
2009 VERSION BEFORE EDITS1 Working with Consumers Mark McMahon Grant Sara NSWIOP Career and...
38
2009 VERSION BEFORE EDITS 1 Working with Consumers Mark McMahon Grant Sara NSWIOP Career and Consultancy Module Nov 2009
-
Upload
liam-alderson -
Category
Documents
-
view
216 -
download
0
Transcript of 2009 VERSION BEFORE EDITS1 Working with Consumers Mark McMahon Grant Sara NSWIOP Career and...

2009 VERSION BEFORE EDITS 1
Working with Consumers
Mark McMahonGrant Sara
NSWIOP Career and Consultancy ModuleNov 2009

2009 VERSION BEFORE EDITS 2
Purpose and overview
• Working with consumers in non-clinical roles1: Background knowledge
2: Specific issues and challenges
3: Practical tips – what to do and what to avoid

2009 VERSION BEFORE EDITS 3
Introductions
• Mark
• Grant
• This collaboration

2009 VERSION BEFORE EDITS 4
Part 1: Background knowledge

2009 VERSION BEFORE EDITS 5
Consumer Time: (Consumer Time: (notnot to scale) to scale)
Consumers asInpatients
Consumers during times of Wellness(episodic illness)
Consumers as Outpatients
The MHS
Question: what can consumers do during their times of wellness, in conjunction with the MHS, to improve the time consumers spend as patients? If the MHS fails to do this are they neglecting a resource?

2009 VERSION BEFORE EDITS 6
Typical Characteristics of MHS Consumers*
• While it is said that one in five Australians have mental illness at some time, you will not encounter such a diverse group at public MHS services.
Often chronic MH problems, declined and “fallen” into the MHS as a last resort.
initially they don’t have many things better to do
Have a lived experience: survived difficult lives to survive past age 18 - all this has value. The challenge is to enhance the positives and build a pathway out……. *initially

2009 VERSION BEFORE EDITS 7
Recovery Values:
• Key Concepts of Recovery**• Hope (resilience, unconscious competence)
• Personal Responsibility (not dependence)
• Education (incl. common language)
• Self Advocacy (self-directed)
• Support (own networks, connectedness)
• ** “Recovery” implies a continuous (but non-linear) pathway rather than a set of disconnected outcomes. Consumer view: would not refer to recovery as a “model” which implies medicalisation.
Consumers tend to view mental health as much bigger than the mental health system. Involuntary visits to the acute care ward are experienced as traumatic interferences to one’s life, so the concern is about getting a life back (and not getting sick again).It’s difficult to find a (sane) human being who wants to be sick and unhappy.

2009 VERSION BEFORE EDITS 8
History of consumer involvement
• - overseas experience (SAMHSA in USA)
• - Australian experience:
• Book “Partnership or Pretence”
• Recognition that consumers do get well
• How did this start, how implemented, how evaluated? (high point reached 2005)
• Enormous change since 2005 (see later)

