PASTE EXTRUSION OF POLYTETRAFLUOROETHYLENE FINE POWDER RESINS

7/31/2019 2010 Tsai - Myopexy of the Vertical Rectus Muscles Using Expanded Polytetrafluoroethylene for Management of a…
http://slidepdf.com/reader/full/2010-tsai-myopexy-of-the-vertical-rectus-muscles-using-expanded-polytetrafluoroethylene 1/3
Myopexy of the vertical rectus muscles using expanded polytetrafluoroethylene for management of a lost medial rectus muscleChong-Bin Tsai, MD, Po-Min Yang, MD, Chau-Yi Tan, MD, and Kuo-Pin Chang, MD
Strabismus due to a lost rectus muscle is uncommon. Surgical treat-
ment of the condition by means of scleral augmented myopexy ofthe vertical rectus muscles canreducethe potential for anterior seg-ment ischemia by leaving the vascular supply intact. We reporta successful use of expanded polytetrafluoroethylene in this proce-
dure to correct long-term exotropia caused by a lost medial rectusmuscle.
Case Report
A 70-year-old woman presented to the Chiayi
Christian Hospital, Chiayi, Taiwan, with exodevi-ation of the right eye of more than 50 years’ dura-tion. The right eye had been amblyopic since childhood. Asan adolescent she had extraocular muscle surgery per-formed on this eye; an exodeviation developed gradually thereafter.
On examination, best-corrected visual acuity was 20/400in the right eye and 20/125 in the left. Grade 2 nuclear scle-rosis was present in both eyes. With the left eye fixating inprimary position, the right eye had an exodeviation of 90D.
The right eye maintained abduction in all gaze positions(Figure 1). Active force generation test of the right eye de-tected only minimal abducting movements. Passive force
duction test under topical anesthesia could bring the right eye to the midline.
After obtaining written informed consent regarding theoff-label use of the product, we performed an expanded-polytetrafluoroethylene (ePTFE) augmented muscletransposition on the patient’s right eye. To relieve the re-striction, we first detached the lateral rectus muscle, whichshowed fibrotic scarring at its insertion. An intraoperativepassive forced duction test thereafter showed unrestrictedadduction to cross the midline. The lateral rectus muscle
was recessed 10 mm. No medial rectus muscle capsulecould be found, confirming our diagnosis of lost rather
than slipped medial rectus muscle. A 0.5 Â 2 Â 120 mmePTFE band (France Chirurgie Instruments, Paris,
France) was interwoven with a 4-0 PDS-II suture (EthiconInc, NJ) for added strength (Figure 2). This band wasanchored at its middle to the previous insertion site of the lost medial rectus muscle with 4-0 Surgilon (US Surgi-cal, CT). The 2 ends of ePTFE bands were threadedthrough the middle of the superior and inferior rectus mus-cles, respectively, and trimmed to be just long enough to
wrap the muscles and thus avoid the long-term erosionthrough conjunctiva associated with use of PDS-II suturealone. The sutures were tied together to enhance pulling
strength for adduction of the globe (Figure 3). The tempo-ral conjunctival wound was recessed to help prevent futurerestriction.
Postoperatively, the patient had 15D of exotropia inprimary gaze that was stable through her final follow-up
visit 7 months after surgery. The right eye was able toabduct 30 and to adduct 4. Neither implant exposurenor any other complications were noted (Figure 4).
Discussion
A variety of transposition procedures, with and without augmentation sutures, are available to treat ocular
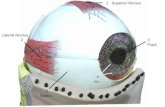
FIG 1. Preoperative photograph. A, Right exotropia in primary
position; B, right gaze; C, left gaze.
Author affiliations: Department of Ophthalmology, Chiayi Christian Hospital, Chiayi,Taiwan
The authors have no conflicts of interest to report.Submitted May 4, 2010. Revision accepted July 26, 2010. Reprint requests: Po-Min Yang, MD, Department of Ophthalmology, Chiayi Christian
Hospital, 539 Jhongsiao Road, Chiayi, Taiwan (email: [email protected] ). J AAPOS 2010;14:550-552.
Copyright Ó 2010 by the American Association for Pediatric Ophthalmology and Strabismus.
1091-8531/$36.00doi:10.1016/j.jaapos.2010.07.014
550 Journal of AAPOS

