2013 Rate Card - CAP TODAY · 2013-03-06 · 2013 Rate Card 4-color 1,400 2nd color matched from...
4
UNITS 1x 4x 6x 12x 18x 24x 36x 48x 60x Tabloid 5,810 5,680 5,590 5,520 5,340 5,230 5,060 4,960 4,910 2/3 5,150 4,940 4,790 4,630 4,450 4,310 4,200 4,070 3,900 1/2 4,470 4,390 4,240 4,160 3,970 3,860 3,690 3,610 3,510 1/4 3,270 3,160 3,060 3,020 2,810 2,750 2,630 2,550 2,460 Standard 4,570 4,480 4,390 4,240 4,110 3,950 3,820 3,680 3,630 2/3 3,060 2,950 2,840 2,790 2,740 2,720 2,630 2,540 2,410 1/2 2,650 2,560 2,460 2,380 2,290 2,250 2,180 2,110 2,020 1/3 1,980 1,910 1,820 1,640 1,600 1,510 1,480 1,410 1,370 1/4 1,440 1,380 1,340 1,300 1,250 1,210 1,170 1,140 1,100 Advertising Rates Commission: 15% to recognized agencies Inserts: Consult publisher 2013 Rate Card 4-color 1,400 2nd color matched from process 700 5th color or Pantone 900 Color Ads produced with combinations of process inks (cyan, magenta, yellow, and black) use color most economically. Many Pantone (PMS) specified colors can often be approximated using process inks. CAP TODAY can help you plan the most efficient use of your color. Call Al McAtee, 847-832-7514, for specific information. Circulation Frequency: Monthly Mailing: Periodical Class Publisher/Sales Office Bob McGonnagle 325 Waukegan Road, Northfield, IL 60093 Phone: 847-832-7476; Fax: 847-832-8873 [email protected] Production Al McAtee, Production Manager 325 Waukegan Road, Northfield, IL 60093 Phone: 847-832-7514; Fax: 847-832-8514 [email protected] Keith Eilers, Production Editor 325 Waukegan Road, Northfield, IL 60093 Phone: 847-832-7528; Fax: 847-832-8528 [email protected] Advertising Representatives East: Hally Birnbaum Mount Kisco, NY Phone: 914-218-1943; Fax: 847-832-8514 [email protected] Midwest: Lori Prochaska 6327 South 73rd Avenue, Omaha, NE 68127 Phone: 402-290-7670; Fax: 847-832-8514 [email protected] West: Diana Kelker 2337 California Avenue, Carmichael, CA 95608 Phone: 847-832-7749; Fax: 847-832-8749 [email protected] Classified KERH Group, PO Box 207 Parker Ford, PA 19457 Phone: 888-489-1555 [email protected]
Transcript of 2013 Rate Card - CAP TODAY · 2013-03-06 · 2013 Rate Card 4-color 1,400 2nd color matched from...

UNITS 1x 4x 6x 12x 18x 24x 36x 48x 60x
Tabloid 5,810 5,680 5,590 5,520 5,340 5,230 5,060 4,960 4,910
2/3 5,150 4,940 4,790 4,630 4,450 4,310 4,200 4,070 3,900
1/2 4,470 4,390 4,240 4,160 3,970 3,860 3,690 3,610 3,510
1/4 3,270 3,160 3,060 3,020 2,810 2,750 2,630 2,550 2,460
Standard 4,570 4,480 4,390 4,240 4,110 3,950 3,820 3,680 3,630
2/3 3,060 2,950 2,840 2,790 2,740 2,720 2,630 2,540 2,410
1/2 2,650 2,560 2,460 2,380 2,290 2,250 2,180 2,110 2,020
1/3 1,980 1,910 1,820 1,640 1,600 1,510 1,480 1,410 1,370
1/4 1,440 1,380 1,340 1,300 1,250 1,210 1,170 1,140 1,100
Advertising Rates Commission: 15% to recognized agencies Inserts: Consult publisher
2013 Rate Card
4-color 1,400
2nd color matched from
process700
5th color or Pantone 900
Color
Ads produced with combinations of process inks (cyan, magenta, yellow, and black) use color most economically. Many Pantone (PMS) specified colors can often be approximated using process inks. CAP TODAY can help you plan the most efficient use of your color. Call Al McAtee, 847-832-7514, for specific information. Circulation Frequency: Monthly Mailing: Periodical Class
Publisher/Sales Office Bob McGonnagle 325 Waukegan Road, Northfield, IL 60093 Phone: 847-832-7476; Fax: 847-832-8873 [email protected]
Production Al McAtee, Production Manager 325 Waukegan Road, Northfield, IL 60093 Phone: 847-832-7514; Fax: 847-832-8514 [email protected]
Keith Eilers, Production Editor 325 Waukegan Road, Northfield, IL 60093 Phone: 847-832-7528; Fax: 847-832-8528 [email protected]
Advertising Representatives East: Hally Birnbaum Mount Kisco, NY Phone: 914-218-1943; Fax: 847-832-8514 [email protected]
Midwest: Lori Prochaska 6327 South 73rd Avenue, Omaha, NE 68127 Phone: 402-290-7670; Fax: 847-832-8514 [email protected]
West: Diana Kelker 2337 California Avenue, Carmichael, CA 95608 Phone: 847-832-7749; Fax: 847-832-8749 [email protected]
Classified KERH Group, PO Box 207 Parker Ford, PA 19457 Phone: 888-489-1555 [email protected]

Benefits of diagramming tools to the clinical laboratoryIntegrating laboratory workflow with informa-
tion system operations to maximize productivity is a challenging task, but diagramming tools can simplify the process.
How diagramming tools work and which types of diagrams are most helpful to labs are the focus of “Diagramming Tools for Requirements Analy-sis and Workflow Redesign,” a section of the book Laboratory Administration for Pathologists, published by CAP Press last year. This section of the book, written by James H. Harrison Jr., MD, PhD, is excerpted and adapted for cap today here.
Dr. Harrison, one of the book’s several contrib-uting authors, is associate professor and director of the Division of Biomedical Informatics, Depart-ment of Public Health Sciences and Pathology, University of Virginia, Charlottesville.
———————————Requirements and workflow analyses are impor-
tant parts of planning the installation of a new sys-tem and improving existing systems. To effectively support a workflow with an information system, pathologists must understand the key tasks and actors in the work-flow, their association with each other, and the data elements that are captured or communicated as part of that workflow. Document-ing this information accurately is very chal-lenging because it re-quires collaboration between individuals who normally play different roles in differ-ent work domains and often have different vocabularies and assumptions. These communication problems were the impetus for the develop-
ment of the Unified Model-ing Language (UML [www.uml.org]), a standardized set of diagramming techniques de-signed for collaborative doc-umentation and cross-do-main communication of work processes and informa-tion system design concepts. Workflows and information models captured in UML diagrams clarify complex real-world environments and relate directly to infor-mation system requirements and design elements.
