(2014) Revised Parkinson's Drugs Handout
22
1 PARKINSON'S DISEASE Parkinson's disease (PD) is a progressive neurological disorder that results from degeneration of neurons in the neostriatum. This degeneration creates a shortage of dopamine, causing the movement impairments that characterize the disease, The condition affects about 1 to 2 percent of people over the age of 60 years and the chance of developing PD increases as we age. HISTORY Parkinson's disease was first formally described in "An Essay on the Shaking Palsy," published in 1817 by a London physician named James Parkinson, but it has probably existed for many thousands of years. Its symptoms and potential therapies were mentioned in the Ayurveda, the system of medicine practiced in India as early as 5000 BC, and in the first Chinese medical text, Nei Jing, which appeared 2500 years ago. In the early 1960s, scientists identified the primary problem underlying the disease: the loss of brain cells that produce dopamine. This discovery led to the first successful treatment for PD and suggested ways of devising new and even more effective therapies. ETIOLOGY A. Genetics Until relatively recently, Parkinson disease was not though to be heritable, and research was primarily focused on environmental risk factors such as viral infection or neurotoxins, However, a positive family history was gradually perceived to be a risk factor, a view that was confirmed last year (2003) when a candidate gene for some cases of Parkinson disease was mapped to chromosome 4. Mutations in this gene have now been linked to several Parkinson disease families. The product of this gene is the protein called alpha-synucIein. The finding was published online by Neuron on October 22, 2004. The collaborative work was spearheaded by National Institute on Aging (USA), The Institut de Biomedicina (Spain), and The Institute of Neurology in London. B. Environmental Factors Although the importance of genetics in PD is increasingly recognized, many researchers still believe that environmental exposures also increase a person's risk of developing the disease. Even when genes are a factor in the disease, as with many familial cases, exposure to toxins or other environmental factors may influence when symptoms of the disease appear and/or how the disease progresses.
-
Upload
suneil-r-als -
Category
Documents
-
view
9 -
download
0
Transcript of (2014) Revised Parkinson's Drugs Handout

1
PARKINSON'S DISEASE Parkinson's disease (PD) is a progressive neurological disorder that results from degeneration of neurons in the neostriatum. This degeneration creates a shortage of dopamine, causing the movement impairments that characterize the disease, The condition affects about 1 to 2 percent of people over the age of 60 years and the chance of developing PD increases as we age. HISTORY
Parkinson's disease was first formally described in "An Essay on the Shaking Palsy," published in 1817 by a London physician named James Parkinson, but it has probably existed for many thousands of years. Its symptoms and potential therapies were mentioned in the Ayurveda, the system of medicine practiced in India as early as 5000 BC, and in the first Chinese medical text, Nei Jing, which appeared 2500 years ago. In the early 1960s, scientists identified the primary problem underlying the disease: the loss of brain cells that produce dopamine. This discovery led to the first successful treatment for PD and suggested ways of devising new and even more effective therapies.
ETIOLOGY A. Genetics Until relatively recently, Parkinson disease was not though to be heritable, and research was primarily focused on environmental risk factors such as viral infection or neurotoxins, However, a positive family history was gradually perceived to be a risk factor, a view that was confirmed last year (2003) when a candidate gene for some cases of Parkinson disease was mapped to chromosome 4. Mutations in this gene have now been linked to several Parkinson disease families. The product of this gene is the protein called alpha-synucIein. The finding was published online by Neuron on October 22, 2004. The collaborative work was spearheaded by National Institute on Aging (USA), The Institut de Biomedicina (Spain), and The Institute of Neurology in London. B. Environmental Factors Although the importance of genetics in PD is increasingly recognized, many researchers still believe that environmental exposures also increase a person's risk of developing the disease. Even when genes are a factor in the disease, as with many familial cases, exposure to toxins or other environmental factors may influence when symptoms of the disease appear and/or how the disease progresses.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
2
One of the primary pieces of evidence that environmental factors play a role in the development of PD is that the relative risk of the disease is higher in industrialized countries than in less industrialized ones. In addition, studies have found that farmers and other agricultural workers have an increased risk of developing PD.
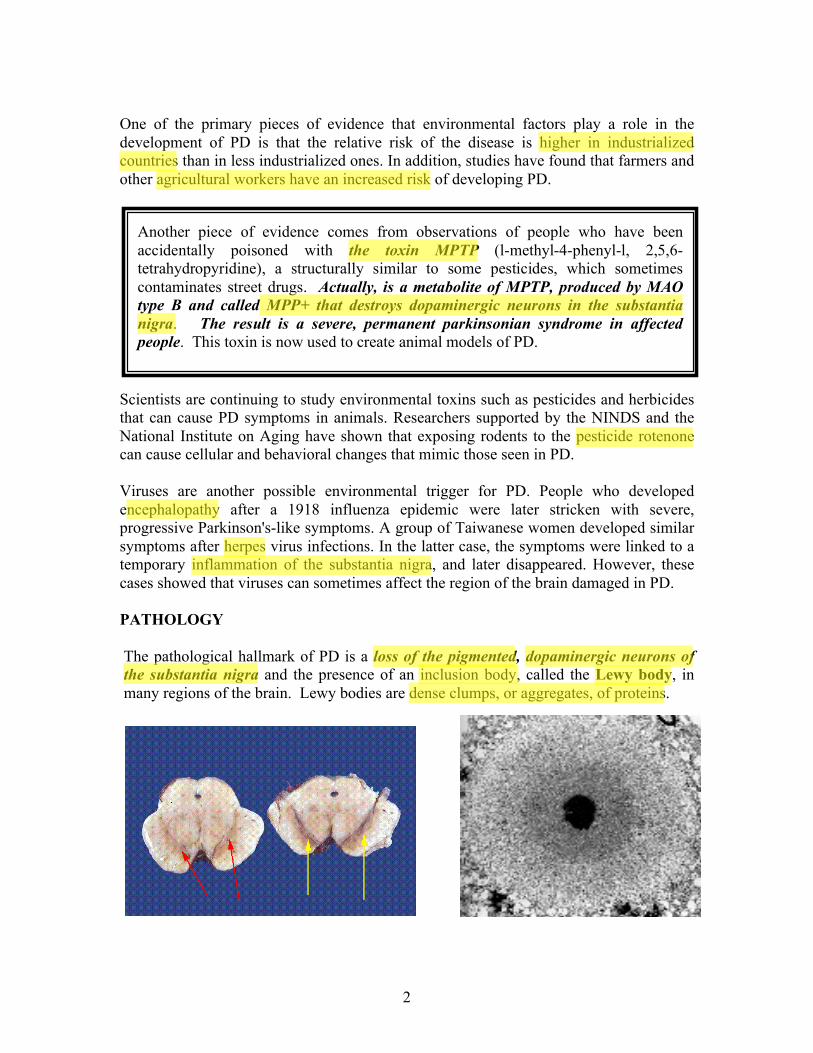
Scientists are continuing to study environmental toxins such as pesticides and herbicides that can cause PD symptoms in animals. Researchers supported by the NINDS and the National Institute on Aging have shown that exposing rodents to the pesticide rotenone can cause cellular and behavioral changes that mimic those seen in PD. Viruses are another possible environmental trigger for PD. People who developed encephalopathy after a 1918 influenza epidemic were later stricken with severe, progressive Parkinson's-like symptoms. A group of Taiwanese women developed similar symptoms after herpes virus infections. In the latter case, the symptoms were linked to a temporary inflammation of the substantia nigra, and later disappeared. However, these cases showed that viruses can sometimes affect the region of the brain damaged in PD. PATHOLOGY The pathological hallmark of PD is a loss of the pigmented, dopaminergic neurons of the substantia nigra and the presence of an inclusion body, called the Lewy body, in many regions of the brain. Lewy bodies are dense clumps, or aggregates, of proteins.
Another piece of evidence comes from observations of people who have been accidentally poisoned with the toxin MPTP (l-methyl-4-phenyl-l, 2,5,6-tetrahydropyridine), a structurally similar to some pesticides, which sometimes contaminates street drugs. Actually, is a metabolite of MPTP, produced by MAO type B and called MPP+ that destroys dopaminergic neurons in the substantia nigra. The result is a severe, permanent parkinsonian syndrome in affected people. This toxin is now used to create animal models of PD.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
3
Another cellular characteristic of PD is the presence of Lewy neurites - swollen nerve fibers containing alpha-synuclein and other proteins. The accumulation of alphasynuclein in these nerve fibers may interfere with transmission of nerve signals or other important neuronal functions.
