2010 Guidelines Case Study #2: Mrs. BR 2010 Guidelines.
46
2010 Guidelines 2010 Guidelines Case Study #2: Case Study #2: Mrs. BR Mrs. BR 2010 Guidelines
-
Upload
thomasine-riley -
Category
Documents
-
view
225 -
download
5
Transcript of 2010 Guidelines Case Study #2: Mrs. BR 2010 Guidelines.

2010 Guidelines2010 Guidelines
Case Study #2:Case Study #2:Mrs. BRMrs. BR
2010 Guidelines
2010 Guidelines2010 Guidelines
Case PresentationCase Presentation
• 65-year-old woman• Natural menopause at age 50• 10-year history of hypertension (currently
treated and controlled)• Presents for periodic health examination
2010 Guidelines2010 Guidelines
Physical ExaminationPhysical Examination
• Height: 160 cm (5'3")– 1 cm less than self-reported historic peak height
• Weight: 63.5 kg (140 lbs.)• Body mass index (BMI): 24.8 kg/m2
• Blood Pressure: 136 / 84 mmHg• Physical examination is unremarkable
2010 Guidelines2010 Guidelines
MedicationsMedications
• Perindopril 8 mg once daily (OD)• Multivitamin (for adults over 50)

2010 Guidelines2010 Guidelines
Screening and Risk AssessmentScreening and Risk Assessment
• Mrs. BR meets the 2010 guideline criteria for screening using dual energy X-ray absorptiometry (DXA) – All women and men age > 65
• Current recommendations are to use one of these validated tools to assess 10-year risk of osteoporotic fractures– CAROC developed by The Canadian Association of
Radiologist and Osteoporosis Canada– FRAX Fracture Risk Assessment Tool developed by The
World Health Organization
2010 Guidelines2010 Guidelines
Ms. BR: Risk Factor AssessmentMs. BR: Risk Factor Assessment
• No hormone treatment• No personal fracture history• Positive family history: Hip fracture in her mother at
age 75 (fell in own home; ended up in personal-care home)
• Non smoker • No history of systemic steroid use• No history of rheumatoid arthritis• No potential secondary causes of osteoporosis• Alcohol use: < 3 drinks/day

2010 Guidelines2010 Guidelines
QuestionQuestion
• What is the impact of family history of hip fracture on risk assessment?

2010 Guidelines2010 Guidelines
CAROC: Using Age, Sex, and BMD to CAROC: Using Age, Sex, and BMD to Estimate 10-year Risk of FractureEstimate 10-year Risk of Fracture
• Age: 65• BMD T-score:
– Femoral neck: -2.3
– Spine: -2.2
Mrs. BR is at moderate risk of fractures using the CAROC model
0.0
-0.5
-1.0
-1.5
-2.0
-2.5
-3.0
-3.5
-4.050 55 60 65 70 75 80 85
Age (years)
Fem
ora
l n
eck
T-s
co
re
LOW RISK (<10%)
MODERATE RISK
HIGH RISK (> 20%)
2010 Guidelines2010 Guidelines
Impact of Family History of Hip Fracture Impact of Family History of Hip Fracture
on CAROC Risk Assessmenton CAROC Risk Assessment• The CAROC risk-assessment tool does not
include family history of hip fracture among its variables
• Family history is one of the potential additional factors that can be considered in decision-making if the patient is at moderate risk

2010 Guidelines2010 Guidelines
Impact of Family History of Hip Fracture Impact of Family History of Hip Fracture
on FRAX Risk Assessmenton FRAX Risk Assessment• FRAX does include a family history of hip
fracture as one of its variables• The presence or absence of this risk factor
dramatically changes the 10-year absolute-risk calculation (see next two slides)

2010 Guidelines2010 Guidelines
FRAX Risk Calculation for Mrs. BR,FRAX Risk Calculation for Mrs. BR,withwith Family History of Hip Fracture Family History of Hip Fracture

2010 Guidelines2010 Guidelines
FRAX Risk Calculation for Mrs. BR, Hypothetical FRAX Risk Calculation for Mrs. BR, Hypothetical Situation Situation WithoutWithout Family History of Hip Fracture Family History of Hip Fracture

2010 Guidelines2010 Guidelines
Impact of Family History of Hip Fracture Impact of Family History of Hip Fracture
on FRAX Risk Assessmenton FRAX Risk Assessment• For a person like Mrs. BR, the family history of
parental hip fracture increases her absolute 10-year risk of major osteoporotic fractures by 9.0%
• This has potential major implications for treatment
• In Mrs. BR's case, this factor moved her from the lower end to the higher end of the moderate-risk range using FRAX

2010 Guidelines2010 Guidelines
QuestionQuestion
• What laboratory tests are recommended for patients with a diagnosis of osteoporosis?

