
2012 W S P II: T ETHNOGERIATRICS - Stanford...
13
SGEC Webinar Handouts 8/6/12 This work is licensed under a Creative Commons Attribution 3.0 Unported License . 1 2012 WEBINAR SERIES PART II: TACKLING THE TOUGH TOPICS IN ETHNOGERIATRICS Please visit our website for more informa�on h�p://sgec.stanford.edu/ 2012 WEBINAR SERIES PART II: TACKLING THE TOUGH TOPICS IN ETHNOGERIATRICS Sponsored by Stanford Geriatric Educa�on Center in conjunc�on with American Geriatrics Society, California Area Health Educa�on Centers, & Na�vidad Medical Center Please visit our website for more informa�on h�p://sgec.stanford.edu/ CULTURAL HUMILITY:THE NEXT LEVEL OF CULTURAL COMPETENCE Dr. Nancy Hikoyeda, DrPH, MPH, Associate Director, Stanford GEC August 9 2012 This project is/was supported by funds from the Bureau of Health Professions (BHPr), Health Resources and Services Administra�on (HRSA), Department of Health and Human Services (DHHS) under UB4HP19049, grant �tle: Geriatric Educa�on Centers, total award amount: $384,525. This informa�on or content and conclusions are those of the author and should not be construed as the official posi�on or policy of, nor should any endorsements be inferred by the BHPr, HRSA, DHHS or the U.S. Government.
Transcript of 2012 W S P II: T ETHNOGERIATRICS - Stanford...

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 1
2012 WEBINAR SERIES PART II: TACKLING THE TOUGH TOPICS IN
ETHNOGERIATRICS
Please visit our website for more informa�on -‐ h�p://sgec.stanford.edu/
2012 WEBINAR SERIES PART II: TACKLING THE TOUGH TOPICS IN
ETHNOGERIATRICS
Sponsored by Stanford Geriatric Educa�on Center in conjunc�on with American Geriatrics Society, California Area Health Educa�on Centers,
& Na�vidad Medical Center
Please visit our website for more informa�on -‐ h�p://sgec.stanford.edu/
CULTURAL HUMILITY: THE NEXT LEVEL OF
CULTURAL COMPETENCE
Dr. Nancy Hikoyeda, DrPH, MPH, Associate Director, Stanford
GEC August 9 2012
This project is/was supported by funds from the Bureau of Health Professions (BHPr), Health Resources and Services Administra�on (HRSA), Department of Health and Human Services (DHHS) under UB4HP19049, grant �tle: Geriatric Educa�on Centers,
total award amount: $384,525. This informa�on or content and conclusions are those of the author and should not be construed as the official posi�on or policy of, nor should any endorsements be inferred by the BHPr, HRSA, DHHS or the U.S. Government.

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 2
“Cultural Humility: The Next Level of Cultural Competence” Natividad Medical Center CME Committee Planner Disclosure Statements:
The following members of the CME Committee have indicated they have no conflicts of interest to disclose to the learners: Kathryn Rios, M.D.; Janet Bruman; Tami Robertson; Christina Mourad and Nobi Riley
Stanford Geriatric Education Center Webinar Series Planner Disclosure Statements:
The following members of the Stanford Geriatric Education Center Webinar Series Committee have indicated they have no conflicts of interest to disclose to the learners: Gwen Yeo, Ph.D. and Kala M. Mehta, DSc, MPH
Faculty Disclosure Statement:
As part of our commercial guidelines, we are required to disclose if faculty have any affiliations or financial arrangements with any corporate organization relating to this presentation. Dr. Nancy Hikoyeda has indicated she has no conflicts of interest to disclose to the learners, relative to this topic. Dr. Hikoyeda will inform you if she discusses anything off-label or currently under scientific research.
About the Presenter Dr. Nancy Hikoyeda is Associate Director of the Stanford Geriatric Educa�on Center and a Consultant in Aging, Health, and Diversity. She received her B.S. in Educa�on from the University of Utah; an M.P.H. and Cer�ficate in Applied Social Gerontology from San Jose State University; and a Doctor of Public Health (Dr.P.H.) from the UCLA School of Public Health. Dr. Hikoyeda’s areas of exper�se are in ethnogerontology and ethnogeriatrics – issues of aging, ethnicity, and health with a focus on Asian/Pacific Islander elders, health literacy, long term care u�liza�on, and end-‐of-‐life issues. She has co-‐authored and edited numerous curriculum and training materials as well as chapters on Asian American elders in Social Work Prac�ce with the Asian American Elderly; Cultural Issues in End-‐of-‐Life Decision Making; the Handbook of Geriatric Care Management (3rd ed); and Ethnicity and the Demen�as (2nd ed). Dr. Hikoyeda is re�red Director of the San Jose State University (SJSU) Gerontology Program; served on the Execu�ve Commi�ee of the Santa Clara County Aging Services Collabora�ve; Past President of the California Council on Gerontology and Geriatrics; and is Coordinator of the Stanford Geriatric Educa�on Center Faculty Development Program in Ethnogeriatrics.
Cultural Humility: The Next Level of
Cultural Competence Nancy Hikoyeda, DrPH, MPH
Associate Director Stanford Geriatric Educa�on Center
August 9, 2012