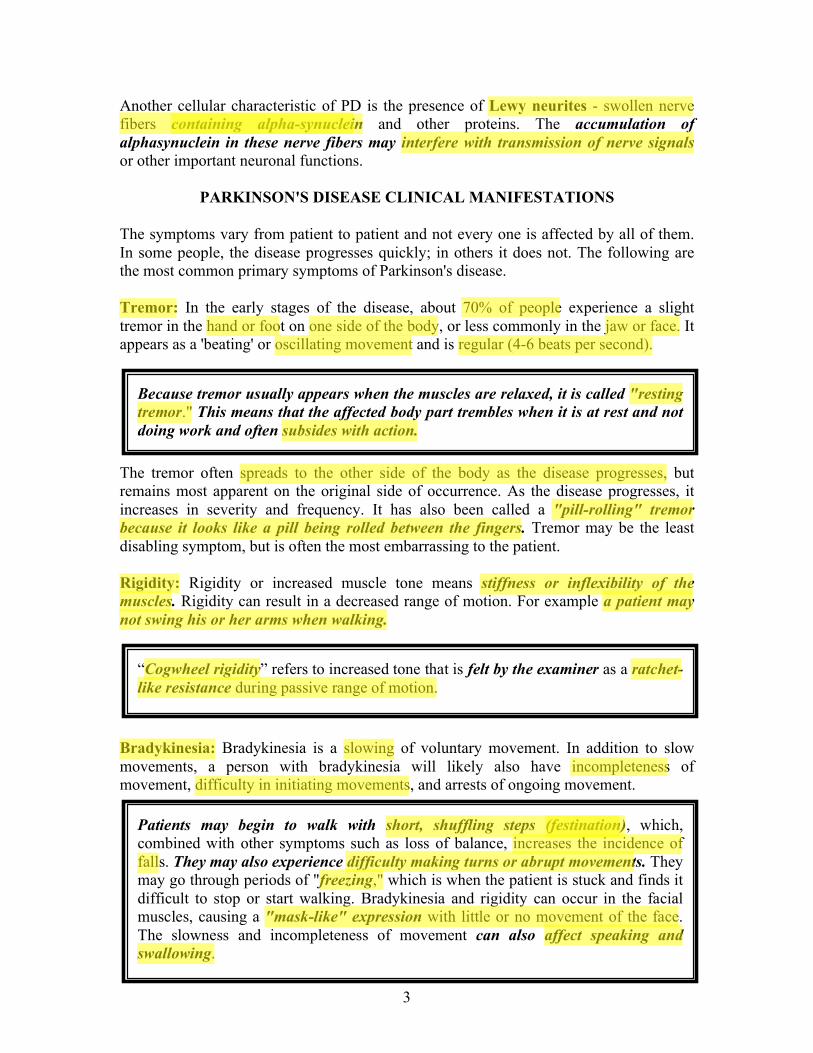
PARKINSON'S DISEASE CLINICAL MANIFESTATIONS The symptoms vary from patient to patient and not every one is affected by all of them. In some people, the disease progresses quickly; in others it does not. The following are the most common primary symptoms of Parkinson's disease. Tremor: In the early stages of the disease, about 70% of people experience a slight tremor in the hand or foot on one side of the body, or less commonly in the jaw or face. It appears as a 'beating' or oscillating movement and is regular (4-6 beats per second).
The tremor often spreads to the other side of the body as the disease progresses, but remains most apparent on the original side of occurrence. As the disease progresses, it increases in severity and frequency. It has also been called a "pill-rolling" tremor because it looks like a pill being rolled between the fingers. Tremor may be the least disabling symptom, but is often the most embarrassing to the patient. Rigidity: Rigidity or increased muscle tone means stiffness or inflexibility of the muscles. Rigidity can result in a decreased range of motion. For example a patient may not swing his or her arms when walking.
Bradykinesia: Bradykinesia is a slowing of voluntary movement. In addition to slow movements, a person with bradykinesia will likely also have incompleteness of movement, difficulty in initiating movements, and arrests of ongoing movement.
Because tremor usually appears when the muscles are relaxed, it is called "resting tremor." This means that the affected body part trembles when it is at rest and not doing work and often subsides with action.
“Cogwheel rigidity” refers to increased tone that is felt by the examiner as a ratchet-like resistance during passive range of motion.
Patients may begin to walk with short, shuffling steps (festination), which, combined with other symptoms such as loss of balance, increases the incidence of falls. They may also experience difficulty making turns or abrupt movements. They may go through periods of "freezing," which is when the patient is stuck and finds it difficult to stop or start walking. Bradykinesia and rigidity can occur in the facial muscles, causing a "mask-like" expression with little or no movement of the face. The slowness and incompleteness of movement can also affect speaking and swallowing.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight

4
Postural Instability: The unsteadiness with walking and turning, as well as occasional falls in Parkinson's disease patients is due in part to the postural instability. A patient suffering from mildly impaired postural mechanisms will recover by stepping back one or two paces after being nudged at the sternum. After a sternal nudge, a more disabled patient will attempt to recover by stepping backwards, however they will continue in this fashion until they either fall or hit something (called retropulsion). An extremely disabled patient, being extremely rigid, may fall back straight as a board, without any attempt at recovery, When the patient reaches end-stage, they are not able to stand without assistance.
PATHOPHYSIOLOGY It is a chronic, progressive disease that results when nerve cells in the substantia nigra, die or are impaired. These nerve cells produce dopamine that transmits signals from the substantia nigra to the corpus striatum. These signals allow for coordinated movement. When the dopamine-secreting cells in the substantia nigra die, the other movement control centers in the brain become unregulated. When 80% of the dopamine-producing cells in the substantia nigra are depleted, symptoms of PD develop. In Parkinson’s disease the loss of dopamine on both the Direct and Indirect Pathways in combination with a predominance of Ach actions in interneurons results in a reduction in the activity of VA/VL and, in turn, motor cortical neurons. This explains the hypokinetic symptoms seen in this neurological disease.
A normally pigmented substantia nigra is seen in the midbrain on the right but the midbrain on the left from the patient with Parkinson's disease shows a pale substantia nigra. As the pigmented nigral cells degenerate, the neuromelanin is dispersed and taken up by macrophages; thus, one of the diagnostic histopathologic hallmarks of PD is DEPIGMENTATION of the substantia nigra.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
5
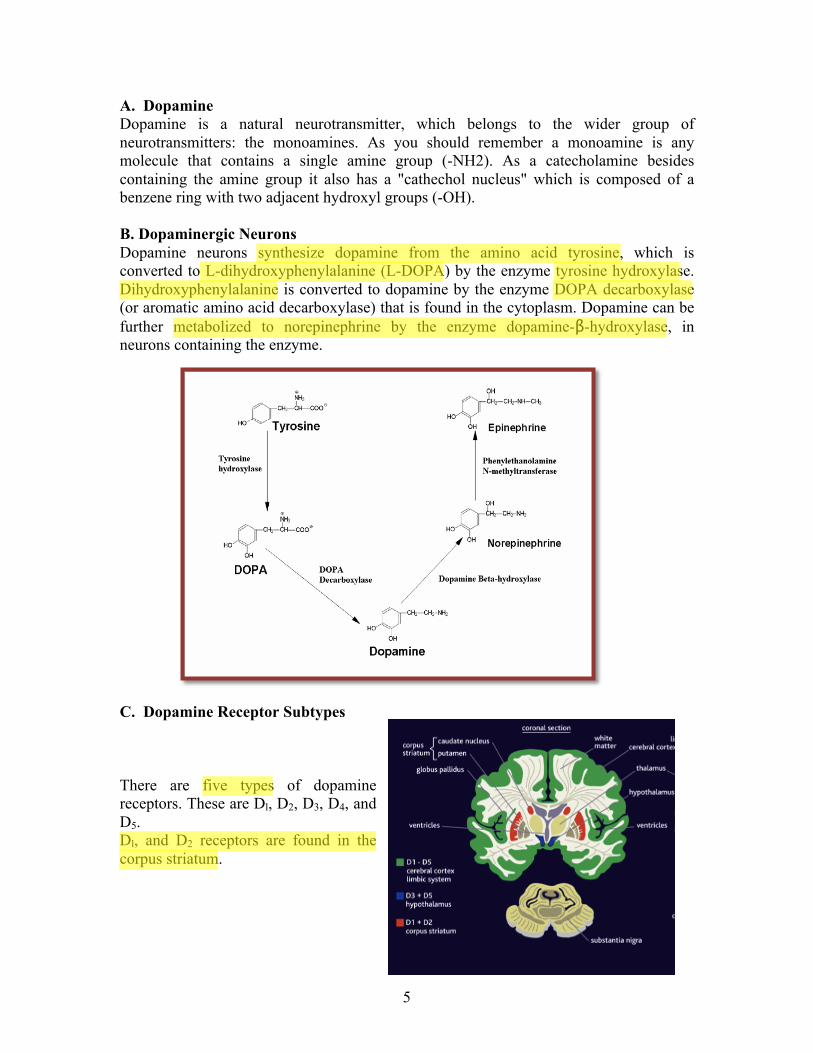