2010 Guidelines2010 Guidelines
Recommended Biochemical Tests for Patients Recommended Biochemical Tests for Patients Being Assessed for OsteoporosisBeing Assessed for Osteoporosis
• Calcium, corrected for albumin • Complete blood count• Creatinine• Alkaline phosphatase• Thyroid stimulating hormone (TSH)• Serum protein electrophoresis for patients with vertebral
fractures• 25-hydroxy vitamin D (25-OH-D)*
* Should be measured after three to four months of adequate supplementation and should not be repeated if an optimal level ≥75 nmol/L is achieved.

2010 Guidelines2010 Guidelines
Treatment Considerations Treatment Considerations for Moderate-risk Individualsfor Moderate-risk Individuals
• The 2010 guidelines’ integrated management model recommends consideration of:– Additional clinical risk factors to refine assessment– Lateral thoracolumbar X-ray (T4-L4) or
vertebral fracture analysis (VFA) to aid in decision-making by identifying vertebral fractures
2010 Guidelines2010 Guidelines
Vitamin D, Calcium and Other Vitamin D, Calcium and Other Nonpharmacologic InterventionsNonpharmacologic Interventions
• The 2010 guidelines have new recommendations for vitamin D and calcium intake
• Optimal treatment strategies can also include other lifestyle interventions (e.g., physical activity, nutrition)

2010 Guidelines2010 Guidelines
Mrs. BR: To Treat or Not to TreatMrs. BR: To Treat or Not to Treat
• Decision whether or not to treat patients at moderate risk with pharmacologic therapy also involves– Discussion of benefits (e.g., fracture risk reduction)
and risks (e.g., adverse events) of treatment– Assessment of patient preferences and health
priorities to come up with an "individualized intervention threshold"

2010 Guidelines2010 Guidelines
Mrs. BR: ConclusionsMrs. BR: Conclusions
• Diagnosis and treatment decisions should be based on 10-year assessment of risk using a validated tool– Mrs. BR is moderate risk using both the CAROC and FRAX
tools
• Patients at moderate risk (10-year risk 10% – 20%) may benefit from pharmacologic therapy– Decision of whether to initiate treatment can be made after a
discussion of benefits and risks with the patient
• Mrs. BR’s fear of hip fracture leads her to decide to initiate therapy
2010 Guidelines2010 Guidelines
Case 2 Case 2 – – Mrs. BR
Back-up MaterialBack-up MaterialAdditional slides that can be accessed from hyperlinks on case slides

2010 Guidelines2010 Guidelines
Indications for BMD TestingIndications for BMD Testing
• All women and men age > 65 • Postmenopausal women, and men aged 50 – 64 with clinical risk factors
for fracture:– Fragility fracture after age 40 – Prolonged glucocorticoid use † – Other high-risk medication use* – Parental hip fracture – Vertebral fracture or osteopenia
identified on X-ray – Current smoking – High alcohol intake – Low body weight (< 60 kg) or major weight loss (>10% of weight at age 25) – Rheumatoid arthritis – Other disorders strongly associated with osteoporosis
Return to case†At least three months cumulative therapy in the previous year at a prednisone-equivalent dose > 7.5 mg daily;* e.g. aromatase inhibitors, androgen deprivation therapy.

2010 Guidelines2010 Guidelines
Importance of WeightImportance of Weight
• In men > 50 years and postmenopausal women, the following are associated with low BMD and fractures– Low body weight (< 60 kg)– Major weight loss (> 10%
of weight at age 25)
1. Papaioannou A, et al. Osteoporos Int 2009; 20(5):703-715.2. Waugh EJ, et al. Osteoporos Int 2009; 20:1-21.
3. Cummings SR,et al. N Engl J Med 1995; 332(12):767-773.4. Papaioannou A, et al. Osteoporos Int 2005; 16(5):568-578.
5. Kanis J, et al. Osteoporos Int 1999; 9:45-54.6. Morin S, et al. Osteoporos Int 2009; 20(3):363-70.Return to case

