2006, Vol.19, Issues 4, Cataract Surgery in the New Millennium
117
-
Upload
patriciachristiani -
Category
Documents
-
view
218 -
download
1
description
catarak surgery
Transcript of 2006, Vol.19, Issues 4, Cataract Surgery in the New Millennium

Ophthalmol Clin N Am 19 (2006) ix
Preface
Guest Editor
Mark H. Blecher, MD
We live in times when ideas, research, and expe-rience are shared almost instantly, mostly to the
benefit of our patients. And in few areas more thanin cataract surgery, does the state of the art changemore rapidly. It can then be difficult to decide
when a compendium of the current knowledgebase should be committed to hard copy, and prob-ably great hubris to commit it to hard cover.
I think that in 2006, we have come to a reason-
able consensus on a number of important clinicalquestions in cataract surgery. More importantly,we have been able to enlist the help of surgeons
considered the final word in these areas. It istherefore with some trepidation, but with great
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All r
doi:10.1016/j.ohc.2006.07.010
pride, that I offer to you some of the best articles Ihave ever read on 10 critically important subjects
that I encounter in my practice very day. I amdeeply indebted to some of the smartest andbusiest ophthalmologists for taking the time to
help with this project and hope that you will findit an interesting and useful resource.
Mark H. Blecher, MDPhiladelphia Eye Associates
1703 South Broad Street, Suite 207Philadelphia, PA 19148, USA
E-mail address: [email protected]
ights reserved.
ophthalmology.theclinics.com

Ophthalmol Clin N Am 19 (2006) 415–425
The New Epidemiology of CataractAlison G. Abraham, MHSa, Nathan G. Condon, MD, MPHb,
Emily West Gower, PhDa,*aDana Center for Preventive Ophthalmology, Wilmer Eye Institute, Johns Hopkins School of Medicine,
600 North Wolfe Street, 116 Wilmer Building, Baltimore, MD 21287, USAbHelen Keller International, 352 Park Avenue South, 12th Floor, New York, NY 10010, USA
Cataract poses a substantial economic andpublic health burden and is the leading cause of
blindness worldwide, accounting for nearly 48%of all blindness [1]. As such it is also a disease thathas been and will continue to be a target of epide-
miologic research. Insights into causative factorsamenable to intervention, genetic factors thatpredispose to disease, and avenues for novel
treatment serve to reduce the disease burden.As a result of decades of research into factors
that may cause age-related cataract, several risk
factors have been well-identified and reviewed indetail in other manuscripts [2–6]. More recentstudies, however, have found conflicting resultsfor some risk factors, and have identified other
potential risk factors of interest that need furtherstudy. This article reviews evidence for well-known risk factors, but focuses primarily on
more recent findings and factors in which researchis still evolving.
The burden of disease
Many surveys have been conducted in variouscountries to estimate the prevalence of blindness
and low vision in diverse populations. Data on thecauses of visual impairment yield estimates of thecontribution of cataract to disability. The World
Health Organization estimates that the currentglobal prevalence of blindness is 0.57% (range:0.2%–1%), with more than 82% of all blindness
occurring in individuals aged 50 and older.Cataract accounts for 47.8% of the world’s
* Corresponding author.
E-mail address: [email protected] (E. West Gower).
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All ri
doi:10.1016/j.ohc.2006.07.008
roughly 37 million blind individuals [1]. Of note,approximately 90% of the contribution of cata-
ract to blindness in this study was seen indeveloping countries [1].
The three subtypes of cataract (nuclear, corti-
cal, and posterior subcapsular [PSC]) are seen tovarious extents in different populations. Preva-lence and incidence estimates across populations
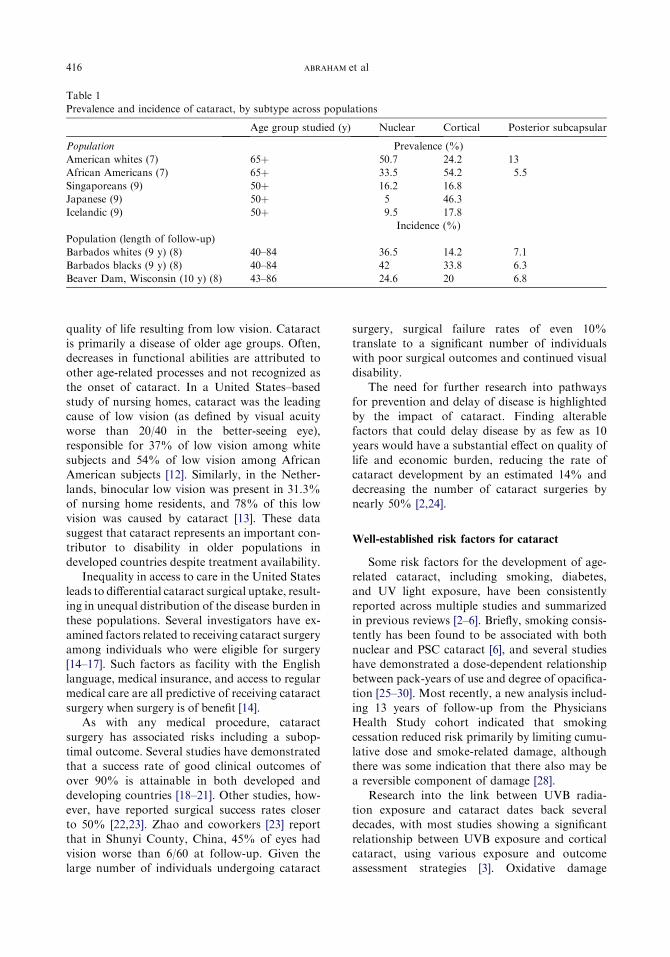
are summarized in Table 1. In the United States,nuclear cataract is seen more commonly in whites,whereas cortical is seen more commonly in Afri-
can Americans; however, PSC cataract is preva-lent at roughly the same, much lower, rate inboth groups [7]. In studies of populations outsidethe United States, various prevalence estimates
for each cataract subtype have been reportedthat may reflect differences in either environmentor predisposition (see Table 1) [7–9].
Impact of disease
Although 90% of cataract cases are found in
developing countries, the disease has a substantialimpact in developed world countries as well fromsocial, physical, and financial perspectives. In the
early 1990s, Steinberg and coworkers [10] esti-mated that Medicare spent more than $3.4 billiondollars annually on routine cataract procedures.Furthermore, approximately 60% of Medicare
spending in the 1990s was devoted to cataractsurgery and associated costs [11]. With the grayingof the United States population, it is expected that
this number will continue to rise dramatically.The burden of cataract extends beyond the
financial costs to society. Patients with prevalent
cataract are likely to have significantly reduced
ghts reserved.
ophthalmology.theclinics.com
416 ABRAHAM et al
Table 1
Prevalence and incidence of cataract, by subtype across populations
Age group studied (y) Nuclear Cortical Posterior subcapsular
Population Prevalence (%)
American whites (7) 65þ 50.7 24.2 13
African Americans (7) 65þ 33.5 54.2 5.5
Singaporeans (9) 50þ 16.2 16.8
Japanese (9) 50þ 5 46.3
Icelandic (9) 50þ 9.5 17.8
Incidence (%)
Population (length of follow-up)
Barbados whites (9 y) (8) 40–84 36.5 14.2 7.1
Barbados blacks (9 y) (8) 40–84 42 33.8 6.3
Beaver Dam, Wisconsin (10 y) (8) 43–86 24.6 20 6.8
quality of life resulting from low vision. Cataractis primarily a disease of older age groups. Often,decreases in functional abilities are attributed to
other age-related processes and not recognized asthe onset of cataract. In a United States–basedstudy of nursing homes, cataract was the leading
cause of low vision (as defined by visual acuityworse than 20/40 in the better-seeing eye),responsible for 37% of low vision among white
subjects and 54% of low vision among AfricanAmerican subjects [12]. Similarly, in the Nether-lands, binocular low vision was present in 31.3%of nursing home residents, and 78% of this low
vision was caused by cataract [13]. These datasuggest that cataract represents an important con-tributor to disability in older populations in
developed countries despite treatment availability.Inequality in access to care in the United States
leads to differential cataract surgical uptake, result-
ing in unequal distribution of the disease burden inthese populations. Several investigators have ex-amined factors related to receiving cataract surgeryamong individuals who were eligible for surgery
[14–17]. Such factors as facility with the Englishlanguage, medical insurance, and access to regularmedical care are all predictive of receiving cataract
surgery when surgery is of benefit [14].As with any medical procedure, cataract
surgery has associated risks including a subop-
timal outcome. Several studies have demonstratedthat a success rate of good clinical outcomes ofover 90% is attainable in both developed and
developing countries [18–21]. Other studies, how-ever, have reported surgical success rates closerto 50% [22,23]. Zhao and coworkers [23] reportthat in Shunyi County, China, 45% of eyes had
vision worse than 6/60 at follow-up. Given thelarge number of individuals undergoing cataract
surgery, surgical failure rates of even 10%translate to a significant number of individualswith poor surgical outcomes and continued visual
disability.The need for further research into pathways
for prevention and delay of disease is highlighted
by the impact of cataract. Finding alterablefactors that could delay disease by as few as 10years would have a substantial effect on quality of
life and economic burden, reducing the rate ofcataract development by an estimated 14% anddecreasing the number of cataract surgeries bynearly 50% [2,24].
Well-established risk factors for cataract
Some risk factors for the development of age-related cataract, including smoking, diabetes,and UV light exposure, have been consistently
reported across multiple studies and summarizedin previous reviews [2–6]. Briefly, smoking consis-tently has been found to be associated with both
nuclear and PSC cataract [6], and several studieshave demonstrated a dose-dependent relationshipbetween pack-years of use and degree of opacifica-
tion [25–30]. Most recently, a new analysis includ-ing 13 years of follow-up from the PhysiciansHealth Study cohort indicated that smokingcessation reduced risk primarily by limiting cumu-
lative dose and smoke-related damage, althoughthere was some indication that there also may bea reversible component of damage [28].
Research into the link between UVB radia-tion exposure and cataract dates back severaldecades, with most studies showing a significant
relationship between UVB exposure and corticalcataract, using various exposure and outcomeassessment strategies [3]. Oxidative damage

417NEW EPIDEMIOLOGY OF CATARACT
resulting from UVB exposure is hypothesized tobe the mechanism through which UVB may in-duce cataract, and the anterior cortical surfacelikely receives the most radiant energy, explaining
the predominant findings of higher cortical cata-ract risk with less or no effect on rates of nuclearcataract and PSC [31]. Furthermore, three studies
characterized the distribution of the position ofopacities, and each found increased risk of corti-cal cataract in the lower nasal quadrant compared
with other areas of the lens [32–34]. It has beenhypothesized that the lower nasal quadrant ofthe lens is the most effected by solar UV exposure
given the angle of the sun during peak UV hours.Quantifying the magnitude of the association isdifficult, however, given that methodology fordetermining exposure varies widely across studies.
Odds ratios range from 1.10 (95% confidenceinterval [CI], 1.02–1.20) per 0.01 Maryland sun-year [35] to 2.48 (95% CI, 1.24–4.99) for cortical
cataract comparing annual exposures greaterthan 564.5 KJ/cm2 with exposures of less than516.7 KJ/cm2 [36].
Study results are highly dependent on themethod used to quantify the exact UV dosagereceived by the lens. Ambient levels are an
imperfect surrogate, because individual behaviorsgreatly modify actual lens exposure given constantambient UVB. Some studies have attempted toovercome this problem by asking detailed ques-
tionnaires that can be used to quantify lifetimesun exposure. Such questionnaires are time-consuming to administer, however, and are lim-
ited by the difficulty that respondents may havewith accurately reporting behaviors from thedistant past. Personal traits, such as iris color
and nutritional status, also may alter the effect ofUVB radiation that reaches the eye. UVB radia-tion may act primarily as a synergistic effect,increasing the rate of an ongoing opacification
process or adding to other oxidative insults toexceed a threshold for cataract formation.
Research into the association between diabetes
and cataract formation dates back to the 1960s. Itwas not until much more recently that prospectivestudies were conducted that allowed examination
of the temporal association between diabetesand incident cataract. Three population-basedprospective studies have reported that diabetes is
a risk factor for both cortical and PSC cataract. Inthe Beaver Dam Eye Study, diabetes mellitus wasassociated with the 5-year incidence of bothcortical and PSC cataract [37]. The Blue Moun-
tains Eye Study yielded similar results, finding
a twofold higher 5-year incidence of cortical cata-ract in participants with impaired fasting glucose(odds ratio, 2.2; 95% CI, 1.1–4.1) and morefrequent PSC incident cataract among diabetics
with newly diagnosed diabetes (odds ratio, 4.5;95% CI, 1.5–13) [38]. A history of diabetes was as-sociated with incident cortical cataract (relative
risk ¼ 2.4; 95% CI, 1.8–3.2) and PSC (relativerisk ¼ 2.9; 95% CI, 1.9–4.5) in the BarbadosEye Study in addition to the finding of a dose-
response relationship between these incidentopacities and increased levels of glycosylatedhemoglobin at baseline [39].
Different effect estimates for diabetes on cata-ract formation have been reported both from agegroups less than approximately 60 years and thoseolder than approximately 60 years. This finding
has been repeated in a number of studies [40–42].A diminishing effect of diabetes on cataractogene-sis in older age groups may indicate either an in-
creasing influence of other factors therebywashing out the effect of diabetes or a survivorbias, such that severe diabetes leads to early
mortality leaving only healthier survivors in theolder age groups. An interaction has also beennoted in some studies with glycated hemoglobin
such that an association between glycated hemo-globin and cataract is seen only in diabetics[37,43]. Such a result may indicate tight glucosecontrol can minimize the risk of cataract in those
with diabetes, as has been demonstrated withother diabetes-associated ocular conditions [44].
Risk factors where current understanding
is evolving or reflects conflicting results
Myopia
Population studies suggest that the prevalenceof myopia may be increasing over time in someareas, the implication of which is higher rates of
some of the myopia-associated ocular pathologicconditions [45]. Recent research provides clinicalevidence for an association between myopia andnuclear cataract formation. Several cross-sec-
tional studies reported an association betweenmyopia and prevalent nuclear cataract; however,prospective studies were needed to confirm the
temporality of the association because nuclearcataract itself can contribute to increased lenspower and myopia. Indeed, recently published
prospective studies have reported somewhat dif-ferent results from cross-sectional studies of thesame population. In the prevalence study of the
418 ABRAHAM et al
Visual Impairment Project conducted in Aus-tralia, an association between myopia and alltypes of cataract was reported [46]. In the prospec-
tive study published in 2006, myopia was onlya risk factor for cortical cataract, reportinga 2.2-fold increased risk (95% CI, 1.4–3.4) of inci-dent cortical cataract [47]. This study is the first to
report an association between myopia and inci-dent cortical cataract. In Beaver Dam, anassociation between myopia and prevalent nuclear
cataract was seen; however, no association wasseen between myopia and incident cataract [48].The Blue Mountains Eye Study reports a 3.3-
fold increased risk of incident nuclear cataractamong individuals with high myopia (�6 diopter[D]) and a 5.4-fold increased risk of PSC (95%CI, 2.5–11.9) cataract formation among individ-
uals with moderate to high myopia (�3.5 D). Fur-thermore, for persons aged 70 years or older,a myopic shift in refraction was associated with
incident nuclear cataract, cortical cataract, andPSC [49,50]. In the Barbados Eye Study, myopia,defined as less than �0.5 D, was associated with
incident nuclear cataract (relative risk ¼ 2.8) [51].Recent findings reported from the Salisbury Eye
Evaluation demonstrate the importance in the
temporality of this association. Cross-sectionalassociations were reported for both nuclearcataract and PSC. An additional finding was anassociation between early spectacle wear and PSC,
a possible indicator of the temporality of therelationship between myopia and PSC [52]. Themechanism throughwhichmyopiamay act to cause
cataract is unknown, although damage-inducedlipid-peroxidation has been hypothesized [45].
Nutrition and supplement usage
Oxidative damage is a putative contributor tothe mechanisms of cataractogenesis for bothnuclear and cortical cataract. Much interest has
been generated by dietary constituents that haveantioxidative properties. Levels of many antioxi-dants exist naturally in the various structures ofthe eye, protecting tissues from the myriad
oxidative insults to which the eye is subject [53].Many epidemiologic studies have evaluated therole of vitamins and micronutrients in preventing
cataract, with nutrient measurements varyingfrom dietary intake to supplement use and plasmalevels of the vitamins in question. The types of
measurement used and the outcome types, rang-ing from cataract extraction to prevalence of cat-aract at 5-year follow-up, make comparisons
across studies difficult. Additionally, teasing outthe association of an individual nutritional factoris difficult because of the colinearity among
various nutritional factors. Individuals who arenutritionally replete in one factor are likely repletein most factors of interest.
A 2000 review of the literature of observational
studies conducted by Wu and Leske [54] high-lights the conflicting data on nutrients in preven-tion of cataract and demonstrates that even
within the same study population, results mayvary over time. For instance, within their ownstudies, the Lens Opacities Case-Control Study
(LOCS) [55] and the Longitudinal Cataract Study[56], a longitudinal study of the LOCS population,discrepant results were found. In LOCS, dietaryintake of vitamin C seemed to provide protection
against nuclear cataract [55], whereas in the longi-tudinal study more recently reported [56], theassociation was not found. On the contrary,
when evaluating vitamin E supplementation, noassociation was seen in the case control study[55] but a protective association with nuclear opa-
cification was reported in the longitudinal study[56]. Similar conflicting results have been reportedfor the Nurses’ Health Study and the Physicians’
Health Study.Researchers have hoped that clinical trials
would help to clarify the role of nutrients andcataract prevention, and would demonstrate pro-
tection against cataract development or progres-sion. The Physicians’ Health Study II evaluatingbetacarotene, vitamin A and E, and multivitamins
[57] and the Italian-American Clinical Trial ofNutritional Supplements and Age-related Cata-ract evaluating multivitamin use [58] are currently
underway, and follow-up will be completed in thenext few years; however, most recently reportedtrial results do not support the hypothesis ofprotection from vitamins. The Age-related Eye
Disease Study reported no association betweensupplementation with vitamin C, vitamin E, andbetacarotene and 7-year risk of development or
progression of lens opacities [59]; likewise, theVitamin E, Cataract and Age-related Maculop-athy Trial evaluating vitamin E given for 4 years
reported no overall association between supple-mentation and incidence or progression of lensopacities [60]. These findings are in contrast to
two earlier clinical trials of vitamin supplementa-tion in a population in China with borderline nu-tritional status, which demonstrated a protectiveeffect of supplementation on development of nu-
clear opacities, albeit in only one supplement

419NEW EPIDEMIOLOGY OF CATARACT
combination out of several studied [61]. Theseconflicting results highlight the importance ofthe nutritional status of the population beingstudied. Although evidence of a role for nutri-
tional supplementation in retarding the progressof cataract is currently lacking for nutritionallyreplete populations, an ongoing study in southern
India, the Antioxidants and Prevention of Cata-ract Study, may provide further insight into thepotential role of supplementation in less well-
nourished groups, where the bulk of cataractblindness exists.
Weight status and fat consumption
Many factors relating to health and nutritionare interrelated, making the individual associationof a specific factor difficult to tease apart. Severalstudies have evaluated the relationship between
body mass index and cataract. The Nurses’ HealthStudy cohort, the Physicians Health Study cohort,the Framingham cohort, and the Beaver Dam Eye
Study cohort have all reported associationsbetween body mass index and PSC cataract[37,62–65]. The nature of the relationship between
bodymass index and cataract has not been fully elu-cidated; however, some studies suggest a U-shapedrelationship. Numerous other studies have re-
ported associations with cortical and nuclear cata-racts and null findings [63,66–69]. The role ofcentral adiposity is even more unclear [41,62].
Research also has focused on the contribution
of dietary fat and serum lipids to cataract risk[70,71]. Of particular interest may be the contribu-tion of fatty acids to both cataract development
and protection. One cross-sectional study in theNurses Health Study cohort found a higher riskof nuclear cataract among nurses who consumed
the highest amount of linoleic and linolenic acid[72]. Lens research has confirmed a cytotoxiceffect of these and other unsaturated, cis-config-
ured fatty acids on lens epithelial cells, an effectthat seems to be moderated by aqueous albuminconcentrations that may rise with age [73]. Suchresults could have implications for diseases, such
as diabetes where plasma free fatty acid levelstend to be elevated. In a second longitudinal studyof the Nurses Health Study cohort eicosapentae-
noic and docosahexaenoic acid were found to beprotective against cataract extraction, whereaslinoleic and linolenic acid were not strongly
associated with the outcome [74].Findings from the various studies of lipid
metabolism, obesity, diabetes, and opacification
of the lens may be scratching the surface ofa complex etiologic web. Animal studies mayindicate that these factors interact to promotecataract development and modification of one
factormay be used to reduce risk from another [75].
Corticosteroids
Numerous studies have reported associations
between oral corticosteroid use and cataractformation. As early as 1960, studies indicateda causal role of systemic steroids in PSC de-
velopment [76]. Many reviews have been writtenon the topic summarizing the evidence for anassociation between cataract and both oral and in-
haled steroids [77–81]. Evidence for oral steroiduse as a risk factor for cataract is stronger thanthat for inhaled steroids. The use of oral cortico-steroids for the treatment of inflammatory and
immune disorders, such as asthma, rheumatoidarthritis, and lupus erythematosus, providedearly evidence of an increased prevalence of PSC
formation in exposed individuals, particularlychildren [76,82–87]. Controlled trials of steroidsused in combination with other therapy have
strengthened the case for a causative role of oralsteroids in PSC progression. Patients randomizedto receive oral steroids for immunosuppression
showed consistently higher rates of PSC[80,88,89]. The prevalence of PSC seems to be sen-sitive to both the dose and duration of steroid ad-ministration [76,80,82,83,90].
More recent literature has focused on the roleof inhaled corticosteroids on cataract formation.A review by Allen and coworkers [81] summarizes
the data through 2003. A cursory review of theliterature might suggest conflicting informationbecause multiple studies report no association
between inhaled corticosteroids and cataract[90–92]. These studies are based on small popula-tions of primarily children and young adults who
are unlikely to develop this typically age-relatedcondition [91,92], however, or they focus ona small population in which oral steroids were
used, making it more difficult to isolate the associ-
ation with inhaled steroids [90]. Three case-con-trol studies examining cataract diagnosis andextraction without regard to type found
participants taking inhaled steroids to be at higherrisk of prevalent cataract [93–96]. Most recently,a large cross-sectional survey of the Blue Moun-
tains Eye Study cohort found a relative prevalenceof 1.9 (95% CI, 1.3–2.8) for PSC and 1.5 (95% CI,1.2–1.9) for nuclear cataract among subjects using

420 ABRAHAM et al
inhaled corticosteroids compared with those withno inhaled corticosteroid use [95]. Cumming andMitchell [97] suggest that the evidence for inhaled
steroid on cataract formation is at least as strongas that for oral steroid use in their cross-sectionalstudy and that future studies should evaluatewhether direct entry of corticosteroid into the
eye because of poor inhaler technique may playa role. Prospective studies of inhaled steroid usersmay help to confirm the role of their use in
cataract development.It should be noted that several factors may
complicate the detection of small effects from
inhaled steroids. The particular lesions associatedwith steroid use may have a reversible componentand can be difficult to detect because they rarelyaffect vision [80,98]. In addition, there may be
a large degree of variability in individual suscepti-bility, and synergism with other cataractogenicfactors may ultimately determine any individual’s
PSC outcome [78,80,99].
Exogenous estrogens
A large body of evidence suggests that across
racial groups, women have higher rates of cata-ract, even when adjusting for women’s greaterlongevity [31,39,46,100–104]. Postmenopausal es-
trogen decline has been hypothesized to playa role. Research into the causal relationship of ex-ogenous hormone use and cataract risk, however,
has provided conflicting results. In both the Bea-ver Dam and Salisbury populations, prevalencedata suggested a relationship between current hor-
mone-replacement therapy use and decreased nu-clear cataract. In Salisbury, an association alsowas seen with PSC. Recently published prospec-tive evaluations of both of these two populations
reported no association, however, between hor-mone-replacement therapy and any cataract for-mation. Additionally, whereas the Blue
Mountains research group concludes that thereis some evidence of a protective associationbetween estrogen use and incident cataract
formation [105], the recently reported Visual Im-pairment Project found no association betweenfemale hormonal use and cataract [47]. Clearly,the role of hormone-replacement therapy in
cataract prevention has not been fully elucidated.
Genetics
The role of genetics in the development ofcataract is a question of increasing interest. Findinggenes that contribute to the mechanism of
cataractogenesismayeventually lead togeneproducttargets for intervention. Further, such informationcould aid in identifying predisposed individuals who
might be more susceptible to other cataract riskfactors, such as UV exposure [24]. The FraminghamEye Study examined familial aggregation of lensopacities and found that the odds of a nuclear cata-
ract or PSC were three times higher among thosewith affected siblings compared with those withoutan affected sibling [106]. In the Beaver Dam Eye
Study, the contribution of a single gene to the vari-ability in sex- and age-adjusted measures of nuclearand cortical cataract was estimated to be as high as
35% and 58%, respectively [107,108].The Twin Eye Study went one step further,
estimating both the contribution of genetic andenvironmental factors to various cataract pheno-
types. The authors found that the total variability innuclear cataract development was partitioned asfollows: heritability accounted for 48% (95% CI,
42%–54%); age accounted for 38% (95%CI, 31%–44%); and unique environmental effects accountedfor 14% (95%CI, 12%–18%) [109]. A similar inves-
tigation of cortical cataract found that dominantgenes were estimated to contribute to 38% (95%CI, 1%–64%); additive genes contributed to
20% (95% CI, 0%–57%); age contributed to 16%(95% CI, 12%–21%); and the environment ac-counted for 26% (95% CI, 22%–31%) [110]. Twostudies in the Salisbury cohort estimated the magni-
tude of heritability to be 35.6% (95% CI, 21%–50.3%) for nuclear cataract and 24% (95% CI,6%–42%) for cortical cataract [111,112].
At least two genes have been reported to beassociated with an increased risk for age-relatedcataract itself among Japanese populations;
however, the relationships have not been replicatedin other populations. Sekine and coworkers [113]found a significantly higher frequency of deletionof the gene for glutathione-S-transferase, a key
enzyme involved in free-oxygen radical scavenging,among Japanese patients with typical age-relatedcataract as compared with age-matched controls.
The mean age of cataract patients with the genedeletion was significantly younger than for patientspossessing the normal gene. Alberti and coworkers
[114] failed to replicate these results in an Italianpopulation, and the role of this gene also seemsvariable in other populations [115,116].
Another candidate gene currently available for
age-related cataract is galactokinase. A deficiencyof this enzyme is the cause of a disorder involvinghypergalactosemia and early cataract formation.
A novel variant of galactokinase, identified during

421NEW EPIDEMIOLOGY OF CATARACT
newborn screening for hypergalactosemia, hasbeen associated with a twofold increased risk forage-related nuclear cataract among Japaneseindividuals [117]. The original investigators failed
to find evidence of this particular variant amongblacks andwhites in theUnited States, andother in-vestigators have failed to find an association
between galactokinase alleles and cataract in anItalian population [118]. Finally, a locus associatedwith cortical cataract on chromosome 6 has been
reported from the Beaver Dam population [119].
Markers of inflammation
A very recent interest in markers of inflamma-
tion and vascular endothelial dysfunction aspredictors of cataract has yielded some results.Inflammation is thought to play a role in thepathogenesis of at least PSC. A study by Klein
and coworkers [120] using serum samplesobtained between 1988 and 1990 from the BeaverDam cohort found that higher levels of tumor
necrosis factor-a, interleukin-6, and serum solubleintercellular adhesion molecule-1 were associatedwith prevalent nuclear cataract. Little previous
evidence exists concerning these and othermarkers of inflammation and the risk of cataract.It is hoped that further studies will follow.
Future directions
Recent research supports the theory that the
development of any cataract phenotype is likelythe result of a multifactorial process except in rareinstances of very large occupational exposures.
The future of cataract research will be in morecomplex study designs looking at multiple factorsthat contribute to a single mechanism of
cataractogenesis.The need to standardize exposure and outcome
measurements will become more important asclinicians seek to synthesize data better from
multiple studies. Standardizing exposure assess-ment entails finding a consensus on the mostbiologically meaningful measure of the exposure
of interest. Not only must an appropriatemeasurement instrument be considered but alsofinding a relevant exposure time window. For
exposures with a hypothesized long lag periodbetween exposure and a detectable preclinicalphase of disease, such as smoking and environ-
mental UV, quantifying the appropriatemagnitude of exposure can be challenging. Mea-surements may be subject to recall bias in
nonprospective study designs. Further, systemicor environmental measures of an exposure maynot be linearly related to ocular exposures, such asin studies of antioxidants and dietary constituents.
Outcome assessment is complicated by themany systems of cataract severity measurement.These systems rely on different standards for
judging levels of severity. Often these ordinalscales are reduced to a dichotomous measure ofcataract or no cataract and information regarding
the progression of early disease is lost.Cataract research is still a fertile field for
investigation. The high prevalence of the disease
in older age groups makes the elucidation of evenweak modifiable risk factors clinically significant.Few diseases have as great an impact on publichealth worldwide.
References
[1] Resnikoff S, Pascolini D, Etya’ale D, et al. Global
data on visual impairment in the year 2002. Bull
World Health Organ 2004;82:844–51.
[2] West SK, Valmadrid CT. Epidemiology of risk
factors for age-related cataract. Surv Ophthalmol
1995;39:323–34.
[3] McCarty CA, Taylor HR. A review of the epidemi-
ologic evidence linking ultraviolet radiation and
cataracts. Dev Ophthalmol 2002;35:21–31.
[4] Hodge WG, Whitcher JP, Satariano W. Risk
factors for age-related cataracts. Epidemiol Rev
1995;17:336–46.
[5] Taylor HR. Epidemiology of age-related cataract.
Eye 1999;13(Pt 3b):445–8.
[6] DeBlack SS. Cigarette smoking as a risk factor for
cataract and age-related macular degeneration:
a review of the literature. Optometry 2003;74:
99–110.
[7] West SK, Munoz B, Schein OD, et al. Racial
differences in lens opacities: the Salisbury Eye
Evaluation (SEE) Project. Am J Epidemiol 1998;
148:1033–9.
[8] Klein BE, Klein R, Lee KE, et al. Socioeconomic
and lifestyle factors and the 10-year incidence of
age-related cataracts. Am J Ophthalmol 2003;136:
506–12.
[9] Sasaki K, Sasaki H, Jonasson F, et al. Racial differ-
ences of lens transparency properties with aging
and prevalence of age-related cataract applying
a WHO classification system. Ophthalmic Res
2004;36:332–40.
[10] Steinberg EP, Javitt JC, Sharkey PD, et al. The con-
tent and cost of cataract surgery. Arch Ophthalmol
1993;111:1041–9.
[11] Ellwein LB, Urato CJ. Use of eye care and associ-
ated charges among the Medicare population:
1991–1998. Arch Ophthalmol 2002;120:804–11.

422 ABRAHAM et al
[12] Friedman DS, West SK, Munoz B, et al. Racial
variations in causes of vision loss in nursing homes:
the Salisbury Eye Evaluation in Nursing Home
Groups (SEEING) Study. Arch Ophthalmol 2004;
122:1019–24.
[13] de Winter LJ, Hoyng CB, Froeling PG, et al. Prev-
alence of remediable disability due to low vision
among institutionalised elderly people. Gerontol-
ogy 2004;50:96–101.
[14] BromanAT,HafizG,Munoz B, et al. Cataract and
barriers to cataract surgery in a US Hispanic pop-
ulation: Proyecto VER. Arch Ophthalmol 2005;
123:1231–6.
[15] Javitt JC, Kendix M, Tielsch JM, et al. Geographic
variation in utilization of cataract surgery. Med
Care 1995;33:90–105.
[16] Younan C, Mitchell P, Cumming R, et al. Socio-
economic status and incident cataract surgery: the
Blue Mountains Eye Study. Clin Experiment Oph-
thalmol 2002;30:163–7.
[17] Orr P, Barron Y, Schein OD, et al. Eye care uti-
lization by older Americans: the SEE Project.
Salisbury Eye Evaluation. Ophthalmology 1999;
106:904–9.
[18] Hennig A, Evans JR, Pradhan D, et al. Rando-
mised controlled trial of anterior-chamber intraoc-
ular lenses. Lancet 1997;349:1129–33.
[19] Natchiar GN, Thulasiraj RD, Negrel AD, et al.
TheMadurai Intraocular Lens Study. I: A random-
ized clinical trial comparing complications and vi-
sion outcomes of intracapsular cataract extraction
and extracapsular cataract extraction with poste-
rior chamber intraocular lens. Am J Ophthalmol
1998;125:1–13.
[20] PoweNR, Schein OD,Gieser SC, et al. Synthesis of
the literature on visual acuity and complications
following cataract extraction with intraocular lens
implantation. Cataract Patient Outcome Research
Team. Arch Ophthalmol 1994;112:239–52.
[21] Desai P, Minassian DC, Reidy A. National Cata-
ract Surgery Survey 1997–8: a report of the results
of the clinical outcomes. Br J Ophthalmol 1999;
83:1336–40.
[22] HeM, Xu J, Li S, et al. Visual acuity and quality of
life in patients with cataract in Doumen County,
China. Ophthalmology 1999;106:1609–15.
[23] Zhao J, Sui R, Jia L, et al. Visual acuity and quality
of life outcomes in patients with cataract in Shunyi
County, China. Am J Ophthalmol 1998;126:
515–23.
[24] McCarty CA, Taylor HR. The genetics of cataract.
Invest Ophthalmol Vis Sci 2001;42:1677–8.
[25] Hiller R, Sperduto RD, PodgorMJ, et al. Cigarette
Smoking and the risk of development of lens opac-
ities. The Framingham Studies. Arch Ophthalmol
1997;115:1113–8.
[26] Flaye DE, Sullivan KN, Cullinan TR, et al. Cata-
racts and cigarette smoking. The City Eye Study.
Eye 1989;3(Pt 4):379–84.
[27] West S, Munoz B, Emmett EA, et al. Cigarette
smoking and risk of nuclear cataracts. Arch Oph-
thalmol 1989;107:1166–9.
[28] ChristenWG, Glynn RJ, Ajani UA, et al. Smoking
cessation and risk of age-related cataract in men.
JAMA 2000;284:713–6.
[29] Hankinson SE, Willett WC, Colditz GA, et al.
A prospective study of cigarette smoking and
risk of cataract surgery in women. JAMA 1992;
268:994–8.
[30] West S, Munoz B, Schein OD, et al. Cigarette
smoking and risk for progression of nuclear opaci-
ties. Arch Ophthalmol 1995;113:1377–80.
[31] West SK,DuncanDD,Munoz B, et al. Sunlight ex-
posure and risk of lens opacities in a population-
based study: the Salisbury Eye Evaluation Project.
JAMA 1998;280:714–8.
[32] Sasaki H, Kawakami Y, OnoM, et al. Localization
of cortical cataract in subjects of diverse races and
latitude. InvestOphthalmolVis Sci 2003;44:4210–4.
[33] Schein OD,West S, Munoz B, et al. Cortical lentic-
ular opacification: distribution and location in
a longitudinal study. Invest Ophthalmol Vis Sci
1994;35:363–6.
[34] Rochtchina E,Mitchell P, CoroneoM, et al. Lower
nasal distribution of cortical cataract: the Blue
Mountains Eye Study. Clin Experiment Ophthal-
mol 2001;29:111–5.
[35] Bochow TW, West SK, Azar A, et al. Ultraviolet
light exposure and risk of posterior subcapsular
cataracts. Arch Ophthalmol 1989;107:369–72.
[36] Delcourt C, Carriere I, Ponton-Sanchez A, et al.
Light exposure and the risk of cortical, nuclear,
and posterior subcapsular cataracts: the Patholo-
gies Oculaires Liees a L’Age (POLA) Study. Arch
Ophthalmol 2000;118:385–92.
[37] Klein BE, Klein R, Lee KE. Diabetes, cardiovascu-
lar disease, selected cardiovascular disease risk fac-
tors, and the 5-year incidenceof age-related cataract
and progression of lens opacities: the Beaver Dam
Eye Study. Am J Ophthalmol 1998;126:782–90.
[38] Saxena S,Mitchell P, Rochtchina E. Five-year inci-
dence of cataract in older persons with diabetes
and pre-diabetes. Ophthalmic Epidemiol 2004;11:
271–7.
[39] Hennis A, Wu SY, Nemesure B, et al. Risk factors
for incident cortical and posterior subcapsular lens
opacities in the Barbados Eye Studies. Arch Oph-
thalmol 2004;122:525–30.
[40] Ederer F, Hiller R, Taylor HR. Senile lens changes
and diabetes in two population studies. Am J Oph-
thalmol 1981;91:381–95.
[41] Leske MC, Wu SY, Hennis A, et al. Diabetes, hy-
pertension, and central obesity as cataract risk fac-
tors in a black population. The Barbados Eye
Study. Ophthalmology 1999;106:35–41.
[42] Tavani A, Negri E, La Vecchia C. Selected diseases
and risk of cataracts in women: a case-control study
from northern Italy. Ann Epidemiol 1995;5:234–8.

423NEW EPIDEMIOLOGY OF CATARACT
[43] Miglior S, Bergamini F, Migliavacca L, et al. Met-
abolic and social risk factors in a cataractous pop-
ulation: a case-control study. Dev Ophthalmol
1989;17:158–64.
[44] Cundiff DK, Nigg CR. Diet and diabetic retinopa-
thy: insights from the Diabetes Control and Com-
plications Trial (DCCT). MedGenMed 2005;7:3.
[45] Saw SM, Gazzard G, Shih-Yen EC, et al. Myopia
and associated pathological complications. Oph-
thalmic Physiol Opt 2005;25:381–91.
[46] McCarty CA,Mukesh BN, FuCL, et al. The epide-
miology of cataract in Australia. Am J Ophthalmol
1999;128:446–65.
[47] Mukesh BN, Le A, Dimitrov PN, et al. Develop-
ment of cataract and associated risk factors: the Vi-
sual Impairment Project. Arch Ophthalmol 2006;
124:79–85.
[48] Wong TY, Klein BE, Klein R, et al. Refractive
errors and incident cataracts: the Beaver Dam
Eye Study. Invest Ophthalmol Vis Sci 2001;42:
1449–54.
[49] Panchapakesan J, Rochtchina E, Mitchell P. Myo-
pic refractive shift caused by incident cataract: the
BlueMountains Eye Study. Ophthalmic Epidemiol
2003;10:241–7.
[50] Younan C, Mitchell P, Cumming RG, et al. Myo-
pia and incident cataract and cataract surgery: the
Blue Mountains Eye Study. Invest Ophthalmol
Vis Sci 2002;43:3625–32.
[51] Leske MC,Wu SY, Nemesure B, et al. Risk factors
for incident nuclear opacities. Ophthalmology
2002;109:1303–8.
[52] Chang MA, Congdon NG, Bykhovskaya I, et al.
The association between myopia and various sub-
types of lens opacity: SEE (Salisbury Eye Evalua-
tion) Project. Ophthalmology 2005;112:1395–401.
[53] Trevithick JR, Mitton KP. Vitamin C and E in cat-
aract risk reduction. Int Ophthalmol Clin 2000;40:
59–69.
[54] Wu SY, Leske MC. Antioxidants and cataract for-
mation: a summary review. Int Ophthalmol Clin
2000;40:71–81.
[55] Leske MC, Chylack LT Jr, Wu SY. The lens opac-
ities case-control study: risk factors for cataract.
Arch Ophthalmol 1991;109:244–51.
[56] LeskeMC, Chylack LT Jr, He Q, et al. Antioxidant
vitamins and nuclear opacities: the Longitudinal
StudyofCataract.Ophthalmology 1998;105:831–6.
[57] Christen WG, Gaziano JM, Hennekens CH. De-
sign of Physicians’ Health Study II. A random-
ized trial of beta-carotene, vitamins E and C,
and multivitamins, in prevention of cancer, car-
diovascular disease, and eye disease, and review
of results of completed trials. Ann Epidemiol
2000;10:125–34.
[58] The Italian-American Clinical Trial of Nutritional
Supplements and Age-Related Cataract (CTNS).
Design implications. CTNS Report No. 1. Control
Clin Trials 2003;24:815–29.
[59] A randomized placebo-controlled, clinical trial of
high-dose supplementation with vitamins C and E
and beta carotene for age-related cataract and vi-
sion loss: AREDSReport No. 9. Arch Ophthalmol
2001;119:1439–52.
[60] McNeil JJ, Robman L, Tikellis G, et al. Vitamin E
supplementation and cataract: randomized con-
trolled trial. Ophthalmology 2004;111:75–84.
[61] Sperduto RD, Hu TS, Milton RC, et al. The Lin-
xian Cataract Studies: two nutrition intervention
trials. Arch Ophthalmol 1993;111:1246–53.
[62] Jacques PF, Moeller SM, Hankinson SE, et al.
Weight status, abdominal adiposity, diabetes, and
early age-related lens opacities. Am J Clin Nutr
2003;78:400–5.
[63] GlynnR, ChristenW,Manson JE, et al. Bodymass
index: an independent predictor of cataract. Arch
Ophthalmol 1995;113:1131–7.
[64] Weintraub JM,Willett WC, Rosner B, et al. A pro-
spective study of the relationship between body
mass index and cataract extraction among US
women and men. Int J Obes Relat Metab Disord
2002;26:1588–95.
[65] Hiller R, Podgor MJ, Sperduto RD, et al. A longi-
tudinal study of bodymass index and lens opacities.
The Framingham Studies. Ophthalmology 1998;
105:1244–50.
[66] Ojofeitimi EO, Adelekan DA, Adeoye A, et al. Di-
etary and lifestyle patterns in the aetiology of cata-
racts in Nigerian patients. Nutr Health 1999;13:
61–8.
[67] Caulfield LE, West SK, Barron Y, et al. Anthro-
pometric status and cataract: the Salisbury Eye
Evaluation Project. Am J Clin Nutr 1999;69:
237–42.
[68] Zang EA, Wynder EL. The association between
body mass index and the relative frequencies of dis-
eases in a sample of hospitalized patients. Nutr
Cancer 1994;21:247–61.
[69] Kuang TM, Tsai SY, Hsu WM, et al. Body mass
index and age-related cataract: the Shihpai Eye
Study. Arch Ophthalmol 2005;123:1109–14.
[70] Hiller R, Sperduto RD, Reed GF, et al. Serum
lipids and age-related lens opacities: a longitudinal
investigation: the Framingham Studies. Ophthal-
mology 2003;110:578–83.
[71] Jahn CE, Janke M, Winowski H, et al. Identifi-
cation of metabolic risk factors for posterior
subcapsular cataract. Ophthalmic Res 1986;18:
112–6.
[72] Lu M, Taylor A, Chylack LT Jr, et al. Dietary fat
intake and early age-related lens opacities. Am J
Clin Nutr 2005;81:773–9.
[73] Iwig M, Glaesser D, Fass U, et al. Fatty acid cyto-
toxicity to human lens epithelial cells. Exp Eye Res
2004;79:689–704.
[74] Lu M, Cho E, Taylor A, et al. Prospective study of
dietary fat and risk of cataract extraction among
US women. Am J Epidemiol 2005;161:948–59.

424 ABRAHAM et al
[75] Tsutsumi K, Inoue Y, Yoshida C. Acceleration of
development of diabetic cataract by hyperlipidemia
and low high-density lipoprotein in rats. Biol
Pharm Bull 1999;22:37–41.
[76] Black RL, Oglesby RB, Sallman L, et al. Posterior
subcapsular cataracts induced by corticosteroids in
patients with rheumatoid arthritis. JAMA 1960;
174:166–71.
[77] Carnahan MC, Goldstein DA. Ocular complica-
tions of topical, peri-ocular, and systemic cortico-
steroids. Curr Opin Ophthalmol 2000;11:478–83.
[78] Hanania NA, Chapman KR, Kesten S. Adverse ef-
fects of inhaled corticosteroids. Am JMed 1995;98:
196–208.
[79] Dluhy RG. Effect of inhaled beclomethasone
dipropionate and budesonide on adrenal function,
skin changes and cataract formation. Respir Med
1998;92(Suppl B):15–23.
[80] Urban RC, Cotlier E. Corticosteroid-induced cata-
racts. Surv Ophthalmol 1986;31:102–10.
[81] Allen DB, Bielory L, Derendorf H, et al. Inhaled
corticosteroids: past lessons and future issues. J Al-
lergy Clin Immunol 2003;112(3 Suppl):S1–S40.
[82] Oglesby RB, Black RL, von Sallmann L, et al. Cat-
aracts in patients with rheumatic diseases treated
with corticosteroids. Arch Ophthalmol 1961;66:
41–6.
[83] Sevel D, Weinberg EG, Van Nierkerk CH. Lentic-
ular complications of long-term steroid therapy in
children with asthma and eczema. J Allergy Clin
Immunol 1977;60:215–7.
[84] Bihari M, Grossman BJ. Posterior subcapsular cat-
aracts related to long-term corticosteroid treatment
in children. Am J Dis Child 1968;116:604–8.
[85] Braver DA, Richards RD, Good TA. Posterior
subcapsular cataracts in corticosteroid-treated chil-
dren. J Pediatr 1966;69:735–8.
[86] Havre DC. Cataracts in children on long-term cor-
ticosteroid therapy. Arch Ophthalmol 1965;73:
818–21.
[87] Mino M, Ueda Y, Hayashi M, et al. Posterior sub-
capsular cataract in children on longterm corticoid
therapy. Acta Paediatr Jpn 1969;11:1–5.
[88] Tarantino A, Aroldi A, Stucchi L, et al. A ran-
domized prospective trial comparing cyclospor-
ine monotherapy with triple-drug therapy in
renal transplantation. Transplantation 1991;52:
53–7.
[89] Maiorca R, Cristinelli L, Setti G, et al. Prospective
controlled trial of steroid withdrawal after six
months in renal transplant patients treated with cy-
closporine. Transplant Proc 1988;20(Suppl 3):
121–5.
[90] Toogood JH, Markov AE, Baskervilee J, et al. As-
sociation of ocular cataracts with inhaled and oral
steroid therapy during long-term treatment of
asthma. J Allergy Clin Immunol 1993;91:571–9.
[91] Simons FER, PersaudMP, Gillespie CA, et al. Ab-
sence of posterior subcapsular cataracts in young
patients treated with inhaled glucocorticoids. Lan-
cet 1993;342:776–8.
[92] Agertoft L, Larsen FE, Pedersen S. Posterior sub-
capsular cataracts, bruises and hoarseness in chil-
dren with asthma receiving long-term treatment
with inhaled budesonide. Eur Respir J 1998;12:
130–5.
[93] Jick SS, Vasilakis-Scaramozza C, Maier WC. The
risk of cataract among users of inhaled steroids.
Epidemiology 2001;12:229–34.
[94] Smeeth L, Boulis M, Hubbard R, et al. A popula-
tion based case-control study of cataract and in-
haled corticosteroids. Br J Ophthalmol 2003;87:
1247–51.
[95] Cumming RG, Mitchell P, Leeder SR. Use of
inhaled corticosteroids and the risk of cataracts.
N Engl J Med 1997;337:8–14.
[96] Garbe E, Suissa S, LeLorier J. Association of in-
haled corticosteroid use with cataract extraction
in elderly patients. JAMA 1998;280:539–43.
[97] Cumming RG, Mitchell P. Inhaled corticosteroids
and cataract: prevalence, prevention and manage-
ment. Drug Saf 1999;20:77–84.
[98] Shun-Shin GA, BrownNP, Bron A, et al. Dynamic
nature of posterior subcapsular cataract. Br J Oph-
thalmol 1989;73:522–7.
[99] Chylack LT. Cataracts and inhaled corticosteroids.
N Engl J Med 1997;337:46–8.
[100] Cheng CY, Liu JH, Chen SJ, et al. Population-
based study on prevalence and risk factors of age-
related cataracts in Peitou, Taiwan. Zhonghua Yi
Xue Za Zhi (Taipei) 2000;63:641–8.
[101] Leske MC, Wu SY, Nemesure B, et al. Incidence
and progression of lens opacities in the Barba-
dos Eye Studies. Ophthalmology 2000;107:
1267–73.
[102] Mitchell P, Cumming RG, Attebo K, et al. Preva-
lence of cataract in Australia: the Blue Mountains
Eye Study. Ophthalmology 1997;104:581–8.
[103] Klein BE, Klein R, Linton KL. Prevalence of
age-related lens opacities in a population. The
Beaver Dam Eye Study. Ophthalmology 1992;99:
546–52.
[104] Sperduto RD, Hiller R. The prevalence of nuclear,
cortical, and posterior subcapsular lens opacities in
a general population sample. Ophthalmology 1984;
91:815–8.
[105] Younan C, Mitchell P, Cumming RG, et al. Hor-
mone replacement therapy, reproductive factors,
and the incidence of cataract and cataract surgery:
the Blue Mountains Eye Study. Am J Epidemiol
2002;155:997–1006.
[106] Familial aggregation of lens opacities: the Fra-
mingham Eye Study and the Framingham Off-
spring Eye Study. Am J Epidemiol 1994;140:
555–64.
[107] Heiba IM, Elston RC, Klein BE, et al. Evidence for
a major gene for cortical cataract. Invest Ophthal-
mol Vis Sci 1995;36:227–35.