A. Dopamine Dopamine is a natural neurotransmitter, which belongs to the wider group of neurotransmitters: the monoamines. As you should remember a monoamine is any molecule that contains a single amine group (-NH2). As a catecholamine besides containing the amine group it also has a "cathechol nucleus" which is composed of a benzene ring with two adjacent hydroxyl groups (-OH). B. Dopaminergic Neurons Dopamine neurons synthesize dopamine from the amino acid tyrosine, which is converted to L-dihydroxyphenylalanine (L-DOPA) by the enzyme tyrosine hydroxylase. Dihydroxyphenylalanine is converted to dopamine by the enzyme DOPA decarboxylase (or aromatic amino acid decarboxylase) that is found in the cytoplasm. Dopamine can be further metabolized to norepinephrine by the enzyme dopamine-β-hydroxylase, in neurons containing the enzyme. C. Dopamine Receptor Subtypes There are five types of dopamine receptors. These are Dl, D2, D3, D4, and D5. Dl, and D2 receptors are found in the corpus striatum.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
6
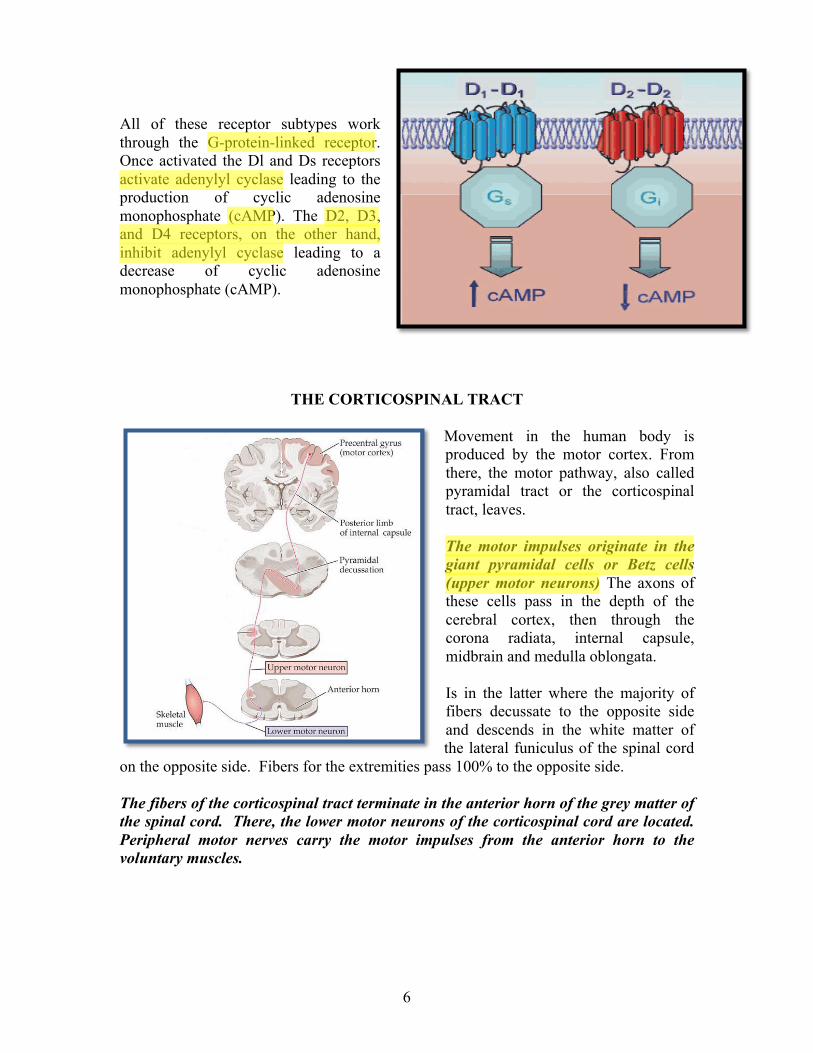
All of these receptor subtypes work through the G-protein-linked receptor. Once activated the Dl and Ds receptors activate adenylyl cyclase leading to the production of cyclic adenosine monophosphate (cAMP). The D2, D3, and D4 receptors, on the other hand, inhibit adenylyl cyclase leading to a decrease of cyclic adenosine monophosphate (cAMP).
THE CORTICOSPINAL TRACT
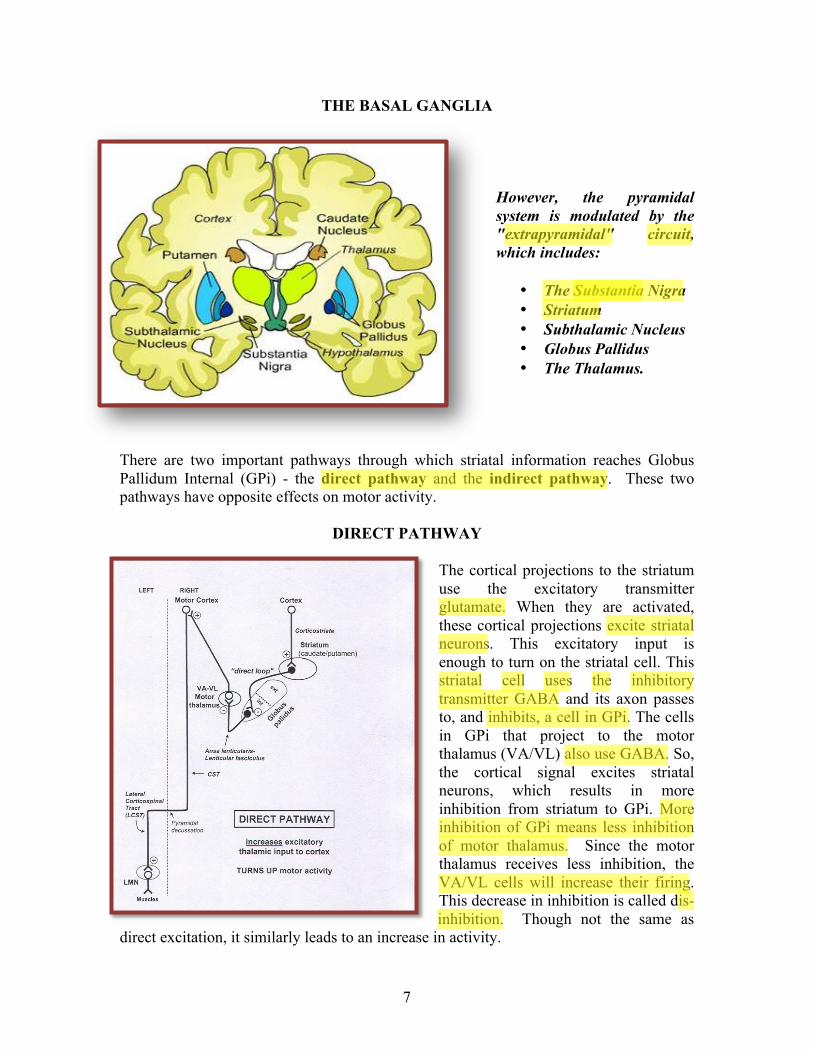
Movement in the human body is produced by the motor cortex. From there, the motor pathway, also called pyramidal tract or the corticospinal tract, leaves. The motor impulses originate in the giant pyramidal cells or Betz cells (upper motor neurons) The axons of these cells pass in the depth of the cerebral cortex, then through the corona radiata, internal capsule, midbrain and medulla oblongata. Is in the latter where the majority of fibers decussate to the opposite side and descends in the white matter of the lateral funiculus of the spinal cord
on the opposite side. Fibers for the extremities pass 100% to the opposite side. The fibers of the corticospinal tract terminate in the anterior horn of the grey matter of the spinal cord. There, the lower motor neurons of the corticospinal cord are located. Peripheral motor nerves carry the motor impulses from the anterior horn to the voluntary muscles.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
7
THE BASAL GANGLIA
However, the pyramidal system is modulated by the "extrapyramidal" circuit, which includes:
• The Substantia Nigra • Striatum • Subthalamic Nucleus • Globus Pallidus • The Thalamus.
There are two important pathways through which striatal information reaches Globus Pallidum Internal (GPi) - the direct pathway and the indirect pathway. These two pathways have opposite effects on motor activity.
DIRECT PATHWAY The cortical projections to the striatum use the excitatory transmitter glutamate. When they are activated, these cortical projections excite striatal neurons. This excitatory input is enough to turn on the striatal cell. This striatal cell uses the inhibitory transmitter GABA and its axon passes to, and inhibits, a cell in GPi. The cells in GPi that project to the motor thalamus (VA/VL) also use GABA. So, the cortical signal excites striatal neurons, which results in more inhibition from striatum to GPi. More inhibition of GPi means less inhibition of motor thalamus. Since the motor thalamus receives less inhibition, the VA/VL cells will increase their firing. This decrease in inhibition is called dis-inhibition. Though not the same as
direct excitation, it similarly leads to an increase in activity.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
8
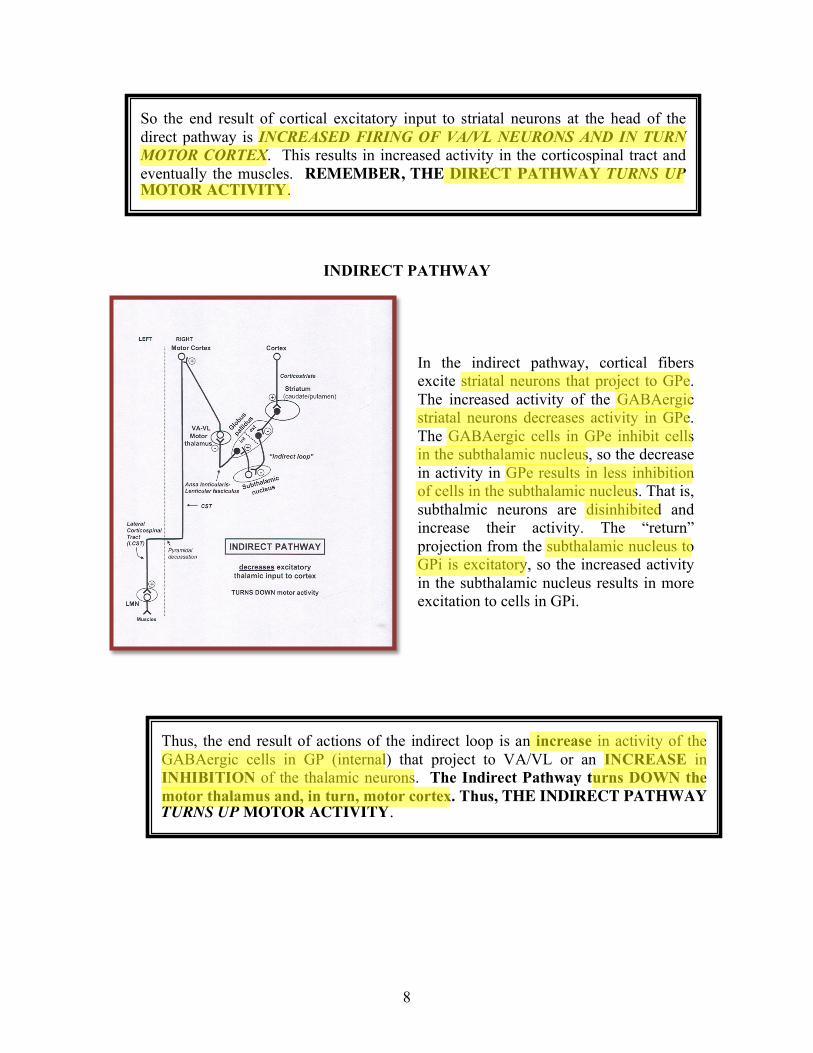
INDIRECT PATHWAY In the indirect pathway, cortical fibers excite striatal neurons that project to GPe. The increased activity of the GABAergic striatal neurons decreases activity in GPe. The GABAergic cells in GPe inhibit cells in the subthalamic nucleus, so the decrease in activity in GPe results in less inhibition of cells in the subthalamic nucleus. That is, subthalmic neurons are disinhibited and increase their activity. The “return” projection from the subthalamic nucleus to GPi is excitatory, so the increased activity in the subthalamic nucleus results in more excitation to cells in GPi.