The most useful diagrams for clinical laboratory settings are use case models, activity diagrams, and class diagrams. Use case models (above) are very simple and are designed to clearly depict key tasks and actors (human and technological). They are easy to create during a discussion, and they may be supplemented with a brief paragraph providing details for each task. All requirements analysis and workflow redesign should be rooted in use cases.
Activity diagrams (below), also known as swim-lane diagrams, are flow charts in which each actor has a lane, and the sequence of events moves down the chart and across the lanes to indicate the flow of actions and information between the actors. Class diagrams (at right) display data models that map all the data elements used in a workflow and their relationships with each other. Unlike activity diagrams, class diagrams are static; they do not specify a particular sequence of use of the data ele-ments they depict.
The combination of these three diagram types supplemented with some textual description can capture most of the information needed for the discussion and analysis of infor-mation flow in laboratory work processes. Most technical dia-gramming software includes templates for UML diagrams, and dedicated UML diagram-ming software is available com-mercially and in open source.
———————————Laboratory Administration for
Pathologists is $85 for CAP mem-bers and $100 for nonmembers. To order, call 800-323-4040, option 1, and request Pub. No. 312, or down-load an order form at www.cap.org.
CompuGroup Medical introduces cloud-based lab outreach software
CompuGroup Medical US has released Lab-Nexus, a software solution to help hospitals and reference labs with their outreach programs. LabNexus allows laboratories to send orders and review results within a cloud-based system.
LabNexus works independently from Com-puGroup’s LabDaq family of products. The system connects easily to an institution’s labora-tory information system or anatomic pathology system. CompuGroup provides a secure hosting environment for the product.
The LabNexus portal offers order-entry capabil-ity for multiple lab facilities, batch printing, label printing, and customizable lab branding. It can generate preliminary and final reports
March 2012 CAP TODAY / 83 82 / CAP TODAY March 2012
March 2012 page 83 March 2012 page 82
With DigitalScope®, power meets controlFinally, whole slide imaging (WSI) that is fast and easy to use. DigitalScope WSI-viewing technology incorporates advanced controls for an intuitive slide-viewing experience. Test drive it today and see how we’ve raised the bar on digital slide navigation.
Panwithout distracting
screen tiling
Brightness and Contrastfor improved visualization
Magnificationup to 100x
oil immersion
Measureaccurately at
any magnification College of American Pathologists
800-323-4040 | 847-832-7000 option 1
cap.org/DigitalScope
Powered by DigitalScope
Tap into the future of whole slide imagingIntegrating the latest technology with the CAP’s expertise, DigitalScope® enhances proficiency testing and education for your laboratory.
• View cells and the surrounding environment • Maneuver easily, quickly, and fluidly • Experience superior image accuracy and clarity • Benefit from peer consensus of cell identification • Eliminate physical slide management
Start experiencing CAP Surveys powered by DigitalScope.
© 2012 College of American Pathologists. All rights reserved.
Clinician
Transporter /Tube
Phlebotomist
Patient
SpecimenProcessor
Technologist
Figure 6-8. Use CaseDiagram of Preanalytical,Analytical, and Postana-lytical Laboratory Work-flow. Key tasks arecaptured in bubbles, andactors (personnel andtechnical systems) areshown as stick figureslinked to the tasks theyperform. Use case tasksmay be broad, as shownhere, or specific, andanalysis typically pro-gresses from broad tospecific.Task bubbles areoften arranged in se-quence, and brief textualdescriptions may accom-pany diagrams.
Orderlaboratory
test
Viewresult
Accessionand processspecimen
Analyzeand report
result
Drawspecimen
Deliverspecimen
Clinician EHR Phlebotomist Transporter /Tube
LIS SpecimenProcessing
Technologist Figure 6-9. Activity Di-agram of LaboratoryWorkflow. The actorsand tasks from the usecase diagram in Figure 6-8 are mapped in se-quence to an extendedflow chart, with one lanefor each actor. Some ad-ditional actors that werenot shown in the usecases (EHR and LIS) areincluded here to com-plete the informationflow. Activity diagramsshow the flow of tasksand information both intime and across partici-pants and systems.
Order testin EHR
Add tophlebotomy
worklist
Pass orderto LIS
Deliver tolaboratory
Accessionand prep
Drawspecimenand send
Add toanalysisworklist
Analyze andreport
Pass reportto EHRStore
dataView
report
Figure 6-10. Simplified Class Dia-gram for Laboratory Workflow.This diagram shows data elementsand their relationships from thesimple workflow shown in figures6-8 and 6-9. The boxes representclasses (entities for which data willbe collected). Items within theboxes are simple data elements,sometimes called attributes.Classes can also contain otherclasses as complex data elements,and these associations are shownas lines. Multiplicity relationshipsare shown as numbers on the as-sociations; for example, a patientcan have any number of visits (thepermissible range is shown as 0..*,where the asterisk indicates “anynumber”), but a visit can have onlyone patient. The clinician class isused in several settings; it repre-sents the patient’s primary physi-cian, and it also represents thephysician of record for a visit andthe ordering physician for a test.These may be different physicians,but the clinician class provides adata model for all of them.Class di-agrams express data models onlyand do not depict data flow or ac-tion sequences. Definitions: ICD,ICD-9-CM code; MRN, medicalrecord number.
Patient
MRNDemographicsContact
Clinician
IDDemographicsContact
Phlebotomyworklist
Analysisworklist
1
1
1
0..*
Test order
Test nameICDDate / timeComment
Specimen
ContainerID (barcode)Date / timePatient namePhlebotomistAccession #
1
0..*
Visit
DateChief complaint
1
0..*
0..*1
0..*1
11
0..*1
0..*
1
Test result
Analysis dateResultReference rangeFlagComment
Use case diagram of preanalytical, analytical, and postanalytical laboratory workflowUse case tasks may be broad or specific, and analysis typically progresses from broad to specific. Task bubbles are often arranged in sequence, and brief textual descriptions may accompany the diagram.
Activity diagram of laboratory workflowThe actors and tasks from the use case diagram are mapped in sequence to an extended flow chart. Additional actors are included to complete the information flow. Activity diagrams show the flow of tasks and information in time and across participants and systems.