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 3
Introduc�on & Background
Why are cultural competence & cultural humility important?
v Desire to provide the best health care possible v U.S. popula�on is increasingly more diverse & complex
§ Need to learn about history/culture of pa�ents/clients to understand their health behaviors & beliefs
v IOM reports: Crossing the Quality Chasm (2001) & Unequal Treatment (2003) emphasized pa�ent-‐centered care & cultural competence to: § Meet the needs/preferences of a diverse popula�on § Improve provider/pa�ent communica�on & gain trust to eliminate racial dispari�es in health care
§ Reduce risk & medical liability (and meet other requirements) § Ul�mately improve pa�ent adherence & health outcomes
Introduc�on & Background (cont’d.)
Pa�ent-‐Centered Health Care v Respect for pa�ent’s values, needs, & preferences v Informa�on, communica�on, educa�on needed/wanted by
pa�ents v Accommodate physical comfort, emo�onal support, &
family involvement v Shared decision-‐making
IOM, 2001

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 4
Objec�ves v Define culture, cultural competence (CC) & cultural humility (CH)
v Discuss their roles in our health care system v Compare CC & CH assessment tools v Iden�fy communica�on strategies to enhance CH in the medical encounter
v Discuss a case example v Reflect on ways to use today’s informa�on to improve your work, your prac�ce and/or your organiza�on
What is CULTURE?
Culture v Include learned core values, beliefs, norms, behaviors, customs shared & transmi�ed by a group of people
v People may be phenotypically similar, but culture is not race v Dynamic, responsive, coherent systems; evolve/adapt; visible/invisible aspects
v Cultural processes differ within the same group due to: age, cohort, gender, poli�cal climate, class, religion, ethnicity, personality, sexual orienta�on, voca�on, disability, language, immigra�on, & other factors
(California Endowment; Kagawa-Singer & Kassim-Lakha, 2003)

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 5
Culture from a Cultural/Social Anthropology Perspec�ve
Seven Elements of Culture v Environment v Economy v Technology v Religion/world view v Language v Social structure v Beliefs & values (Hammond, 1978)
What is Cultural Competence?
Cultural Competence (CC) v Con�nuum of behaviors, a�tudes, & policies that ensure that a system, agency, program, or individual can func�on effec�vely & appropriately in diverse cultural interac�ons/se�ngs
v Promotes understanding, apprecia�on, & respect for cultural differences/similari�es within, among, & between groups
v Goal that a system, agency, program, and/or individual con�nually aspires to achieve
(U.S. DHHS Workgroup)

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 6
Organiza�onal Cultural Competence
CONTINUUM OF CULTURAL PROFICIENCY
(Cross et al, 1989)
Destructiveness Blindness Proficiency
Incapacity Competence
Cultural Competence Training v Typically, in healthcare se�ngs, CC training assumes gathering/hearing informa�on about a culture results in mastery/exper�se about that culture (technical skill)
v In general, CC training tends to be somewhat vague & frequently
inaccurately used in the medical se�ng which can lead to: § Mere accumula�on of knowledge § Lists of do’s and don’ts § Crea�on of stereotypes
(Kleinman & Benson, 2006)
What is Cultural Humility?