2009 VERSION BEFORE EDITS 9
Consumer participation
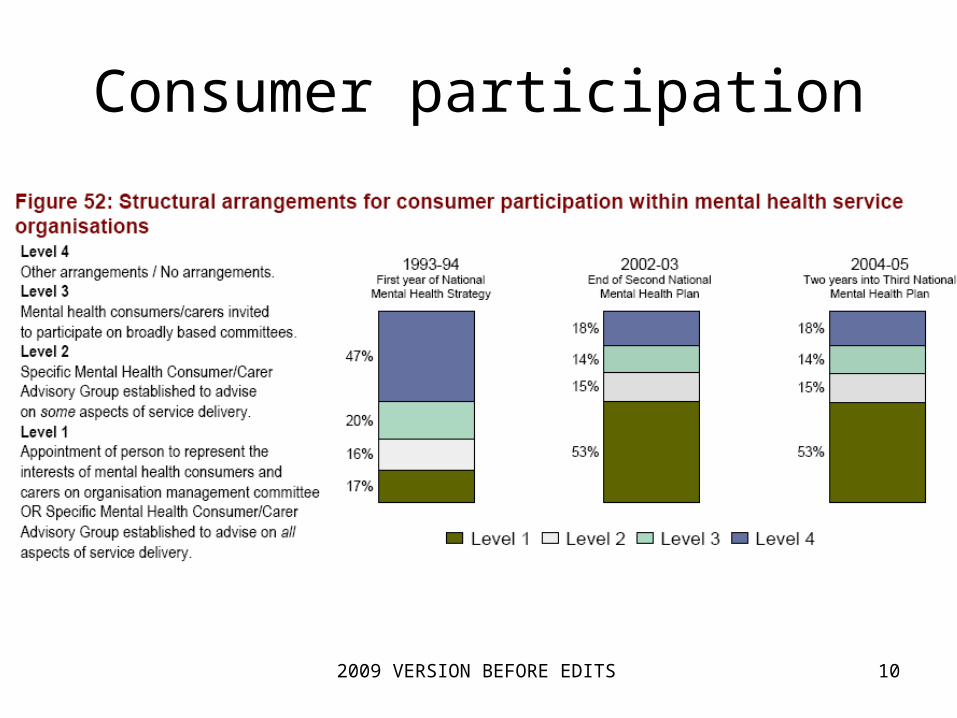
2009 VERSION BEFORE EDITS 10
Consumer participation

2009 VERSION BEFORE EDITS 11
What’s in it for me? Consumer motivations for participation
• for consumers,
• for professionals,
• for system/society
• Refer characteristics of commonly encountered consumers (above)

2009 VERSION BEFORE EDITS 12
Types & Models of Consumer Participation
• Range/ type of consumer involvement: consumer advocates consumer representatives (elected) consumer support/ peer workers (goal setting, warm lines, etc) consumer consultants or appointees (often independent) consumer Co-ordinators/Directors consumer liaison workers (to community/ NGO)
(taken from roles endorsed by AMHCN** for National Relapse Prevention Plan 2004)
• spectrum of models: activity driven – include consumers on committees communication driven – improve relationships with consumers, maybe using
consumers as trainers feedback – actively seek feedback from past/present consumers advocacy – consumers promote/share rights of consumer individuals/groups accountability - plan, implement and evaluate at executive level: do reports (adapted from IOP course notes by A.Prof. Margaret Tobin 2005)
** Australian Mental Health Consumer Network Inc.

2009 VERSION BEFORE EDITS 13
AUSTRALIA 1: – National Policies and Practices recognise the existence of consumers as MHS stakeholders and invite them to
take up roles within or allied to the MHS
During times of wellness, are there more positives than negatives for consumers having a role in/ allied to the MHS?
No. Since the MHS is perceived to be primarily about illness, eg, minimising symptoms, so it cannot help consumers develop wellness skills.
Yes. But does that mean consumers see themselves as (a) Participating in the system, ie, another variety of staff…..ORas (b) Policing the system, ie, peer support workers, or acute ward advocates?
A Third Path?Consumer run NGOs which contract with the MHS, thereby removing industrial, OH+S, training and discipline issues from the MHS

2009 VERSION BEFORE EDITS 14
AUSTRALIA 2: – National Policies and Practices entirely subordinated to a Promotion, Prevention and Early Intervention culture (PPEi). Consumers are not recognised as a stakeholder group because they are never separated from their family, local community, school, etc. for long enough to identify as “a mental
health consumer”
• examples: Geoff Gallup and Andrew Johns ie, they just don’t turn up when MHS advertises consumer role vacancies.
• MHS workers and Community workers only, so the inefficiencies arising from splitting into consumers, carers and ‘other community’ do not occur.
• New Zealand (single government) may be close to this, but driven by many times more expenditure per capita on mental health than in Australia.
• Arguable that Australia is a long way from this possibility because Federal Health, and the 8 State/Territory Healths, can and do have different policies on less central matters. Even if these are not different, consumers are often said to fall through the ‘gaps’ between them, as there is no tradition of clear demarcation.

