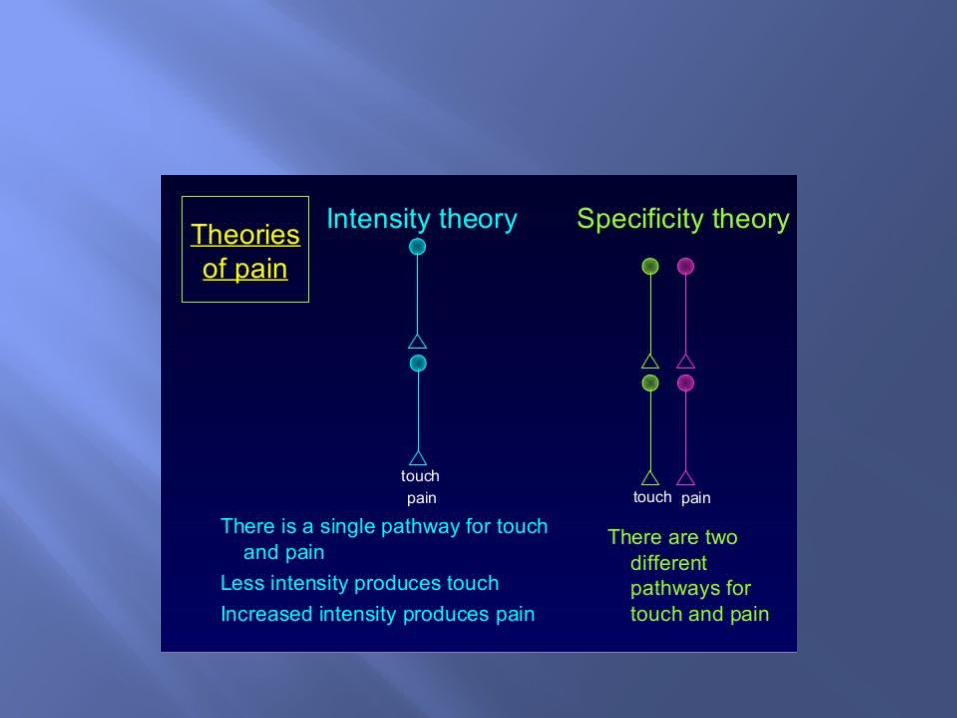
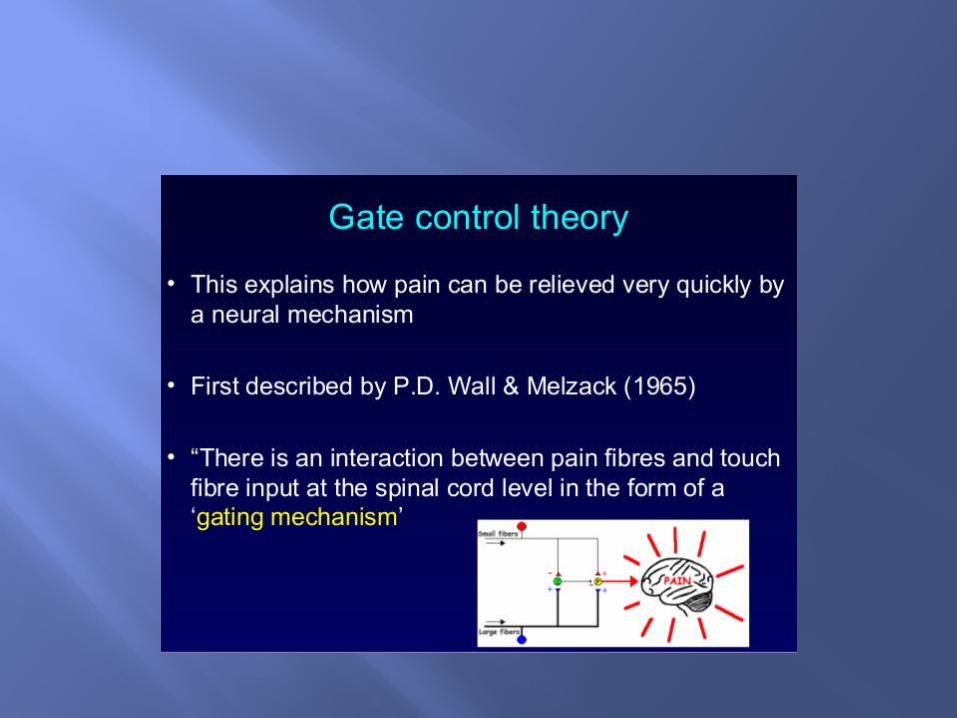
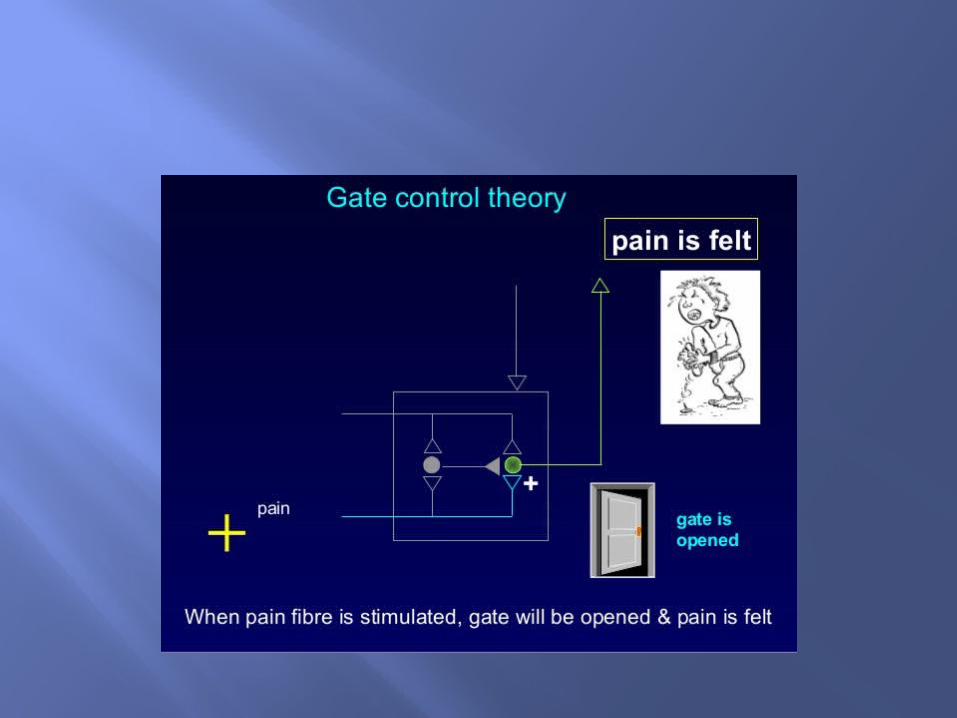
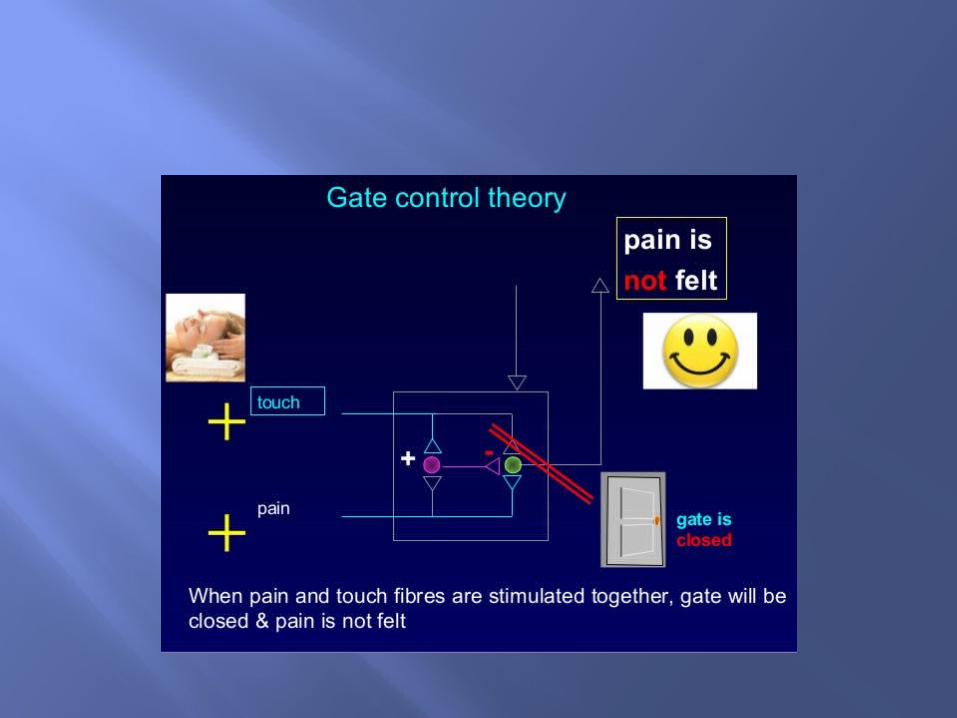
Gate theory
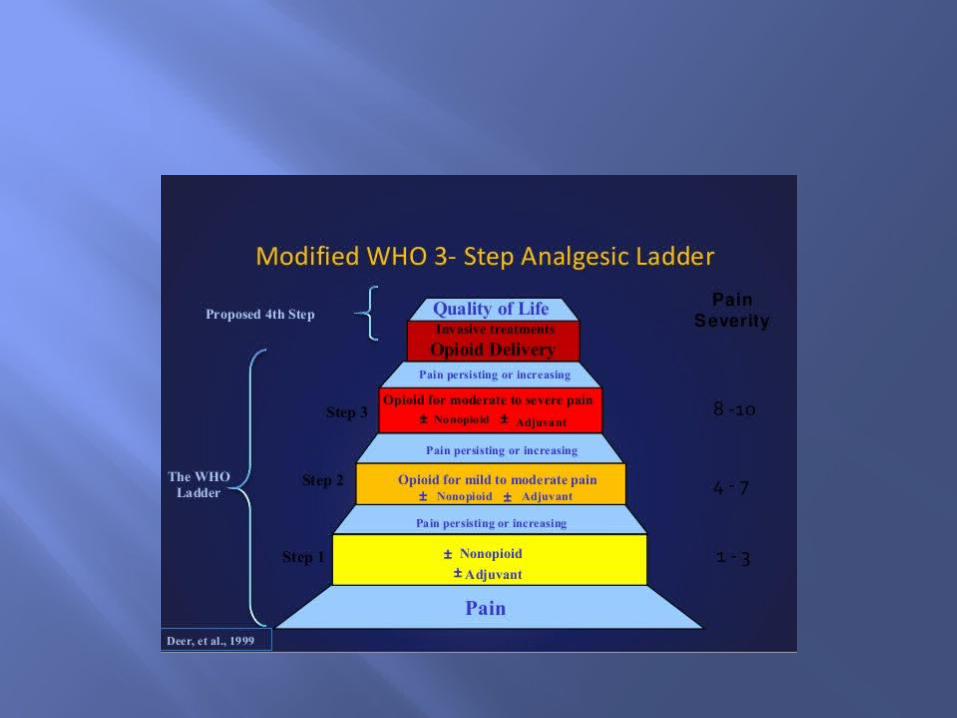
Pain Therapy Approaches Can be classified mostly into 3 broad
groups:- Curative/Disease modifying- Rehabilitative- Palliative
Curative / disease modifying
Simplest and preferred when the identifiable pathophysiological process is present and becomes the target of treatment.
Typically pain should resolve once the underlying process resolves
Examples – ORIF, Appendectomy, Angioplasty for ischemia
Difficult to treat ‘upstream’ pathophysiologic process
Rehabilitative Approach Appropriate when 2 conditions apply - the curative model is not appropriate - major goal of treatment is improving
patient’s ability to function- Examples – multidisciplinary pain rehabilitation (PT, OT, counselling, biofeedback, CAM, vocational rehab, etc.,)
Palliative approach Combination of Medication management
to control pain And/or Less demanding rehabilitative therapies
Pain in Elderly Low levels of pain can cause high
functional impact, depression
Although pain threshold increases with age, tolerance for pain decreases.
