2009 Strategic Plan Presentation Final2
45
Strategic Plan 2009-2013 Cleveland County HealthCare System “Chart a New Course”
Transcript of 2009 Strategic Plan Presentation Final2
Strategic Plan 2009-2013Cleveland County HealthCare System
Chart a New Course
A Time of Change After many years of successful Growth, leading Quality, improving Service, high employee morale and exceeding our budget 2007 and 2008 have seen declines in several elements of performance at CCHS Previous Strategic Plans have predicted a coming time of turmoil..
Those time are here. We have entered the Perfect Storm!Cleveland County HealthCare System2
The Perfect Storm
Cleveland County HealthCare System
3
The Perfect StormThe Dilemma of Multiple Sites
What are the elements of this perfect storm? In the analogy, the following would be suggested:
Cleveland County HealthCare System
4
The Perfect StormThe Dilemma of Multiple Sites
What are the elements of this perfect storm? In the analogy, the following would be suggested: The merger between CRMC and KMH has changed the focus from one hospital to multiple hospitals. This has left a vacuum that to date have not addressed. The strategy for managing this vacuum was to have each hospital run by a COO/CNE, Despite heroic effort by Veronica and Sherri, this strategy was not successful in filling the vacuum An additional negative artifact of the COO/CNE strategy is that the CNE function was over-run by the COO function.
Brian Gwyn, as the new Executive VP & COO is fully empowered going forward..he is the boss.
Cleveland County HealthCare System
5
Past CCHS Org Chart
Cleveland County HealthCare System
6
The Perfect StormThe Dilemma of Multiple Sites
What are the elements of this perfect storm? In the analogy, the following would be suggested: Along with this org chart problem, communications back to all stakeholders became insufficient This will be resolved going forward in that it is one of Brians core strengths, I am meeting more frequently with physicians on strategy and we will significantly increase our marketing efforts both externally and internally.
Cleveland County HealthCare System
7
The Perfect StormThe Dilemma of Multiple Sites
What are the elements of this perfect storm? In the analogy, the following would be suggested: Some stakeholders have never accepted the logic of the CRMC / KMH merger, Without the real growth potential to be had in Kings Mountain, living the Mission at any location will be difficult given our community growth and our demographicsIf we are able to expand the primary care base at KMH, this strategy will work The new strategic plan lays out complimentary options for growth outside of Kings Mountain as well
Cleveland County HealthCare System
8
The Perfect StormThe Regulatory Imperative
What are the elements of this perfect storm? In the analogy, the following would be suggested: The CAP & JCAHO surveys were significantly different and their findings and conditional accreditation required 24 months of consuming Leadership focus leaderships eye was diverted from other important strategies and communications
Cleveland County HealthCare System
9
The Perfect StormOther Elements of the perfect storm
What are the elements of this perfect storm? In the analogy, the following would be suggested: We have been without a Strategic Plan for 18 months. This was mostly because of our interest in implementing the Clinical Practice Council strategy and because we were waiting to see what Gaston Memorial Hospital was going to do in system affiliation. That has been resolved now as our competitor is standing alone and coming at us competitively with both guns blazing.
Cleveland County HealthCare System
10
The Perfect StormOther Elements of the perfect storm
What are the elements of this perfect storm? In the analogy, the following would be suggested: The Clinical Council process has struggled No CMO leadership until recently Even though it was always intended as a control sharing strategy, many issues have not gone through this process.
Cleveland County HealthCare System
11
The Perfect StormA New Way to Care for Patients - Hospitalists
What are the elements of this perfect storm? In the analogy, the following would be suggested: The conversion from SMA as an admitting group to employed Hospitalists taking care of both un-assigned patients as well as patients for an expanding number of non-admitting practices has been challenging challenging in staffing, challenging in coordinated quality, challenging in community acceptance and challenging in integrating the service into the overall care structures.
We have come to a point where CCHS has a team that we can build upon.Cleveland County HealthCare System12
The Perfect StormA New Way to Care for Patients - EMR
What are the elements of this perfect storm? In the analogy, the following would be suggested: The EPACT conversion was a major shift in how care is delivered for almost every care giver leading to huge learning curve anguish along with real system failures and software bugs. This system is what Mayo Clinic pegs their national and international reputation partly upon We have often seen first hand what happens to patients when information is not able to be shared horizontally
This conversion was painful for all and I understand the medical staffs frustration The worst is behind us !