So the end result of cortical excitatory input to striatal neurons at the head of the direct pathway is INCREASED FIRING OF VA/VL NEURONS AND IN TURN MOTOR CORTEX. This results in increased activity in the corticospinal tract and eventually the muscles. REMEMBER, THE DIRECT PATHWAY TURNS UP MOTOR ACTIVITY.
Thus, the end result of actions of the indirect loop is an increase in activity of the GABAergic cells in GP (internal) that project to VA/VL or an INCREASE in INHIBITION of the thalamic neurons. The Indirect Pathway turns DOWN the motor thalamus and, in turn, motor cortex. Thus, THE INDIRECT PATHWAY TURNS UP MOTOR ACTIVITY.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
9
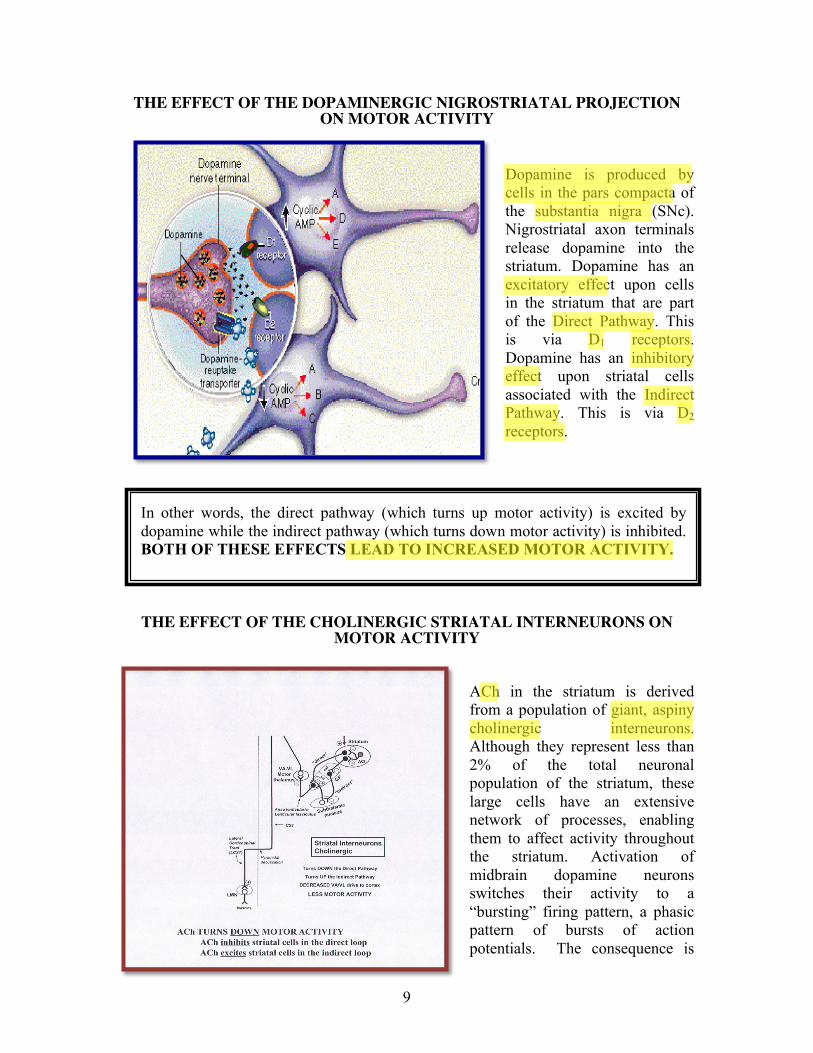
THE EFFECT OF THE DOPAMINERGIC NIGROSTRIATAL PROJECTION ON MOTOR ACTIVITY
Dopamine is produced by cells in the pars compacta of the substantia nigra (SNc). Nigrostriatal axon terminals release dopamine into the striatum. Dopamine has an excitatory effect upon cells in the striatum that are part of the Direct Pathway. This is via D1 receptors. Dopamine has an inhibitory effect upon striatal cells associated with the Indirect Pathway. This is via D2 receptors.
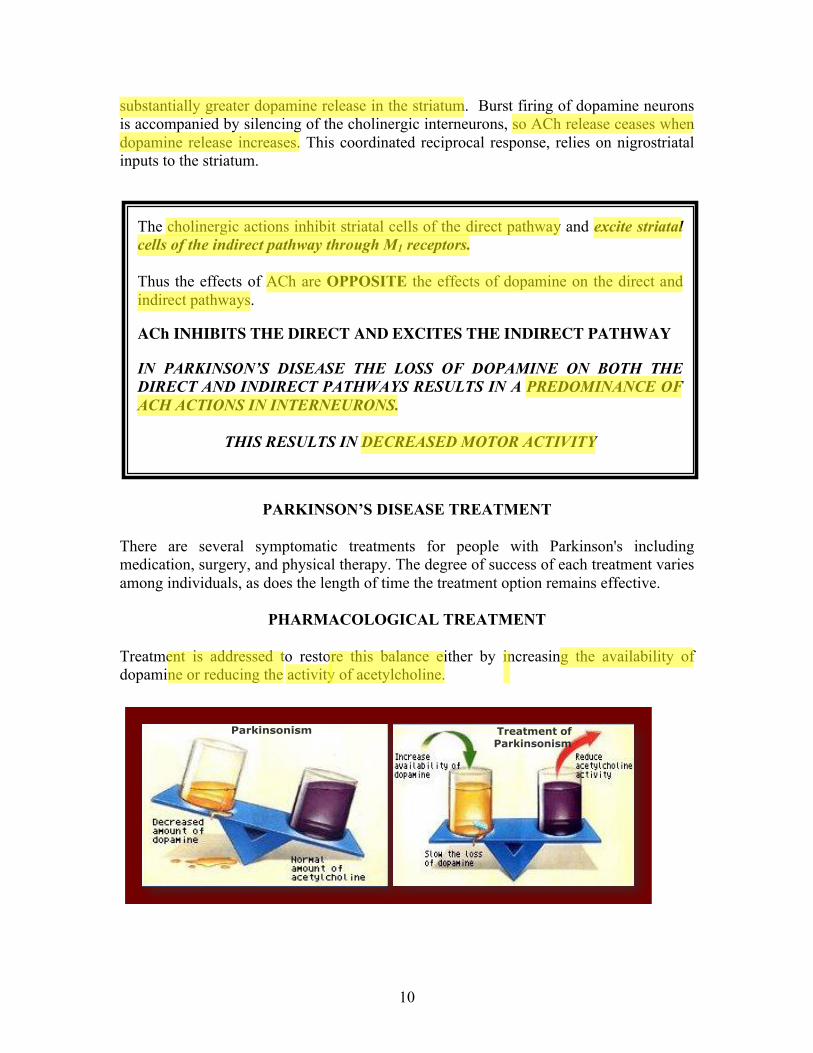
THE EFFECT OF THE CHOLINERGIC STRIATAL INTERNEURONS ON MOTOR ACTIVITY
ACh in the striatum is derived from a population of giant, aspiny cholinergic interneurons. Although they represent less than 2% of the total neuronal population of the striatum, these large cells have an extensive network of processes, enabling them to affect activity throughout the striatum. Activation of midbrain dopamine neurons switches their activity to a “bursting” firing pattern, a phasic pattern of bursts of action potentials. The consequence is
In other words, the direct pathway (which turns up motor activity) is excited by dopamine while the indirect pathway (which turns down motor activity) is inhibited. BOTH OF THESE EFFECTS LEAD TO INCREASED MOTOR ACTIVITY.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
10
substantially greater dopamine release in the striatum. Burst firing of dopamine neurons is accompanied by silencing of the cholinergic interneurons, so ACh release ceases when dopamine release increases. This coordinated reciprocal response, relies on nigrostriatal inputs to the striatum.