Barriers to Pain management in elderly groups
Multiple pain complaints, multiple medical problems, poor communication/under-reporting
Cognitive decline, depression, anxiety, insomnia, fatigue
Poor nutrition, poor tolerance to tests and procedures.
Pain Behaviors Can be more reliable than just pain
reporting, especially in low cognitive patients.
Facial expressions Verbalizations Body movements
Pain behaviors Changes in interpersonal interactions
Changes in activity patterns or routine
Mental status changes
Physiological changes with Aging
Decreased renal function (decrease in glomeruli, decrease in renal excretion, low GFR, higher serum drug levels)
Decreased hepatic function (decreased Cyt.P450 oxidation causing higher serum drug levels
Decreased serum protein, decreased functional binding to proteins – Less unbound drug, increased CNS effect.
Morphine Two metabolites – M3G, M6G (6 is more
active and leads to sedation, as this is renally excreted)
Elimination by hepatic metabolism to glucuronides
T1/2 is 2-4 hrs. may be elevated in elderly up to 15 hrs.
Meperidine Metabolized to normeperidine Not reversible by naloxone This leads to respiratory depression and
excitatory neurotoxicity, anti-cholinergic effects, urinary retention
Blocks reuptake of NE and HT, can cause fatal reaction with concomitant SSRI (Fluoxetine)
Neurological changes
Decreased nerve conduction velocity (loss of myelin on axons, decrease axonal synapses)
Elderly adults rely on C-fiber input when reporting pain ; whereas, younger patients use C and A-delta.
Non-pharmacologic treatments
TENS, heat, acupuncture, relaxation techniques.
Exercise – targeted therapies with realistic achievable goals, should be integrated into daily routine and ADL’s, progress slowly as function and strength improve.
PT / OT , custom adaptive equipment as needed to decrease pain and improve function.
Pharmacologic Treatments ASA Acetaminophen NSAIDS Tramadol Opioids Anti-Depressants Anti-Epileptics Local Anesthetics / Topicals
Non-opioid Medications NSAIDS – exercise caution due to renal,
GI and CV risks Anti-depressants and Anti-convulsants -
adjunctive role in chronic pain especially neuropathic pain states. Dosing limited by side effects
Topical anesthetic / NSAID patches – limited penetration into the tissues, effective only at superficial targets
Opioid managment Equalizing the ‘Pain Pendulum’
‘Balance’ pain relief with risks associated with opioids.
(Not too much…not too little…just enough !!)
