2010: The Evolving Pharmacy Marketplace
13
The Evolving Pharmacy Marketplace: Engagement, Automation and Outcomes By George Van Antwerp Vice-President, Solutions Strategy Group Silverlink Communications WHITE PAPER
-
Upload
george-van-antwerp -
Category
Health & Medicine
-
view
782 -
download
1
Transcript of 2010: The Evolving Pharmacy Marketplace

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes
By George Van Antwerp
Vice-President, Solutions Strategy Group
Silverlink Communications
WHITE PAPER

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 1Copyright © 2009 Silverlink Communications, Inc.
Executive SummaryIn the next several years, we believe that three changes will drive the pharmacy mar-ketplace and ultimately change the business model for PBMs. These changes will be accelerated by the current financial crisis which may drive further consolidation in the short-term. Consolidation which we believe will accelerate the “race to the bottom” where the traditional model of scale has been maxed out with parity achieved among the large PBMs.
1. The need to better engage the consumer in understanding their benefits and ultimately responsibility for their care;
2. The effort to automate and integrate data across a fragmented system and across siloed organizations; and
3. The shift from trend management to being responsible for outcomes.
The CrisisThe rising cost of healthcare is astounding. In 2008, national health expenditures increased by 6.9% — two times the rate of inflation totaling $2.4 trillion or $7,900 per person. Healthcare spending represented 17% of the gross domestic product (GDP). Spending is expected to increase at similar levels for the next decade reaching $4.3 trillion by 2017 — 20% of the GDP. Employer health insur-ance premiums increased by 5% – again two times the rate of inflation — costing employers $12,700 to insure a family of four and $4,700 for an individual.1
Workers are now paying $1,600 more in premiums annually for family coverage than they did in 1999. Since then, employment-based health insurance premiums have increased 120%, compared to cumulative inflation of 44% and wage growth of 29%. Average out-of-pocket costs for deductibles, co-payments for medications and co-insurance for physician and hospital visits rose 115% during the same period — and the percentage of Americans whose out-of-pocket spending for healthcare including health insurance that exceeds $2,000 a year, rose to 43%.2
1National Coalition on Healthcare, Healthcare Insurance Costs, March 17, 2009. www.nchc.org/facts.2National Coalition on Healthcare, Healthcare Insurance Costs, March 17, 2009. www.nchc.org/facts.
Table of Contents
Executive Summary . . . . . . . . . . . . 1
The Crisis . . . . . . . . . . . . . . . . . . . . 1
Consumer Engagement . . . . . . . . . 2
Consumerism in Healthcare . . . . . . 3
Ubiquity and the Changing Paradigm . . . . . . . . . . . . . . . . . . . . 4
Effective Communications: The Key to Patient Involvement . . . . 5
Resources: Back To The Future . . . 6
Cross-Channel View of the Patient . . 7
Evolving Predictive Models . . . . . . . 8
E-prescribing . . . . . . . . . . . . . . . . . 8
Evolving Business Models . . . . . . . 9
Plan Design Loses Luster . . . . . . . 10
Theranostics (or Personalized Medicine) . . . . . . . . . . . . . . . . . . . 11
Summary . . . . . . . . . . . . . . . . . . . 11
Silverlink’s Pharmacy Solutions . . . 12
About Silverlink . . . . . . . . . . . . . . . 12
The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes
By George Van AntwerpVice-President, Solutions Strategy GroupSilverlink Communications
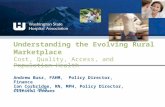
Healthcare Spending is Projected tp Represent 20% of GDP by 2017
$0
$500
$1,000
$1,500
$2,000
$2,500
$3,000
$3,500
$4,000
$4,500
9.5%2003 2006
Nat
iona
l Hea
lthca
re E
xpen
iture
s ($
bn)
Dru
g S
pen
d a
s a
% o
f NH
E
2009 2012 2015
10.5%
11.5%
12.5%
Source: Center for Medicare and Medicaid Services (CMS)
e e e

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 2Copyright © 2009 Silverlink Communications, Inc.
“PBMs are not currently organized or rewarded to maximize value. They are judged largely on their ability to reduce costs and have little incentive to enhance appropriate prescribing and adherence.”3
3 William H. Shrank, MD, MSHS; Michael E. Por-ter, PhD, MBA; Sachin H. Jain, MD, MBA; and Niteesh K. Choudhry, MD, PhD, A Blueprint for Pharmacy Benefit Managers to Increase Value, Am J Manag Care. 2009;15(2):87-93
Consumer Engagement
The industry-wide movement to consumerism will continue to affect plan design, but it will also thrust PBMs and pharmacies into the critical path of member engagement. With phar-macy being the most used benefit as well as the volume and accessibility of retail pharma-cies, they will play a critical role in driving adherence and helping consumers understand healthcare. This will renew the focus on cognitive skills, medication therapy management and ultimately drive the desire for a more traditional “corner store” approach that can be scaled using technology.
Combining this with the macro-economic forces that are driving ubiquity of technology through mobile media and the evolution of the Internet from a pull media to a push media will also challenge the PBMs and pharmacies to innovate. They will be required to look outside of healthcare models to identify the right communications to drive behavior. PBMs and phar-macies will have to leverage behavioral economics and personalization technology to get the right message to the right consumer at the right time through the right medium.
Automation and Integration
The consumer engagement challenges will only exasperate some ongoing challenges within the PBM and pharmacy community. This will include the lack of staff to provide more cogni-tive services and the general fragmentation of data across organizations and functional silos. Figuring out an overall “single view of the patient” which shows all the touch points and offers a coordinated multi-channel strategy for inbound and outbound communications will become a major focus.