Cleveland County HealthCare System
13
The Perfect StormA Change in our Growth Curve
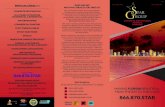
What are the elements of this perfect storm? In the analogy, the following would be suggested: Declining utilization of hospital services have take significant focus of Administration 50% is accounted for in less admissions to anywhere 50% is accounted for by a loss of marketshare to our primary competitor
Patient Discharges16,000 14,000 12,000 10,000 8,000 6,000 4,000 2,000 013547 13851 14167 14443 12776 10663 9295 8702 9015 9130 10593 12402
6775
7482
7866
2008 P
1994
1997
1999
2001
2003
2005
2007
1995
1996
1998
2000
2002
2004
2006
2008 B
Cleveland County HealthCare System
14
The Perfect StormA Change to our Physicians Economic Model
What are the elements of this perfect storm? In the analogy, the following would be suggested: Declining practice profitability leading to real physician economic needs that have been difficult for CCHS to address Increasing rules and regulations keeping us from helping as we once could Declining profitability keeping us from helping because we can no longer afford to
Such issues have taken huge amounts of Administrative time and focus and in some cases also damaged trust This same problem is going on in every marketplace right now
Cleveland County HealthCare System
15
A Different Ending! This strategic plan will take courage, cooperation and great effort to accomplish, but it will assure that healthcare in Cleveland County continues to make a difference in the lives of the people we serve We will come through this storm Together!Cleveland County HealthCare System16
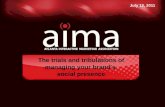
Tough QuestionWhy is Administration getting bigger and the people who do the work are getting smaller?2003 2006
CEO
John Young
CEO
John Young
COO/CNE CRMC
Veronica Poole-Adams
COO/CNE CRMC
Veronica Poole Adams
COO KMH
Vacant (Hank Neal)
COO/CNE KMH
Sheri DeShazo
VP CNE KMH
Regina Gregg
AVP KMH
Nadine Harris
VP Med Staff Dev
Sam Cooper
VP Med Staff Dev
Sam Cooper
VP Support
Alex Bell
VP Support
Alex Bell
Executive VP
Mark Hudson
Executive VP
Mark Hudson
VP Outreach
Dotty Leatherwood
VP Outreach
Dotty Leatherwood
VP CFO
Rose Coyne
VP CFO
Rose Coyne
VP Corporate Counsel
AVP HR
VP Systems
2003 Dan Sweat 23 FTEs 1206 total FTEs Debbie Kale 52.43 FTEs / Exec 4.2 FTEs / AOBLiz Popwell
VP Corporate Counsel
VP HR
VP Systems
Cleveland County Liz Popwell HealthCare System
2006 Dan Sweat 25 FTEs 1301 total Debbie Kale FTEs 52.04 FTEs / Exec 4.6FTEs / AOB
17
Tough QuestionWhy is Administration getting bigger and the people who do the work are getting smaller?2008
CEO
John Young
CNE CRMC
Veronica Poole Adams
2008 17 FTEs 1260 total FTEs 74.11 FTEs / Exec 4.2FTEs / AOB
CNE KMH
Sheri DeShazo
AVP KMH
Nadine Harris
VP Med Staff Dev
Sam Cooper
Retiring end of 08
VP Support
Alex Bell
Executive VP (COO)
Vacant
VP Outreach
Dotty Leatherwood
VP CFO
Rose Coyne
VP Corporate Counsel
Dan Sweat
Promotion to CMC NorthEast
VP HR
Debbie Kale
VP Chief Ancillary Officer (CAO)
Liz Popwell Cleveland County HealthCare System
18
Brian.this is where I end and you begin. I have given you a few slides for each pillar and one slide for 2009 2013 strategy. Feel free to adapt to your needs and style These are all the points in the strategic plan I will take no more than 15 - 20 minutes
Cleveland County HealthCare System
Cleveland County HealthCare System
Strategic Plan 2009-2013
Chart a New Course
Mission StatementCleveland Regional Medical CenterCRMC Kings Mountain Hospital&
As a member of the Cleveland County HealthCare System family serving our community and the surrounding region, Cleveland Regional Medical Center and Kings Mountain Hospital provide a focused variety of safe, high quality, patientcentered services and educational programs for the benefit of the people we serve, regardless of their ability to pay. As a part of the Carolinas HealthCare System, we strive to offer seamless, coordinated systems of clinical care.
