
20130427 Castel Hepatocellular Carcinoma What the ... Lifelong Learning/Meetings/ASM2013... · -...
22
Hepatocellular Carcinoma: What the hepatologist wants to know Hélène Castel, MD Liver Unit Hôpital St-Luc CHUM CAR Annual Scientific Meeting Saturday, April 27 th 2013 ?
Transcript of 20130427 Castel Hepatocellular Carcinoma What the ... Lifelong Learning/Meetings/ASM2013... · -...

Hepatocellular Carcinoma: What the hepatologist wants to know
Hélène Castel, MD Liver Unit Hôpital St-Luc CHUM
CAR Annual Scientific Meeting Saturday, April 27th 2013
?

Disclosure statement
I do not have an affiliation, financial or otherwise, with a pharmaceutical company, medical device or communications organization. I have no conflicts of interest to disclose ( i.e. no industry funding received or other commercial relationships). I have no financial relationship or advisory role with pharmaceutical or device-making companies, or CME provider. I will not discuss or describe in my presentation at the meeting the investigational or unlabeled ("off-label") use of a medical device, product, or pharmaceutical that is classified by Health Canada as investigational for the intended use.
Learning objectives
1. Discuss the HCC management guidelines.
2. Recognize the hierarchy of treatment in the BCLC staging system.
3. Identify the role of the radiologist in the clinical management of HCC.
At the conclusion of this session, participants should be able to:

Burden of HCC
6th most frequent cancer 3rd cause of death by cancer AASLD
Guidelines on the Management of HCC. 2010

Trends in the diagnosis of HCC
Categorization of nodules (<2 cm) as pre-neoplastic lesions or early
HCC remains a diagnostic challenge

Tumor staging and prognosis score
Coexistence of two life-threatening conditions

Tools for staging and treatment of HCC
¡ Liver biopsy
¡ • Tumor staging: ¡ -size
-number ¡ -vascular invasion ¡ -extra hepatic disease
¡ • Liver function, ¡ • Portal hypertension ¡ • Clinical performance status
• Biological markers (AFP)
Minimum If needed
Treatment allocation – prognostic prediction

Tumor staging and prognosis score
Tumor stage Liver function Health status
CLIP* Tumor morphology, AFP, vascular invasion
Child -
GRETCH vascular invasion, AFP bilirubin, ALP Karnofsky
BCLC* Number of nodules, size, vascular invasion
Child, portal hypertension
Performance status
CUPI* TNM, AFP bilirubin, ALP, ascites
symptoms
JIS* TNM Child -
* External validation
treatment allocation

Current guidelines: BCLC

BCLC and prognosis
Marrero J, Hepatology 2005

BCLC management and staging system
EASL EORTC Clinical Guidelines on the Management of HCC. 2012

Radiological criteria for treatment decision
- Size
- Number - Localization
sub capsular, peri vascular 1 or >1 hepatic segment uni or bilobar
- Macroscopic vascular invasion - Biliary invasion