7/31/2019 2010 Tsai - Myopexy of the Vertical Rectus Muscles Using Expanded Polytetrafluoroethylene for Management of a…
http://slidepdf.com/reader/full/2010-tsai-myopexy-of-the-vertical-rectus-muscles-using-expanded-polytetrafluoroethylene 2/3
deviation created by a dysfunctional rectus muscle.1,2 Inour case, the Jensen muscle–tendon transfer procedure
was not an option due to the absence of a medial rectusmuscle. A full or partial transposition of both verticalrectus muscles combined with a lateral rectus recession inthe setting of an absent lateral rectus muscle was not feasible due to the high risk of anterior segment ischemia. Helveston and colleagues2 described scleral aug-mentation of a tendon transfer procedure to reduce this po-tential risk; however, scleral tissue is not always readily available. Moreover, synthetic materials are preferred dueto concerns about potential infection through use of allo-graft tissue.3
Materials such as PTFE or Mersilene (Ethicon Inc) havegood biocompatibility and can allow fibrovascular in-growth and hence better tissue integration. Both materialshave the disadvantages of possible complications of extru-sion, infection, and granuloma formation. PTFE is alsoavailable as a thermomechanically expanded porous formcalled ePTFE. Aggarwal and colleagues4 first described
a technique using PTFE as extraocular muscle implantsfor large-muscle recessions in a rabbit model; clinical oph-thalmological uses of ePTFE have since been reported.5-8
Tsai and Tan9 reported a similar case of muscle–tendontransposition with an ePTFE band using Helveston’smethod, but in their case, band extrusion occurred
2 months postoperatively. Even though ePTFE is welltolerated under conjunctiva, it is not biodegradable. Wemodified Helveston’s technique in our case to minimizecontact of the ePTFE with conjunctiva. As a result, theePTFE implant was well tolerated and band extrusionhas not occurred after 7 months.
In our case residual exotropia remains. With a less pow-erful transposition method (vis-a-vis full transposition),a more powerful weakening of the antagonist might havegiven a better result. Velez and colleagues10 reporteda technique to fix rectus muscles on the orbital wall. Theprocedure provides profound weakening and is reversible;
assistance of an orbit surgeon may be helpful.
References
1. Struck MC. Augmented vertical rectus transposition surgery withsingle posterior fixation suture: Modification of Foster technique.
J AAPOS 2009;13:343-9.2. Helveston EM, Merriam W, Ellis FD. Extraocular muscle-tendon
transfer with scleral augmentation. Am J Ophthalmol 1980;89:819-23.
3. Mehta JS, Franks WA. The sclera, the prion, and the ophthalmolo-gist. Br J Ophthalmol 2002;86:587-92.
4. Aggarwal RK, Willshaw HE, Townsend P. New materials for rectusmuscle tendon extension in strabismus surgery. Eye 1993;7:40-42.
FIG 3. Artist’s conception of the surgical procedure. The ePTFE band
was sutured at the original medial rectus muscle insertion site. Bothends of the ePTFE band were passed through the 2 adjacent muscles,
and extra length was trimmed. The PDS-II Sutures were tied together.
FIG 4. Photograph obtained 7 months postoperatively. A, 15D resid-
ual exotropia in primary position; B, the right eye could abduct
30; C, adduction of 4. No conjunctival elevation was noted nasally.
FIG 2. A 0.5 mm  2 mm  120 mm ePTFE band was threaded with
a 4-0 PDS-II Suture woven through at 4 mm intervals for added
strength.
Journal of AAPOS
Volume 14 Number 6 / December 2010 Tsai et al 551

7/31/2019 2010 Tsai - Myopexy of the Vertical Rectus Muscles Using Expanded Polytetrafluoroethylene for Management of a…
http://slidepdf.com/reader/full/2010-tsai-myopexy-of-the-vertical-rectus-muscles-using-expanded-polytetrafluoroethylene 3/3
5. Harrer S, Stangler-Zuschrott E, Rossmann M, et al. Polytetrafluoro-ethylene in the surgery of cases with severe limitation of abduction:Long-term results. Neuro-ophthalmology 1999;22:177-85.
6. Langmann A, Lindner S, Wackernagel W, et al. Polytetrafluoroethy-lene (Goretex) for muscle elongation in the surgical treatment of strabismus with restricted motility. Acta Ophthalmol Scand 2006;84:250-53.
7. Choi YJ, Kim CS, Ahn BH. A comparison of the clinical effect between ePTFE membrane-tube implant and Ahmed glaucoma valve
implant for the treatment of refractory glaucoma. Korean J Ophthal-mol 2003;17:106-13.
8. Huang WJ, Hu FR, Chang SW. Clinicopathologic study of Gore-Tex patch graft in corneoscleral surgery. Cornea 1994;13:82-6.
9. Tsai CB, Tan CY. Muscle-tendon transposition with expanded poly-tetrafluoroethylene(e-PTFE)augmentation for strabismus due to lost rectus muscle: A case report. Taiwan J Ophthalmol 2007;46:468-74.
10. VelezFG, ThackerN, BrittMT,et al.Rectusmuscleorbital wall fixation: A reversible profound weakening procedure. J AAPOS 2004;8:473-80.
Journal of AAPOS
552 Tsai et al Volume 14 Number 6 / December 2010