
2014 Annual Report PUBLIC - INTEGRIS OK
22
INTEGRIS Baptist Medical Center cancer program is accredited through the ACoS, CoC (American College of Surgeons, Commission on Cancer). The INTEGRIS Cancer Institute is part of the INTEGRIS Baptist Medical Center cancer program, delivering integrated, comprehensive and advanced cancer care across Oklahoma. PUBLIC REPORTING OF OUTCOMES 2014 Annual Report
Transcript of 2014 Annual Report PUBLIC - INTEGRIS OK

INTEGRIS Baptist Medical Center cancer program is accredited through the ACoS, CoC (American College of Surgeons, Commission on Cancer).
The INTEGRIS Cancer Institute is part of the INTEGRIS Baptist Medical Center cancer program, delivering integrated, comprehensive and advanced cancer care across Oklahoma.
PUBLIC REPORTING OF OUTCOMES
2014 Annual Report

2
Our Mission
To improve the health of the people and communities we serve.
Caring for our patients is our top priority. As the largest health care sys-tem in Oklahoma, we feel it’s our responsibility to improve the health of the citizens of our great state. But we learned a long time ago that we can’t fully care for our community by staying exclusively within the walls of our facilities.
That’s why “returnship” is such an important part of our philosophy. What is returnship? It’s giving back part of ourselves to the communities we serve.
At INTEGRIS Health, the physicians, employees and volunteers take their education and skills into the community to make a difference in the lives of fellow Oklahomans. Their education, combined with our resources, helps accomplish a variety of things – from providing free clinical services, screenings and education programs to providing activities for senior citizens.
We also realize the health of a community isn’t just physical and mental – it’s economic and spiritual as well. That’s why we offer a myriad of pro-grams that address all of these important issues.
Our Vision
Most Trusted Name in Health Care
When INTEGRIS Health decided to develop a vision statement for the or-ganization, we wanted feedback from our most valuable commodity – our employees. More than 1,500 INTEGRIS Health employees were involved in discussions or surveys to develop our vision.
We feel it says a lot about who we are – we value trust as a guiding prin-ciple – and we aspire to be recognized for that. It is a big vision, but it is also a very personal one, too. From front-line to physician, from manage-ment to medicine, each of our employees can – and must – resolve to be most-trusted day-in and day-out in our given areas of responsibility. It is a commitment to one another as well.
This vision is not defined by geography, nor does it define a local or even national competitor. It says simply, INTEGRIS Health: Most Trusted Name in Health Care.

3
TABLE OF CONTENTS
INTEGRIS Baptist Medical Center and INTEGRIS Cancer Institute ............ 4
Multidisciplinary Clinics and Conference.................................................. 8
Cancer Committee Members .................................................................. 9
Clinical Trial Accruals ............................................................................. 10
CP3R Performance Results ...................................................................... 11
Studies of Quality .................................................................................. 12
Quality Improvements ........................................................................... 12
Who We Serve ...................................................................................... 15
Staying Connected ............................................................................... 20
4
INTEGRIS Baptist Medical Center
INTEGRIS Baptist Medical Center, in Oklahoma City, Okla., is a 511-bed hospital offering a full range of surgical, diagnostic, therapeutic and rehabilitative services.
Centers of Excellence
• INTEGRIS Cancer Institute
• INTEGRIS Heart Hospital
• Hough Ear Institute
• INTEGRIS Jim Thorpe Rehabilitation
• INTEGRIS Nazih Zuhdi Transplant Institute
• INTEGRIS Paul Silverstein Burn Center
• INTEGRIS James R. Daniel Cerebrovascular and Stroke Center
• INTEGRIS M.J. and S. Elizabeth Schwartz Sleep Disorders Center
INTEGRIS Cancer Institute
The INTEGRIS Cancer Institute is more than a cancer treatment facility. It’s a cancer treatment PHI-LOSOPHY treating the whole person, not just the disease. With six campuses statewide including the proton campus (an outpatient campus of INTEGRIS Baptist Medical Center), we provide a holistic approach to fighting cancer – guiding our patients through their journey medically, as well as walking through it with them personally. Every case of cancer is unique and every patient’s needs are different. That’s why we offer more types of treatment and more specialists in every area of cancer. And that’s why no one else but INTEGRIS can claim MORE SURVIVORS of more types of CANCER THAN ANYWHERE ELSE IN THE STATE.
The holistic approach of the INTEGRIS Cancer Institute extends to technology and treatment as well. As the sixth proton therapy center in the nation and part of the largest health care system in the state, the INTEGRIS Cancer Institute sets itself apart by offering more care, more treatment, more choice … more hope.
We offer comprehensive treatment for malignancies and blood disorders. Our services include the following.
PROCURE PROTON THERAPY CENTER
• Four treatment rooms
• Capacity to treat up to 1,500 patients per year