425NEW EPIDEMIOLOGY OF CATARACT
[108] Heiba IM, Elston RC, Klein BE, et al. Genetic
etiology of nuclear cataract: evidence for a major
gene. Am J Med Genet 1993;47:1208–14.
[109] Hammond CJ, Snieder H, Spector TD, et al. Ge-
netic and environmental factors in age-related
nuclear cataracts in monozygotic and dizygotic
twins. N Engl J Med 2000;342:1786–90.
[110] Hammond CJ, Duncan D, Sneider H, et al. The
heritability of age-related cortical cataract: the
Twin Eye Study. Invest Ophthalmol Vis Sci 2001;
42:601–5.
[111] Congdon N, Broman KW, Lai H, et al. Nuclear
cataract shows significant familial aggregation in
an older population after adjustment for possible
shared environmental factors. Invest Ophthalmol
Vis Sci 2004;45:2182–6.
[112] Congdon N, Broman KW, Lai H, et al. Cortical,
but not posterior subcapsular, cataract shows sig-
nificant familial aggregation in an older population
after adjustment for possible shared environmental
factors. Ophthalmology 2005;112:73–7.
[113] Sekine Y, Hommura S, Harada S. Frequency of
glutathione-S-transferase 1 gene deletion and its
possible correlation with cataract formation. Exp
Eye Res 1995;60:159–63.
[114] Alberti G, Oguni M, Podgor M, et al. Glutathione
S-transferase M1 genotype and age-related
cataracts: lack of association in an Italian popula-
tion. Invest Ophthalmol Vis Sci 1996;37:1167–73.
[115] Hao Y, He S, Gu Z, et al. Relationship between
GSTM1 genotype and susceptibility to senile cata-
ract. Zhonghua Yan Ke Za Zhi 1999;35:104–6.
[116] Juronen E, Tasa G, Veromann S, et al. Polymor-
phic glutathione S-transferases as genetic risk
factors for senile cortical cataract in Estonians. In-
vest Ophthalmol Vis Sci 2000;41:2262–7.
[117] Okano Y, Asada M, Fujimoto A, et al. A genetic
factor for age-related cataract: identification and
characterization of a novel galactokinase variant,
‘‘Osaka,’’ in Asians. Am J Hum Genet 2001;68:
1036–42.
[118] Maraini G,Hejtmancik JF, Shiels A, et al. Galacto-
kinase gene mutations and age-related cataract.
lack of association in an Italian population. Mol
Vis 2003;9:397–400.
[119] Iyengar SK, Klein BE, Klein R, et al. Identification
of a major locus for age-related cortical cataract
on chromosome 6p12–Q12 in the Beaver Dam
Eye Study. Proc Natl Acad Sci U S A 2004;101:
14485–90.
[120] Klein BE, Klein R, Lee KE, et al. Markers of in-
flammation, vascular endothelial dysfunction, and
age-related cataract. Am J Ophthalmol 2006;
141(1):116–22.
Ophthalmol Clin N Am 19 (2006) 427–434
Perioperative and Operative Considerationsin Diabetics
David R. Fintak, MDa, Allen C. Ho, MDb,c,*aDepartment of Ophthalmology, Wills Eye Hospital, 840 Walnut Street, Philadelphia, PA 19107, USA
bDepartment of Ophthalmology, Thomas Jefferson University, 111 South 11th Street, Philadelphia, PA 19107, USAcRetina Service, Wills Eye Hospital, 840 Walnut Street, Philadelphia, PA 19107, USA
Diabetes mellitus has become one of the fastestgrowing health epidemics in the world. According
to data analyzed from the 2002 National HealthInterview Survey, it is estimated that 18.2 millionAmericans are afflicted with this disease, with over
1.3 million new cases diagnosed each year inpeople over the age of 20. Of those with thedisease, approximately 5.2 million are undiag-
nosed or underdiagnosed [1]. With the aging ofthe United States population, the number of olderpersons with diabetes is likely to increase, with anestimated number of diagnosed persons to reach
29 million by 2050 [2].Cataracts are an important cause of visual
impairment in diabetics. Poor diabetic control
increases the incidence of cataract and the rateof cataract progression. Age-adjusted prevalencefor cataracts among those with and without
diabetes is 31.8% and 21.2%, respectively [3].Consequently, the incidence of cataract surgeryin diabetics is higher; two to five times higherthan a comparable nondiabetic population [4].
Among persons with diabetes, the prevalence ofcataracts was higher among women than men(37.3% versus 26.7%); higher among persons
aged R65 years than persons aged 50 to 64(50.3% versus 16.1%); and higher among non-Hispanic whites than those of other racial or
ethnic populations (34.8% versus 24.1%) [3].The presence of baseline proteinuria was also
* Corresponding author. Retinovitreous Associates,
910 East Willow Grove Avenue, Wyndmoor, PA 19038.
E-mail address: [email protected] (A.C. Ho).
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All ri
doi:10.1016/j.ohc.2006.07.003
found to be a significant risk factor associatedwith cataract development [4,5].
Preoperative
The preoperative evaluation should includea detailed ophthalmic and medical history.Duration and type of diabetes mellitus; glycemic
control including hemoglobin A1c levels; visualfunction of the fellow eye; history of neovascularglaucoma, retinal surgery or laser, clinically signif-
icant macular edema (CSME), or proliferativediabetic retinopathy; and outcome of cataract sur-gery in the fellow eye (if applicable) should bepaid particular attention. Other risk factors for
the progression of diabetic retinopathy shouldalso be documented: cholesterol levels; bloodpressure; and the presence or absence of coronary
heart disease, renal disease, or neuropathy.As with any cataract evaluation, a comprehen-
sive eye examination should be performed. In
diabetics, specific aspects of the examination mustbe given special consideration. Potential visualoutcome using the potential acuity meter or laser
interferometry, evaluation of corneal endothelialintegrity, and pupil size are important. Presence orabsence of iris neovascularization should be docu-mented andassessment of the angle structures using
gonioscopy should be considered. A dilated fundu-scopic examination determining the degree ofretinopathy and presence or absence of macular
edema is crucial in determining potential visualoutcome, intraoperative and postoperative compli-cations, and potential deferment of cataract extrac-
tion for retinal surgery or laser.
ghts reserved.
ophthalmology.theclinics.com

428 FINTAK & HO
It is important to differentiate causal visualloss between cataract change and diabeticretinopathy or maculopathy. The type and degree
of cataract should be determined, and correlationwith visual loss calculated. It should be noted thatolder patients who are more likely to havecataracts are also more likely to have retinopathy
or macular edema. This is important in formingexpectation levels and surgical considerations. Insome cases the distinction may be difficult to
make, secondary to poor retinal visualization. Itthen may become necessary to perform cataractsurgery, not only to improve vision but also to
allow for assessment and treatment of diabeticretinopathy.
There has been a recent shift in attitude towardthe timing of cataract surgery in diabetics. Pre-
viously, surgeons deferred cataract extractionuntil the vision deteriorated to 20/100 to 20/200because of the perceived threat of rapidly pro-
gressive postoperative diabetic retinopathy andmaculopathy [6]. When earlier studies reportedonly 9% of diabetic patients achieving postopera-
tive visual acuity better than 20/40 afterextracapsular cataract extraction, a number ofsurgeons advocated deferring surgery indefinitely
[7]. There is growing evidence, however, in sup-port of a more interventional approach. Withmacular edema identified as a major risk factorfor poor postoperative visual acuity, earlier surgi-
cal intervention allows for adequate retinal visual-ization, and identification and treatment ofCSME before lens opacification. This refinement
of approach has helped to optimize postoperativeoutcomes in modern cataract surgery.
Patients known to have proliferative diabetic
retinopathy with high-risk characteristics orCSME should be considered for laser treatmentbefore cataract surgery. Patients not meeting theDiabetic Retinopathy Study’s criteria for laser
panretinal photocoagulation, such as those withproliferative diabetic retinopathy without high-risk characteristics but with significant nonperfu-
sion, or those with nonproliferative diabeticretinopathy with significant nonperfusion andhigh-risk systemic factors, should also be
considered for laser treatment because of theirrisk for progression of retinopathy followingcataract extraction. Although regression is often
difficult to assess after completion of laser treat-ment, an interval of 3 months is typically usedbefore initiating surgery.
For early or suspected macular edema and
CSME, fluorescein angiography should be used to
determine treatable lesions (Fig. 1). Focal lasersurgery or intravitreal steroids should be used
where appropriate. Treated lesions should be re-evaluated in 3 to 4 months, and cataract surgeryreconsidered once macular edema has resolved
or improved (Fig. 2).Promoting appropriate expectation levels and
discussing any specific risks and complications isessential in maximizing patient satisfaction.
Diabetic patients may be at increased risk fora number of complications including intraoper-ative and postoperative corneal edema,
postoperative inflammation, increased intraocularpressure, intraoperative and postoperativehyphema from iris neovascularization and vessel
fragility, posterior capsular opacification (PCO),vitreous hemorrhage from pre-existing neovascu-larization, progression of retinopathy, macularedema, epiretinal membrane formation, and
endophthalmitis.The use and type of preoperative medications
for diabetics undergoing cataract extraction is
highly variable. Although no study hasdemonstrated its effectiveness, most surgeons usepreoperative antibiotics as prophylaxis against
endophthalmitis. The benefits of this practiceremain controversial. Rationales for using theminclude reducing or eliminating the bacterial load
Fig. 1. Optical coherence tomography demonstrating
clinically significant macular edema.
Fig. 2. Optical coherence tomography demonstrating
resolution of macular edema following focal grid laser.

429CONSIDERATIONS IN DIABETICS
on the ocular surface, and aqueous penetration toeradicate bacteria introduced at the time ofsurgery. In this regard, an ideal antibiotic wouldhave a broad spectrum of bactericidal activity,
sufficient solubility to reach therapeuticconcentrations, and negligible side effects ortoxicity. The fluoroquinolones, namely the
fourth-generation moxifloxacin and gatifloxacin,fulfill these conditions and are the most com-monly prescribed prophylactic antibiotics.
The routine use of nonsteroidal anti-inflamma-tory drugs before surgery is recommended bymanysurgeons. Multiple studies have demonstrated the
anti-inflammatory effect of these drugs, andwith analready compromised blood aqueous barrier andincreased risk for postoperative inflammation,nonsteroidal anti-inflammatory drugs have proved
to decrease the risk of CME. Additionally, thesedrugs help to prolong the mydriatic effect ofperioperative dilating drops.
Perioperative and operative
As with any surgery, patients must beinstructed to take nothing by mouth for at least
6 hours before surgery. It is generally recommen-ded that insulin-dependent diabetics take onlyhalf of their NPH insulin and no regular insulin
on the day of surgery. Oral hypoglycemic agentsalso should be held. Optimally, schedulingdiabetic patients for surgery early in the morningfacilitates maintenance of ideal glucose levels. If
the ophthalmologist and anesthesiologist areconcerned with preoperative and postoperativeglucose control, the advice of an internist or
endocrinologist should be sought [8].Pupillary dilation and maintenance in diabetic
patients can be challenging at times. Patients with
long-standing diabetes may dilate poorly second-ary to an ischemic and spastic pupil. In addition,neovascular iris changes may promote fibrotic
ring development at the pupil margin. To maxi-mize preoperative dilation, the use of tropicamide1%, phenylephrine 2.5% to 10%, cyclopentolate0.5% to 1%, and flurbiprofen 0.03% or ketorolac
tromethamine 0.5% every 10 minutes for threedoses should be used, starting 1 hour beforesurgery.
Patients with diabetes mellitus may alreadyhave compromised corneas, so care must be takenin deciding wound construction. Affected corneas
may not tolerate a clear cornea incision, leading todelayed wound healing, corneal edema, woundleak, and an increased risk of endophthalmitis. In
these cases a scleral tunnel-limbal approach maybe considered, especially in patients who mayrequire immediate postoperative panretinalphotocoagulation that necessitates a clear corneal
view.Visualization is critical for successful cataract
surgery, requiring adequate pupil dilation to de-
crease the chance of complications. Liberal useof high-molecular-weight viscoelastics (Healon,Healon GV, PROVISC, Coease, or Amvisc Plus)
and mechanical dilation should be used. Pupillarystretching using two instruments is a popularand effective technique. Other methods include
pupillary stretching with the Beehler pupil dilator,and insertion of iris retractor hooks or pupillaryrings. In rare cases, radial iridotomy may benecessary for adequate visualization. Generally,
a pupil size greater than 6 mm is desired. Avoidexcessive manipulation of the pupil becausethis may lead to hyphema and postoperative
inflammation.A large continuous curvilinear capsulorrhexis
is preferable for these cases, to accommodate
a large optic intraocular lens (IOL). With anincreased incidence of anterior capsular contrac-tion in diabetics [9,10], a larger capsulorrhexis and
IOL optic allows for improved postoperativeretinal visualization and facilitates peripheral laseradministration; this is very important for futuremonitoring and treatment.
Hydrodissection should be performed carefully,especially in patients with previous vitreoretinalsurgery. Lack of an intact anterior vitreous to
cushion the posterior capsule increases the risk ofzonular stretching and breaking. In addition, anypatient who has undergone a vitrectomy may
already have weak zonules and a possible posteriorcapsular break. For this reason, it is important toavoid overfilling the anterior chamber with visco-elastic. Posterior capsular ‘‘trampolining’’ is more
common with absent vitreous, so care must betaken when near the capsule.
Phacoemulsification techniques that minimize
phaco time are preferable to minimize energytransmitted to the endothelium and subsequentcorneal edema. Phacoemulsification at the papil-
lary plane or ‘‘in the bag’’ also helps to limitdamage to the corneal endothelium. Thoroughcortical cleanup, including careful polishing of
the posterior capsule and anterior rim, should beperformed after phacoemulsification because ofthe higher incidence of PCO in diabetics [11]. AKu-glen hook or similar instrument may be used to
retract the pupil and inspect the capsule for

430 FINTAK & HO
residual cortical material. Meticulous cleanup mayhelp to decrease the severity and delay presentationof PCO and anterior capsular opacification.
The material type and size of IOL used forimplantation should be considered carefully. Alarge optic IOL should be used to minimize anycontraction of the anterior capsule. In general,
a 6-mm or greater optic is preferable. Whenchoosing the type of IOL material, silicone isgenerally avoided for multiple reasons. These
implants are not a good choice if the patient hassilicone oil in the posterior chamber or is likely torequire silicone oil in the future, secondary to
irreversible silicone oil adhesion to the siliconeIOL. Those patients possibly needing to undergoa fluid-air exchange in the future are also poorcandidates because of an increased risk of
condensation on the silicone lens. Furthermore,studies have shown that silicone IOLs maystimulate inflammation in diabetic eyes.
To reduce postsurgical inflammation, foldableacrylic IOLs and lenses made from heparin-coatedpolymethyl methacrylate are now being used by
many surgeons. Although studies have showna reduction in lens-induced postoperative inflam-mation with the heparin-coated polymethyl meth-
acrylate lenses [12], the possibility of increasedinflammation caused by the larger surgical woundnecessary to insert this rigid IOL must be consid-ered. A study by Krepler and coworkers [13]
found no statistical difference in the amount ofpostoperative inflammation between diabeticpatients receiving a heparin-coated polymethyl
methacrylate lens through a 6-mm sclerocornealincision compared with those inserted with a fold-able acrylic lens through a 4-mm sclerocorneal
incision. Gatinel and coworkers [14] also foundno statistical difference when comparing inflam-mation with either an acrylic or heparin-coatedpolymethyl methacrylate lens through an
identically sized sclerocorneal incision in patientswith diabetes.
Although modern small-incision cataract
surgery with phacoemulsification has become theprocedure of choice for most cases, extracapsularcataract extraction should be considered in special
situations. Dense nuclear sclerotic changes, pseu-doexfoliation, inadequate pupillary dilationimpeding adequate visualization, and notation of
excessive lens mobility on hydrodissection may allbe indications for conversion to extracapsularcataract extraction. This is advisable to preventpossible capsular disruption and loss of nucleus or
lens fragments into the vitreous.
Cataract surgery in those patients withprevious vitrectomy and existing intraocularsilicone oil should be approached differently. In
these patients, cataract formation has been accel-erated and is generally quite soft because of theshort period in which they develop. If possible, oilremoval before cataract extraction is preferable.
If unable, however, care must be taken not tooverfill the anterior chamber with viscoelastic,because this can push silicone oil through the
zonules and into the anterior chamber. For thesame reason, low-flow and lowered infusionpressure should be used during lens removal.
The use of a silicone IOL in these cases isabsolutely contraindicated, secondary to irrevers-ible silicone oil adhesion to the silicone IOL andvisual obscuration for the patient and retinal
surgeon. Final viscoelastic removal should includemeticulous removal of any silicone oil that hasentered the anterior chamber. Although common
to find some residual silicone oil droplets in theanterior chamber on the first postoperative day,a large layer of silicone oil (O10% of anterior
chamber volume) should be considered forremoval.
In select cases, cataract extraction with IOL
placement may be combined with concomitantpars plana vitrectomy. Indications for combinedsurgery include proliferative diabetic retinopathy,diabetic tractional retinal detachment, vitreous
hemorrhage, proliferative vitreoretinopathy, andothers. Although once thought to have an in-creased risk of complications, the combined pro-
cedure has been shown to be a safe and effectivealternative to sequential surgery [15,16]. Advan-tages include a shorter postoperative recovery
time with faster visual improvement, optimal visu-alization of the posterior pole during vitrectomy,avoidance of anesthesia risk from a secondsurgery, and significant cost savings. Postopera-
tive visual outcomes between combined surgeryand sequential surgery patients were notsignificantly different as shown in multiple studies
[15,16]. The combined procedure has been associ-ated, however, with a slightly higher risk of post-operative neovascular glaucoma [15,17–19].
Postoperative
Studies of cataract surgery in diabetics confirmpreoperative retinopathy severity and macular
edema as the principal determinants of postoper-ative visual acuity. The Early Treatment DiabeticRetinopathy Study Report Number 25 (ETDRS

431CONSIDERATIONS IN DIABETICS
#25) also found poor preoperative visual acuity tobe a statistically significant risk factor for pooroutcome. Other systemic risk factors, such as age,sex, race, body mass index, type of diabetes,
duration of diabetes, blood pressure, serum cho-lesterol levels, urine proteinuria, and glycosylatedhemoglobin concentration, were not associated
with poor visual outcomes [5].Severity of retinopathy at the time of lens
removal is the most important predictor of poor
visual acuity outcome [5,20,21]. More severeretinopathy may be associated with an increasedprevalence of macular ischemia, or a reduced
tendency to spontaneous resolution of macularedema [22]. It should be noted, however, that inthe ETDRS #25 study most patients with moresevere retinopathy improved by at least two lines
of vision (55%), with 25% achieving a finalvisual acuity of 20/40 or better and 42% achiev-ing 20/100 or better [5].
Although many studies have been published onthe influence of cataract surgery on diabeticretinopathy, considerable controversy exists over
whether cataract extraction accelerates retinopa-thy progression. Earlier studies reporting onretinopathy changes following intracapsular cata-
ract extraction and extracapsular cataract extrac-tion found that patients undergoing surgery didexhibit disease progression [23–27]. With the ad-vent of phacoemulsification, some articles report
a similar progression of diabetic retinopathy[5,21,28–32], whereas others report no significantprogression postoperatively [33–36]. Most note-
worthy of these is the ETDRS #25, which founda borderline statistically significant risk of acceler-ated retinopathy progression in operated eyes
compared with fellow unoperated eyes. Greaterweight can be applied to this study because ofits superior methodology in grading retinopathy,and its use of the fellow unoperated eye as a con-
trol [5]. In contrast, Wagner and coworkers [33]and Kato and coworkers [36] have found thatworsening of diabetic retinopathy reflects the nat-
ural course of the disease, systemic factors, orboth rather than the influence of the cataract sur-gery. Regardless, early and frequent postoperative
evaluation of the level of retinopathy is importantto determine the need for panretinal photocoagu-lation. In general, dilated funduscopy is recom-
mended at 1 week, 3 to 4 weeks, 6 weeks, and3 months following cataract extraction.
Multiple studies have also tried to elucidatespecific patient demographic and surgical factors
that may have influence on the risk of retinopathy
progression. Poor blood sugar control, male sex[37], and limited surgical experience (ie, longersurgery duration) [30] were all found to accelerateretinopathy in diabetic patients. Longer surgery
duration is associated with increased postopera-tive inflammation [38], and this may result in anincreased breakdown of the blood-retinal barrier
and play a role in the progression of retinopathy.If this mechanism proves to be critical in thedevelopment of progression, then aggressive
preoperative and postoperative therapy withanti-inflammatory medications and attempts toshorten the surgical time should prove to be
beneficial.The ETDRS #25 study found no statistically
significant difference in the proportions of eyeswith clinically significant macular edema before or
after lens surgery, and that CSME found aftersurgery was not markedly different between eyesthat underwent surgery and those that did not [5].
Similar findings were reported in another concur-rent study [22]. At first, these findings seem tocontradict earlier studies reporting a significant
prevalence of macular edema after surgery[21,23], but on further investigation are entirelyconsistent with natural history studies. Although
these studies report a 56% incidence of new clini-cally detectable macular edema in the first yearafter surgery, spontaneous resolution occurredwithout treatment in 50% of affected eyes by 6
months and in 75% by 1 year after surgery [22].Patients with CSME at the time of surgerybehaved quite differently, however, with none
resolving spontaneously by 1 year, and mostshowing clinical and angiographic deterioration.With this in mind, it may be possible that previous
case reports of severe macular edema after cata-ract surgery were described in patients who hadunrecognized or untreated edema before lensextraction. This also reinforces the need for
aggressive treatment of CSME before surgery.
The incidence of PCO is slightly higher indiabetics than in nondiabetics [11]. Additional risk
factors include young age [39] and pseudoexfolia-tion syndrome [40]. A recent study published byHayashi [11] found no significant difference in
the incidence of PCO for the first 12 months,but that at 18 months and later, the PCO valuein the diabetic group increased significantly and
was significantly greater than in the control group.In addition, no significant correlation was foundbetween degree of PCO and stage of retinopathy,type of diabetic treatment, duration of diabetes,
and hemoglobin A1c level.

432 FINTAK & HO
An yttrium-aluminum-garnet laser capsulot-omy may become necessary in cases of significantPCO to improve vision or improve visualization
of the retina. In these cases, a large capsulotomy ispreferable. Generally, the capsulotomy should bedelayed until absolutely necessary because of theincreased risk of macular edema in diabetics.
Multiple studies have also demonstrated theincreased incidence of anterior capsular contractionin diabetics, possibly related to the greater degree
of postoperative inflammation these patientsexhibit [9,10]. Confounding risk factors includepseudoexfoliation syndrome [41], pigmentary reti-
nal degeneration [42–44], uveitis [41,42], and oldage [45]. No correlation was found between the de-gree of PCO and anterior capsular contraction [9].
The development of anterior capsular rim
opacification can be unfavorable because propervisualization of the entire retina is important forboth monitoring and treatment in the postopera-
tive period. Kato and coworkers [10] found thatdiabetic patients had a statistically significantlysmaller anterior capsular opening at 3, 6, and 12
months when compared with nondiabetic controls.This stresses the need for a large capsulorrhexisin conjunction with a large optic IOL.
Ocular inflammation is a common cause ofreduced vision after cataract surgery. Factorscontributing to the degree of inflammationinclude duration of surgery, wound size, posterior
capsule rupture, and vitreous loss. In diabetics,the increased risk of postoperative inflammationarises from a compromised blood-aqueous bar-
rier. This risk is apparent in all diabetics, regard-less of the presence of diabetic retinopathy. Theprolonged use of topical steroids and nonsteroidal
anti-inflammatory drugs can help prevent seriouscomplications related to this issue.
Postoperative endophthalmitis is one of themost serious and potentially devastating compli-
cations after cataract surgery. Although mostcases are still infectious (69%), diabetics have anincreased tendency to develop sterile endophthal-
mitis. The Endophthalmitis Vitrectomy Studyfound that diabetics tend to have more virulentorganisms, a higher percentage of gram-negative
isolates, and are less likely to be culture-negative[46]. Risk factors include inadequate disinfectionof the eyelid and conjunctiva, surgery longer
than 60 minutes, vitreous loss, use of prolene hap-tics, wound leak or dehiscence, and inadequatelyburied sutures [47]. The mainstay of treatmentfor patients with hand motion vision or better still
includes vitreous tap and injection of antibiotics.Vancomycin, 1 mg/0.1 mL, and ceftazidime, 2.25mg/0.1 mL, or amikacin, 0.4 mg/0.1 mL, were
found by the Endophthalmitis Vitrectomy StudyGroup to cover 100% of gram-positive organismsand 97% to 100% of gram-negative organisms[48,49]. If no clinical improvement is noted in
the first 48 to 72 hours, or if the presenting visionis light perception only, a vitrectomy should beconsidered. In all cases, concomitant use of corti-
costeroids, either topically, intravitreally, or sys-temically, has been shown to reduce intraocularinflammation and secondary complications asso-
ciated with infectious endophthalmitis [50,51],but also has been shown to have no effect on vi-sual outcome [52]. Unfortunately, diabetics tendto have worse vision after treatment of endoph-
thalmitis, with only 56% of patients achieving20/100 versus 77% of nondiabetics [53].
Summary
Diabetes mellitus is one of the fastest growing
health epidemics in the world, and with a highpercentage of these patients developing visuallysignificant cataracts, the number of cataract
surgeries for diabetics is only expected to increase.Surgical outcomes have improved in recent yearswith the advent of early intervention, and im-
proved preoperative diagnosis and treatment ofretinopathy and macular edema. Although thesepatients present unique challenges to the cataract
surgeon, appropriate preoperative and intraoper-ative considerations lend to good outcomes.
References
[1] National Diabetes Information Clearinghouse.
National diabetes statistics. Available at: http://
diabetes.niddk.nih.gov/dm/pubs/statistics. Accessed
September 24, 2005.
[2] Boyle JP, Honeycutt AA, Narayan KM, et al. Pro-
jection of diabetes burden through 2050: impact of
changing demography and disease prevalence in
the US. Diabetes Care 2001;24:1936–40.
[3] Centers for Disease Control and Prevention. Preva-
lence of visual impairment and selected eye diseases
among persons agedR 50 years with and without di-
abetesdUnited States, 2002. CDCMMWRWeekly
2004;53:1069–71.
[4] Klein BE, Klein R, Moss SE. Incidence of cataract
surgery in the Wisconsin epidemiologic study of dia-
betic study of diabetic retinopathy. Am J Ophthal-
mol 1995;119:295–300.

433CONSIDERATIONS IN DIABETICS
[5] Chew EY, Benson WE, Remaley NA, et al. Results
after lens extraction in patients with diabetic
retinopathy: Early Treatment Diabetic Retinopathy
Study Report Number 25. Arch Ophthalmol 1999;
117:1600–6.
[6] Pollack A, Leiba H, Bukelman A, et al. Cystoid
macular edema following cataract extraction in
patients with diabetes. Br J Ophthalmol 1992;76:
221–4.
[7] Schatz H, Atienza D, McDonald HR, et al. Severe
diabetic retinopathy after cataract surgery. Am J
Ophthalmol 1994;117:314–21.
[8] Sinskey RM, Patel JV. Manual of cataract sur-
gery. 1st edition. Boston: Butterworth-Heinemann;
1997.
[9] Hayashi Y, Kato S, Fukushima H, et al. Relation-
ship between anterior capsule contraction and poste-
rior capsule opacification after cataract surgery in
patients with diabetes mellitus. J Cataract Refract
Surg 2004;30:1517–20.
[10] Kato S, Oshika T, Numaga J, et al. Anterior capsu-
lar contraction after cataract surgery in eyes of dia-
betic patients. Br J Ophthalmol 2001;85:21–3.
[11] Hayashi K. Posterior capsule opacification after cat-
aract surgery in patients with diabetesmellitus. Am J
Ophthalmol 2001;134:10–6.
[12] Borgioli M, Coster DJ, Fan RF, et al. Effect of hep-
arin surface modification of polymethylmethacry-
late intraocular lenses on signs of postoperative
inflammation after extracapsular cataract extrac-
tion; one-year results of a double-masked multicen-
ter study. Ophthalmology 1992;99:1248–54.
[13] Krepler K, Ries E, Derbolav A, et al. Inflammation
after phacoemulsification in diabetic retinopathy:
foldable acrylic versus heparin-surface-modified
polymethylmethacrylate intraocular lenses. J Cata-
ract Refract Surg 2001;27:233–8.
[14] Gatinel D, Lebrun T, Le Toumelin P, et al. Aqueous
flare induced by heparin surface modified poly(me-
thylmethacrylate) and acrylic lenses implanted
through the same-size incision in patients with diabe-
tes. J Cataract Refract Surg 2001;27:855–60.
[15] Chung T, Chung H, Lee JH. Combined surgery and
sequential surgery comprising phacoemulsification,
pars plana vitrectomy, and intraocular lens implan-
tation: comparison of clinical outcomes. J Cataract
Refract Surg 2002;28:2001–5.
[16] Senn P, Schipper I, Perren B. Combined pars plana
vitrectomy, phacoemulsification, and intraocular
lens implantation in the capsular bag: a comparison
to vitrectomy and subsequent cataract surgery as
a two-step procedure. Ophthalmic Surg Lasers 1995;
26:420–8.
[17] Rice TA,Michels RG,MaguireMG, et al. The effect
of lensectomy on the incidence of iris neovasculari-
zation and neovascular glaucoma after vitrectomy
for diabetic retinopathy. Am J Ophthalmol 1983;
95:1–11.
[18] Mamalis N, Teske MP, Kreisler KR, et al. Phacoe-
mulsification combined with pars plana vitrectomy.
Ophthalmic Surg 1991;22:194–8.
[19] Scharwey K, Pavlovic S, Jacobi KW. Combined
clear corneal phacoemulsification, vitreoretinal sur-
gery, and intraocular lens implantation. J Cataract
Refract Surg 1999;25:693–8.
[20] Dowler JG, Hykin PG, Lightman SL, et al. Visual
acuity following extracapsular cataract extraction
in diabetes: a meta-analysis. Eye 1995;9:313–7.
[21] Dowler JG, Hykin PG, Hamilton AM. Phacoemul-
sification versus extracapsular cataract surgery in
diabetes. Ophthalmology 2000;107:457–62.
[22] Dowler JG, Sehmi KS, Hykin PG, et al. The natural
history of macular edema after cataract surgery in
diabetes. Ophthalmology 1999;106:663–5.
[23] BensonWE, BrownGC, TasmanW, et al. Extracap-
sularcataract extractionwithplacementofaposterior
chamber lens in patients with diabetic retinopathy.
Ophthalmology 1993;100:730–8.
[24] Alpar JJ. Diabetes: cataract extraction and intra-
ocular lenses. J Cataract Refract Surg 1987;13:
43–6.
[25] Jaffe GJ, Burton TC. Progression of nonprolifera-
tive diabetic retinopathy following cataract extrac-
tion. Arch Ophthalmol 1988;106:745–9.
[26] Pollack A, Dotan S, Oliver M. Progression of dia-
betic retinopathy after cataract extraction. Br J Oph-
thalmol 1991;75:547–51.
[27] Jaffe GJ, Burton TC, Kuhn E, et al. Progression of
nonproliferative diabetic retinopathy and visual
outcome after extracapsular cataract extraction
and intraocular lens implantation. Am J Ophthal-
mol 1992;114:448–56.
[28] Henricsson M, Heijl A, Janzon L. Diabetic retinop-
athy before and after cataract surgery. Br J Ophthal-
mol 1996;80:789–93.
[29] Antcliff RJ, Poulson A, FlanaganW. Phacoemulsifi-
cation in diabetics. Eye 1996;10:737–41.
[30] Mittra RA, Borrilo JL, Dev S, et al. Retinopathy
progression and visual outcomes after phacoemulsi-
fication in patients with diabetesmellitus. ArchOph-
thalmol 2000;118:912–7.
[31] Chung J, KimMY, Kim HS, et al. Effect of cataract
surgery on the progression of diabetic retinopathy.
J Cataract Refract Surg 2002;28:626–30.
[32] Funatsu H, Yamashita H, Noma H, et al. Predic-
tion of macular edema exacerbation after phacoe-
mulsification in patients with nonproliferative
diabetic retinopathy. J Cataract Refract Surg 2002;
28:1355–63.
[33] Wagner T, Knaflic D, Rauber M, et al. Influence of
cataract surgery on the diabetic eye: a prospective
study. Ger J Ophthalmol 1996;5:79–83.
[34] Squirrell D, Bhola R, Bush J, et al. A prospective,
case controlled study of the natural history of dia-
betic retinopathy and maculopathy after uncompli-
cated phacoemulsification cataract surgery in

434 FINTAK & HO
patients with type 2 diabetes. Br J Ophthalmol 2002;
86:565–71.
[35] Krepler K, Biowski R, Schrey S, et al. Cataract
surgery in patients with diabetic retinopathy: visual
outcome, progression of diabetic retinopathy, and
incidence of diabetic macular oedema. Graefes
Arch Clin Exp Ophthalmol 2002;240:735–8.
[36] Kato S, FukadaY,Hori S, et al. Influence of phacoe-
mulsification and intraocular lens implantation on
the course of diabetic retinopathy. J Cataract Re-
fract Surg 1999;25:788–93.
[37] Hauser D, Katz H, Pokroy R, et al. Occurrence and
progression of diabetic retinopathy after phacoe-
mulsification cataract surgery. J Cataract Refract
Surg 2004;30:428–32.
[38] Fujishima H, Toda I, Yagi Y, et al. Quantitative
evaluation of postsurgical inflammation by infrared
radiation thermometer and laser flare-cell meter.
J Cataract Refract Surg 1994;20:451–4.
[39] Jamal SA, Solomon LD. Risk factors for posterior
capsular pearling after uncomplicated extracapsular
cataract extraction and plano-convex posterior
chamber lens implantation. J Cataract Refract
Surg 1993;19:333–8.
[40] Kuchle M, Amberg A, Martus P, et al. Pseudoexfo-
liation syndrome and secondary cataract. Br J Oph-
thalmol 1997;81:862–6.
[41] Davison JA. Capsule contraction syndrome. J Cata-
ract Refract Surg 1993;19:582–9.
[42] Namiki M, Yamamoto N, Tagami Y. Risk factors
for anterior capsular shrinkage in intraocular lens im-
plantation. Jpn J Clin Ophthalmol 1991;45:1828–31.
[43] Hayashi K, Hayashi H, Matsuo K, et al. Anterior
capsule contraction and intraocular lens dislocation
after implant surgery in eyes with retinitis pigmento-
sa. Ophthalmology 1998;105:1239–43.
[44] Nishi O, Nishi K. Intraocular lens encapsulation by
shrinkage of the capsulorhexis opening. J Cataract
Refract Surg 1993;19:544–5.
[45] Sakamoto Y, Sasaki K. Accuracy of biometrical
data obtained from the NIDEK EAS-1000. Oph-
thalmic Res 1994;26:26–32.
[46] Endophthalmitis Vitrectomy Study Group. Results
of the Endophthalmitis Vitrectomy Study: a ran-
domized trial of immediate vitrectomy and of intra-
venous antibiotics for the treatment of postoperative
bacterial endophthalmitis. Arch Ophthalmol 1995;
113:1479–96.
[47] Meinkoff JA, SpeakerMG,MarmorM, et al. A case
control study of risk factors for postoperative
endophthalmitis. Ophthalmology 1991;98:1761–8.
[48] Endophthalmitis Vitrectomy Study Group. Micro-
biologic factors and visual outcomes in the endoph-
thalmitis vitrectomy study. Am J Ophthalmol 1996;
122:830–46.
[49] Irvine DW, Flynn HW Jr, Miller D, et al. Endoph-
thalmitis caused by gram-negative organisms. Arch
Ophthalmol 1992;110:1450–4.
[50] Cole HP, Stallman J, Diamond J. High dose intravi-
treal dexamethasone for infectious endophthalmitis.
Invest Ophthalmol 1989;30:509.
[51] Maxwell DP Jr, Brent DB, Diamond JG, et al. Effect
of intravitreal dexamethasone on ocular histopa-
thology in a rabbit model of endophthalmitis. Arch
Ophthalmol 1991;98:1370–5.
[52] Aaberg TM Jr, Flynn HW Jr, Schiffman J, et al.
Nosocomial acute-onset postoperative endophthal-
mitis survey. Ophthalmology 1998;105:1004–10.
[53] Doft BH, Wisniewski SR, Kelsey SF, et al. Diabetes
and postoperative endophthalmitis in the endoph-
thalmitis vitrectomy study. Arch Ophthalmol 2001;
119:650–6.

Ophthalmol Clin N Am 19 (2006) 435–448
Enhancing Intraocular Lens Outcome Precision:An Evaluation of Axial Length Determinations,
Keratometry, and IOL FormulasThomas C. Prager, PhD, MPHa,*, David R. Hardten, MDb,c,
Benjamin J. Fogal, ODb
aDepartment of Ophthalmology and Visual Science, Hermann Eye Center, University of Texas Health
Science Center–Houston, 6411 Fannin Street, Houston, TX 77030, USAbMinnesota Eye Consultants, 710 East 24th Street, Suite 106, Minneapolis, MN 55404, USAcUniversity of Minnesota, 710 East 24th Street, Suite 106, Minneapolis, MN 55404, USA
With increased safety of the procedure itself,cataract surgery now is being performed in
patients who have less visual disability thanseveral years ago. Today’s cataract surgery occursat an earlier age, and with implants for monofocal
and multifocal corrections, patients now antici-pate excellent uncorrected acuity, not just im-proved best corrected vision. Because patients
have come to view cataract surgery as botha rehabilitative and refractive procedure, sur-geons, for better or for worse, now are being
judged mainly for their refractive outcomes. Thisexpectation places increased importance on accu-rate biometry and intraocular lens (IOL) calcula-tions, the topics covered in this article. Accuracy
of the measurements has a consequence in patientsatisfaction and depends on correct determinationof eye length, IOL position, refractive power of
the cornea, and selection of the proper IOLformula. Familiarity with these variables willmake it easier to achieve precise results in both
the intact eye and in eyes that have had previoussurgeries, including keratorefractive procedures.
The first section discusses considerations per-taining to IOL formulas. The other sections
Thomas C. Prager, PhD, MPH has a financial in-
terest in the Prager Shell (ESI, Plymouth, Minnesota).
* Corresponding author.
E-mail address: [email protected]
(T.C. Prager).
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All r
doi:10.1016/j.ohc.2006.07.009
address the details of measuring axial length andcorneal curvature accurately. The second section
focuses on the advantages and disadvantages ofvarious methods of measuring biometry as well astips and practical information to reduce biometry
errors. The third section addresses variousmethods of determining corneal power. Keratom-etry after refractive surgery can be difficult, and
several measurement strategies are presented.
Calculation formulas for intraocular lens
The first estimation of IOL power was made in1967 by Federov and colleagues [1]. Based on ver-
gence formulas, the basics of the original calcula-tions have not changed much. Only slightvariations in the formula have occurred with the
onset of new technological advances such as ultra-sonography. In the 1970s, several investigatorsdevised a variety of theoretical formulas to
describe the various relationships of the differentocular components [2,3]. With the advent of accu-rate ‘‘A scan’’ ultrasound, they were better able topredict the axial length of the eye and therefore
achieve reliable IOL power predictions.Slight variations in the formulas accounted for
the different values by different investigators, but
for the most part, only a few variables were usedin the formula: corneal power, axial length, de-sired postoperative refraction, effective lens posi-
tion, power of the IOL, and vertex distance. Some
ights reserved.
ophthalmology.theclinics.com

436 PRAGER et al
minor differences in the values for the cornealindex of refraction and the thickness of the retinaexisted. Effective lens position is the only variable
that cannot be measured directly preoperatively.There are two basic groups of formulas:
theoretical formulas that use geometrical opticsand empiric studies based on retrospective case
studies and statistical analysis. The Sanders-Retzlaff-Kraff (SRK) formula was one such em-piric regression formula [4]:
IOL power ¼ A constant� 2:5 AL� 0:9 K;
where AL represents axial length, andK representscorneal power as measured with keratometry inDiopters.
Today, the theoretical formulas are consideredmore reliable in predicting correct IOL power. Inthe first-generation theoretical formulas, the effec-
tive lens position was actually the anterior cham-ber depth, and it was a constant factor (4 mm)dependant on the IOL position [2,3]. The second-generation formulas related the axial length to
the effective lens position [5]. By 1988, it wasproven that accuracy could be improved furtherby using a two-variable predictor of effective lens
position [6]. The third-generation, and more reli-able, formulas vary the effective lens position asa function of the axial length and the corneal
power. Examples of these formulas are the Holla-day 1, the SRK/T, and the Hoffer Q [6–8].
Later-generation formulas include the Holla-
day 2 and Olsen formulas. These formulas calcu-late the effective lens position using more than twovariables. The Holladay 2, for example, uses sevendifferent variables to describe the effective lens
position accurately: axial length, corneal power,white-to-white corneal diameter, anterior cham-ber depth, age, lens thickness, and preoperative
refraction [9].
Measurement of parameters for calculation
IOL formulas depend on accurate measure-ments of the various components of the formulas
such as axial length, anterior chamber depth, andcorneal power. IOL prediction changes dramati-cally with keratorefractive procedures because of
errors in measurement of corneal power [10–36].The instrumentation used today in the measure-ment of corneal curvature and corneal power
make basic assumptions about the refractive prop-erties of the eye that do not hold once the anatomyis altered with surgery. These breakdowns in the
formulas for IOL calculation may cause increasedinaccuracy in the refractive error after cataractsurgery. Many patients have now undergone re-
fractive surgical correction of ametropia, andsome have developed cataractous changes requir-ing surgery.
The various theoretical and empiric formulas
rely on accurate measurement of the axial lengthas part of the calculations. As discussed, immer-sion ultrasound and partial coherence interferom-
etry (or optical coherence biometry) show a highdegree of correlation.
Although many formulas work well in many
eyes, certain formulas may be more accurate,depending on the axial length of the eye. Formu-las that may have an advantage in accuracy basedon axial length are
Axial length less than 22 mm: Hoffer Q, Holla-
day IIAxial length 22 to 26 mm:Holladay I, Hoffer Q,
SRK/TAxial length greater than 26 mm: SRK/T, Hol-
laday II
Biometry
Cataract surgery and refractive surprises
Significant cataract formation is estimated tooccur in 18% of persons aged 65 to 74 years
[37]. Consistent with this high prevalence, cataractextractions are the single most commonly reim-bursed surgery (1.3 million/year) in the Medicare
system [38,39]. With today’s multifocal lensesand patient expectations of perfection in what isoften referred to as the most successful surgeryin medicine, accuracy in preoperative measure-
ments is paramount. An early article by Holladayand colleagues [40] estimated that refractive sur-prises, defined as a 2-diopter (D) difference in
the predicted results, might occur in 5% of thecataract population. Such results can lead to a di-minished quality of life [41–43], binocular diplo-
pia, altered depth perception, possible lensexchange, or loss of patient referrals.
Axial length errors are the most likely sourceof refractive surprises and methods of measurement
The greatest source of refractive surprise seemsto be differences in measuring axial length, which
are estimated to account for 54% of postoperativerefractive error [40]. Great precision is requiredfor correct eye length measurement, and an

437ENHANCING IOL OUTCOME PRECISION
inaccuracy of only 1 mm can result in a 3-D re-fractive error.
Optical coherence biometry (OCB), such as theZeiss IOL Master (Dublin, California), has
emerged as a new modality for biometry [44]. Itsaccuracy compares closely with that of immersionultrasound biometry [45–49] One advantage is
that OCB is not subject to cross-contamination be-cause it is a noncontact procedure, but visual acu-ity must be equal to or better than 20/200 [45]. In
eyes with silicone in the posterior vitreous, theOCB technology is clearly superior to ultrasound.An advantage of the IOL Master is in its ease of
use and speed of testing. Scanning with the IOLMaster takes about 1 minute, whereas immersionultrasound takes a few minutes longer. OCB mea-sures the optical axial length, that is, the cornea–
fovea vertex distance, rather than the anatomiclength of the eye as measured by ultrasound[50,51]. This measurement is important in eyes
that are affected by a posterior pole staphyloma,such as those seen in the higher myopes, in whichthe fovea actually may lie along the slope of the
staphyloma wall [50,51]. This difference would ac-count for potentially erroneous axial measure-ments (falsely long axial length) with ultrasound.
There are disadvantages associated with OCB,which does not allow reliable measurements inthe presence of any significant axial opacity (eg,corneal scars, keratopathy, severe tear film
problems, dense posterior subcapsular cataracts,brunescent cataracts or vitreous hemorrhage, neo-vascular membranes, maculopathy, and retinaldetachment) [45,49,52,53]. OCB cannot be per-
formed when the subject has tremor, respiratorydistress, nystagmus, or lid abnormalities or cannotfixate on a target [45,50]. Consequently, the eyes of
8% to 17% of patients cannot be measured withOCB [45,50,52–54]. In addition, instrumentationmay be prohibitively expensive for a small practice.
Thus, there will always be a role for immersionbiometry in the foreseeable future.
The contact technique or direct applanation on
the eye is used commonly but is fraught withproblems. Even the skilled technician may haveparallax difficulties: in centering the probe on thecornea there is always the potential of indenting
the eye, especially in patients who have lowerintraocular pressure. The immersion techniqueeliminates these problems by using a liquid in-
terface between the eye and the ultrasound probe.Early pioneers include Ossoinig [55,56] and Hoffer[57]. Immersion may be performed with an open
cylinder (eg, the Hansen Shell, Iowa City, Iowa)filled with Goniosol or with a fixed immersionshell (eg, the Prager Shell, ESI, Inc., Plymouth,
Minnesota). The Prager Shell (Fig. 1) was first de-signed in 1982, with several improvements alsoimproving upon an immersion shell created byColeman [58]. In the authors’ opinion, the use of
Fig. 1. Prager Immersion Shell and special tubing. (Courtesy of Thomas C. Prager, PhD, Houston, TX.)