2009 VERSION BEFORE EDITS 15
Psychiatrist roles in working with consumers
• Some examples of different roles• Committees
– Co-members– Chair / member
• As service manager– Support– Employer– Leadership, resources– Working with advocacy groups– In service partnerships and contracts
• Many others …– Consumers on interview panels

2009 VERSION BEFORE EDITS 16
Legal requirements and standards
• Mental Health Act• Governance and Conflicts of Interest – poorly
understood – so much attention to staff and admin rules, standards, etc, yet not those of consumers?
• Protected Disclosures Act• National Standards for Mental Health• Enormous change since 2005 – impact on “least
restrictive environment”: OH+S, Records Act, UN Disability Rights
2009 VERSION BEFORE EDITS 17
Other literature / further reading …
• Browne, G. & Hemsley, M. (2008) Consumer participation in mental health in Australia: what progress is being made?, Australasian Psychiatry, 16, 446-449.
• Stewart, S., Watson, S., Montague, R. & Stevenson, C. (2008) Set up to fail? Consumer participation in the mental health service system, Australasian Psychiatry, 16, 348-353.
• Nestor, P. & Galletly, C. (2008) The employment of consumers in mental health services: politically correct tokenism or genuinely useful?, Australasian Psychiatry, 16, 344-347.
• Gordon, S. (2005) The role of the consumer in the leadership and management of mental health services, Australasian Psychiatry, 13, 362-365.
• Lloyd, C. & King, R. (2003) Consumer and carer participation in mental health services, Australasian Psychiatry, 11, 180-184.
2009 VERSION BEFORE EDITS 18
Part 2: Specific issues and challenges

2009 VERSION BEFORE EDITS 19
Psychiatrists and organisations
• Professional role critical, but not universal• Any role in organisation / health system requires
broader models– Eg Bolman and Deal “Four Frames”: Structural,
Human Resources, Political, Symbolic
• Many of the challenges of organisational work with consumers are a subset of broader issue of working within a complex system
• Professionals, consumers are just some of the many voices

2009 VERSION BEFORE EDITS 20
Focus
Recovery
versus. Symptoms/illness
RECOVERY MODEL MEDICAL MODEL
Distressing experience Psychopathology
Biography Pathography
Interest centred on the person interest centred on the disorder
Pro-health Anti-disease
Strengths-based Treatment-based
Experts by experience Doctors and patients
Personal meaning Diagnosis
Understanding Recognition
Value-centred (Apparently) Value-free
Humanistic Scientific
Growth and discovery Treatment
Choice Compliance
Modelled on heroes Underpinned by meta-analysis
Guiding narratives Randomised control trials
Transformation Return to normal
Self-management Expert care coordinators
Self-control Bringing under control
Personal responsibility Professional accountability
Within a social context Decontextualised
Table from:
Roberts, G & Wolfson, P (2004) The Rediscovery of Recovery: Open to All.
Advances in Psychiatric Treatment, 10, pp. 37-49 (both authors are consultant psychiatrists)

2009 VERSION BEFORE EDITS 21
Language• “Consumers, clients, customers, patients …”
• Does it matter?
• One view– People have a right to own what they are called – Respect is not a “zero sum” process– Language does reflect thought and attitude– In most situations “person” is the best word

2009 VERSION BEFORE EDITS 22
Participation or Ownership
• NSAMHS Consumer Policies and Structure (handout) Note covering memo
• Consumer advocates vs. Official Visitors (ie, “warm” vs. “cold” contacts)
• Consumer NGO’s ?
• Consumers don’t like having their views trivialised