In addition, in order to make these solutions efficient, the development of predictive models, much like the clinical and underwriting solutions being used today, will become the norm across the industry. As these models are fine tuned and the promise of e-prescribing be-comes more of a reality, the channel for engaging physicians in the member’s care will finally exist. PBMs and pharmacies will be able to use data to allow physicians to understand when patients aren’t being compliant and when there is an opportunity to drive change.
From Trend Management to Outcomes
The traditional business model for the PBMs has been based on large scale negotiations to drive rebates and efficiencies within mail service – cost to fill and acquisition costs. At the same time as those efficiencies reach a maximum discount, the traditional tools for managing trend will have run their course. Although plan design won’t “die”, comparative effectiveness may reduce (or eliminate) the need for formularies, and in general, the ability to shift cost to the consumer above the 25-30% level will be difficult.
Both of these challenges will push the PBMs and pharmacies into a role where they are focused on driving health outcomes and being part of the bigger solution across the indus-try. They have a strong footprint to drive this change and as theranostics (or personalized medicine) evolves there will be an opportunity to find cost effective solutions to change the prescription landscape.

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 3Copyright © 2009 Silverlink Communications, Inc.
• Healthcare enterprises must prepare for greater patient in-volvement in health decisions.
• Newbenefitplansandprod-ucts are designed to increase the cost share with the patient and reduce plan and em-ployer costs.
• Consumer-directed plans in-tend to place more emphasis on wellness care and preven-tion than traditional plans but have been viewed as simply cost-shifting tools.
• CDHPs have helped consum-ers become more conscious of healthcare costs, but without data transparency and tools, their impact will be limited.
Consumer Preferences in Healthcare
• 34% would use a retail clinic; 16% already have.
• 60% want physicians to provide online access to medi-cal records, test results and appointment scheduling.
• 1 in 3 consumers want more holistic or alternative thera-pies.
• 3 in 4 consumers want ex-panded use of in-home moni-toring devices and online tools that would reduce the need for visits and allow them to be more active in their care.
• 66% strongly favor state-man-dated health insurance.
• 84% prefer generics to name-brand drugs.
• 29% support a tax increase to help cover the uninsured; 37% would consider a tax hike.
• 52% understand their insur-ance coverage.
• 1 in 4 consumers maintain a personal health record.
(Source: Deloitte, Many U.S. Consumers Want Major Changes in Healthcare Design and Deliv-ery, March 17, 2009. www.deloitte.com)
4Aetna, Consumerism in Healthcare, March 2009. www.aetna.com
5Barres, Ann, The State of Consumerism in Healthcare: SWOT Analysis Courtesy of EBRI, Workforce Management, March 2009. www.compforce.typepad.com/compensation_force
Consumerism in HealthcareThe healthcare system is in the midst of a transformation from event-centric (i.e., claim or visit) to consumer-centric. This new focus is about engaging and enabling consumers in their healthcare decision-making process. The traditional one-way conversation is giving way to dialogue as healthcare enterprises make the transition (willingly or unwillingly) to involve pa-tients in healthcare decisions. Healthcare enterprises must prepare to address the challenges and opportunities that consumerism presents and the system must find a way to reward them for these cognitive services.
As individuals pay a greater share of the costs associated with healthcare, they demand greater control over decisions and services affecting their health. This trend includes services aided by Health Savings Accounts (HSAs) and Health Reimbursement Arrangements (HRAs) — savings vehicles generally paired with High-Deductible Health Plans (HDHPs).
Consumer-Directed Health Plans (CDHPs) typically consist of three components: a health savings account; a high-deductible plan that includes preventive care not charged against the deductible; and access to information and tools that help consumers make better health-care decisions. Monthly premiums are lower in these plans and, once the deductible is met, CDHPs pay benefits like traditional health plans.
As shown in the recent survey conducted by Medco Health Solutions below, payors are at a point where the economic realities are forcing them to take a more aggressive stance on cost management. It will no longer be a question of how rich are the healthcare benefits at one employer compared to another, but does the employer offer any coverage at all.
(Chart Source: Presentation at PCMA on March 25, 2009 by Joe Marabito, VP and GM of CDH at Medco Health Solutions, Inc. titled “Impact of the Economy on Pharmacy Benefits and Use”)
These new consumer-directed products have four critical attributes:
• Provide access to information and more control over the member’s own healthcare allow-ing them to make informed decisions about treatment and provider options;
• Increase consumer involvement and awareness about the real cost of healthcare which research has shown reduces total healthcare spending;
• Offer lower monthly premiums making healthcare benefits more affordable for employers and employees; and
• Encourage healthy behavior with no out-of-pocket costs for routine physicals, child immu-nizations or weight-loss programs — placing the focus on wellness care and prevention4.
The financial incentives embedded in these plans seem to be working. Participants in CDHPs and HDHPs report being more cost conscious about healthcare than participants in tradi-tional plans. Almost 75% of CDHP participants and 60% of HDHP participants say that the health plan has made them think more about the cost when deciding whether to see a doc-tor or to fill a prescription compared with 47% of traditional plan participants5.
This creates a wedge for PBMs and pharmacies to become a go-to resource for helping consumers make decisions about their healthcare dollars. On top of general consumer branding awareness, the challenge they have to address is how to push information out to consumers in a timely fashion rather than simply providing reactive tools like portals. It will be important to drive price transparency so that members can make decisions about costs and to find ways to do this without reducing satisfaction or negatively impacting health outcomes due to members being less adherent.
Which one of the statements bestreflects your organization’sbenefit philosophy regardingprescription benefit coverage?
Provide BroadestCoverage
Balance Cost with Care Limit Coverage
52%
13%
46%
81%
2%7%
5 Years AgoToday

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 4Copyright © 2009 Silverlink Communications, Inc.
• Patients are increasingly more informed about healthcare issues due to the availability of information online.
