2008 BIOM 463 Dr. Nasser Rizk. Secretion: The human adrenal cortex secretes two main...
43
2008 BIOM 463 Dr. Nasser Rizk
-
Upload
angelina-greer -
Category
Documents
-
view
218 -
download
0
Transcript of 2008 BIOM 463 Dr. Nasser Rizk. Secretion: The human adrenal cortex secretes two main...

2008BIOM 463
Dr. Nasser Rizk

Secretion: The human adrenal cortex secretes two main
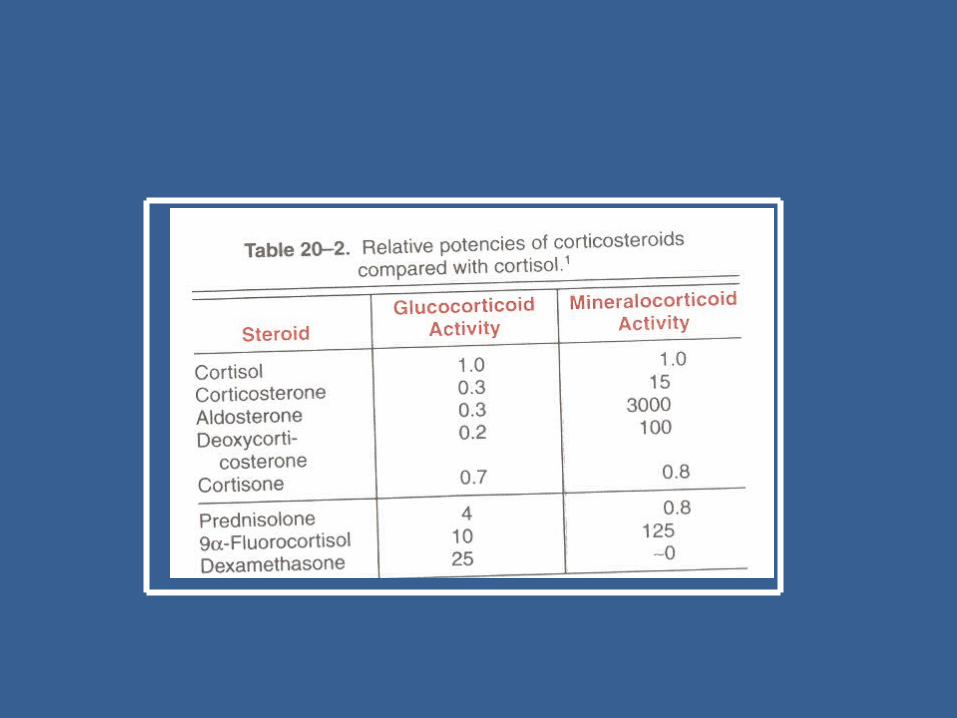
glucocorticoids:1- Cortisol2- Corticosterone
Transport:75% of Cortisol, bound to Globulin (transcortin), and
Corticosterone.15 % bound to albumin10 % is free (active)
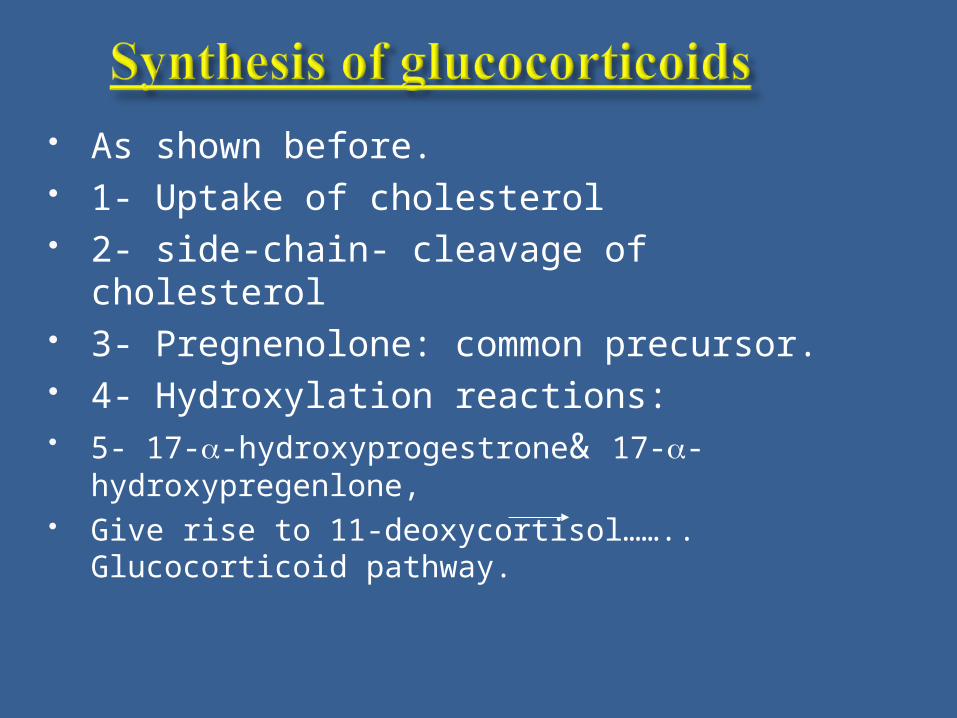
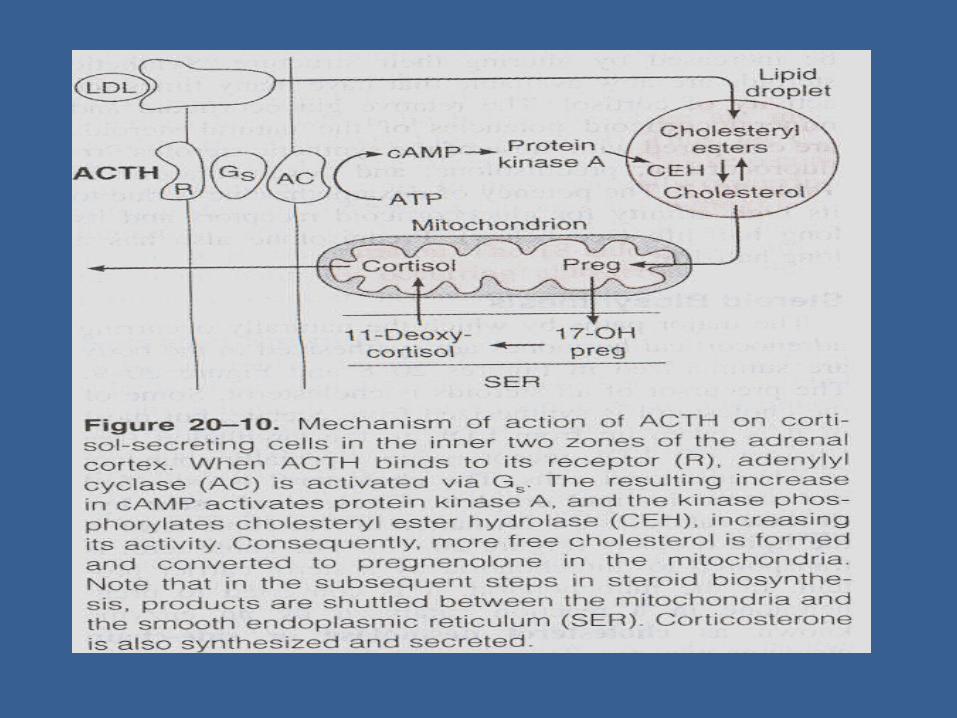
As shown before. 1- Uptake of cholesterol 2- side-chain- cleavage of cholesterol 3- Pregnenolone: common precursor. 4- Hydroxylation reactions: 5- 17--hydroxyprogestrone& 17--
hydroxypregenlone, Give rise to 11-deoxycortisol……..
Glucocorticoid pathway.