Chart a New Course
Mission StatementCleveland Regional Medical CenterCRMC Kings Mountain Hospital&
As an organization that values people, we will live this mission by practicing caring, commitment, integrity and teamwork!
Chart a New Course
Vision StatementCleveland Regional Medical CenterCRMC Kings Mountain Hospital&
Cleveland County HealthCare System will serve the patient first, consistently respond with our best, and champion health in our community. As an integral component of the Carolinas HealthCare System, we will align and grow our services based upon the needs of those we serve and the strategies of our regional system. We will realize this vision through the empowered efforts of a caring, committed healthcare family and an engaged and talented medical staff.Chart a New Course
Strategic Plan 2009 2013Seven Pillars of Commitment
Patients - Families - Community - Physicians - Hospital Family
Employee Satisfaction
QUALITY
Customer Service
Financial / Operational
GROWTH
Community Benefit
Medical Staff
Cleveland County HealthCare System
Chart a New Course
Cleveland County HealthCare System
24
Key Assumptions of the Environment 2009 - 2013 Community growth will slowly accelerate Economic Development will improve gradually Demand for caregivers will exceed supply Competition will increase from many providers Consolidation of healthcare will continue Slow-down of national economy will continue Governmental and payor oversight on quality and access Higher expectations from consumers Declining margins for medical staff Behavioral Health will continue to impact Emergency Rooms HealthCare reform will come, not in the near futureCleveland County HealthCare System25
Pillar for Employee SatisfactionLong Term Goal: To be the Employer of Choice as measured by being in the top decile of Employee Satisfaction Surveys
Quality
Service
Financial Viability
Growth
Employee Satisfaction
Cleveland County HealthCare SystemWe believe that our success is founded on our hospital family; if we focus on our people, everything else gets better! We further believe that the best way to focus on our people is to develop our leaders!Cleveland County HealthCare System26
The Right Mix is essential to Quality% of total employment by employee type2006 NC Hospitals 2008 CRMC & KMH
Nursing 46%
Other 29%Nursing 43%
Other 35%
Administrativ e 11% Allie d he alth 12%
Pharmacy 2%
Allied health 17%
Pharmacy 2% Administrativ e 3%
*NCHA 2008
Cleveland County HealthCare System
Employee Turnover- CCHS
2007 - 20083.0% 2.5% 2.0% 1.5% 1.0% 0.5% 0.0%2.57% 2.72%
Turnover Rate
1 .96% 1 .39% 1 .59% 1 .52% 1 .77% .39% 0.95% 1 .20% 1 .03% 1 0.97%
Threshold
Target
Ju l Au g Se p O ct N ov D ec Ja n Fe b M ar Ap r M ay Ju ne
Maximum Probable
Advisory Board Benchmark Overall Turnover Rate 18.3% annually or 1.5% per month
Cleveland County HealthCare System
Work Climate Survey- CRMC
C R M C E m p lo ye e S u rv e y O v e ra ll S a tis fa c tio n84 82 80 78 76 74 72 2007* 2006*
* CEP Pr o c e s s
2005*
2004*
Ju n e -0 2
M a y -0 0
F e b ru a ry -9 8
Cleveland County HealthCare System
Work Climate Survey- KMH
K M H E m p lo ye e S u rv e y O v e ra ll S a tis fa c tio n80 79 78 77 76 75 74 2007*
* CEP Pr o c e s s
2006*
2003
Cleveland County HealthCare System
Employee Satisfaction Strategic Priorities 2009 - 2013Foster a culture that recognizes the importance of employees and their contributions to system goals: Leadership Development, Sustainability Prioritizing objectives MIP Restructuring
Identify and develop future leaders Employee / Leadership Accountability Recognition Orientation and Re-orientation Care giver training and continuing education Retention of productive members of team Benefit Structure analysis
Maximizing the supply chain of care giver training Leadership Best Practice Principles