• Social media is growing in im-portance as patients dialogue online to support others with similar health issues.
• E-patients expect to par-ticipate fully in a cooperative relationship with healthcare providers to ensure they are receiving appropriate care.
• Healthcare providers must be ready to educate questioning e-patients.
• Smart devices and mobile applications will continue to dominate the communications space for certain generations.
...[When patients] participate more actively in the process of medical care, we can cre-ate a new healthcare system with higher quality services, better outcomes, lower costs, fewer medical mis-takes, and happier, healthier patients. We must make this the new gold standard of healthcare quality and the ultimate goal of our improve-ment efforts:
• Not better hospitals
• Not better physician practices
• Not more sophisticated elec-tronic medical systems.
• Happier, healthier patients.
— CHARLES SAFRAN
Source: e-patients: how they can help us heal health care, Tom Ferguson, MD, pg. 5 - http://e-patients.net/e-Patients_White_Paper.pdf
6David Ranii, More Companies Use Social Media for Marketing, The News & Observer, December 12, 2008. www.newsobserver.com
7David Ranii, More Companies Use Social Media for Marketing, The News & Observer, December 12, 2008. www.newsobserver.com
8Pr-inside, MedTouch CEO to Discuss Impact of Social Media in Healthcare Marketing, June 4, 2008. www.pr-inside.com/print624567.htm
Ubiquity and the Changing ParadigmThe Internet has become a huge resource of healthcare information with the advent of comprehensive third-party sites like WebMD, Medispan and Family Doctor along with a large number of Health2.0 companies that are developing innovative tools for consumers. In ad-dition, healthcare providers have developed extensive online libraries for their participating members and physicians to research and reference to gain a better understanding of health conditions and prescribed therapies. Today, an astounding 95 million Americans and 95% of physicians use the Internet for health research6.
Electronic social media — blogs, chat rooms, networking sites — also plays an important role in educating patients by facilitating dialogue among people who have experienced the same medical conditions. According to Forrester Research, the number of social media “spectators” — people who read or watch social media — has increased from 48% in 2007 to 69% of people who venture online today.7 Through these vehicles, patients learn first-hand what works and doesn’t work in the treatment of their specific medical conditions from a global network of patients (aka e-patients). These patients are willing and anxious to share and support others in dealing with their healthcare issues, and their testimonials are a power-ful influence on patient biases toward their treatments.
The Internet has placed vast amounts of medical information at the patients’ fingertips. As technology becomes more ubiquitous with tools like the iPhone, patients have unprec-edented access to information, opinions, experiences, testimonials and case-studies that are prompting a new wave of patients who are knowledgeable and informed. They understand their disease or condition, medications available to cure or control them, diagnostic testing, surgical procedures and treatments — and treat their physicians more as an advisor in the process not the expert. These patients are questioning their physicians and healthcare pro-viders to not only understand the therapies prescribed but participate in the decisions made on their behalf. In the next few years, the vast majority of patients will be e-patients armed with an arsenal of information about their health issues and will require participation in the decisions made regarding their care.
Additionally, these new online tools have evolved from a pull medium to a push medium. Traditional member portals provided great information to the engaged consumer who sought it out, but they didn’t reach out and pull in the at-risk consumers. With social media and mobile technology, consumers are engaged by these tools in new ways that may eventu-ally activate more of these consumers and push them to take a role in improving their health outcomes.
“Healthcare providers are aware the impact of traditional media outlets are shrink-ing,”saidPaulGriffiths,CEO,MedTouch.“Butthegreatopportunitysocialmediaaffords is vastly superior to anything we’ve seen before. Healthcare consumers are self-organizing in a way that was impossible a few years ago and the [healthcare providers]whoengagefirstwillreaprewardsdisproportionatefortheirinvestment.”8
E-patients, a new breed of informed patient seeking knowledge about their healthcare situa-tions on the Internet, are demonstrating the power of participatory healthcare. E-patients are:
• Equipped with the skills to manage their own condition;
• Enabled to make choices about self-care and those choices are respected;
• Empowered to share in decisions in their care;
• Engaged in understanding their health situations and treatments;
• Emancipated from accepting decisions made for them without their input; and
• Expert in improving their health status, cope better with fatigue, role limitations, reduced disability and their dependence on hospital care.
Source - David Ranii, More Companies Use Social Media for Marketing, The News & Observer, December 12, 2008. www.newsobserver.com

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 5Copyright © 2009 Silverlink Communications, Inc.
• Individuals need to be motivated to care about healthcare costs and to adopt healthy lifestyles.
• Individuals don’t understand their plan designs and don’t have information about formularies, copays or prior authorizations available to them when they are with their providers or at the Point of Sale (POS).
• Physicians don’t have the time to provide cognitive ser-vices to fully educate patients about their medications or their condition.
• Member turnover from plans limits the return-on-invest-ment (ROI) that payors can realize in preventative care.
• No one is responsible for outcomes.
“Persistent challenges call for new strategies. Ameri-can industry knows that the benefitsofqualityhealthcareand effective cost manage-ment have not been fully real-ized. This will only happen when employees and their dependents are activated to participate willingly in making wiser healthcare and person-al lifestyle choices. Human Resources executives are hungry for evidence-based insightsthatreflectthemostadvanced understanding of the healthcare marketplace and the science of human behavior.”
HELEN DARLING
President, National Business Group on Health
Board Member, The Center for Cost-Effective Consumerism9
9 Quote from the Express Scripts Consumerol-ogy website, accessed on April 1, 2009, http://www.consumerology.org/consumerology.html
Effective Communications: The Key to Patient InvolvementIn order to ensure that patients receive quality healthcare from their providers, both patients and the organizations which govern the healthcare industry are demanding timely, meaning-ful and easy-to-understand communications throughout the entire healthcare continuum. Unfortunately, a synthesized approach is still out of reach given the fragmented healthcare system of today. Coordination among the different entities is often difficult since each of them have functional silos with their own objectives, processes and databases.