2010 Guidelines2010 Guidelines
Importance of Height LossImportance of Height Loss
• Increased risk of vertebral fracture– Historical height loss (> 6 cm)1,2
– Measured height loss (> 2 cm)3-5
• Significant height loss should be investigated by a lateral thoracic and lumbar spineX-ray
1. Siminoski K, et al. Osteoporos Int 2006; 17(2):290-296.2. Briot K, et al. CMAJ 2010; 182(6):558-562.
3. Moayyeri A, et al. J Bone Miner Res 2008; 23:425-432.4. Siminoski K, et al. Osteoporos Int 2005; 16(4):403-410.
5. Kaptoge S, et al. J Bone Miner Res 2004; 19:1982-1993.Return to case

2010 Guidelines2010 Guidelines
10-year Risk Assessment: CAROC10-year Risk Assessment: CAROC
• Semiquantitative method for estimating 10-year absolute risk of a major osteoporotic fracture* in postmenopausal women and men over age 50– Stratified into three zones (Low: < 10%, moderate,
high: > 20%)
• Basal risk category is obtained from age, sex, and T-score at the femoral neck
• Other fractures attributable to osteoporosis are not reflected; total osteoporotic fracture burden is underestimated
Siminoski K, et al. Can Assoc Radiol J 2005; 56(3):178-188.
* Combined risk for fractures of the proximal femur, vertebra [clinical], forearm, and proximal humerus
2010 Guidelines2010 Guidelines
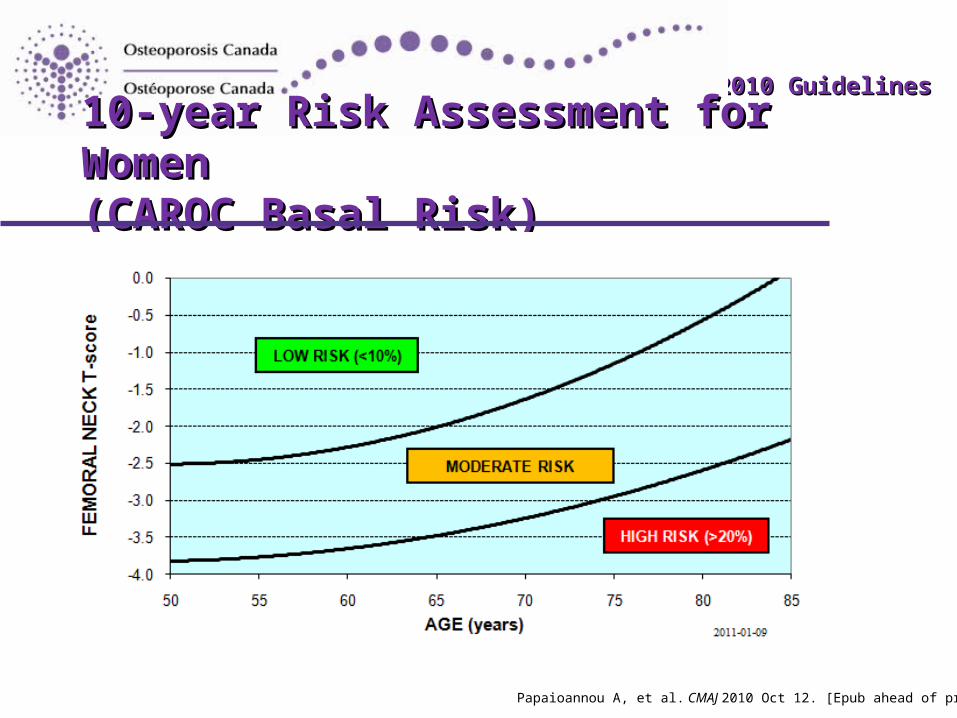
10-year Risk Assessment for Women 10-year Risk Assessment for Women (CAROC Basal Risk)(CAROC Basal Risk)
Papaioannou A, et al. CMAJ 2010 Oct 12. [Epub ahead of print].