5
RADIATION ONCOLOGY • Full-service physics support
• Oklahoma’s first Novalis TXTM with BrainLab, a multimodality radiosurgery system
• Trilogy
• HDR (high dose rate) acuity
RADIATION THERAPYComprehensive state-of-the-art diagnostic treatments available for all types of cancers.
• IGRT (image-guided respiratory gating radiation therapy)
• IMRT (intensity modulated radiation therapy)
• Stereotactic radiation therapy
• Conformal 3D radiation therapy
• High-dose rate brachytherapy
• Radionuclide therapy
IMAGING
• GE’s most advanced equipment including digital radiographic and fluoroscopic capabilities; one 64-slice CT; ultrasound – oncology specific; PET/CT – 16 slice
• MRI – 3 Tesla with CinemaVision
• PACS system for multidisciplinary review
• American College of Radiology accreditation
MEDICAL ONCOLOGY/INFUSION THERAPY
• Dedicated group of medical oncologists
• Private, semi-private and open infusion suites equipped with flat screen TVs and heated recliners for patient comfort
• Pain management
• Physical medicine and rehabilitation
• Multi-disciplinary cancer care delivering a team approach to provide customized treatment plans for patients
• Accredited by the American College of Surgeons and American College of Radiology

6
TROY AND DOLLIE SMITH WELLNESS CENTER
• Survivorship programs
• Comprehensive resource center for patients, their families and caregivers
• Complementary therapies including massage, yoga and art
• Clinical research and trials; genetic and nutritional consultations
• Pastoral care, spiritual support and clinical social work services
BILL WALLING JR. MEDITATION ROOM
• Multi-faith resources, prayer labyrinth for meditation and reflection, and outdoor seating
INTEGRIS PHARMACY AT THE INTEGRIS CANCER INSTITUTE
• Convenient location and patient centered
• Competitive pricing
• Flexible transfer of prescriptions
• Private consultations available
• Delivery
JIM THORPE REHABILITATION
• STAR Program® in Oncology Rehabilitation
• Highest level of survivorship services
• Personalized rehab plan with an interdisciplinary approach
SURVIVORFIT: FREE CANCER RECOVERY FITNESS PROGRAM
• Encourages participants to take charge of their recovery
• Addresses the spiritual dimension of recovery through mind-body awareness
• Helps sort out the causes of stress and anxiety
• Helps manage emotional health and enhance the recovery process
• Helps to reduce the severity of cancer side effects, prevent unwanted weight changes and improve participant’s energy level and self-esteem
CONCIERGE SERVICES
• Hotels and Housing
• Transportation
• Dining
• Entertainment and Recreation
• Personal Care
• Houses of Worship

8
Multidisciplinary Cancer ClinicsThe INTEGRIS Cancer Institute Multidisciplinary Cancer Clinics bring together physicians including medical oncologists, radiation oncologists, surgeons and radiologists to provide specialized care in a multidisciplinary environment. This provides a crucial bridge between diagnosis and treatment. A comprehensive, streamlined approach to treatment planning increases timely optimal cancer care. The goal of the clinics is to provide consensus treatment decisions for medical and surgical management of the following sites and symptoms.
Following the Multidisciplinary Cancer Clinics, patients are seen the same day and assessed by the physician(s) who were involved in developing treatment plans and options. Through studies of quality and performance improvement efforts, the patient’s time from diagnosis to treatment has been signifi-cantly decreased.
Multidisciplinary Breast ConferenceThe INTEGRIS Baptist Medical Center Breast Conference improves the care of patients with breast cancer by providing multidisciplinary treatment planning and contributing to physician and allied medical staff education.
Each conference covers discussion of stage including prognostic indicators, and treatment planning using evidence-based guidelines, and options for clinical trial participation.
• Esophagus
• Liver
• Gallbladder
• Stomach
• Large intestines
• Small intestines
• Cecum
• Appendix
• Rectum
• Anus
• Pancreas
• Lung
• Bladder
• Testicular
• Kidney
• Prostate
• Increasing PSA level
• Enlarged prostate