Effective communication begins from the first contact and continues throughout the member lifecycle. These communications need to cut through the information clutter that overwhelms consumers and most importantly, provide them with a call to action. Many of the techniques to accomplish this have been deployed in other industries (e.g., financial services) where segmentation, channel preference and predictive algorithms have been used for years.
These sciences are just being introduced in the healthcare industry and need to evolve to meet the dynamic nature of health consumers. Members’ interest changes as they move through different stages from being newly diagnosed with a chronic disease to being an ac-tive patient. But, the other challenge is integrating data across the care team and building a service culture where motivational interviewing and other techniques are deployed in every mode of communication to engage the member.
For example, we know that customized and relevant communications are essential to patient adherence and loyalty, but look at how many companies still have a one-size-fits-all ap-proach. Effective communications must instill confidence and obtain buy-in from patients to form a cooperative effort to improve their health outcomes. Express Scripts has been the most vocal PBM in this space with The Center for Cost Effective Consumerism (www.consumerology.org).
This integrated inter-company and intra-company solution is still futuristic in most cases, but companies are beginning to address one issue at a time to improve the ROI on their member interactions.
• How do I interact with them?
• How do they want to be interacted with?
• When do I have to override their preferences to make sure they get a message (e.g., drug recall)?
• How have they responded and acted previously?
• How do I predict they will act in the future?
• What data-driven triggers can I use to launch a communications campaign?
• What messaging will get them to take action?
With workflow and campaign management technology, companies will achieve this “segment-of-one” over the next five years. With that evolution, communications will begin with plan selection and continue through the member’s plan lifetime. They will continue to increase in relevancy and personalization specific to individual healthcare needs, stages of awareness and concerns. This will greatly reduce patient confusion and increase buy-in for a cooperative wellness and healthcare effort.

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 6Copyright © 2009 Silverlink Communications, Inc.
• The aging baby boomer population uses a large share of total prescription drugs — significantlytaxingpharmacyresources.
• Medication Therapy Manage-ment (MTM) type services for the commercial population continue to be needed to pro-vide a front-line care manage-ment system.
• Workflowautomationandimprovements in pharmacy technician skills will free up resources for pharmacists to spend more time counseling patients.
10Sharon K. Gershon, R.Ph., James M. Cultice, B.S., Katherine Knapp, Ph.D., How Many Pharmacists Are in Our Future?, The Bureau of Health Professionals, June 5, 2000. www.hhs.gov/pharmacy
11Medco’s Specialized Pharmacists, Safety Pro-grams Gain Therapy Management Accreditation, Medco press release from 1/10/08, accessed 4/9/09 at http://medco.mediaroom.com/index.php?s=43&item=295
12Christopher, Abby, The Future of Pharmacy, Pharmacy Times, September 2007. www.pharmacytimes.com
Resouces: Back To The FutureWhile the pharmacy industry is poised to and wants to take a greater role in patient manage-ment, the greatest limitation facing the industry today is the shortage of pharmacy profes-sionals. There are several factors which have converged to cause this shortage:
• Rapid growth in prescription volume;
• Increase in new medications with greater complexities;
• New administrative requirements for handling third-party payments consuming 10% to 20% of the pharmacist’s time;
• Expanding population of 65 years or older which uses a disproportionately high share of prescription drugs;
• Medication therapies are increasing in size, complexity and volume; and
• Decline of the number of applications to pharmacy schools in the late 1990s, leading to reduced class sizes and today’s shortage.
According to the Bureau of Health Professions, the number of graduates entering the phar-macy profession by 2015 will exceed population growth by 1%, supplying 76 pharmacists to every 100,000 people10. This is a good initial step, but it does not take into account:
• The unprecedented growth of the aging population in the next decade;
• The fact that the median age of accredited pharmacy professionals is 46; and
• That it will take years to backfill the current shortage before the industry can catch up.
Going forward, the pharmacists of the future will be more like the corner pharmacist of the past who played a significant role in direct patient care. Pharmacists will become an integral part of the healthcare team through collaboration with physicians to improve medication safety and health outcomes while helping to reduce the overall cost of healthcare.
While there are several smaller pharmacies that provide this level of service, one of the most scalable models can be found in the Therapeutic Resource Centers (TRCs) that Medco Health Solutions has developed. These TRCs offer members direct access to specialized pharmacists that are trained in complex and chronic diseases such as diabetes, cardiovascu-lar disease and gastro-intestinal disorders11.
The evolution of this model into a scalable, technology-enabled solution, which is deployed universally across the industry, will begin to happen over the next decade. This increased burden on the pharmacist will also accelerate the need for technology automation at the Point-of-Sale (POS) and push for a more educated and experienced base of pharmacy tech-nicians. At a minimum, this will manifest itself in accreditation of pharmacy technicians with ongoing continuing education (CE) requirements.
“We employ over 40,000 pharmacy technicians,” said Papatya Tankut, Vice Presi-dent of Pharmacy Professional Services, CVS Corp. “I believe that the correct utiliza-tion and training for technicians provides and affords the pharmacist the opportunity to be able to do the things only they are trained to do and spend more time counsel-ing and interacting with the patients.”12
Medication Therapy Reviews (MTRs)MTR is a clinical evaluation of a patient’s medication therapy by the pharmacist in person at the point of purchase. As mail order pharmacy utilization grows and the shortage of pharmacists continues, the MTR may expand to utilize other communications channels.