2010 Guidelines2010 Guidelines
10-year Risk Assessment for Women 10-year Risk Assessment for Women (CAROC Basal Risk)(CAROC Basal Risk)
Age Low Risk Moderate Risk High Risk
50 above -2.5 -2.5 to -3.8 below -3.8
55 above -2.5 -2.5 to -3.8 below -3.8
60 above -2.3 -2.3 to -3.7 below -3.7
65 above -1.9 -1.9 to -3.5 below -3.5
70 above -1.7 -1.7 to -3.2 below -3.2
75 above -1.2 -1.2 to -2.9 below -2.9
80 above -0.5 -0.5 to -2.6 below -2.6
85 above +0.1 +0.1 to -2.2 below -2.2
Papaioannou A, et al. CMAJ 2010 Oct 12. [Epub ahead of print].Papaioannou A, et al. CMAJ 2010 Oct 12. [Epub ahead of print].
2010 Guidelines2010 Guidelines
Risk Assessment with CAROC: Risk Assessment with CAROC: Important Additional Risk FactorsImportant Additional Risk Factors
• Factors that increase CAROC basal risk by one category (i.e., from low to moderate or moderate to high)– Fragility fracture after age 40*1,2
– Recent prolonged systemic glucocorticoid use**2
1. Siminoski K, et al. Can Assoc Radiol J 2005; 56(3):178-188.2. Kanis JA, et al. J Bone Miner Res 2004; 19(6):893-899.Return to case
* Hip fracture, vertebral fracture, or multiple fracture events should be considered high risk** >3 months use in the prior year at a prednisone-equivalent dose ≥ 7.5 mg daily

2010 Guidelines2010 Guidelines
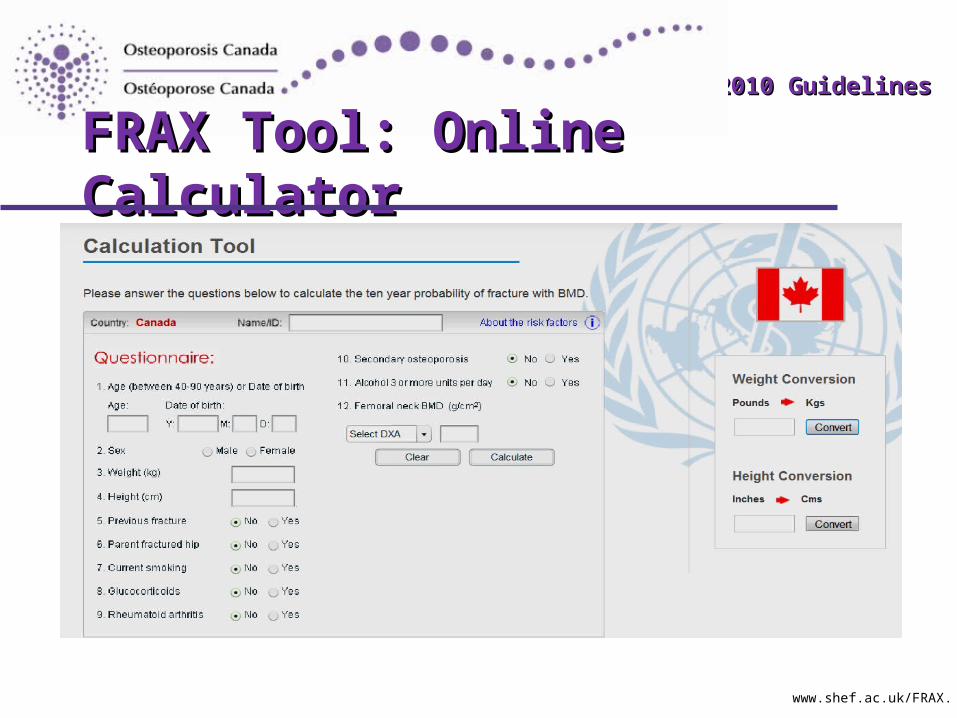
Risk Assessment Using FRAXRisk Assessment Using FRAX
• Uses age, sex, BMD, and clinical risk factors to calculate 10-year fracture risk*– BMD must be femoral neck
– FRAX also computes 10-year probability of hip fracture alone
• This system has been validated for use in Canada1
• There is an online FRAX calculator with detailed instructions at: www.shef.ac.uk/FRAX
1. Leslie WD, et al. Osteoporos Int; In press.
* composite of hip, vertebra, forearm, and humerus
2010 Guidelines2010 Guidelines
FRAX Tool: Online CalculatorFRAX Tool: Online Calculator
www.shef.ac.uk/FRAX.