0312_82-85_Newsb-QandA.indd 82 3/7/12 2:07 PM
Essential monthly reporting on the clinical laboratory for lab managers and administrators, physicians, lab directors, and supervisory technologists.
Combined Frequency Discounts:Insertions in CAP TODAY and the Archives of Pathology & Laboratory Medicine combine to determine the earned rate in each publication. Call your representative for details.
Digital Advertising:Print advertisers receive value-added online ads. See our digital edition at http://www.captodayonline.com/mag. In addition, CAP TODAY advertisers have exclusive digital advertising opportunities available. Please see separate CAP TODAY 2013 Digital Rate Card.
Every month CAP TODAY brings essential news to all key decisionmakers responsible for clinical laboratory purchases. This news includes advances in tests and equipment, trends in management and clinical operation, regulatory changes, and finance, plus news about the laboratory improvement programs of the College of American Pathologists.
August 2012 page 42
42 / CAP TODAY
August 2012
New screening guidelines—order amid complexity
Barbara A. Crothers, DO
Ritu Nayar, MD
Cervical cancer screening guide-�
lines were updated recently in
an effort to bring order to the com-
plexity and multiplicity of screen-
ing practices, with special consid-
eration to age and type of testing
used.1 The recommendations also
address followup, primary screen-
ing with HPV testing only, and the
impact of HPV vaccination on
screening. The American Cancer
Society led the effort in collaboration
with the American Society for Col-
poscopy and Cervical Pathology and
American Society for Clinical Pa-
thology. The U.S. Preventive Ser-
vices Task Force has also updated its
cervical cancer screening recommen-
dations, which closely parallel those
from the ACS/ASCCP/ASCP.2
The consensus meeting took
place in November 2011 at the Na-
tional Institutes of Health. Represen-
tatives from 25 organizations with
an interest in women’s health at-
tended. Guidelines were evidence-
based and constructed using the
Grading Recommendations Assess-
ment, Development, and Evaluation
(GRADE) system3 as a framework
for the process. Benefits and harms
were evaluated and strongly influ-
RODOLFO LAUCIRICA, MD, EDITOR
continued on page 44
Ann T. Moriarty, MD
“What a great case!” my pathologist ex-�
claimed as she first reviewed all
10 of my parts under the microscope. I had
been growing slowly, in a warm, subcu-
taneous location, until my life changed
abruptly. I suddenly found myself flow-
ing through a small caliber stainless steel
tunnel as I was rapidly aspirated, smeared be-
tween two glass slides, and unceremoniously
dunked into ethanol. Part of me was left out to
dry. After being delivered to a well-lit, organized
laboratory, I was carefully stained with a Papani-
colaou stain that left me a riotous kaleidoscope of
green, purple, pink, and orange, and given a
matching modified Giemsa stain that gave me a
general purple hue. After that, I had been covered
in glass after being swathed in a permanent mount-
ing media. I was gorgeous (if I do say so myself)
and apparently worth a second look. I was passed
around the department so all the cytologists could
appreciate my features.
After my debut, I was carefully filed into a
study set where I languished in the darkness for
years. After 10 years, I was scheduled to be dis-
carded with all my neighbors, to make room for
a new generation. My pathologist was pained to
see me leave, as I had managed to increase the
expertise of the entire laboratory. But the time had
come for me to move to glass disposal.
At the last minute, I was carefully culled from
the discard stack, packaged lovingly along with
my history before I became glass, and sent by mail
to a wonderful world called the College of Ameri-
can Pathologists. It was at the CAP that I came into
my true purpose as glass. First, I was given a
number. Then I was reviewed by a CAP cytotech-
nologist who understood what a treasure I was
(and I had been stored so well that I had not faded
or aged at all over 10 years). The cytotechnologist
took all my information and me along with about
2,000 other interesting new neighbors to
something called a Cytopathology Committee
meeting. Over the course of four days, at least three
American-Board-of-Pathology–certified anatomic
pathologists scrutinized me and my compatriots.
They unanimously agreed that I was a truly great
case and was going to play a role in three different
programs for the CAP.
First, I was going to get some enhancements.
The special stains performed on my cell block were
going to be photographed and electronically stored
in the computer system at the CAP. Then all my
parts were going to be digitized so I could be vir-
tual glass and immortalized as a great case, in case
my parts became too faded or (heaven help me)
broken. Once I was sent to virtual heaven, I would
circulate as a pair to as many laboratories that
subscribed to an educational interlaboratory com-
parison program. Any cytotechnologist or patholo-
gist who received me could go online and see my
special stains. After successfully identifying me
and understanding the importance of my ancillary
stains, they could answer a short scored assess-
ment and receive educational credits to maintain
their certification or fulfill their educational re-
quirements for credentialing or licensure. I was
proudly teaching in my field, once again.
The most exciting turn of events happened with
my virtual reincarnation. I was released as an on-
line challenge that could be viewed by hundreds
of people simultaneously. In that life, the
viewers saw me on their computer screens
and got to make a general diagnosis and
then to choose the special stains accompa-
nying me. It was like being reborn with
each viewing. The cytologists got to “work
me up” just like my original brilliant patholo-
gist had when she first encountered me. Once they
had all the available ancillary information, the
participants would make the most specific diag-
nosis they could. Then they have the opportunity
to prove they learned from me by passing an as-
sessment. I was a great teacher.
Not only am I now electronically immortal, but
I have gone on to have an impact on the whole
field of pathology, as more and more people have
had a chance to view my parts. My original pa-
thologist was brilliant to have shared me with her
colleagues in the United States and internation-
ally. My glass has been to 18 different countries
and my virtual self has beamed all around the
world. Who would have thought that a mere
lump could have had such a great legacy? I am a
truly great case.
If you have great cases to share with the world,
be a brilliant pathologist and share them. Dona-
tions for the nongynecologic and fine-needle as-
piration glass slide and virtual programs are be-
ing accepted (gynecologic cases welcome too).
Donation forms and instructions can be obtained
from the CAP Web site or by calling Larry Flen-
noy at 847-832-7275 or 800-323-4040 ext. 7275.
Donors are reimbursed for their clerical expenses
when donating slides to any CAP program.
Dr. Moriarty, chair of the CAP Cytopathology Com-
mittee, is in the Department of Pathology, AmeriPath
Indiana, Indianapolis.