MTRs establish and enhance the pharmacist- patient relationship allowing the pharmacist to observe visual cues that indicate adverse reactions to medications. This can result in early detection of medication-related problems thus reduc-ing emergency room visits and medication misadventures. (J. Am, Core Components of Community Pharmacy MTM, American Pharmacy Association, 2005. www.medscape.com)
In a comprehensive MTR, the patient presents all current medications to the pharmacist, prescription and OTC, herbal products and dietary supplements. The pharmacist then assesses the medication therapy for appropriateness and works with both patient and prescriber providing education and information to improve the patient’s self-management of their medications.
Targeted MTRs are used to address new medication problems or for ongoing monitoring during follow-up visits. The pharmacist assesses the specific therapy problem, intervenes, and provides education and information to both the patient and prescriber as appropriate.
The MTR is tailored to the individual needs of the patient at each visit. For optimal health outcomes, a patient would receive an annual comprehensive MTR and targeted MTRs throughout the year to address new medication problems or
ongoing medication therapy issues.

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 7Copyright © 2009 Silverlink Communications, Inc.
• Patient communications to-day are fraught with confusion andconflictingmessages.
• Sequencing of messaging (e.g., call then letter followed by e-mail) can drive dramatic improvements in program results.
• Organizational and technol-ogy-related barriers must be overcome to achieve a cross-channel view.
• Data is typically captured at a campaign level in marketing or at a call level in opera-tions. A member-centric view across events (i.e., claims) doesn’t exist.
Table source - Kreuter, M. W., Farrell, D., Olev-itch, L., Brennan, L., Tailoring Health Messages: Customizing Communication Using Computer Technology, Lawrence Erlbaum, Mahwah, NJ. 2000
13Todd Greenwood, Ph.D., M.PH, Michele Demak Epstein, M.PH, Joan Sinopoli, M.A. Lynn Benzing, M.J, Individualization vs. Segmentation in Prescription Therapy Adherence Programs, Patient Marketing Group, Inc, 2006. www.patientmarketing.com/media/pdf/individualiza-tion.pdf
14Kreuter, M. W., Farrell, D., Olevitch, L., Bren-nan, L., Tailoring Health Messages: Customizing Communication Using Computer Technology, Lawrence Erlbaum, Mahwah, NJ. 2000
Cross-Channel View of the PatientDriving patients to change behavior requires a new strategy. People are too overwhelmed today. And, confusion has become a major problem as competing entities send the same patient conflicting messages. Not only do healthcare professionals often disagree on appro-priate therapies for the same condition, but a patient is often treated for multiple conditions by different physicians who do not communicate with each other. To add to the confusion, outside entities such as pharmaceuticals manufacturers are aggressively advertising their medications directly to the consumer.
“Taking an individualized approach to patient communications is more likely to produce desired outcomes — motivating patients to engage in a complex set of behaviors over a period of time. Driving appropriate medication use requires an un-derstanding of patients’ individual barriers to compliance and persistency. This need for discrete messaging is even more pronounced for chronic conditions that call forsignificantlifestylechangesandhavecomplex,long-termtreatmentregimens.The need to provide dynamic and appropriate support to patients in order to yield increased adherence compels the use of an individualized approach to communica-tion that is sensitive to the needs of patients.”13
Leading healthcare researchers have already begun to leverage new technologies to create individually-tailored messaging that drive behavioral changes and address adherence issues in a wide variety of therapeutic regimens. Kreuter & Skinner define tailoring as “any combi-nation of information or change strategy intended to reach one specific person based on characteristics that are unique to that person and related to the outcome of interest that has been derived from an individual assessment.”14 The main concept is that tailoring creates communications specific to the individual rather than for a group of people.
Ten most important aspects of patient healthcare communications:
• Responsiveness • Understandability • Personalization • Overall tone• Relevance • Credibility • Follow-through• Helpfulness • Privacy • Convenience
To optimize individualized communication, a comprehensive view of each patient’s healthcare history is required. Healthcare providers need to have the capability to access and review the patient’s health profile aggregated over a lifetime including health issues, tests, diagnoses, sur-geries, medication therapies and outcomes in one place. They also need to understand how the patient uses the Internet, how they use the call center for support, how they interact with the disease management company and all the other relevant information that creates a demo-graphic and psychographic profile of the individual. The information within the profile can then be utilized to generate large-scale, customized patient communications appropriate for their unique health situations and incorporating their specific preferences and predicted responses.
The other untapped potential in channel coordination is in sequencing of messaging. A single communication is unlikely to capture all the likely responses. Additionally, without knowing how someone learns, you don’t know if a letter, a call or an online tool is most ef-fective in compelling them to act. As companies begin to segment their members, they will have a framework with different communications campaigns or strategies. The likely axis of the cube would include:
• Likelihood to take action • Value of the target • Segment
For example, a person who is at high risk for development of co-morbidities; is unlikely to be adherent; and who is in the “Sick but Invincible” segment would receive a very different set of communications when they forgot to refill than the person who is low risk; likely to be adher-ent; and in the “Diligent Family Provider” segment.
Based on what we have observed across over 50,000 different healthcare communications programs, we have found six levers that consistently can be applied to improve outcomes:
1. Channel selection;2. Messaging;3. Timing and frequency;4. Branding; 5. Packaging; and6. Incentives.

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 8Copyright © 2009 Silverlink Communications, Inc.
• Predictive modeling helps healthcare providers:
- Identify high-risk patients.
- Identify gaps-in-care.
- Underwrite new business.
• New models will begin to predict responses to interven-tions.