438 PRAGER et al
the fixed immersion shell, a one-handed proce-dure, is easier to master; it does not require theuse of Goniosol, which may blur the vision and
prevent additional testing that same day. The im-mersion technique minimizes technician variablessuch as corneal compression, alignment of the ul-trasound beam, and probe insertion, leading to
more reproducible results. After practice, immer-sion biometry using the Prager Shell has been re-ported to be faster than the contact method [46].
A partial explanation is that historically, withcontact biometry, after obtaining several axialmeasurements, the technician or physician must
take considerable time to review the scans and de-lete those that present corneal compression errors.
In the quest of greater accuracy in surgicaloutcome, there have been many comparisons
between applanation and immersion techniques.In 1984 Shammas [59] was the first to report thatimmersion scans consistently result in longer axial
lengths and less variability than the contact tech-nique. These findings have been replicated innumerous studies during the past 20 years
[46,59–67]. The Prager Shell and other immersionapproaches have been compared directly with thenoncontact interferometer (Zeiss IOL Master)
determination of axial length; there is no clinicaldifference in precision between the two methodol-ogies, although there is a significant difference incost [45,46,61]. A study by Packer and colleagues
[46] looked at 50 cataractous eyes and comparedthe Axis II (immersion ultrasound unit) with theIOL Master (OCB). Results showed a high corre-
lation between the two units in axial length calcu-lation (Pearson correlation coefficient ¼ 0.996). Ina cohort of 253 patients, axial length measure-
ments using the IOL Master were unobtainablein 17% of the population because of low visualacuity and dense cataracts [49].
Considerations when using the fixedimmersion shell
The balance of this section describes the properuse of the fixed immersion Prager Shell and
a commonsense approach to reduce measurementerror. Simply using an immersion shell does notguarantee perfect results on every patient. The
biometrist must understand the potential sourcesof error and a use mental checklist when perform-ing immersion biometry. An inexperienced techni-
cian who does not understand the basic principlesunderlying axial length scanning can underminethe efforts of the most skillful cataract surgeon.
Read the chart before measuring the eyeMost refractive surprises occur in eyes of
unusual length, more frequently in short eyes.
Proportionately, a 1-mm mistake in a 21-mm eyehas a greater postoperative refractive consequencethan the same 1-mm error in a 30-mm eye.Although staphylomas may make it more difficult
to locate foveal spikes in a long eye, the smallerdimensions encountered in the short eye requiregreater accuracy of measurement to maintain
error tolerance. Thus, before making an ocularmeasurement, the biometrist should determine ifthe eye is unusual in any way. A previous scleral
buckle can change shape of the eye, producinga significant difference in axial length between theeyes. In most patients both eyes are approximatelythe same length, typically within 0.3 mm of one
another. Replicate measurement findings severaltimes; if a difference of 0.3-mm or more remains,note in the chart that the ‘‘measurements exceed
normal physiologic findings.’’ Determine if eithereye is aphakic, because this condition will requirea change in sound velocity to compensate for the
missing lens. Similarly, a pseudophakic eye willrequire a change in tissue velocity. Many instru-ments have settings for eyes with implanted IOLs,
although an alternative method is to measureevery pseudophakic eye at the aphakic setting(1550 m/s) and then add 0.4 mm to the anterior-posterior length if the lens is made of polymethyl-
methacrylate, subtract 0.8 mm if the IOL lens issilicone, or add 0.2 mm for an acrylic lens.
Measuring eyes that contain silicone oil in the
posterior vitreous poses another difficulty inobtaining accurate axial length measurements.Silicone oil in the eye, used to replace vitreous in
eyes with retinal detachments, changes the speedof sound through the eye. To further complicatematters, the two most common types of siliconehave different tissue velocities, 1050 or 980 m/s,
and the clinician must know which velocity toselect to avoid a small mistake in axial length.Sandra Frazier Byrne’s [68] excellent book on ax-
ial length measurements details procedures to cor-rect for silicone in the posterior vitreous cavity.Each ocular component of the eyedanterior
chamber, lens, and posterior vitreous cavitydmust be measured individually. Each componentcan be measured at 1532 m/s. Although the ante-
rior chamber does not require a mathematical ad-justment, to obtain true values for the lens use1641/1532 times the measured lens thickness and980 (most cases)/1532 times the measured vitreous
length. Final IOL power determination is made

439ENHANCING IOL OUTCOME PRECISION
more confusing because the index of refractiondiffers in the eye with silicone and the normaleye and requires the addition of more refractivepower. Given these problems, OCB technology
will produce a more accurate axial length mea-surement than the ultrasound technique in theeye with silicone.
Search the chart for other information thatpotentially can affect the surgical outcome. Whatis the IOL power requested? If there is an
anticipated difference of 2 D or more in the finalrefraction, and the other eye does not requirecataract surgery, patients may not be able to
tolerate the anisometropia. Look at the currentglasses prescription to estimate the anticipatedaxial length. The average eye is 23.3 mm; 1 mmequals 3 D; therefore a 24-mm eye should be
myopic by roughly by 3 D. If the glasses havea hyperopic optical correction of þ3.00 D, and theaxial length measurement is 26 mm, this should
alert the biometrist to a possible mistake.
Practical tips in obtaining immersionanterior-posterior length measurements
To be in compliance with Centers for DiseaseControl and Prevention (CDC) guidelines [69], be-fore the eye is measured the shell and probe
should be soaked in alcohol or hydrogen peroxidefor at least 5 minutes. The immersion shell shouldbe allowed to dry completely and flushed withbalanced saline solution (BSS). Alcohol can com-
promise the cornea. To reduce the likelihood oftransmitting pathogens from patient to patient,it is important to change the connecting tubing
and BSS with each patient. A study conductedat 34 ophthalmology clinics showed wide variabil-ity in probe cleanliness [70]. After a single immer-
sion biometry measurement, 18 of 34 samples(53%) grew organisms from either the probe/shellor the tubing. Positive cultures were found in 32%
of the immersion shell/probes (11 of 34) and in31% of the infusion tubing samples (10 of 32).The bacterium most commonly cultured fromboth probe/shell and tubing was coagulase-nega-
tive Staphylococcus. Although Staphylococcus isassociated with conjunctival flora, its presence stillindicates poor hygiene. Fungus potentially puts
patients at risk, especially if the cornea has beencompromised. Penicillium species were the mostcommonly cultured fungi (exclusively from the
probe/shell). Overall, fungi (Penicillium and Alter-naria species) were cultured in 12% of the probe/shell samples. Only 14% of the study sites
adequately disinfected the probe/shell accordingto CDC guidelines [69].
The Prager Shell has a Luer fitting to facilitatechanging the tubing. A bottle of BSS can
be attached directly to the tubing, or BSS canbe placed in a syringe. Always replace the BSSbottle or BSS-filled syringe after every patient
(unless the tubing contains a check valve, if so,the BSS source can continue to be used). Tubing isstrictly single use. The minimal cost of new sterile
tubing and BSS for each cataract patient representsless than 3% of the Medicare reimbursement forbiometry and ensures that there is no patient cross-
contamination. In terms of cost/benefit, rather thanattempting to clean and reuse the tubing, bio-metrists can more efficiently use their time seeingother patients.
If there is a plastic sheath for applanation, pullit away from the probe. Insert the biometry probeinto the shell. The software will capture scans only
if the probe (main bang) is at the exact distancefrom the cornea specified by each ultrasoundmanufacturer. The Prager Shell has an automatic
stop feature that seats the probe at the instrumentmanufacturer’s specified distance from the cornea.This feature ensures that the ‘‘corneal gate’’ on the
biometer is positioned on the anterior cornea andnot on the posterior cornea, thus precluding theintroduction of a 0.5-mm error. Note that internalcentering guides hold the probe in place at six lo-
cations, so perpendicularity is assured. Observethat the probe tip is placed at the scored line ofthe Prager Shell. Once the probe has been posi-
tioned to the score line/auto-stop, gently tightenthe setscrew and seat against the probe. Routinetopical anesthesia is administered to the patient’s
eyes. Have the patient seated with the head tiltedslightly back against a counter or use an ordinarychair (Fig. 2).
Both patient and biometrist will benefit from
the use of a regular reclining examination chairwith a headrest. A fixation light on a flexible stemis crucial. Be sure that it is far enough from the
patient’s eyes so that the eyes are not stimulatedto converge, thus increasing the difficulty oflocating the fovea during biometry (Fig. 3). The
patient’s attention is normally drawn to a fixationlight, which is beneficial if language difficultiesmake communication difficult.
When examining a one-eyed patient, it can bedifficult to ensure proper fixation. Have thepatient extend the arm, make a fist, and thenstare at the thumb. Even in blind patients the eye
will be able to locate and follow the thumb
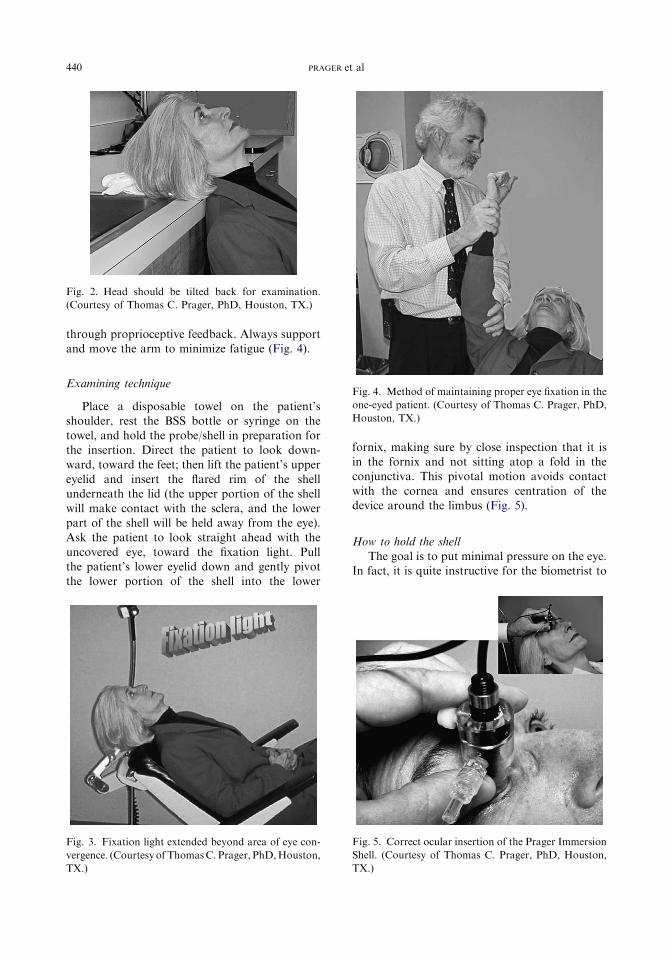
440 PRAGER et al
through proprioceptive feedback. Always supportand move the arm to minimize fatigue (Fig. 4).
Examining technique
Place a disposable towel on the patient’sshoulder, rest the BSS bottle or syringe on thetowel, and hold the probe/shell in preparation forthe insertion. Direct the patient to look down-
ward, toward the feet; then lift the patient’s uppereyelid and insert the flared rim of the shellunderneath the lid (the upper portion of the shell
will make contact with the sclera, and the lowerpart of the shell will be held away from the eye).Ask the patient to look straight ahead with the
uncovered eye, toward the fixation light. Pullthe patient’s lower eyelid down and gently pivotthe lower portion of the shell into the lower
Fig. 3. Fixation light extended beyond area of eye con-
vergence. (Courtesy of ThomasC. Prager, PhD,Houston,
TX.)
Fig. 2. Head should be tilted back for examination.
(Courtesy of Thomas C. Prager, PhD, Houston, TX.)
fornix, making sure by close inspection that it isin the fornix and not sitting atop a fold in theconjunctiva. This pivotal motion avoids contact
with the cornea and ensures centration of thedevice around the limbus (Fig. 5).
How to hold the shell
The goal is to put minimal pressure on the eye.In fact, it is quite instructive for the biometrist to
Fig. 4. Method of maintaining proper eye fixation in the
one-eyed patient. (Courtesy of Thomas C. Prager, PhD,
Houston, TX.)
Fig. 5. Correct ocular insertion of the Prager Immersion
Shell. (Courtesy of Thomas C. Prager, PhD, Houston,
TX.)
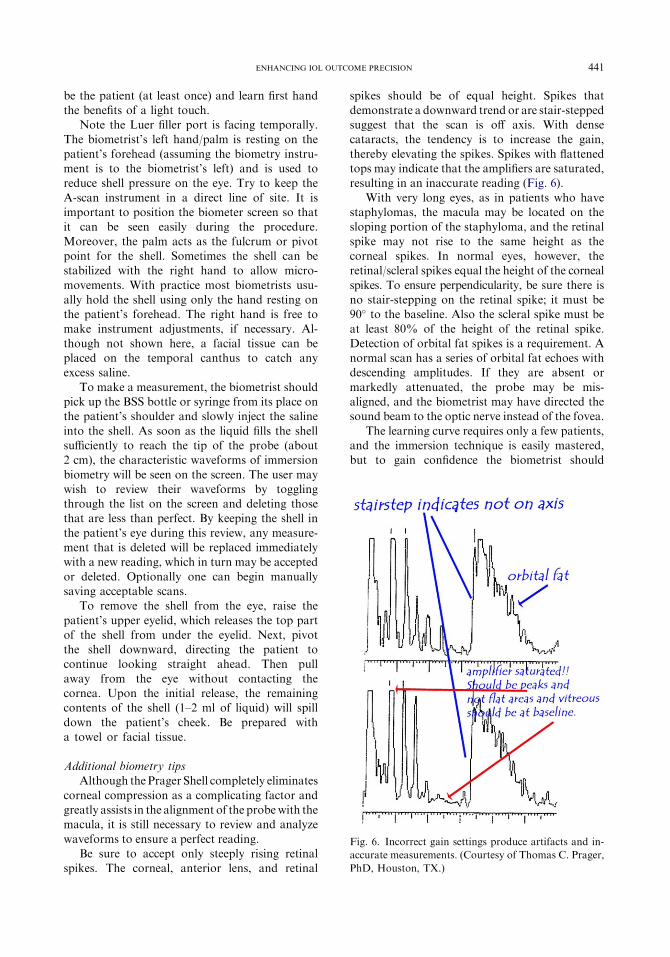
441ENHANCING IOL OUTCOME PRECISION
be the patient (at least once) and learn first handthe benefits of a light touch.
Note the Luer filler port is facing temporally.The biometrist’s left hand/palm is resting on the
patient’s forehead (assuming the biometry instru-ment is to the biometrist’s left) and is used toreduce shell pressure on the eye. Try to keep the
A-scan instrument in a direct line of site. It isimportant to position the biometer screen so thatit can be seen easily during the procedure.
Moreover, the palm acts as the fulcrum or pivotpoint for the shell. Sometimes the shell can bestabilized with the right hand to allow micro-
movements. With practice most biometrists usu-ally hold the shell using only the hand resting onthe patient’s forehead. The right hand is free tomake instrument adjustments, if necessary. Al-
though not shown here, a facial tissue can beplaced on the temporal canthus to catch anyexcess saline.
To make a measurement, the biometrist shouldpick up the BSS bottle or syringe from its place onthe patient’s shoulder and slowly inject the saline
into the shell. As soon as the liquid fills the shellsufficiently to reach the tip of the probe (about2 cm), the characteristic waveforms of immersion
biometry will be seen on the screen. The user maywish to review their waveforms by togglingthrough the list on the screen and deleting thosethat are less than perfect. By keeping the shell in
the patient’s eye during this review, any measure-ment that is deleted will be replaced immediatelywith a new reading, which in turn may be accepted
or deleted. Optionally one can begin manuallysaving acceptable scans.
To remove the shell from the eye, raise the
patient’s upper eyelid, which releases the top partof the shell from under the eyelid. Next, pivotthe shell downward, directing the patient tocontinue looking straight ahead. Then pull
away from the eye without contacting thecornea. Upon the initial release, the remainingcontents of the shell (1–2 ml of liquid) will spill
down the patient’s cheek. Be prepared witha towel or facial tissue.
Additional biometry tipsAlthough thePrager Shell completely eliminates
corneal compression as a complicating factor andgreatly assists in the alignment of the probewith themacula, it is still necessary to review and analyze
waveforms to ensure a perfect reading.Be sure to accept only steeply rising retinal
spikes. The corneal, anterior lens, and retinal
spikes should be of equal height. Spikes thatdemonstrate a downward trend or are stair-steppedsuggest that the scan is off axis. With densecataracts, the tendency is to increase the gain,
thereby elevating the spikes. Spikes with flattenedtops may indicate that the amplifiers are saturated,resulting in an inaccurate reading (Fig. 6).
With very long eyes, as in patients who havestaphylomas, the macula may be located on thesloping portion of the staphyloma, and the retinal
spike may not rise to the same height as thecorneal spikes. In normal eyes, however, theretinal/scleral spikes equal the height of the corneal
spikes. To ensure perpendicularity, be sure there isno stair-stepping on the retinal spike; it must be90� to the baseline. Also the scleral spike must beat least 80% of the height of the retinal spike.
Detection of orbital fat spikes is a requirement. Anormal scan has a series of orbital fat echoes withdescending amplitudes. If they are absent or
markedly attenuated, the probe may be mis-aligned, and the biometrist may have directed thesound beam to the optic nerve instead of the fovea.
The learning curve requires only a few patients,and the immersion technique is easily mastered,but to gain confidence the biometrist should
Fig. 6. Incorrect gain settings produce artifacts and in-
accurate measurements. (Courtesy of Thomas C. Prager,
PhD, Houston, TX.)

442 PRAGER et al
follow the additional suggestions and be familiarwith the sources of error discussed in this article.
Corneal power measurements
In most eyes with normal corneas, cornealpower is measured with keratometry using a stan-dard keratometer. It is important to calibrate the
keratometers frequently to obtain accurate results.With the advent of keratorefractive surgery,
previous methods for calculating the corneal
power after corneal refractive surgery are inaccu-rate [10–15,17–36,71]. The instrumentation usedin the calculation of keratometric power makes
basic assumptions about corneal physiology thatchange with refractive surgery. These changes in-fluence accurate computation of corneal power.For example, the keratometer assumes that the
central cornea is spherical and prolate, with a pos-terior radius of curvature that is 1.2 mm less thanthe anterior (that is, steeper curvature posteriorly
with respect to the anterior surface). Seitz and col-leagues [18] found a mean increase in the posteriorcurvature of 0.11 D in 57 eyes after myopic
surgery. Refractive surgery changes the basicanatomy of the cornea through ablationdthe an-terior central cornea becomes oblate and aspheri-
cal, and the rate of curvature is changed respect tothe posterior surface [18–20]. These basic changesskew the measurements of corneal power takenwith current instrumentation, and without know-
ing the true corneal power it is difficult to calcu-late the necessary IOL power needed.
There are problems with keratometer accuracy
even in patients who have had radial keratometry,whose corneal radii of curvature are assumed toremain relatively unchanged [17]. It has been sug-
gested that these problems are caused by a flattercentral zone, which falls inside the keratometer’sannulus. The keratometer reads the steeper para-
central zone outside the transition zone of the ra-dial keratometry treatment, which erroneouslyindicates a higher keratometry (K) value. Evenwith corneal topography (CT), incorrect assump-
tions of corneal anatomy lead to errors: true cen-tral readings of corneal power are missed withkeratometry, because the actual readings are para-
central [72,73].Individuals who have undergone keratorefrac-
tive procedures expect accurate results after cata-
ract surgery, because they had accurate results withtheir refractive surgery. It therefore is important toidentify themost accuratemeansof calculating IOL
power. There are many methods and theories as tothe best way to measure the true central cornealpower after refractive surgery. The theoretical
optical formulas (Haigas, Hoffer Q, and Holladay1 and 2) determine the effective lens positionthrough additional parameters such as horizontalwhite-to-white distance, anterior chamber depth,
lens thickness, and (in the Holladay 2 formula)age of patient, because the effective lens positioncannot be measured preoperatively [9,74].
There are both indirect and direct methods ofcalculating keratometric power after refractivesurgery. These methods help the surgeon circum-
vent the inability to measure the central cornealpower directly after refractive surgery. The in-direct methods are so named because they usemeasurements other than post–refractive surgery
corneal powers to calculate IOL power. Thesemethods include the clinical history method, thecontact lens over-refraction (ORx) method, the
vertexed IOL power method, and the intraoper-ative autorefraction method.
Indirect measurements
Clinical history method
The clinical history method traditionally hasbeen considered the best indirect method ofderiving postoperative keratometric power. In-
troduced by Holladay in 1989, this method usespreoperative K values and manifest refractionalong with stable postoperative manifest refrac-tion values [11,12,15–17,21,22,32,36]. The formula
is shown by:
Kpost ¼ Kpre� difference in SphEq;
where Kpost represents the postoperative K value,Kpre represents the preoperative K value, and
SphEq represents the spherical equivalent.This method relies on the ability to obtain
preoperative K values and refraction as well as
a stable postoperative refraction before any in-fluence from cataract. A review of patients in theauthors’ practice who had been treatedwith laser insitu keratomileusis (LASIK) showed that using the
historical K method would have resulted in a post-operative refractive error of þ1.25 � 1.75 D.
Contact lens over-refraction methodThe contact lens over-refraction (ORx) method
was first described for IOL calculations afterradial keratometry in 1989 and for calculationsafter LASIK in 1997 [15,16]. It can be used when

443ENHANCING IOL OUTCOME PRECISION
no presurgical data are available. Four differentparameters are needed in the calculations:
Base curve of contact lens in Diopters (BC)Power of contact lens (P)Manifest refraction (MRx) before ORx
This formula is shown by:
Kpost ¼ BCþ Pþ ðORx�MRxÞ
The main limitation of this method is the
reliability of the refraction in the patient whohas a cataract [10,14,75]. As well, a stable contactlens fit is often difficult to achieve in eyes with
especially flat postsurgical corneas; excessive pool-ing of tears under the contact lens may affect theORx results. A review of patients in the authors’practice who had been treated with LASIK
showed that with use of the contact lens ORxmethod a postoperative result of þ1.91 � 2.31 Dwould have occurred.
Vertexed intraocular lens methodThe vertexed IOL method is based on theoret-
ical studies by Feiz and colleagues [13] and Lat-kany and colleagues [32] using the SRK/Tformula following LASIK and three methods forcalculating IOL power. They looked at standard
keratometric power after LASIK and the clinicalhistory method. They then determined the IOLpower for emmetropia based on pre-LASIK cor-
neal powers. The change in spherical equivalentafter LASIK was then used to modify the IOLpower. Using linear regression of the vertexed
IOL power method compared with standard kera-tometry (K), they developed some nomograms:
Post-myopic LASIK : IOLadj
¼ IOLk� 0:231þ ð0:595� SErxÞ
Post-hyper LASIK : IOLadj
¼ IOLk� 0:751þ ð0:862� SErxÞ
where IOLadj is the adjusted IOL power toimplant for emmetropia, IOLk is the IOL powerusing standard K values of the of post-LASIK
cornea and SRK/T, and Serx is the sphericalequivalent after LASIK (absolute value).
One limitation of this study is the theoretical
nature of the study. There are no publishedreports that tested this technique in a prospectivefashion. Essentially this study assumed that 1 D of
change at the spectacle plane corresponds to 0.7 Dat the IOL plane.
Intraoperative refraction methodThe intraoperative refraction method calcu-
lates the IOL power without requiring axial length
measurements or corneal power readings by usingintraoperative refractive determination to calcu-late the IOL required for emmetropia [76]. A for-mula to describe the IOL power for a given A
constant is used [76]. This method has not gainedwidespread popularity [10,23,77,78].
Direct methods
The direct methods are so named because they
make direct measurements of the postoperativecornea to calculate effective keratometric diopters[10]. These methods must correct somehow for in-
herent inaccuracies in the instruments taking themeasurements (ie, change in the relationship ofanterior and posterior corneal curvature). Experi-ence has shown that the keratometer makes basic
assumptions about the cornea that do not holdtrue after keratorefractive surgery. There are tech-niques that ignore the posterior corneal curvature
change, such as simulated keratometric diopters(SimK). Modern corneal topographers have so-phisticated algorithms to calculate estimated cor-
neal powers that reflect anterior corneal powerover a 3-mm annular zone [79]. Effective refractivepower (EffRP) is another parameter whereby the
mean refractive power is calculated for the central3-mm corneal surface (Holladay Diagnostic Sum-mary, EyeSys Vision, Houston, Texas) [74]. Noneof these techniques accurately accounts for the
posterior curvature, which is known to be variableafter keratorefractive surgery [80,81]. Topographyunits do not measure the true central corneal cur-
vature, because Placido-based units have ringsthat are displaced peripherally because of the flat-tening of the central cornea.
Gaussian optics formula and linear regression
Hamed and colleagues [24] looked at 100 eyesand compared five different methods for deter-mining corneal power after myopic LASIKdEffRP, standard keratometry (K), the Gaussianoptics formula (GauRP), and EffRP and K bothmodified by linear regression (according to the
amount of LASIK-induced refractive change)dwith the traditional clinical history method. TheGaussian formula uses the radius of curvature of

444 PRAGER et al
the anterior and posterior cornea, along with theindex of refraction of air (1.00), anterior K surface(1.376), and aqueous humor (1.336), and also the
corneal thickness to determine the EffRP of thecornea. The posterior curvature was not measureddirectly but was estimated based on findingsfrom Olsen and colleagues [82] that stated that
the two curvatures are related by a constant:R2 ¼ K � R1 (where K ¼ 0.883). Posterior curva-ture (R2) and anterior curvature (R1) therefore
were estimated based on preoperative EffRP.The Gaussian formula offers an improved estima-tion of keratometric diopters when compared with
standard keratometry and videokeratometers. Thisformula suggested using an adjusted K reading of
Kadj ¼ K� 0:24� SE change from refractivesurgeryþ 0:15 D
In the authors’ practice, using this method to
adjust manually or topographically derived simu-lated K readings still results in a residual meanhyperopic error of more than 1 D. By using thisadjustment to the flattest central K reading on
Placido topography, however, the refractive errorpostoperatively is reduced to a slight myopiccorrection on average of �0.09 � 1.36 D.
Aramberri ‘‘double K’’ methodIn 2001 Aramberri [83] reported that the flatter
postsurgical K measurements should not be used
in modern formulas to calculate effective lens po-sition. The flattening and thinning of the corneawith keratorefractive surgery does not affect the
biometric measurements of the anterior chamberstructures (the cornea is the same distance fromthe lens position and iris). The preoperative Kvalues are used to predict the effective lens posi-
tion (essentially the anterior chamber depth),and the postoperative K values are used in the for-mula to compute IOL power. Holladay recog-
nized the importance of this concept andincorporated it in the Holladay IOL Consultantsoftware. The Holladay 2 calculation formula
uses the K value in a vergence formula to calculatethe power of the eye and in determining the effec-tive lens position [9].
Camellin and Calossi methodCamellin and Calossi [36] reported a formula
that uses either the induced refractive change or
the anterior and posterior curvature of the corneato adjust for IOL power in eyes that have under-gone prior refractive surgery. In a series of 20
eyes with prior refractive surgery, they reporteda mean postoperative spherical equivalent ofþ0.26 � 0.73 D (range, �0.25 to þ1.58 D).
Topographic method
When information is not available for amethod calculation, one can take a keratometricreading and use the flattest corneal power within
the central 3 mm of the cornea mapping [32]. Thesimulated keratometry from the topography al-most always leads to a K reading that is too steep,
but by finding the very flattest reading, the powerobtained is usually a flatter keratometry reading.
Maloney topographic methodThe Maloney topographic method uses the
postoperative SimK reading from the centralcornea from the topography unit [71]. The valuethen is used in the formula
K ¼ 376=ð337:5=SimKÞ � 5:5
to derive a K reading to be used in the IOLcalculation software. The results of this methodhave not been reported in a large series of eyes.
Shammas ‘‘no history’’ methodThe benefit of the Shammas ‘‘no history’’
method is that it requires only postoperative
average values for manual keratometry [34]. Tocalculate the eye’s estimated corneal power, thefollowing formula is used:
K ¼ 1:143� ðaverage KÞ � 6:8
The results of this method have not beenreported in a large series of eyes.
Rosa methodRosa and colleagues [23,84] suggested yet an-
other method for calculating IOL power after re-
fractive surgery. They used a correcting factor forcorneal radius (R factor) that was derived froma regression formula (Y ¼ 0.0276 � þ0.3635)and compared it with clinical history and
double-K methods. Nineteen eyes were evaluatedafter refractive surgery, and IOL powers were cal-culated with SRK/T, Hoffer Q, and Holladay 1
formulas. A test for correlation was then con-ducted (Wilcoxon test and Spearman correlation).They found that the R factor used with both
SRK/T and Holladay 1 formulas gave the best re-sults (84.2% and 89.5% of eyes seeing within 2 Dof emmetropia, respectively). The R factor seemed

445ENHANCING IOL OUTCOME PRECISION
superior in this study to both the clinical historymethod and the double-K method. The actual for-mula used in the calculation of IOL power is de-rived from manual measurements of corneal
power and axial length:
K ¼ ð0:0276�ALþ 0:3635Þ �manual K;
where AL represents axial length, and K repre-sents corneal power.
Measurement of anterior and posteriorcorneal surfaces
There are two instruments that may be able to
measure corneal power of the anterior and poste-rior surface of the cornea and provide a moreaccurate direct measurement of the corneal powerfor use in the IOL calculation formulas. The
Orbscan (Bausch & Lomb, Miami, Florida) hasbeen in use for several years and is capable ofmeasuring the front and back surface of the
cornea, although its accuracy has been debated[85–88]. In a series of eyes undergoing cataractsurgery after LASIK in their practice, the authors
retrospectively calculated the actual cornealpower from the refractive results from the cata-ract surgery. This measurement indicated that
the 3.0-mm mean total axial power calculationon the Orbscan correlated relatively well withthe power needed for the SRK/T formula for em-metropia. The axial total power at the 3.0-mm
zone had a relatively small SD of � 0.87 D in10 eyes with prior LASIK, with a mean error of�0.16 D and an error range of �1.72 to þ1.02 D.
The Pentacam has become available recentlyand also is capable of directly measuring the frontand back surfaces of the cornea [89–91]. This sys-
tem allows measurement of the direct center ofthe cornea, unlike Placido topographers. The Pen-tacam can report the true net power of the cornea,
but the IOLcalculation formulas contain an adjust-ment factor for the fact that theKvaluemeasured isactually about 0.75 D more than the actual powerof the normal cornea. The equivalent K reading
of the Pentacam reports what the equivalent Kreading shouldbe for use in the IOLcalculation for-mulas. It is anticipated that the 4-mm equivalent K
reading on the Pentacam may be slightly more ac-curate than theOrbscan readings. This comparisonhasnot yet been reported inpatients actually under-
going cataract surgery but seems to correlate withpre- and postoperative refractive information inpatients undergoing LASIK.
Summary
Lens-based surgery, in the form of cataractsurgery or refractive lens exchange surgery forrefractive error, is growing each year as the
population ages and as the improved IOL choicesallow younger patients to undergo lens exchangefor surgical refractive correction. Because of in-
creasing patient expectations, the accuracy ofthese calculations is important. The accuracy ofthe calculations depends on the choice of an
appropriate formula for calculating IOL, accuratemeasurement of corneal power and axial length,lens thickness, anterior chamber depth, and an
accurate estimation of effective lens position.
References
[1] Fedorov SN, Kolinko AI. [A method of calculating
the optical power of the intraocular lens]. Vestn
Oftalmol 1967;80:27–31 [in Russian].
[2] Binkhorst CD. Power of the prepupillary pseudo-
phakos. Br J Ophthalmol 1972;56:332–7.
[3] Colenbrander MC. Calculation of the power of an
iris clip lens for distant vision. Br J Ophthalmol
1973;57:735–40.
[4] Sanders D, Retzlaff J, KraffM, et al. Comparison of
the accuracy of the Binkhorst, Colenbrander, and
SRK implant power prediction formulas. J Am
Intraocul Implant Soc 1981;7:337–40.
[5] Binkhorst R. Intraocular lens power calculation
manual. A guide to the author’s TI 58/59 IOL power
module. New York: Binkhorst RD; 1981.
[6] Holladay JT, Prager TC, Chandler TY, et al. A
three-part system for refining intraocular lens power
calculations. J Cataract Refract Surg 1988;14:17–24.
[7] Hoffer KJ. The Hoffer Q formula: a comparison of
theoretic and regression formulas. J Cataract Re-
fract Surg 1993;19:700–12.
[8] Retzlaff JA, Sanders DR, Kraff MC. Development
of the SRK/T intraocular lens implant power calcu-
lation formula. J Cataract Refract Surg 1990;16:
333–40.
[9] Hoffer KJ. Clinical results using the Holladay 2 in-
traocular lens power formula. J Cataract Refract
Surg 2000;26:1233–7.
[10] Hamilton DR, Hardten DR. Cataract surgery in pa-
tients with prior refractive surgery. Curr Opin Oph-
thalmol 2003;14:44–53.
[11] Seitz B, Langenbucher A. Intraocular lens calcula-
tions status after corneal refractive surgery. Curr
Opin Ophthalmol 2000;11:35–46.
[12] Speicher L. Intra-ocular lens calculation status after
corneal refractive surgery. Curr Opin Ophthalmol
2001;12:17–29.
[13] Feiz V, Mannis MJ, Garcia-Ferrer F, et al. Intraoc-
ular lens power calculation after laser in situ

446 PRAGER et al
keratomileusis for myopia and hyperopia: a stan-
dardized approach. Cornea 2001;20:792–7.
[14] Haigis W. Corneal power after refractive surgery for
myopia: contact lens method. J Cataract Refract
Surg 2003;29:1397–411.
[15] Holladay JT. Consultations in refractive surgery.
IOL calculations following RK [comment]. Refract
Corneal Surg 1989;5:203.
[16] Holladay JT. Cataract surgery in patients with previ-
ous keratorefractive surgery. Ophthalmic Practice
1997;15:238–44.
[17] Hoffer KJ. Intraocular lens power calculation for
eyes after refractive keratotomy. J Refract Surg
1995;11:490–3.
[18] Seitz B, Torres F, Langenbucher A, et al. Posterior
corneal curvature changes after myopic laser in situ
keratomileusis. Ophthalmology 2001;108:666–72
[discussion: 673].
[19] Naroo SA, Charman WN. Changes in posterior
corneal curvature after photorefractive keratec-
tomy. J Cataract Refract Surg 2000;26:872–8.
[20] Kamiya K, Oshika T, Amano S, et al. Influence of
excimer laser photorefractive keratectomy on the
posterior corneal surface. J Cataract Refract Surg
2000;26:867–71.
[21] Odenthal MT, Eggink CA, Melles G, et al. Clinical
and theoretical results of intraocular lens power cal-
culation for cataract surgery after photorefractive
keratectomy for myopia. Arch Ophthalmol 2002;
120:431–8.
[22] Hoffer KJ. Calculating intraocular lens power after
refractive corneal surgery. Arch Ophthalmol 2002;
120:500–1.
[23] Rosa N, Iura A, Romano M, et al. Correlation be-
tween automated and subjective refraction before
and after photorefractive keratectomy. J Refract
Surg 2002;18:449–53.
[24] HamedAM,Wang L,MisraM, et al. A comparative
analysis of five methods of determining corneal re-
fractive power in eyes that have undergone myopic
laser in situ keratomileusis. Ophthalmology 2002;
109:651–8.
[25] Seitz B, Langenbucher A, Nguyen NX, et al. Under-
estimation of intraocular lens power for cataract
surgery after myopic photorefractive keratectomy.
Ophthalmology 1999;106:693–702.
[26] Hugger P, Kohnen T, La Rosa FA, et al. Compari-
son of changes in manifest refraction and corneal
power after photorefractive keratectomy. Am J
Ophthalmol 2000;129:68–75.
[27] Wang L, Jackson DW, Koch DD. Methods of esti-
mating corneal refractive power after hyperopic
laser in situ keratomileusis. J Cataract Refract
Surg 2002;28:954–61.
[28] Gimbel H, Sun R, Kaye GB. Refractive error in cat-
aract surgery after previous refractive surgery. J Cat-
aract Refract Surg 2000;26:142–4.
[29] Ladas JG, Boxer Wachler BS, et al. Intraocular lens
power calculations using corneal topography after
photorefractive keratectomy. Am J Ophthalmol
2001;132:254–5.
[30] Gimbel HV, Sun R. Accuracy and predictability of
intraocular lens power calculation after laser in situ
keratomileusis. J Cataract Refract Surg 2001;27:
571–6.
[31] Gimbel HV, Sun R, Furlong MT, et al. Accuracy
and predictability of intraocular lens power calcula-
tion after photorefractive keratectomy. J Cataract
Refract Surg 2000;26:1147–51.
[32] Latkany RA, Chokshi AR, Speaker MG, et al. In-
traocular lens calculations after refractive surgery.
J Cataract Refract Surg 2005;31:562–70.
[33] Cheng AC, Lam DS. Correcting the corneal power
measurements for intraocular lens power calcula-
tions after myopic laser in situ keratomileusis. Am
J Ophthalmol 2004;137:970 [author reply: 970].
[34] Shammas HJ, Shammas MC, Garabet A, et al. Cor-
recting the corneal power measurements for intraoc-
ular lens power calculations after myopic laser in
situ keratomileusis. Am J Ophthalmol 2003;136:
426–32.
[35] Randleman JB, Loupe DN, Song CD, et al. Intraoc-
ular lens power calculations after laser in situ kerato-
mileusis. Cornea 2002;21:751–5.
[36] Camellin M, Calossi A. A new formula for intraoc-
ular lens power calculaton after refractive corneal
surgery. J Refract Surg 2006;22:187–99.
[37] KahnHA, LeibowitzHM,Ganley JP, et al. The Fra-
mingham Eye Study. I. Outline and major preva-
lence findings. Am J Epidemiol 1977;106:17–32.
[38] Four costliest outpatient procedures. Hospitals and
Health Networks 1998;72:32–3.
[39] Steinberg EP, Javitt JC, Sharkey PD, et al. The con-
tent and cost of cataract surgery. Arch Ophthalmol
1993;111:1041–9.
[40] Holladay JT, Prager TC, Ruiz RS, et al. Improving
the predictability of intraocular lens power calcula-
tions. Arch Ophthalmol 1986;104:539–41.
[41] Javitt JC, Brenner MH, Curbow B, et al. Outcomes
of cataract surgery. Improvement in visual acuity
and subjective visual function after surgery in the
first, second, and both eyes. Arch Ophthalmol
1993;111:686–91.
[42] Mangione CM, Phillips RS, Lawrence MG, et al.
Improved visual function and attenuation of de-
clines in health-related quality of life after cataract
extraction. Arch Ophthalmol 1994;112:1419–25.
[43] Prager TC, Chuang AZ, Slater CH, et al. The Hous-
ton Vision Assessment Test (HVAT): an assessment
of validity. The Cataract Outcome Study Group.
Ophthalmic Epidemiol 2000;7:87–102.
[44] Drexler W, Findl O, Menapace R, et al. Partial co-
herence interferometry: a novel approach to biome-
try in cataract surgery. Am J Ophthalmol 1998;126:
524–34.
[45] HaigisW, Lege B,Miller N, et al. Comparison of im-
mersion ultrasound biometry and partial coherence
interferometry for intraocular lens calculation

447ENHANCING IOL OUTCOME PRECISION
according to Haigis. Graefes Arch Clin Exp Oph-
thalmol 2000;238:765–73.
[46] Packer M, Fine IH, Hoffman RS, et al. Immersion
A-scan compared with partial coherence interferom-
etry: outcomes analysis. J Cataract Refract Surg
2002;28:239–42.
[47] Kiss B, Findl O, Menapace R, et al. Biometry of
cataractous eyes using partial coherence interfer-
ometry: clinical feasibility study of a commercial
prototype I. J Cataract Refract Surg 2002;28:
224–9.
[48] Kiss B, Findl O, Menapace R, et al. Refractive out-
come of cataract surgery using partial coherence in-
terferometry and ultrasound biometry: clinical
feasibility study of a commercial prototype II. J Cat-
aract Refract Surg 2002;28:230–4.
[49] Tehrani M, Krummenauer F, Blom E, et al. Evalua-
tion of the practicality of optical biometry and
applanation ultrasound in 253 eyes. J Cataract Re-
fract Surg 2003;29:741–6.
[50] RajanMS, Keilhorn I, Bell JA. Partial coherence la-
ser interferometry vs conventional ultrasound biom-
etry in intraocular lens power calculations. Eye 2002;
16:552–6.
[51] Nemeth J, Fekete O, Pesztenlehrer N. Optical
and ultrasound measurement of axial length and
anterior chamber depth for intraocular lens
power calculation. J Cataract Refract Surg 2003;
29:85–8.
[52] Tehrani M, Krummenauer F, Kumar R, et al. Com-
parison of biometric measurements using partial co-
herence interferometry and applanation ultrasound.
J Cataract Refract Surg 2003;29:747–52.
[53] Verhulst E, Vrijghem JC. Accuracy of intraocular
lens power calculations using the Zeiss IOL master.
A prospective study. Bull Soc Belge Ophtalmol
2001;281:61–5.
[54] Hasemeyer S, Hugger P, Jonas JB. Preoperative bi-
ometry of cataractous eyes using partial coherence
laser interferometry. Graefes Arch Clin Exp Oph-
thalmol 2003;241:251–2.
[55] Hoffer KJ. Biometry of 7,500 cataractous eyes. Am J
Ophthalmol 1980;90:360–8.
[56] Hoffer KJ. Steps for IOL power calculation. J Am
Intraocul Implant Soc 1980;6:370.
[57] Ossoinig KC. Standardized echography: basic prin-
ciples, clinical applications, and results. Int Ophthal-
mol Clin 1979;19:127–210.
[58] Coleman J, Lizzi F, Jack R. Ultrasonography of
the eye and orbit. Philadelphia: Lea & Febiger;
1977.
[59] Shammas HJ. A comparison of immersion and con-
tact techniques for axial length measurement. J Am
Intraocul Implant Soc 1984;10:444–7.
[60] Lai PC, Savage HI, Payman AS. Refractive surprise
after contact ultrasonography. Invest Ophthalmol
Vis Sci 2003;44: E-Abstract 212.
[61] Hill W. Axial length: do you measure up? Ophthal-
mology Management 2002;6:58–60.
[62] Watson A, Armstrong R. Contact or immersion
technique for axial length measurement? Aust N Z
J Ophthalmol 1999;27:49–51.
[63] Fries U, Hoffmann PC, Hut WW, Echardt HM,
et al. [IOL calculations and ultrasonic biometry: im-
mersion and contact procedures]. Klin Monatsbl
Augenheilkd 1999;214(1):55 [in German].
[64] Hoffmann PC, Hutz WW, Eckhardt HB, et al. [In-
traocular lens calculation and ultrasound biometry:
immersion and contact procedures]. Klin Monatsbl
Augenheilkd 1998;213:161–5 [in German].
[65] Giers U, Epple C. Comparison of A-scan device ac-
curacy. J Cataract Refract Surg 1990;16:235–42.
[66] Schelenz J, Kammann J. Comparison of contact and
immersion techniques for axial length measurement
and implant power calculation. J Cataract Refract
Surg 1989;15:425–8.
[67] Olsen T, Nielsen PJ. Immersion versus contact
technique in the measurement of axial length by ul-
trasound. Acta Ophthalmol (Copenh) 1989;67:
101–2.
[68] Byrne SF. A-scan axial eye length measurements.
Mars Hill (NC): Grove Park Publishers; 1995.
[69] CDC. Current trends recommendations for prevent-
ing possible transmission of human T-lymphotropic
virus type III/ lymphadenopathy-associated virus
from tears. MMWR Morb Mortal Wkly Rpt 1985;
34:533–4.
[70] Velazquez-Estades LJ, Wanger A, Kellaway J, et al.
Microbial contamination of immersion biometry ul-
trasound equipment. Ophthalmology 2005;112:
e13–8.
[71] Wang L, Booth MA, Koch DD. Comparison of in-
traocular lens power calculation methods in eyes
that have undergone laser-assisted in-situ keratomi-
leusis. Trans Am Ophthalmol Soc 2004;102:189–96
[discussion: 196–7].
[72] Celikkol L, Pavlopoulos G, Weinstein B, et al. Cal-
culation of intraocular lens power after radial kera-
totomywith computerized videokeratography. Am J
Ophthalmol 1995;120:739–50.
[73] Husain SE, Kohnen T, Maturi R, et al. Computer-
ized videokeratography and keratometry in deter-
mining intraocular lens calculations. J Cataract
Refract Surg 1996;22:362–6.
[74] Holladay JT. Corneal topography using the Holla-
day diagnostic summary. J Cataract Refract Surg
1997;23:209–21.
[75] Zeh WG, Koch DD. Comparison of contact lens
overrefraction and standard keratometry for mea-
suring corneal curvature in eyes with lenticular opac-
ity. J Cataract Refract Surg 1999;25:898–903.
[76] Ianchulev T, Salz J, Hoffer K, et al. Intraoperative
optical refractive biometry for intraocular lens
power estimation without axial length and keratom-
etrymeasurements. J Cataract Refract Surg 2005;31:
1530–6.
[77] Oyo-Szerenyi KD, Wienecke L, Businger U, et al.
Autorefraction/autokeratometry and subjective
448 PRAGER et al
refraction in untreated and photorefractive keratec-
tomy-treatedeyes.ArchOphthalmol 1997;115:157–64.
[78] Salchow DJ, Zirm ME, Stieldorf C, et al. Compari-
son of objective and subjective refraction before and
after laser in situ keratomileusis. J Cataract Refract
Surg 1999;25:827–35.
[79] Wilson SE, Klyce SD. Quantitative descriptors of
corneal topography. A clinical study. Arch Ophthal-
mol 1991;109:349–53.
[80] Maeda N, Klyce SD, Smolek MK, et al. Disparity
between keratometry-style readings and corneal
power within the pupil after refractive surgery for
myopia. Cornea 1997;16:517–24.
[81] Wilson SE. Cautions regarding measurements of the
posterior corneal curvature. Ophthalmology 2000;
107:1223.
[82] Olsen T. On the calculation of power from curvature
of the cornea. Br J Ophthalmol 1986;70:152–4.
[83] Aramberri J. Intraocular lens power calculation
after corneal refractive surgery: double-K method.
J Cataract Refract Surg 2003;29:2063–8.
[84] Rosa N, Capasso L, Lanza M, et al. Reliability of
a new correcting factor in calculating intraocular
lens power after refractive corneal surgery. J Cata-
ract Refract Surg 2005;31:1020–4.
[85] Iskander NG, Anderson Penno E, Peters NT,
et al. Accuracy of Orbscan pachymetry measure-
ments and DHG ultrasound pachymetry in
primary laser in situ keratomileusis and LASIK
enhancement procedures. J Cataract Refract Surg
2001;27:681–5.
[86] Boscia F, La Tegola MG, Alessio G, et al. Accuracy
of Orbscan optical pachymetry in corneas with haze.
J Cataract Refract Surg 2002;28:253–8.
[87] Prisant O, Calderon N, Chastang P, et al. Reliability
of pachymetric measurements using Orbscan after
excimer refractive surgery. Ophthalmology 2003;
110:511–5.
[88] Srivannaboon S, Reinstein DZ, Sutton HF, et al.
Accuracy of Orbscan total optical power maps in
detecting refractive change after myopic laser in
situ keratomileusis. J Cataract Refract Surg 1999;
25:1596–9.
[89] O’DonnellC,Maldonado-CodinaC.Agreement and
repeatability of central thickness measurement in
normal corneas using ultrasound pachymetry and
the OCULUS Pentacam. Cornea 2005;24:920–4.
[90] Buehl W, Stojanac D, Sacu S, et al. Comparison of
three methods of measuring corneal thickness and
anterior chamber depth. Am J Ophthalmol 2006;
141:7–12.
[91] Barkana Y, Gerber Y, Elbaz U, et al. Central cor-
neal thickness measurement with the Pentacam
Scheimpflug system, optical low-coherence reflec-
tometry pachymeter, and ultrasound pachymetry.
J Cataract Refract Surg 2005;31:1729–35.
Ophthalmol Clin N Am 19 (2006) 449–456
Endophthalmitis ProphylaxisJudy I. Ou, MD1, Christopher N. Ta, MD*
Department of Ophthalmology, Stanford University School of Medicine, 900 Blake Wilbur Drive,
W3036, Stanford, CA 94305, USA
Endophthalmitis is a rare but devastatingcomplication of intraocular surgery that oftencarries a poor prognosis. This article examines
the rising incidence of endophthalmitis and re-views perioperative techniques used to reduce therate of endophthalmitis.
Incidence
Rising incidence of endophthalmitis
It has been suggested that there may be a recent
increase in the prevalence of postcataract endoph-thalmitis [1–5]. This increase may be associatedwith the rising popularity of clear cornea incision.In a multicenter prospective randomized trial con-
ducted by Nakagi and coworkers [3] betweenMarch 1998 and March 2001, a statistically signif-icant increase in endophthalmitis was observed
with clear cornea incision as compared with scle-rocorneal incisions (0.29% versus 0.05%). In a ret-rospective case-control study conducted between
January 1997 and December 2000 by Cooperand coworkers [1], a threefold greater risk of en-dophthalmitis was observed with clear cornea
wounds as compared with scleral tunnel wounds.In a larger single-center observational retrospec-tive study of acute postoperative endophthalmitisdiagnosed between January 2000 and November
2004 at Bascom Palmer Eye Institute, a trend (al-though not statistically significant) toward in-creased rate of endophthalmitis was seen with
clear cornea incision [2].
* Corresponding author.
E-mail address: [email protected] (C.N. Ta).1 Present address: Proctor Foundation, University of
California, San Francisco, Department of Ophthalmol-
ogy, 95 Kirkham Street, San Francisco, CA 94143.
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All rig
doi:10.1016/j.ohc.2006.07.005
The true incidence of endophthalmitis is difficultto determine given its rare occurrence withina single institution. A review of the literature may
provide a greater number of patients and increasethe power of the study. In a recent systematic reviewof the literature by Taban and coworkers [4] of 215studies of 3,140,650 cataract extractions published
between 1963 and 2003, a higher overall postcatar-act endophthalmitis rate occurred between 2000and 2003 (0.265%) as compared with between
1963 and 2000 (0.128%). The rate of endophthal-mitis was higher with clear cornea incision(0.189%) versus scleral incision (0.079%) between
1992 and 2003. In another recent large popula-tion-based review of United States Medicare bene-ficiary claims between 1994 and 2001 of 447,627cataract surgeries, 1026 cases of presumed endoph-
thalmitis was diagnosed and an increased incidencewas associatedwith the introductionof clear corneaincision [5]. The incidence of endophthalmitis was
higher from 1998 to 2001 (2.5 per 1000) as com-pared with between 1994 and 1997 (1.8 per 1000),possibly reflecting the increasing use of clear cornea
incision by ophthalmologists.These reviews of the literature and Medicare
beneficiary claims provide a large amount of data.
There are inherent limitations to any large reviewofthe literature, however.For example, the reviews byTaban and coworkers [4] and West and coworkers[5] are retrospective in nature and included smaller
studies that differ in methodology and definitions.In addition, decreased preoperative use of povi-dine-iodine and fewer administrations of subcon-
junctival injections at the end of surgery may haveoccurred as ophthalmologists converted from ret-robulbar or peribulbar anesthesia to topical anes-
thesia during this time period; these changes mayserve as confounding factors that could lead to anincreased rate of endophthalmitis. Therefore, data
hts reserved.
ophthalmology.theclinics.com