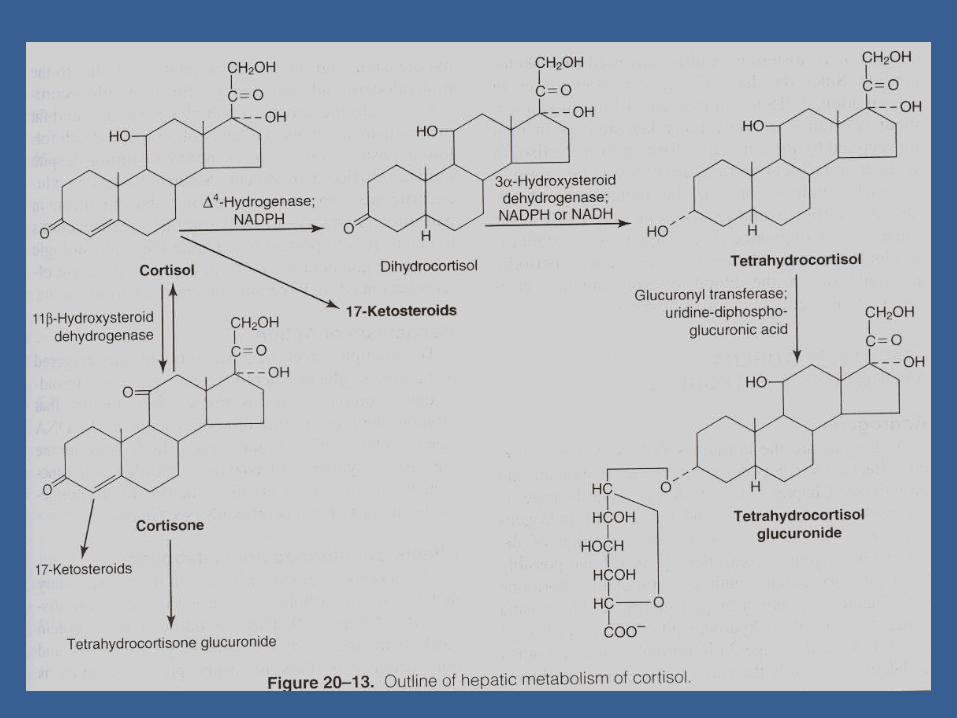
A- general: inactivation of corticosteroids by: 1- Enzymatic reduction to :
2- Conjugation reaction, excreted by kidney. Major urinary metabolite of Cortisol is:
Tetrahydrocortisol glucuronide B- Liver: is the main extra-adrenal site of metabolism.
Cortisol is converted into Cortisone
which is conjugated and reduced to be excreted.
Dihydrocortisol Tetrahydrocortisol