Cleveland County HealthCare System
31
Pillar of QualityLong Term Goal: To be in the top Decile in selected publicly reported vertical Quality Indicators
Quality
Service
Financial Viability
Growth
Employee Satisfaction
Cleveland County HealthCare SystemWe believe Quality, from the vertical individual or component level perspective, is the essential foundation of healing.We define Quality as safe, effective, appropriate care that meets or exceeds the needs of all those we serve. Cleveland County HealthCare System
32
CHS & CCHS Enterprise= CRMC Performance = KMH Performance = CHS Performance
Acute Myocardial Infarction100
Heart Failure100 90NC Avg CHS
90
NC Avg CHS
80
80 70
70 Q1 07 n=604 Q2 07 n=565 Q3 07 n=656 Q4 07 n=675 Q1 08 n=632
Q1 07 Q2 07 n=1039 n=976
Q3 07 n=969
Q4 07 Q1 008 n=1161 n=1066
Pneumonia100 90 80 70 60 Q1 07 Q2 07 n=1417 n=1007 Q3 07 n=934 Q4 07 =1469 Q1 08 n=1422NC Avg CHS
Surgical Care Improvement Project*100 90 80 70 Q1 07 Q2 07 Q3 07 Q4 07 Q1 08 n=1926 n=1794 n=1959 n=1696 n=2329*Dotted line represents change in SCIP methodology.
NC Avg CHS
Cleveland County HealthCare System
AHRQ Survey 2008: Overall BenchmarkTeamwo Supervisor rk in expectation units Mgt support Continuous Improvement Overall Feedback and Open-ness Perception of Commun. Safety Frequency of events Teamwork across units Staffing Handoffs Nonpunitive Response
CMC Mercy Pineville University Randolph CMC-Northeast
CRMC KMH
Cleveland County HealthCare System
= above mean
= below mean
Quality Strategic Priorities 2009 - 2013 System-wide approach to Quality and Patient Safety Vision CHS / CCHS CRMC / KMH Acute / Sub Acute Nursing / Radiology (example)
Place the physician in front of the Quality Agenda Maintain existing outcome excellence and develop new outcome excellence Maximize publicly reported Quality Indicators Strategic plan for imaging and hospitalists Patient safety strategy implementation Electronic Medical Records strategyCleveland County HealthCare System35
Pillar of ServiceLong Term goal: To be in the Top Decile in Patient Satisfaction and develop strategies, tactics and systems for excellent horizontal patient care
Quality
Service
Financial Viability
Growth
Employee Satisfaction
Cleveland County HealthCare SystemWe believe Service is quality from the patients perspective and encompasses the horizontal system of healing and compassionate caring.
We define Service as safe, effective, comprehensive, coordinated care that meets or exceeds the needs of all those 36 we serve. Cleveland County HealthCare System
Focus Group PerceptionsMeasure First Mention Awareness Overall Preference Factor Association - Best Doctors - Best Nursing Care - Advanced Equipment/Technology - Caring/Friendly Staff - Most Convenient - Best Reputation for Quality - Best Overall 31% 22% 45% 21% 2% 36% 37% 23% 33% 19% 36% 69% 24% 28% 9% 9% 11% 10% 8% 10% 11% 3% 3% 2% 5% 17% 3% 3% Carolinas Med. Ctr. 7% 19% Cleveland Regional 71% 48% Gaston Memorial 9% 15% Kings Mount. 11% 6%
Cleveland County HealthCare System
Measure - Inpatient Medical/Surgical - Obstetrics - OP Surgery - Emergency - Heart - Cancer - Orthopedic Surgery - Womens Health - Neurological/Neurosurgical - Pediatrics - Diagnostic Imaging Inpatient Utilization Share Emergency Utilization Share OP Surgery Utilization Share OP Services Utilization Share
Carolinas Med. Ctr. 21% 6% 8% 10% 46% 34% 25% 9% 35% 19% 11% 18% 3% 6% 2%
Cleveland Regional 49% 53% 59% 61% 23% 26% 39% 53% 31% 39% 55% 56% 70% 50% 53%
Gaston Memorial 14% 19% 15% 13% 11% 13% 15% 17% 12% 13% 14% 14% 10% 19% 14%
Kings Mount. 5% 3% 6% 10% 2% 1% 3% 5% 4% 4% 8% 4% 16% 9% 15%
Cleveland County HealthCare System
Emergency Department by Calendar Year
Service % Excellent
CRMC Emergency Department
KMH Emergency Department
Cleveland County HealthCare System