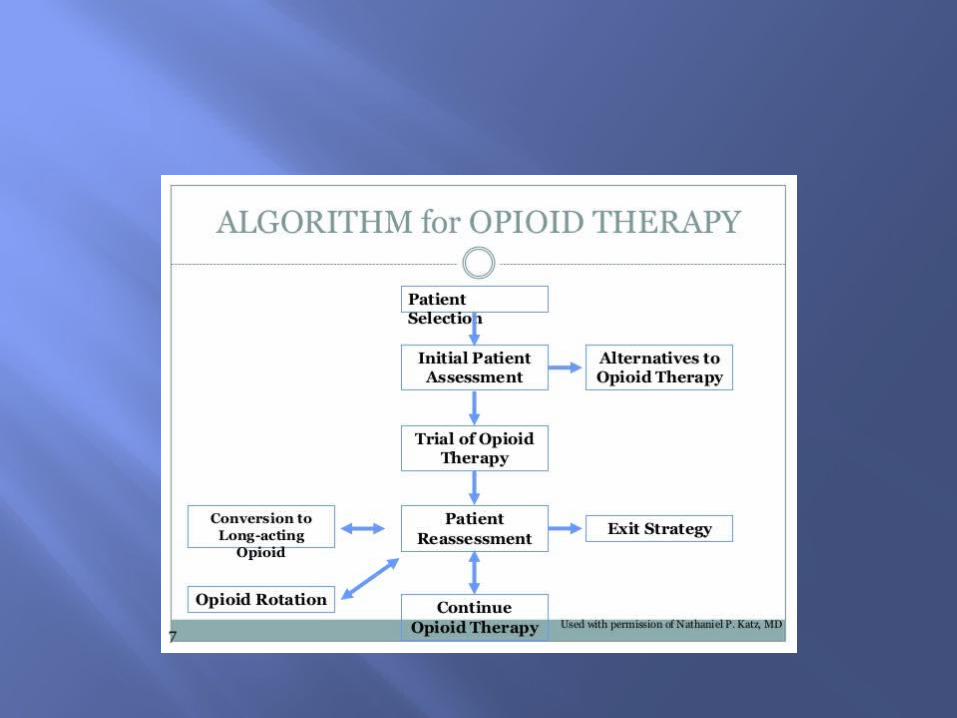
Initiating opioid management
Always administer tools for risk assessment (COMM, DIRE, ORT, SOAPP, SOAPP-R)
Have a clear written agreements / documentation / ‘opioid contract’
All opioid contracts should be simple and written at ‘6th or 7th’ grade level or even lower !
Written consent from patient that ‘contract’ was read and clearly understood by the patient.
Initiating opioid management
Opioid contract/Agreement sets precedence to ‘Rules/responsibilities on patients and reviews risks involved. Not a binding agreement but a good practice for every provider.
Templates of medication agreements can be downloaded from www.SanDiego-SafePrescribing.org
Create function based treatment plans with goals, e.g, begin PT, document improvement in ADL’s and daily routine. Review partner or care-giver input apart from patients self report. Review therapy notes.
Components of treatment plan
Must have a good collaboration between patient and clinician
Apart from pain scores, goals should be realistic, meaningful and verifiable.
Treatment plan should be periodically re-assessed, modified based on goals and functional outcomes
Always have a ‘Exit strategy’ or plan termination that is mutually agreed upon by the patient.
Opioid mechanism of action
works on 3 receptors- mu, kappa, delta. Exerts 3 actions – 1.inhibits transmission
of nociceptive input from the periphery to the spinal cord, 2.activation of descending inhibitory pathways that modulate transmission in the spinal cord (pain “dampening”), 3. Alteration of limbic system activity.
Thus, opioids modify sensory and affective aspects of pain.
Opioid selection Start at lowest possible dose for opioid –
naïve patients – ‘start low go slow’ Opioid tolerant patients – select dose and
medication on case by case basis. When converting from other opioid start at 50% equianalgesic dose and titrate per response.
May use ER/LA therapy alone, SA only, or a combination of ER/LA with a SA opioid.
Recommend not to use more than one SA concurrently.
Opioid selection SA opioids typically have rapid onset (10-60
min) and relatively short duration (2-4 hrs) ER/LA opioids have relatively slow onset
(between 30 to 90 min) and relatively long duration of action (4 to 72 hrs)
Combination with non-opioid adjunctives can be beneficial and can have opioid sparing effects. But monitor for non-opioid drug toxicity.
No ‘ceiling’ effect for opioid analgesic dosing. Selecting ‘Abuse-Deterrent’ formulations may
minimize the opioid abuse.