9
PHYSICIAN MEMBERS .................................. SPECIALTY
*David Burger, M.D. ............................................... Radiology
*Maria Ochoa, M.D. ............................................... Pathology
Derek Irwin, M.D. ................................................... Pathology (Alt)
*Michael Holzer, M.D. ............................................ Surgery
Vivek Kohli, M.D. ................................................... Surgery (Alt)
*Romeo Mandanas, M.D., CLP ............................... Medical Oncology
Community Outreach Coordinator
*Kiran Prabhu, M.D. ............................................... Radiation Oncology
Lucius Doh, M.D. ................................................... Radiation Oncology (Alt)
*Lara Theobald, M.D. ............................................. Genetics/Medical Oncology
*Steve Drabek, M.D. .............................................. Palliative Care
Abbas Raza, M.D. ................................................... Gastroenterology
Dawn Tartaglione, D.O. .......................................... Neurosurgery
NON-PHYSICIAN MEMBERS
Phil Lance, FACHE .................................................. President, INTEGRIS Cancer Institute
Lynda Van Horn, B.S., RT(T) ................................... Administrative Director of Operations
*Joe Holcomb, B.S., M.B.A. .................................... Director, Oncology Wellness
*Kim Frank, RN, B.S.N. ........................................... Metro Director, Medical Oncology
Nikki Arnett, RN ..................................................... Clinical Manager 9E (Alt)
*Susan Coatney, ACSW, LCSW ............................... Social Worker
Psychosocial Services Coordinator
*Anna McIntosh, RHIA, CTR ................................... Cancer Registry
Cancer Registry Quality Coordinator
*Denise Dunn, RN, B.S.N. ...................................... Quality Management
Quality Improvement Coordinator
Debbie McCullock, M.S., APRN-CNP, RN-BC ......... Palliative Care
*Kellie Larsen, CCRP .............................................. Clinical Research
Clinical Research Coordinator
Lana Hale, M.S., CCRP ........................................... Clinical Research (Alt)
Sylvia Dillard .......................................................... Special Programs Coordinator
Terry Gonsoulin, RN ............................................... Director, Hospice of Oklahoma County
*Aleisha Williams .................................................... Cancer Registry
Cancer Conference Coordinator
Janet Pulliam .......................................................... American Cancer Society Representative
Kellye Elliott, M.S., CCC-SLP ................................. Rehabilitation Jim Thorpe/Senior Marketing
Connie Berlin, RN, B.S.N. ....................................... Survivorship Navigator
Carol Lott .............................................................. Director, Radiation Therapy
Jeananne Huffman, RT (R), (M) .............................Manager, Comprehensive Breast Center
2014 Cancer Committee Members
*Required member Alt = Alternate

10
Clinical Trial Accruals Clinical research advances science and ensures that patient care approaches the highest possible level of quality. Patients who participate in clinical trials have the opportunity to advance evi-dence-based medicine.
Our cancer program accrued 7 percent of patients (analytic cases) to a treatment or registry clinical trial in 2012. For 2013, 5 percent of patients (analytic cases) were accrued to a clinical trial.
The CoC requires Comprehensive Community Cancer Programs to accrue a minimum of 2 percent of patients to clinical trials. However, in 2015, the CoC will require a minimum of 4 percent of pa-tients be enrolled in clinical trials. Our program continues to exceed this requirement, demonstrating our commitment to quality, advanced care for our patients.
CP3R – Cancer Program Practice Profile ReportsThe Web-based CP3R offer local providers comparative information to assess adherence to and consideration of standard of care therapies for major cancers. This reporting tool provides a platform from which to promote continuous practice improvement to improve quality of patient care at the local level and also permits hospitals to compare their care for these patients relative to that of other providers. The aim is to empower clinicians, administrators and other staff to work cooperatively and collaboratively to identify problems in practice, and to deliver and implement best practices that will diminish disparities in care across CoC accredited cancer programs.
The CP3R provides feedback to our programs to:
• improve the quality of data across several disease sites;
• foster pre-emptive awareness to the importance of charting and coding accuracy;
• improve clinical management and coordination of patient care in the multidisciplinary setting.
The Cancer Committee ensures and monitors on a quarterly basis that patients treated at our facility receive care according to nationally accepted measures. At right is the CP3R performance grid that reports 2011 cases treated at INTEGRIS Baptist Medical Center and INTEGRIS Cancer Institute.