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 7
Cultural Humility (CH) v On-‐going process of acquiring knowledge about health beliefs/prac�ces of diverse pa�ents
v Provider is “life-‐long learner” vs. “knower” with commitment to self-‐evalua�on, cri�que, & reflec�on
v Focus on individual pa�ents & not stereotypes § Pa�ent is best source of informa�on to understand how s/he sees, feels, perceives, & responds to illness
§ Mutually respec�ul, beneficial, non-‐paternalis�c, clinical partnership between providers, pa�ents, families, & communi�es
(Tervalon & Murray-Garcia, 1998)
Cultural Humility (cont’d.)
v Physician/provider relinquishes role of the expert; emphasis on pa�ent/client’s priori�es, beliefs, concerns
v Power imbalances & inequi�es in physician & pa�ent communica�on are reduced due to emphasis on pa�ent/client-‐focused interviewing & care
(Tervalon & Murray-Garcia, 1998; Juarez, Marvel, Brezinski, et al., 2006)
How are Cultural Competence & Cultural Humility Assessed?
SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 8
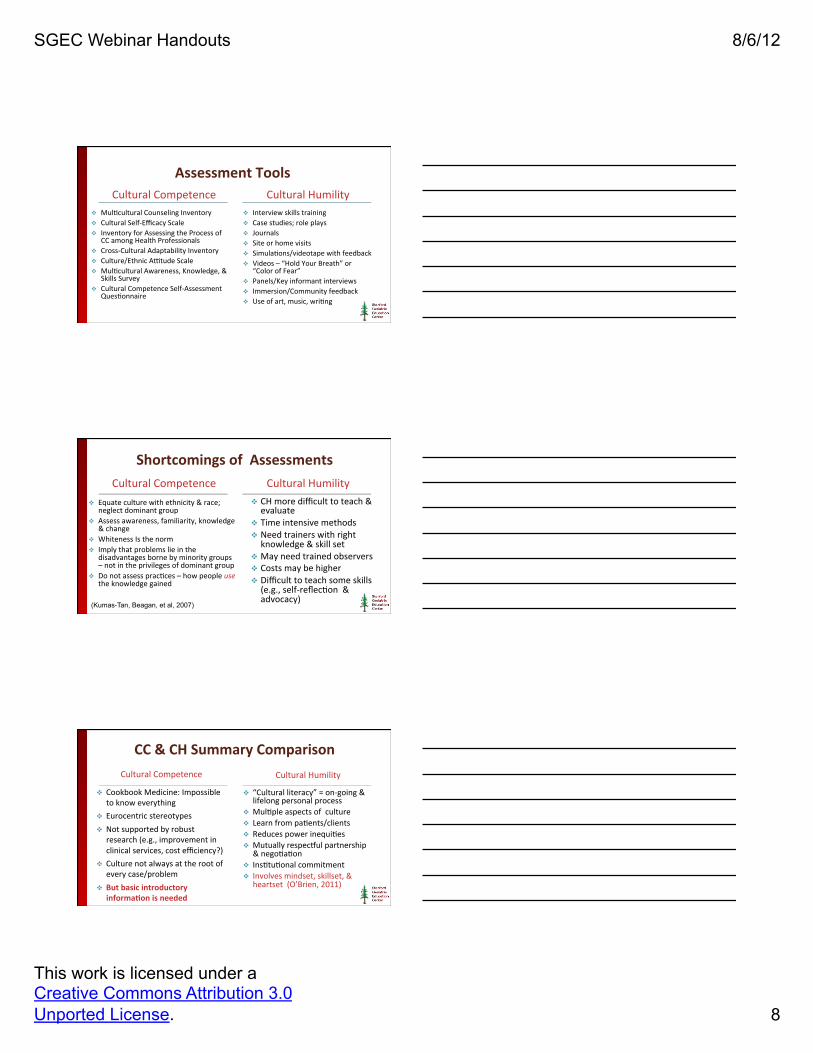
Assessment Tools Cultural Competence Cultural Humility
v Mul�cultural Counseling Inventory v Cultural Self-‐Efficacy Scale v Inventory for Assessing the Process of
CC among Health Professionals v Cross-‐Cultural Adaptability Inventory v Culture/Ethnic A�tude Scale v Mul�cultural Awareness, Knowledge, &
Skills Survey v Cultural Competence Self-‐Assessment
Ques�onnaire
v Interview skills training v Case studies; role plays v Journals v Site or home visits v Simula�ons/videotape with feedback v Videos – “Hold Your Breath” or
“Color of Fear” v Panels/Key informant interviews v Immersion/Community feedback v Use of art, music, wri�ng
Shortcomings of Assessments Cultural Competence
v Equate culture with ethnicity & race; neglect dominant group
v Assess awareness, familiarity, knowledge & change
v Whiteness Is the norm v Imply that problems lie in the
disadvantages borne by minority groups – not in the privileges of dominant group
v Do not assess prac�ces – how people use the knowledge gained
Cultural Humility v CH more difficult to teach & evaluate
v Time intensive methods v Need trainers with right knowledge & skill set
v May need trained observers v Costs may be higher v Difficult to teach some skills (e.g., self-‐reflec�on & advocacy)
(Kumas-Tan, Beagan, et al, 2007)
CC & CH Summary Comparison Cultural Competence
v Cookbook Medicine: Impossible to know everything
v Eurocentric stereotypes v Not supported by robust research (e.g., improvement in clinical services, cost efficiency?)
v Culture not always at the root of every case/problem
v But basic introductory informa�on is needed
Cultural Humility
v “Cultural literacy” = on-‐going & lifelong personal process
v Mul�ple aspects of culture v Learn from pa�ents/clients v Reduces power inequi�es v Mutually respec�ul partnership & nego�a�on
v Ins�tu�onal commitment v Involves mindset, skillset, & heartset (O’Brien, 2011)