2010 Guidelines2010 Guidelines
FRAX Clinical Risk FactorsFRAX Clinical Risk Factors
• Parental hip fracture• Prior fracture• Glucocorticoid use• Current smoking• High alcohol intake• Rheumatoid arthritis
Return to case

2010 Guidelines2010 Guidelines
Integrated Approach to Management ofIntegrated Approach to Management ofPatients Who Are at Risk for FracturePatients Who Are at Risk for Fracture
Age < 50 yr Age 50-64 yr Age > 65 yr
Encourage basic bone health for all individuals over age 50, including regular active weight-bearing exercise, calcium (diet and supplementation) 1200 mg daily, vitamin D 800-2000 IU (20-50µg) daily and fall-prevention strategies
•Fragility fracture after age 40•Prolonged use of glucocorticoids or other high-risk medications•Parental hip fracture•Vertebral fracture or osteopenia identified on radiography•High alcohol intake or current smoking•Low body weight (< 60 kg) or major weight loss (> 10% of body weight at age 25)•Other disorders strongly associated with
osteoporosis
•Fragility fractures•Use of high-risk
medications•Hypogonadism•Malabsorption syndromes•Chronic inflammatory
conditions•Primary
hyperparathyroidism•Other disorders strongly
associated with rapid bone loss or fractures
•All men and women
Initial BMD Testing

2010 Guidelines2010 Guidelines
Assessment of fracture risk
Moderate risk(10-year fracture risk 10%-20%)
Low risk(10-year fracture risk < 10%)
Lateral thoracolumbar radiography (T4-L4) or vertebral fracture assessment may aid in decision-making by identifying
vertebral fractures
High risk(10-year fracture risk > 20% or prior fragility fracture of hip or spine or > 1 fragility fracture)
Good evidence of benefit from
pharmacotherapy
Always consider patient
preference
Unlikely to benefit from pharmacotherapy
Reassess in 5 yr
Factors warranting consideration of pharmacologic therapy…
Integrated Approach, ContinuedIntegrated Approach, Continued
Initial BMD Testing

2010 Guidelines2010 Guidelines
Integrated Approach, ContinuedIntegrated Approach, Continued
Assessment of fracture risk
Moderate risk(10-year fracture risk 10%-20%)
Low risk(10-year fracture risk < 10%)
Lateral thoracolumbar radiography (T4-L4) or vertebral fracture assessment may aid in decision-making by identifying
vertebral fractures
High risk(10-year fracture risk > 20% or prior fragility fracture of hip or spine or > 1 fragility fracture)
Good evidence of benefit from
pharmacotherapy
Always consider patient
preference
Unlikely to benefit from pharmacotherapy
Reassess in 5 yr
Factors warranting consideration of pharmacologic therapy…
Initial BMD Testing

2010 Guidelines2010 Guidelines
Integrated Approach, ContinuedIntegrated Approach, Continued
Assessment of fracture risk
Moderate risk(10-year fracture risk 10%-20%)
Low risk(10-year fracture risk < 10%)
Lateral thoracolumbar radiography (T4-L4) or vertebral fracture assessment may aid in decision-making by identifying
vertebral fractures
High risk(10-year fracture risk > 20% or prior fragility fracture of hip or spine or > 1 fragility fracture)
Good evidence of benefit from
pharmacotherapy
Always consider patient
preference
Unlikely to benefit from pharmacotherapy
Reassess in 5 yr
Factors warranting consideration of pharmacologic therapy…
Initial BMD Testing
2010 Guidelines2010 Guidelines
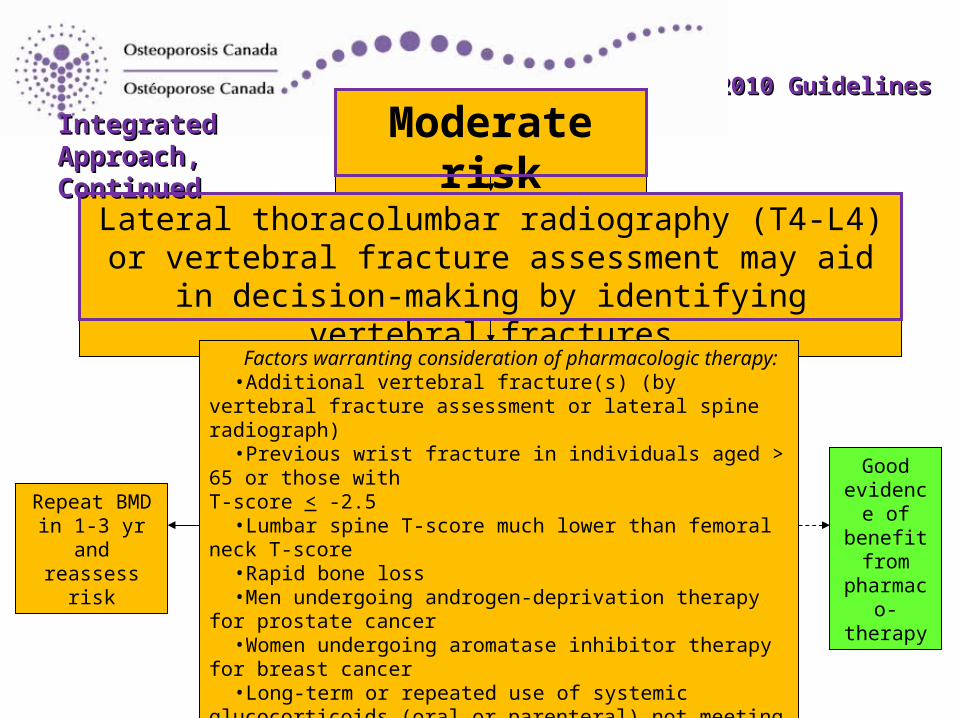
Moderate risk(10-year fracture risk 10%-20%)
Lateral thoracolumbar radiography (T4-L4) or vertebral fracture assessment may aid in decision-making by
identifying vertebral fractures
Factors warranting consideration of pharmacologic therapy:•Additional vertebral fracture(s) (by vertebral fracture assessment
or lateral spine radiograph)•Previous wrist fracture in individuals aged > 65 or those with
T-score < -2.5•Lumbar spine T-score much lower than femoral neck T-score•Rapid bone loss•Men undergoing androgen-deprivation therapy for prostate cancer•Women undergoing aromatase inhibitor therapy for breast cancer•Long-term or repeated use of systemic glucocorticoids (oral or
parenteral) not meeting conventional criteria for recent prolonged use•Recurrent falls (> 2 in the past 12 mo)•Other disorders strongly associated with osteoporosis, rapid bone
loss or fractures
Good evidence of benefit
from pharmaco-
therapy
Repeat BMD in 1-3 yr and
reassess risk
Integrated Approach, Integrated Approach, ContinuedContinued