My life as glass‘I was great and gorgeous’
Gil Adams
0812_42-48_Cytopath.indd 42
8/8/12 2:54 PM
Distribution
Readers* All key decisionmakers, no excess
Pathologists and Laboratory Directors 19,000Laboratory Managers and Laboratory Administrators 6,000Chief Techs; Section Managers/Supervisors of Chemistry, Hematology, Microbiology, Immunology, Blood Bank, Cytology, or Histotechnology
20,000
Hospital Administrators 5,000
TOTAL 50,000* This listing is specially grouped for convenience. See the BPA Publisher’s Statement for detailed circulation data.
Independent research studies show that CAP TODAY is #1 in total ad exposures for the marketplace. PERQ/HCI and/or Analytical Research Service Inc.
have completed recent studies on pathologists (PERQ/HCI), clinical lab directors, lab managers and administrators, and purchasing influence. In 2012, CAP TODAY carried more advertising than any other book in the field.
April 2012 Pathology/Laboratory Medicine/Laboratory Management
Vol. 26 No. 4
For respiratory virus detection, a golden ageWilliam Check, PhDWhen it comes to molecular detection of res- piratory viruses, laboratorians today have an embarrassment of riches. “This talk would have been very different five years ago,” Christine C. Ginocchio, PhD, MT(ASCP), said at last year’s Association for Molecular Pathol-ogy meeting at the outset of her review of multianalyte platforms for detecting respiratory viruses. The advances in this area have been substantial, she told CAP TODAY recently, adding: “There has been an explosion of molecu-lar assays, both IVD cleared and not.” Dr. Ginocchio, who is senior medical director and chief, Division of Infec-tious Disease Diagnostics, Depart-ment of Pathology and Laboratory Medicine, North Shore-LIJ Health System Laboratories in New York, calls this “an excellent time to be working in infectious diseases.”“We now have several FDA-cleared assays for detection of mul-tiple respiratory viruses in the same sample, and they have a wide range of multiplexity,” she says.With so many platforms avail-able—Dr. Ginocchio discussed 13, seven cleared and six in trials—and with such a wide range in multiplexity, turnaround time, throughput, degree of automation, and cost, how is a lab to know which system best fits its
needs? Or, for that matter, whether it even needs a multiplex platform? Laboratorians might follow the real estate mantra: “Location, location, location.” “It would seem that use of the new viral panels would be a no-brainer, but that is not the case,” says Richard B. Thomson, PhD, medical director of the microbiology laboratories at Evanston (Ill.) Hospital of NorthShore Uni-
versity Health System and clinical professor of pathology, University of Chicago. Reagent expense is a major reason, Dr. Thomson told CAP TODAY, as is capital expense. That makes it crucial to think about where specimens are coming from. “Right now there are many different outpatient and inpa-tient settings where viral diagnostics are used,” Dr.
Contaminated blood cultures: taking bold steps to lower ratesAnne PaxtonA frequent failure that is costly for a hospital can rightly be called a serious problem, but when the failure stems from avoidable er-ror, it’s especially troub ling. Blood culture contamination, a cause of false-positive results, diagnostic er-rors, and frustration, is one such fail-ure, says Dennis Ernst, MT(ASCP), executive director of the Center for Phlebotomy Education, Corydon, Ind. While high rates of blood culture contamination are common, they don’t have to be permanent, he says. Institutions can slash their contamination rates to two percent or less by mustering the will to tackle the causes. Ernst compares blood culture contamination to
The many new and varied assays for molecular detection of respiratory viruses make today “an excellent time to be working in infectious diseases,” says Dr. Christine Ginocchio.
Jenn
ifer
Altm
an
Two for the road with companion diagnosticsKaren TitusForget about the emerging world of personalized medicine. It’s now a merging world, one in which pharmaceutical companies and diag-nostics firms are shaking hands on any number of deals to develop drugs
and companion tests for oncology. Consider these recent partnership announcements: • Abbott and Pfizer • Pfizer and Ventana • Ventana and Bayer • Life Technologies and GSK • Roche and, well, Roche
Such unions may not count as kumbaya moments for these medical behemoths, but they do point to bud-ding awareness of how to pull drugs and tests alongside each other and before the FDA.Along the way, both pharma and diagnostics firms have encountered a few jolts. So has the FDA. This may have slowed things down over the years, though many in the field mere-ly shrug when asked about the pace at which drug-test pairs have come to market. Scientific knowledge may grow quickly, but putting it into a drug and onto a test platform doesn’t happen overnight.
Mara Aspinall, president/CEO, Ventana Medical Systems, has watch-ed personalized medicine unfold in a
TM
continued on page 50
continued on page 12
continued on page 28
April 2012 page 1
LPL software companies plug the gaps, hold their own
Page 3
Laboratory-provider links software, pages 71–820412_1_MultPx-APcan-Phleb2.indd 1
4/9/12 12:42 PM
CAP TODAY is available via mobile device
Tabulation does not represent an endorsement by the College of American Pathologists.
Blood bank information systems
September 2010 Page 71
Tabulation does not represent an endorsement by the College of American Pathologists.
Blood bank information systems
70 / CAP TODAY
September 2012
October 2011 Page 70
September 2012
CAP TODAY / 71
Part 1 of 5
Blood Bank Computer SystemsCerner Corp.