2009 VERSION BEFORE EDITS 23
Support
• Tokenism?
• Set up to fail …
• Independence vs. employment/contract

2009 VERSION BEFORE EDITS 24
Representation
• One v many
• Under-represented groups
• How representative are any of us?
– “The loudest voices are not always the right voices regardless of whether they are the expert providers or the expert users.” (Margaret Tobin)
2009 VERSION BEFORE EDITS 25
Managing complex relationships and boundaries
• Major problems very rare
• Dual relationships: clinical and organisational contact with a person and their family
• Confidentiality
• Multiple responsibilities
2009 VERSION BEFORE EDITS 26
Counter-transference• Important NOT to bring clinical frameworks
into organisational roles, however …
• Each psychiatrist can represent other/past psychiatrists, all past and traumatic experiences within the system
• Can be a mismatch between your personal values/aims and how you are experienced
• Intensity of negative feelings can be confronting and unexpected

2009 VERSION BEFORE EDITS 27
Part 3: Practical issues

2009 VERSION BEFORE EDITS 28
When to seek a consumer representative
See: National Standards for Mental Health Standard 3:
- Consumer and Carer Participation: Consumers and carers are involved in the planning, implementation and evaluation of the MHS. (handout)
Other Standards also cover consumers
2009 VERSION BEFORE EDITS 29
How to seek a consumer nominee
• NSW Government Action Plan (‘GAP’), Partners in Health - Sharing information and making decisions together (Summary – handout)
• Further details at: http://www.health.nsw.gov.au/mhdao/participation.asp#para_2
• NGOs, advertising, word of mouth, relative?
2009 VERSION BEFORE EDITS 30
GAP Now/ …….
• Now...Consultation not participation• Edmond gets a call from someone at the Health
Department about a meeting next week.They are setting up a committee to look at priorities for the future and they want a consumer on the committee.
• Edmond is the only consumer on the committee.The health people use a lot of abbreviations and terms that no one explains. He feels anxious about talking and thinks the others will not take him seriously.
• Edmond stays on the group and they identify priorities for the future.The priorities are sent out for public comment but there is not much time allowed.

2009 VERSION BEFORE EDITS 31
GAP ……the Future• NSW Health and the community working together• Edmond is representing his cardiac support group on a Department
committee along with three other consumer representatives.• Before the first meeting Edmond gets a call to say that the
Department will pay for his travel costs and day respite care for his wife who was diagnosed with Alzheimers last year. He is asked if there is any other help he needs to take part in the meetings like meeting papers in large print. Edmond takes part in a training program for consumer representatives.
• At the meetings the Chairperson interrupts people who use technical language and asks them to explain. The Chairperson asks the consumer members for their views on issues discussed.
• The committee identifies a number of priorities but agree that it is important to see what the public thinks. They plan how to get the views of different people in the community and Edmond is able to contribute a lot of information about reaching people in their homes. After the consultation process, the future priorities are reviewed and changed.The final priorities are widely publicised and Edmond is asked to be involved in the evaluation of their work.

2009 VERSION BEFORE EDITS 32
Prepare and support consumer workers
• Exercise in feeling powerless: role play being a psychiatrist expert witness in the Supreme Court of NSW (if time allows)
• ………...yes, this is a joke!!
• Have you read DOH Memo GL2005_043: “Consumers Representatives - Working with Consumers in NSW - Health, Guidelines for Secretariat” (note: not a Mental Health document)