Emergency Service Scores thru July 2008
Cleveland Regional Medical Center
Kings Mountain Hospital
Cleveland County HealthCare System
Inpatient Services by Calendar Year Service % Excellent
CRMC Inpatient Satisfaction
KMH Inpatient Satisfaction
Cleveland County HealthCare System
Customer Service Strategic Priorities 2009 - 2013 Develop and deploy a patient relationship management focus for service Strategic Plan for patient advocacy Improve ED throughput Maximize satisfaction scores
Develop, implement and monitor Horizontal Care Hospitalists Oncology Breast Center Medical Patients
Maximize Customer satisfaction ED Outpatient Inpatient HCAPS
Cleveland County HealthCare System
42
Pillar of Financial Viability/ Operational ExcellenceLong Term Goal: On average, meet or exceed A rated and budgeted performance
Quality
Service
Financial Viability
Growth
Employee Satisfaction
Cleveland County HealthCare SystemWe believe in our mission of caring for those in need regardless of ones ability to pay. Though we know the margin is not the mission. We also understand that without a margin there is no Cleveland County HealthCare System mission! 43
Operating MarginCCHS Operating Margin7.00% 6.00%4. 3% 5. 3% 4. 6% 5. 5%3.1% through the second Quarter 08
5.00% 4.00% 3.00% 2.00% 1.00%
4. 2%
4. 4%
3. 4%
3. 6%
3. 3%
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008 B
Actual Operating M argin
Budgeted Operating Margin
3. 1%
Cleveland County HealthCare System
44
Financial Viability/Operational Excellence Strategic Priorities 2009 - 2013 Organizational design and corporate infrastructure for planning and execution Identify opportunities for maximizing economies of scale, efficiencies and productivity Consolidation of Services Prioritization of Services
Advance operational excellence Lean
Maintain A rating in margins and ratio Adopt Management Action Plan process
Cleveland County HealthCare System
45
Pillar of GrowthLong Term Goal: 80% market share in our primary market (CHS & CCHS)
Quality
Service
Financial Viability
Growth
Employee Satisfaction
Cleveland County HealthCare SystemWe believe it unlikely there will be a trend towards higher reimbursement As margins decline, growth becomes essential!Cleveland County HealthCare System46
Outpatient VolumesOut- Patient Visits100000 90000 80000 70000 60000 50000 40000 30000 20000 10000 088,534 74,904 75,635 77,987 87,580
Annualized through second quarter
82,622
33,452 17,146 19,652 22,254
38,257
37,537
39,599
44,650
45,946
ED Visits80,000 70,000 60,000 50,000 40,000 30,000 20,000 10,000 064,645
20 08
20 08 B
Annualized through second quarter
19 94
19 95
19 96
19 97
19 98
19 99
20 00
20 01
20 02
20 03
20 04
20 05
20 06
20 07
P
69,132 70,822
75,796
61,796
61,412
37,094 36,546
33,138
39,405 35,592 38,022 33,336 33,751 35,205
CRMC & KMH ED Visits
2008 Budget
20 08
P 20 08 B
19 94
19 95
19 96
19 97
98
19 99
20 00
20 01
02
03
04
20 05
20 06
20 07
19
20
20
20
Cleveland County HealthCare System
47
Inpatient & Surgery VolumesPatient Discharges16,000 14,000 12,000 10,000 8,000 6,000 4,000 2,000 013547 13851 14167 14443 12776 10663 9295 8702 9015 9130 10593 12402
Annualized through second quarter
6775
7482
7866
2008 P
1994
1997
1999
2001
2003
2005
2007
1995
1996
1998
2000
2002
2004
2006
CCHS Surgical Volume14,000 12,000 10,000 8,000 6,000 4,000 2,000 0 2008 P 2008 B 1994 1996 1999 2001 2003 2004 2006 1995 1997 1998 2000 2002 2005 2007
2008 B
Annualized through second quarter
Inpatient
outpatient
CAS
Column 448
Cleveland County HealthCare System
CMC, CRMC & KMHAll Marketshare from 1993 - 2007 NC Database
Primary Service AreaExpected Marketplace decline =
Updated Q3 2007
Through
-134CMC Actual Decline = -19 115 Discharge gain in CMC Marketshare (code STEMI)