Opioids Phenanthrene (Morphine, codeine,
Thebaine, Papaveretum)
Semi-synthetic (hydrocodone, hydromorphone, oxycodone, oxymorphone)
Synthetic (Fentanyl, Demerol, methadone)
Opioid partial Antagonist / Agonist
Buprenorphine
Butorphanol
Nalbuphine
Opioid Receptors 3 principal classes - Mu 1, 2, 3 . 1-supraspinal analgesia . 2-respiratory depression, physical
dependence
-Kappa . Sedation, spinal analgesia
Delta – Anti-depressant, dependence, Analgesia
opioids Morphine dose is used as a ‘standard’ for
dose comparison of other opioids. Morphine equivalent daily dose (MEDD)
Recommend not to exceed >100 mg/day MEDD
exercise caution with morphine and Demerol use in renal insufficiency patients. Most other opioids eliminated by hepatic metabolism.
Codeine is a prodrug and not all patients convert it to an active form.
Opioids When treating chronic pain with opioids,
also be prepared to proactively treat side effects.
Common side effects include respiratory depression, sedation, mental clouding or confusion, nausea, vomiting, constipation, pruritus and urinary retention.
Side effects tend to subside with time with the “exception” of Constipation.
Opioid monitoring Periodic urine drug screens (should be
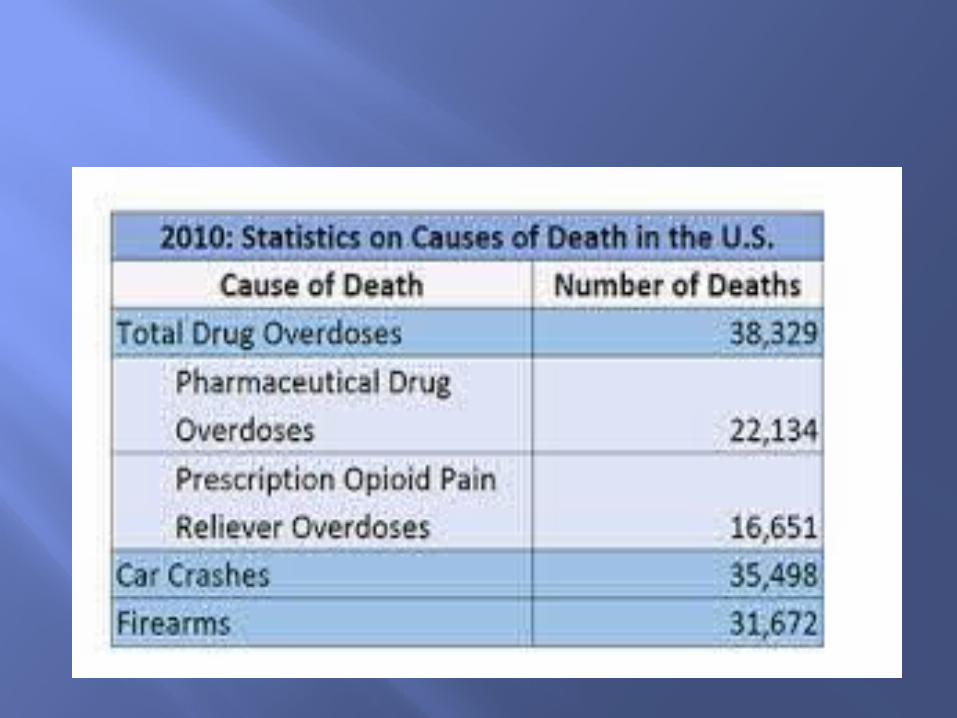
performed for the duration of COT) 244 un-intentional Rx drug related deaths in San Diego county in 2014, 5723 ER
discharges related to pain killers in 2013
Utilizing ‘CURES’/PDMP system for monitoring and surveillance (CONTROLLED SUBSTANCE UTILIZATION REVIEW AND EVALUATION SYSTEM). Register by Jan 1st, 2016.
Can complete registration online at https://pmp.doj.ca.gov/pmpreg
Perform Pill counts at each visit, especially in high risk patients.
Introduction July 2012, FDA released ‘final’ guidelines
to REMS for ER/LA formulations.
2014-2015 – Government move to initiate an action plan to formulate ‘National Pain Strategy’(NPS)
Opioid monitoring Urine drug screens typically done every
1-3 months. More frequently done in high risk
patients, e.g, Prior history of addiction, past abuse, aberrant behavior, occupations
demanding mental acuity, elderly, unstable or dysfunctional social environment, comorbid psychiatric or medical conditions
Sometimes daily or weekly monitoring may be necessary for patients at very high risk of adverse outcomes.
Urine specimens can be adulterated and should be aware.
Oral swab tests more easy to administer and can be more valuable than urine drug screens.