PARKINSON’S DISEASE TREATMENT
There are several symptomatic treatments for people with Parkinson's including medication, surgery, and physical therapy. The degree of success of each treatment varies among individuals, as does the length of time the treatment option remains effective.
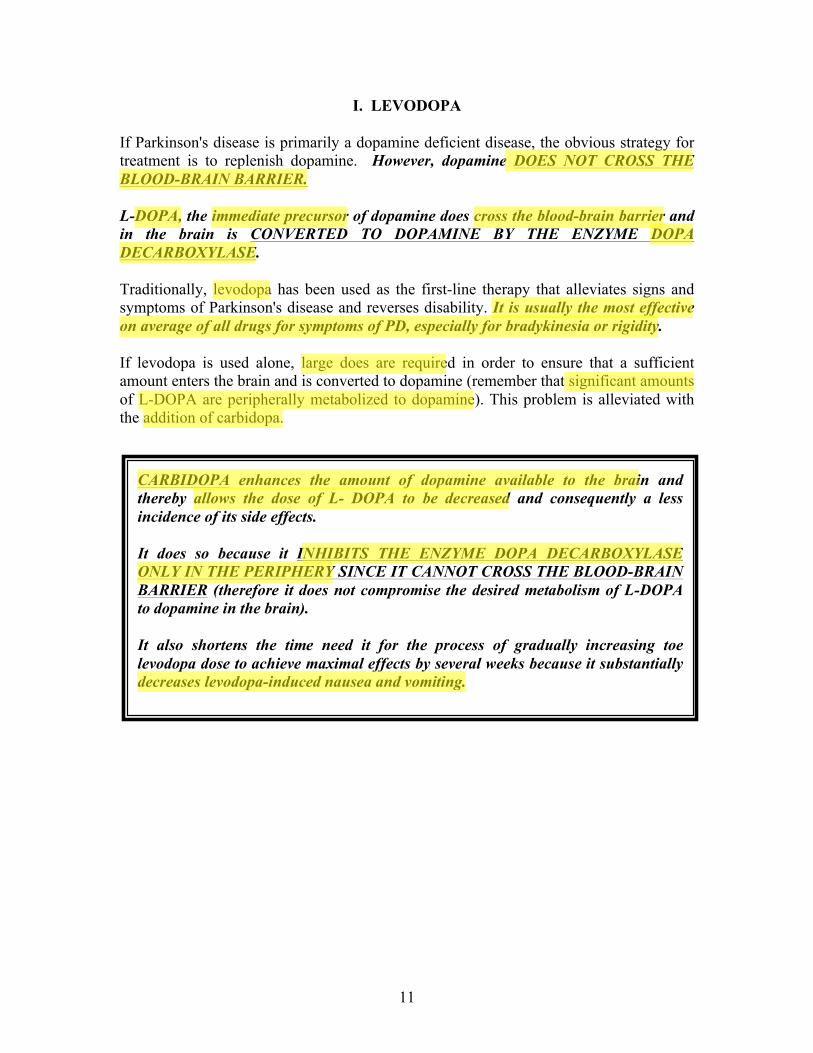
PHARMACOLOGICAL TREATMENT Treatment is addressed to restore this balance either by increasing the availability of dopamine or reducing the activity of acetylcholine.
The cholinergic actions inhibit striatal cells of the direct pathway and excite striatal cells of the indirect pathway through M1 receptors. Thus the effects of ACh are OPPOSITE the effects of dopamine on the direct and indirect pathways. ACh INHIBITS THE DIRECT AND EXCITES THE INDIRECT PATHWAY IN PARKINSON’S DISEASE THE LOSS OF DOPAMINE ON BOTH THE DIRECT AND INDIRECT PATHWAYS RESULTS IN A PREDOMINANCE OF ACH ACTIONS IN INTERNEURONS.
THIS RESULTS IN DECREASED MOTOR ACTIVITY
BASED ON PD PATHOPHYSIOLOGY WHAT PHARMACOLOGICAL APPROACH WOULD YOU TAKE?
Increasing the dopaminergic activity Decreasing the cholinergic activity
Parkinsonism Treatment of Parkinsonism
Increasing the dopaminergic activity Decreasing the cholinergic activity
Parkinsonism Treatment of Parkinsonism
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
11
I. LEVODOPA If Parkinson's disease is primarily a dopamine deficient disease, the obvious strategy for treatment is to replenish dopamine. However, dopamine DOES NOT CROSS THE BLOOD-BRAIN BARRIER. L-DOPA, the immediate precursor of dopamine does cross the blood-brain barrier and in the brain is CONVERTED TO DOPAMINE BY THE ENZYME DOPA DECARBOXYLASE. Traditionally, levodopa has been used as the first-line therapy that alleviates signs and symptoms of Parkinson's disease and reverses disability. It is usually the most effective on average of all drugs for symptoms of PD, especially for bradykinesia or rigidity. If levodopa is used alone, large does are required in order to ensure that a sufficient amount enters the brain and is converted to dopamine (remember that significant amounts of L-DOPA are peripherally metabolized to dopamine). This problem is alleviated with the addition of carbidopa.
CARBIDOPA enhances the amount of dopamine available to the brain and thereby allows the dose of L- DOPA to be decreased and consequently a less incidence of its side effects. It does so because it INHIBITS THE ENZYME DOPA DECARBOXYLASE ONLY IN THE PERIPHERY SINCE IT CANNOT CROSS THE BLOOD-BRAIN BARRIER (therefore it does not compromise the desired metabolism of L-DOPA to dopamine in the brain). It also shortens the time need it for the process of gradually increasing toe levodopa dose to achieve maximal effects by several weeks because it substantially decreases levodopa-induced nausea and vomiting.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
12
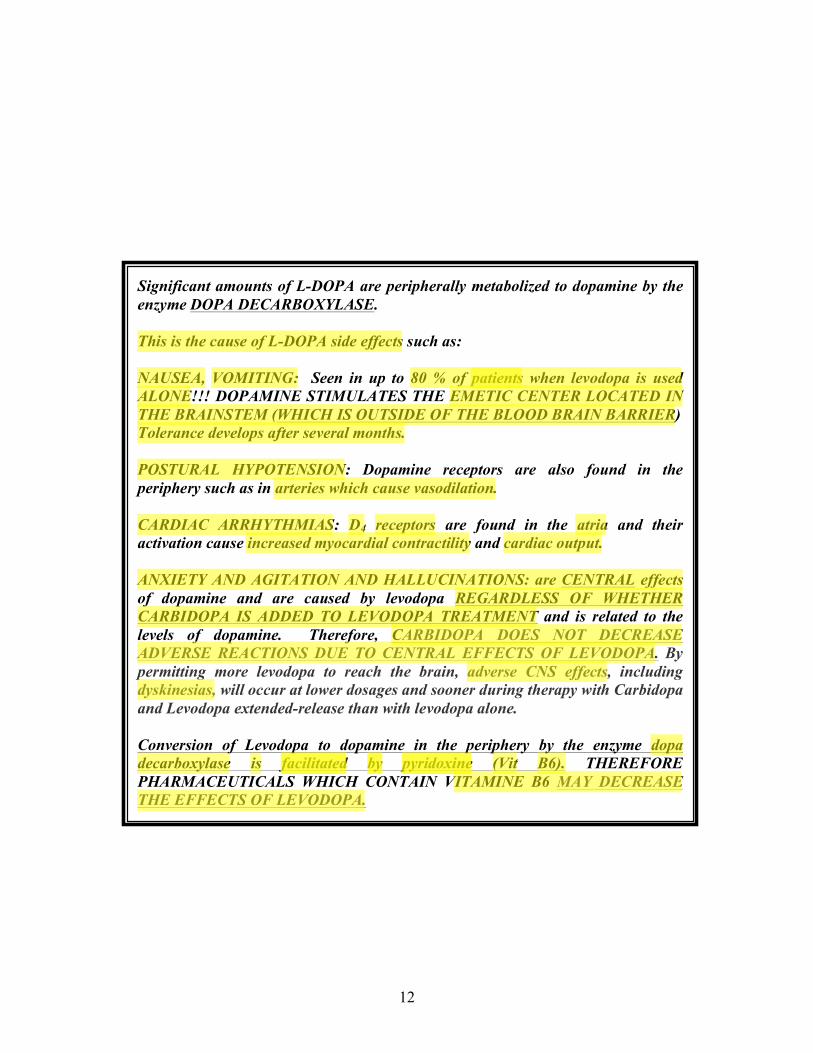
Significant amounts of L-DOPA are peripherally metabolized to dopamine by the enzyme DOPA DECARBOXYLASE. This is the cause of L-DOPA side effects such as: NAUSEA, VOMITING: Seen in up to 80 % of patients when levodopa is used ALONE!!! DOPAMINE STIMULATES THE EMETIC CENTER LOCATED IN THE BRAINSTEM (WHICH IS OUTSIDE OF THE BLOOD BRAIN BARRIER) Tolerance develops after several months. POSTURAL HYPOTENSION: Dopamine receptors are also found in the periphery such as in arteries which cause vasodilation. CARDIAC ARRHYTHMIAS: D4 receptors are found in the atria and their activation cause increased myocardial contractility and cardiac output. ANXIETY AND AGITATION AND HALLUCINATIONS: are CENTRAL effects of dopamine and are caused by levodopa REGARDLESS OF WHETHER CARBIDOPA IS ADDED TO LEVODOPA TREATMENT and is related to the levels of dopamine. Therefore, CARBIDOPA DOES NOT DECREASE ADVERSE REACTIONS DUE TO CENTRAL EFFECTS OF LEVODOPA. By permitting more levodopa to reach the brain, adverse CNS effects, including dyskinesias, will occur at lower dosages and sooner during therapy with Carbidopa and Levodopa extended-release than with levodopa alone. Conversion of Levodopa to dopamine in the periphery by the enzyme dopa decarboxylase is facilitated by pyridoxine (Vit B6). THEREFORE PHARMACEUTICALS WHICH CONTAIN VITAMINE B6 MAY DECREASE THE EFFECTS OF LEVODOPA.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