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 9
The Journey toward Cultural Humility
Communica�on Strategies to Enhance CH
Interview strategies to transi�on from “Knower to Learner ”
v LEARN [Listen, Explain, Acknowledge, Recommend, Nego�ate] (Berlin & Fowkes, 1983)
v PEARLS [Partnership, Empathy, Apology, Respect, Legi�miza�on, Support] (Steele & Harrison, 2002)
v Six Steps of Culturally Informed Care (Kleinman & Benson, 2006) : (1) ethnic iden�ty; (2) what is at stake? (3) illness narra�ve; (4) stresses; (5) cultural influence on pa�ent care & pa�ent/provider rela�onship
Addi�onal Communica�on Strategies to Enhance CH
v CRASH [Culture, Respect, Assess/Affirm, Sensi�vity/Self-‐Awareness, Humility] (Rust, Kondwani, Mar�nez, 2006)
v RISK Assessment [Resources, Individual Iden�ty, Skills to Cope/Adapt, Knowledge about Ethnic Groups] (Kagawa-‐Singer & Kassim-‐Lakha, 2003)
v QIAN [Self-‐Ques�oning, Immersion, Ac�ve Listening, Nego�a�on] (Chang, Simon, & Dong , 2010)
v 4 C’s of Culture [Call, Cause, Cope, Concerns] (Galan�, 2008)

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 10
Things to Remember v CC is important but not an endpoint in the provider/pa�ent encounter
v Elicit pa�ent informa�on respec�ully to make an accurate diagnosis/assessment = Build trust!
v Nego�ate mutually sa�sfactory goals v Learn & Incorporate various interview strategies v U�lize self-‐reflec�on about personal biases, use of tradi�onal medicine, healers, etc.
v In prac�ce: If you don’t know, ASK; if you do know, ASK! This is the essence of CH.
The Case of Mr. Chang
Mr. Chang is a 65 year old Chinese male who appeared in the Emergency Dept. with chest pain las�ng two weeks. His vital signs are all normal. He speaks only Mandarin Chinese. What informa�on is missing in this introduc�on that is needed to provide culturally appropriate care for Mr. Chang?
Reflect on specific ways you can use what you’ve learned today to improve: (1) your own work (2) your prac�ce or (3) your agency/organiza�on

SGEC Webinar Handouts 8/6/12
This work is licensed under a Creative Commons Attribution 3.0 Unported License. 11
Thank you!
Nancy Hikoyeda, DrPH, MPH Stanford Geriatric Educa�on Center
Phone: (408) 251-‐3736 [email protected] [email protected]
Q & A � We now have some �me to answer your ques�ons. if you have any ques�ons, please use the “Chat” feature located on the right side of your screen.
� A�er the Q and A, We would like to ask each of the par�cipants to answer the short evalua�on ques�onnaire.
Please complete our short survey, We appreciate your feedback. NOTE: Continuing Education Participants must complete a final survey in order to receive CEU/CME credit
Thank You for Par�cipa�ng!
Reminder: Please complete our short survey. We appreciate your feedback.
NOTE: Continuing Education Participants must complete a final survey in order to receive CEU/CME credit