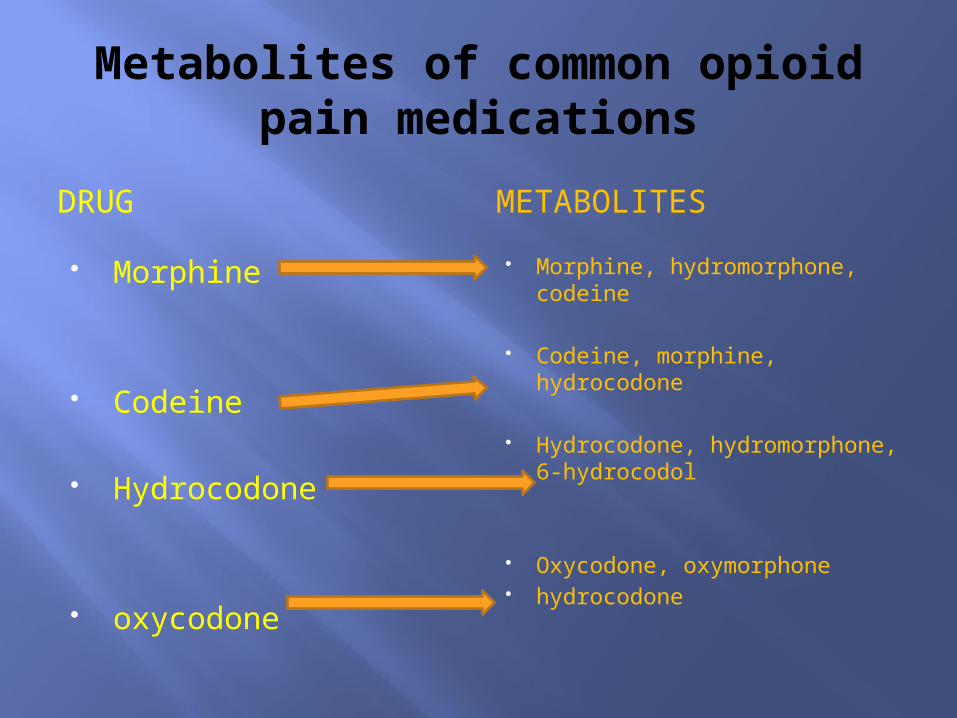
Metabolites of common opioid pain medications
DRUG METABOLITES Morphine
Codeine
Hydrocodone
oxycodone
Morphine, hydromorphone, codeine
Codeine, morphine, hydrocodone
Hydrocodone, hydromorphone, 6-hydrocodol
Oxycodone, oxymorphone hydrocodone
Opioid monitoring Screen for hypogonadism in patients on
COT, especially with signs and symptoms of fatigue, mood changes, decreased libido, loss of muscle mass and osteoporosis.
Perform opioid rotation if lack of efficacy, side-effects of one opioid class, altered pharmaco-kinetics, changes in absorption.
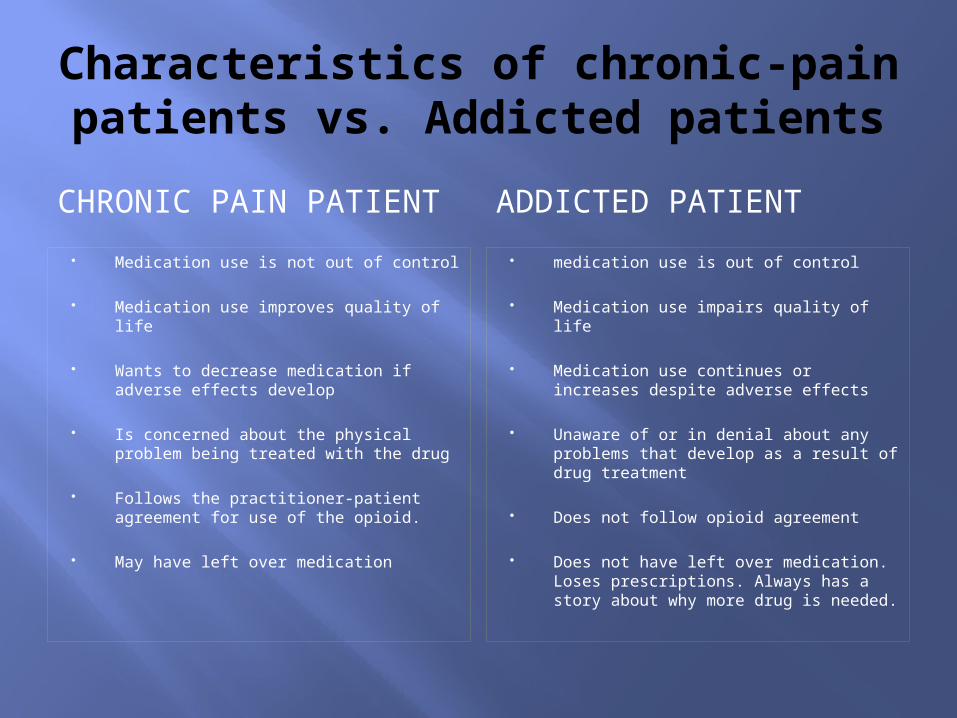
Characteristics of chronic-pain patients vs. Addicted patients
CHRONIC PAIN PATIENT ADDICTED PATIENT Medication use is not out of control
Medication use improves quality of life
Wants to decrease medication if adverse effects develop
Is concerned about the physical problem being treated with the drug
Follows the practitioner-patient agreement for use of the opioid.