11
Radiation is administered within 1 year (365 days) of diagnosis for women under the age of 70 receiving 96.40% >=90% or upper breast conservation surgery for breast cancer bound of 95% (Accountability)
Combination chemotherapy is considered or administered within 4 months (120 days) of diagnosis for women 94.70% >=90% or upper bound under 70 with AJCC T1cN0, or stage IB - III hormone of 95% receptor negative breast cancer (Accountability)
Tamoxifen or third generation aromatase inhibitor is considered or administered within 1 year (365 days) of 92.10% >=90% or upper bound diagnosis for women with AJCC T1c or stage IB - III hormone of 95% receptor positive breast cancer (Accountability)
Breast conservation surgery rate for women with AJCC 50.00% Not Applicable clinical stage 0, I, or II breast cancer (Surveillance)
Image or palpation-guided needle biopsy (core or FNA) is performed to establish diagnosis of breast cancer 92.40% >80% or upper bound (Quality Improvement) of 95%
Radiation therapy is considered or administered following any mastectomy within 1 year (365 days) of diagnosis of 100% >90% or upper bound breast cancer for women with >= 4 positive regional of 95% lymph nodes (Accountability)
At least 12 regional lymph nodes are removed and pathologically examined for resected colon cancer 93.40% >=85% or upper bound (Quality Improvement) of 95%
Adjuvant chemotherapy is considered or administered within 4 months (120 days) of diagnosis for patients 95.50% >=90% or upper bound under the age of 80 with AJCC stage III (lymph node of 95% positive) colon cancer (Accountability)
Radiation therapy is considered or administered within 6 months (180 days) of diagnosis for patients under 76.90% Not applicable the age of 80 with clinical or pathologic AJCC T4N0M0 or stage III receiving surgical resection for rectal cancer (Surveillance)
CP3R Measure Our Cancer Required Program Performance Rate

12
Studies of Quality The INTEGRIS Baptist Medical Center Cancer Committee commissioned two quality studies. Both studies were conducted using the PDCA methodology. The following are the identified measures, results, implications and recommendations reviewed by the Cancer Committee.
Time from Diagnosis to Treatment
The study chosen by the Cancer Committee was to examine the time from diagnosis to treatment in lung pa-tients who have been diagnosed and treated at the INTEGRIS Cancer Institute – Proton Campus.
Physician stakeholders and Cancer Committee members reviewed data from 2012 for lung patients presented at the Lung Multidisciplinary Conference and seen at the Lung Clinic. Average time from diagnosis to treat-ment was 42 days.
There were no national benchmarks identified. An internal benchmark was set at 42 days.
At the completion of the study, action taken included recruitment of a cardiothoracic surgeon to attend the Lung Multidisciplinary Conference and Clinic.
Quarterly reports will be given to Cancer Committee.
Lynch Syndrome Testing
Another study chosen was to examine Lynch Syndrome Testing in colon cancer patients under 50 years old who have been diagnosed and treated at INTEGRIS Cancer Institute - Proton Campus.
Three years of data were reviewed (2010 – 2012). The national benchmark states that the test should be con-sidered for patients with a colon cancer diagnosis at or before age 50. There were five patients in 2010, five pa-tients in 2011, and seven patients in 2012 who met the criteria for testing. Of these patients, 52.9 percent were tested for Lynch Syndrome. One patient’s test kit was sent to be processed, but the patient ended up canceling the test. If the patient had not canceled, the testing rate would be 58.8 percent.
At the completion of the study, action taken included genetics training regarding “red flags” that identify candi-dates appropriate for testing.
Lynch Syndrome testing will continue to be monitored quarterly.
Quality Improvements The INTEGRIS Baptist Medical Center Cancer Committee reviewed and discussed two improvements for our cancer patients’ care.
Decrease in Time from Diagnosis to Treatment for Lung Cancer patients and development of a Low-dose CT Lung Screening
Lung cancer affects more than 200,000 Americans each year. 2007 incidence rate in Oklahoma per 100,000 people is 81. Death rate for the state of Oklahoma is 2,395 per year in the reporting period 2003 – 2007. A large study called the NLST (National Lung Screening Trial) showed that, in patients who are current or former heavy smokers, the use of a screening test called low-dose computed tomography scan decreases the risk of death from lung cancer by 20 percent. NCCN guidelines include a screening (baseline low-dose computed tomography) modality for high-risk patients.