15Carlson, Bob, Predictive Modeling: Sharp Lens on Near Future, Managed Care Magazine, March 2007. www.managedcaremag.com
16Dunham, Will, E-Prescribing to Soar with Increased Spending, Reuters, March 16, 2009 http://www.reuters.com/article/healthNews/idUSTRE52F4VD20090316
Evolving Predictive ModelsHealth insurers have long been utilizing predictive modeling tools as part of their underwriting arsenal to help set premiums for employer groups. Over the years, predictive modeling has been gaining credibility as a tool to aid health plans, physicians and disease / case managers in identifying high-risk members to control costs and disease progression. These models are then used to identify data triggers (i.e., gaps-in-care) which initiate an intervention.
Proponents of predictive modeling see it as the step beyond disease management; they detect health issues that are otherwise not visible. The models help people make decisions that maximize better outcomes.
“Thegoalofaclinicalstrategyistofindtherightinterventionfortherightpersonat the right time, says Carol McCall, Vice President of Humana’s Center for Health Metrics, “and ultimately, we want to understand enough about the person to be able to custom-tailor the exact intervention that is best for them.”15
Over the next few years, predictive modeling will evolve into new areas such as healthcare communications. As PBMs become more consumer-centric, they will embrace their rich data to develop models that answer the following:
• Which members are most likely to be adherent?
• What members are most likely to convert to a generic? To mail?
• What members are most likely to stay at mail once I get them there (i.e., not churn)?
• Which channel is the member most likely to respond to – letter, call, e-mail, text message?
• Which message is most likely to get the member to act?
These models can then be used to drive highly relevant, customized communications and in-terventions regarding medication therapies, purchasing options, utilization, specific condition and disease information, preventative therapies and much more.
E-prescribingWith Medco Health Solutions now claiming that more than 10% of their claims are coming through e-prescribing, we may have achieved a tipping point. While the technology has existed for several years, adoption has been very slow. Now, with the economic stimulus bill signed by President Obama in February 2009, there is renewed hope that e-prescribing will have the funding and support to finally be adopted.
Ultimately e-prescribing (in some form) will replace paper prescriptions, and that may be ac-complished within the next decade. In the United States, the prediction is that 75% of physi-cians will be writing electronic prescriptions within five years and 90% by 201816. One of the key questions still to be decided is whether the technology simply replaces the prescription pad or whether clinical edits and cost savings messaging can be driven down to the physi-cian through this technology.
With the merger of RxHub and SureScripts, there is a centralized hub that has the backing of the PBM industry and the retail pharmacy industry. That means that 75% of retail pharma-cies can now handle electronic prescriptions, and as physician adoption grows, there will be a channel for communication between the three entities – physician, pharmacist and PBM.
The question is how to leverage this technology to improve patient outcomes and reduce their out-of-pocket spending. This adoption creates a new platform that the PBMs and phar-macies can leverage to build their relationships with consumers and will also be an outlet for driving behavior change.

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 9Copyright © 2009 Silverlink Communications, Inc.
• Prescription growth has slowed dramatically in 200817.
• Numerous surveys have shown people skipping doses,notfillingmedications,splitting pills and ultimately being less adherent due to the current recession18.
• Since 1999, employment-based health insurance pre-miums have increased 120%, comparedtocumulativeinfla-tion of 44% and cumulative wage growth of 29% during the same period19.
• PBMs are moving to trans-parent pricing models.
• PBMs must use every means available to accelerate patient conversion to generic drugs, when clinically appropriate.
• Competition in the retail pharmacysectorisfierce,resulting in unprecedented programs offering free and very low cost medications.
17Pierson, Ransdell, U.S. Drug Sales Show Anemic Growth in ’08, http://www.reuters.com/article/healthNews/idUSTRE52I5G320090319
18Consequences of Health Care Costs, Kaiser Family Foundation, Kaiser Health Tracking Poll, March 17, 2009, http://slides.kff.org/chart.aspx?ch=840
19The Henry J. Kaiser Family Foundation. Employee Health Benefits: 2008 Annual Survey. September 2008.
20Bajaj, Vikas, Household Wealth Falls By Tril-lions, The New York Times, March 12, 2009, http://www.nytimes.com/2009/03/13/business/economy/13wealth.html?_r=1
21The National Coalition on Health Care, The Impact of Rising Health Care Costs on the Economy, March 17, 2009, www.nchc.org,
22Martin Sipkoff, PBMs Raise the Curtain, Man-aged Care Magazine, September 2006. www.managedcaremag.com
Evolving Business ModelWith high unemployment and more than $11 trillion in wealth having been destroyed20, an-nual healthcare spending increases have come under even more scrutiny. The annual year-over-year increases have driven costs to the point where the ability of employers to continue health coverage for employees and retirees is being jeopardized. Employers, on average, have seen their health insurance premiums increase nearly 120% since 199921. Combine these cost increases with the consumer crisis and you have the perfect storm.
Although prescription drugs only represent about 10% of total healthcare costs, these cost pressures have focused themselves on the pharmaceutical industry for several reasons:
• It is more easily understood than other areas of healthcare.• It has traditionally been very visible in their marketing activities and shown high profit
margins.• There is a large amount of competition between drugs, pharmacies and PBMs.
That focus has forced PBMs into incorporating several changes into their business model and thus created new competitors. A more transparent contract model has emerged as a result of the work of the Pharmaceutical Purchasing Coalition, a group of 56 large employers, led by the HR Policy Association, a policy group representing about 250 employers that col-lectively spent over $5 billion on their pharmaceutical benefits. Through this program, PBMs participating in transparency programs will disclose to their clients the actual acquisition costs for retail and mail-order drugs. The PBMs will also pass drug company rebates directly to their clients, and they will agree to be audited by the employers22.
Although this contract structure does provide more information, the ultimate role of the PBM has remained the same:
• Drive down costs through economies of scale (rebates, acquisition costs, retail contracting);• Implement plan design solutions and adjudicate claims;• Provide formulary management services;• Provide Drug Utilization Review (DUR) and other clinical services; and in many cases,• Provide mail order and/or specialty pharmacy fulfillment services.