2010 Guidelines2010 Guidelines
Moderate risk(10-year fracture risk 10%-20%)
Lateral thoracolumbar radiography (T4-L4) or vertebral fracture assessment may aid in decision-making by identifying vertebral fractures
Factors warranting consideration of pharmacotherapy:•Additional vertebral fracture(s) (by vertebral fracture
assessment or lateral spine radiograph)•Previous wrist fracture in individuals aged > 65 or those
with T-score < -2.5•Lumbar spine T-score much lower than femoral neck T-
score•Rapid bone loss•Men on ADT for prostate cancer•Women on AI for breast cancer•Long-term or repeated use of systemic glucocorticoids
(oral or parenteral) not meeting conventional criteria for recent prolonged use
•Recurrent falls (> 2 in the past 12 mo)•Other disorders strongly associated with osteoporosis,
rapid bone loss or fractures
Good evidence of benefit
from pharmaco-
therapy
Repeat BMD in 1-3 yr and
reassess risk
Integrated Approach, Integrated Approach, ContinuedContinued
Return to case

2010 Guidelines2010 Guidelines
Factors that Warrant Consideration for Factors that Warrant Consideration for Pharmacological Therapy in Moderate Risk PatientsPharmacological Therapy in Moderate Risk Patients
• Additional vertebral fracture(s) (> 25% height loss with end-plate disruption) identified on VFA or lateral spine X-ray
• Previous wrist fracture in individuals > 65 or those with T-score < -2.5 • Lumbar spine T-score much lower than femoral neck T-score • Rapid bone loss • Men on androgen deprivation therapy for prostate cancer • Women on aromatase inhibitor therapy for breast cancer • Long-term or repeated systemic glucocorticoid use (oral or parenteral) that
does not meet the conventional criteria for recent prolonged systemic glucocorticoid use (i.e., > 3 months cumulative during the preceding year at a prednisone equivalent dose > 7.5 mg daily)
• Recurrent falls defined as falling 2 or more times in the past 12 months • Other disorders strongly associated with osteoporosis, rapid bone loss or
fractures
2010 Guidelines2010 Guidelines
Disorders Associated with Osteoporosis and Disorders Associated with Osteoporosis and Increased Fracture RiskIncreased Fracture Risk
• Primary hyperparathyroidism• Type I diabetes• Osteogenesis imperfecta• Untreated long-standing hyperthyroidism, hypogonadism,
or premature menopause (< 45 years)• Cushing’s disease• Chronic malnutrition or malabsorption• Chronic liver disease• Chronic obstructive pulmonary disease• Chronic inflammatory conditions (e.g., rheumatoid arthritis
inflammatory bowel disease)
Return to case