13
Time from diagnosis to treatment in 2012 was 42 days.
The improvements were the implementation of the Lung Multidisciplinary Cancer Clinic for newly diagnosed lung cancer patients and the development of the Low-Dose CT Lung Screening offering to the public. This is based on the ACS (American Cancer Society) and the NCCN (National Comprehensive Cancer Network) published guide-lines, due to the results of the NLST for low-dose computed tomography.
As a result of the improvement, the time from diagnosis to treatment decreased by 12 days, from 42 days to 30 days. This represents a 40 percent decrease.
Community Resource information available for patients
Patient satisfaction scores for “Community Resource Information” being available to our patients has been below our goal of 90 percent. In the ACS and CoC document called “Working Together to Improve Cancer Outcomes,” found at www.facs.org, both organizations acknowledge the impact of the importance of their collaboration. The collaboration has had “tremendous impact on the support available to newly diagnosed cancer patients, the education of the public about cancer prevention and early detection, and physician engagement in cancer control activities at the state and community level.”
As an organization dedicated to meeting the patient’s expectations regarding “Community Resource Information,” we have developed strategies to address the actual vs. goal/target variance.
Improvements implemented include the following.
• Social worker introduction/communication letter sent to newly diagnosed patients by registration department
• “Community Resource Information” collateral material developed by business development and corporate communications departments
• Digital boards promoting “Community Resource Information” availability in the Troy and Dollie Smith Wellness Center
• Development of New Patient Orientation class
• Social worker visiting all newly diagnosed cancer patients during treatment visits with 90-day follow-ups
• Referrals by the clinical staff to the Troy and Dollie Smith Wellness Center
• Clinical staff making “Community Resource Information” collateral material available in exam rooms and waiting areas
• Distribution of ACS Personal Health Managers
• ACS Days
As a result of the improvements, patient satisfaction scores steadily increased.
• Received date June 30, 2012 - Dec. 31, 2012 ...... 88.5%
• Received date Jan. 1, 2013 - June 30, 2013 ......... 90.6%
• Received date July 1, 2013 - Dec. 31, 2013 .......... 91.6%

14

1515
INTEGRIS Baptist Medical Center Cancer Program
Who We Serve
The cancer program of INTEGRIS Baptist Medical Center serves the needs of our community and surrounding areas. In 2013, 1,452 new cases were added to the Cancer Registry, represent-ing an increase of 1 percent over 2012. The chart below provides a comparison of the top 10 sites with lung and breast accounting for the most common malignancy diagnosed among all years.
TOP 10 SITES 2010 – 2013

16
An analysis of cancer cases by sex showed that our program treats more women than men, a relatively consistent trend in 2010 through 2013.
GENDER DISTRIBUTION 2010 – 2013
Review of registry data revealed that race and ethnicity is largely Caucasian, although there are documented smaller amounts of other races and ethnicity depicted below.
RACE AND ETHNICITY 2010 – 2013