May have left over medication
medication use is out of control
Medication use impairs quality of life
Medication use continues or increases despite adverse effects
Unaware of or in denial about any problems that develop as a result of drug treatment
Does not follow opioid agreement
Does not have left over medication. Loses prescriptions. Always has a story about why more drug is needed.
Pain Tolerance – decreased efficacy over time Dependence – tolerance +withdrawal
symptoms Addiction – ‘neurobiological disease’.
Strong genetic influence. Preoccupied with continued use despite harm
Pseudoaddiction – happens when pain is undertreated. “drug seeking” or “clock watching”. Usually resolves with effective pain management.
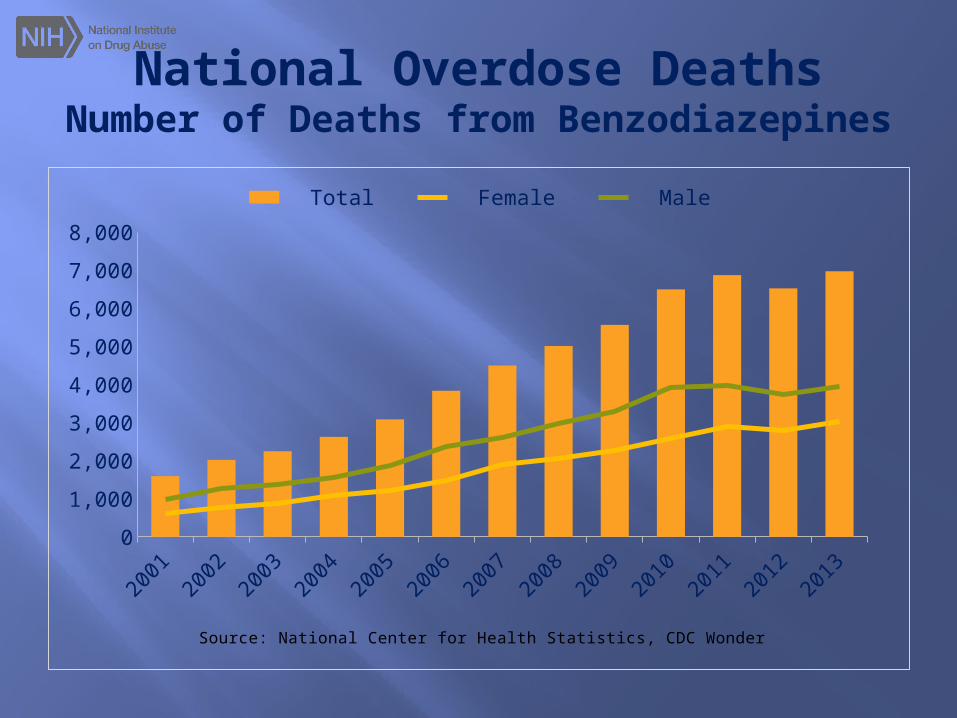
National Overdose DeathsNumber of Deaths from Benzodiazepines
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
01,0002,0003,0004,0005,0006,0007,0008,000
Total Female Male
Source: National Center for Health Statistics, CDC Wonder
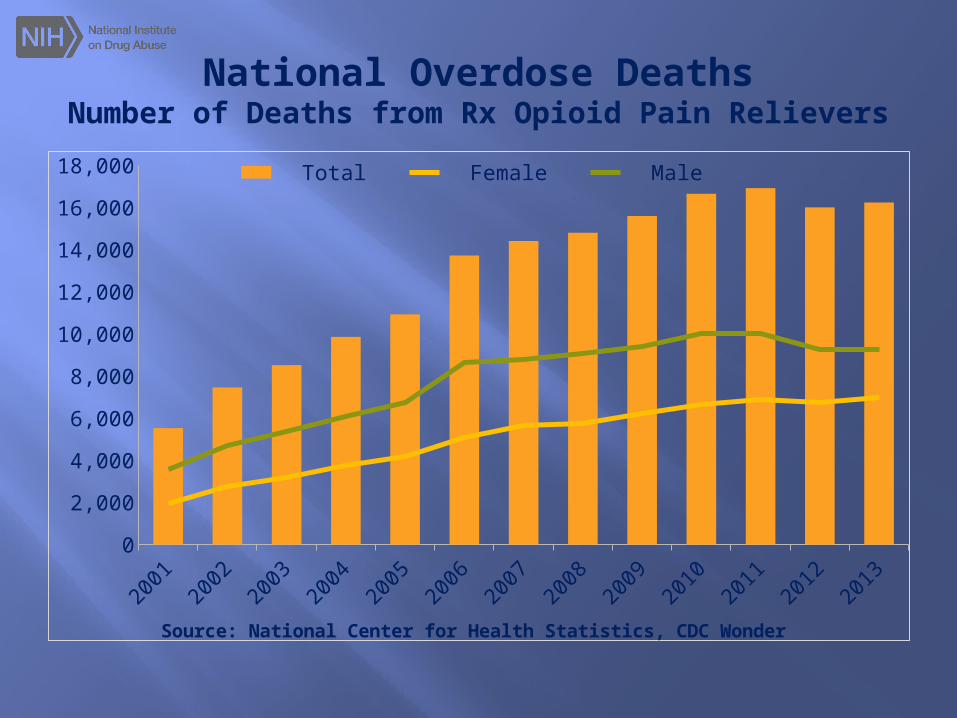
National Overdose DeathsNumber of Deaths from Rx Opioid Pain Relievers
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
02,0004,0006,0008,000
10,00012,00014,00016,00018,000 Total Female Male
Source: National Center for Health Statistics, CDC Wonder
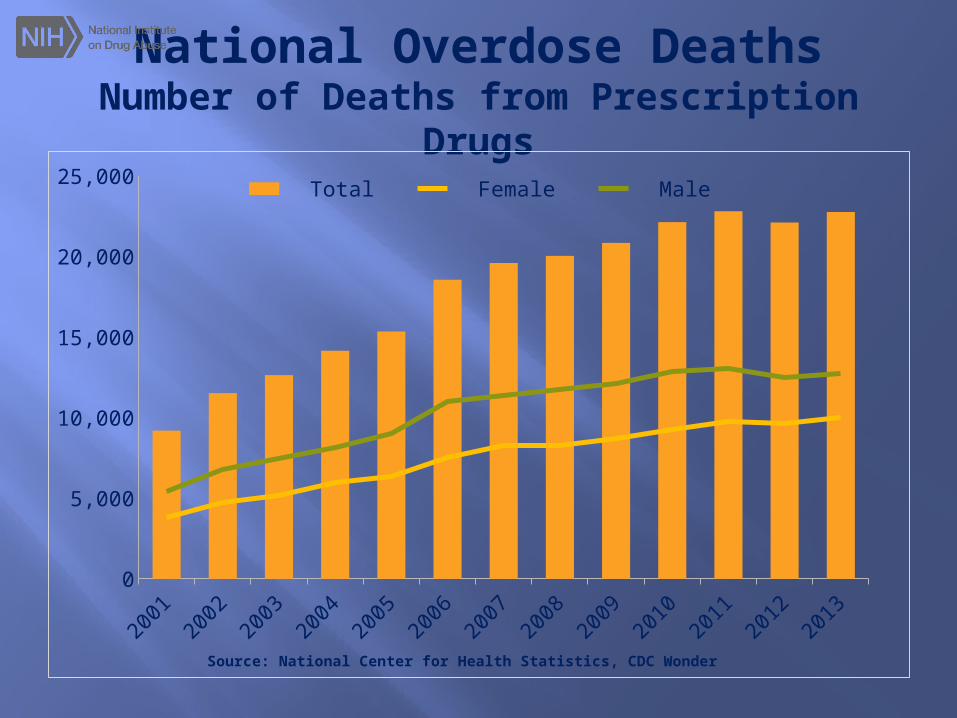
National Overdose DeathsNumber of Deaths from Prescription
Drugs
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
0
5,000
10,000
15,000
20,000
25,000 Total Female Male
Source: National Center for Health Statistics, CDC Wonder
Opioid treatment termination