2009 VERSION BEFORE EDITS 33
Chairing a meeting with consumers
2009 VERSION BEFORE EDITS 34
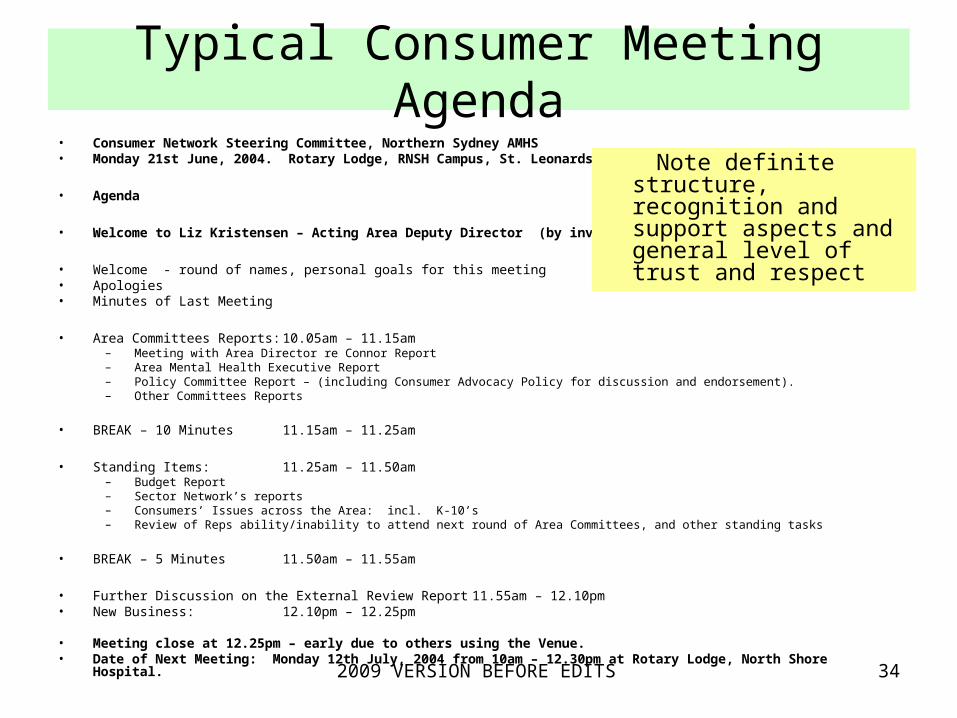
Typical Consumer Meeting Agenda• Consumer Network Steering Committee, Northern Sydney AMHS• Monday 21st June, 2004. Rotary Lodge, RNSH Campus, St. Leonards
• Agenda
• Welcome to Liz Kristensen – Acting Area Deputy Director (by invitation)
• Welcome - round of names, personal goals for this meeting • Apologies• Minutes of Last Meeting
• Area Committees Reports: 10.05am – 11.15am– Meeting with Area Director re Connor Report– Area Mental Health Executive Report– Policy Committee Report – (including Consumer Advocacy Policy for discussion and endorsement).– Other Committees Reports
• BREAK – 10 Minutes 11.15am – 11.25am
• Standing Items: 11.25am – 11.50am– Budget Report– Sector Network’s reports– Consumers’ Issues across the Area: incl. K-10’s– Review of Reps ability/inability to attend next round of Area Committees, and other standing tasks
• BREAK – 5 Minutes 11.50am – 11.55am
• Further Discussion on the External Review Report 11.55am – 12.10pm• New Business: 12.10pm – 12.25pm • Meeting close at 12.25pm – early due to others using the Venue.• Date of Next Meeting: Monday 12th July, 2004 from 10am – 12.30pm at Rotary Lodge, North Shore Hospital.
Note definite structure, recognition and support aspects and general level of trust and respect

2009 VERSION BEFORE EDITS 35
Handling differences and disagreements
• Be prepared……• Consultation isn't always agreement: “Hai!” • Conflicts: identify interests first• Social contracts, advance directives• Myths – consumers: overly violent, have to
be cured to work.• Myths - you can tell what a psychiatrist
prescribes by the colour of his/her pen
2009 VERSION BEFORE EDITS 36
Support when someone is personally unwell
• Is it possible just to let some time pass?...
• Things usually occur leading up to a person being noticeably unwell….
• Is this person supported by local consumers?
• Do they have a support system in place?
• Are there arrangements to mitigate?
• How good’s your conflict resolution toolkit?
2009 VERSION BEFORE EDITS 37
Consumer Tools and Training• “The Kit” (advocacy) sponsored by MHCA
• WRAP groups – before relapse; overcoming barriers to participation and improvement
• Peer support/ Peer worker training by CAN Inc. (Federal suicide prevention funding)
• NSW Mental Health Consumer of the Year Awards at Parliament House (Eli Lily)
• IOP Consumer Advocate/ Representatives Training – 3 days early-bird rate $150 - bargain!

2009 VERSION BEFORE EDITS 38
Conclusions and questions


