Steroids with 17- hydroxyl groups appear in urine in the form of:
17- Ketosteroids (marker of corticosteroid secretion in humans)
3- Conversion in other extra-adrenal tissues:
Like muscles, skin, fibroblasts, intestine; by oxidation-reduction reactions.

Cortisol
Metabolic
Stressresponse
Mineralocorticoidactivity
Excretionof water
Immune response
CVS role
Pharmacological effectsImmunosuppressive actions
Anti-allergic effectAnti-inflammatory effect

Metabolic effects: 1- Carbohydrate: Hyperglycemic ? A- Gluconeogensis especially Sk.M,
and B- Hepatic glycogenolysis, and C- Anti-insulin effect, decreasing
glucose transport in Sk.M and adipose tissue by inhibiting GLUT1&4 activity.
2- Protein Metabolism: A- Enhance protein breakdown and
release of A.A. in extrahepatic tissue esp. Sk.M & Fat.
B- Liver deals mobilized A.A by deamination, gluconeogensis, Ptn synthesis and Plasma protein formation
It is catabolic hormone.

3- Fat metabolism: It is lipolytic hormone Increased mobilization of fatty acids. This effect is due to potenetiation by other lipolytic
hormones as catecholamines and Somatotrophins. When large amounts of Cortisol are secreted,
could lead to: Centripetal Distribution of fat ( Increased deposition of fat in: trunk, face and neck
regions), as in Cushing's syndrome.

1- Cortisol has a weak mineralocorticoid activity. It helps Na+ reabsorption and enhances excretion of K+ in urine.
2- This weak effect is due to presence of enzyme: 11- hydroxysteroid dehydrogenase ( 11 HSD), which catalyses conversion of active Cortisol into inactive Cortisol.
This enzyme is present in Aldosterone-sensitive tissues.

3- Water metabolism: Depends on the water content of the body; 1- Dehydration: Cortisol has antidiuretic effect
secondary to increased Na+ reabsorption. 2- Hydration: Cortisol has a diuretic effect by: a- Increased renal blood flow and GFR b- Inhibit action of ADH on collecting tubules.
4- CVS effects: Increase vascular tone by potenetiation the effects of catecholamines on blood vessels.