2010 Guidelines2010 Guidelines
VFA Recognition and ReportingVFA Recognition and Reporting
• VFA is a scanning and software option on bone densitometers
• A fracture detected by VFA or radiograph should be considered a prior fracture under the FRAX or CAROC system
Return to case
2010 Guidelines2010 Guidelines
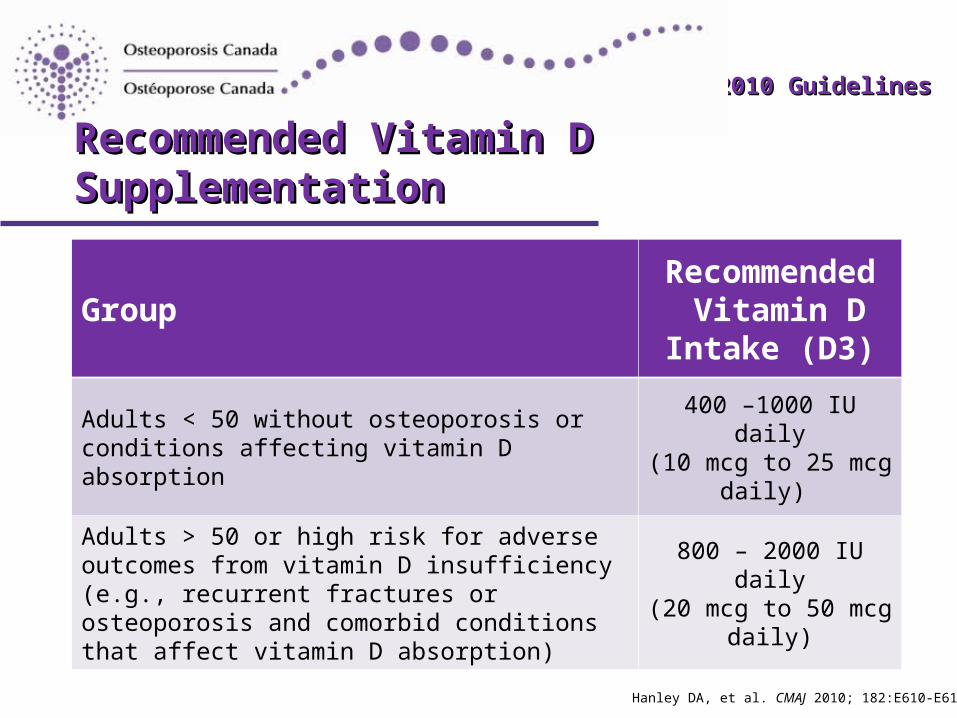
Recommended Vitamin D SupplementationRecommended Vitamin D Supplementation
GroupRecommended
Vitamin D Intake (D3)
Adults < 50 without osteoporosis or conditions affecting vitamin D absorption
400 –1000 IU daily(10 mcg to 25 mcg
daily)
Adults > 50 or high risk for adverse outcomes from vitamin D insufficiency (e.g., recurrent fractures or osteoporosis and comorbid conditions that affect vitamin D absorption)
800 – 2000 IU daily(20 mcg to 50 mcg
daily)
Hanley DA, et al. CMAJ 2010; 182:E610-E618.
2010 Guidelines2010 Guidelines
Vitamin D: Optimal LevelsVitamin D: Optimal Levels
• To most consistently improve clinical outcomes such as fracture risk, an optimal serum level of 25-hydroxy vitamin D is probably > 75 nmol/L– For most Canadians,
supplementation is needed to achieve this level
Hanley DA, et al. CMAJ 2010; 182:E610-E618.

2010 Guidelines2010 Guidelines
When to Measure Serum 25-OH-DWhen to Measure Serum 25-OH-D
• In situations where deficiency is suspected or where levels would affect response to therapy– Individuals with impaired intestinal absorption– Patients with osteoporosis requiring pharmacotherapy
• Should be checked no sooner than three months after commencing standard-dose supplementation in osteoporosis
• Monitoring of routine supplement use and routine screening of otherwise healthy individuals are not necessary
Hanley DA, et al. CMAJ 2010; 182:E610-E618.