Reasons to terminate may include (healing or recovery from the treatment condition, intolerable side-effects, lack of response, discovery of abuse or misuse or addiction)
Typically 10% dose reduction per week. Slower taper will minimize unpleasant withdrawal symptoms.
Clonidine can be used. 0.1 – 0.2mg PO every 6 hrs daily or patch at 0.1mg/24 hours.
Drug rehab - Methadone
Opioid overdose Respiratory depression usually preceded
by warning signs and can be prevented with careful monitoring
Take home Naloxone Rx for patients with high risk for overdose
. In 2014 FDA approved hand held auto-injector (Evzio) and can be used at home by family members or caregivers.
Methadone Mu-1 agonist and NMDA antagonist Analgesic duration of 4-6 hrs Elimination t1/2 15-60 hrs Can cause QT prolongation, Torsade de
pointes
Methadone Has been long used to treat addiction. Long plasma elimination half life,
relatively short analgesic half life makes it optimal for maintenance.
Has opioid and non-opioid receptor effects causing varied effects – ‘Broad spectrum opioid’
Metabolized by liver enzymes that differ from those associated with most other opioids, leading to drug-drug interactions.
methadone Significant genetic variations in the liver
enzymes that metabolize methadone Metabolism effected by cigarette smoking
and alcohol consumption. Lowest possible dose titration should be
followed even for opioid tolerant patients.
Rx to be ‘Pain-free’
Important Principles to remember
1 provider and 1 pharmacy for all controlled substances
Use CURES/PDMP Use medication agreements when
prescribing ‘COT’ Don’t mix opioids and CNS
depressants/sedatives. Monitor polypharmacy
Implement multidisciplinary approach to treat chronic pain.

THANK YOU !


