Haemonetics Software Solutions
Brian Forbis [email protected] Walker [email protected] Scott Dustin [email protected]
1002 15th St. SW, Suite 1202800 Rockcreek Parkway
4925 Robert J. Mathews Parkway, Suite 100
See accompanying article on page xxAuburn, WA 98001
Kansas City, MO 64117El Dorado Hills, CA 95762
See captodayonline.com/productguides for an interactive version of guide 888-738-2227 www.bbcsinc.com816-201-2854 www.cerner.com
916-404-8415 www.haemonetics.com
Name of blood bank systemBlood Bank Control System Primary Application (BBCSP) Cerner Millennium PathNet Blood Bank Transfusion ElDorado Donor
First ever/Most recent blood bank system installation* 1987/July 20121986/July 2012
1996/June 2012
Last major product release for version of product featured July 2012
January 2012June 2012
Total number of contracts for sites operating blood bank system 30
388†
26
•Contracts for U.S. hospitals with donor and transfusion services 1
25†
14
•Contracts for U.S. hospitals with transfusion services only 0
363†
0
•Contracts for U.S. regional blood centers with donor services only 21
0
4
• Contracts for U.S. regional blood centers with donor and transfusion services 5
0
2
•Contracts for foreign hospitals and regional blood centers 0
70† (Australia, Canada, England, Guam, Saudi Arabia, Singapore, Egypt, United Arab Emirates) 4 (Egypt, Puerto Rico, Guam, Dubai)
•Contracts for other sites
3 (2 medical research facilities; 1 hospital with donor service only) 0
2 (hospitals with donor service only)
Number of contracts signed between June 2011–June 2012 1
52† (for calendar-year 2011)4
Total number of sites operating blood bank system123
388
14
Number of sites that went live between June 2011–June 2012 1
48
3
Installations not yet live (hospitals/regional blood centers/others) 1 (0/1/0)
34 (34/0/0)
17 (10/4/3)
Percentage of installations that are standalone blood bank systems 100%
0
100%
No. of employees in entire company/Dedicated solely to blood bank systems development, installation, support 30/25
10,072 (as of January 2012)/4202,374/338
Number of different versions of this software installed12
2
4
•Versions of product in field covered by FDA 510(k) clearance BBCSP 5.2.2, 5.3, 5.3.1, 5.3.2, 5.3.3, 5.3.4, 5.3.5, 5.3.6, 5.3.7, 5.3.8, 5.4, 5.4.1 Cerner Classic PathNet, Cerner Millennium PathNet 2.0, 2.1, 2.2, 2.3
•Versions of product that did not require FDA 510(k) clearance 0
0
0
Range in number of user workstations in live sites (average) 10–200 (average, 40)—
6–40 (average, 15)
Server platforms
IBM iSeries
IBM, Hewlett-Packard—
PC or workstation platformsIBM-compatible workstation, PCs
Microsoft Windows locally or via Citrix thin client Windows
Software programming language(s)RPG 400, Java
Java, Visual Basic, C++, C#, Visual CC#
Operating system(s)
OS/400
HP-UX, AIX, VMSWindows
Databases and tools
IBM DB2
Oracle
Oracle, Crystal Reports
Features (listed as percentage of live installs or based on availability)•Biometric ID of donors and/or patients
installed
available but not tracked—
•Full support of ISBT 128 unit labelinginstalled
100%
100%
•Bar-code reading of donor and unit informationinstalled
100%
100%
•Unit inventory
installed
100%
100%
•Autologous and directed unit trackinginstalled
100%
100%
•Direct entry of test resultsinstalled
100%
100%
•Crossmatch results
installed
99%
available via Haemonetics’ SafeTrace Tx
•Electronic crossmatch decisionmakinginstalled
>50%
available via Haemonetics’ SafeTrace Tx
•Antigen typing
installed
99%
100%
•Integrated bedside check for transfusion using positive patient ID not available
1%
available via Haemonetics’ BloodTrack
•Track all steps in production of productinstalled
99%
100%
•Print donor unit labels—bar codedinstalled
99%
100%
•Interface with blood irradiator or centrifugesnot available
not available
—
•Centralized transfusion service capabilityinstalled
available
available via Haemonetics’ SafeTrace Tx
•Donor recruitment and managementinstalled
available through partnership with a third party available via Haemonetics’ eDonor
•Donor questionnaire
installed
available through partnership with a third party available via Haemonetics’ Donor Doc
•Mobile scheduling
installed
available through partnership with a third party available via Haemonetics’ Hemasphere/eDonor
•Laptop-based mobile donor registration moduleinstalled
available through partnership with a third party installed
•Source or recovered plasma managementinstalled
available through partnership with a third party installed
•Accounts receivable
installed
15%
installed
•Management reports
installed
100%
100%
•Ad hoc report writer
installed
100%
available via Haemonetics’ ElDorado Donor Report Server
•Quality control managementinstalled
25%
available via Haemonetics’ ElDorado Control
•Collection management
installed
100%
100%
Interfaces to automated donor infectious disease testing instruments yes
yes
yes
Interfaces to automated ABO/Rh/antibody screening instruments yes
yes
yes
Electronic interface to bedside patient ID system from other vendors no
no
no
Languages (other than English) offered on systemnone
German, French, Spanishnone
Recommended tools to help clients validate their systems validation protocols, flow charts, risk mitigation online portal, installation and verification instructions, others
certification guidelines, design and build instructions and online help files for end-users, blood bank validation services for organizations that want to outsource their validation activities
validation templates and validation test plan for safety critical control checks, validation services through Haemonetics’ PeopleMed subsidiary
System available via ASP or cloud-based data centeryes
yes
yes
System provides indexed field in each test definition for LOINC code no
yes
no
Provide LOINC dictionary for each new installationno
yes
no
Other vendors to which software has a lab system-related interface Haemonetics Software Solutions, Ortho Clinical Diagnostics Haemonetics Software Solutions—
User group
yes (meets via Webinar and in person)yes (meets via Webinar and in person)
yes (meets via Webinar and in person)
Source code
no
no
escrow
Methods by which users can tailor blood bank system in their own setting
ad hoc query tools, user-defined interfaces, dictionary settings, BBCS configuration options user programming, ad hoc query tools, user-defined interfaces, dictionary settings, others user programming, ad hoc query tools, user-defined interfaces, table settings
Cost for software modifications to comply with federal regs and laws standard (no charge)standard (no charge)
standard (no charge)
Total cost for smallest standalone blood bank system installation** —
—
—
Total cost for largest standalone blood bank system installation** —
—
—
Total incremental cost for smallest blood bank configuration installed** —
—
—
Total incremental cost for largest blood bank configuration installed** —
—
—
Distinguishing features (supplied by company)
*based on July 2012 survey deadline**total cost includes hardware, software, installation, and trainingNote: a dash in lieu of an answer means company did not answer question or question is not applicable
• over 25 years of consistent client-driven design• provides an entirely integrated, real-time, fully customizable electronic questionnaire module capable of utilizing touch-screen/tablet technology, supporting a fully paperless donor room• controls within BBCS applications allow managers to be more effective by minimizing distractions and controlling risk
• positive patient ID capabilities at the patient bedside, from specimen collection to transfusion administration• increased efficiencies through such capabilities as mother-baby linking, online secondary review of results, QC specific to blood bank workflows, etc.• support for blood bank within a single lab information system and electronic medical record architecture
†sites, not contracts
• extensive safety checks throughout system with a commitment to compliance• open workflow with extensive user-defined, table-based rules• Service 360 commitment to ensure quality customer implementation and support experience
Product guide editors: Raymond D. Aller, MD, and Hal Weiner
Part 2 of 5
Haemonetics Software SolutionsMcKesson
Medical Information Technology
Scott Dustin [email protected] Joseph R. Stabile [email protected] Paul Berthiaume [email protected]
4925 Robert J. Mathews Parkway, Suite 100 5995 Windward ParkwayMeditech Circle
El Dorado Hills, CA 95762Alpharetta, GA 30005