450 OU & TA
suggesting an increase in the prevalence of endoph-thalmitis and the association with clear cornea inci-sionmust be interpretedwith caution.Nonetheless,
these two reviews provide large amounts of infor-mation and support the overall increased rate of en-dophthalmitis associated with clear corneaincision.
The increased prevalence of postoperative en-dophthalmitis is an important observation sincethe number of cataract surgeries performed each
year and demand for cataract surgery continue torise. In 2002, there were approximately 2.5 millioncataract surgeries performed in the United States
[6]. According to the annual survey of the Ameri-can Society of Cataract and Refractive Surgeonsthe popularity of clear cornea incision is increas-ing; 47% of ophthalmologists used clear cornea
incision in 1997 compared to 72% in 2003 [7,8].Prophylaxis to prevent endophthalmitis is criticalgiven the increased use of clear cornea incision
and associated endophthalmitis.
Endophthalmitis and clear cornea incision
Endophthalmitis rates may be increasing with
clear cornea incision because of decreased woundintegrity associated with clear cornea incision.Variation in intraocular pressure (as caused by
eyelid squeezing or eye rubbing) can introduceocular surface bacteria into the anterior chamber[9,10]. In a study by Taban and coworkers [10],
entrance of surface fluid into the sutureless corneaof cadaveric eyes (as marked by India ink) oc-curred with fluctuations of intraocular pressure.
In addition, McDonnell and coworkers [9] showedwith optical coherence tomography that at low in-traocular pressures, the clear cornea wound ofrabbit and cadaveric eyes tended to gape at the in-
ternal aspect of the wound and allowed fluid fromoutside the eye into the cornea wound and ante-rior chamber.
Risk factors
The relative risks of developing postoperativeendophthalmitis depend on a number of factors,
including the presence of eyelid or conjunctivaldiseases, the patient’s general health, the use ofimmunosuppressant medications, the type of in-
traocular surgery, and intraoperative complica-tions. Systemic risk factors, such as diabetes, havebeen associated with endophthalmitis. In a review
by Phillips and Tasman [11] of 162 consecutivepatients treated for endophthalmitis, 21% haddiabetes. These patients had poorer visual
outcomes and had higher incidences of gram-negative endophthalmitis.Onepossible explanationfor the association between diabetes and endoph-
thalmitis is that diabetics have delayedwound heal-ing and may eradicate bacteria more slowly. Thisassociation was observed in the EndophthalmitisVitrectomy Study, a multicenter randomized pro-
spective clinical trial of 420 patients with acutepostoperative endophthalmitis. Patients with dia-betes had a trend toward worse vision at baseline,
higher incidence of positive cultures and need foradditional surgeries during follow-up, and worsefinal visual outcome [12].
Specific eyelid or periorbital diseases also maypredispose these patients to endophthalmitis. Ina case-report study, Scott and coworkers [13]studied 10 cases of endophthalmitis following sec-
ondary intraocular lens implantation and com-pared this with 34 control patients who had thesame surgery but did not develop endophthalmi-
tis. The study revealed that 5 (50%) out of 10 pa-tients in the study group had preoperative eyelidabnormalities, such as blepharitis or ectropion,
compared with four (11.8%) patients in the con-trol group (P ¼ .018). Further evidence regardingthe relationships between eyelid or conjunctiva
abnormalities is provided by de Kaspar and col-leagues [14]. In this prospective study, conjuncti-val cultures were obtained from patients beforethe application of antibiotics and before intraocu-
lar surgery. Antibiotic susceptibility tests wereperformed on all bacterial isolates. The resultsshowed that patients with local risk factors, de-
fined as the presence of scurf, eyelid, or conjuncti-val hyperemia, chemosis, or discharge, were morelikely to harbor multiresistant organisms, defined
as bacteria resistant to five or more of the 21antibiotics tested (P ¼ .0049). As a result, thesepatients may be more likely to develop postopera-tive endophthalmitis. Furthermore, multiresistant
bacteria have been shown to cause more inflam-mation resulting in worse prognosis comparedwith non-multiresistant bacteria in an endoph-
thalmitis rabbit model [15].A study by Mayer and coworkers [16] suggests
that minimizing contact between the intraocular
lens and the ocular surface may reduce the riskof endophthalmitis. In this 10-year retrospectivestudy, the rate of endophthalmitis was 0.28%
for injectable intraocular lens as compared1.21% for foldable lenses. Injectable intraocularlenses avoid the ocular surface and may be associ-ated with lower rates endophthalmitis. A Swedish
study of 58 cases of endophthalmitis in 54,666

451ENDOPHTHALMITIS PROPHYLAXIS
cataract operations revealed that polymethylmethacrylate lenses were associated with a higherrate of endophthalmitis as compared with acrylicintraocular lens [17].
Perhaps the most significant risk factor for thedevelopment of endophthalmitis is intraoperativecomplications, specifically posterior capsular
break or vitreous loss. In the study published byNorregaard and coworkers [18] involving 19,426patients who underwent cataract surgery from
1985 to 1987, the odds ratio for endophthalmitisassociated with an anterior vitrectomy was 4.86(P ¼ .03) compared with patients without anterior
vitrectomy. Menikoff and coworkers [19] found ina case-control study involving 54 patients diag-nosed with endophthalmitis that the odds ratioafter anterior vitrectomy compared with patients
who did not have an anterior vitrectomy was13.7 (P ! .001).
Targets for prophylaxis
Given that the endophthalmitis rate has in-
creased since the mid to late 1990s it is importantto evaluate methods to decrease the rate ofendophthalmitis with proper prophylaxis. The
authors examine the role of conjunctival flora,povidone-iodine, preoperative antibiotics, intra-operative antibiotics, subconjunctival antibioticinjection, and preoperative patient preparation
as techniques for endophthalmitis prophylaxis.
Role of conjunctiva flora
The conjunctival flora contains bacteria that
cause endophthalmitis. In a study by Speaker andcoworkers [20], in 14 (82%) of 17 cases of endoph-thalmitis the organisms from the vitreous were the
same as that found on the patient’s eyelid, con-junctiva, or nose. This study implicated the exter-nal conjunctiva, eyelid, and nose as sources ofbacteria that lead to endophthalmitis. In another
prospective study by Mistlberger and coworkers[21], 76.6% of preoperative conjunctival smearof 700 consecutive patients who underwent cata-
ract extraction were positive; of these, 75% werecoagulase-negative staphylococci. Furthermore,14.1% of the anterior chamber aspirates were
positive for bacteria, with coagulase-negativestaphylococci and corynebacterium as the mostcommon organisms isolated from the aqueous
fluid. In the Endophthalmitis Vitrectomy Study,69.3% of patients had culture-positive end-ophthalmitis [22]. Of these patients, 70% had
gram-positive bacteria, the source presumably be-ing from the external ocular surface. Bannermanand coworkers [23] further analyzed the datafrom the Endophthalmitis Vitrectomy Study and
found that 68% of the 225 patients diagnosedwith endophthalmitis had the identical bacteriaas those found on their eyelids. Because the pa-
tient’s conjunctiva and lid are implicated as thesource of infection, prophylaxis, such as properpatient preparation, povidone-iodine, and preop-
erative antibiotics, are aimed toward decreasingthe bacterial load in this area.
Povidone-iodine
Povidone-iodine is the only prophylactic agentthat has been shown to reduce the rate ofendophthalmitis. Povidone-iodine is a complexpolymer of polyvinyl pyrolidine and iodine,
a complex that enhances the bactericidal activityof iodine. In a study by Speaker and Menikoff[24], a significant fourfold reduction of culture-
positive endophthalmitis was seen in patientswho underwent preparation with povidone-iodine(0.06%) as compared with silver protein solution
(0.24%). A survey of German ophthalmologistsregarding the rate of endophthalmitis suggeststhat the application of povidone-iodine was asso-
ciated with a lower rate of postoperative endoph-thalmitis [25]. The findings are supported bystudies demonstrating that povidone-iodine is ef-fective in killing conjunctival bacteria flora. In
a study by Apt and coworkers [26], applicationof povidone-iodine significantly decreased the col-onies of bacteria on the conjunctiva surface of 30
patients from 91% to 50%. Five percent povi-done-iodine solution applied at the conclusion ofsurgery also significantly decreased the number
of colony-forming units immediately postopera-tively and at 24 hours following surgery, therebydecreasing bacteria that may enter the surgical
wound postoperatively [27]. This may be of partic-ular importance given the recent evidence regard-ing the possible compromised wound architectureof a clear cornea incision [9,10].
The concentration and technique of povidone-iodine application varies widely. In a prospective,randomized, double-blind study of 105 patients
in the United Kingdom, preoperative conjunc-tival fornices irrigation with 5% rather than 1%povidone-iodine resulted in greater decrease in
colony-forming units, especially with heavier ini-tial bacterial load (greater than 100 colony-form-ing units before irrigation with povidone-iodine)

452 OU & TA
[28]. A statistically significant drop of 96.7% col-ony-forming units was seen in the 5% povidone-iodine group as compared with the 40% decrease
in the 1% povidone-iodine group when there washeavier initial bacterial load. In another prospec-tive, randomized, controlled trial of 200 eyes un-dergoing anterior segment surgery treated with
topical ofloxacin, the study group that underwentirrigation of the fornices with 10 mL of povi-done-iodine had fewer positive conjunctival cul-
tures than the control group that received twodrops of povidone-iodine preoperatively [29]. Inthis study, 26% of study eyes had positive conjunc-
tival cultures immediately before surgery com-pared with 43% of control eyes. At the end ofthe surgery, 18% and 32% of eyes had positiveconjunctival culture in the study and control
group, respectively. This suggests that irrigationof conjunctival sac may be more effective in reduc-ing the conjunctival bacterial load and possibly de-
crease susceptibility to endophthalmitis.
Antibiotics
The use of topical antibiotics preoperatively to
decrease conjunctival bacterial flora has beenstudied extensively. Although no clear study hasshown that the application of antibiotics decreases
the risk of endophthalmitis, it is presumed thatreducing bacterial load may lead to decreasedincidence of endophthalmitis. In a prospective,randomized controlled trial of 92 eyes of 89
patients undergoing anterior segment surgery,application of topical ofloxacin for 3 days (studygroup) compared with 1 hour before surgery
(control group) resulted in greater reduction ofconjunctival bacterial flora [30]. All patients weretreated with topical povidone-iodine. Nineteen
percent of eyes in the study group versus 42% ofthe control group had positive conjunctival floraimmediately before surgery. Fourteen percent of
eyes in the study group versus 34% in the controlgroup had positive conjunctival flora at the con-clusion of surgery. This research group alsoshowed the rate of contamination of intraopera-
tive microsurgical knives to be 5% versus 26%in eyes that received ofloxacin for 3 days versus1 hour preoperatively [31]. These studies suggest
that 3-day preoperative use of ofloxacin resultsin greater reduction of conjunctival bacterial loadcompared with a 1-hour application and thereby
may decrease the risk for endophthalmitis.The increasing use of fluoroquinolones may
result in a higher prevalence of antibiotic
resistance. In a prospective observational studyof 120 eyes, 15% and 16% cultured coagulase-negative staphylococci isolated from the conjunc-
tiva of patients undergoing intraocular surgerywere resistant to ciprofloxacin and ofloxacin,respectively [32]. The finding of increasing bacte-rial resistance to fluoroquinolone in bacterial ker-
atitis is supported by several other studies [33,34].In a study by Recchia and coworkers [35], reviewof records of microbiologic culture of vitreous of
patients with postoperative endophthalmitis andin vitro antibiotic susceptibility showed an in-creasing resistance among all bacterial isolates to
ciprofloxacin (23%–37%).Recently, new generations of fluoroquinolones,
such as moxifloxacin and gatifloxacin, have beenintroduced. These fluoroquinolones have en-
hanced activity toward gram-positive pathogenswhile still maintaining broad-spectrum coverageagainst gram-negative organisms [36,37]. The
fluoroquinolones interfere with bacterial deoxyri-bonucleic acid gyrase (topoisomerase II) and top-oisomerase IV and bacterial resistance seems to be
lower because mutations of both bacterial topoi-somerase II and IV are necessary.
Studies have shown that some fluoroquino-
lones can achieve high aqueous humor concentra-tion following topical applications. For example,in a recent prospective, double-masked, clinicalstudy of 52 eyes of 52 patients given preoperative
topical gatifloxacin 0.3%, moxifloxacin 0.5%, orciprofloxacin 0.3% 1 hour before surgery, bothmoxifloxacin and gatifloxacin resulted in signifi-
cantly higher aqueous humor concentration thanciprofloxacin [38]. The use of topical antibioticsfollowing cataract surgery may be even more im-
portant following clear cornea incision. Giventhe recent evidence of suboptimal wound architec-ture and possible influx of tears into the anteriorchamber following clear cornea cataract surgery,
it may be prudent to prescribe topical antibioticsfollowing cataract surgery at least until the woundis covered with epithelium [9,10].
Systemic antibiotics
The role of systemic antibiotics for endoph-thalmitis prophylaxis has historically been un-
certain. The Endophthalmitis Vitrectomy Studyshowed no benefit in using intravenous amikacinand ceftazidime for postoperative endophthalmi-
tis (because of poor intravitreal antibiotic pene-tration) [39–41]. Recent studies have shown thatoral fluoroquinolones, such as levofloxacin, have

453ENDOPHTHALMITIS PROPHYLAXIS
much improved vitreous penetration and exceededthe 90% minimum inhibitory concentration formany organisms that cause endophthalmitis [42],such as Streptococcus pneumonia and Bacillus ce-
reus [43]; the addition of oral ofloxacin to topicalofloxacin increased vitreous penetration sevenfoldin one study [44] and may be effective for the pro-
phylaxis of endophthalmitis.The use of the more recent oral fluoroquinoles,
such as gatifloxacin and moxifloxacin, for en-
dophthalmitis prophylaxis is also promising. Forexample, Hariprasad and coworkers [45] con-ducted a prospective, nonrandomized study of
24 consecutive patients who underwent pars planavitrectomy between September 2001 and May2002 during which aqueous, vitreous, and serumsamples were obtained after administration of
two 400-mg gatifloxacin tablets taken 12 hoursapart. The mean � standard deviation gatifloxa-cin concentrations in serum (N ¼ 23), vitreous
(N ¼ 23), and aqueous (N ¼ 11) were 5.14 �1.36 mg/mL, 1.34 � 0.34 mg/mL, and 1.08 � 0.54mg/mL, respectively. Mean inhibitory vitreous
and aqueous MIC90 level was achieved againstmany pathogens including S pneumoniae andStaphylococcus epidermidis. The use of oral moxi-
floxacin, two tablets containing 400 mg of moxi-floxacin 12 hours apart, has also resulted inMIC90 levels that exceed a wide spectrum ofgram-positive and gram-negative pathogens in
the vitreous [46]. These studies suggest that oralgatifloxacin and moxifloxacin maybe useful in en-dophthalmitis prophylaxis especially in high-risk
cases, such as when the posterior capsule is bro-ken and vitreous loss occurs.
Irrigation and intracameral antibiotics
The use of intracameral antibiotics and anti-biotics in irrigation solution is controversial. Gills[47] suggested the use of vancomycin (20 mg/mL)
in the infusion fluid in order to decrease the rateof endophthalmitis. Beigi and coworkers [48]showed a statistically significant decrease in posi-tive anterior chamber aspirate cultures (from
20% to 2.7%) in a group that received balancedsalt solution with vancomycin (20 mg/mL) andgentamicin (8 mg/mL) compared with control. In
contrast, a paper by Feys and coworkers [49] of372 patients showed no significant difference inbacteria load in the study group that underwent
surgery with vancomycin irrigating solution com-pared with control groups. Cultures of the ante-rior chamber aqueous fluid can be quite difficult
to obtain, however, and the results unreliable[50]. Interestingly, there was a case report of coag-ulase-negative staphylococcus endophthalmitis af-ter cataract surgery despite the use of intraocular
vancomycin (20 mg/mL in 75 mL of balanced sa-line solution) [51].
Vancomycin may be toxic to the retina in
addition to being ineffective. In a prospective,randomized, double-masked clinical study of 118patients, postoperative cystoid macular edema
was significantly higher in the study patientsreceiving irrigating balanced salt solution supple-mented with vancomycin (10 mg/mL) compared
with control group (angiographic cystoid macularedema rate of 55% versus 19% at 1 month; clini-cal macular edema of 23% versus 7% at 1 month)[52]. Finally, there is increasing bacterial resis-
tance to vancomycin and the Centers for DiseaseControl and Prevention has advocated againstthe routine use of vancomycin in intraoperative ir-
rigating bottles [53].
Subconjunctival antibiotics
Subconjunctival injection of antibiotics is rou-
tinely used, although no study has clearly showna decreased rate of endophthalmitis. In a study byDallison and coworkers [54], perioperative sub-
conjunctival cephazolin reduced or eliminated lidand conjunctival microflora 48 hours followingsurgery. In another small retrospective, case con-
trol study none of the nine patients with endoph-thalmitis received perioperative subconjunctivalcefuroxime, whereas in the control group 47.8%
received perioperative subconjunctival cefurox-ime, suggesting that by not using subconjunctivalantibiotic injection, this may be associated with anincreased rate of endophthalmitis [55]. A trend to-
ward decreasing endophthalmitis rate was seenalso with patients who underwent periocular post-operative injection in a cross-sectional German
survey [25]. Although there are no studies thatclearly show an association between subconjuncti-val antibiotic injection and decreased endophthal-
mitis, many surgeons perform this technique givenits low risk and toxicity.
Patient preparation
Routine preparation of patients undergoingintraocular surgery includes draping the eyes andkeeping eyelashes out of the surgical field. Sterile
drapes and speculum are used to isolate the lashesfrom the surgical field. Buzard and Liapis [56]demonstrated the use of two Steri-Strips to isolate

454 OU & TA
the upper eyelid and a single Steri-Strip to isolatethe lower eyelid before the application of plasticdrapes. Although in a study by Perry and Skaggs
[57] efforts to decrease bacterial load by trimminglashes did not alter periocular bacterial flora, mostsurgeons routinely keep lashes away from the sur-gical field because they are a source of bacterial
contaminant. In addition to the use of povidone-iodine and antibiotics, it is important to maintaina sterile surgical field and strict adherence to ster-
ile techniques.
Summary
Recent publications have produced a body of
evidence suggesting an increase in the prevalenceof endophthalmitis caused by poor wound archi-tecture sometimes associated with a clear cornea
incision. Local risk factors, such as blepharitis,systemic risk factors, such as diabetes, and intra-operative complications, such as vitreous loss,further increase the risk of endophthalmitis.
Endophthalmitis prophylaxis, such as the use ofpovidone-iodine, has been shown to decrease therate of endophthalmitis. The use of 5% povidone-
iodine and irrigation in the fornices and use ofpreoperative antibiotics may decrease conjunctivalbacterial load and in turn lower the rates of
endophthalmitis. In addition, it may be importantto apply povidone-iodine and antibiotics at theconclusion of a clear cornea cataract surgery.
The role of postoperative subconjunctival an-
tibiotic injection is not clear but has been associ-ated with decreased ocular bacterial flora. Finally,discretion should be used with intracameral anti-
biotics, especially vancomycin, because data havenot been clear regarding efficacy and may lead tocystoid macular edema and increased resistance of
bacteria to vancomycin.
References
[1] Cooper BA, Holekamp NM, Bohigian G, et al.
Case-control study of endophthalmitis after cataract
surgery comparing scleral tunnel and clear corneal
wounds. Am J Ophthalmol 2003;136:300–5.
[2] Miller JJ, Scot IU, Flynn HW Jr, et al. Acute-onset
endophthalmitis after cataract surgery (2000–2004):
incidence, clinical settings, and visual acuity out-
comes after treatment. Am J Ophthalmol 2005;139:
983–7.
[3] Nagaki Y, Hayasaka S, Kadoi C, et al. Bacterial
endophthalmitis after small-incision cataract sur-
gery: effect of incision placement and intraocular
lens type. J Cataract Refract Surg 2003;29:20–6.
[4] Taban M, Behrens A, Newcomb RL, et al. Acute
endophthalmitis following cataract surgery: a sys-
tematic review of the literature. Arch Ophthalmol
2005;123:613–20.
[5] West ES, Behrens A, McDonnell PJ, et al. The inci-
denceofendophthalmitis after cataract surgeryamong
the US Medicare population increased between 1994
and 2001. Ophthalmology 2005;112:1388–94.
[6] Leaming DV. Practice styles and preferences of
ASCRS members: 2002 survey. J Cataract Refract
Surg 2003;29:1412–20.
[7] Leaming DV. Practice styles and preferences of
ASCRS members: 1997 survey. J Cataract Refract
Surg 1998;24:552–61.
[8] Leaming DV. Practice styles and preferences of
ASCRS members: 2003 survey. J Cataract Refract
Surg 2004;30:892–900.
[9] McDonnell PJ, Taban M, Sarayba M, et al. Dy-
namic morphology of clear corneal cataract inci-
sions. Ophthalmology 2003;110:2342–8.
[10] TabanM, SaraybaMA, Ignacio TS, et al. Ingress of
India ink into the anterior chamber through suture-
less clear corneal cataract wounds. Arch Ophthal-
mol 2005;123:643–8.
[11] Phillips WB II, Tasman WS. Postoperative endoph-
thalmitis in association with diabetes mellitus. Oph-
thalmology 1994;101:508–18.
[12] Doft BH, Wisniewski SR, Kelsey SF, et al. Diabetes
and postoperative endophthalmitis in the endoph-
thalmitis vitrectomy study. Arch Ophthalmol 2001;
119:650–6.
[13] Scott I, Flynn H Jr, Feuer W. Endophthalmitis after
secondary intraocular lens implantation: a case-
report study. Ophthalmology 1995;102:1925–31.
[14] Mino De Kaspar H, Shriver EM, Nguyen EV, et al.
Risk factors for antibiotic resistant conjunctival bac-
terial flora inpatients undergoing intraocular surgery.
Graefes Arch Clin Exp Ophthalmol 2003;241:730–3.
[15] Mino De Kaspar H, Hoepfner AS, Engelbert M,
et al. Antibiotic resistance pattern and visual out-
come in experimentally-induced Staphylococcus epi-
dermidis endophthalmitis in a rabbit model.
Ophthalmology 2001;108:470–8.
[16] Mayer E, Cadman D, Ewings P, et al. A 10 year ret-
rospective survey of cataract surgery and endoph-
thalmitis in a single eye unit: injectable lenses lower
the incidence of endophthalmitis. Br J Ophthalmol
2003;87:867–9.
[17] Montan P, LundstromM, Stenevi U, et al. Endoph-
thalmitis following cataract surgery in Sweden. The
1998 national prospective survey. Acta Ophthalmol
Scand 2002;80:258–61.
[18] Norregaard J, Thoning H, Bernth-Petersen P, et al.
Risk of endophthalmitis after cataract extraction:
results from the International Cataract Surgery Out-
comes Study. Br J Ophthalmol 1997;81:102–6.
[19] Menikoff J, Speaker M, Marmor M, et al. A case-
control study of risk factors for postoperative
endophthalmitis. Ophthalmology 1991;98:1761–8.

455ENDOPHTHALMITIS PROPHYLAXIS
[20] Speaker MG, Milch FA, Shah MK, et al. Role of
external bacterial flora in the pathogenesis of acute
postoperative endophthalmitis. Ophthalmology 1991;98:
639–49 [discussion: 650].
[21] Mistlberger A, Ruckhofer J, Raithel E, et al. Ante-
rior chamber contamination during cataract surgery
with intraocular lens implantation. J Cataract Re-
fract Surg 1997;23:1064–9.
[22] Han DP, Wisniewski SR, Wilson LA, et al. Spec-
trum and susceptibilities of microbiologic isolates
in the Endophthalmitis Vitrectomy Study. Am J
Ophthalmol 1996;122:1.
[23] Bannerman TL, Rhoden DL, McAllister SK, et al.
The source of coagulase-negative staphylococci in
the Endophthalmitis Vitrectomy Study: a compari-
son of eyelid and intraocular isolates using pulsed-
field gel electrophoresis. Arch Ophthalmol 1997;
115:357–61.
[24] Speaker MG, Menikoff JA. Prophylaxis of endoph-
thalmitis with topical povidone-iodine. Ophthalmol-
ogy 1991;98:1769–75.
[25] Schmitz S, Dick HB, Krummenauer F, et al.
Endophthalmitis in cataract surgery: results of a
German survey. Ophthalmology 1999;106:1869–77.
[26] Apt L, Isenberg S, Yoshimori R, et al. Chemical
preparation of the eye in ophthalmic surgery. III. Ef-
fect of povidone-iodine on the conjunctiva. Arch
Ophthalmol 1984;102:728–9.
[27] Apt L, Isenberg SJ, Yoshimori R, et al. The effect of
povidone-iodine solution applied at the conclusion
of ophthalmic surgery. Am J Ophthalmol 1995;
119:701–5.
[28] Ferguson AW, Scott JA, McGavigan J, et al. Com-
parison of 5% povidone-iodine solution against
1% povidone-iodine solution in preoperative cata-
ract surgery antisepsis: a prospective randomised
double blind study. Br J Ophthalmol 2003;87:163–7.
[29] Mino de Kaspar H, Chang RT, Singh K, et al. Pro-
spective randomized comparison of 2 different
methods of 5% povidone-iodine applications for an-
terior segment intraocular surgery. Arch Ophthal-
mol 2005;123:161–5.
[30] Ta CN, Egbert PR, Singh K, et al. Prospective ran-
domized comparison of 3-day versus 1-hour preoper-
ative ofloxacin prophylaxis for cataract surgery.
Ophthalmology 2002;109:2036–40 [discussion: 2040].
[31] De Kaspar HM, Chang RT, Shriver EM, et al.
Three-day application of topical ofloxacin reduces
the contamination rate of microsurgical knives in
cataract surgery: a prospective randomized study.
Ophthalmology 2004;111:1352–5.
[32] Ta CN, Chang RT, Singh K, et al. Antibiotic resis-
tance patterns of ocular bacterial flora: a prospective
study of patients undergoing anterior segment sur-
gery. Ophthalmology 2003;110:1946–51.
[33] Alexandrakis G, Alfonso EC, Miller D. Shifting
trends in bacterial keratitis in south Florida and
emerging resistance to fluoroquinolones. Ophthal-
mology 2000;107:1497–502.
[34] Goldstein MH, Kowalski RP, Gordon YJ. Emerg-
ing fluoroquinolone resistance in bacterial keratitis:
a 5-year review. Ophthalmology 1999;106:1313–8.
[35] Recchia FM, Busbee BG, Pearlman RB, et al.
Changing trends in the microbiologic aspects of
postcataract endophthalmitis. Arch Ophthalmol
2005;123:341–6.
[36] Alfonso E, Crider J. Ophthalmic infections and their
anti-infective challenges. Surv Ophthalmol 2005;
50(Suppl 1):S1–6.
[37] Ruiz J. Mechanisms of resistance to quinolones: tar-
get alterations, decreased accumulation and DNA
gyrase protection. J Antimicrob Chemother 2003;
51:1109–17.
[38] Solomon R, Donnenfeld ED, Perry HD, et al. Pene-
tration of topically applied gatifloxacin 0.3%, moxi-
floxacin 0.5%, and ciprofloxacin 0.3% into the
aqueous humor. Ophthalmology 2005;112:466–9.
[39] Results of the Endophthalmitis Vitrectomy Study. A
randomized trial of immediate vitrectomy and of in-
travenous antibiotics for the treatment of postoper-
ative bacterial endophthalmitis. Endophthalmitis
Vitrectomy Study Group. Arch Ophthalmol 1995;
113:1479–96.
[40] el-Massry A, Meredith TA, Aguilar HE, et al. Ami-
noglycoside levels in the rabbit vitreous cavity after
intravenous administration. Am J Ophthalmol
1996;122:684–9.
[41] Aguilar HE, Meredith TA, Shaarawy A, et al. Vitre-
ous cavity penetration of ceftazidime after intrave-
nous administration. Retina 1995;15:154–9.
[42] Garcia-Saenz MC, Arias-Puente A, Fresnadillo-
Martinez MJ, et al. Human aqueous humor levels
of oral ciprofloxacin, levofloxacin, and moxifloxa-
cin. J Cataract Refract Surg 2001;27(12):1969–74.
[43] Fiscella RG, Nguyen TK, Cwik MJ, et al. Aqueous
and vitreous penetration of levofloxacin after oral
administration. Ophthalmology 1999;106:2286–90.
[44] Donnenfeld ED, Perry HD, Snyder RW, et al. Intra-
corneal, aqueous humor, and vitreous humor pene-
tration of topical and oral ofloxacin. Arch
Ophthalmol 1997;115:173–6.
[45] Hariprasad SM,MielderWF,Holz ER. Vitreous and
aqueous penetration of orally administered gatifloxa-
cin inhumans.ArchOphthalmol 2003;121(3):345–50.
[46] Harisprasad SM, Shah GK, Mieler WF, et al. Vitre-
ous and aqueous penetration of orally administered
moxifloxacin in humans. Arch Ophthalmol 2006;
124:178–82.
[47] Gills JP.Filters andantibiotics in irrigating solution for
cataract surgery. J Cataract Refract Surg 1991;17:385.
[48] Beigi B, Westlake W, Chang B, et al. The effect of
intracameral, peri-operative antibiotics onmicrobial
contamination of anterior chamber aspirates during
phacoemulsification. Eye 1998;12(Pt 3a):390–4.
[49] Feys J, Salvanet-Bouccara A, Emond JP, et al. Van-
comycin prophylaxis and intraocular contamination
during cataract surgery. J Cataract Refract Surg
1997;23:894–7.
456 OU & TA
[50] Ta CN, Egbert PR, Singh K, et al. The challenge of
determining aqueous contamination rate in anterior
segment intraocular surgery. Am J Ophthalmol
2004;137:662–7.
[51] Townsend-Pico WA, Meyers SM, Langston RH,
et al. Coagulase-negative Staphylococcus endoph-
thalmitis after cataract surgery with intraocular van-
comycin. Am J Ophthalmol 1996;121:318–9.
[52] Axer-Siegel R, Stiebel-Kalish H, Rosenblatt I, et al.
Cystoid macular edema after cataract surgery with
intraocular vancomycin. Ophthalmology 1999;106:
1660–4.
[53] Recommendations for preventing the spread of van-
comycin resistance. Recommendations of theHospi-
tal Infection Control Practices Advisory Committee
(HICPAC). MMWR Recomm Rep 1995;44(RR-
12):1–13.
[54] Dallison IW, Simpson AJ, Keenan JI, et al. Topical
antibiotic prophylaxis for cataract surgery: a con-
trolled trial of fusidic acid and chloramphenicol.
Aust N Z J Ophthalmol 1989;17:289–93.
[55] Lehmann OJ, Roberts CJ, Ikram K, et al. Associa-
tion between nonadministration of subconjunctival
cefuroxime and postoperative endophthalmitis.
J Cataract Refract Surg 1997;23:889–93.
[56] Buzard K, Liapis S. Prevention of endophthalmitis.
J Cataract Refract Surg 2004;30:1953–9.
[57] Perry LD, Skaggs C. Preoperative topical antibiotics
and lash trimming in cataract surgery. Ophthalmic
Surg 1977;8:44–8.

Ophthalmol Clin N Am 19 (2006) 457–468
Phaco Fluidics and Phaco UltrasoundPower Modulations
Uday Devgan, MD, FACSa,b,c,*aMaloney Vision Institute, 10921 Wilshire Boulevard, Suite 900, Los Angeles, CA 90024, USA
bOlive View–UCLA Medical Center, 14445 Olive View Drive, Sylmar, CA 91342, USAcJules Stein Eye Institute, UCLA School of Medicine, 100 Stein Plaza, Los Angeles, CA 90095, USA
The most common surgical procedure in theUnited States is cataract surgery [1]; more specif-
ically, phacoemulsification. Understanding thefluidics and ultrasonic power fundamentals forphacoemulsification machines is instrumental for
their safe and efficient use. Although phaco ma-chines have evolved considerably since they wereintroduced a few decades ago, the basic conceptshave remained the same.
Phaco machines allow ultrasonic-assisted aspi-ration of the cataract while maintaining stabilitywithin the eye and minimizing the trauma of
surgery to ocular structures. In this light, the twoprimary concepts are the fluidics of the lens aspira-tion and the application of the ultrasound power.
Fluidics
The fluidics of phaco machines allows aspira-
tion of the cataract while keeping the eye inflatedand stable, and prevents collapse of the anteriorchamber. The basic concepts of phaco fluidics are
flow and vacuum.
Flow
The fluid used in phaco machines is a balancedsaline solution that mirrors the composition of
aqueous humor. It behaves like a classic New-tonian fluid, being a noncompressible solution,and therefore the simple concepts of laminar flow
* Jules Stein Eye Institute, UCLA School of Medi-
cine, 100 Stein Plaza, Los Angeles, CA 90095.
E-mail address: [email protected]
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All ri
doi:10.1016/j.ohc.2006.08.001
explain its behavior. The flow of the fluid islaminar and the tubing walls are straight, fixed,
and inelastic, in contrast with cardiology, whichdeals with pulsatile flow, elastic and variablevessel walls, and viscous suspension fluid, blood.
The basics for all fluidics in phacoemulsifica-tion surgery can be analyzed with Poiseuille’sequation:
F ¼ DPpr4
8hL
F ¼ flowDP ¼ change in pressure/vacuum level
p ¼ the mathematical constant pir ¼ radius of the tubingh ¼ viscosity of fluid
L ¼ length of tubing
Because the viscosity of the balanced salinesolution (h) is constant, as is the length of phacotubing that is used (L) in every case, the only
variables that need to be considered in determin-ing flow rate are the change in pressure or vacuumlevel (DP) and the radius of the tubing. Because
the radius is to the fourth power, a slight changein the radius of the tubing can make a dramaticdifference in the flow of fluid. If the diameter isused instead of the radius, the formula’s denom-
inator is changed by a factor of 16.
r ¼½dthus : r4 ¼ ð½dÞ4 ¼ ð½Þ4d4 ¼ d4=16
ghts reserved.
ophthalmology.theclinics.com

458 DEVGAN
F ¼ DPpd4
128hL
F ¼ flow
DP ¼ change in pressure/vaccum levelp ¼ the mathematical constant pid ¼ diameter of the tubing
h ¼ viscosity of fluidL ¼ length of tubing
The balanced saline solution flows in and outof the eye, primarily limited to the anterior andposterior chamber in routine phacoemulsification
surgery. Therefore flow balance is easy to evaluatebased on the inflow versus the outflow.
Inflow versus outflow
The source of the inflow fluid is from the bottle
of balanced saline solution that hangs on thephaco machines. The two primary sources ofoutflow are through the lumen of the phaco needleduring aspiration of the lens material, and
through any leaks from surgical incisions. Keep-ing the inflow of fluid greater than the outflow isimportant in maintaining stability and preventing
collapse of the eye during surgery.
Inflow
To keep the inflow higher than the outflow, the
diameter of the inflow infusion tubing is largerthan that of the outflow suction tubing. Otherdifferences can also be seen when examining
a cross-section of the phaco machine tubing.The inflow infusion tubing has a larger borewith thinner, more compliant tubing. The outflow
suction tubing has a narrower bore and thicker,more rigid tubing. This difference is because of thedifferent vacuum level each tube must withstand
during surgery, and is discussed in more detail inthe ‘‘Vacuum’’ section.
The inflow of the infusion fluid is increased bycontrolling the height of the balanced saline
solution bottle. As the height of the infusionbottle is increased, gravity increases the pressuregradient (DP from Poiseuille’s equation). Phaco
machines use an indirect measure of the infusioninflow: the bottle height, typically listed in centi-meters. The difference in height between the
infusion bottle and the patient’s eye determinesthe pressure gradient. If the operating room tableis raised without an equal elevation in the bottle
height, then the inflow will decrease. This fact isimportant for tall surgeons who require morelegroom under the operating room table and in
treating patients who have cardiac, pulmonary, orspinal problems that prevent them from lying flat.
Because the bottle height is limited by thephaco machine apparatus or perhaps the ceiling
height in the operating room, surgeons can in-crease inflow by using a second inflow line, such asan anterior chamber maintainer. An additional
incision into the anterior chamber is made and theadditional infusion line is inserted, thereby dou-bling the effective inflow rate.
Current phaco machine platforms use gravityalone to achieve the pressure gradient required forinflow. Similar to residential water towers, theheight of the water column in the tubing will
determine the infusion inflow pressure gradient.Retinal surgeons use vitrectomy machines thathave a forced infusion through a pump, therefore
achieving higher pressure gradients than simplegravity can provide. Future phaco machines mayalso incorporate this technology.
Outflow
The primary source of fluid outflow duringphacoemulsification is the phaco needle during
aspiration, and the secondary source is leakagefrom the incisions. The total outflow of fluid fromthe eye must be less than the inflow to preventinstability and collapse of the eye. Therefore, the
radius of the outflow suction tubing must be keptsmaller than that of the inflow tubing. The outflowrate through the phaco needle, often measured in
milliliters per minute, can be directly adjusted onmachines with peristaltic pumps, and indirectly ad-justed on machines with venturi pumps.
The most restrictive part of the outflow tubingis typically the phaco needle, and therefore phaconeedle selection is important when choosing
fluidic parameters. As the phaco needle sizedecreases, the flow drops exponentially becausePoiseuille’s equation has this factor raised to thefourth power. To achieve the same inflow while
decreasing the needle size, a very substantialincrease in the pressure gradient (DP from Pois-euille’s equation) is required.
According to Poiseuille’s equation, flow isproportional to the radius of the tube to thefourth power, meaning that a small change in the
size of the phaco needle can result in a very largechange in the flow. When two common-sizedphaco needles (0.9 mm versus 1.1 mm) are

459PHACO FLUIDICS & ULTRASOUND POWER
compared, with all other factors equal, the flowthrough the larger 1.1-mm needle is more thantwice that of the 0.9-mm needle (Fig. 1).
Because the change in flow is exponential,
a lower limit to size exists where the lumen is sosmall that flow approaches zero (Fig. 2). For sur-geries to be efficient, ultrasmall bores will unlikely
be used in traditional phacoemulsification. Theefficiency of surgery, which is better with largerbores, must be balanced with the benefits of
smaller incisions, which better accommodatesmaller bores.
A simple analogy for understanding Pois-
euille’s equation is drinking a milkshake througha straw: if one drinks the milkshake with a small-caliber cocktail straw, then a much higher pres-sure gradient will be needed in the mouth and only
a low flow rate will be achieved. However, ifa larger-bore straw is used, then the requiredpressure gradient is much less and a higher flow
rate can be achieved, resulting in more efficientaspiration of the shake (Fig. 3).
Confounding factors
Matters are further complicated if a phaconeedle with an additional hole in its side-wall is
used, such as those that are intended to maintainlow flow during complete occlusion. AlthoughPoiseuille’s equation and the milkshake analogystill apply, in this instance the straw has a small
hole in its side. During states of higher flow andlower vacuum, the flow through the additionalbypass hole is limited. However, when the end of
the needle is occluded, the vacuum increasesdramatically, the flow through the end of theneedle drops, and the flow through the bypass
Fig. 1. Comparing tubing tips with a seemingly small
difference in diameter can result in a dramatic difference
in flow because of the exponential nature of tubing
radius in Poiseuille’s equation.
hole increases. Compared with a traditional phaco
needle, higher phaco-machine vacuum levels arerequired to achieve the same holding power at thephaco tip (Fig. 4).
Outflow restrictors are available for phacomachines that create a bottleneck distal to thephaco needle in the outflow suction tubing. Theseflow restrictors further decrease the outflow to
ensure that the inflow is never outstripped, therebyincreasing stability within the eye, although at thecost of reduced flow (Fig. 5).
For split-infusion cataract surgery, oftentermed bimanual small incision cataract surgery,the infusion line is split from the aspiration line.
The advantage of this technique is the ability to usethe infusion separately from the aspiration line,compared with traditional coaxial phaco whereboth irrigation infusion and aspiration are on the
same handpiece. The limitation of split-infusioncataract surgery is that the irrigating infusioninstruments are typically of a smaller bore than
the coaxial infusion line, resulting in a significantdecrease in inflow. Surgeons can attempt tocompensate for this decrease in flow by increasing
the pressure gradient (DP) by way of raising theinfusion bottle to its maximum height or evenfurther using an anterior chamber maintainer or
forced infusion. If this technique is not sufficient,the outflow from the eye must be decreased usingthe phaco machine settings (Fig. 6).
Vacuum
Vacuum within the phaco machine must be
created to provide the driving force for the out-flow of fluid during cataract extraction. Thevacuum level is dynamic and changes during the
various parts of surgery. The machines allowselection of a maximum vacuum level, typicallyexpressed in mm Hg, and surgeons can have
Fig. 2. As the size of the phaco needle decreases linearly,
the relative flow through the needle decreases
exponentially.