Expected Marketplace decline = -906 CCHS Actual Decline = -1,366 -460 Discharge lost to Competitors Marketshare Gain
Expected Marketplace decline =
-159Caromont Actual Gain = 195 354 Discharge gained in Caromont Marketshare
Expected Marketplace decline = -136 Other Actual Gain = 10 146 Discharge gained in Other Marketshare
h s t e k r a M %
70 60 50 40 30 20 10 0
6 . 8 5
. 8 5
6 . 9 5
3 . 6 5
. 2 1 9 . 0 1
2 1
2 1
4 . 0 1 3 1
3 . 1
5 . 1
5 . 9
3 . 9
6 . 8
4 . 8
. 8
9 . 8
CMC
7 . 9
CRMC
KMH
GMH
Other
1
2004
2005
2006Expected Marketplace decline = -183 KMH Actual Decline = -339 -156 Discharge lost to Competitors Marketshare Gain
2007
HCIA SoleSource
0 1 49
Cleveland County HealthCare System
Growth Strategic Priorities 2009 - 2013 Advance development and alignment of physician and hospital networks Look for partnering opportunities Complete the primary care base expansion around KMH Find new product lines or marketplaces with growth and margin potential Regional approach to cancer care Cardiology at KMH Vascular Surgery Breast Center CT Virtual Cath Wound Management Behavioral Health expansion/replacement Strategies to win back market share Expand campuses to allow for future growth Determine and implement Hallmark Services Compete into Rutherford County Spine Surgery Cardiac Rehab/Wellness Center South Carolina Strategies Medical Oncology Strategic plan Western CHVI strategic plan50
Cleveland County HealthCare System
Pillar of Community BenefitLong Term Goal: Remain a leader in philanthropy and assure that our services to the community exceed our estimated tax liabilityPatients - Families - Community - Physicians - Hospital Family
Employee Satisfaction
QUALITY
Customer Service
Financial / Operational
GROWTH
Community Benefit
Medical Staff
Cleveland County HealthCare SystemWe believe that CCHS must be a good corporate citizen and lead our community in philanthropy.Cleveland County HealthCare System51
Pillar of Medical Staff RelationsLong Term Goal: Significant changes in clinical operations and capital investments will be evaluated and prioritized through the Clinical Council Process with recommendations going to the Medical Executive Committee or the Administrative Council for final approval as appropriate.
Employee Satisfaction
QUALITY
Customer Service
Financial / Operational
GROWTH
Community Benefit
Medical Staff
We believe that our medical staff should be our active partners through the Clinical Practice Councils. Through that partnership, we will maximize the care of the patient as well as the work environment of the caregivers and the physicians.Cleveland County HealthCare System52
Cleveland County HealthCare System
Clinical CouncilsChosen ModelFunctional Integration: Clinical Council Model
CMO
*
TRUSTEES
MECCMO
EXECUTIVES
MANAGERSSERVICE CHIEFS
MEDICAL STAFF
CLINICAL PRACTICE COUNCILS
STAFF
* Dotted line to the Trustees for credentialing and quality issues
The Bard Group 2006- All rights reserved
Cleveland County HealthCare System
53
Medical Staff Relations Strategic Priorities 2009 - 2013 Improve partnerships relationships with physicians in leadership and operational excellence Assure Clinical Councils are successful in guiding change Increase face time with medical staff Increase IT and communication connections with medical staff Assure non-admitting physicians remain connected to hospitals CRMC/KMH Medical Staff Relationships Graduate Medical Education Accelerating process and greater choices for interested acquisition opportunities
Cleveland County HealthCare System
54
The Perfect Storm?
2009 2013 will be a time of change, and a new course will adjust our sails as the head winds arrive!
Chart a New Course
Cleveland County HealthCare System
55
Marketplace Analysis
Cleveland County HealthCare System
56
QUESTIONS
Chart a New Course
Cleveland County HealthCare System
57