5- Response to stress Stressors as: trauma., hemorrhage, acute
hypoglycemia, febrile stimuli, emotions. All these conditions characterized by marked
increase in ACTH and glucocorticoid concentrations.
This effect is due to: 1- Increase vascular reactivity, 2- Mobilization of F.F.A. from adipose
tissue, and its use as source of energy
Inflammation is characterized by increased capillary permeability, edema, WBC infiltration release of proteolytic enzymes by WBCs, and increase collagen activity.
1-Anti-inflammatory actions: 1- Decrease capillary permeability 2- Stabilize lysosomal membrane of WBCs, inhibit
proteolytic enzymes 3- Decreased infiltration of WBCs into the inflamed area 4-Inhbited fibroblastic activity and collagen deposition
2- Anti-allergic actions: Allergy is characterized by histamine release
from basophil and mast cell which produces: edema, inflammation, V.D in capillaries,
decrease B.P, bronchospasm and could lead to anaphylactic shock, also stimulates salivary, gastric secretions.
Anti-allergic effects: Cortisol inhibits the release of histamine.
3- Immunosuppressive effects:Therapeutic effect of large amounts of
glucocorticoids, inhibit the normal immune response by:
1- Gradual destruction of lymphoid tissues Decrease antibody production, Lymphocytes, Basophiles, and Esinophiles.
This effect is used in tissue transplant , but decrease the ability of the body defense against infections.

Physiologically:
It has a role in regulating the immune response and prevent damage to body. How?
Via interaction between the hypothalamo-hypophyseal- adrenal axis and the immune system as shown in the next fig.
e.g., TNF- released by macrophages is under control by increased production of Cortisol which in turn inhibits macrophages

Adrenalcortex
Macrophages
Cortisol
CRH VP
+VE
+VE
Interleukins(e.g. IL-1)
TNF-( and other toxic substances)
ACTH
ACTH
Hypothalamus
Ant. pit.gland
- Ve
Immune challenge
Interactions between Hypothalamo-hypophysealAdrenocortical axisAnd immune system

4- Effect on blood cells: Decrease number of: Eosinophils, Basophils, and
lymphocytes. Increase: total count of RBCs, WBCs, platelets,
Monocytes and PMNs.
CellCell NormalNormal Cortisol-effectCortisol-effectWBCsWBCsTotal
PMNs
Lymphocytes
Eosinophils
Basophils
Monocytes
RBCsRBCs
90009000
57605760
23702370
270270
6060
450450
5 million5 million
10.00010.000
83008300
10801080
2020
3030
540540
5.2 million5.2 million

5- Effect on calcium and bone:large amounts of glucocorticoids,
1- Antagonizes the effect of Vit D metabolites on calcium absorption of the gut
2- Increase excretion of Ca++ in urine via increase in GFR.
3- May inhibit the secretion of growth hormone from ant. Pituitary gland.
All these effects lead to increase incidence of:
Osteoporosis

6- Other effects: Gastric secretion: increases,
increase incidence of gastric & peptic ulcers.
Nervous system: change in personality.
ACTH secretion: inhibited
1- Like other steroids: affects gene transcription and translation
2- Rapid action: via Lipocortin1 which causes rapid inhibition of ACTH secretion.
The following Fig. show such mechanisms.

Phospholipase A
Arachidonic acid
Prostaglandins &Leukotriens synthesis
Actions
Lipocortin 1
mRNA
New proteinsynthesis
Cortisol
Cortisolreceptor
Actions ? Autocrine effectVia Lipocortin receptor ?
Mechanism of action of Cortisol