460 DEVGAN
Fig. 3. A simplification of Poiseuille’s equation at work. (A) When a small caliber cocktail straw is used to drink a milk-
shake, very high vacuum is required in the mouth to create relatively little flow through the straw. (B) A larger-bore
straw is used and low vacuum in the mouth can be used to achieve high flow in the straw. (C) The vacuum generator
of choice for aspiration of milkshakes. (Courtesy of Uday Devgan, MD, FACS, Los Angeles, CA.)
relative control of the vacuum level up to this limitthrough foot pedal positioning, depending on the
type of vacuum pump.Two primary vacuum pumps are used in
phacoemulsification platforms: peristaltic and
Venturi. Although they work in different ways,each has its advantages.
The peristaltic pump uses rollers to compressthe phaco outflow tubing in a peristaltic manner,
thereby creating flow. Although the phaco
Fig. 4. By allowing a small constant flow of fluid even
when the phaco tip is occluded, the phaco needles with
additional bypass holes can help maintain flow; how-
ever, a higher vacuum level would likely be required to
achieve the same holding power at the tip.
machine can directly control this flow level, thepreset vacuum level is only achieved when the
outflow line is occluded, typically from cataractmaterial at the phaco needle tip. As the occlusionoccurs, the vacuum builds, the rollers slow down,
and the outflow level decreases. On completeocclusion, the rollers stop, the outflow approacheszero, and the vacuum is at its highest level (Fig. 7).
The Venturi pump uses the Venturi effect to
create a vacuum. The Venturi effect creates
Fig. 5. Restrictive outflow tubing decreases the size of
the outflow tubing, thereby limiting the flow. This mech-
anism helps ensure that the inflow of fluid into the eye is
always greater than the outflow from the eye, which is
crucial to prevent surge. The purpose of the filter is to
prevent the cataract pieces from clogging the tubing.
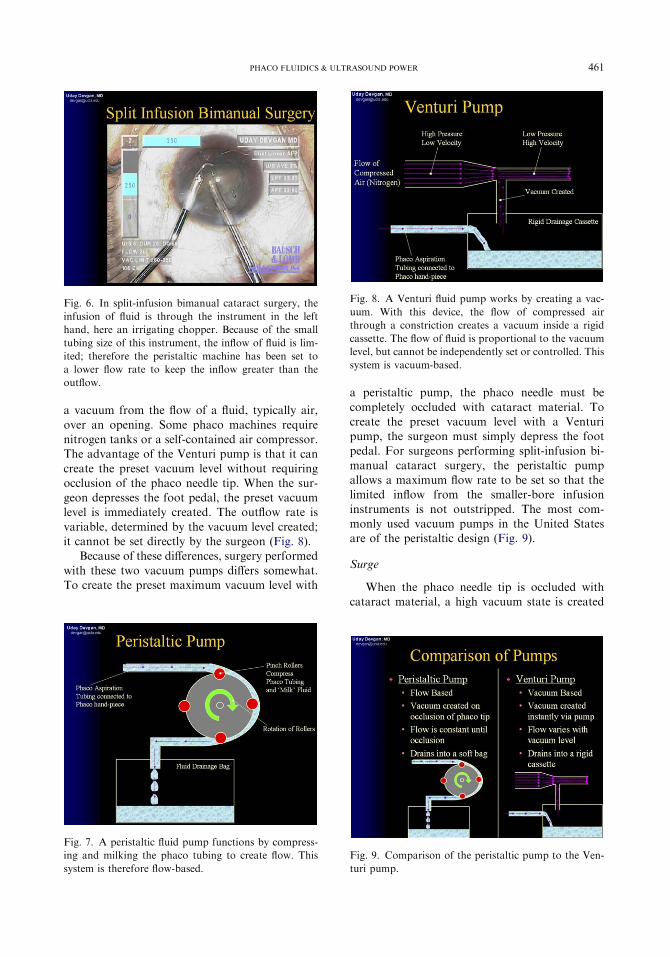
461PHACO FLUIDICS & ULTRASOUND POWER
a vacuum from the flow of a fluid, typically air,
over an opening. Some phaco machines requirenitrogen tanks or a self-contained air compressor.The advantage of the Venturi pump is that it can
create the preset vacuum level without requiringocclusion of the phaco needle tip. When the sur-geon depresses the foot pedal, the preset vacuumlevel is immediately created. The outflow rate is
variable, determined by the vacuum level created;it cannot be set directly by the surgeon (Fig. 8).
Because of these differences, surgery performed
with these two vacuum pumps differs somewhat.To create the preset maximum vacuum level with
Fig. 6. In split-infusion bimanual cataract surgery, the
infusion of fluid is through the instrument in the left
hand, here an irrigating chopper. Because of the small
tubing size of this instrument, the inflow of fluid is lim-
ited; therefore the peristaltic machine has been set to
a lower flow rate to keep the inflow greater than the
outflow.
Fig. 7. A peristaltic fluid pump functions by compress-
ing and milking the phaco tubing to create flow. This
system is therefore flow-based.
a peristaltic pump, the phaco needle must be
completely occluded with cataract material. Tocreate the preset vacuum level with a Venturipump, the surgeon must simply depress the footpedal. For surgeons performing split-infusion bi-
manual cataract surgery, the peristaltic pumpallows a maximum flow rate to be set so that thelimited inflow from the smaller-bore infusion
instruments is not outstripped. The most com-monly used vacuum pumps in the United Statesare of the peristaltic design (Fig. 9).
Surge
When the phaco needle tip is occluded withcataract material, a high vacuum state is created
Fig. 8. A Venturi fluid pump works by creating a vac-
uum. With this device, the flow of compressed air
through a constriction creates a vacuum inside a rigid
cassette. The flow of fluid is proportional to the vacuum
level, but cannot be independently set or controlled. This
system is vacuum-based.
Fig. 9. Comparison of the peristaltic pump to the Ven-
turi pump.

462 DEVGAN
within the outflow tubing. This high vacuum levelwould collapse the walls of elastic tubing and, oncethe occlusion breaks, thewalls would rebound back
into shape, thereby rapidly sucking fluid from theeye and creating surge. Because the volume of theanterior and posterior chamber is so small, a slightcollapse in the length of the long outflow tubing
would create a significant surge and increase therisk for collapse of the eye and aspiration of theposterior capsule during surgery (Fig. 10).
To combat this problem of surge, phacomachines use outflow aspiration tubing that is oflow compliance. This tubing is very rigid, with
thick walls that are resistant to collapse. Com-pared with the inflow tubing, the outflow tubinghas a smaller diameter; thicker, more rigid walls;and low compliance (Figs. 11 and 12).
Surge can also be addressed with a quick-reacting pump that drops the vacuum level as theocclusion breaks. However, no machine can
adequately compensate for high compliance elas-tic tubing and improperly selected fluidic settings.
Choosing fluidic settings
The basic fluidic variables that can be set for
peristaltic phaco machines include bottle height(cm) to determine the inflow infusion, outflow rate(mL/min) through the phaco handpiece, maxi-
mum vacuum level limit (mm Hg), and phaconeedle diameter. The choice of phaco needle is
Fig. 10. The use of compliant tubing allows collapse of
the tubing and storage of energy in the walls. Once the
occlusion breaks, the tubing rebounds as the energy is
released, creating a sharp rise in the outflow from the
eye and potentially causing a surge with resultant col-
lapse of the eye and rupture of the posterior capsule.
Therefore, stiff, rigid, noncompliant outflow tubing
should be used.
important to determine appropriate machine-based settings.
Technique
Different techniques, even different parts of the
same technique, can benefit from tailored fluidicsettings. For sculpting or grooving a nucleus, lowvacuum and low aspiration rates can be used
because the primary purpose of the fluidics is toremove small amount of nucleus that has beenemulsified (Fig. 13).
For a chopping technique, the fluidics must
allow the phaco needle to firmly hold a nuclearpiece so that it may be mechanically disassembled.In this case, a higher vacuum level is required to
create holding power, and the phaco needle mustbe occluded to achieve this higher preset vacuum.A range of aspiration rates may be effectively used
with chopping.
Fig. 11. The outflow tubing, shown in red, has thick
walls and therefore low compliance. The inflow tubing,
shown in blue, has thinner walls and is more compliant.
Fig. 12. Comparison of the inflow versus outflow tub-
ing, shown in cross-section.

463PHACO FLUIDICS & ULTRASOUND POWER
For quadrant or nuclear segment removal,a more moderate vacuum level but a higher
aspiration rate is needed for efficiency. For re-moving the epinuclear shell, the vacuum level andaspiration rates can be decreased to prevent
inadvertent touching of the posterior capsule asthe last bits of cataract are removed.
Patient variables
A dense cataract behaves like a solid, whereasa soft cataract often exhibits fluid motions.Therefore, the grade of cataract influences the
fluidic settings used for its removal. Because a softcataract tends to deform and collapse whenvacuum is applied through the phaco needle,
lower levels should be used.Eyes with shallow anterior chambers would
benefit from a higher bottle height because thiswould increase the infusion pressure and push the
lens–iris diaphragm posterior. Eyes with lowscleral rigidity, such as high myopes, tend tohave an overdeepening of the anterior chamber
and may benefit from a lower bottle height.
Phaco power
Ultrasound energy can be used to emulsify and
aspirate the cataract. The high frequency pro-duces a piston-like movement of the phaco needleat a constant frequency, typically between 28.5
and 40 kHz, depending on the machine. Althoughthis frequency cannot be adjusted, the surgeon cancontrol the stroke length of each piston-like
Fig. 13. While creating a groove in the nucleus, the tip is
nonoccluded and the vacuum level is low, whereas the
flow is high. Once occlusion occurs, the vacuum level
rises to the higher preset maximum level as the flow
drops.
movement. The surgeon can set the maximumpower level, and then the phaco foot pedal can beused to deliver varying amounts of energy up tothis maximum. The units of power provided by
the manufacturers of the current phaco machinesare ‘‘percent of maximum,’’ rather than a truemeasure of power, such as milliwatts, and there-
fore comparison of relative power levels from onephaco platform to another is inexact.
The ultrasonic power has four components: the
mechanical impact, the fluid/particle wave, thecavitation effect, and the acoustical wave. Thesefour components together allow emulsification of
the cataract.The mechanical impact is the actual force of
the phaco needle hitting the cataract nucleus,much like a jackhammer. Standard Newtonian
forces apply, with the force of the impact de-termined by the product of the mass and acceler-ation (F ¼ MA). The force of the impact is
applied at the phaco needle tip, and thereforea sharper needle will have less surface area andwill provide more force per unit area. If a dull
phaco needle is used, a higher phaco power level isrequired to achieve the same cutting efficiency.This scenario is similar to a sharp knife creating
a higher force per unit area at the blade edge andthus cutting better given the same overall forceversus a dull knife. A dull knife requires moreapplication of force to achieve the same cut as
a sharp knife.The fluid/particle wave is like a fire hose as it
shoots the saline irrigation solution and tiny
phaco fragments out of the phaco tip on applica-tion of ultrasound energy. This fluid/particle wavehas some ability to break down the nuclear
cataract material at the phaco tip.Cavitation is the effect of shooting the fluid
wave from the phaco tip and creating an area oflow pressure immediately in front of the phaco
needle. This lower pressure area causes implosionof nuclear cataract pieces that are in the vicinity.
Finally, the acoustical wave is the soundwave
created by the phaco needle’s vibrations. Thiswave travels at the speed of sound and providesthe auditory feedback that the surgeon hears
during phacoemulsification. The acoustical waveplays a small role in the break down of thecataract.
The ultrasonic energy delivered into the eye isgreat for emulsification of cataracts, but can alsodamage other ocular structures, particularly thedelicate corneal endothelium. In early phacoemul-
sification surgery, the level of corneal endothelial

464 DEVGAN
cell loss was high and many patients developedcorneal failure. With the development of betterways to protect the cornea through viscoelastics,
and methods to modulate and decrease the phacoenergy, the rate of pseudophakic bullous keratop-athy has decreased dramatically.
Phaco power modulations are methods to
program the way ultrasonic energy is delivered.By delivering smaller pulses or bursts of energy invariable patterns, the phaco efficiency can be
maximized while decreasing the total amount ofphaco energy, phaco time, and phacogeneratedheat placed into the eye.
Measuring phaco energy
Phacoemulsification machines can measure theaverage phaco power and the phaco time (the
total amount of time spent on the foot pedal atposition 3). However, no standard method existsto quantify and measure the units of energy
delivered to the eye. What can be measured isthe absolute amount of phaco energy deliveredinto the eye at 100% power, known as absolutephaco time (APT). More specifically, APT can be
considered the product of phaco time multipliedby the average phaco power. For example, 15seconds � 100% power level ¼ 15 seconds of
APT; 30 seconds � 50% power level ¼ 15 secondsof APT; and 60 seconds � 25% power level ¼ 15seconds of APT.
Therefore, a decrease in APT signifies a de-crease in phaco time and average phaco power. Asurgeon can attain an ultralow time or ‘‘0-second
phaco,’’ for example, by having a phaco time of17 seconds � 4% power ¼ 0.68 seconds, or lessthan 1 second of APT (Fig. 14). An ultralow APTresults in clearer corneas and sharper vision on the
first postoperative day, thus achieving a high pa-tient satisfaction rate.
Decreasing phaco time and energy
To reduce total phaco time and energy placedinto the eye, a mechanical method of breaking thenucleus, such as chopping, must be used.
Mechanical nuclear disassembly using the chop-ping technique allows the surgeon to mechanicallybreak the nucleus into small fragments. Addition-
ally, switching from a four-quadrant to a stop-and-chop technique allows for less grooving.During theprocedure, the surgeon must also switch from the
four-quadrant divide-and-conquer technique toa stop-and-chop approach and avoid using single-handed phacoemulsification.
The surgeon may lessen time on the foot pedalby phacoemulsifying only on the forward strokes
during grooving or divide-and-conquer. Addition-ally, phacoemulsification should only be per-formed when the phaco tip is occluded with
nuclear material, because otherwise aspiration iscompromised.
Basic versus advanced power modulations
The basic power settings are continuous, pulse,and burst. The continuous power setting delivers
energy continuously, with variable power, de-pending on how long the foot pedal is depressed.The maximum power setting can be preset, thus
allowing surgeons to control the maximumamount of phaco power delivered. In other words,the longer the foot pedal is depressed, the greater
the phaco power (Fig. 15).In pulse mode, the pulses of energy dispensed
have variable power, depending on how long the
foot pedal is depressed. The longer it is depressed,the greater the power of each sequential pulse ofenergy. The defining feature of pulse mode is thatafter each pulse of energy is delivered, a period
occurs during which no energy is supplied be-tween increasing pulses of energy, which is the‘‘off’’ period. Alternating between the ‘‘on’’ and
‘‘off’’ periods reduces heat and dispenses half theenergy into the eye (Fig. 16).
Finally, in burst mode, each burst of energy
has the same amount of power, but the intervalbetween each burst increases as the foot pedal isdepressed. The longer the foot pedal is depressed,
Fig. 14. An eye immediately after phacoemulsification
in which phaco power modulations have been used to
truly minimize the amount of ultrasound energy deliv-
ered into the eye.
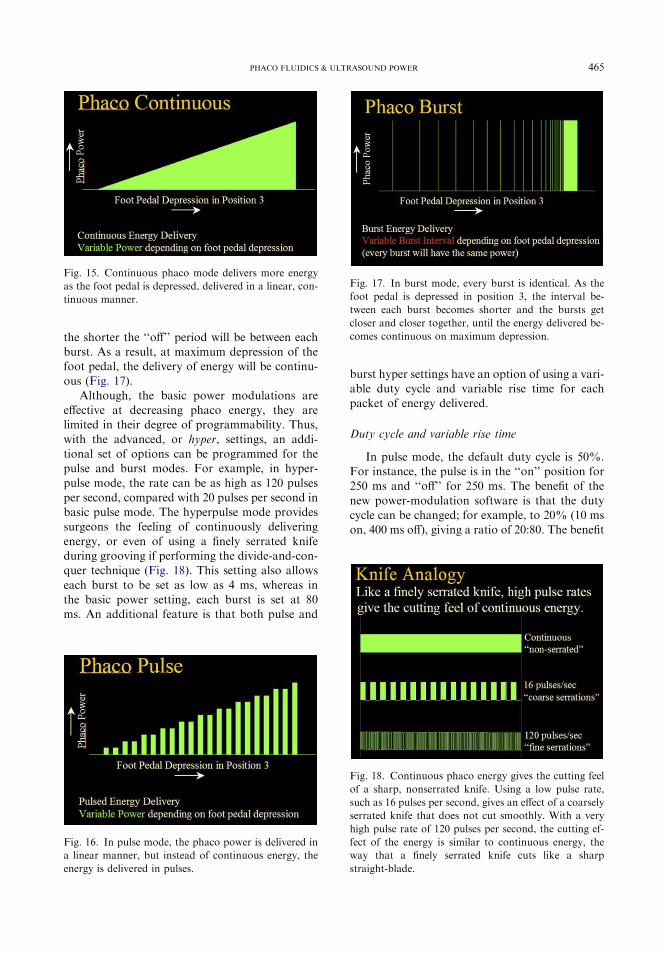
465PHACO FLUIDICS & ULTRASOUND POWER
the shorter the ‘‘off’’ period will be between eachburst. As a result, at maximum depression of thefoot pedal, the delivery of energy will be continu-ous (Fig. 17).
Although, the basic power modulations areeffective at decreasing phaco energy, they arelimited in their degree of programmability. Thus,
with the advanced, or hyper, settings, an addi-tional set of options can be programmed for thepulse and burst modes. For example, in hyper-
pulse mode, the rate can be as high as 120 pulsesper second, compared with 20 pulses per second inbasic pulse mode. The hyperpulse mode providessurgeons the feeling of continuously delivering
energy, or even of using a finely serrated knifeduring grooving if performing the divide-and-con-quer technique (Fig. 18). This setting also allows
each burst to be set as low as 4 ms, whereas inthe basic power setting, each burst is set at 80ms. An additional feature is that both pulse and
Fig. 16. In pulse mode, the phaco power is delivered in
a linear manner, but instead of continuous energy, the
energy is delivered in pulses.
Fig. 15. Continuous phaco mode delivers more energy
as the foot pedal is depressed, delivered in a linear, con-
tinuous manner.
burst hyper settings have an option of using a vari-able duty cycle and variable rise time for each
packet of energy delivered.
Duty cycle and variable rise time
In pulse mode, the default duty cycle is 50%.For instance, the pulse is in the ‘‘on’’ position for250 ms and ‘‘off’’ for 250 ms. The benefit of the
new power-modulation software is that the dutycycle can be changed; for example, to 20% (10 mson, 400 ms off), giving a ratio of 20:80. The benefit
Fig. 17. In burst mode, every burst is identical. As the
foot pedal is depressed in position 3, the interval be-
tween each burst becomes shorter and the bursts get
closer and closer together, until the energy delivered be-
comes continuous on maximum depression.
Fig. 18. Continuous phaco energy gives the cutting feel
of a sharp, nonserrated knife. Using a low pulse rate,
such as 16 pulses per second, gives an effect of a coarsely
serrated knife that does not cut smoothly. With a very
high pulse rate of 120 pulses per second, the cutting ef-
fect of the energy is similar to continuous energy, the
way that a finely serrated knife cuts like a sharp
straight-blade.

466 DEVGAN
of a lower duty cycle is a longer cooling time for thephaco needle, which decreases the amount ofphaco energy delivered into the eye. In addition,
during the ‘‘on’’ time, ultrasound energy is dis-pensed with a jackhammer repulsion effect. Duringthe ‘‘off’’ time, no energy is delivered, and nuclearfragments may be aspirated (Figs. 19 and 20).
With the variable rise-time option, during eachpreset pulse of 250 ms, a 100-ms ramp of in-creasing energy can be set to lead up to the
remaining 150-ms pulse of phaco energy deliv-ered, with cooling periods in between. Again, thebenefits of this option are less energy going into
the eye and a reduction in the repulsive effect ofphacoemulsification that pushes nuclear piecesaway from the phaco tip. Immediately afterward,the surgeon may use higher phaco power to
aspirate the nuclear fragments.
The author’s personal settings in pulse and burstmodes
The author routinely works with three differentphaco machines, one from each of the major
manufacturers. The following settings are appli-cable to all machines and illustrate the fluid andultrasound principles discussed earlier.
To decrease APT and, consequently, endothe-lial damage to the cornea, the author uses thefollowing settings, which lower the phaco powerby approximately 10% to 20% during each
routine case and 20% to 30% during cases ofdense cataracts. In pulse mode, the author sets the
Fig. 19. Decreasing the duty cycle is a way to deliver less
phaco energy and allow for more cooling while keeping
the pulse rate the same (here two pulses per second for
simplicity).
power at 10%, with 50 pulses per second anda 25% duty cycle. Decreasing the duty cycle by upto 40% is not noticeable to the surgeon but candramatically decrease APT. For the vacuum re-
sponse, the author keeps the settings at level 1with a maximum vacuum of 200 and yaw at 250mm Hg using a large-bore 1.1-mm needle. Finally,
the author sets the flow rate at 50 mL/min and thebottle height at 95 cm.
Similarly, in hyperburst mode, the author uses
a power of 5% to 10% and a burst width of 15 to25 ms with an end point of 50% duty cycle. Thevacuum response is level 1, with a maximumvacuum of 200 and yaw of 250 with a flow rate
of 50 mL/min and a bottle height of 95 cm.
Suggested settings for surgeons
First, surgeons should remember to keep thephaco needle and all vacuum and flow levels thesame as usual; no change in surgical technique is
needed. Only the delivery of the phaco power willchange.
If surgeons are accustomed to working in
continuous phaco mode, they will likely have aneasy time starting with a hyperpulse mode at 60 to120 pulses per second, initially at a 50% dutycycle, and using their same maximum phaco
power. This one simple change will likely cut thetotal phaco time and energy in half with no effecton technique.
If surgeons are accustomed to a pulsed phacomode, they will have an easy time staying withinthe same number of pulses per second and keeping
the maximum phaco power the same while de-creasing the duty cycle to 25% to 45%. They canthen implement a variable rise time to further
Fig. 20. Comparison of the ‘‘on’’ time versus ‘‘off’’ time
for different duty cycles.

467PHACO FLUIDICS & ULTRASOUND POWER
decrease the total phaco time and energy andenhance purchasing power and followability.
To program a pulse mode, surgeons can enterthe data in two manners: setting the rates or direct
pulse programming. For example, setting the ratesof 10 pulses per second with a 40% duty cycle willproduce individual pulses, each having an ‘‘on’’
time of 40 ms and an ‘‘off’’ time of 60 ms. Thepulse mode could also be directly programmed tohave an ‘‘on’’ time of 40 ms and an ‘‘off’’ time of
60 ms to achieve the same result (Fig. 21).Phaco chop surgeons will have an easier time
adapting to hyperburst mode. Because the sur-
geon will be controlling the interval betweenidentical bursts through the third position, theyshould keep the maximum phaco power level low.Because the percentage power level cannot be
varied using the foot pedal, setting a maximumlevel of 10% to 30% is advisable. The burst widthshould be kept short, between 10 and 30 ms, and
an end point duty cycle of 50% should be used.Depending on the machine, this may need to beentered as a ‘‘minimum-burst interval,’’ which
should be set equal to the burst width in millisec-onds to achieve the effective end point duty cycleof 50% (Fig. 22).
Further tailoring the settings
To get a customized fit that is appropriate tothe surgical technique, the settings can be fine-
tuned to maximize particular characteristics of thephaco probe.
To increase grooving or cutting power inhyperpulse mode and facilitate nuclear sculpting
Fig. 21. The pulse rate and duty cycle can be pro-
grammed through programming the rates or by directly
programming each specific pulse and rest period. The net
result is the same.
in the divide-and-conquer technique, the dutycycle should be increased to 50% to 75%. This
change alone should be sufficient to help nuclearcutting. If an even bigger boost is desired, thevariable rise times should be removed to return to
square wave forms, and then the maximum phacopower level increased.
Todecrease chatter at the phaco tip and enhance
the removal of nuclear segments, one should keepin mind that the phaco energy is a repulsive forceand therefore the ‘‘on’’ time of the ultrasoundenergy should be decreased. In hyperpulse mode,
this entails increasing the pulse rate, implementinga variable rise time, decreasing the duty cycle to50% or less, and perhaps decreasing maximum
phaco power. In hyperburst mode, ‘‘on’’ time canbe decreased by lessening the burst width andkeeping the end point duty cycle at 50%.
The following options should be considered forcustomized tailoring:
Pulse mode
� Pulse rate (pulses per second)� Duty cycle (ratio of on:off for each pulse)
� Rise time: square waves versus sloped waves� Phaco power (percent of maximum)
Burst mode
� Burst width (milliseconds duration of eachburst)� End point duty cycle (ratio of on:off at the
end of foot position 3)� Rise time: square waves versus sloped waves� Phaco power (percent of maximum)
Fig. 22. Elements of the pulse mode can be combined
with the burst mode by preventing continuous delivery
of ultrasound energy, even with maximum foot pedal de-
pression, through using an end point duty cycle.

468 DEVGAN
Further shaping of the pulses
As software for modulating phaco powerevolves, new methods for further shaping thephaco power pulse are being designed, such as
the concept of a ‘‘micro-punch.’’Creating a microvoid between the occluded
phaco tip and the nuclear material can help betterharness the cavitational effects of phacoemulsifi-
cation. By using a very brief higher-powered‘‘micro-punch’’ of phaco power to repel thenucleus, a microvoid is created that allows fresh
balanced saline solution to flow between thephaco needle and the nuclear piece. The cavitationeffects are accelerated and therefore the efficiency
of the ultrasound power is increased.The major equipment manufacturers are cur-
rently developing more innovations in the delivery
of phaco power, which will allow safer, moreefficient surgery.
The large range of programming options avail-
able with the new power-modulation softwareprovides a personalized fit for every surgeon andevery technique during cataract surgery. Not onlywill surgeons enjoy the flexibility of all the options
but also patients will benefit from significantly lessphaco energy in the eye. Postoperatively, theresults will be clearer corneas, minimal endothelial
damage, and a high degree of patient satisfactionwith each procedure.
Reference
[1] Javitt JC, et al. Geographic variation in utilization of
cataract surgery. Med Care 1995;33(1):90–105.
Ophthalmol Clin N Am 19 (2006) 469–483
New Technology IOL OpticsLiliana Werner, MD, PhD*, Randall J. Olson, MD,
Nick Mamalis, MDJohn A. Moran Eye Center, University of Utah, 50 North Medical Drive, Salt Lake City, UT 84132, USA
Modern cataract surgery is now in the realm ofrefractive surgery and patients expect almost
perfect results. The development and manufactureof intraocular lenses (IOLs) is evolving rapidly.The most energy and funding is probably being
spent on the development of new and complexIOLs that not only restore the refractive power ofthe eye after cataract surgery, but also providespecial features, including multifocality, toric
corrections, pseudoaccommodation, and so forth[1,2]. This article describes some of the new tech-nology regarding materials and designs currently
available or under development for the manufac-ture of modern IOLs.
Multifocal intraocular lenses
Before choosing multifocal IOLs, astigmatismcontrol and precise biometry are required, and
careful patient selection. This is especially impor-tant because of concerns related to the possibilityof a higher incidence of decreased contrast sensi-
tivity and glare with these lenses. Success withmultifocal lenses (and other complex IOLs) is alsodependent on surgical technique: in-the-bag
implantation and appropriate capsulorrhexis arenecessary to ensure good centration, avoid
Supported in part by a grant from Research to
Prevent Blindness, Inc., New York, NY, to the
Department of Ophthalmology and Visual Sciences,
University of Utah. Drs Werner and Mamalis are
members of the scientific advisory board of Visiogen
(Irvine, CA). Dr. Olson is consultant for Advanced
Medical Optics (Santa Ana, CA).
* Corresponding author.
E-mail address: [email protected]
(L. Werner).
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All r
doi:10.1016/j.ohc.2006.07.007
myopic shift, and reduce posterior capsule opaci-fication (PCO).
The Array lens (Advanced Medical Optics,Santa Ana, California) is a three-piece multifocalIOL manufactured from a silicone material hav-
ing a refractive index of 1.46 (Fig. 1). It has angu-lated ‘‘C’’ haptics made of extruded polymethylmethacrylate. It is the first multifocal IOL ap-proved by the Food and Drug Administration
(FDA). The optical design of this lens is azonal-progressive multifocal optic with five con-centric zones. This lens design is a distance-domi-
nant, zonal progressive optic. The center of thelens is primarily for distance. All of the otherzones have distance and near in different propor-
tions (50% of the available light is devoted to dis-tance vision, 13% to intermediate vision, and 37%to near vision). No available light is lost in the lens
because the optic is refractive and not diffractive.The addition for near is þ3.5 diopters (D). TheIOL is available from þ6 to þ30 D in 0.5-D steps.
Javitt and coworkers [3] compared bilateral
implantation of the Array lens with a monofocallens with respect to visual function, patient satis-faction, and quality of life. They found that those
patients who had bilateral implantation of theArray obtained better uncorrected and distance-corrected near visual acuities and reported better
overall vision, less limitation in visual function,and less spectacle dependency than patients withbilateral monofocal lenses. In the study bySchmitz and coworkers [4] reduced contrast sensi-
tivity was found in the multifocal group (also im-planted with the Array) only at the lowest spatialfrequency without halogen glare. The monofocal
and multifocal groups of patients studied bythem had no statistically significant differences incontrast sensitivity with moderate and strong
ights reserved.
ophthalmology.theclinics.com
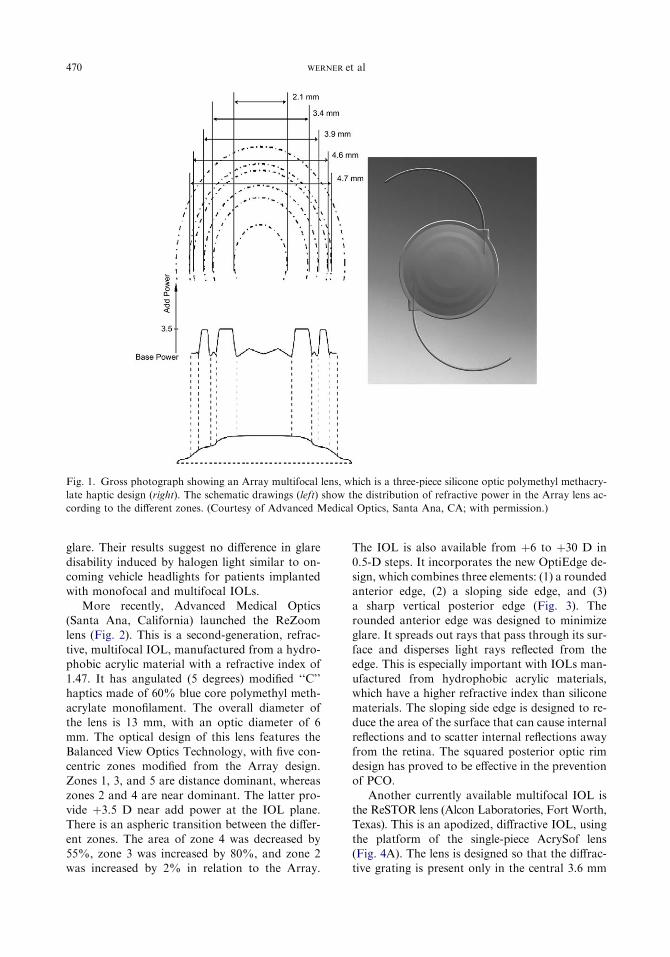
470 WERNER et al
Fig. 1. Gross photograph showing an Array multifocal lens, which is a three-piece silicone optic polymethyl methacry-
late haptic design (right). The schematic drawings (left) show the distribution of refractive power in the Array lens ac-
cording to the different zones. (Courtesy of Advanced Medical Optics, Santa Ana, CA; with permission.)
glare. Their results suggest no difference in glare
disability induced by halogen light similar to on-coming vehicle headlights for patients implantedwith monofocal and multifocal IOLs.
More recently, Advanced Medical Optics(Santa Ana, California) launched the ReZoomlens (Fig. 2). This is a second-generation, refrac-
tive, multifocal IOL, manufactured from a hydro-phobic acrylic material with a refractive index of1.47. It has angulated (5 degrees) modified ‘‘C’’haptics made of 60% blue core polymethyl meth-
acrylate monofilament. The overall diameter ofthe lens is 13 mm, with an optic diameter of 6mm. The optical design of this lens features the
Balanced View Optics Technology, with five con-centric zones modified from the Array design.Zones 1, 3, and 5 are distance dominant, whereas
zones 2 and 4 are near dominant. The latter pro-vide þ3.5 D near add power at the IOL plane.There is an aspheric transition between the differ-
ent zones. The area of zone 4 was decreased by55%, zone 3 was increased by 80%, and zone 2was increased by 2% in relation to the Array.
The IOL is also available from þ6 to þ30 D in
0.5-D steps. It incorporates the new OptiEdge de-sign, which combines three elements: (1) a roundedanterior edge, (2) a sloping side edge, and (3)
a sharp vertical posterior edge (Fig. 3). Therounded anterior edge was designed to minimizeglare. It spreads out rays that pass through its sur-
face and disperses light rays reflected from theedge. This is especially important with IOLs man-ufactured from hydrophobic acrylic materials,which have a higher refractive index than silicone
materials. The sloping side edge is designed to re-duce the area of the surface that can cause internalreflections and to scatter internal reflections away
from the retina. The squared posterior optic rimdesign has proved to be effective in the preventionof PCO.
Another currently available multifocal IOL isthe ReSTOR lens (Alcon Laboratories, Fort Worth,Texas). This is an apodized, diffractive IOL, using
the platform of the single-piece AcrySof lens(Fig. 4A). The lens is designed so that the diffrac-tive grating is present only in the central 3.6 mm

471NEW TECHNOLOGY IOL OPTICS
Fig. 2. Gross photograph showing a ReZoom multifocal lens, which is a three-piece hydrophobic acrylic optic poly-
methyl methacrylate haptic design (right). The schematic drawings (left) show the distribution of refractive power in
the ReZoom lens according to the different zones. (Courtesy of Advanced Medical Optics, Santa Ana, CA; with
permission.)
of the optic. Apodization is the gradual tapering
of the diffractive steps from the center to the pe-riphery. The largest diffractive step is at the lenscenter and sends most of the light to a near focus.
As the steps move away from the center, theygradually decrease in size, blending into the
periphery, and sending a decreasing proportion
of light to a near focus. As a result of this design,when the pupil is small, such as during readingtasks, the lens provides appropriate near and dis-
tance vision. In large pupil situations, however,such as at night, the ReSTOR lens becomes
Fig. 3. Scanning electron microscopy showing the characteristics of the OptiEdge design, incorporated in the ReZoom
lens. (Courtesy of Advanced Medical Optics, Santa Ana, CA; with permission.)
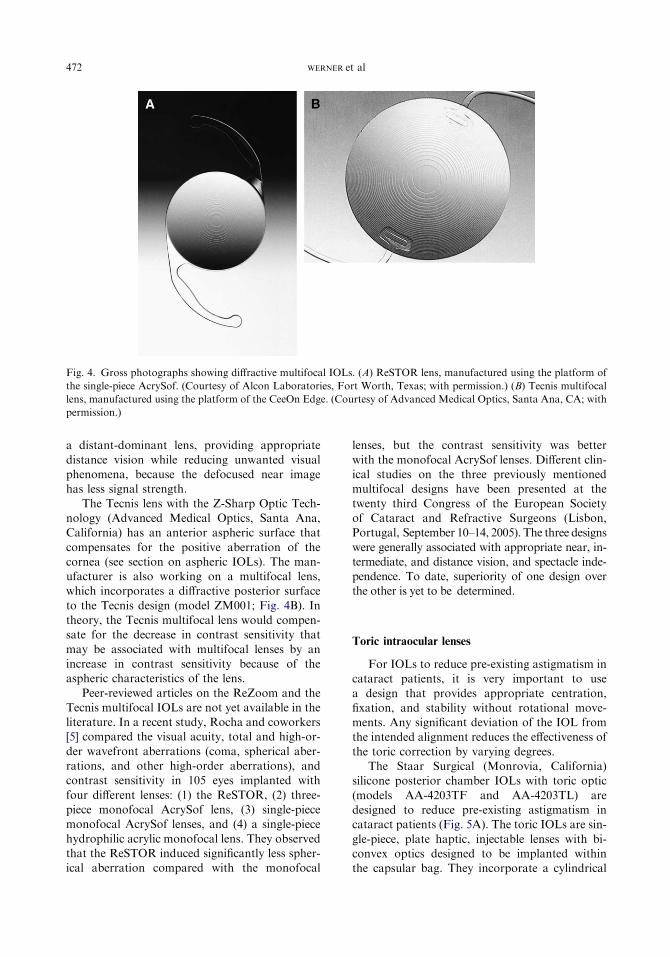
472 WERNER et al
Fig. 4. Gross photographs showing diffractive multifocal IOLs. (A) ReSTOR lens, manufactured using the platform of
the single-piece AcrySof. (Courtesy of Alcon Laboratories, Fort Worth, Texas; with permission.) (B) Tecnis multifocal
lens, manufactured using the platform of the CeeOn Edge. (Courtesy of Advanced Medical Optics, Santa Ana, CA; with
permission.)
a distant-dominant lens, providing appropriate
distance vision while reducing unwanted visualphenomena, because the defocused near imagehas less signal strength.
The Tecnis lens with the Z-Sharp Optic Tech-nology (Advanced Medical Optics, Santa Ana,California) has an anterior aspheric surface that
compensates for the positive aberration of thecornea (see section on aspheric IOLs). The man-ufacturer is also working on a multifocal lens,which incorporates a diffractive posterior surface
to the Tecnis design (model ZM001; Fig. 4B). Intheory, the Tecnis multifocal lens would compen-sate for the decrease in contrast sensitivity that
may be associated with multifocal lenses by anincrease in contrast sensitivity because of theaspheric characteristics of the lens.
Peer-reviewed articles on the ReZoom and theTecnis multifocal IOLs are not yet available in theliterature. In a recent study, Rocha and coworkers[5] compared the visual acuity, total and high-or-
der wavefront aberrations (coma, spherical aber-rations, and other high-order aberrations), andcontrast sensitivity in 105 eyes implanted with
four different lenses: (1) the ReSTOR, (2) three-piece monofocal AcrySof lens, (3) single-piecemonofocal AcrySof lenses, and (4) a single-piece
hydrophilic acrylic monofocal lens. They observedthat the ReSTOR induced significantly less spher-ical aberration compared with the monofocal
lenses, but the contrast sensitivity was better
with the monofocal AcrySof lenses. Different clin-ical studies on the three previously mentionedmultifocal designs have been presented at the
twenty third Congress of the European Societyof Cataract and Refractive Surgeons (Lisbon,Portugal, September 10–14, 2005). The three designs
were generally associated with appropriate near, in-termediate, and distance vision, and spectacle inde-pendence. To date, superiority of one design overthe other is yet to be determined.
Toric intraocular lenses
For IOLs to reduce pre-existing astigmatism incataract patients, it is very important to use
a design that provides appropriate centration,fixation, and stability without rotational move-ments. Any significant deviation of the IOL fromthe intended alignment reduces the effectiveness of
the toric correction by varying degrees.The Staar Surgical (Monrovia, California)
silicone posterior chamber IOLs with toric optic
(models AA-4203TF and AA-4203TL) aredesigned to reduce pre-existing astigmatism incataract patients (Fig. 5A). The toric IOLs are sin-
gle-piece, plate haptic, injectable lenses with bi-convex optics designed to be implanted withinthe capsular bag. They incorporate a cylindrical

473NEW TECHNOLOGY IOL OPTICS
Fig. 5. Toric IOLs. (A) Gross photograph showing the Staar toric lens, which is a single-piece silicone plate design, with
large fixation holes. (B) Gross photograph showing the AcrySof toric. (Courtesy of Alcon Laboratories, Fort Worth,
TX; with permission.)
correction with a spherical optic to create a toriclens. The toric IOL has an overall diameter of10.8 mm in the TF version and of 11.2 mm in
the TL version to fit in different size capsularbags. Large fenestration holes are created to allowfibrous tissue to grow through them and lock the
lens to the equator of the capsular bag for addi-tional stability. These IOLs are available inpowers from þ4 to þ35 D, in 0.5-D increments.
The cylindrical powers of the IOLs are of 2 and3.5 D in the long axis of the lens. The cylindricalpower of the toric IOLs at the corneal plane for
a 2-D lens is about 1.4 D, and about 2.3 D forthe 3.5-D IOL.
Patel and coworkers [6] compared the postop-erative rotation of plate- and loop-haptic implants
of spherical power to ascertain the optimal designappropriate for toric lenses. Severe early rotation(up to 2 weeks after surgery) was observed in
24% of plate-haptic lenses, compared with 9%for loop-haptic lenses. Rotation observed between2 weeks and 6 months after implantation was less
common, however, with plate-haptic lenses.Chang [7] demonstrated that adequate overalllength is a critical factor in the rotational stabilityof plate-haptic lenses, and early rotational stabil-
ity is enhanced by use of longer IOLs.Another toric lens recently approved and
available is Alcon’s model SA60TT, using the
platform of the single-piece AcrySof IOL (AlconLaboratories, Fort Worth, Texas; Fig. 5B). Thisdesign has been chosen because of its reported
great stability within the capsular bag, and with-out significant postoperative rotation. TheSA60TT is available in three models: (1) 1.50 D
(SA60T3); (2) 2.25 D (SA60T4); or (3) 3 D(SA60T5) of cylindrical correction at the IOLplane. The IOLs feature three alignment marks
on each side of the lens to assist with axis orienta-tion. The toric component is present on the poste-rior optic surface of the lens. Implantation is also
performed by injection with the Monarch II sys-tem. Horn [8] has recently presented the resultsof a multicenter, randomized study comparing
the SA60TT with the AcrySof single-piece plat-form. Eligibility criteria for the study includedadults aged 21 years or older, age-related cataracts
in one or both eyes, minimum astigmatism criteriaper protocol, potential postoperative visual acuityof 0.3 logMAR or better, and preoperative visual
acuity worse than 0.2 logMAR with or withoutglare. Clinical outcomes indicated a significant re-duction in the postoperative residual refractivecylinder in subjects implanted with the investiga-
tional AcrySof toric versus the spherical control.
Blue blocking intraocular lenses
The natural human crystalline lens yellows
with age, which is attributable to oxidationproducts of tryptophan and to glycosylation oflens proteins. This change results in a progressive
increase in absorbance within the blue range ofthe visible spectrum [9]. Studies suggest that blue-light absorbing IOLs, by replicating the transmis-sion characteristics of the aging crystalline lens,
protect lipofuscin-containing retinal pigment epi-thelial cells from blue-light damage. There is indi-rect evidence showing that this may result in
a reduction of the risk for macular degeneration,or its progression [10].
The AcrySof Natural (SN60AT) provides in-
cremental light protection above and beyondtraditional UV protection. This technology isincorporated into the platform of the single-piece

474 WERNER et al
AcrySof. It contains a proprietary, integratedpolymer dye (blue light–filtering chromophore,ImprUV) designed to filter both invisible UV rays
and visible blue rays of light. The addition ofa covalently bonded yellow dye results in an IOLUV-visible light transmittance curve that mimicsthe protection provided by the natural, precatar-
actous adult human crystalline lens [11]. Althoughthe traditional UV-absorbing lenses provide lightfiltration from 200 to 400 nm, the AcrySof Natu-
ral lens provides variable filtration propertiesfrom 200 to 550 nm.
Possible limitations associated with implanta-
tion of these yellow IOLs include the potentialimpact on color and night vision. Althoughdifferent studies did not demonstrate any effectof yellow-tinted IOLs on color vision [12], the is-
sue of night vision remains controversial [13].Blue light is more important for scotopic (night-time) than photopic (daytime) vision. With age,
scotopic sensitivity declines twice as fast as doesphotopic sensitivity. Night vision is a major prob-lem for older adults. Cataract surgery with im-
plantation of standard UV absorbing (clear)IOLs has the potential to improve night visionfor these patients.
Scotopic and photopic luminous efficienciespeak at 507 nm (blue-green) and 555 nm (green-yellow), respectively. In addition to blockingharmful 330- to 400-nm UV radiation, a þ20-DAcrySof Natural also blocks 50% of blue light at450 nm and 25% at 480 nm. According toMainster [13], this is enough to decrease rod-me-
diated visual sensitivity, although the clinical sig-nificance of this fact remains to be demonstratedin clinical studies.
A different approach to the possible associationbetween blue light and macular degeneration isbeing investigated by Medennium (Irvine, Califor-nia), with the development of a new IOL with
photochromic properties [14]. According to themanufacturer, the lens has a UV–near blue absorp-tion curve similar to theAcrySofNatural lens when
exposed to UV light, whereas it behaves as a stan-dard UV-absorbing IOL in an indoor or night en-vironment. The lens optic changes from colorless
to yellow when exposed to UV light, and back tocolorless in indoor environments. The SmartYel-low IOL ismanufacturedwith a proprietary hydro-
phobic acrylic material (photochromic matrix).The preliminary design is a three-piece lens withblue-colored polyvinylidene fluoride haptics. Theoverall diameter of the lens is 12.5 mm, with a
6-mm optic. The lens has a 5-degree posterior
optic-haptic angulation, and square optic edges.The authors have recently investigated this lens inthe laboratory, in vitro and in vivo. They found
the photochromic change to be reversible, repro-ducible, and stable over time, and the lens biocom-patible in rabbits after a 6-month follow-up period.This approach would put an end to the controversy
regarding the impact of yellow lenses on nightvision.
Accommodative intraocular lenses
IOLs proposed to restore accommodationhave initially been designed to do so by enabling
a forward movement of the optic componentduring an accommodation effort. The Eyeonics(Aliso Viejo, California) CrystaLens (model AT-45) is a modified plate haptic lens manufactured
from a third-generation silicone material (Biosil)with a refractive index of 1.43 [15]. The design ofthe lens was developed by Dr. J. Stuart Cumming
(Fig. 6). It is hinged adjacent to the optic and hassmall looped polyimide haptics, which have beenshown to fixate firmly in the capsular bag. The
grooves across the plates adjacent to the opticmake the junction of the optic with the plate hap-tic the most flexible part of the optic-haptic de-
sign. The overall length of the lens is 11.5 mm(loop tip to loop tip measurement), whereas theoverall length as measured from the ends of theplate haptics is 10.5 mm. The optic is biconvex
and is 4.5 mm in diameter; the recommendedA constant is 119.24, and the lens is designed forplacement in the capsular bag. The theoretical
mechanism of efficacy of this lens is based onthe concept that with accommodative effort, redis-tribution of the ciliary body mass results in in-
creased vitreous pressure, which moves the opticforward anteriorly within the visual axis, creatinga more plus-powered lens. One drop of atropine
administered at the time of the surgery and onedrop on the first day after surgery allows thelens to remain in the maximal posterior positionwithin the capsular bag and not move forward
during the period of fibrosis around the lens hap-tics. This should result in a greater potential forforward movement of the lens on ciliary body
constriction. The hinge was incorporated to facil-itate the forward movement of the optic by mini-mizing the resistance to the possible pressure
exerted on the lens by the forward movement ofthe vitreous body on contraction of the ciliarymuscle.