One area of pricing that will change will be the unbundling of services. As transparency theoretically minimizes the margin which can be made in the traditional areas of the busi-ness – mail order and generics, PBMs will have to act more like health plans do with their self-insured clients. We can expect to see more services provided as line items within the contract on a per member basis which will open the market up to best-of-breed providers of niche services.
Over the next few years, PBMs will have to be increasingly innovative in how they demon-strate value. The traditional functions of negotiating leverage through economies of scale will no longer be a sufficient strategy to demonstrate value. This will require PBMs to play a more active role in outcomes and become a more central player in the care team for patients. As this occurs, several areas which will have renewed interest are:
• Adherence programs;• Partnerships with manufacturers to drive disease awareness or specialty drug compliance;• Integration of lab, medical and pharmacy data into predictive models;• Some form of disease management as an area for partnership, acquisition or build out; and• Vertical integration with managed care or retailers.
These changes will likely validate the CVS acquisition of Caremark and MinuteClinic and put Walgreens in a critical position. But, the rest of the retail pharmacies are not going to go without a fight. After Wal-Mart began offering some generics for $4 in 2006, numerous other chains jumped onboard with similar programs or discount card programs. All of these pro-grams are oriented at retaining or growing market share. Additionally, the retail chains con-tinue to develop and push models that show them at the heart of the patient care continuum.
Consequences of Healthcare CostsIn the past 12 months, have you oranother family member living in yourhousehold done each of the followingbecause of cost, or not?
Relied on home remidies or over the counterdrugs instead of going to see a doctor
Skipped dental care or checkups
35%
34%
27%
23%
21%
15%
7%
Put off or postponed getting health care you needed
Skipped a recommended medical test or treatment
Not filled a prescription for a medicine
Cut pills in half or skipped doses of medicine
Had problems getting mental health care
Did any of the above 53%

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 10Copyright © 2009 Silverlink Communications, Inc.
• Traditional cost management tools will be maxed out:
- On average, members pay
nearly 27% of retail pre-
scription and 19% of mail
prescription costs today.23
- Over 80% of employers
lower costs with utilization
management tools24.
- 93% of employers use a
mail-service pharmacy op-
tion25.• Although payors may be
more aggressive in the near future, they generally like less disruptive tools with similar effectiveness to hard edits.
• Participants need to know their options and generally have a lack of understanding oftheirbenefits.
23Pharmacy Benefit Management Institute, Prescription Drug Benefit Cost and Plan Design Online Report, 2008-09 Edition, March 3, 2009. www.pbmi.com/2008_report
24Pharmacy Benefit Management Institute, Prescription Drug Benefit Cost and Plan Design Online Report, 2008-09 Edition, March 3, 2009. www.pbmi.com/2008_report
25Pharmacy Benefit Management Institute, Prescription Drug Benefit Cost and Plan Design Online Report, 2008-09 Edition, March 3, 2009. www.pbmi.com/2008_report
26Pharmacy Benefit Management Institute, Prescription Drug Benefit Cost and Plan Design Online Report, 2008-09 Edition, March 3, 2009. www.pbmi.com/2008_report
27National Association of Chain Drug Stores (NACDS), Industry Facts-at-a-Glance, http://www.nacds.org/wmspage.cfm?parm1=507
28CVS Caremark 2008 Trends Rx Report, pg. 15
Plan Design Loses LusterThe majority of effective trend management tools used today in the pharmacy space are based on plan design (i.e., formulary, copays, utilization management, distribution manage-ment). Plans increasingly deploy a broad range of utilization management (UM) tools for numerous diseases and conditions. The most popular UM tools are step therapy, quantity limits and prior authorization which block targeted prescriptions at the point-of-service (POS). In addition, most employers have adopted multi-tier formularies that align with financial incen-tives to use lower cost medications as appropriate alternatives.
Table1.SummaryofCostSharingforCommonPlanConfigurations1
Cost Sharing Structure
Percentage of Employers UsingPlanConfiguration
2008 2007
Two-tier Plan Design with Dollar Co-payments 14.8% 16.8%
Two-tier Plan Design with Co-insurance 4.5% 7.9%
Three-tier Plan Design with Dollar Co-payments 60.5% 45.3%
Three-tier Plan Design with Co-insurance 17.9% 14.4%
Four-tier Plan Design with Dollar Co-payments 20.2% 11.5%
Four-tier Plan Design with Co-insurance 9.4% 4.1%
These trends of tighter management of the benefit will continue until saturation is achieved, but may lose some focus with comparative effectiveness. A national standard might allow payors to limit reimbursement within drug classes (i.e., implement a therapeutic Maximum Allowable Cost (MAC)). Therefore, these solutions and changes force us to address three topics:
1. Have we reached a maximum in terms of the cost sharing that can be pushed to individual members?
2. Can we hold members responsible for their involvement in their care (i.e., are they adherent)?3. How do we push information to members in a timely and easy to understand format?
The other component to be addressed is management of the distribution channel. Payors (health plans, unions, employers, government entities) have implemented and will continue to increase their optimization of channel selection – retail, mail order, specialty – through copay incentives and mandatory programs. There is still significant upside here as only 12% of employers require maintenance medications to be dispensed by a mail-service pharmacy26, commonly referred to as “mandatory mail” and mail order prescriptions only represent about 20% of all prescriptions dispensed27 in the United States.
Over the next few years, the distribution side of the business will continue to change with retailers using central fill; mail facilities allowing pick up at retail pharmacies; or even an open mail order network where you could go to any PBM’s mail order facility regardless of cover-age and they would be forced to compete on service and price like retailers.