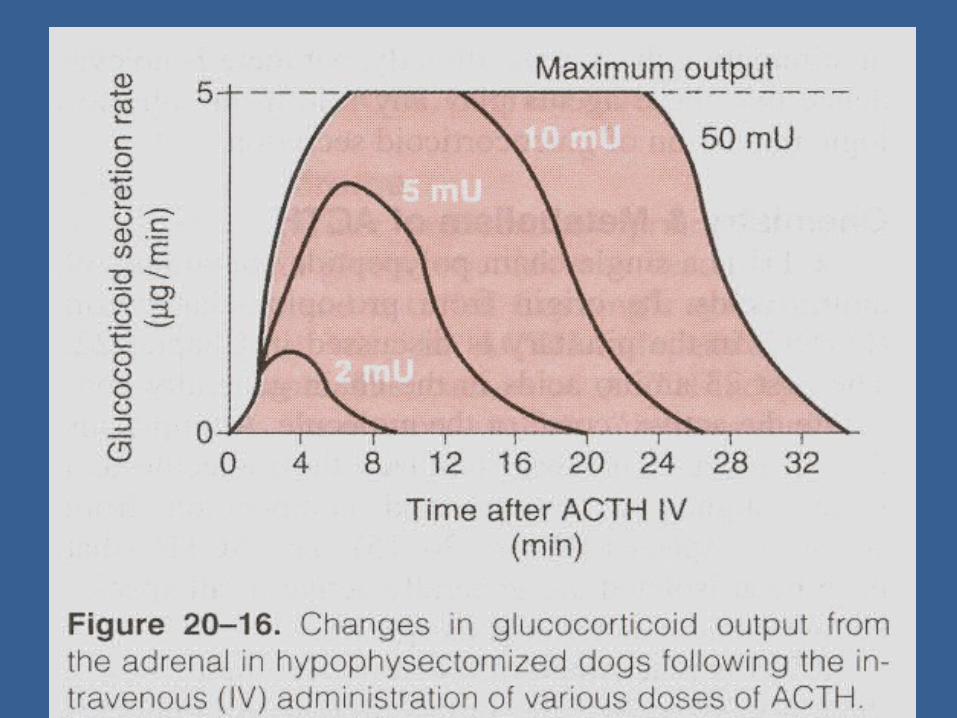
Synthesis and secretion of glucocorticoids is under control of ACTH released from ant.pit.gland (act via cyclic AMP).
ACTH is under control of CRF (CRH) by the hypothalamus.
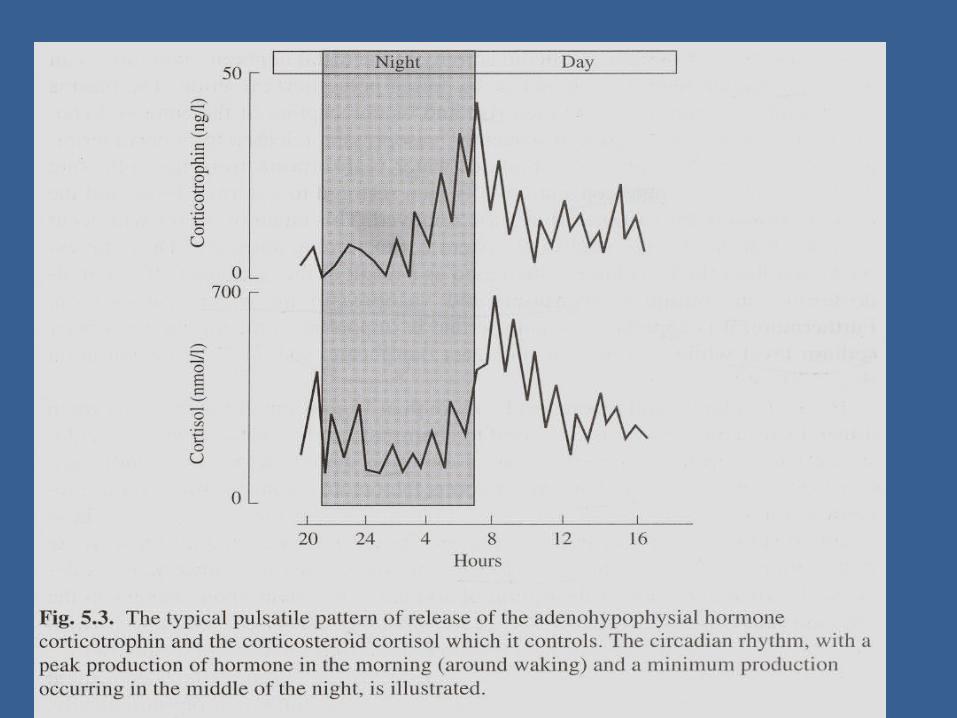
ACTH is secreted in pulsatile manner. Pulses are more frequent early in morning,
least in evening (circadian rhythm). Only Cortisol has a negative –feedback effect
on ACTH and CRH.