475NEW TECHNOLOGY IOL OPTICS
The Crystalens received FDA approval inNovember 2003 for the claim of adding approxi-mately 1 D of accommodation over monofocal
lenses. Different studies, however, could not dem-onstrate a correlation between the objective mea-surement of the anterior shift of the Crystalens and
the reported near vision of the patients [16,17]. Insome cases, a backward shift of the lens was ob-served. It is likely that pseudoaccommodation, be-cause of such factors as an increased depth of focus,
may play a significant role in the reading perfor-mance of patients implanted with this lens design.
Theoretical studies using model eyes demon-
strated that dual-optic IOL systems may representan advantage over mono-optic systems in terms ofamplitude of accommodation obtained with optic
movement during efforts for accommodation[18,19]. This seems to be particularly valid if thereis anterior translation of the anterior optic with anunchanged position of the posterior optic. The
Synchrony IOL (Visiogen, Irvine, California) isa one-piece lens manufactured from silicone [20].
Fig. 6. Photographs of the CrystaLens (Eyeonics, Aliso
Viejo, California). (A) Gross photograph. (B) Clinical
picture (retroillumination) of a patient implanted with
the CrystaLens. (Courtesy of John F. Doane, MD,
Kansas City, MO.)
The lens has two major optic components (ante-rior and posterior) connected by a bridge throughthe haptics, which act like a spring. The posterioraspect of the device is designed with a significantly
larger surface area than the anterior, to maintainstability within the capsular bag during the ac-commodation-relaxation process. The anterior
optic has two expansions oriented parallel to thehaptic component that lift the capsulorrhexisedge, preventing complete contact of the anterior
capsule with the anterior surface of the lens. Inthis dual optic lens system the anterior lens hasa high plus power beyond that required to pro-
duce emmetropia, whereas the posterior lens hasa minus power to return the eye to emmetropia.The lens is designed to work in concert with thecapsular bag, according to the traditional Helm-
holtz’s theory of accommodation. The distancebetween the two optics is stated to be minimumin the unaccommodated state and maximum in
the accommodated state, with anterior displace-ment of the anterior optic (Fig. 7).
Studies performed in the authors’ laboratory
using rabbits demonstrated that significantly lessanterior capsule opacification and PCO wereobserved in rabbit eyes after implantation of the
Synchrony lens in comparison with plate hapticsilicone lenses [21]. The presence of two IOL op-tics in the capsular bag raises concerns related tothe possibility of ingrowth of regenerative-prolif-
erative crystalline lens material between them,with formation of interlenticular opacification.This issue was also addressed in the authors’ lab-
oratory, by using a rabbit model. They demon-strated that interlenticular opacification wassignificantly associated with pairs of hydrophobic
acrylic lenses implanted in the bag, but not withthe Synchrony [22]. This same study seemed toconfirm clinical observations that implantationof two silicone plate lenses in the bag is not asso-
ciated with interlenticular opacification. The Syn-chrony is currently under clinical trials overseas.Since the last quarter of 2005, it is being implanted
through a 3.6- to 3.8-mm incision, by using a pre-loaded injector that only requires balanced salt so-lution for IOL lubrication. In a recently reported
series of 24 patients implanted with this lens,100% of them had a distance-corrected near vi-sion of 20/40 or better. Defocus curve analysis
showed a mean accommodative range of 2.83 �0.16 D [23].
Another dual-optical accommodating IOL sys-tem was invented by Dr. Faezeh M. Sarfarazi, and
it is now being developed by Bausch and Lomb
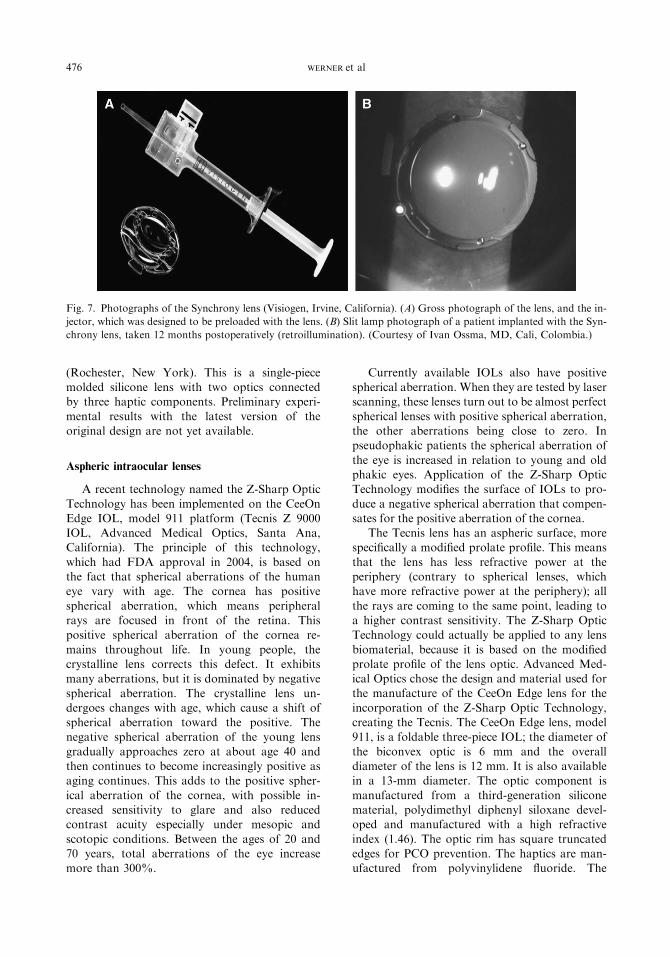
476 WERNER et al
Fig. 7. Photographs of the Synchrony lens (Visiogen, Irvine, California). (A) Gross photograph of the lens, and the in-
jector, which was designed to be preloaded with the lens. (B) Slit lamp photograph of a patient implanted with the Syn-
chrony lens, taken 12 months postoperatively (retroillumination). (Courtesy of Ivan Ossma, MD, Cali, Colombia.)
(Rochester, New York). This is a single-piecemolded silicone lens with two optics connectedby three haptic components. Preliminary experi-
mental results with the latest version of theoriginal design are not yet available.
Aspheric intraocular lenses
A recent technology named the Z-Sharp Optic
Technology has been implemented on the CeeOnEdge IOL, model 911 platform (Tecnis Z 9000IOL, Advanced Medical Optics, Santa Ana,California). The principle of this technology,
which had FDA approval in 2004, is based onthe fact that spherical aberrations of the humaneye vary with age. The cornea has positive
spherical aberration, which means peripheralrays are focused in front of the retina. Thispositive spherical aberration of the cornea re-
mains throughout life. In young people, thecrystalline lens corrects this defect. It exhibitsmany aberrations, but it is dominated by negative
spherical aberration. The crystalline lens un-dergoes changes with age, which cause a shift ofspherical aberration toward the positive. Thenegative spherical aberration of the young lens
gradually approaches zero at about age 40 andthen continues to become increasingly positive asaging continues. This adds to the positive spher-
ical aberration of the cornea, with possible in-creased sensitivity to glare and also reducedcontrast acuity especially under mesopic and
scotopic conditions. Between the ages of 20 and70 years, total aberrations of the eye increasemore than 300%.
Currently available IOLs also have positivespherical aberration. When they are tested by laserscanning, these lenses turn out to be almost perfect
spherical lenses with positive spherical aberration,the other aberrations being close to zero. Inpseudophakic patients the spherical aberration of
the eye is increased in relation to young and oldphakic eyes. Application of the Z-Sharp OpticTechnology modifies the surface of IOLs to pro-
duce a negative spherical aberration that compen-sates for the positive aberration of the cornea.
The Tecnis lens has an aspheric surface, morespecifically a modified prolate profile. This means
that the lens has less refractive power at theperiphery (contrary to spherical lenses, whichhave more refractive power at the periphery); all
the rays are coming to the same point, leading toa higher contrast sensitivity. The Z-Sharp OpticTechnology could actually be applied to any lens
biomaterial, because it is based on the modifiedprolate profile of the lens optic. Advanced Med-ical Optics chose the design and material used forthe manufacture of the CeeOn Edge lens for the
incorporation of the Z-Sharp Optic Technology,creating the Tecnis. The CeeOn Edge lens, model911, is a foldable three-piece IOL; the diameter of
the biconvex optic is 6 mm and the overalldiameter of the lens is 12 mm. It is also availablein a 13-mm diameter. The optic component is
manufactured from a third-generation siliconematerial, polydimethyl diphenyl siloxane devel-oped and manufactured with a high refractive
index (1.46). The optic rim has square truncatededges for PCO prevention. The haptics are man-ufactured from polyvinylidene fluoride. The

477NEW TECHNOLOGY IOL OPTICS
haptic design is a cap C with a 90-degree exit andan angulation of 6 degrees. As is standard withmodern IOLs, the Tecnis has an incorporated UVabsorber (benzotriazole) to protect the retina
from radiation in the 300- to 400-nm range. Anacrylic platform based on the Advanced MedicalOptics AR40e (Sensar) is also available.
The haptic design is intended to maintain theshape of the capsular bag offering more clockhours of contact between the haptics and the
capsule. These characteristics help in the pre-vention of lens decentration and tilt in cases ofcapsular bag contraction. This is very important
because, qualitatively, any aberration correction issensitive to decentration and tilt. Patients benefitfrom the advanced technology of Tecnis withinthe normal clinical limits of lens decentration less
than 0.4 mm and lens tilt less than 7 degrees.The Tecnis is typical of IOLs developed with
the help of wavefront technology. Corneal ante-
rior surface shapes of different patients weremeasured and used to determine the wavefrontaberration of each cornea. These were then used
to design a model cornea to reproduce the averagespherical aberration found in the patients evalu-ated. An IOL having negative spherical aberration
was designed to compensate for the averagepositive spherical aberration of the model cornea.
In recently published studies comparing Tecniswith a standard three-piece hydrophobic acrylic
lens with posterior square optic edge (AR40e,Advanced Medical Optics, Santa Ana, Califor-nia), Packer and coworkers [24,25] demonstrated
that the modified prolate IOL surface has the po-tential to improve contrast sensitivity under bothmesopic and photopic conditions. Mester and co-
workers [26] evaluated 45 patients with bilateralcataract implanted with the Tecnis lens in oneeye, and a three-piece silicone lens (SI40, Ad-vanced Medical Optics, Santa Ana, California)
in the other. Their clinical results confirmed thetheoretical preclinical calculations that the spher-ical aberration of the eye after cataract surgery
can be eliminated by modifying the anterior sur-face of the IOL. Kershner [27] demonstratedthat Tecnis provided a significant improvement
in retinal image contrast and visual performancemeasured by visual acuity and functional acuitycontrast testing in 221 eyes of 156 patients. This
improvement was greatest in night vision andnight vision with glare compared with the perfor-mance of conventional spherical silicone(AA4207VF, Staar Surgical) and hydrophobic
acrylic (SA60AT, Alcon) lenses. Finally, in a study
comparing patients implanted with the Tecnis orthe single-piece AcrySof (SA60AT), Bellucci andcoworkers [28] demonstrated significantly betterdistance contrast sensitivity with the aspheric lens.
The AcrySof aspheric (model SN60WF), man-ufactured by using the platform of the single-pieceAcrySof, is also a negative spherical aberration
lens. As with the Tecnis, the goal of the SN60WFlens is to counteract the mean spherical aberrationin the cataract patient population, so that the
resulting total spherical aberration of the eye iszero. Although the Tecnis lens accomplishes thiswith a modified anterior prolate surface, the
SN60WF has an aspheric posterior surface.The SofPort Advanced Optics (AO) (model
LI61AO), manufactured by Bausch and Lomb(Rochester, New York), is a three-piece silicone
lens. The optic material has a refractive index of1.43, and the modified C loops are made ofpolymethyl methacrylate. The lens has an overall
diameter of 13 mm, with an optic diameter of6 mm, and a 5-degree posterior optic-hapticangulation. The SofPort AO also incorporated
square optic edges, for PCO prevention. Bothanterior and posterior optic surfaces of this lensare aspheric, with uniform power from the center
to the edge. In contrast to the previous twoaspheric designs, the SofPort AO does not addnegative spheric aberration to the eye, but it isaberration free. In theory, this means that the
SofPort AO may improve vision over standardIOLs for all patients, including the estimated 5%to 7% who do not have any or minimal positive
corneal spherical aberration. Also, in case ofdecentration, the lens would not induce otheraberrations as negative-aberration and spherical
IOLs may do. This last fact was verified in a recentin vitro study [29]. A ray-tracing program wasused to evaluate the effect of IOL decentrationon the optical performance of three silicone
IOLs: (1) the LI61U (Bausch and Lomb); (2) theTecnis; and (3) the SofPort AO. The optical per-formance of the model eye was not affected by de-
centration of the SofPort AO lens. Withdecentration, the performance of this new IOLwas better than with the conventional spherical
LI61U and the Tecnis.
Intraocular lenses for very small incisions
The advent of microincision surgical tech-niques rendered cataract removal through clearcorneal incisions as small as 1 mm possible. The

478 WERNER et al
natural consequence of this advance is the de-velopment of IOLs that can be inserted throughsuch small incisions. One of the recently devel-
oped lenses that can be inserted through a sub2-mm incision (1.45-mm) is the UltraChoice 1.0Rollable ThinLens (ThinOptX, Abingdon, Vir-ginia) IOL (Fig. 8). It is manufactured from a hy-
drophilic acrylic material with 18% water content.The refractive index of the material is 1.47. The di-optric power of this lens ranges from�25 toþ25D.
The optical thickness is 300 to 400mm,with a bicon-vex optical configuration having a meniscus shape.The overall diameter of the lens is 11.2 mm, and the
optical diameter is 5.5 mm [30].The ultrathin properties of the lens are attrib-
utable to its optical design. The optic featuresthree to five concentric optical zones with steps of
50 mm. Each Fresnel-like ring or segment of thelens has a small change in the radius to correct forspherical aberration. The difference in radius is
Fig. 8. Photographs of the UltraChoice lens. (A) Gross
photograph showing its optic steps. (B) Clinical picture
obtained through an operating microscope, showing in-
jection of the lens through a 1.45-mm incision, using the
new roller-injector system. The lens unrolls in 20 seconds
once injected into the eye. (Courtesy of ThinOptX,
Abingdon, VA; with permission.)
stated to ensure that each ring of the lens focuseslight at nearly the same point as the primemeridian. According to the manufacturer, by
making the lens thinner, other aberrations, suchas coma, and the potential for distortion and glareare reduced. The four tips of the haptic compo-nent have a thickness of 50 mm. They are stated to
roll once in the capsular bag, absorbing capsularcontraction forces, an issue that still needs to beaddressed in long-term clinical studies. The edge
of the lens is also 50-mm thick, which is stated toreduce the potential for halos and glare. Theteardrop-shaped holes in the haptic component
should point in a clockwise direction. A speciallydesigned roller-injector system with an autoclav-able, reusable cartridge made of Teflon is nowavailable for this lens.
In the first clinical studies involving this lensdesign, many of the patients presented with betterthan expected near vision. It has been hypothe-
sized that the thin nature of this design providesincreased amplitude of pseudoaccommodation,which will be further investigated. One explana-
tion could be that the thin lens is associated withincreased depth of field. Another possibility is thatthe lens moves with the capsular bag during
efforts for accommodation, because it is thin andlight, and exerts little force against the equator. Ina recently published, prospective, clinical study,16 eyes of eight patients implanted with the
UltraChoice were compared with 20 eyes of 10patients implanted with a three-piece AcrySof(MA60BM) lens [31]. The UltraChoice lens pro-
vided better best-corrected near and distancevisual acuities, and significantly higher contrastacuities than the control lens. Alio and coworkers
[32] evaluated the modulation-transfer function ineyes implanted with a conventional IOL (AcrySofMA60BM) and the UltraChoice. This lattershowed excellent modulation-transfer function
performance when implanted after cataract sur-gery, equal to the conventional lens. At this timeit is uncertain whether the company has the finan-
cial resources to continue development of thislens.
A new concept of very-small-incision IOLs is
being developed at Medennium and is called theSmartIOL (Fig. 9). This lens uses a thermody-namic hydrophobic acrylic material that is pack-
aged as a solid rod approximately 30 mm longand 2 mm wide. The refractive index of the mate-rial is 1.47, and the softening temperature is 20�Cto 30�C. When implanted through a small inci-
sion, body temperature transforms the solid rod

479NEW TECHNOLOGY IOL OPTICS
Fig. 9. (A–D) Gross photographs of a human eye obtained postmortem (posterior view) implanted with a prototype of
the single-piece SmartIOL. The rod gradually transformed into a full size lens, after instillation of balanced salt solution
at body temperature.
into a soft gel-like material, which has the shape
of a full-sized biconvex lens that completely fillsthe capsule. The entire transformation takes about30 seconds and results in a lens about 9.5 mm
wide and from2 to 4mmthick (but averaging about3.5mm) at the center, depending ondioptric power.The lens is highly flexible, more closely resembling
a gel, and it recovers its full shape when not com-pressed. Before being formed into a rod, the precisedioptric power and dimensions that the trans-formed material takes on thermal activation in
the eye can potentially be imprinted.Besides being implanted through a very small
incision, another potential advantage is to restore
accommodation. By combining a full-sized opticwith a very flexible material, Medennium scien-tists hope to be able to mimic the accommodative
action of the young, natural lens and achievea larger potential accommodation than otheroptical-mechanical designs, according to the clas-
sical Helmholtz theory. Also, complete filling ofthe capsular bag eliminates space for cell growth.The hydrophobic acrylic material of this lens
exhibits high tackiness, which might promote its
attachment to the capsular bag, further enhancingPCO prevention. A new design of this lens is beingdeveloped, which is a three-piece lens with poly-
vinylidene fluoride haptics. This will probablyeliminate potential problems related to the differ-ent diameters of the capsular bags in different
eyes.
Light adjustable lens
Calhoun Vision (Pasadena, California) is de-veloping a three-piece silicone lens with photo-
sensitive silicone subunits, which move within thelens on fine tuning with a low-intensity beam ofnear-UV light (light adjustable lens [LAL]). The
refractive power of the lens can be adjustednoninvasively after implantation to give thepatient a definitive refraction [33–35]. The LAL
is a foldable three-piece lens; the diameter of thebiconvex optic is 6 mm and the overall diameterof the lens is 13 mm. The optic component is
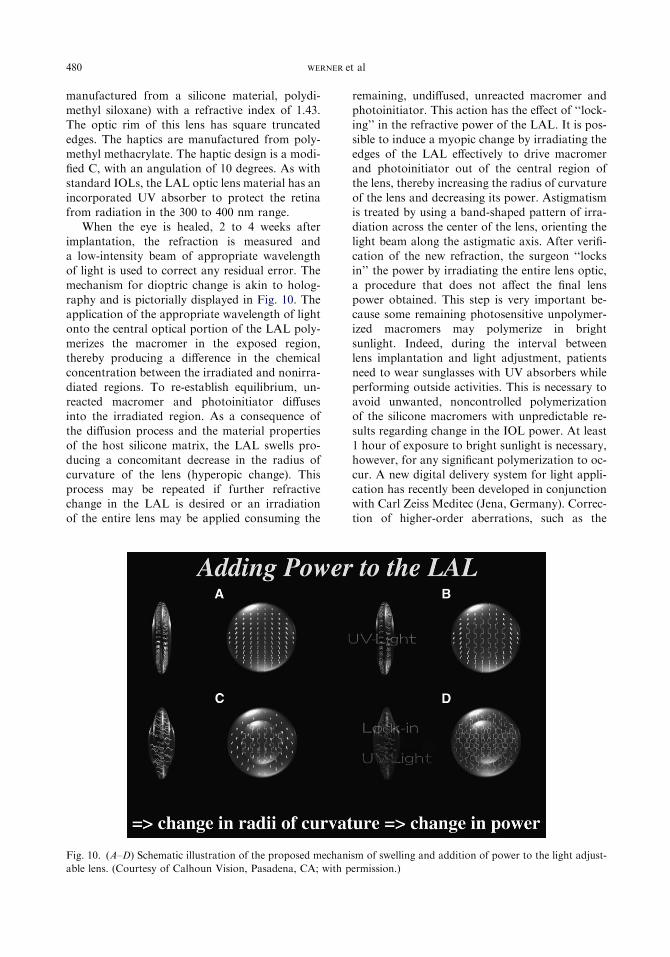
480 WERNER et al
manufactured from a silicone material, polydi-methyl siloxane) with a refractive index of 1.43.The optic rim of this lens has square truncated
edges. The haptics are manufactured from poly-methyl methacrylate. The haptic design is a modi-fied C, with an angulation of 10 degrees. As withstandard IOLs, the LAL optic lens material has an
incorporated UV absorber to protect the retinafrom radiation in the 300 to 400 nm range.
When the eye is healed, 2 to 4 weeks after
implantation, the refraction is measured anda low-intensity beam of appropriate wavelengthof light is used to correct any residual error. The
mechanism for dioptric change is akin to holog-raphy and is pictorially displayed in Fig. 10. Theapplication of the appropriate wavelength of lightonto the central optical portion of the LAL poly-
merizes the macromer in the exposed region,thereby producing a difference in the chemicalconcentration between the irradiated and nonirra-
diated regions. To re-establish equilibrium, un-reacted macromer and photoinitiator diffusesinto the irradiated region. As a consequence of
the diffusion process and the material propertiesof the host silicone matrix, the LAL swells pro-ducing a concomitant decrease in the radius of
curvature of the lens (hyperopic change). Thisprocess may be repeated if further refractivechange in the LAL is desired or an irradiationof the entire lens may be applied consuming the
remaining, undiffused, unreacted macromer andphotoinitiator. This action has the effect of ‘‘lock-ing’’ in the refractive power of the LAL. It is pos-
sible to induce a myopic change by irradiating theedges of the LAL effectively to drive macromerand photoinitiator out of the central region ofthe lens, thereby increasing the radius of curvature
of the lens and decreasing its power. Astigmatismis treated by using a band-shaped pattern of irra-diation across the center of the lens, orienting the
light beam along the astigmatic axis. After verifi-cation of the new refraction, the surgeon ‘‘locksin’’ the power by irradiating the entire lens optic,
a procedure that does not affect the final lenspower obtained. This step is very important be-cause some remaining photosensitive unpolymer-ized macromers may polymerize in bright
sunlight. Indeed, during the interval betweenlens implantation and light adjustment, patientsneed to wear sunglasses with UV absorbers while
performing outside activities. This is necessary toavoid unwanted, noncontrolled polymerizationof the silicone macromers with unpredictable re-
sults regarding change in the IOL power. At least1 hour of exposure to bright sunlight is necessary,however, for any significant polymerization to oc-
cur. A new digital delivery system for light appli-cation has recently been developed in conjunctionwith Carl Zeiss Meditec (Jena, Germany). Correc-tion of higher-order aberrations, such as the
Fig. 10. (A–D) Schematic illustration of the proposed mechanism of swelling and addition of power to the light adjust-
able lens. (Courtesy of Calhoun Vision, Pasadena, CA; with permission.)

481NEW TECHNOLOGY IOL OPTICS
tetrafoil pattern, and inducing asphericity besideshyperopic, myopic, and astigmatic corrections isnow possible. Preliminary in vitro and in vivostudies with the rabbit model have demonstrated
appropriate accuracy and reproducibility of thecorrections obtained with the new digital system.The biocompatibility of the lens material has
also been assessed in rabbit eyes, with no adverseeffect observed in different ocular tissues.
This foldable lens will be available in different
dioptric powers and can be implanted througha small incision like a standard three-piece siliconeIOL. The initial clinical application will be a pseu-
dophakic lens for use after cataract surgery, butthe technology can potentially be applied to anytype of IOL, including accommodative or phakiclenses. Use in conjunction with wavefront sensing
allows full customization of the lens. Initialhuman clinical studies of the LAL have beenperformed by Dr. Arturo Chayet in Tijuana,
Mexico. The predictability in actual human pa-tients using the LAL with the slit lamp deliverysystem was found to be excellent. It is anticipated
that trials will begin this year in Europe witheventual trials and submission for FDA approvalin the United States to follow.
Implantable miniature telescope
The implantable miniature telescope, manufac-tured by VisionCare Ophthalmic Technologies(Saratoga, California), and invented by company
founders Dr. Isaac Lipshitz and Yossi Gross, isa unique visual prosthetic device designed specif-ically to improve vision of patients suffering from
late-stage age-related macular degeneration [36–38]. The second-generation telescope is a wide-angle version of the device that allows for a largerview of the central visual field than previous
models. This device is an optical apparatus com-prised of two main components: a pure glass opti-cal cylinder and a carrying device constructed
from standard biocompatible materials suitablefor implantation in the eye (Fig. 11A). The opticalportion contains ultraprecise, wide-angle micro-
lenses that provide retinal image enlargement ofthe central visual field. Two models are available,allowing for a magnification of �2.2 or �3, withan enlarged retinal image produced over approxi-mately 52 to 60 degrees of the central retina. Thecarrying device is comprised of a clear carrier anda blue light restrictor. The carrier has two modi-
fied C-loops that hold the prosthetic device inthe capsular bag. Once secured inside the bag,the anterior window of the optic extends margin-
ally through the pupil (Fig. 11B). It is designed toallow a clearance of approximately 2 to 3 mmfrom the corneal endothelium.
The wide-angle model is currently in late-stageclinical trials in the United States. Enrolledpatients are at least 55 years of age; have stable
bilateral macular degeneration (disciform scar orgeographic atrophy); and visual acuity between20/80 and 20/800. The device is implanted in oneeye to improve central vision, whereas the other
eye remains as is to continue to provide peripheralvision. No other IOL is used in conjunction withthe implantable telescope. Promising results from
the prospective, multicenter phase II-III trial haverecently been reported by Packer and coworkers[39] at the twenty-third Congress of the European
Fig. 11. (A) Gross photograph showing the current version of the telescope (anterior view). (Courtesy of VisionCare,
Saratoga, California; with permission.) (B) Clinical slit lamp photograph of an eye implanted with the device by an
11-mm superior limbal incision. (Courtesy of Doyle Stulting, MD, Atlanta, GA; James P. Gilman, CRA, Atlanta,
GA.) (C) Gross photograph of a human eye obtained postmortem (posterior view) implanted with a prototype of the
pseudophakic wide angle implantable miniature telescope. The prosthetic device has been experimentally fixated in
the ciliary sulcus by Mark Packer, MD (Eugene, OR).

482 WERNER et al
Society of Cataract and Refractive Surgeons (Lis-bon, Portugal, September 2005). At 6 months,mean distance and near best-corrected visual acu-
ity improved 3.3 and 3 Snellen lines, respectively.According to the manufacturer, the device has anoptimal focusing distance of 250 cm in front of theeye. This is designed to improve activities of daily
living, and reading may be accomplished withstandard spectacles to bring the enlarged retinalimage into focus. A patient with an implantable
miniature telescope should be able to scan thefield of view for reading and distance visual activ-ities through natural eye movements, because the
device is placed entirely in the eye. In addition,the implantable miniature telescope allows fora natural cosmetic appearance. Another modelof the telescope is being specially modified for
patients who are pseudophakic (Fig. 11C).
Summary
There has been a rapid evolution in the field ofIOL technology, much of it influenced by the
development of surgical techniques, such as verysmall incisions, and wavefront aberrometry. Withbetter evidence that blue light is an important
variable in age-related macular degeneration, theuse of IOLs with blue-light blockers, or eventuallyphotochromic lenses, could rapidly become the
standard in IOL manufacture. The developmentof improved multifocal and accommodative lensesis a consequence of the increasing popularity of
the refractive lens exchange procedure. Whichoptic technology will provide the best patientsatisfaction is unclear at this time.
References
[1] Werner L, Apple DJ, Schmidbauer JM. Ideal IOL
(PMMA and foldable) for Year 2002. In:
Buratto L, Werner L, Zanini M, et al, editors. Pha-
coemulsification: principles and techniques. Thoro-
fare (NJ): Slack; 2003. p. 435–51.
[2] Olson RJ, Werner L, Mamalis N, et al. New IOL
technology. Am J Ophthalmol 2005;140:709–16.
[3] Javitt J, Brauweiler HP, Jacobi KW, et al. Cataract
extraction withmultifocal intraocular lens implanta-
tion: clinical, functional, and quality-of-life out-
comes. Multicenter clinical trial in Germany and
Austria. J Cataract Refract Surg 2000;26:1356–66.
[4] Schmitz S, Dick HB, Krummenauer F, et al. Con-
trast sensitivity and glare disability by halogen light
after monofocal and multifocal lens implantation.
Br J Ophthalmol 2000;84:1109–12.
[5] Rocha KM, ChalitaMR, Souza CE, et al. Postoper-
ative wavefront analysis and contrast sensitivity of
a multifocal apodized diffractive IOL (ReSTOR)
and three monofocal IOLs. J Refract Surg 2005;21:
S808–12.
[6] Patel CK, Ormonde S, Rosen PH, et al. Post-
operative intraocular lens rotation: a randomized
comparison of plate and loop haptic implants. Oph-
thalmology 1999;106:2190–5.
[7] Chang DF. Early rotational stability of the longer
Staar toric intraocular lens: fifty consecutive cases.
J Cataract Refract Surg 2003;29:935–40.
[8] Horn J. Analysis of residual refractive cylinder with
the investigational AcrySof toric IOL. Presented at
the XXIII Congress of the European Society of Cat-
aract and Refractive Surgeons. Lisbon, Portugal,
September 12, 2005.
[9] Gaillard ER, Zheng L, Merriam JC, et al. Age-re-
lated changes in the absorption characteristics of
the primate lens. Invest Ophthalmol Vis Sci 2000;
41:1454–9.
[10] Sparrow JR, Miller AS, Zhou J. Blue light-absorb-
ing intraocular lens and retinal pigment epithelium
protection in vitro. J Cataract Refract Surg 2004;
30:873–8.
[11] Ernest PH. Light-transmission-spectrum compari-
son of foldable intraocular lenses. J Cataract Refract
Surg 2004;30:1755–8.
[12] Rodriguez-Galietero A, Montes-Mico R, Munoz G,
et al. Comparison of contrast sensitivity and color
discrimination after clear and yellow intraocular
lens implantation. J Cataract Refract Surg 2005;31:
1736–40.
[13] Mainster MA. Intraocular lenses should block UV
radiation and violet but not blue light. Arch Oph-
thalmol 2005;123:550–5.
[14] Werner L, Mamalis N, Romaniv N, et al. New pho-
tochromic foldable intraocular lens: preliminary
study on feasibility and biocompatibility. J Cataract
Refract Surg 2006;32(7):1214–21.
[15] Alio JL, Tavolato M, de la Hoz F, et al. Near vision
restoration with refractive lens exchange and pseu-
doaccommodating andmultifocal refractive and dif-
fractive intraocular lenses: comparative clinical
study. J Cataract Refract Surg 2004;30:2494–503.
[16] Koeppl C, Findl O, Menapace R, et al. Pilocarpine-
induced shift of an accommodating intraocular lens:
AT-45 Crystalens. J Cataract Refract Surg 2005;31:
1290–7.
[17] Cazal J, Lavin-Dapena C,Marin J, et al. Accommo-
dative intraocular lens tilting. Am J Ophthalmol
2005;140:341–4.
[18] Rana A, Miller D, Magnante P. Understanding the
accommodating intraocular lens. J Cataract Refract
Surg 2003;29:2284–7.
[19] Langenbucher A, Reese S, Jakob C, et al. Pseudo-
phakic accommodation with translation lenses - dual
optic vs mono optic. Ophthalmic Physiol Opt 2004;
24:450–7.

483NEW TECHNOLOGY IOL OPTICS
[20] McLeod SD, Portney V, Ting A. A dual optic ac-
commodating foldable intraocular lens. Br J Oph-
thalmol 2003;87:1083–5.
[21] Werner L, Pandey SK, Izak AM, et al. Capsular bag
opacification after experimental implantation of
a new accommodating intraocular lens in rabbit
eyes. J Cataract Refract Surg 2004;30:1114–23.
[22] Werner L, Mamalis N, Stevens S, et al. Interlenticu-
lar opacification: dual-optic versus piggyback intra-
ocular lenses. J Cataract Refract Surg 2006;32(4):
655–61.
[23] Ossma-Gomez I. Long-term follow up of the Syn-
chrony accommodating IOL: two-year data. Pre-
sented at the International Society of Refractive
Surgery of the American Academy of Ophthalmol-
ogy Meeting. Chicago, October 15, 2005.
[24] Packer M, Fine IH, Hoffman RS, et al. Prospective
randomized trial of an anterior surfacemodified pro-
late intraocular lens. J Refract Surg 2002;18:692–6.
[25] Packer M, Fine IH, Hofman RS, et al. Improved
functional vision with a modified prolate intraocular
lens. J Cataract Refract Surg 2004;30:986–92.
[26] Mester U, Dillinger P, Anterist N. Impact of a mod-
ified optic design on visual function: clinical compar-
ative study. J Cataract Refract Surg 2003;29:627–8.
[27] Kershner RM. Retinal image contrast and func-
tional visual performance with aspheric, silicone,
and acrylic intraocular lenses: prospective evalua-
tion. J Cataract Refract Surg 2003;29:1684–94.
[28] Bellucci R, Scialdone A, Buratto L, et al. Visual acu-
ity and contrast sensitivity comparison between Tec-
nis and AcrySof SA60AT intraocular lenses:
a multicenter randomized study. J Cataract Refract
Surg 2005;31:712–7.
[29] Altmann GE, Nichamin LD, Lane SS, et al. Optical
performance of 3 intraocular lens designs in the pres-
ence of decentration. J Cataract Refract Surg 2005;
31:574–85.
[30] Pandey SK, Werner L, Agarwal A, et al. Phakonit
cataract removal through a sub-1.0 mm incision
and implantation of the ThinOptX rollable intraoc-
ular lens. J Cataract Refract Surg 2002;28:1710–3.
[31] DogruM,HondaR,OmotoM, et al. Early visual re-
sults with the rollable ThinOptX intraocular lens.
J Cataract Refract Surg 2004;30:558–65.
[32] Alio JL, Schimchak P, Montes-Mico R, et al. Reti-
nal image quality after microincision intraocular
lens implantation. J Cataract Refract Surg 2005;31:
1557–60.
[33] Schwartz DM. Light-adjustable lens. Trans Am
Ophthalmol Soc 2003;101:417–36.
[34] Werner L, Mamalis N, Apple DJ. Biomaterials for
wavefront customization. In: Krueger RR,
Applegate RA, MacRae SM, editors. Wavefront
customized visual correction. Thorofare (NJ): Slack;
2004. p. 271–8.
[35] Werner L, Mamalis N. Wavefront corrections of in-
traocular lenses. Ophthalmol Clin North Am 2004;
17:233–45.
[36] Werner L, Kaskaloglu M, Apple DJ, et al. Aqueous
infiltration into an implantable miniaturized tele-
scope. Ophthalmic Surg Lasers 2002;33:343–8.
[37] Lane SS, Kuppermann BD, Fine IH, et al. A pro-
spective multicenter clinical trial to evaluate the
safety and effectiveness of the implantable minia-
ture telescope. Am J Ophthalmol 2004;137:
993–1001.
[38] Chun DW, Heier JS, Raizman MB. Visual pros-
thetic device for bilateral end-stagemacular degener-
ation. Expert Rev Med Devices 2005;2:657–65.
[39] Packer M, Fine IH, Hoffman R, et al. Phase II/III
study of a visual prosthetic device for the treatment
of vision loss due to advancedmacular degeneration.
Presented at the 23rd Congress of the European So-
ciety of Cataract and Refractive Surgeons, Lisbon,
Portugal, September 10, 2005.

Ophthalmol Clin N Am 19 (2006) 485–493
Astigmatism ControlLouis D. Nichamin, MD
The Laurel Eye Clinic, 50 Waterford Pike, Brookville, PA 15825, USA
Over the past several years the concept ofrefractive cataract surgery has received increased
attention from surgeons, and the need for itsadoption has recently been made more urgent bythe approval and availability of new presbyopia-
correcting intraocular lenses (IOL). Indeed, theneed to manage pre-existing astigmatism has be-come a requisite aspect of modern phacosurgery.
Experience with keratorefractive surgery hasproved that astigmatism of as little as 0.75 diopters(D) may leave a patient symptomatic with visualblur, ghosting, and halos. To embrace this notion
of refractive cataract surgery fully, the dedicatedsurgeon must aspire to a level of accuracy thatequates with corneal-based refractive surgery. For-
tunately, techniques have emerged that afford therefractive lens surgeon the ability to effectively,safely, and reproducibly reduce cylinder error to
acceptable levels of 0.50 D or less, either at the timeof cataract surgery, or through a subsequent en-hancement procedure.
Patient selection and considerations
Estimates of the incidence of significant, nat-
urally occurring astigmatism vary widely from7.5% to 75% [1]. In my experience with the gen-eral cataract population, approximately 10% of
patients come to surgery with greater than 2 Dof cylinder, 20% have between 1 and 2 D, and70% have less than 1 D. One can therefore expect
to treat pre-existing astigmatism in greater thanone out of every three patients. Again, the goalis to leave the patient with a refractive outcomefor both sphere and cylinder of 0.50 D or less.
When planning astigmatism correction, onemust consider the location of the cylinder, the age
E-mail address: [email protected]
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All r
doi:10.1016/j.ohc.2006.07.004
of the patient, and the status of the fellow eye.Given that most patients drift against-the-rule over
their lifetime (eg, toward plus cylinder at 180degrees) many surgeons advocate a slightly lessaggressive approach to the reduction of with-
the-rule cylinder. Furthermore, some authors havesuggested that residual with-the-rule astigmatismmay favor better uncorrected distance acuity given
that most visual stimuli are of a vertical nature [2].Similarly, it has been contended that residualagainst-the-rule cylinder may improve uncorrectednear vision [3]. The long-standing tenet that resid-
ual (myopic) with-the-rule astigmatism is a desir-able goal to lengthen the conoid of Sturm andoptimize depth perception has recently, however,
been called into question [4]. In addressing today’scataract patient, given recent refinements in surgi-cal technique and increased use of presbyopia-
correcting implants, the goal of a spherical outcomeseems to be optimal.
Options to reduce astigmatism
The first decision one is faced with is whetherto address pre-existing astigmatism at the time ofcataract surgery, or to defer and treat the cylinder
separately. Historically, it has been argued thatgreater accuracy might be achieved if sufficienttime were allotted for adequate wound healing,
and a stable refraction documented before takingon astigmatic correction. Today, with the use offoldable IOLs and incision sizes now well under
3.5 mm, essentially neutral astigmatic outcomesmay be consistently achieved [5]. As such, mostsurgeons opt to treat pre-existing cylinder concur-rently with the implant procedure. This obviates
the time and energy required for a second surgicalsitting, and is the approach most widely takenwhen dealing with cataract patients, most often
through the use of limbal relaxing incisions
ights reserved.
ophthalmology.theclinics.com

486 NICHAMIN
(LRIs) as described later. Given the exacting needfor near-perfect refractive results today, however,particularly when using presbyopia-correcting
IOLs, along with an increasing acceptance anduse of bioptics (using excimer laser technology),some cataract surgeons are beginning to prefera staged procedure should the patient possess
any significant level of preoperative astigmatism.The second fundamental decision is whether to
treat the astigmatism througha lenticular approach
(ie, to use a toric IOL) or to use a keratorefractivetechnique. From a theoretical perspective a toricIOL has the advantage of avoiding corneal manip-
ulation and, as such, the possibility of inducingirregular astigmatism, and also potentially pro-vides for reversibility. Their effectiveness has beenwidely reported [6,7]. Until recently, however, the
availability of lens choices, at least within theUnited States, has been limited. In addition, post-operative rotation of the first Food and Drug
Administration–approved device, the STAARToric (STAAR Surgical Co., Monrovia, Califor-nia) single-piece plate-haptic IOL, has been a
well-documented issue [6,8]. Fortunately, newer de-vices are reaching the marketplace and are provingto be more effective with better rotational stability,
as seen with the Alcon (Alcon Laboratories, Inc.,Fort Worth, Texas) single-piece acrylic lens [9,10].As with any form of astigmatic correction, thekey to obtaining propitious outcomes hinges on
proper centration with the axis of astigmatism, inthat relatively small degrees of misalignment maylead to a profound loss of effect, as discussed in
more detail later [1].
Treatment options
The notion of reducing astigmatism at the time
of IOL surgery, specifically by way of astigmatickeratotomy, dates back to the mid-1980s [11–13].Throughout the 1990s a number of authors began
to recognize the advantages of moving corneal-relaxing incisions out toward the limbus [14–16].These so-called LRIs have become the most pop-ular way to manage astigmatism at the time of
cataract surgery and are discussed in detail later.Another viable and relatively simple way to
decrease astigmatism is to manipulate the cataract
incision to impact favorably pre-existing astigma-tism. This is accomplished by first centering theincision on the steep corneal meridian, and then
by varying its size and design, affect a desiredamount of wound flattening, and hence a decreasein cylinder [17]. This approach, however, presents
logistical challenges including movement aroundthe surgical table, often producing awkwardhand positions. In addition, varying instrumenta-
tion may be needed from case to case, along witha dynamic rather than consistent mindset and rep-ertoire. For these reasons, this technique haslargely been supplanted by the use of a consistent
and astigmatically neutral phacoincision (typicallyplaced temporally for stability) and then addingsupplemental relaxing incisions (LRIs). A recent
study by Kaufmann and coworkers [18] concludedthat LRIs in combination with a temporal clearcorneal incision provided superior astigmatic out-
comes to that of ‘‘on-axis’’ surgery.Several other options deserve mention. Lever
andDahan [19] have suggested a novel technique ofusing opposing clear corneal incisions to address
pre-existing astigmatism. In this technique, a sec-ond opposite penetrating clear corneal incision isplaced over the steep meridian 180 degrees away
from the main incision. This approach is techni-cally simple and requires no additional instrumen-tation; however, a second substantial penetrating
incision is now present, possibly increasing therisk of wound leak or even infection. In addition,single-plane beveled incisions are known to be
less effective, for a given arc length, at flatteningthe cornea as compared with traditional perpendic-ular relaxing incisions [20,21].
Yet another important and increasingly popu-
lar alternative is that of bioptics, a techniqueoriginally described to address residual refractiveerror following implantation of myopic phakic
IOLs, but one that is just as useful in the settingof pseudophakic lens surgery [22–24]. In thisapproach, one exploits the advanced technology
and exquisite accuracy of the excimer laser. Ina staged manner, one may treat both residualspherical and astigmatic error following implantsurgery. In Zaldivar’s original description, a la-
ser-assisted in situ keratomileusis flap was createdbefore the implant procedure, and then as neces-sary, the flap was lifted and residual refractive er-
ror was corrected with the laser. Today, mostsurgeons prefer to perform both the flap and laserablation concurrently following cataract surgery,
as needed, reducing the number of unnecessaryflaps that would otherwise be created. It hasbeen my experience that laser-assisted in situ ker-
atomileusis may be performed safely followingIOL surgery at 6 weeks, perhaps earlier. Woundstability and healing must be confirmed, alongwith a stable refractive error. It might be further
argued that custom wavefront-guided ablation is

487ASTIGMATISM CONTROL
particularly well suited in the pseudophakic eyebecause the dynamic lens component no longerexists [25]. For most refractive cataract surgeons,bioptics has become an integral part of the preop-
erative discussion with the patient, and in my ex-perience its use is required in approximately 10%of cases, depending on the patient’s preoperative
refractive error. Finally, conductive keratoplastyused in an off-label fashion has also recentlybeen described as a means by which residual hy-
peropia and hyperopic astigmatism may be effec-tively reduced following cataract surgery [26].
Limbal-relaxing incisions
The first description of the astigmatic effect ofnonpenetrating incisions placed near the limbusdates back to 1898 and is credited to the Dutchophthalmologist L.J. Lans [27]. As noted, LRIs
have become the most popular technique used to-day to reduce pre-existing astigmatism at the timeof cataract surgery. Although my preference is to
use a temporal single-plane clear corneal phacoincision, one may use LRIs with any type ofphaco incision as long as the astigmatic effect is
known and factored into the surgical plan. LRIsoffer several advantages over astigmatic incisionsplaced within the cornea, at smaller optical zones.
These include less chance of causing a shift in theresultant cylinder axis. This presumably is causedby a diminished need for precise centration on thesteep meridian. More importantly, there is less of
a tendency to cause irregular corneal flattening,and hence less chance of inducing irregular astig-matism. Technically, LRIs are easier to perform
and more forgiving than shorter and more centralcorneal astigmatic incisions, and patients gener-ally report less discomfort. Another important ad-
vantage gained by moving out to the limbusinvolves the ‘‘coupling ratio,’’ which describesthe amount of flattening that occurs in the incised
meridian relative to the amount of steepening thatresults 90 degrees away; paired LRIs (when keptat or under 90 degrees of arc length) exhibita very consistent 1:1 ratio, and elicit little change
in spheroequivalent, obviating the need to makeany change in implant power.
Admittedly, these more peripheral incisions are
less powerful, but are still capable of correcting upto 3.5 D of astigmatism in the cataract-agedpopulation. One must keep in mind that the goal
is to reduce the patient’s cylinder, without over-correcting or shifting the resultant axis. To achievea given amount of correction, these peripheral
intralimbal incisions must be longer in total arclength than more centrally placed corneal astig-matic incisions; however, unlike longer radialkeratotomy incisions, they seem to be stable with
regard to refractive effect, and show little sign ofinducing problems, such as dry eye syndrome orother pejorative effects from corneal denervation
[16]. Their stability may well be caused by the prox-imity of well-vascularized limbal tissue. There are,of course, potential complicationswith any surgical
technique and these are addressed later.
The plan
Perhaps the most challenging aspect of astig-matism surgery involves the determination of the
quantity and exact location of the cylinder that is tobe corrected, and thereby formulating a surgicalplan. Unfortunately, preoperative measurements
(keratometry, refraction, and corneal topography)do not always correlate. Lenticular astigmatismmay account for some of this disparity, particularlyin cases where there is a wide variance between
refraction and corneal measurements; however,some discrepancies are likely caused by the inherentshortcomings of traditional measurements of astig-
matism. Standard keratometry, for example, mea-sures only two points in each meridian at a singleoptical zone of approximately 3 mm.
When confounding measurements do arise, onemay compromise and average the disparate read-ings. For example, if refraction shows 2 D of
astigmatism and keratometry reveals only 1 D, itis reasonable to correct for 1.5 D. Alternatively, ifpreoperative calculations vary widely, one maydefer placing the relaxing incisions until a stable
refraction postimplantation is obtained, and thencorrect the astigmatism; LRIs may be safelyperformed in the office in an appropriate treat-
ment-room setting. Corneal topography can bevery helpful when refraction and keratometry donot agree, and it is increasingly becoming the
overall guiding measurement on which the sur-gical plan is based. Topography is also helpful indetecting subtle corneal pathology, such as kerato-
conus fruste, which likely negates the use of LRIs,or subtle irregular astigmatism, such as that causedby epithelial basement membrane dystrophy.
Nomograms
Once the amount of astigmatism to be cor-rected has been determined, a nomogram must beconsulted to determine the appropriate arc length

488 NICHAMIN
of the incisions. A number of popular nomogramsare currently available [28]. My nomogram ofchoice originated from the work of Dr. Stephen
Hollis and incorporates concepts taught byThornton [21], particularly his age modifiers. Asseen in Table 1, astigmatism is considered to bewith-the-rule if the steep axis (plus cylinder) is be-
tween 45 and 135 degrees. Against-the-rule astig-matism is considered to fall between 0 and 44,and 136 and 180 degrees. One aligns the patient’s
age with the amount of preoperative cylinder to becorrected and finds the suggested arc length thatthe incisions should subtend.
Paired incisions are preferred to optimizesymmetric corneal flattening and they are ex-pressed in degrees of arc rather than chord length.This is done to diminish overcorrections and
undercorrections for unusually small or largecorneas, because corneal diameter may signifi-cantly impact the relative length of the arcuate
incision and its resultant effect (Fig. 1). An em-piric blade depth setting is commonly used whenperforming LRIs, typically at 600 mm. This seems
to be a reasonable practice when treating cataractpatients; however, in the setting of refractive lensexchange surgery or when using presbyopia-cor-
recting IOLs (where ultimate precision is required)
it is my preference to perform pachymetry and useadjusted blade depth settings and a slightly moreaggressive nomogram (Table 2). Pachymetry
may be performed either preoperatively or at thetime of surgery. Readings are taken over the entirearc length of the intended incision, and an adjust-able micrometer diamond blade is then set to
approximately 90% of the thinnest reading ob-tained. Refinements to the blade depth settingand nomogram adjustments are often necessary
depending on individual surgeon technique; theinstruments used; and, in particular, the style ofthe blade. As a final note, in eyes that have previ-
ously undergone radial keratotomy, the length ofthe incisions should be reduced by approximately50%, and in eyes that have undergone significantprior keratotomy surgery, it may be best to avoid
additional incisional surgery and use a toric IOLor laser technology instead.
Surgical technique
In most cases, the relaxing incisions are placed
at the outset of surgery to minimize epithelialdisruption. The one exception to this rule occurswhen the phaco incision intersects or is
Table 1
Intralimbal relaxing incision nomogram for modern phaco surgery: empiric blade-depth setting of 600 mm
Spherical (up to þ 0.75 � 90 or þ 0.50 � 180)
Incision design: ‘‘Neutral’’ temporal clear corneal incision (ie, 3.5 mm or less, single plane, just anterior to vascular
arcade)
Against-the-rule, (Steep axis 0–44�/136–180�)
Paired incisions in degrees of arc
Preoperative cylinder 30–40 y 41–50 y 51–60 y 61–70 y 71–80 y 81–90 y 91þyNasal limbal arc only 35�
þ 0.75 – þ 1.25 55� 50� 45� 40� 35�
þ 1.50 – þ 2.00 70� 65� 60� 55� 45� 40� 35�
þ 2.25 – þ 2.75 90� 80� 70� 60� 50� 45� 40�
þ 3.00 – þ 3.75 90�
o.z ¼ 5 mm
90�
o.z ¼ 9 mm
85� 70� 60� 50� 45�
Incision design: The temporal incision, if greater than 40� of arc, is made by first creating a two-plane, grooved phaco
incision (600 m depth), which is then extended to the appropriate arc length at the conclusion of surgery.
With-the-rule, (Steep axis 45�–135�)
þ 1.00 – þ 1.50 50� 45� 40� 35� 30�
þ 1.75 – þ 2.25 60� 55� 50� 45� 40� 35� 30�
þ 2.50 – þ 3.00 70� 65� 60� 55� 50� 45� 40�
þ 3.25 – þ 3.75 80� 75� 70� 65� 60� 55� 45�
Incision design: ‘‘Neutral’’ temporal clear corneal along with the following peripheral arcuate incisions.
When placing intralimbal relaxing incisions following or concomitant with radial relaxing incisions, total arc length is
decreased by 50%.