2010 Guidelines2010 Guidelines
Recommended Calcium IntakeRecommended Calcium Intake
• From diet and supplementscombined: 1200 mg daily– Several different types of calcium
supplements are available
• Evidence shows a benefit ofcalcium on reduction of fracturerisk1
• Concerns about serious adverse effects with high-dose supplementation2-4
1. Tang BM, et al. Lancet 2007; 370(9588):657-666.2. Bolland MJ, et al. J Clin Endocrinol Metab 2010; 95(3):1174-1181.
3. Bolland MJ, et al. BMJ 2008; 336(7638):262-266.4 Reid IR, et al. Osteoporos Int 2008; 19(8):1119-1123.Return to case

2010 Guidelines2010 Guidelines
Summary Statement for Other Summary Statement for Other Nonpharmacologic TherapiesNonpharmacologic Therapies
Statement Strength
Weight bearing, balance, and strengthening exercises can improve outcomes in individuals with osteoporosis
Level 2
Exercise-focused interventions improve balance and reduce falls in community-dwelling older people
Level 2
Hip protectors may reduce the risk of hip fractures in long-term care residents; however adherence with their use may pose a challenge for the older adult
Level 2
Return to case
2010 Guidelines2010 Guidelines
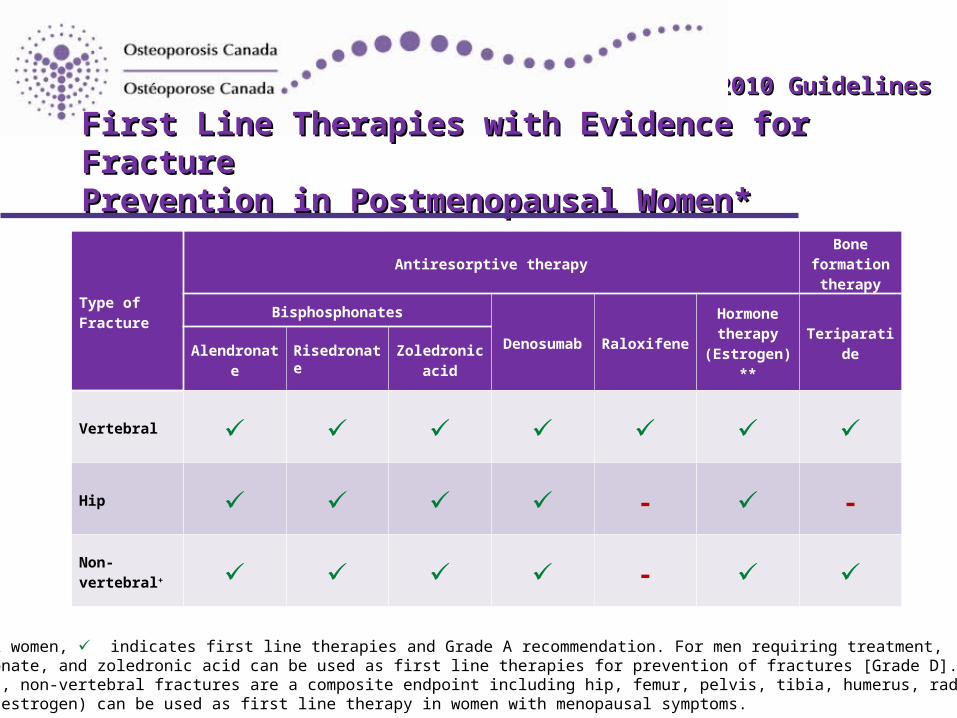
First Line Therapies with Evidence for Fracture First Line Therapies with Evidence for Fracture Prevention in Postmenopausal Women* Prevention in Postmenopausal Women*
Type of Fracture
Antiresorptive therapyBone
formation therapy
Bisphosphonates
Denosumab RaloxifeneHormone therapy
(Estrogen)**Teriparatide
Alendronate RisedronateZoledronic
acid
Vertebral
Hip - -
Non-vertebral+ -
* For postmenopausal women, indicates first line therapies and Grade A recommendation. For men requiring treatment,alendronate, risedronate, and zoledronic acid can be used as first line therapies for prevention of fractures [Grade D]. + In clinical trials, non-vertebral fractures are a composite endpoint including hip, femur, pelvis, tibia, humerus, radius, and clavicle. ** Hormone therapy (estrogen) can be used as first line therapy in women with menopausal symptoms.
2010 Guidelines2010 Guidelines
Adverse Events of Osteoporosis TherapiesAdverse Events of Osteoporosis Therapies
• Consult individual product monographs for adverse event information for approved therapies (click on drug names below to link to online resources)– Bisphosphonates: alendronate, risedronate,
zoledronic acid– Calcitonin– Denosumab– Raloxifene– Teriparatide
Return to case




![Trend Book 2010 [ BR / EN ]](https://static.fdocuments.us/doc/165x107/568c33731a28ab02358cc29c/trend-book-2010-br-en-.jpg)