Hypothalamo-hypophyseal-adrenocortical axis are stimulated by a wide range of stress conditions including:
Trauma, infections, hypoglycemia Acute anxiety, exercise, pain, Surgery, shock, inflammation, Cold exposure and Psychological stress.

AdrenalCortexCortisol
Stress
Hypothalamus
Direct - ve
Indirect -Ve
Adenohypophesis
Hypothalamo-HypophysealPortal system
Corticotrophin, ACTH
Control of secretionof Cortisol
CRH VP


Functions : In males: little effect compared to testosterone. In females: 1- Appearance and maintenance of pubic and Axillary hair
growth of clitoris. 2- Protein anabolism which promotes physical growth esp.
in prepuberatl stage. 3- Increased secretion of sebaceous glands of the skin and
acne formation.
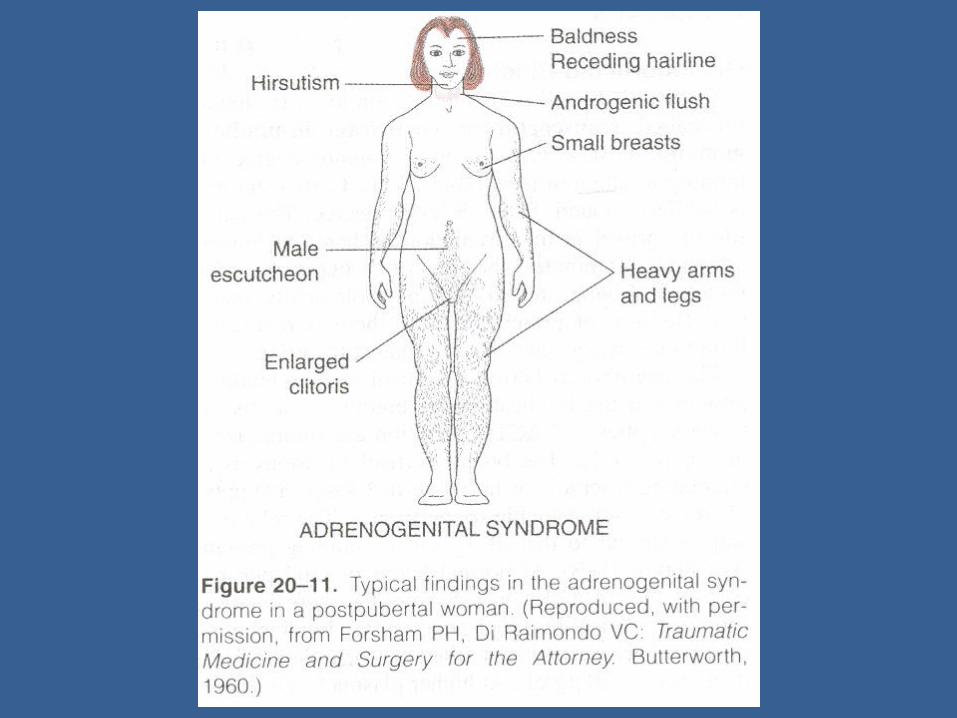
Excess secretion: 1- Excess androgen: adrogenital syndrome and
masculinization in females. 2- Excess glucocorticoids: Cushing’s syndrome: moon face, plethoric appearance, trunk obesity, purple abdominal striae, hypertension, osteoporosis,
protein depletion, mental abnormalities, frequent diabetes mellitus.
3- Excess mineralcorticosteroids lead to: 1- K+ depletion, Na+ retention 2- No edema 3- Weakness, hypertension, tetany, polyurea 4-Hypokalaemic alkalosis.


Addison disease: destruction of adrenal cortex by autoimmune diseases/T.B.
C/P: 1- weight loss, tired, hypotensive, hypoglycemia 2- response to stress leads to shock and collapse “
addisonian crisis” 3- increase ACTH level; which has MSH activity
leads to: tanning of the skin, pigmentation 4- Menstrual abnormalities.


C/p:
Hyperkalemia Salt wasting Hypotension Metabolic acidosis
End of this gland Dr. Nasser Rizk
2008