Westwood, MA 02090
See captodayonline.com/productguides for an interactive version of guide 916-404-8415 www.haemonetics.com404-338-4363 www.mckesson.com/laboratory 781-821-3000 www.meditech.com
Name of blood bank systemSafeTrace Tx†
Horizon Blood Bank†
Blood Bank System–6.0
First ever/Most recent blood bank system installation* 1996/July 20122004/June 2012
1981/June 2012
Last major product release for version of product featured March 2012
March 2011
January 2011
Total number of contracts for sites operating blood bank system 353
113
81†
•Contracts for U.S. hospitals with donor and transfusion services 19
0
—
•Contracts for U.S. hospitals with transfusion services only 312
110
—
•Contracts for U.S. regional blood centers with donor services only 0
0
—
• Contracts for U.S. regional blood centers with donor and transfusion services 10
0
—
•Contracts for foreign hospitals and regional blood centers 9 (Botswana, Puerto Rico, Canada, Guam, Ethiopia) 3 (Canada)
5† (Canada)
•Contracts for other sites
3 (regional donor centers with transfusion only) 0
—(acute care, behavioral health, critical access, long-term care, rehabilitation, others)
Number of contracts signed between June 2011–June 2012 47
0
1†
Total number of sites operating blood bank system444
174
118
Number of sites that went live between June 2011–June 2012 46
17
53
Installations not yet live (hospitals/regional blood centers/others) 59 (59/0/0)
13 (13/0/0)
61 (60/0/1)
Percentage of installations that are standalone blood bank systems 100%
0
0
No. of employees in entire company/Dedicated solely to blood bank systems development, installation, support 2,374/338
44,000/328 (from Haemonetics Software Solutions) 3,830/202 (for all LIS-related applications)
Number of different versions of this software installed6
5
1
•Versions of product in field covered by FDA 510(k) clearance SafeTrace Tx 3.4, 3.4.1, 3.5. 3.5.1, 3.6, 3.7 SafeTrace Tx 3.2, 3.3, 3.4, 3.5, 3.6Meditech 6.0
•Versions of product that did not require FDA 510(k) clearance 0
0
0
Range in number of user workstations in live sites (average) 1–105 (average, 7)1–7 (average, 2)
—
Server platforms
Windows-based servers, Intel based (determined by Oracle) Windows-based serversminimal 64-bit 2 GHz+ dual core processors operating Microsoft Windows Server 2003/2008 Standard Edition
PC or workstation platformsWindows
Windows
Windows PCs with 2 GHz or higher Intel or equivalent processor and minimum 2 GB RAM
Software programming language(s)Delphi
Delphi
Meditech-developed programming language
Operating system(s)
Windows
Windows
servers: Windows 2003/2008 SE; clients: Windows 2000 Professional, XP, XP Tablet, Vista, 7
Databases and tools
Oracle, Crystal ReportsOracle
Meditech Database Management System
Features (listed as percentage of live installs or based on availability)•Biometric ID of donors and/or patients
not available
not available
installed
•Full support of ISBT 128 unit labeling100%
installed
100%
•Bar-code reading of donor and unit information100%
installed
100%
•Unit inventory
100%
installed
100%
•Autologous and directed unit tracking100%
installed
100%
•Direct entry of test results100%
installed
100%
•Crossmatch results
100%
installed
100%
•Electronic crossmatch decisionmaking70%
installed
installed
•Antigen typing
100%
installed
installed
•Integrated bedside check for transfusion using positive patient ID available via a third partynot available
installed
•Track all steps in production of product100%
installed
100%
•Print donor unit labels—bar codedinstalled
installed
installed
•Interface with blood irradiator or centrifugesinstalled
installed
installed
•Centralized transfusion service capability100%
installed
100%
•Donor recruitment and managementavailable via Haemonetics’ eDonor
available via a third partyinstalled
•Donor questionnaire
available via Haemonetics’ ElDorado Donor Doc available via a third partyinstalled
•Mobile scheduling
available via Haemonetics’ Hemasphereavailable via a third party
installed
•Laptop-based mobile donor registration moduleavailable via Haemonetics’ ElDorado Donor available via a third party
installed
•Source or recovered plasma managementavailable via Haemonetics’ ElDorado Donor available via a third party
installed
•Accounts receivable
available via a third partyavailable via a third party
installed
•Management reports
100%
installed
100%
•Ad hoc report writer
available via a third partyinstalled
100%
•Quality control managementinstalled
installed
—
•Collection management
available via Haemonetics’ ElDorado Donor available via company’s LISinstalled
Interfaces to automated donor infectious disease testing instruments no
no
yes
Interfaces to automated ABO/Rh/antibody screening instruments yes
yes
yes
Electronic interface to bedside patient ID system from other vendors yes
no
no
Languages (other than English) offered on systemnone
none
Spanish in development
Recommended tools to help clients validate their systems validation guidelines, templates and test plan for critical control checks, validation services through Haemonetics’ PeopleMed subsidiary
validation services and guidelines from recommended third party testing scripts available on company Web site through Meditech validation guides
System available via ASP or cloud-based data centeryes
yes
no
System provides indexed field in each test definition for LOINC code no
no
yes
Provide LOINC dictionary for each new installationno
no
no
Other vendors to which software has a lab system-related interface McKesson, Cerner, Siemens, GE, CPSI, Meditech, Keane, SCC Soft Computer, Sysmex, Allscripts, Orchard, Sunquest, Quality Software Systems
Siemens, Meditech, Epic, Cerner (all interface to McKesson Horizon Lab or Paragon and then to Horizon Blood Bank)
—User group
yes (meets via Webinar and in person)yes (in person only)
yes (meets via Webinar and in person)
Source code
escrow
escrow
escrow
Methods by which users can tailor blood bank system in their own setting
ad hoc query tools, user-defined interfaces, table settings ad hoc query tools, dictionary settingsad hoc query tools, user-defined interfaces, dictionary settings, customer-defined screens, desktop preferences, rules-based logic
Cost for software modifications to comply with federal regs and laws standard (no charge)—
standard (no charge)
Total cost for smallest standalone blood bank system installation** —
—
—
Total cost for largest standalone blood bank system installation** —
—
—
Total incremental cost for smallest blood bank configuration installed** —
—
—
Total incremental cost for largest blood bank configuration installed** —
—
—
Distinguishing features (supplied by company)
*based on July 2012 survey deadline**total cost includes hardware, software, installation, and trainingNote: a dash in lieu of an answer means company did not answer question or question is not applicable
• extensive safety checks throughout system with a commitment to compliance• patents for Patient-At-A-Glance bar, antigen-antibody identification, and central transfusion service functionality• Service 360 commitment to ensure quality customer implementation and support experience
†also marketed by McKesson as Horizon Blood Bank
• extensive safety checks throughout system with a commitment to compliance• patents for Patient-At-A-Glance bar, antigen-antibody identification, and central transfusion service functionality• Service 360 commitment to ensure quality customer implementation and support experience
†also marketed by Haemonetics as SafeTrace Tx
• integrated component of Meditech EHR, providing a seamless exchange of data across the continuum• features centralized access to common routines and reports via roles-based desktops• blood bank and patient care and patient safety solu-tions fully integrated, fostering the sharing of blood bank unit and patient data between the products†sites, not contracts
8
Arch
ives of Path
ology & L
aboratory Med
icine
Au
gust 2012
Volu
me 136, N
um
ber 8
Pages 841–972
August 2012Special Section—2011 New Frontiers in Pathology
“Starry-Sky” Pattern and High Proliferative Fraction in an Aggressive B-Cell Lymphoma

2013 CAP TODAY Media Planner
2013 Issues
Bonus Distribution
Instrument and Software System Product Guides Editorial Forecast*
JanuaryCervical health/thyroid awareness
Coagulation analyzers Start here For planning acquisitions of new systems, most laboratories begin here. Detailed 40- to 50-point comparative charts provide criteria essential to lab directors, administrators, and managers.