13
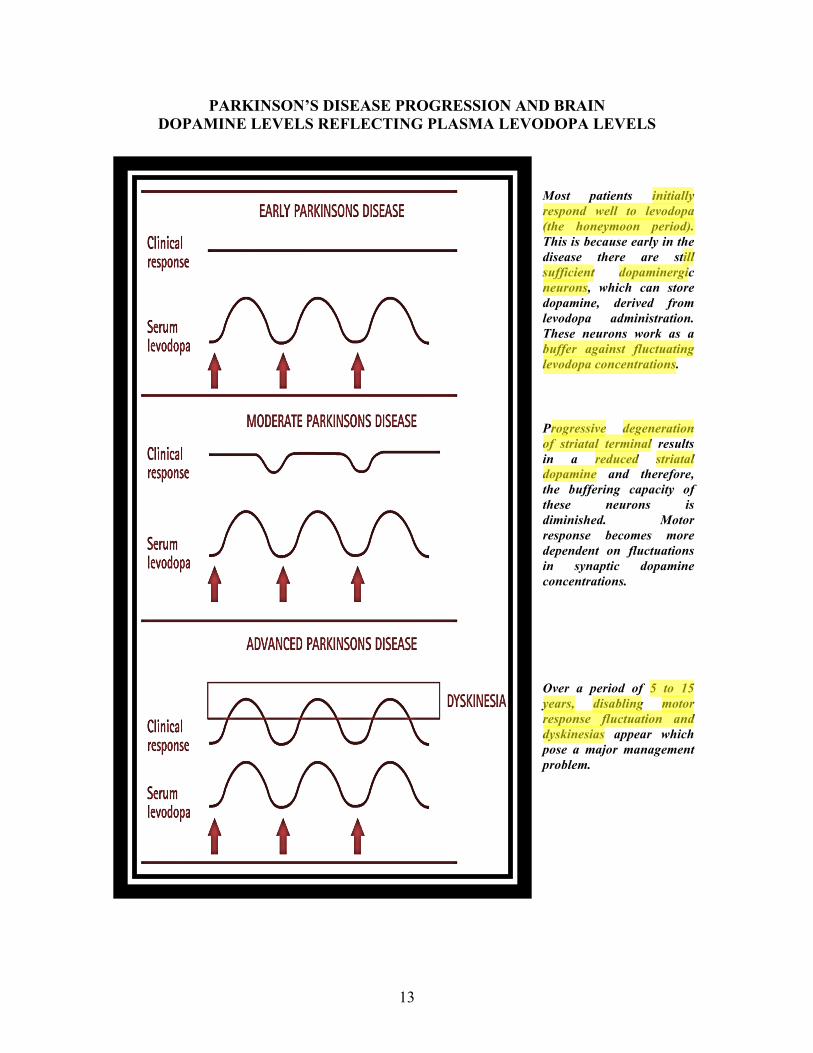
PARKINSON’S DISEASE PROGRESSION AND BRAIN DOPAMINE LEVELS REFLECTING PLASMA LEVODOPA LEVELS
Most patients initially respond well to levodopa (the honeymoon period). This is because early in the disease there are still sufficient dopaminergic neurons, which can store dopamine, derived from levodopa administration. These neurons work as a buffer against fluctuating levodopa concentrations. Progressive degeneration of striatal terminal results in a reduced striatal dopamine and therefore, the buffering capacity of these neurons is diminished. Motor response becomes more dependent on fluctuations in synaptic dopamine concentrations. Over a period of 5 to 15 years, disabling motor response fluctuation and dyskinesias appear which pose a major management problem.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
14
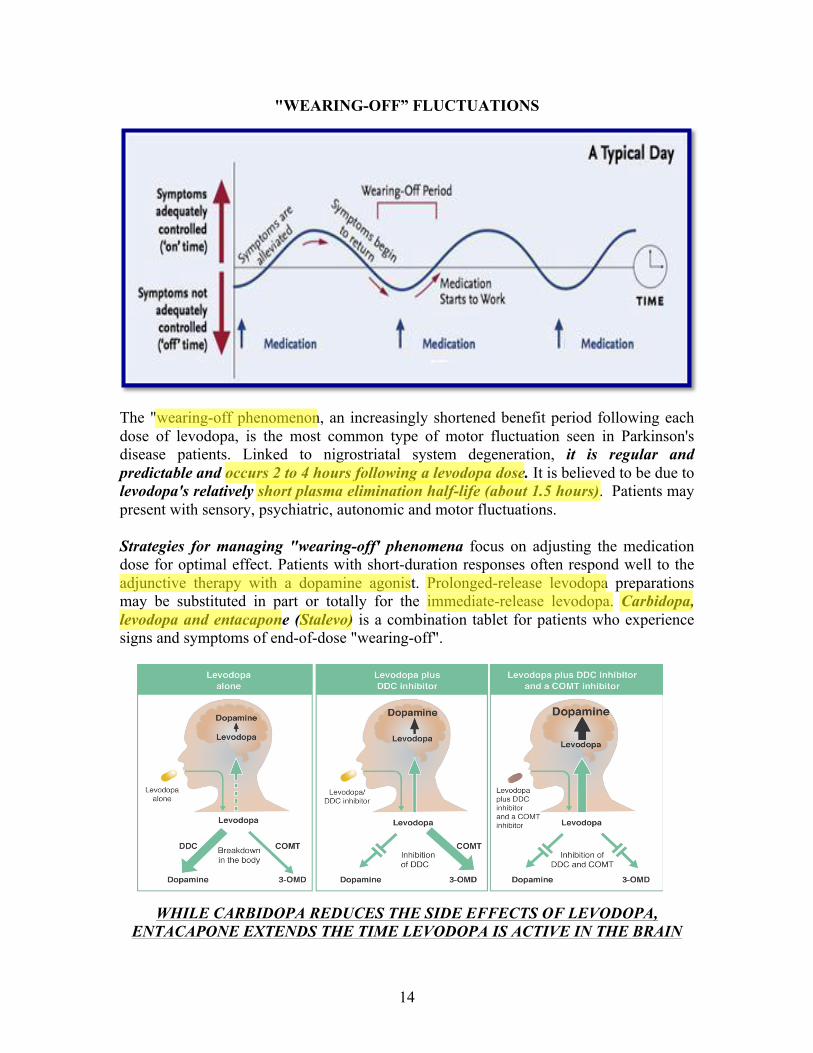
"WEARING-OFF” FLUCTUATIONS
The "wearing-off phenomenon, an increasingly shortened benefit period following each dose of levodopa, is the most common type of motor fluctuation seen in Parkinson's disease patients. Linked to nigrostriatal system degeneration, it is regular and predictable and occurs 2 to 4 hours following a levodopa dose. It is believed to be due to levodopa's relatively short plasma elimination half-life (about 1.5 hours). Patients may present with sensory, psychiatric, autonomic and motor fluctuations. Strategies for managing "wearing-off' phenomena focus on adjusting the medication dose for optimal effect. Patients with short-duration responses often respond well to the adjunctive therapy with a dopamine agonist. Prolonged-release levodopa preparations may be substituted in part or totally for the immediate-release levodopa. Carbidopa, levodopa and entacapone (Stalevo) is a combination tablet for patients who experience signs and symptoms of end-of-dose "wearing-off".
WHILE CARBIDOPA REDUCES THE SIDE EFFECTS OF LEVODOPA, ENTACAPONE EXTENDS THE TIME LEVODOPA IS ACTIVE IN THE BRAIN
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
15
"ON-OFF" FLUCTUATIONS The "on-off' phenomenon is characterized by sudden, unpredictable shifts between undertreated and overtreated states. These motor shifts appear to be an indirect result of the destruction of presynaptic dopamine terminals resulting from fluctuation transmitter levels. During the off period the patient becomes immobile or unable to perform activities of daily living (e.g., inability to rise from a chair, to speak. or to walk). Because they are sudden and unpredictable, "on-off' responses are very difficult to treat. The addition of or increased dosage of a dopamine agonist or larger doses of levodopa can be tried; however, most pharmacologic interventions that improve the" on" time will also increase dyskinesias.
LEVODOPA AND HIGH PROTEIN MEALS Large neutral amino acid transporter (LNNAs) is a heterodimeric membrane transport protein that preferentially transports the essential amino acids tyrosine, tryptophan, phenylalanine, leucine, isoleucine, histidine, methionine and threonine. This transporter is mainly expressed in the blood brain barrier and in the gut. All of the LNNAs compete for places on the same “carrier” system for movement into the brain and gut. Levodopa crosses the gut and the blood brain barrier using this transporter.