17
Cancer incidence increases with age. The majority of cancer cases were diagnosed between ages 50 to 79 years, as indicated in the graph below.
AGE AT DIAGNOSIS 2010 – 2013
A comparison of analytic cases added to the registry was done using the AJCC (American Joint Committee on Cancer) TNM Cancer Staging System. The majority of cancer cases were diag-nosed at an early stage of illness, AJCC Stage I, although there were a significant number of later stage cancers diagnosed, indicating the importance of earlier detection and screening efforts and public education.
AJCC CANCER STAGE AT DIAGNOSIS 2010 – 2013
18
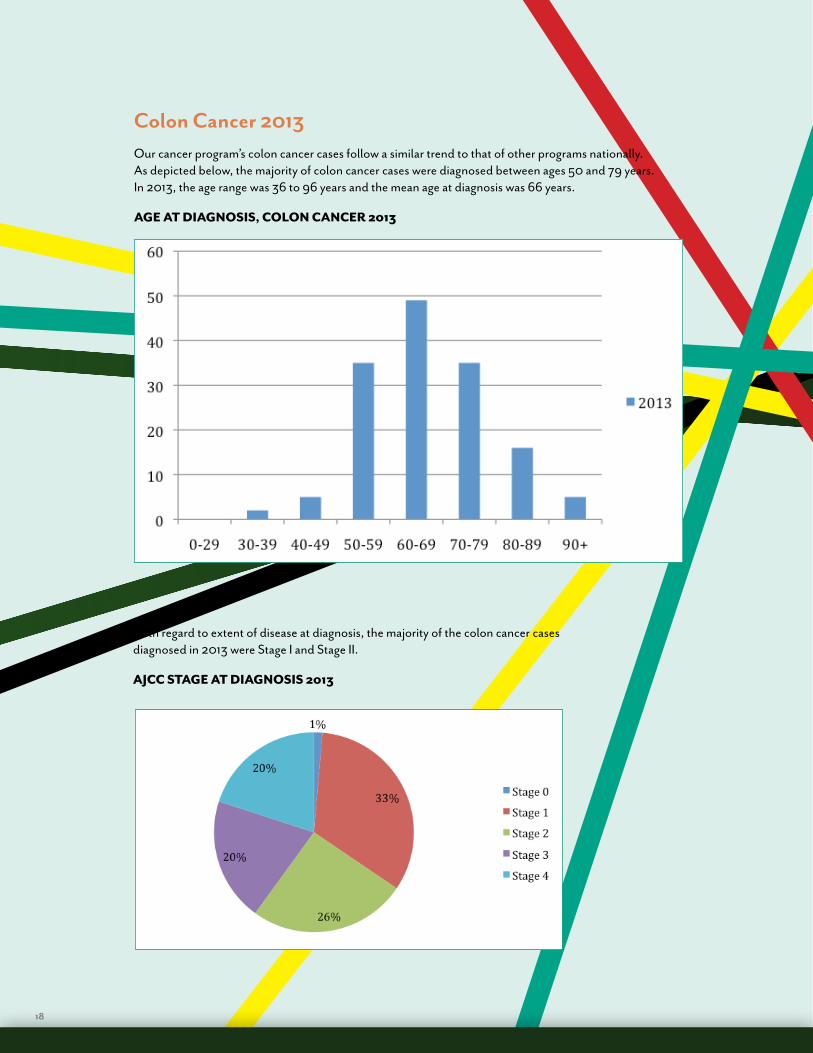
Colon Cancer 2013 Our cancer program’s colon cancer cases follow a similar trend to that of other programs nationally. As depicted below, the majority of colon cancer cases were diagnosed between ages 50 and 79 years. In 2013, the age range was 36 to 96 years and the mean age at diagnosis was 66 years.
AGE AT DIAGNOSIS, COLON CANCER 2013
With regard to extent of disease at diagnosis, the majority of the colon cancer cases diagnosed in 2013 were Stage I and Stage II.
AJCC STAGE AT DIAGNOSIS 2013

19
The following Colon Cancer First Course Surgery graphs show a comparison between our cancer program and all types of hospitals in all states as represented by the NCDB (National Cancer Data Base). Both graphs highlight that a subtotal colectomy or hemicolectomy was the most common surgical procedure performed.
INTEGRIS BAPTIST MEDICAL CENTER 2013
NCDB 2012

20
Staying ConnectedMeet some of our cancer survivors and watch their inspiring stories at integriscancer.com.
INTEGRIS CANCER INSTITUTE PROTON CAMPUS
A campus of INTEGRIS Baptist Medical Center
5911 W. Memorial Road • Oklahoma City, OK 73142
405-773-6400 • toll free 877-811-4246
INTEGRIS BAPTIST MEDICAL CENTER
3300 NW Expressway • Oklahoma City, OK 73112
405-949-3296
INTEGRIS CANADIAN VALLEY HOSPITAL
1201 Health Center Parkway • Yukon, OK 73099
405-717-6800
INTEGRIS CLINTON REGIONAL HOSPITAL
100 N. 30th Street • Clinton, OK 73601
580-323-2363
INTEGRIS HEALTH EDMOND
4833 INTEGRIS Parkway • Edmond, OK 73034
405-773-6400 • toll free 877-811-ICIO
INTEGRIS SOUTHWEST MEDICAL CENTER
4401 S. Western • Oklahoma City, OK 73109
405-631-0919

21

5911 W. Memorial Road, Oklahoma City, OK 73142
integrisok.com/cancer 405-773-6400
Fax 405-621-5443


