Product guide listings, an editorial feature, are always free and companies approve their listings.
Full-page ads can be placed adjacent to company listings for 12 months’ worth of maximum impact.
Digital editions showcase product guides electronically for convenient reference, to save, and to distribute to colleagues.
Interactive guides allow labs and companies to make custom comparisons.
The publication 56 percent of respondents in a leading, independent study chose cap today as the one publication most important to their job. The second-place score? Only 17 percent.
AD-MARK AD-MARK is a quarterly, cover-to-cover, readership and advertising research study.
Advertise in these quarterly issues, get a comparative report of every article and ad in the issue—priceless marketing intelligence!
For 2013, we’ve highlighted relevant ‘disease awareness’ items under each month. We aim to assemble relevant PR and other items in one place— both to inform our readers and underscore the crucial role played by pathologists and labs in the gamut of disease.
Pharmacogenomics program—coagulationPhlebotomy Cytopathology Flu season forecast
FebruaryAmerican heart month
USCAP (Baltimore)HIMSS (New Orleans)
Anatomic pathology softwareLab automation systems and workcells
Molecular pathologyBlock and slide trackingTesting strategies for CVD assessment
MarchColorectal cancer awareness
AACR (Washington, DC)CLMA (Orlando)ACP (San Francisco)
MiddlewareGlucose analyzers
Molecular pathology—colonPhlebotomyPOC update Microbiology—best practices
AprilIrritable bowel syndrome awarenessHead and neck cancer awareness
Clinical Virology Symposium (Daytona Beach, Fla.)Executive War College (New Orleans)
Lab portals Viral load testing—CMV, HCVLab outreach toolsLung cancer
MayAllergy-asthma/Hepatitis awareness
ASM (Denver)ASCO (Chicago)
POC coagulation analyzersBilling systems
Molecular pathologyInfectious disease of lower respiratory tractCytopathology
JuneMelanoma awarenessScleroderma awareness
AACC (preview issue) Immunoassay analyzers Test utilizationThyroid testingESR testing todayCompanion diagnostics—Town v. Gown
JulyInternational Group B Strep awarenessBladder cancer awareness
AACC (Houston) Chemistry analyzersPositive patient ID
Heart failure—role of biomarkersNext-gen sequencingQuality control
AugustSpinal muscular atrophy awareness
Pathology Informatics (Pittsburgh)
Blood gas analyzersPOC chemistry/immuno instruments
Group practice labs todayLIS-EMR connectionsCytopathology
SeptemberLeukemia and lymphoma awarenessProstate cancer awareness
NSH (Providence, RI)AABB (Denver)DPA Pathology Visions (San Antonio)
Blood bank information systems TransfusionHistologyDigital pathology update HPV
OctoberBreast cancer awareness
CAP ’13 (Orlando)ASC (Orlando)AMP (preview issue)
Automated molecular platforms Reference lab strategiesMolecular pathology—breastBacterial resistance
NovemberDiabetes awarenessLung cancer awareness
AMP (Phoenix)ASH (New Orleans)
Next-gen sequencing instrumentsLaboratory information systems
Next-gen sequencingMolecular pathology—head and neckLIS
DecemberWorld AIDS Day Dec.1
Hematology analyzers Body fluid analysisHIV testing advancesBrain cancers
What’s inside a full issue:20–25 editorial items, highlighted by in-depth, front-cover features with long
story continuations that support back-and-forth reading patterns—readers return to the front cover up to three times.
Real-world interviews with experts from forefront institutions who discuss up-to-the-minute technologies (some new, some tried and true) in anatomic, clinical, and molecular pathology and dozens of subspecialties.
Clinical and anatomic abstracts of relevant peer-reviewed papers—columns that receive extremely high readership scores every month.
A special cytopathology section featuring what’s new.
A monthly Newsbytes column of software news—a great draw for IT-related products.
A Q & A column covering many diagnostic disciplines. Placed at the back of the magazine, this section is one of our best read.
Special Laboratory Accreditation Program updates.*Two weeks before reservation deadlines, CAP TODAY sales representatives can forecast major cover stories linked to significant meetings and bonus distribution issues.