489ASTIGMATISM CONTROL
encompassed within a long LRI. For example, inthe case of high against-the-rule astigmatismwherein the nomogram calls for a temporal arcu-ate incision of greater than 40 degrees of arc, the
temporal LRI is superimposed on the (temporal)phaco incision and if it is extended to its full arclength at the start of surgery, significant gaping
and edema may result secondary to intraoperativewound manipulation. In this setting, the temporal
Fig. 1. Nomogram design. Note relative disparity in in-
cision length between a large and small corneal diameter
if measured in millimeters. Degrees of arc lend consis-
tency irrespective of corneal size.
incision is first made by creating a shortened LRIwhose arc length corresponds to the width of thephacoincision and IOL incision. This amounts toa two-plane grooved phacoincision whose depth is
either 600 mm or has been determined by pachy-metry, as described previously. Following IOLimplantation and before viscoelastic removal,
while the globe is still firm, the relaxing incisionis extended to its full arc length as dictated by thenomogram. When an LRI is superimposed on the
phacotunnel, the keratome entry is accomplishedby pressing the bottom surface of the keratomeblade downward on the outer or posterior edge of
the LRI. The keratome is then advanced into theLRI at an iris-parallel plane. This angulationpromotes a dissection that takes place at mid-stromal depth, which helps ensure adequate tun-
nel length and a self-sealing closure.Proper centration of the incisions over the steep
corneal meridian is of utmost importance. Accord-
ing to Euler’s theorem, an axis deviation of 5, 10, or15 degrees results in 17%, 33%, and 50% re-duction, respectively, in effect [1]. This reduction
in effect holds true for both relaxing incisions and
Table 2
Intralimbal arcuate astigmatic nomogram
With-the-rule (Steep axis 45�–135�)
Paired incisions in degrees of arc
Preoperative
cylinder (Diopters) 20–30 yo 31–40 yo 41–50 yo 51–60 yo 61–70 yo 71–80 yo
0.75 40 35 35 30 30
1.00 45 40 40 35 35 30
1.25 55 50 45 40 35 35
1.50 60 55 50 45 40 40
1.75 65 60 55 50 45 45
2.00 70 65 60 55 50 45
2.25 75 70 65 60 55 50
2.50 80 75 70 65 60 55
2.75 85 80 75 70 65 60
3.00 90 90 85 80 70 65
Against-the-rule (Steep axis 0–44�/136–180�)
0.75 45 40 40 35 35 30
1.00 50 45 45 40 40 35
1.25 55 55 50 45 40 35
1.50 60 60 55 50 45 40
1.75 65 65 60 55 50 45
2.00 70 70 65 60 55 50
2.25 75 75 70 65 60 55
2.50 80 80 75 70 65 60
2.75 85 85 80 75 70 65
3.00 90 90 85 80 75 70
Blade depth setting is at 90% of the thinnest pachymetry.

490 NICHAMIN
toric IOLs. Also, increasing evidence supports thenotion that significant cyclotorsion may occurwhen assuming a supine position [29]. For this rea-
son,most surgeons advocate placing an orientationmark at the 12-o’clock or 6-o’clock limbus whilethe patient is in an upright position. This is partic-ularly important when using injection anesthesia
wherein unpredictable ocular rotation may occur.An additional measure that may be used to helpcenter the relaxing incisions is to identify the steep
meridian (plus cylinder axis) intraoperatively usingsome form of keratoscopy. The steepmeridian overwhich the incisions are to be placed corresponds to
the shorter axis of the reflected corneal mire. A sim-ple hand-held device, such as the Maloney (Storz,St. Louis, Missouri; Katena, Denville, New Jersey)or Nichamin (Mastel Precision, Rapid City, South
Dakota) keratoscope, works well or a more robustand well-defined mire may be obtained through anelaboratemicroscope-mounted instrument, such as
the Mastel Ring of Light (Mastel Precision). An-other common way in which the steep meridian ismarked uses a Mendez Ring or similar degree
gauge, which is aligned with the previously placedlimbal orientation mark, and then locating the cyl-inder axis on the 360-degree gauge.
The LRI should be placed at the most periph-eral extent of clear corneal tissue, just inside of thetrue surgical limbus. This holds true irrespectiveof the presence of pannus. If bleeding does occur,
it may be ignored and will cease spontaneously.One must avoid placing the incisions further outat the true surgical limbus in that a significant
reduction of effect will likely occur because ofboth increased tissue thickness and a variation intissue composition; these incisions are really intra-
limbal in nature. In creating the incision, it isimportant to hold the knife perpendicular to thecorneal surface to achieve consistent depth andeffect, and help to avoid gaping of the incision.
Good hand and wrist support is important, andthe blade ought to be held as if one were throwinga dart such that the instrument may be rotated
between thumb and index finger as it is beingadvanced, leading to smooth arcuate incisions.Typically, the right hand is used to create incisions
on the right side of the globe, and the left hand forincisions on the left side. In most cases it is moreefficient to pull the blade toward oneself, as
opposed to pushing it away.The extent of arc to be incised may be de-
marcated in several different ways. My preferredmethod makes use of a modified Fine-Thornton
fixation ring (the Nichamin Fixation Ring and
Gauge, available from Mastel Precision, Storz,Rhein Medical, Tampa, Florida). This instrumentserves to fixate and position the globe to optimize
incision placement, and to delineate the extent ofarc to be incised. One visually extrapolates fromthe limbus to marks on the surface of the ring.Each incremental mark is 10 degrees apart, and
bold hash marks (180 degrees) opposite to eachother serve to align and center the incision overthe steep meridian. This approach obviates the
need to ink and physically mark the cornea. Ifone desires, particularly when first gaining experi-ence with LRIs, a two-cut radial keratotomy (RK)
marker may be used to place ink marks upon thecornea to show the exact extent of arc that is to beincised, in conjunction with the fixation ring-gauge (Fig. 2). Alternatively, various press-on
markers are available, such as the Dell-NichaminMarker or Nichamin-Kershner Marker manufac-tured by Rhein Medical. ASICO and many other
instrument companies also offer a full line of ded-icated markers, rings, and blades for performingLRIs.
Various knives have been designed specificallyfor this application, ranging from disposable steelblades to exquisite gemstone diamond knives.
Synthetic (and less expensive) diamond materialsare also available and are intended for limitedreuse. My preference is for diamond blade tech-nology, which incorporates a single small and
arced footplate for enhanced visualization at thelimbus (Mastel Precision, Storz). Two models areavailable, one with a preset depth of 600 mm, and
the other with an adjustable micrometer handle,
Fig. 2. The Nichamin Fixation Ring and Gauge serves
both to fixate the globe and delineate the extent of arc
to be incised; a two-cut radial marker may be used to
mark the extent of arc to be incised, and the Mastel Ni-
chamin Force AK Diamond Blade with preset depth of
600 mm. (Courtesy of Mastel Precision, Rapid City, SD;
with permission.)

491ASTIGMATISM CONTROL
which is preferred for refractive lens exchange(RLE) surgery and when using presbyopia-correcting IOLs with cataract patients (Fig. 3).
Another less common method of creating
peripheral relaxing incisions is to use a devicesuch as the Terry/Schanzlin Astigmatome (OasisMedical, Glendora, California), which circum-
vents the need to create a free-hand incision.This trephine-like device has been designed toproduce consistent and symmetric peripheral ar-
cuate corneal-relaxing incisions. It uses a vacuumspeculum that mates with various reusable tem-plates that are selected based on the amount of as-
tigmatic correction that is desired. The incision iscreated by simply turning a disposable steel bladeunit that fits inside of the template.
Complications
LRIs are proving to be a safer and more
forgiving approach to managing astigmatism ascompared with more central corneal incisions.Nonetheless, as with any surgical technique,potential complications exist, and several are
listed in Box 1. Of these, the most likely to be en-countered is the placement of incisions on thewrong axis. When this occurs, it typically takes
the form of a 90-degree error with positioningon the opposite, flat meridian. This results in anincrease and likely doubling of the patient’s pre-
existing cylinder. Compulsive attention is requiredin this regard. The surgeon ought to considerusing safety checks to prevent this frustratingcomplication from occurring, such as having
a written plan that is brought into the operatingroom and is kept visible and properly oriented. In-cisions are always placed on the plus (þ) cylinderaxis, and opposite to the minus (�) cylinder axis.
Although very rare, corneal perforation ispossible. This may be caused by improper setting
Fig. 3. Mastel Profile Blade. (Courtesy of Mastel Preci-
sion, Rapid City, SD; with permission.)
of the blade depth, or as a result of a defect in themicrometer mechanism. This latter problem may
arise after repeated autoclaving and many sterili-zation runs. Periodic inspection and calibration iswarranted, even with preset single-depth knives.
When encountered, unlike radial microperfora-tions, these circumferential perforations rarelyself-seal and likely require placement of temporary
sutures.
Enhancement techniques
LRIs lend themselves well to in-office ‘‘touch-ups.’’ Although some surgeons place or extend
incisions at the slit-lamp, it is my preference to usea small operating microscope and to perform theprocedure within a dedicated treatment room. Ithas been my experience that this provides far
better surgical control and patient comfort. In thecase of residual astigmatism without prior inci-sional correction, one uses the same technique and
nomogram as described previously.In the case of an undercorrection following
previous LRIs, one should inspect the length and
positioning of the incisions. Placement of theincisions too far out into the true surgical limbusand beyond clear cornea often leads to under-
correction. If this is the case, new incisions may beplaced insideof theoriginalLRIs, butwithamodestreduction in arc length from that which is dictatedby the nomogram. If the incision placement seems
to be appropriate then one can simply extend theoriginal LRIs. When faced with an overcorrection,one should resist the temptation to place additional
incisions in the opposite meridian. This can lead toan unstable cornea with unpredictable refractiveresults, or worse, induce irregular astigmatism.
Rather, one should consider nonincisional modal-ities, such as photorefractive keratectomy or laser-assisted in situ keratomileusis.
Box 1. Potential problems
� Infection� Weakening of the globe� Perforation� Decreased corneal sensation� Induced irregular astigmatism� Misalignment or axis shift� Wound gape and discomfort� Operating on the wrong (opposite)
axis

492 NICHAMIN
To correct unusually high levels of astigma-tism, LRIs may be used in conjunction with a toricIOL or excimer laser surgery (bioptics). In several
rare cases I have combined all three modalitiesand safely corrected up to 9 D of pre-existingastigmatism.
Summary
Refinement of the refractive outcome may
arguably be the single most pressing and importantchallenge faced by today’s cataract surgeon. Alongwith spherical error, pre-existing astigmatism may
now be safely and effectively reduced at the time ofcataract surgery. Astigmatic relaxing incisions arethe most common method used to accomplish this
goal. By moving these incisions out to an intra-limbal location, the complications and difficultiesassociated with astigmatic keratotomy have beengreatly reduced. Toric IOLs represent another
viable mode by which the surgeon may decreaseor eliminate cylinder. Enhancement techniques arealso important to help reduce residual astigmatism.
LRIs may be used in a similar fashion, postopera-tively, to accomplish this, or bioptics may be usedwith excimer laser technology. The future will
undoubtedly yield further breakthroughs, such aswavefront-guided customized IOLs or perhapslaser-adjustable implants, all leading to better
refractive outcomes and improved quality of visionfor pseudophakic patients.
References
[1] Abrams D. Ophthalmic optics and refraction. In:
Duke-Elder SS, editor. System of ophthalmology.
St. Louis: Mosby; 1970. p. 671–4.
[2] Novis C. Astigmatism and toric intraocular lenses.
Curr Opin Ophthalmol 2000;11:47–50.
[3] Trindade F, Oliveira A, Frasso M. Benefit of
against-the-rule astigmatism to uncorrected near
acuity. J Cataract Refract Surg 1997;23:82–5.
[4] Savage H, Rothstein M, Davuluri G, et al. Myopic
astigmatism and presbyopia trial. Am J Ophthalmol
2003;135:628–32.
[5] Masket S, Tennen DG. Astigmatic stabilization of
3.0 mm temporal clear corneal cataract incisions.
J Cataract Refract Surg 1996;22:1451–5.
[6] SunXY, VicaryD,Montgomery P, et al. Toric intra-
ocular lenses for correcting astigmatism in 130 eyes.
Ophthalmology 2000;107:1776–81.
[7] Till JS, Yoder PR, Wilcox TK, et al. Toric intraocu-
lar lens implantation: 100 consecutive cases. J Cata-
ract Refract Surg 2002;28:295–301.
[8] Ruhswurm I, Scholz U, Zehetmayer M, et al. Astig-
matism correction with a foldable toric intraocular
lens in cataract patients. J Cataract Refract Surg
2000;26:1022–7.
[9] FDA approves AcrySof toric IOL for cataract
patients. Fort Worth (TX): Alcon Laboratories,
Inc. Ophthalmology Times November 1, 2005.
[10] Food andDrugAdministration. Available at: http://
www.fda.gov/cdrh/pdf/p930014s015.html. Accessed
February 27, 2006.
[11] Osher RH. Combining phacoemulsification with
corneal relaxing incisions for reduction of preexist-
ing astigmatism. Presented at the annual meeting
of the American Intraocular Implant Society. Los
Angeles, 1984.
[12] Maloney WF. Refractive cataract replacement:
a comprehensive approach to maximize refractive
benefits of cataract extraction. Presented at the an-
nual meeting of the American Society of Cataract
and Refractive Surgery. Los Angeles, 1986.
[13] Osher RH. Transverse astigmatic keratotomy com-
bined with cataract surgery. Ophthalmol Clin North
Am 1992;5:717–25.
[14] BudakK, FriedmanNF,KochDD. Limbal relaxing
incisions with cataract surgery. J Cataract Refract
Surg 1998;24:503–8.
[15] Muller-Jensen K, Fischer P, Siepe U. Limbal relax-
ing incisions to correct astigmatism in clear corneal
cataract surgery. J Refract Surg 1999;15:586–9.
[16] Nichamin LD. Changing approach to astigmatism
management during phacoemulsification: peripheral
arcuate astigmatic relaxing incisions. Presented at
the annual meeting of the American Society of Cat-
aract and Refractive Surgery. Boston,May 20, 2000.
[17] Koch MJ, Kohnen T. Refractive cataract surgery.
Curr Opin Ophthalmol 1999;10:10–5.
[18] Kaufmann C, Peter J, Ooi K, et al. Limbal relaxing
incisions versus on-axis incisions to reduce corneal
astigmatism at the time of cataract surgery. J Cata-
ract Refract Surg 2005;31:2261–5.
[19] Lever J, Dahan E. Opposite clear corneal incisions
to correct preexisting astigmatism in cataract sur-
gery. J Cataract Refract Surg 2000;26:803–5.
[20] Nichamin LD. Opposite clear corneal incisions.
J Cataract Refract Surg 2001;27:7–8.
[21] Thornton SP. Radial and astigmatic keratotomy:
the American system of precise, predictable refrac-
tive surgery. Thorofare (NJ): Slack; 1994.
[22] Zaldivar R, Davidorf JM, Oscerow S, et al. Com-
bined posterior chamber phakic intraocular lens
and laser in situ keratomileusis: bioptics for extreme
myopia. J Refract Surg 1999;15:299–308.
[23] Nichamin LD. Bioptics: expanding its role to pseu-
dophakia. Presented at the annual meeting of the
American Society of Cataract and Refractive Sur-
gery. Philadelphia, June 1, 2002.
[24] Nichamin LD. Expanding the role of bioptics to the
pseudophakic patient. J Cataract Refract Surg 2001;
27:1343–4.
[25] Nichamin LD. Bioptics for the pseudophakic pa-
tient. In: Gills JP, editor. A complete guide to

493ASTIGMATISM CONTROL
astigmatism management. Thorofare (NJ): Slack;
2003. p. 37–9.
[26] Nichamin LD. Results of CK after cataract surgery.
Presented at Annual Meeting of the American Soci-
ety of Cataract and Refractive Surgery. San Diego,
May 2, 2004.
[27] Schimmelpfenning BH, Waring GO. Development
of radial keratotomy in the nineteenth century. In:
Waring GO, editor. Refractive keratotomy for myo-
pia and astigmatism. St Louis: Mosby-Year Book;
1992. p. 174–5.
[28] Gills JP. A complete guide to astigmatism manage-
ment. Thorofare (NJ): Slack; 2003.
[29] Swami AU, Steinert RF, Osborne WE, et al. Rota-
tional malposition during laser in situ keratomileu-
sis. Am J Ophthalmol 2002;133:561–2.

Ophthalmol Clin N Am 19 (2006) 495–506
Management of Vitreous Loss and DroppedNucleus During Cataract Surgery
Lisa Brothers Arbisser, MDa,b,*, Steve Charles, MDc,d,Michael Howcroft, MDa, Liliana Werner, MD, PhDb
aEye Surgeons Associates P.C., Iowa and Illinois Quad Cities, 777 Tanglefoot Lane, Bettendorf, IA 52722, USAbDepartment of Ophthalmology and Visual Sciences, John A. Moran Eye Center, University of Utah,
50 North Medical Drive, Salt Lake City, UT 84132, USAcDepartment of Ophthalmology, University of Tennessee, 6401 Poplar Avenue, Suite 190, Memphis, TN 38119, USA
dDepartment of Ophthalmology, Columbia College of Physicians and Surgeons, 630 West 168th Street,
Room 218, New York, NY 10032, USA
Vitreous loss is inevitable. Given the variety of
pathology presented by the human eye, even thebest surgeons have some complications. Despitethe application of vigilant maneuvers, broken
capsules still occur at a rate between 0.45% forvery experienced surgeons [1] and up to 14.7% forresidents in training [2]. The frequency of retainedlens fragments is estimated at 0.3% to 1.1% [3,4].
The challenge of cataract surgery is to minimizethe risk of complications and to manage optimallycomplications that do occur.
Intraoperative complications can be placedinto three categories: (1) broken capsule or lossof zonular integrity with an intact anterior hya-
loid; (2) vitreous prolapse (defined as vitreouswithin the confines of the anterior chamber); and(3) vitreous loss through the incision. Retainedlens material adds to the complicated picture. The
likelihood of postoperative sequelae increasessignificantly with each of these categories, andmotivates the surgeon to recognize and limit
damage at the earliest stage.This article provides a review and update of
techniques for handling complications when they
occur. The management of vitreous loss andretained lens fragments is the biggest determiningfactor influencing the likelihood of an excellent
visual outcome [5].
* Corresponding author.
E-mail address: [email protected] (L.B. Arbisser).
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All ri
doi:10.1016/j.ohc.2006.07.002
Sequelae
Complications of vitreous loss at cataractsurgery are as follows:
Cystoid macular edemaRetinal detachmentPersistent increase in intraocular pressure
Intraocular lens dislocation or subluxationChoroidal detachmentEndophthalmitisSuprachoroidal hemorrhage
Corneal edema
Retinal detachment may occur at the rate of 1%after uncomplicated cataract surgery and increasesto between 6.8% and 8.6% following intraoper-ative vitreous loss [6]. This jump in incidence is
related to vitreoretinal traction at the time of theprimary surgery or later secondary to biochemicaland structural changes in the vitreous accelerating
the development of a postoperative acute posteriorvitreous detachment. The incidence of retinal de-tachment increases to 14.5% when lens fragments
are retained. This statistic includes eyes with giantretinal tears [7]. Eyes with giant retinal tears havea particularly bad prognosis for successful reat-tachment and visual recovery [8]. It is not the drop-
ped nucleus or vitreous loss that directly causesmost vision threatening complications but their in-appropriate management risks retinal detachment.
By far the most common sequela of compli-cated surgery is an increased risk of cystoid
ghts reserved.
ophthalmology.theclinics.com

496 ARBISSER et al
macular edema. Cystoid macular edema seemsrelated to the increased levels of inflammatorymediators released by iris and ciliary body uveal
tissues, which are increased when the anteriorhyaloid face is ruptured and when there areretained lens fragments. Comorbidities leadingto poor visual outcome include acute and chronic
glaucoma and corneal edema. The incidence ofthese sequelae can be minimized by appropriatemanagement of complicated cataract surgery both
intraoperatively and postoperatively.In the heat of the battle one is least likely to be
logical and analytical. It behooves all to prepare
a mental flow chart of maneuvers and a sequenceof decisions before entering a patient’s eye. Thewell-prepared surgeon anticipates potential prob-lem cases, as listed below, and keeps the required
instrumentation on stand-by. This article providesa framework to maximize chances of an optimalresult.
Pseudoexfoliation syndromeTraumatic cataract
Fellow eye of complicated cataract surgeryEyes with transillumination defects in irisPreviously vitrectomized eyes
Eyes with phacodonesisDense brunescent cataractsHypermature cataracts
Very aged patientIntraoperative floppy iris syndromeHigh ammetropia
Prevention
‘‘An ounce of prevention is worth a pound ofcure.’’ One heard it from their mother as a young-ster, and the adage remains valuable today in
every endeavor. Each step of cataract surgery isbuilt on the solid foundation of the prior maneu-ver. If one has misjudged the patient’s ability to
tolerate the choice of anesthesia (or the lackthereof), or one’s own ability to communicateand work on a moving target, the stage has beenset for disaster. Clinicians advocate always having
a ‘‘plan B’’ (ie, standby intravenous anesthesia orsub-Tenon’s injection intraoperatively).
Wound construction is central to the mainte-
nance of the chamber. Minimal leak through themain incision and the paracentesis results ina deep chamber and minimization of surge and
turbulence. An understanding of the fluidics anddynamics of the phacoemulsification machineused is critical for the clinician to respond to
untoward occurrences and to optimize the in-traocular environment.
Anticipate poor zonular integrity preopera-
tively in pseudoexfoliation syndrome, traumatizedeyes, vitrectomized eyes, and the very elderly andintraoperatively by the ease with which the anteriorcapsule can be perforated and the response to
applied vectors of force during the continuouscircular capsulotomy (CCC). Be prepared withtechniques to minimize zonular stress, such as
phaco chop or supracapsular phaco.Keep capsulartension rings available. Extra dispersive viscoelas-tic (ophthalmic viscosurgical device [OVD]) and
compartmentalization of the area over zonulolysiswith viscoadaptives can save the day and preventegress of vitreous around defects. Capsular suspen-sion hooks may be rarely needed. Maintain a flat
lens dome during capsulorrhexis. The choice ofa more viscous OVD in the settings of capsuleelasticity as in the pediatric cataract or with
spherical lens morphology as in the high hyperopeis helpful. Regrasp the CCC edge frequently so thevector force is always in the right direction in case of
sudden patient movement during creation of theCCC under topical anesthesia. Improve visualiza-tion of the lens capsule in hypermature cataracts by
using capsular dye. In myopes and vitrectomizedeyes prevent or relieve reverse pupillary block toavoid an overdeep anterior chamber. Hydrodissec-tion and delineation are risky in the face of a very
shallow anterior chamber. Be careful to avoidposterior capsular rupture secondary to bag over-inflation. Risk is reduced by ‘‘burping’’ the bag as
the fluid wave progresses thereby preventing tam-ponade of the CCC edge by the nucleus. Adequatemobility of lens material inside the bag must be
established before initiating phaco to avoid stresson the zonules and a complicated disassemblyphase. Beware of capsular-cortical adhesions visi-ble as discreet broad opacities. These may contrib-
ute to capsule rupture on rotation if not gently lysedby hydrodissection or viscodissection.
During phacoemulsification keep the phaco tip
in the safe zone within the center of the pupil asmuch as possible. Only use ultrasound to gainpurchase on fragments in the periphery and limit
emulsification only to the safe zone. Always placethe nondominant hand instrument under the phacotip to avoid contact with the posterior capsule in
case of surge when emulsifying the last fragments.Silicone sleeves for irrigation and aspiration
provide a good seal and a controlled chamberwhile removing cortex. An open bag fornix cannot
be achieved with a metal sleeve because the rigid

497VITREOUS LOSS, DROPPED NUCLEUS, CATARACT SURGERY
tube permits leakage around it. Remove thesubincisional cortex first while the bag is heldopen by the remaining more easily accessedcortical material. During insertion of the intraoc-
ular lens (IOL) be certain the capsular bag issufficiently concave to avoid snagging the poste-rior capsule and disinserting proximal zonules.
Try to maintain positive pressure in the ante-rior segment at all times. This habit becomesespecially valuable when patients Valsalva, as
with unpredicted coughing. Do not withdraw thephaco tip. Instead, have the assistant hold theforehead firmly down against the headrest, affix
the hands to the patient’s face, and stay in footposition one. In this way positive pressure ismaintained and the risk of complications reduced.
Early recognition
The index of suspicion must be high toappreciate the early signs of complication and
allow optimum corrective action. Something assubtle as a bounce of the iris diaphragm, change inanterior chamber depth, or a change in pupil size
may be caused by the sudden redistribution offluid associated with a break in the posteriorcapsule.
Assuming that one has checked the phacoparameters and eliminated the possibility ofa clogged tip, loss of followability of lens materialand phaco efficiency during phaco or irrigation
and aspiration is a reliable sign that vitreous ispresent. It is vital that aspiration be discontinuedbecause vitreous cannot be ‘‘phacoed’’ and con-
tinued traction is transmitted to the retina.Phacoemulsification energy may give the surgeonthe impression that it can be used for vitrectomy
but it only liquefies the hyaluronate gel whileleaving the collagen fibers intact. It is very unsafeto place a phacoemulsifier in the vitreous to
remove the nucleus or lens fragments. Even lowflow or suction levels result in unsafe vitreoretinaltraction when the tip engages vitreous collagenfibers.
Tilting of the lens equator, loss of the ability torotate the nucleus, or a deepening of the anteriorsegment during emulsification are ominous signs
of impending loss of lens material into theposterior segment. These signs deserve immediateattention.
Anything between the lips of the incisionprevents an internal seal from forming. Ina well-constructed wound that fails to prove
watertight, after irrigating the tunnel to eliminatedebris, suspect an occult strand of vitreous in-sinuating itself invisibly and take steps to identifyit. A peaked pupil or movements of the pupil edge
with remote touch are classic signs not to beignored.
Early response
When one touches a hot stove the innate re-sponse is withdrawal. One must control that
natural response to pull out of the eye whenrecognizing a complication. The phaco tip betweenthe lips of the wound controls the intraocular
environment. On recognition of a problem goto foot position zero to maintain the anteriorchamber but do not move the phaco tip.Remove the nondominant hand instrument
from the paracentesis, which does not result inchamber instability. After removing the secondinstrument, prepare to inject OVD through the
paracentesis incision. Once the cannula is pastthe internal Descemet’s membrane while in footposition zero and instill OVD (dispersive ideally)
through the paracentesis between the posteriorcapsule and any remaining lens fragments untilthe anterior chamber is normal depth. Only then
can the phaco tip be withdrawn from the eyewithout anterior chamber collapse. If the cham-ber is permitted to collapse in the presence ofa tear in the capsule, vitreous pressure extends
the tear and the stage of complication mayprogress from capsular rupture to vitreous pro-lapse or from prolapse to vitreous loss. Vitreous
always follows the path of lowest pressure.With the incision effectively closed and the
condition static, it is time to assess the situation,
inspect, relax, and think. Announce the delay tothe operating room staff to avoid having the nextpatient, who may be on the cart in the next room,
prepared and draped prematurely. Remember,too, to relax yourself and your voice. Many timesfamily is watching and patients are awake, alert,and aware of what is going on and they need to
know that you are in calm control of the situation.Once the complication is identified the staff shouldbe able to spring into action with a prepared and
well-rehearsed plan. The vitrector should beseamlessly assembled with predetermined cuttingand aspirating parameters. The surgeon should be
familiar with the operation of the foot pedal invitrectomy mode, which is always cutting beforevacuum. Additional instruments and medications

498 ARBISSER et al
should be included in a ‘‘vitrectomy kit’’ with theitems needed to respond to the situation assem-bled as follow:
Vitrector setMicrovitreoretinal blade
Chamber maintainerWashed Kenalog (instructions)Lidocaine for subconjunctival injectionCautery
8-0 Vicryl suture (unless sutureless technique isused with 23 gauge)
Kansas forceps
CaliperVectusMiochol E
Conjunctival scissorPostoperative medicines (subconjunctival in-jection or oral)
Alternate implantOcular hypotensivesAntibiotic prophylaxis of choice
Anesthesia
In potentially difficult cases or for patients whocannot follow directions during an indirect retinalexamination, the surgeon may wish to consider
peribulbar anesthesia preoperatively. For patientswho cannot be relied on to remain still during theprocedure (pediatric, retarded, or severely claus-trophobic patients) the surgeon may consider
general anesthesia. Topical anesthesia is not,however, incompatible with managing complica-tions. Without pain receptors, the vitreous cannot
‘‘hurt.’’ Topical or intracameral anesthesia maynot require supplementation except when the parsplana incision is used, or the wound needs to be
significantly enlarged. A bleb of subconjunctivallidocaine 2% over the intended scleral incisionbefore incising a fornix flap for pars incision is
appropriate. A cellulose sponge soaked in anes-thetic as a pledget held directly in contact with thesclera for 30 seconds may also suffice.
Avoid reintroduction of intracameral unpre-
served 1% Xylocaine. Although there is evidencethat there is no permanent damage to the neuro-retina [9], there is a transient amaurosis as a result
of contact of the anesthetic with the posterior seg-ment through broken zonules or a capsule rup-ture. This can be disconcerting or even
frightening to both patient and surgeon.The availability of intravenous sedation is
desirable to help the patient cooperate or to
make the time pass more quickly during a pro-longed case. Using a calm voice (vocal local) andhaving an operating room team that can seam-
lessly prepare for a vitrectomy is extremely helpfulin minimizing patient anxiety without sedation.
If these measures fail and the patient looses theability to cooperate akinesia may be required.
First be sure the incisions are closed to avoid lossof the anterior chamber. A snip down to baresclera and use of a Greenbaum or Masket cannula
to perform sub-Tenon’s or parabulbar blockresulting in akinesia without sharp injection isoptimal. This reduces the risk of retrobulbar
hemorrhage, particularly untimely in this setting.
Damage control
After the existing complication is recognized,
one next controls the damage by compartmental-ization with a dispersive OVD. If the rent in theposterior capsule is central or paracentral, this
must be converted to a circular capsulorrhexis ifat all possible. Even when the posterior tearappears round, it still lacks resistance to extension
unless it is converted. Insinuating a small amountof OVD through the tear to push back the intactvitreous face is helpful. While zooming the mi-
croscope to high magnification, the edge of thetear may be grasped with forceps and the propercentripetal vector (directed centrally) should beapplied to minimize the size of the opening. If
there is no edge it may be necessary to start offwith a tiny cut made with a microscissor. Accom-plishing this challenging maneuver results in
a stable tear and permits the use of an ‘‘in-the-bag’’ implantation after clean up.
When the complication is recognized, posterior
chamber nuclear fragments must be raised abovethe iris plane into the anterior chamber. In thepresence of miosis, pupil stretch or microsphinc-
terotomies are helpful. It is imperative to makethe best effort to maintain the integrity of theCCC for implantation of the IOL. If it restrictsa large fragment from forward movement the
CCC can be enlarged. Under OVD control,a tangential cut is made and forceps used toenlarge the continuous tear to the minimum
effective size. Alternatively, radial relaxing in-cisions are the default to prevent a tear extendingaround the equator to the posterior capsule. Next,
maneuvers to dial, lift, cantilever, or float thenucleus or nuclear fragment with OVD can beused making them accessible for removal.

499VITREOUS LOSS, DROPPED NUCLEUS, CATARACT SURGERY
If the lens fragment is below the posteriorcapsule and has descended into the posteriorsegment, at the time of this writing there iscontroversy among anterior segment surgeons as
to its management. No controversy exists amongvitreoretinal surgeons or this article’s authors: thefragments should be left in place for later removal
with a full three-port pars plana vitrectomy andfragmenter as needed.
Dropped nucleus during cataract surgery
Contrary to the belief of some surgeons, lensmaterial cannot damage the retina. Jagged pieces
of very hard nucleus can float around the vitreouscavity and even rest on the retinal surface nevercausing retinal damage unless manipulated bya surgeon. Lens material is only slightly denser
than vitreous and the modulus of water is suchthat movement of the lens material during a sac-cade does not result in retinal damage.
Posterior-assisted levitation was recommendedby Kelman [10] to raise a dropped nucleus into theanterior chamber for removal. Inserting a spatula
through the pars plana creates positive pressure,which pushes the vitreous anteriorly creating un-safe vitreoretinal traction. Anterior displacement
of lens material with a spatula also creates exces-sive vitreoretinal traction. Passing a spatulathrough the pars plana and the choroid in a softeye may result in suprachoroidal hemorrhage
with potentially catastrophic results. Injecting vis-coelastic through the pars plana to support lensmaterial after capsular rupture as suggested by
Chang and Packard [11] also may risk suprachor-oidal hemorrhage and invariably induces anteriordisplacement of the vitreous. In a laboratory with
human eye bank eyes both with a whole eye anda Miyake analysis [12] performed by two of theauthors (LBA, LW) posterior assisted levitation
was tested.The Miyake view was not ideal for allowing
vitreous prolapse; however, it afforded a wonder-ful view of the mechanics of viscolevitation. When
placing the Viscoat cannula through the parsplana incision, it was very difficult, if not impos-sible, to place it reliably between vitreous and
dropped nucleus. It was even challenging to placethe cannula under rather than into the droppednucleus. Also observed were fragments being
directed laterally under the iris, undetectablefrom the usual surgeon’s view. Based on thesefindings, the impression was confirmed that the
risk of retinal damage through vitreous traction orleaving residual material regardless of the use ofthis maneuver outweighed the benefit. The au-thors advocate against this technique.
If a capsular defect is observed and the nucleushas not dropped, Viscoat injected through thelimbus should be used to create a barrier over the
capsular defect. These authors do not recommendviscolevitation from the pars plana.
Some surgeons have recommended using irri-
gation to mobilize the nucleus anteriorly after ithas fallen in the vitreous cavity. This too is a veryunsafe method. Remember that Machemer and
Norton [13] and previously Foulds [14] used jetsof balanced salt solution to create retinal breaksin their experimental retinal detachment model.
A lens loop has also been recommended as
a tool to retrieve a dropped nucleus from thevitreous cavity. This method can also result inretinal breaks because vitreous engaged in the
loop while attempting to lift the nucleus results inunsafe vitreoretinal traction.
There are literally scores of papers in the
literature documenting the dangers of ‘‘fishing’’for lens fragments [15–18]. If the nucleus drops,the surgeon must focus on safe management of
the vitreous, lens implantation, and the wound.It is far better practice to have a vitreoretinal spe-cialist perform vitrectomy followed by removal oflens material with the fragmenter as needed. Min-
imal requirements include a relatively clear cor-nea, a widely dilated pupil, a trained surgeonand staff, endoillumination, a cutter that operates
at 1500 cuts per minute or greater, a fast Venturisuction system, and a fundus contact lens or wideangle visualization system. It is highly unlikely
that a cataract surgery setting can rapidly andefficiently meet these requirements.
The timing of the secondary vitrectomy andfragmenter removal of the dropped nucleus is
determined on an individual case basis. Althoughthe eye sometimes tolerates small amounts of lensmaterial, the chances of chronic inflammation or
ocular hypertension are high. A vitreoretinalsurgeon’s availability to team with the anteriorsegment surgeon at the same surgery or on the
same day may prove ideal both emotionally forthe patient and structurally for the eye [19–21].Early vitrectomy (fewer than 3 weeks postopera-
tively) was associated with better visual results,whereas late vitrectomy resulted in limited visualacuity in a higher percentage of patients and in-creased the risk for glaucoma and retinal detach-
ment [22]. This may be caused in part by

500 ARBISSER et al
selection bias. Some cases may require delay topermit clearing of corneal edema for surgical visu-alization. In cases with markedly elevated intraoc-
ular pressure refractory to medical management,urgent surgical intervention may be indicated. Ingeneral, surgery within 2 weeks is probably pru-dent [5,15].
The anterior segment surgeon may be held tothe standard of care of the vitreous surgeon whencrossing the line into the posterior segment. It is
never pleasant to need two surgeries to achieve thegoal that one was to accomplish, but the pre-ponderance of evidence shows that this course
provides the best long-term outcomes. Patientsshould be counseled accordingly during preoper-ative informed consent.
The cataract surgeon’s job is to finish the case
with a clean anterior segment, a well-placed IOL,and a secure closure paving the way for thevitreoretinal surgeon if needed. Careful follow-
up, honest communication with the patient, andappropriate referral almost always lead to a happyresult. Now that the eye has been stabilized and
the damage controlled a plan must be formulatedto complete the case for the optimal outcome.
To phaco or convert to extracapsular extraction
Strict conditions exist for safely completing theremoval of nuclear fragments with ultrasound inthe setting of vitreous prolapse. It is essential there
be no admixture of vitreous and lens material.Vitreous is preferentially attracted to the phacoport displacing nucleus and preventing aspiration
of lens material. More important than the result-ing inefficiency is the danger of placing traction onthe vitreous, with a high likelihood of retinal tear
and detachment. Unless vitreous can be isolatedand compartmentalized away from lens frag-ments, the phaco handpiece should not be used
to complete the removal of the nucleus.The second condition required is the presence
of a controlled capsule tear. This must be ade-quately covered by OVD, a lens glide, or the iris to
minimize the risk of forcing nuclear fragmentsposteriorly or displacing vitreous. Acetylcholine(Miochol E) can be used to bring the pupil down
behind the fragment.When the decision is made to phaco, a slow
motion technique should be used with low-flow,
moderate vacuum and appropriate pulses ofenergy to promote followability and to minimizechatter. Because this takes place in an OVD-filled
environment, care must be taken to establishadequate flow just before activating ultrasoundenergy to avoid wound burn.
If a stable capsular tear and compartmental-ized vitreous are not the prevailing conditions,conversion to extracapsular extraction techniqueshould be pursued. Choose the incision based on
the size of the remaining fragments. If thefragment is judged to fit through an opening of4 mm or less, the clear corneal incision can be
used. Any longer incision requires at least onesuture, which increases postoperative astigmatismand prolongs healing time. For this reason it is
advisable to ensure that the clear corneal incisionis watertight and abandon it as though it weremerely a super paracentesis. Move superiorly andperform an adequate limbal or scleral tunnel
incision appropriate to the fragment size. Do notexpress with external pressure as used in primaryextracapsular surgery. That technique depends on
an intact vitreous body and, in this case, wouldexpress vitreous along with the nucleus. Instead,remove the fragment with a cystotome used as
a pick, forceps, such as a Kansas forceps, ora vectus, something to glide it out, preferablyunder an OVD sandwich always mindful of
endothelial integrity.
Vitreous management
Because vitreous is virtually invisible, preser-vative-free triamcinolone acetate (Kenalog) par-ticulate marking of the vitreous should be used to
identify its presence and to delineate the extent ofprolapse. This huge advance in the managementof complications cannot be overestimated. The
technique was first suggested by Peyman butpublished by Burk and coworkers [23] in the ante-rior segment literature. Most surgeons recom-
mend ‘‘washing’’ the Kenalog to removepreservatives that may be toxic to the endothe-lium. When the suspension is irrigated into the an-terior chamber it sticks to the vitreous matrix but
washes out of OVD or balanced salt solution andit has the effect of throwing a ‘‘sheet over a ghost’’guiding vitreous removal and providing a secure
end point for its removal (Fig. 1). Care shouldbe taken to remove as much triamcinolone as pos-sible by the conclusion of the case because some
patients may show a steroid response of ocularhypertension. Even when no obvious suspensionremains there is a desirable anti-inflammatory

501VITREOUS LOSS, DROPPED NUCLEUS, CATARACT SURGERY
therapeutic effect along with the diagnosticadvantage.
Cellulose sponges are still used by many
surgeons for anterior vitrectomy and for testingfor vitreous in the anterior chamber, in thewound, or on the iris. This was first introduced
in 1968 [24]. Leading vitreoretinal surgeons haveuniversally recommended against cellulose spongevitrectomy for three decades because it inherently
causes marked instantaneous vitreoretinal trac-tion. Traction on the anterior vitreous is particu-larly dangerous because of proximity to the
strong, permanent vitreoretinal adherence at thevitreous base and the fact that peripheral retinahas approximately 1/100 the tensile strength ofposterior retina. The sponge produces traction
both by wicking and by lifting to cut the vitreousstrand.
The wound should not be swept with a spatula.
This produces vitreoretinal traction with one endof the collagen fibers entrapped in the wound andthe other end adherent to thin peripheral retina at
the vitreous base. The vitreous cutter should beused to amputate any posterior connection towound-entrapped vitreous. In some instances
OVD can be used to reposit vitreous.Unlike scissors, which cause traction, vitreous
cutters section vitreous collagen fibers by shearingas the inner needle moves past a port in the outer
needle. Fast cutting (800 cuts per minute andgreater) reduces vitreoretinal traction as collagenfibers flow through the port. The smaller the
average cut fiber length, the less vitreoretinaltraction that is produced. Fast cutting also limitsflowbecause the port is temporarily obstructed as it
cycles open and closed increasing fluidic stability.This is analogous to the anterior chamber stabilityproduced by high-vacuum, low-flow phaco.
Fig. 1. Kenalog identification of vitreous.
Low suction levels and low flow rates are saferbecause they produce less vitreoretinal tractionbecause of uncut collagen fibers traveling throughthe cutter. The suction or flow rate should be
slowly increased until vitreous starts being re-moved, while always using the highest cutting rateavailable. The cutter should be held stationary or
advanced into the vitreous while suction is appliedto reduce traction; it is unsafe to pull back on theprobe while the foot pedal is in position three with
vacuum engaged. The cutter tip should always bein view.
Laboratory findings
The authors tested various methods to removeprolapsed and lost vitreous in cadaver eyes. Theanterior segment vitrector of the Infiniti phacoe-
mulsification machine (Alcon, Irvine, California)cuts at 800 cuts per minute and the air pumpfrom the Accurus posterior vitrectomy machine
(Alcon) were used.With both Miyake preparations and with
whole eyes the authors performed vitrectomy for
prolapsed and lost vitreous with two techniques:anterior clear cornea vitrectomy under air andpars plana partial vitrectomy with anterior bal-
anced salt solution irrigation. Kenalog tattooedthe vitreous to facilitate visualization [25].
One of the goals was to assess whether onecould be thorough and efficient with air in the
anterior chamber. The motivation was to finda way to keep tenuous anterior segment surgeonsfrom having to learn a pars plana approach
without sacrificing its benefits. The authors aretotally convinced that the pars plana approachwith balanced salt solution is superior to the
standard limbal approach most commonly usedboth by viewing vitreous removal when Kenalog-stained by the surgeon’s view and by the Miyake
view [26,27]. The authors used the Accurus topump air at several intraocular pressures througha chamber maintainer anteriorly and the Infinitivitrector handpiece with a chamber maintainer
for inflow through a clear corneal paracentesis.A tight-fitting incision through the clear corneawas fashioned with the 20-gauge microvitreoreti-
nal blade.Although the authors removed vitreous effi-
ciently under the air bubble, visualization was
compromised. The air-vitreous interface couldonly be seen once the Viscoat in the anteriorchamber (which is normally used to stabilize the