The other component which will complicate the distribution channel is how the PBMs partner or integrate with clinics. A good example of an integrated solution being discussed is the CVS Caremark Proactive Pharmacy Care Continuum28 which was announced last year and is meant to leverage their assets in electronic prescribing, clinics, disease management, retail pharmacy and the PBM space.
CVS Caremark Proactive Pharmacy Care Continuum
Proactive ConsumerEngagement:
HRQ, Biometric Screening,ExtraCare® Health Card
CVS CAREMARKEarly Intervention
CVS CAREMARKContinuous Suppoprt
Script Written
Open Access:Bridge Supply,Maintenance
Choice
Informed PharmacyEngagements:
Mail/Retail Adherence andFace-to-Face Counceling
Proactive PhysicianEngagement:e-Prescribing
Face-to-Face Clinical Consulting
Proactive Real-Time ClinicalInterventions:
Personalized Cost Savings,Gaps in Care Messaging
Informed HealthEngagements:
Coaching, Health Management,CareAlerts
All PBMs
Retail SpecialtyMail Service
Rx

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 11Copyright © 2009 Silverlink Communications, Inc.
• Only 60% of the population respondswellandbenefitsfromaspecificdrugfortreat-ment of disease due to vari-ances in genetic make-up29.
• Genetic drug testing will en-able physicians to prescribe the right drug and dose tai-loredtotheirpatient’sspecificgenetic code.
• Prescribing drugs using ge-neticinformationwillsignifi-cantly reduce waste, improve patient care and raise the safetyprofilefornewmedica-tions.
29Putnam, John, Winning Stocks in the Age of Personalized Medicine, New Wave Research, March 4, 2009. http://seekingalpha.com/article/123963-winning-stocks-in-the-age-of-personalized-medicine
30Putnam, John, Winning Stocks in the Age of Personalized Medicine, New Wave Research, March 4, 2009. http://seekingalpha.com/article/123963-winning-stocks-in-the-age-of-personalized-medicine
Theranostics (or Personalized Medicine)Any discussion of the future would be suspect without at least discussing Personalized Medi-cine, also known as Theranostics, which is the integration of therapeutics and diagnostics. The great promise of personalized medicine is finally on the brink of acceptance and recogni-tion. While Medco Health Solutions has been the most vocal PBM about the topic, several Health2.0 companies such as 23andMe have evolved to do personalized genome mapping.
Since we know that a patient’s unique genotype may respond differently to a drug or therapy than what is perceived as the norm, this science could fundamentally alter the prescription landscape dramatically. Much like we have discussed personalized communications, this information can be used to tailor a patient’s treatment by either eliminating therapies that might not work at all or by altering the amount of drug or therapy that is administered, thus reducing side effects. Most drugs and devices are approved using large cohorts of patients, and it is widely known that their response to the drug or therapy varies widely.
Plavix is a good example. As the second most prescribed drug in the world (25 million prescriptions in 2007 and $8.5 billion in revenues), Plavix is widely prescribed for patients that have experienced heart attack, stroke or other vascular events and who are believed to be at high risk for a recurrent event caused by a blood clot. However, approximately 30% of patients taking Plavix do not metabolize the drug because of genetic variations thus receiving little or no benefit30.
SummaryThe next five to ten years will present challenges and opportunities for the pharmacy and PBM industry. Innovation within the business model and evolution of their role within the healthcare process will allow them to address three critical forces:
1. The need to engage the healthcare consumer in new ways;
2. The need to use technology to augment human interactions and drive personalization; and
3. The need to be more responsible for outcomes not simply trend management.
Healthcare consumers will continue to be overwhelmed with competing sources of infor-mation online and sent to them. Companies that create process-based communication solutions that apply analytics, leverage workflow and campaign management technologies and apply best practices such as adaptive control (aka champion / challenger) will be able to differentiate themselves.
PBMs will have to emerge as stand alone brand names with consumer recognition. They will also have to leverage relationships with the retail network to develop the corner store of the future which blends cognitive skills with technology to integrate with the Internet and other technologies which consumers look to for information.
Additionally, to be an instrumental part of the care team, pharmacies and PBMs will have to figure out a seamless approach to working with physicians through e-prescribing and other technologies. Only then will they be in a position to improve outcomes and shift from their traditional role to a role where they become a healthcare provider.

The Evolving Pharmacy Marketplace:Engagement, Automation and Outcomes | 12Copyright © 2009 Silverlink Communications, Inc.
Silverlink’s Pharmacy SolutionsSilverlink provides consumer communications solutions for the majority of the healthcare industry’s PBMs. These solutions range from data management and segmentation to multi-channel communications programs that leverage automated calls, letters, call center agents, and faxing technology, among other communications technologies to reach, engage and motivate the healthcare consumer. Silverlink combines real-time consumer interactions, behavioral insights and process innovation to optimize behavior change and program results.
Communications programs include:
• Automated refill transactions• Adherence programs• WISMO (What Is the Status of My Order) programs• Retail-to-mail (or specialty)• MTM Programs• Pill Splitting• Brand-to-Generic (or OTC) or Therapeutic Interchange• Utilization Management• Formulary Notification• Member Satisfaction Surveys
About Silverlink CommunicationsSilverlink knows the healthcare consumer – and we know every point of contact offers a chance to impact their behavior.
Our solutions are trusted by 80 of the nation’s largest and most influential health plans, phar-macy benefit managers, and population health companies to build stronger relationships with consumers and dramatically lower costs.
Silverlink’s unique approach combines real-time consumer interactions, behavioral insights and process innovation to unlock the value that consumers represent in healthcare’s complex cost equation. To learn more about what makes Silverlink the leader in healthcare con-sumer communications, please visit www.silverlink.com, email [email protected], or call 1.781.425.5700.