AD-MARK
AD-MARK
AD-MARK
AD-MARK
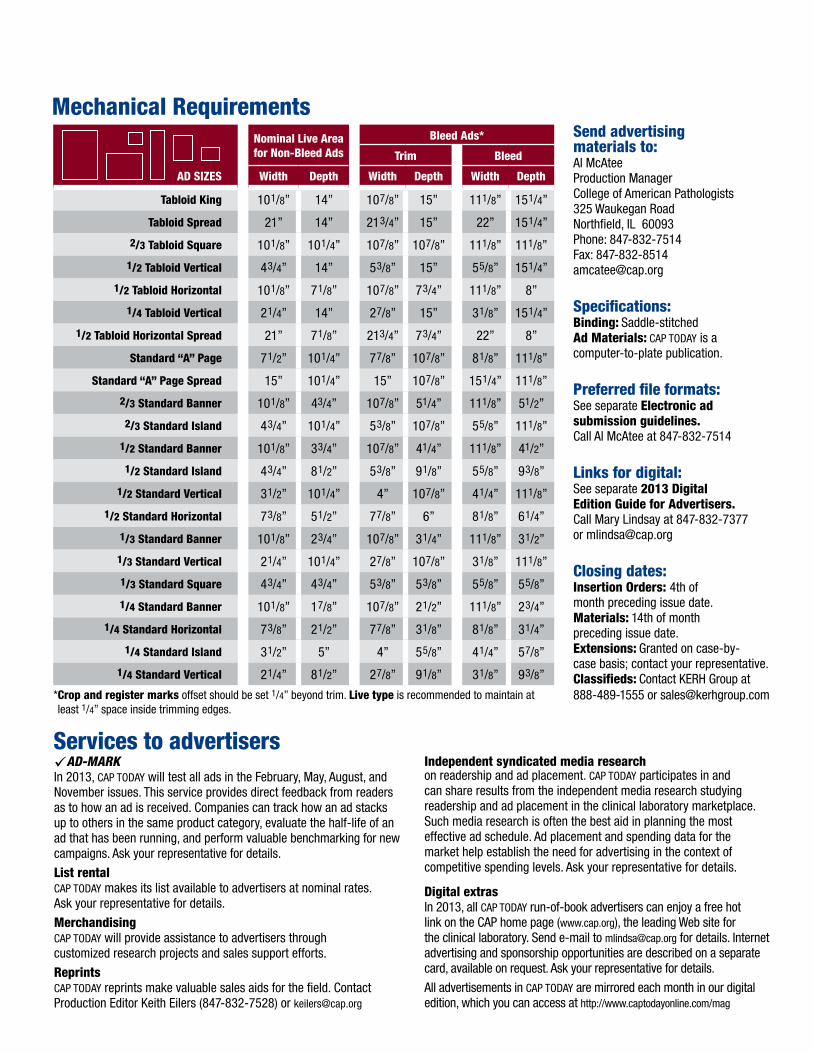
Nominal Live Area for Non-Bleed Ads
Bleed Ads*
Trim Bleed
AD SIZES Width Depth Width Depth Width Depth
Tabloid King 101/8” 14” 107/8” 15” 111/8” 151/4”
Tabloid Spread 21” 14” 213/4” 15” 22” 151/4”
2/3 Tabloid Square 101/8” 101/4” 107/8” 107/8” 111/8” 111/8”
1/2 Tabloid Vertical 43/4” 14” 53/8” 15” 55/8” 151/4”
1/2 Tabloid Horizontal 101/8” 71/8” 107/8” 73/4” 111/8” 8”
1/4 Tabloid Vertical 21/4” 14” 27/8” 15” 31/8” 151/4”
1/2 Tabloid Horizontal Spread 21” 71/8” 213/4” 73/4” 22” 8”
Standard “A” Page 71/2” 101/4” 77/8” 107/8” 81/8” 111/8”
Standard “A” Page Spread 15” 101/4” 15” 107/8” 151/4” 111/8”
2/3 Standard Banner 101/8” 43/4” 107/8” 51/4” 111/8” 51/2”
2/3 Standard Island 43/4” 101/4” 53/8” 107/8” 55/8” 111/8”
1/2 Standard Banner 101/8” 33/4” 107/8” 41/4” 111/8” 41/2”
1/2 Standard Island 43/4” 81/2” 53/8” 91/8” 55/8” 93/8”
1/2 Standard Vertical 31/2” 101/4” 4” 107/8” 41/4” 111/8”
1/2 Standard Horizontal 73/8” 51/2” 77/8” 6” 81/8” 61/4”
1/3 Standard Banner 101/8” 23/4” 107/8” 31/4” 111/8” 31/2”
1/3 Standard Vertical 21/4” 101/4” 27/8” 107/8” 31/8” 111/8”
1/3 Standard Square 43/4” 43/4” 53/8” 53/8” 55/8” 55/8”
1/4 Standard Banner 101/8” 17/8” 107/8” 21/2” 111/8” 23/4”
1/4 Standard Horizontal 73/8” 21/2” 77/8” 31/8” 81/8” 31/4”
1/4 Standard Island 31/2” 5” 4” 55/8” 41/4” 57/8”
1/4 Standard Vertical 21/4” 81/2” 27/8” 91/8” 31/8” 93/8”
AD-MARK In 2013, CAP TODAY will test all ads in the February, May, August, and November issues. This service provides direct feedback from readers as to how an ad is received. Companies can track how an ad stacks up to others in the same product category, evaluate the half-life of an ad that has been running, and perform valuable benchmarking for new campaigns. Ask your representative for details.
List rental CAP TODAY makes its list available to advertisers at nominal rates. Ask your representative for details.
Merchandising CAP TODAY will provide assistance to advertisers through customized research projects and sales support efforts.
Reprints CAP TODAY reprints make valuable sales aids for the field. Contact Production Editor Keith Eilers (847-832-7528) or [email protected]
Independent syndicated media research on readership and ad placement. CAP TODAY participates in and can share results from the independent media research studying readership and ad placement in the clinical laboratory marketplace. Such media research is often the best aid in planning the most effective ad schedule. Ad placement and spending data for the market help establish the need for advertising in the context of competitive spending levels. Ask your representative for details.
Digital extras In 2013, all CAP TODAY run-of-book advertisers can enjoy a free hot link on the CAP home page (www.cap.org), the leading Web site for the clinical laboratory. Send e-mail to [email protected] for details. Internet advertising and sponsorship opportunities are described on a separate card, available on request. Ask your representative for details.
All advertisements in CAP TODAY are mirrored each month in our digital edition, which you can access at http://www.captodayonline.com/mag
Mechanical RequirementsSend advertising materials to:Al McAteeProduction ManagerCollege of American Pathologists325 Waukegan RoadNorthfield, IL 60093Phone: 847-832-7514 Fax: [email protected]
Specifications: Binding: Saddle-stitched Ad Materials: CAP TODAY is a computer-to-plate publication.
Preferred file formats: See separate Electronic ad submission guidelines. Call Al McAtee at 847-832-7514
Links for digital: See separate 2013 Digital Edition Guide for Advertisers. Call Mary Lindsay at 847-832-7377or [email protected]
Closing dates: Insertion Orders: 4th of month preceding issue date. Materials: 14th of month preceding issue date. Extensions: Granted on case-by- case basis; contact your representative. Classifieds: Contact KERH Group at 888-489-1555 or [email protected]
Services to advertisers
* Crop and register marks offset should be set 1/4” beyond trim. Live type is recommended to maintain at least 1/4” space inside trimming edges.