Size, number and recurrence
Decaens T, Liv Transplant 2006 UCSF: 1 nodule ≤ 6.5cm or up to 3 ≤ 4.5cm each (max sum of the Ø ≤ 8cm) Milan: 1 nodule ≤ 5cm or up to 3 ≤ 3cm each
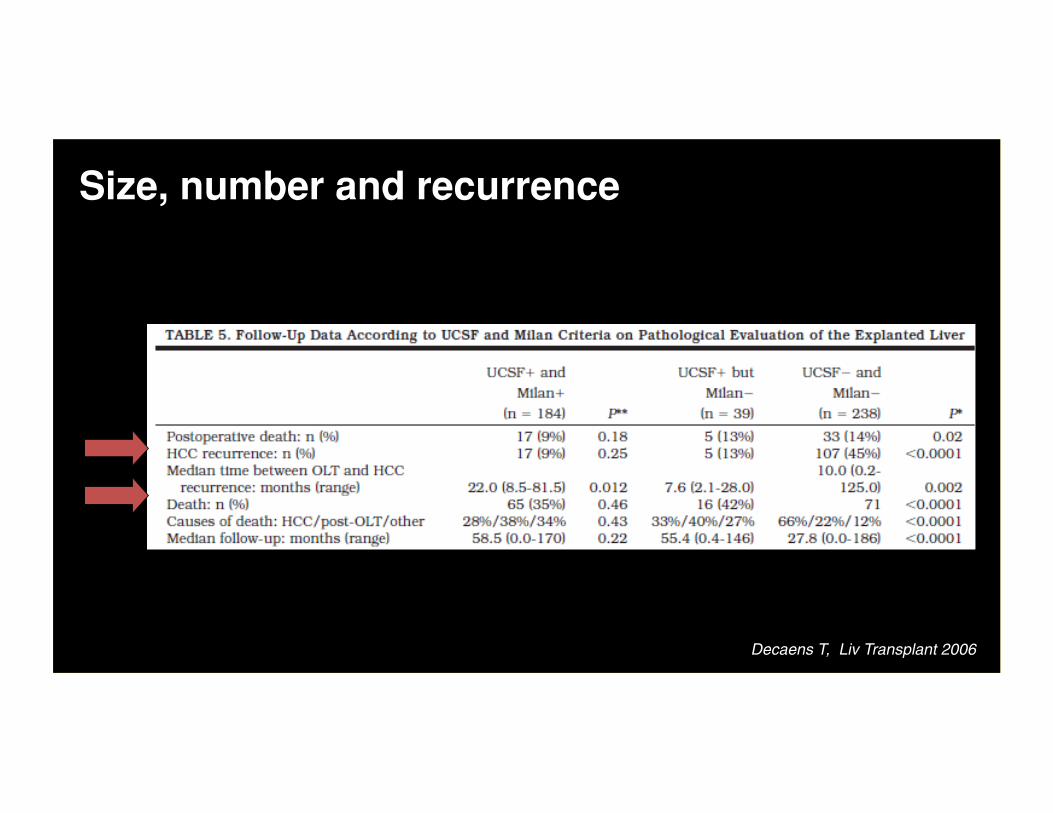
Size, number and recurrence
Decaens T, Liv Transplant 2006

Eligibility criteria for liver transplantation
« Liver transplantation is considered to be the first-line treatment option for patients with single tumors ≤ 5 cm or ≤3 nodules ≤3 cm (Milan criteria). Modest expansion of Milan criteria in patients without microvascular invasion achieves competitive outcomes, and requires prospective validation. »
EASL EORTC Clinical Guidelines on the Management of HCC. 2012

Eligibility criteria for liver transplantation
Toso C, Hepatology 2009
Rate of patients (%) transplanted outside Milan criteria (UNOS).

Criteria for LT and outcome
Mazzaferro V. Liv Transplant 2007 Mazzaferro V. Ann Surg Oncol. 2008

Eligibility criteria for LT: Total Tumor Volume
Toso C, Liver Transpl 2008
Radiology-based staging: cumulative survival and cumulative risk of HCC recurrence.
TTV= sum of the volume of each tumor (4/3)π r3 (r=maximal radius of each HCC)
TTV ≤≤ 115 cm3

Eligibility criteria for LT: TTV and AFP
Toso C, Hepatology 2009

Management after treatment
Importance of the evaluation of the response to treatment (ARTERIAL enhancement).
-Complete response - Partial response - Stable disease
- Progressive disease

Contribution of the radiologist
- Diagnose HCC by noninvasive criteria.
- In case of an atypical lesion: propose another imaging modality, biopsy or follow-up according to the guidelines.
- Describe potential contraindications to treatment:
portal vein thrombosis, ascites, portal hypertension, extra hepatic metastasis…
The radiologist is intimately involved in the treatment decisions
(multidisciplinary team+++)

Take home messages
1. Discuss the HCC management guidelines. - BCLC management guidelines endorsed by AASLD and EASL. 2. Recognize the hierarchy of treatment in the BCLC staging system. - Favor curative treatment - Surgical: resection - transplantation Locoablative: RFA > TACE 3. Identify the role of the radiologist in the clinical management of HCC. - Diagnose HCC by noninvasive criteria - Manage atypical lesions - Identify potential contraindications to treatment


