1
Cultural Humility: The Next Level of Cultural Competence
Nancy Hikoyeda, DrPH, MPH – August 9, 2012
Stanford Geriatric Education Center Webinar Series -
Tackling the Tough Topics in Ethnogeriatrics
References
Berlin, E.A., & Fowkes, W.G. (1983). A Teaching Framework for Cross-Cultural Health Care.
Cross-Cultural Medicine, Western Journal of Medicine. Dec., 139, 934-938.
Chang, E-s., Simon, M., & Dong, XQ. (2010, December 16). Integrating Cultural Humility into
Health Care Professional Education and Training. Advances in Health Science Education, DOI
10.1007/s10459-010-9264-1. Retrieved December 1, 2011.
Cross, T.L., Bazron, B.J., Dennis, K.W., & Isaacs, M.R. (1989). Towards a Culturally
Competent System of Care: A Monograph of Effective Services for Minority Children who are
Severely Emotionally Disturbed. Washington, DC: CASSP Technical Assistance Center,
Georgetown University Child Development Center.
Anderson Juarez, J., Marvel, K., Brezinski, K.L., Glazner, C., Towbin, M.M., & Lawton, S.
(2006). Bridging the Gap: A Curriculum to Teach Residents Cultural Humility. Family
Medicine, 38 (2), 97-102.
Galanti, G-A. (2008). Caring for Patients from Different Cultures. Philadelphia, PA: University
of PA Press.
Hammond, P. (1978). An Introduction to Cultural and Social Anthropology. New York:
McMillan.
Howell, W.S. (1982). The Empathetic Communicator. Belmont, CA: Wadsworth.
Institute of Medicine. (2001). Crossing the Quality Chasm: A New Health System for the 21st
Century. Washington, DC: National Academies Press.
Institute of Medicine. (2002). Unequal Treatment: Confronting Racial and Ethnic Disparities in
Health Care. Washinngton, DC: National Academies Press.
Kagawa-Singer, M., & Kassim-Lakha, S. (2003). A Strategy to Reduce Cross-Cultural
Miscommunication and Increase the Likelihood of Improving Health Outcomes. Academic
Medicine, 78 (6), 577-587.
Kleinman, A., & Benson, P. (2006). Anthropology in the Clinic: The Problem of Cultural
Competency and How to Fix It. PloS Med 3(10): e294. Doi:10.1371/journal.prmed.0030294.

2
Kumay-Tan, Z., Beagan, B., Loppie, C., MacLeod, A., & Frank, B. (2007). Measures of Cultural
Competence: Examining Hidden Assumptions. Academic Medicine, 82 (6), 548-557.
Morell, V.W., Sharp, P.C., & Crandall, S.J. (2002). Creating Student Awareness to Improve
Cultural Competence: Creating the Critical Incident. Medical Teacher, 24 (5), 532-534.
O’Brien, A.J. (2011). Global Citizenship and the Stanford Cross-Cultural Rhetoric Project.
Journal of the NUS Teaching Academy, 1 (1), 32-43.
Rust, G., Kondwani, K., Martinez, R., Dansie, R., Wong, W., Fry-Johnson, Y., et al. (2006). A
CRASH-Course in Cultural Competence. Ethnicity & Disease, 16 (Supple 3), S3 29-36.
Shaya, F.T., & Gbarayor, M. (2006). The Case for Cultural Competence in Health Professions
Education. American Journal of Pharmaceutical Education, 70 (6), Article 124.
Steele, D., & Harrison, J. (2002). Challenging Physician-Patient Interactions. Leawood, Kan:
American Academy of Family Physicians.
Tervalon, M. (2003). Components of Culture in Health for Medical Students’ Education.
Academic Medicine, 78 (6), 570-576.
Tervalon, M., & Murray-Garcia, J. (1998). Cultural Humility Versus Cultural Competence: A
Critical Distinction in Defining Physician Training Outcomes in Multicultural Education.
Journal of Health Care for the Poor and Underserved, 9 (2), 117-125.
Weissman, J.S., Betancourt, J., & Campbell, E.G., Park, E.R., Kim, M., Clarridge, B., et al.
(2011). Resident Physicians’ Preparedness to Provide Cross Cultural Care. JAMA, 294 (9), 1058-
1067.


