Patients should be advised to TAKE LEVODOPA ON AN EMPTY STOMACH. It is recommended to REDUCE DIETARY PROTEIN OR ADJUST MEAL TIMES (an hour before or after) to prevent competition with transport, which may lead to reduced therapeutic effect of the drug.
WHEN PRESCRIBING LEVODOPA PATIENTS SHOULD BE ADVISED OF:
• The risk of HYPERTENSIVE CRISIS IF MAOIs ARE GIVEN
CONCOMITANTLY
• THOSE RECEIVING ANTIPSYCHOTIC TREATMENT SHOULD NOT BE PRESCRIBED LEVODOPA TO TREAT THE EXTRAPYRAMIDAL EFFECTS since L-DOPA enhances dopamine and therefore its interaction with D2 receptors in the mesolimbic and mesocortical pathways. These receptors' blockade is the base of antipsychotic's mechanism of action and therefore, their efficacy could be compromised.
• Metoclopramide DECREASES L-DOPA efficacy.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
16
II. DOPAMINE AGONISTS Dopaminergic agonists can be divided into ERGOT DAs such as BROMOCRIPTINE (Parlodel) and NON-ERGOT DAs, PRAMIPEXOLE (Mirapex), ROPINIROLE (Requip), and APOMORPHINE (Apokyn). Dopamine agonists are effective for all features of the disease, but are not generally as effective as levodopa. Their used is being recommended as monotherapy or as adjunct therapy early in the disease, particularly in younger patients.
Bromocriptine is a dopamine agonist. It directly stimulates postsynaptic dopamine D2 receptors within the corpus striatum. It also has Dl antagonist activity. It is administered orally. Pramipexole and Ropinirole are selective D2 agonists.
DAs VERSUS LEVODOPA
• They ACT DIRECTLY AT DOPAMINE RECEPTORS and therefore metabolic conversion to an active moiety, as in the case of levodopa, is not required.
• They do not undergo oxidation and thus AVOID THE GENERATION OF
FREE RADICALS THAT MAY CONTRIBUTE TO NEURONAL DEGENERATION. This is being currently investigated to demonstrate a potential neuroprotective role of these drugs in PD.
• THE LONGER HALF-LIFE OF THESE DRUGS CAUSE FEWER
MOTOR COMPLICATIONS as they are able to provide continuous stimulation of striatal dopamine receptors and reduce the frequency of doses required to maintain adequate drug levels.
• Unlike levodopa, DAs do not require carrier-mediated transport for
gastrointestinal absorption or entry into the brain and thus DIETARY RESTRICTIONS ARE NOT REQUIRED
• Their use is ASSOCIATED WITH MORE HALLUCINATIONS,
SOMNOLENCE, AND EDEMA THAN WITH LEVODOPA THERAPY.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
17
III. APOMORPHINE
The ERGOT-DAs have been linked to FIBROTIC REACTIONS AFFECTING CARDIAC VALVE, PULMONARY, AND RETROPERITONEAL SOFT TISSUES. DOPAMINERGIC DRUGS have the potential to induce sudden and irresistible drowsiness leading to sudden onset of sleep (“SLEEP ATTACKS”). These episodes have the potential to cause serious accidents e.g. vehicle accidents. DEVELOPMENT OF COMPULSIVE BEHAVIOR MANIFESTED AS PATHOLOGIC GAMBLING, BINGE EATING, COMPULSIVE SHOPPING, AND HYPERSEXUALITY. This is most likely to occur in younger onset PD patients and those with family history of alcohol abuse. Other side effects with these drugs, which are frequent and related to dopamine include nausea, postural hypotension, somnolence, and psychosis.
Although chemically related to morphine, APOMORPHINE LACKS any ANALGESIC ACTIONS or risk for causing dependence OR ADDICTION. It is classified as a dopaminergic agonist. The unique role that apomorphine can offer for PD is the RAPID "RESCUE" IT OFFERS A PD PATIENT FROM AN UNDERMEDICATED OR "FROZEN" STATE. Apomorphine does not relieve all features or symptoms of PD (such as imbalance). Apomorphine needs to be administered by a subcutaneous injection. It has a very rapid onset of action (10-15 min). The first injection of apomorphine should be administered at the doctor’s office to determine the correct dose, train the patient to self-injection and TO MONITOR FOR HYPOTENSION. IT MUST BE TAKEN WITH AN ANTIEMETIC drug because, when taken alone, it causes severe nausea and vomiting. IT MUST NOT BE TAKEN WITH THE 5HT3 ANTAGONISTS (ONDANSETRON AND SIMILAR DRUGS), because the combination of apomorphine and these drugs can lead to very low blood pressure and loss of consciousness.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
18
IV. AMANTADINE (Symmetrel) Amantadine is an antiviral agent that was discovered serendipitously when a patient who was given the drug to treat influenza experienced a remission in her tremor, rigidity, and bradykinesia.
It augments dopamine release from presynaptic nerve terminals.
It may be used as monotherapy in patients with early Parkinson's disease, or as adjunct therapy to levodopa. It is also used in combination with L-DOPA to treat L-DOPA-related dyskinesias It is relatively safe and the major concern with its use is that doses need to be reduced in patients with renal impairment since it is mainly excreted through the kidneys. One of its side effects includes LIVEDO RETICULARIS, a mottled reticulated vascular pattern that appears like a lace-like purplish discoloration of the skin.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
19
V. MONOAMINE OXIDASE (MAO) INHIBITORS
Monoamine oxidase-B inhibitors (e.g., SELEGILINE, RASAGILINE) are used for the treatment of early-stage Parkinson’s disease. They block the breakdown of dopamine to dihydroxyphenylacetic acid in the brain, resulting in an increased supply of dopamine. As a result, inhibition of MAO-B can increase the dopaminergic response without requiring an increase in levodopa dosage. Selegiline (Deprenyl or Eldepryl) has a mild therapeutic effect. It also has mild antidepressant activity that offers modest direct symptomatic benefit for PD.
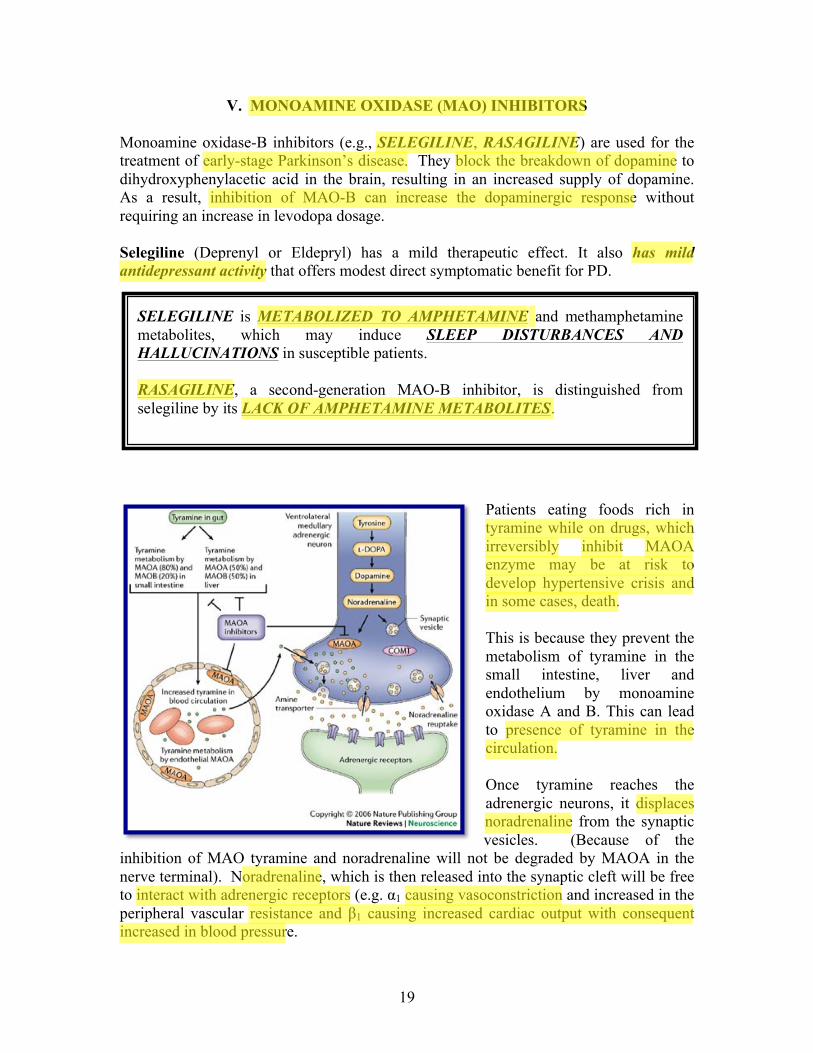
Patients eating foods rich in tyramine while on drugs, which irreversibly inhibit MAOA enzyme may be at risk to develop hypertensive crisis and in some cases, death. This is because they prevent the metabolism of tyramine in the small intestine, liver and endothelium by monoamine oxidase A and B. This can lead to presence of tyramine in the circulation. Once tyramine reaches the adrenergic neurons, it displaces noradrenaline from the synaptic vesicles. (Because of the
inhibition of MAO tyramine and noradrenaline will not be degraded by MAOA in the nerve terminal). Noradrenaline, which is then released into the synaptic cleft will be free to interact with adrenergic receptors (e.g. α1 causing vasoconstriction and increased in the peripheral vascular resistance and β1 causing increased cardiac output with consequent increased in blood pressure.
SELEGILINE is METABOLIZED TO AMPHETAMINE and methamphetamine metabolites, which may induce SLEEP DISTURBANCES AND HALLUCINATIONS in susceptible patients. RASAGILINE, a second-generation MAO-B inhibitor, is distinguished from selegiline by its LACK OF AMPHETAMINE METABOLITES.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
20
The cheese reaction is a MEDICAL EMERGENCY requiring immediate treatment. Acute elevation in BP >180/120 mmHg leading to end-organ damage can start between 10 minutes and 2 hours after meal.
VI. COMT INHIBITORs
Levodopa is extensively metabolized in the periphery to 3-0-methyldopa (3-0MD) by catechol-O-methyltransterase (COMT). COMT thereby reduces the amount of levodopa available for conversion to dopamine. COMT inhibitors such as tolcapone and entacapone increase the bioavailability of levodopa while maintaining more stable plasma concentrations, and therefore enhance the efficacy of levodopa therapy.
CARBIDOPA, LEVODOPA AND ENTACAPONE (STALEVO) is a relatively new combination tablet for patients who experience signs and symptoms of END-OF-DOSE "WEARING-OFF". WHILE CARBIDOPA REDUCES THE SIDE EFFECTS OF LEVODOPA, ENTACAPONE EXTENDS THE TIME LEVODOPA IS ACTIVE IN THE BRAIN. TOLCAPONE is only used for more advanced patients, WHEN OTHER DRUGS HAVE FAILED, because of concerns for LIVER TOXICITY.
In theory, because MAOB is present in the BRAIN BUT NOT IN ADRENERGIC NEURONS, THE CHEESE REACTION IS NOT SEEN WITH IRREVERSIBLE MAOB INHIBITORS, except at higher doses, which cause the selectivity of these inhibitors to be lost. However, selectivity of these drugs for MAO B may not be absolute even at the recommended daily and caution should be exercised.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
21
ANTICHOLINERGIC DRUGS
Anticholinergic agents were commonly used as initial therapy, especially in cases where tremor was predominant. These agents have been used to treat PD since 1867, when it was discovered that symptoms were improved by the belladonna derivative, scopolamine. These drugs remained the mainstay of treatment until the late 1960s when amantadine and levodopa were introduced.
RELEVANT INFORMATION
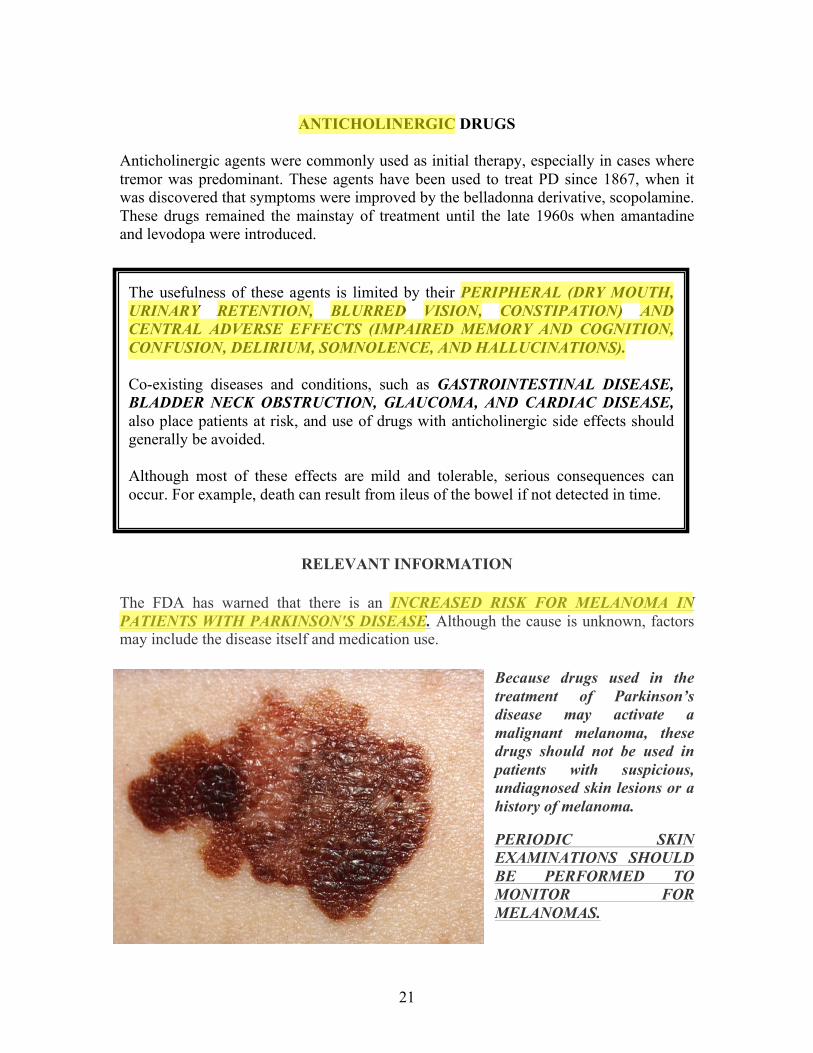
The FDA has warned that there is an INCREASED RISK FOR MELANOMA IN PATIENTS WITH PARKINSON'S DISEASE. Although the cause is unknown, factors may include the disease itself and medication use.
Because drugs used in the treatment of Parkinson’s disease may activate a malignant melanoma, these drugs should not be used in patients with suspicious, undiagnosed skin lesions or a history of melanoma.
PERIODIC SKIN EXAMINATIONS SHOULD BE PERFORMED TO MONITOR FOR MELANOMAS.
The usefulness of these agents is limited by their PERIPHERAL (DRY MOUTH, URINARY RETENTION, BLURRED VISION, CONSTIPATION) AND CENTRAL ADVERSE EFFECTS (IMPAIRED MEMORY AND COGNITION, CONFUSION, DELIRIUM, SOMNOLENCE, AND HALLUCINATIONS). Co-existing diseases and conditions, such as GASTROINTESTINAL DISEASE, BLADDER NECK OBSTRUCTION, GLAUCOMA, AND CARDIAC DISEASE, also place patients at risk, and use of drugs with anticholinergic side effects should generally be avoided. Although most of these effects are mild and tolerable, serious consequences can occur. For example, death can result from ileus of the bowel if not detected in time.
Suneil
Highlight
Suneil
Highlight
Suneil
Highlight
22
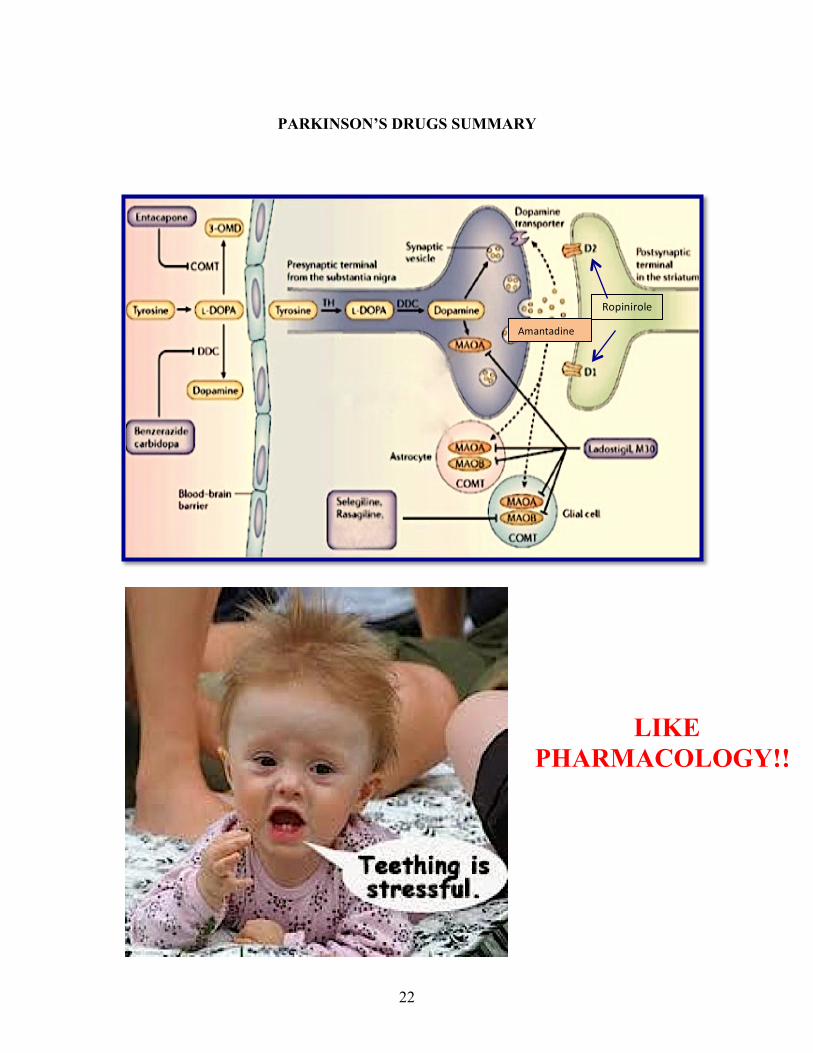
PARKINSON’S DRUGS SUMMARY
1
Amantadine
2
Ropinirole
LIKE PHARMACOLOGY!!!