502 ARBISSER et al
chamber when the complication is recognized)was finally sufficiently removed to allow fora complete bubble. Loculation of the bubble was
a significant factor affecting efficiency. Also, thebubble could leak out of a slightly too largeincision. This impedes chamber maintenance andpressure control. It also was difficult to control the
bubble, which sometimes loculates into the vitre-ous cavity leaving air out of sight (except in theMiyake view). This may be a potential mechanism
for vitreous displacement and traction on theretina or vitreous base. Lastly, vitreous trappedin the incision was flattened by the air and difficult
to remove. The authors feared nipping the iris orcapsule edge during attempts to amputate thisescaped vitreous. To remove residual cortex or toplace an implant (the next steps in vivo), the
bubble had to be removed because the leaves ofthe iris and anterior and posterior capsule flapsare all smashed together by the surface tension of
the bubble precluding access to appropriateplanes of tissue.
Although the authors use a soft shell of
Viscoat against the corneal endothelium to pre-vent corneal contact with the air there remainssome concern about endothelial toxicity especially
if the bubble is left in place long term. Severalarticles from the literature support some degree oftoxicity [28,29]. An additional disadvantage is thatthe patient cannot see until the air bubble
disappears.Most importantly, it was impossible to keep
the pressure from becoming lower in the anterior
segment relative to the posterior segment. Vitre-ous always flows to the path of lower pressurealong a gradient. This had the effect of allowing
vitreous to flow forward again (after apparentadequate vitrectomy) around the bubble duringattempted closure of the incisions or during anymanipulation to complete the case.
Every time the authors finished a specimenthey then completed the vitrectomy with a parsplana incision. They now had a reliable removal
without recurrent prolapse or presentation to theincision despite manipulation of the anteriorchamber or the eye after incision closure. It is
believed that this is caused by better removal ofvitreous behind the iris and by leaving a pressuregradient, causing the vitreous to ‘‘stay at home.’’
The authors also confirmed that sweeping andwecking the incision resulted in traction. With thepars plana approach entrapped vitreous could beamputated below the iris edge severing attach-
ments to vitreous between the lips of the incision.
The remaining anterior vitreous was simplywecked away by touching the exterior of the lim-bus only and without any traction at all. It was
worthwhile retattooing the vitreous with Kenalogto confirm its complete removal and eliminatingthe need to sweep the incision.
With multiple attempts to remove prolapsed
vitreous completely (with Kenalog identification)the authors found that the biaxial pars planaapproach with the vitrector posteriorly and irri-
gation anteriorly was vastly superior in all re-spects to the bubble vitrectomy or standardanterior limbal approach.
Biaxial pars plana vitrectomy
Any phaco incision, clear corneal or scleral, istoo large to secure a closed system with thevitrector handpiece without a coaxial sleeve.
Two-handed vitrectomy has become standard ofcare because of the reduced tendency to displacevitreous and promote further prolapse. The orig-
inal clear corneal paracentesis becomes the portfor irrigation through a chamber maintainer,butterfly needle, or other cannula of 20 or 23
gauge. Thought then needs to be given to thecreation of the vitrectomy port incision. Just asone would never use a leaky incision safely for the
rest of the procedure so does the incision needsnuggly to fit the vitrectomy handpiece. A 20-gauge microvitreoretinal blade or a keratomecapable of creating this size opening can be
used. The goal is to remove all vitreous from theanterior segment and back behind the plane of theposterior capsule. The authors do not recommend
a paracentesis-like clear corneal incision butrather a pars plana approach, which is far moreefficacious because the vitreous is drawn in the
proper direction rather than being encouraged tocome forward. Particularly in the setting ofzonular dehiscence it can be safer to draw vitreous
back down, lowering the risk of further unzippingthe zonular apparatus. The only way to removevitreous behind the iris and leave a lower pressureposteriorly relative to the anterior segment is by
the pars plana. This approach results in the bestamputation of the forward vitreous, severing anyattachments to vitreous in the anterior segment.
The pars plana incision is made by creatinga small fornix-based flap away from the fourcardinal positions to avoid ciliary nerves and
vessels. Apply minimal cautery as needed to anyvessels that bleed and measure with a caliper forthe sclerotomy 3.5 mm posterior to the limbus
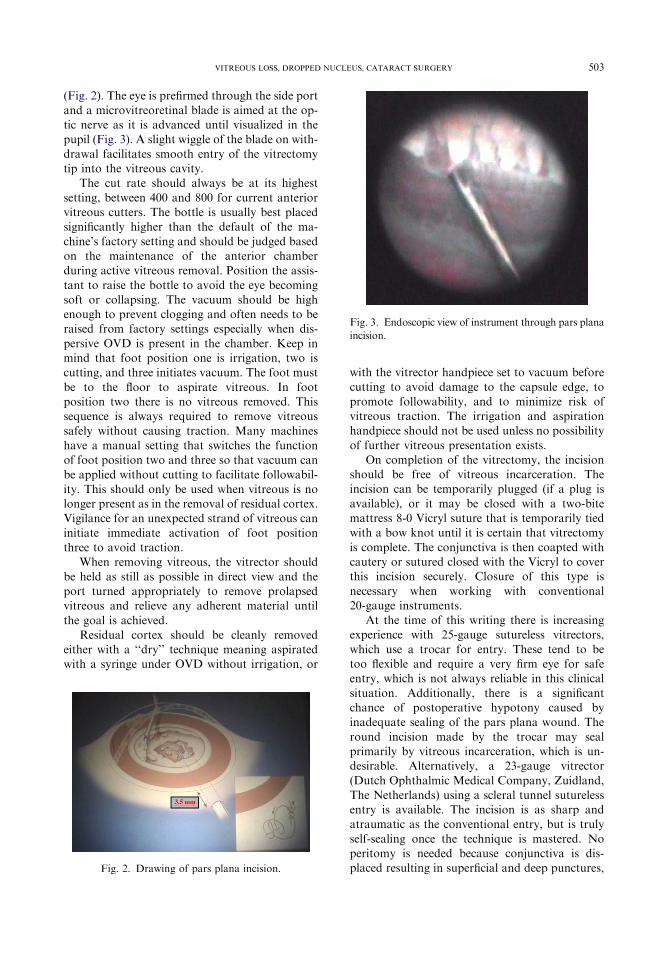
503VITREOUS LOSS, DROPPED NUCLEUS, CATARACT SURGERY
(Fig. 2). The eye is prefirmed through the side portand a microvitreoretinal blade is aimed at the op-tic nerve as it is advanced until visualized in thepupil (Fig. 3). A slight wiggle of the blade on with-
drawal facilitates smooth entry of the vitrectomytip into the vitreous cavity.
The cut rate should always be at its highest
setting, between 400 and 800 for current anteriorvitreous cutters. The bottle is usually best placedsignificantly higher than the default of the ma-
chine’s factory setting and should be judged basedon the maintenance of the anterior chamberduring active vitreous removal. Position the assis-
tant to raise the bottle to avoid the eye becomingsoft or collapsing. The vacuum should be highenough to prevent clogging and often needs to beraised from factory settings especially when dis-
persive OVD is present in the chamber. Keep inmind that foot position one is irrigation, two iscutting, and three initiates vacuum. The foot must
be to the floor to aspirate vitreous. In footposition two there is no vitreous removed. Thissequence is always required to remove vitreous
safely without causing traction. Many machineshave a manual setting that switches the functionof foot position two and three so that vacuum can
be applied without cutting to facilitate followabil-ity. This should only be used when vitreous is nolonger present as in the removal of residual cortex.Vigilance for an unexpected strand of vitreous can
initiate immediate activation of foot positionthree to avoid traction.
When removing vitreous, the vitrector should
be held as still as possible in direct view and theport turned appropriately to remove prolapsedvitreous and relieve any adherent material until
the goal is achieved.Residual cortex should be cleanly removed
either with a ‘‘dry’’ technique meaning aspiratedwith a syringe under OVD without irrigation, or
Fig. 2. Drawing of pars plana incision.
with the vitrector handpiece set to vacuum beforecutting to avoid damage to the capsule edge, to
promote followability, and to minimize risk ofvitreous traction. The irrigation and aspirationhandpiece should not be used unless no possibility
of further vitreous presentation exists.On completion of the vitrectomy, the incision
should be free of vitreous incarceration. Theincision can be temporarily plugged (if a plug is
available), or it may be closed with a two-bitemattress 8-0 Vicryl suture that is temporarily tiedwith a bow knot until it is certain that vitrectomy
is complete. The conjunctiva is then coapted withcautery or sutured closed with the Vicryl to coverthis incision securely. Closure of this type is
necessary when working with conventional20-gauge instruments.
At the time of this writing there is increasingexperience with 25-gauge sutureless vitrectors,
which use a trocar for entry. These tend to betoo flexible and require a very firm eye for safeentry, which is not always reliable in this clinical
situation. Additionally, there is a significantchance of postoperative hypotony caused byinadequate sealing of the pars plana wound. The
round incision made by the trocar may sealprimarily by vitreous incarceration, which is un-desirable. Alternatively, a 23-gauge vitrector
(Dutch Ophthalmic Medical Company, Zuidland,The Netherlands) using a scleral tunnel suturelessentry is available. The incision is as sharp andatraumatic as the conventional entry, but is truly
self-sealing once the technique is mastered. Noperitomy is needed because conjunctiva is dis-placed resulting in superficial and deep punctures,
Fig. 3. Endoscopic view of instrument through pars plana
incision.

504 ARBISSER et al
which are not coincident. The entry is made witha special microvitreoretinal blade followed by atrocar, which is immediately placed gaining a
port for the insertion of the cutter. Real-timeendoscopy reveals a clean entry with no tractionwith this method and a virtually undetectable inci-sion on removal of instruments. Some form of su-
tureless vitrectomy incision may ultimately proveto be the most efficient technique for the anteriorsegment surgeon’s purposes.
The goal is vigilantly to avoid vitreous tractionwhile thoroughly removing any vitreous anteriorto the posterior capsule. A pars plana approach
most effectively accomplishes this goal.
Inspection and intraocular lens choice
One must stop and inspect. Verify a clean bag
and the absence of residual vitreous prolapse. Usean instrument gently to retract the pupil edge, andconsider a slit beam or external illumination. A
last small injection of Kenalog may be indicatedto verify the absence of vitreous. Be sure the pupilis round without a peak, which is pathognomonicof a residual vitreous strand adherent usually to
the incision. The pupil should be constrictedbefore the end of the case to verify symmetry.Be certain all incisions are sealable. Evaluate the
intactness of the CCC and the extent of theposterior capsule tear and residual sulcus support.
A foldable IOL should be placed in the bag
only if the posterior tear has been converted toa CCC or there are less than 3 hours of zonulol-ysis without a capsular tension ring. The haptic
should be placed to support the area of zonulol-ysis. Lacking a posterior capsule if the anteriorCCC is intact the foldable lens should have sulcushaptic placement with the optic captured through
the CCC into the bag. In the absence of an intactCCC, a sulcus-style IOL may be placed entirely inthe sulcus if there is adequate posterior capsule
support 180 degrees apart. Avoid plate haptic andone-piece acrylic lenses. They are not intended forthe sulcus and can only appropriately be placed
into an intact capsular bag. The sulcus lens hapticdiameter should be at least 13 mm from end toend. All of the foldable lenses can be placedthrough any style incision.
A single piece polymethyl methacrylate lensshould only be used through a scleral or limbalwound because a larger than 4-mm incision is
required. In the absence of capsular support onecould use a sutured posterior chamber lens either
iris or scleral fixated or an anterior chamber openloop lens according to surgeon preference. Con-sider reducing operative time and trauma after
a difficult case by the choice of the anteriorchamber lens. A patent peripheral iridectomy isthen needed best accomplished with the vitrectorin an OVD ‘‘dry’’ environment. When appropri-
ately sized for an eye, the modern-style lenses havenot been associated with an increased risk ofcorneal decompensation or glaucoma.
If the surgeon has been unable to clean theanterior chamber or there is significant edema andreduced view by the end of the case, and partic-
ularly if posterior loss of lens material is con-firmed or suspected, leaving the eye temporarilyaphakic may be the wisest option. A poorly placedlens or an unstable one can create increased
inflammation and hamper a subsequent vitreor-etinal procedure.
Postoperative care
Because of the increased surgical time andtissue manipulation associated with these compli-cations, the surgeon should anticipate increased
postoperative inflammation. This requires inten-sive topical steroids and nonsteroidal anti-inflam-matory medications. The surgeon may also wish
to consider peribulbar steroids at the conclusionof the surgery.
Remember that there is a significantly in-
creased risk of endophthalmitis with vitreousloss compared with lens extraction with an intactcapsule. Consideration should be given to more
elaborate antibiotic prophylaxis, such as subcon-junctival injection of antibiotics or oral dosing offourth-generation fluoroquinolone if there is nosystemic contraindication. At the time of this
writing, intracameral antibiotics are being ex-plored for their safety and efficacy.
Intraocular pressure elevation, often severe, is
common. A variety of antihypertensive medica-tions and carbonic anhydrase inhibitors are usu-ally required. High intraocular pressure within the
first 24 hours is often caused by retained OVD,whereas the high pressure from the inflammationsecondary to retained lens fragments takes severaldays to develop.
If there are retained lens fragments, a timelyreferral to a retinal surgeon is well advised. Simi-larly, a careful peripheral indented retinal exami-
nation should be performed in all patients withvitreous loss within 2 to 4 weeks of the surgery [30].
505VITREOUS LOSS, DROPPED NUCLEUS, CATARACT SURGERY
The surgeon must have a frank and completediscussion of the surgical complication with thepatient not only to explain all the steps taken andplanned to minimize the risk of problems but also
to enlist the patient’s vigilance for symptoms ofcomplications in the future [31].
It is important to remember that although
vitreous loss, with or without retained lens frag-ments, is a serious cataract surgery complication,most patients achieve good visual recovery [32].
Careful preoperative, intraoperative, and postop-erative care can help reduce the risk of visual loss.
Summary
Cellulose sponges, sweeping the wound, pull-ing back on the cutter, using scissors to cut thevitreous, a high flow rate or vacuum setting
coupled with low cutting rates, and bubble re-moval all cause anterior movement and tractionon the vitreous, which may result in retinal tearsand detachment. One should never fish for drop-
ped lens fragments. Management of droppednucleus and pars plana biaxial anterior vitrectomyusing the concepts described can reduce retinal
detachment and other complications. Effectivelydealing with crisis is, more often than not, a matterof having prepared for crisis. It is hoped that this
article helps one achieve the excellent visualresults that are still obtainable in these challengingcases.
References
[1] Gimbel HV. Posterior capsule tears using phacoe-
mulsification causes, prevention and management.
Eur J Implant Refract Surg 1990;2:63–9.
[2] Allinson RW, Metrikin DC, Fante RG. Incidence
of vitreous loss among third year residents perform-
ing phacoemulsification. Ophthalmology 1992;99:
726–30.
[3] Leaming DV. Practice styles and preferences of
ASCRS members–1994 survey. J Cataract Refract
Surg 1995;21:378–85.
[4] Pande N, Dabbs TR. Incidence of lens matter dislo-
cation during phacoemulsification. J Cataract
Refract Surg 1996;22:737–42.
[5] Scott IU, Flynn HW Jr, Smiddy WE, et al. Clinical
features and outcomes of pars plana vitrectomy in
patients with retained lens fragments. Ophthalmol-
ogy 2003;110:1567–72.
[6] Aaberg TM Jr. Retinal detachment in eyes undergo-
ing pars plana vitrectomy for removal of retained
lens fragments discussion. Ophthalmology 2003;
110:713.
[7] Aaberg TM Jr, Rubsamen PE, Flynn HW, et al.
Giant retinal tear as a complication of attempted
removal of intravitreal lens fragments during cata-
ract surgery. Am J Ophthalmol 1997;124:222–6.
[8] Blodi BA, Flynn HW Jr, Blodi CF, et al. Retained
nuclei after cataract surgery. Ophthalmology 1992;
99:41–4.
[9] Lincoff H, Zweifach P, Brodie S, et al. Intraocular
injection of lidocaine. Ophthalmology 1985;92(11):
1587–91.
[10] Kelman CD. Posterior capsule rupture: PAL tech-
nique. Video J Cataract Refract Surg 1996;12:2.
[11] Chang DF, Packard RB. Posterior assisted levita-
tion for nucleus retrieval using Viscoat after poste-
rior capsule rupture. J Cataract Refract Surg 2003;
29:1860–5.
[12] Eller AW, Barad RF. Miyake analysis of anterior
vitrectomy techniques. J Cataract Refract Surg
1996;22:213–7.
[13] Machemer R, Norton EW. Experimental retinal
detachment and reattachment: I. Methods, clinical
picture and histology. Bibl Ophthalmol 1969;79:
80–90.
[14] Foulds WS. Experimental detachment of the retina
and its effect on the intraocular fluid dynamics.
Bibl Ophthalmol 1969;79:51–63.
[15] Moore JK, Scott IU, Flynn HW, et al. Retinal de-
tachment in eyes undergoing pars plana vitrectomy
for removal of retained lens fragments. Ophthalmol-
ogy 2003;110:709–14.
[16] Scott IU, Flynn HW Jr. Retained lens fragments
after cataract surgery. Ophthalmol Clin North Am
2001;14:675–9.
[17] Kapusta MA, Chen J, Lam W. Outcomes of drop-
ped nucleus during phacoemulsification. Ophthal-
mology 1996;103:1184–7.
[18] Lambrou FH, Stewart MW. Management of dislo-
cated lens fragments during phacoemulsification.
Ophthalmology 1992;99:1260–2.
[19] Kim JE, Han DP. Managing retained lens frag-
ments. J Cataract Refract Surg Today 2005;8:
63–6.
[20] Kageyama T, AyakiM, OgasawaraM, et al. Results
of vitrectomy performed at the time of phacoemulsi-
fication complicated by intravitreal lens fragments.
Br J Ophthalmol 2001;85:1038–40.
[21] Kim J, Flynn HW, Smiddy WE, et al. Retained lens
fragments after phacoemulsification. Ophthalmol-
ogy 1994;101:1827–32.
[22] Stefaniotou M, Aspiotis M, Pappa C, et al. Timing
of dislocated nuclear fragment management after
cataract surgery. J Cataract Refract Surg 2003;29:
1985–8.
[23] Burk SE,DaMataAP, SnyderME, et al. Visualizing
vitreous using Kenalog suspension. J Cataract
Refract Surg 2003;29:645–51.
[24] Kasner D. Vitrectomy: a new approach to the man-
agement of vitreous. Highlights Ophthalmol 1968;
11:304–29.

506 ARBISSER et al
[25] Apple DJ, Lim ES, Morgan RC, et al. Preparation
and study of human eyes obtained postmortem
with the Miyake posterior photographic technique.
Ophthalmology 1990;97:810–6.
[26] Burk S. Identifying the vile humor. First place video
ESCRS September 6–10, 2003, Munich, Germany.
[27] Eller AW, Barad RF. Miyake analysis of anterior
vitrectomy techniques. J Cataract Refract Surg
1996;22:213–7.
[28] WilsonLDA,YoshizumiMO,HallM.Theocular ef-
fects of gaseswhen infected into the anterior chamber
of rabbit eyes. Arch Ophthalmol 1991;109:571–5.
[29] Green K, Cheeks L, Stewart DA, et al. Intraocular
gas effects on corneal endothelial permeability.
Lens Eye Toxic Res 1992;9:85–91.
[30] BorneMJ, TasmanW, Regillo C, et al. Outcomes of
vitrectomy for retained lens fragments. Ophthalmol-
ogy 1996;103:971–6.
[31] Monshizadeh R, Samiy N, Haimovici R. Manage-
ment of retained intravitreal lens fragments after cat-
aract surgery. Surv Ophthalmol 1999;43:397–404.
[32] Tan JHY, Karwatowski WSS. Phacoemulsifica-
tion cataract surgery and unplanned anterior vitrec-
tomydis it bad news? Eye 2002;16:117–20.

Ophthalmol Clin N Am 19 (2006) 507–519
Capsular Tension Rings: Update on EndocapsularSupport Devices
Khalid Hasanee, MD, FRCSCa, Iqbal Ike K. Ahmed, MD, FRCSCa,b,*aUniversity of Toronto, Toronto, Ontario, Canada
bUniversity of Utah, 201 South Presidents Circle, Room 201, Salt Lake City, UT 84112, USA
Small-incision phacoemulsification with endo-
capsular posterior chamber intraocular lens(PCIOL) fixation has become the standard ofcare in cataract management because of numerous
intraoperative and postoperative advantages.When associated with zonular weakness, cataractsurgery is associated with increased risk of vitre-ous prolapse, capsular rupture, retained lens
material, and postoperative IOL dislocation. Incases of profound zonular dialysis, alternativeapproaches have included intracapsular cataract
extraction or pars plana vitrectomy and lensec-tomy. The capsular tension ring (CTR) and itsderivatives have enabled surgeons to approach
zonular weakness with improved safety, andspawned novel surgical techniques. Successfulphacoemulsification approaches in these cases
requires stabilization of the capsulozonular appa-ratus during surgery, enabling the surgeon safelyto remove the crystalline lens, retain the capsularbag, and place a PCIOL securely. This requires an
understanding of capsule and zonular anatomy,development of a grading system for zonular weak-ness, technique modifications, and an understand-
ing of available capsular tension devices and theirselection criteria.
Approach to weak zonules
It is often helpful to categorize the approach to
compromised zonules into methods of cataract
* Corresponding author. Credit Valley EyeCare,
3200 Erin Mills Parkway, Unit 1, Mississauga, Ontario
L5L 1W8, Canada.
E-mail address: [email protected]
(I.I.K. Ahmed).
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All ri
doi:10.1016/j.ohc.2006.07.001
extraction and IOL fixation. Cataract extraction
options include phacoemulsification and extracap-sular or intracapsular approaches. In severe cases,a posterior approach with pars plana lensectomy
and vitrectomy may also be considered. Phacoe-mulsification, by maintaining the advantages ofsmall-incision surgery, is the preferred option,assuming this can be safely performed.
IOL implantation options include a sulcusPCIOL, an anterior chamber IOL, iris-fixatedIOL, or in-the-bag PCIOL with CTR. Capsular
bag fixation is the ideal location of an IOL,providing optimal biocompatibility, centration,and optics, assuming it can remain in a stable
position in the long-term. The CTR and itsmodifications permit small-incision phacoemulsi-fication and endocapsular PCIOL fixation in mild,
moderate, and severe cases of zonular loss.
Defining zonular weakness: clock hours versus
severity
Zonular weakness can be categorized accordingto the number of clock hours (degree of zonulardialysis) and the severity of generalized zonular
instability [1–4]. This division is key because spe-cific zonular cases each have their own underlyingetiologies or a combination thereof. The choice ofcataract extraction and endocapsular support de-
vice relies greatly on this distinction.
How the capsular tension ring works
The CTR serves two functions: an intraoper-ative support tool during cataract surgery or
a long-term implant device for postoperativeIOL fixation. Because the diameter of the CTR
ghts reserved.
ophthalmology.theclinics.com
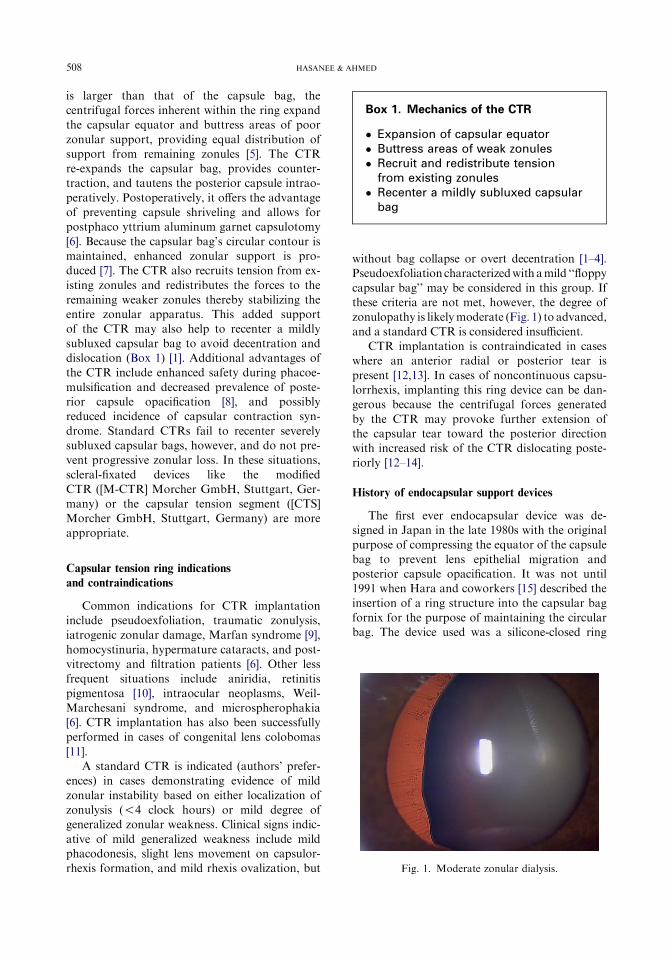
508 HASANEE & AHMED
is larger than that of the capsule bag, thecentrifugal forces inherent within the ring expandthe capsular equator and buttress areas of poor
zonular support, providing equal distribution ofsupport from remaining zonules [5]. The CTRre-expands the capsular bag, provides counter-traction, and tautens the posterior capsule intrao-
peratively. Postoperatively, it offers the advantageof preventing capsule shriveling and allows forpostphaco yttrium aluminum garnet capsulotomy
[6]. Because the capsular bag’s circular contour ismaintained, enhanced zonular support is pro-duced [7]. The CTR also recruits tension from ex-
isting zonules and redistributes the forces to theremaining weaker zonules thereby stabilizing theentire zonular apparatus. This added supportof the CTR may also help to recenter a mildly
subluxed capsular bag to avoid decentration anddislocation (Box 1) [1]. Additional advantages ofthe CTR include enhanced safety during phacoe-
mulsification and decreased prevalence of poste-rior capsule opacification [8], and possiblyreduced incidence of capsular contraction syn-
drome. Standard CTRs fail to recenter severelysubluxed capsular bags, however, and do not pre-vent progressive zonular loss. In these situations,
scleral-fixated devices like the modifiedCTR ([M-CTR] Morcher GmbH, Stuttgart, Ger-many) or the capsular tension segment ([CTS]Morcher GmbH, Stuttgart, Germany) are more
appropriate.
Capsular tension ring indications
and contraindications
Common indications for CTR implantationinclude pseudoexfoliation, traumatic zonulysis,iatrogenic zonular damage, Marfan syndrome [9],
homocystinuria, hypermature cataracts, and post-vitrectomy and filtration patients [6]. Other lessfrequent situations include aniridia, retinitis
pigmentosa [10], intraocular neoplasms, Weil-Marchesani syndrome, and microspherophakia[6]. CTR implantation has also been successfullyperformed in cases of congenital lens colobomas
[11].A standard CTR is indicated (authors’ prefer-
ences) in cases demonstrating evidence of mild
zonular instability based on either localization ofzonulysis (!4 clock hours) or mild degree ofgeneralized zonular weakness. Clinical signs indic-
ative of mild generalized weakness include mildphacodonesis, slight lens movement on capsulor-rhexis formation, and mild rhexis ovalization, but
without bag collapse or overt decentration [1–4].Pseudoexfoliation characterizedwith amild ‘‘floppy
capsular bag’’ may be considered in this group. Ifthese criteria are not met, however, the degree ofzonulopathy is likelymoderate (Fig. 1) to advanced,
and a standard CTR is considered insufficient.CTR implantation is contraindicated in cases
where an anterior radial or posterior tear is
present [12,13]. In cases of noncontinuous capsu-lorrhexis, implanting this ring device can be dan-gerous because the centrifugal forces generated
by the CTR may provoke further extension ofthe capsular tear toward the posterior directionwith increased risk of the CTR dislocating poste-riorly [12–14].
History of endocapsular support devices
The first ever endocapsular device was de-signed in Japan in the late 1980s with the originalpurpose of compressing the equator of the capsule
bag to prevent lens epithelial migration andposterior capsule opacification. It was not until1991 when Hara and coworkers [15] described the
insertion of a ring structure into the capsular bagfornix for the purpose of maintaining the circularbag. The device used was a silicone-closed ring
Box 1. Mechanics of the CTR
� Expansion of capsular equator� Buttress areas of weak zonules� Recruit and redistribute tension
from existing zonules� Recenter a mildly subluxed capsular
bag
Fig. 1. Moderate zonular dialysis.

509CAPSULAR TENSION RINGS
called the ‘‘equator ring.’’ Although the equatorring maintained the circular contour of the cap-sule, its closed-ring structure limited its usebecause it was not designed for capsular bags
of varying sizes. Also in 1991, Nagamoto andBissen-Miyajuma [16] presented a video at thefilm festival of the American Society of Cataract
and Refractive Surgery describing an open poly-methyl methacrylate (PMMA) ring. Known asthe ‘‘capsular bag supporting ring,’’ this device
was further described in an experiment involvinghuman cadaver eyes published in 1994.
Leger and Witschel [5] introduced the CTR at
the American Society of Cataract and RefractiveSurgery meeting in May 1993. The CTR was thefirst open PMMA ring to be implanted during cat-aract surgery, and had the advantage of having
eyelets on either free end. The rounded eyeletsserved to lower the risk of spearing the capsularfornix on insertion and enhancing intracapsular
manipulation of the ring.After the introduction of the CTR, a variety of
devices have been designed to expand further on
the CTR’s initial surgical application. The capsu-lar edge ring addressed the issue that gave birth tothe CTR idea in the first place, namely posterior
capsular opacification. It was devised with asquare-edge intended to repel the advancementof epithelial cells on the posterior capsule thatleads to opacification [17].
In 1998, Cionni and coworkers [18] reportedthe use of an open endocapsular ring with themodification of a fixation hook positioned ante-
rior to the main ring filament. The hook has aneyelet on the tip that acts as an anchor for sutur-ing without damaging the capsular bag. Known as
the ‘‘modified CTR’’ (M-CTR), this ring is of par-ticular importance in cases of profound and pro-gressive zonular weakness.
The CTS, introduced by Ahmed in 2002 [19],
was developed to deal with cases of profoundzonular weakness. The CTS is a 90-degree partialPMMA ring segment that also has a central fix-
ation eyelet. The eyelet offers both intraoperativesupport through iris hooks or long-term postop-erative fixation with scleral sutures. Because of
its smaller size, it can safely be implanted incases of anteroposterior capsule tears or incom-plete rhexis. Multiple (two to three) segments
may be inserted as depending on the amountof zonular support needed. This device mayalso be combined with other endocapsular sup-port devices as needed to address different zonu-
lar concerns.
Current endocapsular devices
Standard capsular tension ring
In 1991, Hara and coworkers [15] andNagamoto and Bissen-Miyajuna [16] introduced
the first endocapsular devices. This was later pop-ularized and further developed by Legler and co-workers [5] in 1993. The standard CTR (Fig. 2)is an open-ring structure made of PMMA. This
compressible circular ring has an oval-shapedcross-section with two smooth-edged end termi-nals. The ‘‘ski ramp’’ design of the end terminals
aids to avoid entrapment of the capsular equatoron insertion and also allows for placement of sec-ondary instrumentation.
Both Morcher GmbH (Stuttgart, Germany)and Ophtec (Groningen, The Netherlands) man-ufacture US Food and Drug Administration–approved CTRs. The Morcher ring (also labeled
the ‘‘reform ring’’) is available in three differentsizes based on an uncompressed diameter: type 14,12.3 mm (compresses to 10 mm); type 14C, 13 mm
(compresses to 11 mm); and type 14A, 14.5 mm(compresses to 12 mm). The Ophtec ring (Ad-vanced Medical Optics, Irvine, California; labeled
as ‘‘StabilEyes’’ in the United States) is availablein a 13-mm ring that compresses to 11 mm, anda 12-mm ring that compresses to 10 mm. Implan-
tation of the CTR may be performed manually orwith an injector (authors’ preference). Both Oph-tec and Geuder (Heidelberg, Germany) manufac-ture CTR injectors.
In a prospective study of 21 eyes, Jacob andcoworkers [1] evaluated the safety and efficacy ofthe CTR in patients with less than 150 degrees of
zonular dialysis (mean follow-up of 242.33 days).
Fig. 2. Standard capsular tension ring.

510 HASANEE & AHMED
They found that phacoemulsification with in-the-bag PCIOL and CTR implantation had a 90.47%success rate. Capsular collapse did not occur in
any eye, but two eyes developed intraoperative ex-tensionof dialysis. Fifteen eyes (71.42%)hadafinalvisual acuity of 20/40 or better. All patients withsuccessful implantation remained well centered at
6 months.There have been few published studies exam-
ining the safety and efficacy of the CTR in
cataract surgery. Bayraktar and coworkers [2]examined the effect of the CTR in preventing zon-ular complications during phacoemulsification in
pseudoexfoliation patients. This prospective ran-domized study of 78 eyes with pseudoexfoliationcataracts was randomly divided into two groups.CTRs were implanted in 39 eyes and 39 served
as controls without CTR implantation. Five eyes(12.8%) in the control group and no eyes in theCTR group developed intraoperative zonular sep-
aration. The posterior capsule rupture rate was7.7% in the control and 5.2% in the CTR groups.Capsular IOL fixation was 94.9% and 74.3% in
the CTR and control groups, respectively.In their retrospective series of 14 cases with
loose or broken zonules managed with CTR,
Gimbel and coworkers [3] concluded that CTRshelp to avoid capsular bag collapse and vitreouspresentation during surgery. No observable IOLdecentration occurred in their group.
Lee and coworkers [20] examined the issue ofIOL tilt and decentration in their report on 40eyes of 20 patients who were followed for
2 months. Each patient had an IOL in one eyeand a CTR with an IOL in the fellow eye. TheIOL-CTR group had a statistically less rate of
IOL decentration versus the IOL-only group.The mean decentration in the IOL-CTR groupwas 0.42 � 0.17 mm, whereas the IOL-onlygroup was 0.57 � 0.16 mm. The amount of IOL
tilt at 60 days was also significantly less in theIOL-CTR group (IOL-CTR: 2.47 � 0.40 degrees;IOL-only: 3.06 � 0.56 degrees).
Price and coworkers [21] reported their resultsof a phase III multicenter, nonrandomized investi-gational study evaluating the safety and efficacy of
the Ophtec CTR in cases of weak zonules duringcataract extraction. A total of 255 CTRs wasplaced in patients who were found to have weak-
ened or broken zonules comprising !34% of thecircumference of the lens capsule. Two CTRmodels were evaluated, with noncompresseddiameters of 12 and 13 mm. It was concluded
that both Ophtec CTR models safely provided
capsular support during and after cataract surgeryin cases of weak zonules. Patients were examined,intraoperatively and postoperatively, at Day 1
and Months 1, 3, 6, and 12. Interim results dem-onstrated that immediately after surgery 98.8%of IOLs were centered. Subsequently, the preva-lence of IOL decentration was 1.7% at 3 months,
3.8% at 6 months, and 2.3% at 12 months. Theprimary complication was posterior capsule opa-cification. Neodymium:yttrium-aluminum-garnet
capsulotomies were performed in 12.8% of eyesby 12 months postoperatively. They concluded,however, that the posterior capsule opacification
was not caused by CTR insertion.
Choosing appropriate capsular tension ring size
The selection of CTR size is based on capsularbag dimensions. Typically, a larger capsular bagrequires a larger ring with the reverse holding
true. Many surgeons prefer to choose a slightlylarger implant, with 13 mm being most common.Overlap of the end terminals is needed to provide
for complete circumferential support. Vass andcoworkers [22] have shown that the size of thecapsular bag positively correlates with the globe’s
axial length. Stepwise multiple regression resultedin the following regression formula: predicted cap-sular bag diameter¼ (3.44 to 0.056� P)þ (0.713�AL) � (0.0135 � AL � 2).
The corneal diameter is also an indicator ofcapsular bag size [22]. Based on this information,white-to-white corneal measurement and axial
measurements can be used as a guide to CTR siz-ing, although many surgeons advocate routinelyusing larger sizes (authors’ preference) to ensure
adequate overlap of end terminals. Furthermore,it is appropriate to use a larger CTR in cataractsurgery involving highly myopic eyes [22].
Modified capsular tension ring
Before the introduction of the M-CTR,profound lens subluxation was managed withmore invasive and complicated surgery. This was
necessary because the standard CTR is unableadequately to provide intraoperative support andcenter the capsule bag in situations of severe
zonulysis. Previous approaches included suturingthe standard CTR through the capsule bag withor without a peripheral capsulorrhexis and then
lassoing the CTR along with the peripheralcapsule [23]. To address the issue of increasedrisks of creating capsular tears with this

511CAPSULAR TENSION RINGS
technique, Cionni developed the M-CTR in 1998(Food and Drug Administration approved inOctober, 2005) (Fig. 3, Box 2). This device ad-dresses extensive or progressive zonular damage
by allowing the surgeon to anchor the capsulebag to the eye wall. The open-ring design withone (model 1-L or 1-R) or two (model 2-L) fixa-
tion eyelets attached to the central ring permitsscleral-suture fixation. The eyelets protrude0.25 mm forward from the body of the CTR
thereby sitting in front of the anterior capsule pre-serving the capsular bag’s integrity on suturing [6].
It is important to perform an adequately sized
capsulorrhexis (ie, 5.5 mm) when working withthe M-CTR. With a smaller capsulorrhexis mar-gin, the hook may drag on the capsulorrhexis edgeand result in iris chafing and related pigment
dispersion and chronic uveitis.Cionni and coworkers [18] studied the effect of
the M-CTR in 90 eyes with congenital loss of
zonular support. In 94% of cases, the M-CTRprovided good centration of the capsular bagand PCIOL. In 80% of eyes, the best-corrected
visual acuity was 20/40 or better. The suturebreakage incidence was 10%. Recommendationswere made to use 9-0 rather than 10-0 sutures to
address this concern.
Fig. 3. Cionni-modified capsular tension ring for suture
scleral fixation. (A) Single eyelet. (B) Double eyelet.
In a series of 68 consecutive patients, Ahmedand coworkers [24] reported their findings on the
M-CTR implantation in cases of profoundzonulopathy caused by a variety of causes. Thedouble eyelet M-CTR was implanted in 10 cases
with the remainder receiving the single eyeletM-CTR. Varying etiologies for zonular weaknessincluded Marfan syndrome (22 cases); trauma (19
cases); ectopia lentis (10 cases); pseudoexfoliation(6 cases); and other (12 cases). The average fol-low-up was 12.4 months with all cases achievingadequate centration. Complications included ele-
vated IOP (six cases); mild posterior capsule opa-cification tilt (five cases); pigment dispersion (twocases); mild iritis (five cases); and cystoid macular
edema (four cases). These results demonstratedthe wide range of clinical situations where theM-CTR may be used. One of the major findings
of these studies is that the need for vitrectomy,which would have been routinely required withmany of these cases, is often obviated with theuse of capsular tension devices.
In their case series of seven eyes (five patients),Moreno-Montanes and coworkers [25] demon-strated that M-CTR implantation was an
acceptable procedure to correct limited lenssubluxation, with preservation of the capsularbag and relatively few complications.
Capsular tension segment
In 2002, Ahmed designed the CTS (Fig. 4A–D).
Also intended for patients with profound zonularinsufficiency, this device is designed for cases re-quiring optimal intraoperative support (see
Box 2. Key points about the standardCTR and M-CTR
When to use a CTR or M-CTR� Mild zonular weakness (<4 clock
hours)� All pseudoexfoliation patients
(debated); does improve centrationand tilt� Scleral fixation required (M-CTR)
When not to use a CTR or M-CTR� Anterior capsule tear� Posterior capsule rent� Incomplete rhexis� Recenter severely subluxed capsular
bag

512 HASANEE & AHMED
Fig. 4. (A) Capsular tension segment (CTS). (B) CTS with iris retractor through eyelet for intraoperative stabilization.
(C) Phacoemulsification with CTS and iris retractor in place. (D) CTS in place postoperatively with well-centered
intraocular lens.
Fig. 4B,C) or for patients in need of long-termpost-operative centration of an IOL within the capsularbag. This partial PMMA ring segment (Fig. 5) is
120 degrees with a radius of 5 mm. Like theM-CTR, the CTS also possesses an anteriorly posi-tioned fixation eyelet.
It may be challenging to place a CTR into aneye with a dense cataract or significant zonularweakness before phacoemulsification with in-
creased risk of creating further zonular damage[26]. This is especially true with the higher tensileM-CTR. The CTS can be implanted with fewertraumas, however, because a dialing technique is
not necessary. Much less force is transmitted tothe zonular apparatus before lens extraction,and this has a distinct advantage over the CTR
and M-CTR in these situations. The CTS isdesigned to slide atraumatically into the capsulebag with minimal effort. This device may be
used in cases of a discontinuous capsulorrhexis,anterior capsule tear, or a posterior capsule rent.It is inserted into the capsule bag after capsulor-rhexis and placed over the area of zonular
weakness. The main body of the device sits insidethe capsule bag supporting and extending the cap-sule equator with the central eyelet remaining
anterior to the capsule. When used forintraoperative support, an inverted iris retractor(by a paracentesis) is placed through the eyelet
acting as a coat hanger to support the capsularbag in the area of zonular weakness (seeFig. 4B,C). Multiple CTS devices may be used in
a similar fashion for cases of global weakness(Fig. 6) [27]. Unlike other endocapsular devices,the CTS may be used only as an intraoperative de-vice and can be easily removed once lens extrac-
tion is complete or, as most surgeons choose todo, it can be permanently suture-fixated to thesclera, much like the M-CTR, for long-term cap-
sular bag support and centration. It should benoted that the CTS provides support in the trans-verse plane when sutured to the scleral wall. To
address circumferential support, a CTR may beimplanted in conjunction with an already posi-tioned CTS (authors’ preference). The CTS isavailable in three different sizes: (1) 4.75 mm

513CAPSULAR TENSION RINGS
Fig. 5. Dimensions of capsular tension segment.
(model 6D); (2) 5 mm (model 6E); and (3) 5.5 mm
(model 6C). Model 6D is the more commonlyused device.
In a consecutive series of 35 patients in which
a CTS was implanted with or without another
Fig. 6. Postoperative photographs of dual CTS. Close-
up view (top left).
support device, IOL centration was achieved in all
cases with no significant IOL tilt [19]. Severalcombinations of devices were used including oneCTS (nine patients); two CTSs (eight patients);
CTS plus CTR (nine patients); CTS plusM-CTR (four patients); CTS plus iris colobomaring (one patient); and CTS plus iris diaphragmrings (four patients). Two patients had an intrao-
perative anterior capsule tear and one patient de-veloped a posterior capsule rent but the CTS wasstill successfully implanted in these cases. Three
patients developed posterior capsule opacifica-tion. Initial outcomes have demonstrated theversatility of the CTS both as an intraoperative
tool and implant support device.
Closed foldable capsular ring
The closed foldable capsular ring was recentlyintroduced byDick [28], which is a foldable capsular
tension and bending ring system designed witha sharp edge. The closed foldable capsular ring haseight hydrophobic and eight hydrophilic ring seg-
ments. The minimum overall diameter is 9.2 mm.This implant device can be inserted either manuallywith forceps and a two-folded technique or through

514 HASANEE & AHMED
an injector cartridge system. In the series of 104 eyes,this implant was inserted through a small incision(1.6–3.2 mm) with no significant complications
over 6-months follow-up. Posterior capsule opacifi-cation was minimal or absent in all cases.
Capsular bending ring
This modification of the CTR theme is anopen-ring design with a 0.7 � 0.2 mm cross-
section at a 90-degree angle with an unpolishedsurface [17]. Designed by Nishi, the capsularbending ring (CBR) is made of PMMA and is en-gineered further to inhibit lens epithelial cell mi-
gration because of the sharp-edge design. The0.7-mm lateral height maintains distance betweenthe anterior and posterior capsules thereby mini-
mizing the risk of capsule sheet adhesion, whichmay lead to capsular fibrosis or posterior capsuleopacification. It also maintains capsular bag con-
tour, reduces capsular contraction, increases in-traoperative safety, and avoids IOL dislocationin cases of zonulysis. The CBR is implanted with
an injector (Geuder, type G 32,965). MorcherGmbH also manufactures this device and it comesin a 13-mm diameter, which compresses to 11 mm.Like CTR insertion, it is important to fill the cap-
sule bag with ophthalmic viscosurgical device sothat the leading edge does not become entrapped.The insertion of the CBR may be slightly more
challenging because of its height and rigidity. Itis recommended to gain experience with CTR im-plantation first.
Aniridia and coloboma rings
The aniridia ring is designed as a CTR with
seven black-dyed PMMA sector shields with a di-ameter of 10.75 mm (Morcher type 50C for 6-mmpupil, type 50D for 4-mm pupil, type 50E for
3.5-mm pupil). Combining two aniridia ringsallows for a full 360-degree shield that acts as aniris substitute.
For patients with isolated regions of irisdeficiency, Morcher manufactures coloboma ringswith a centrally protruding shield of either 60 or 90degrees. The single sector shield, incorporated over
60 or 90 degrees (Rasch 96L and 96F, Morcher),consists of black-dyedPMMA.The ringdiameter is12.6 mm and has a segment width of 2.5 mm. The
end of the ring with the sector shield is brought intothe capsule bag first. After implantation, the ring isrotated into the appropriate position with forceps
and positioning hooks.
Capsular tension ring current issues
Selection of endocapsular device
Some surgeons feel that the choice ofendocapsular support devices depends mainly on
the nature of zonular weakness (nonprogressiveversus progressive) [27]. It is also useful to takeinto consideration the degree of zonular loss or
extent of generalized zonular instability (Table 1).Standard CTRs are appropriate for nonpro-
gressive zonulopathy cases like traumatic,
iatrogenic zonular dialysis, or zonular colobomas.The remaining zonular fibers in these cases areusually quite strong, and with redistribution ofthese forces with the CTR, can support the
capsular bag [27]. In progressive cases, however,such as advanced pseudoexfoliation syndrome orMarfan syndrome with profound zonular dialysis,
a scleral-sutured M-CTR or CTS may be of opti-mal value because it can be permanently secured.Further support can be achieved as necessary by
combining devices depending on the amount ofscleral-fixation needed. Additionally, conventionalCTR implantation does not eliminate the
Table 1
Comparison of CTR, M-CTR, and CTS
CTR M-CTR CTS
Requires continuous curvilinear capsulorrhexis Yes Yes No
May be placed before lens removal With difficulty With difficulty Yes
Use with anterior capsule tear No No Yes
Use with posterior capsule rent No No Yes
Use with large zonular dialysis (O4 clock hours) No Yes Yes (þ/� multiple segments)
Use in progressive zonulysis No Yes Yes
Allows for suture fixation to sclera No Yes Yes
May be easily removed from eye if needed No No Yes
Cortical removal difficulty Yes Yes No
Abbreviations: CTR, capsular tension ring; CTS, capsular tension segment; M-CTR, modified capsular tension ring.

515CAPSULAR TENSION RINGS
underlying cause of zonular weakness and in se-vere cases of progressive dialysis it may be un-avoidable to prevent pseudophakodonesis,further luxation, or dislocation of the capsular
bag complex into the vitreous [4].CTRs are indicated in cases of mild, general-
ized zonular weakness or small, localized zonular
dialysis (!3–4 clock hours). In cases of profoundzonular weakness, a standard CTR may notsupply enough intraoperative and postoperative
support to maintain the desired orientation of thecapsular bag.
In more advanced or progressive cases of
zonular instability, the M-CTR or the CTS isindicated. A 9.0 polypropylene suture withdouble-armed CTC-6 needles (Ethicon, Somer-ville, New Jersey) is passed through the eyelet of
the fixation hook of the CTS or M-CTR before orafter implantation [29]. An ab-externo approachthrough a scleral groove to suture the CTS or
M-CTR has been proposed, which can beperformed under topical anesthesia [30].
Appropriate timing of capsular tension ringplacement
There has been debate as to the optimal timing
of CTR insertion because it can be inserted intothe capsule bag at any time following capsulor-rhexis and hydrodissection (Box 3). CTR im-plantation before nucleus extraction (early
implantation) has been purported to be a safe al-ternative in cases of pseudoexfoliation. By usingthis early implantation technique, reduced
Box 3. Timing of CTR insertiona
Before phaco� Offers better nuclear stability for
phacoemulsification� More difficult with dense lens (higher
risk of iatrogenic zonular damage)� Difficult to remove cortex
After phaco or cortical removal� Use iris hooks during phaco or cortical
irrigation and aspiration� Risk of iris hook dislodgement
(subsequent tears)
a CTS may be inserted at any time becauseof atraumatic entry.
intraoperative complications caused by zonularseparation have been reported [2]. During phacoe-mulsification and cortical aspiration, the dis-tended capsular orientation decreases the risk
of it being aspirated by the phaco or irrigation-aspiration tips [3,31].
Drawbacks to early CTR implantation include
entrapment of cortical material by the CTR in thecapsular bag fornix thereby hindering removal[12]. To solve this problem, however, one could
place the CTS as an intraoperative device duringphaco and cortex because it is much easier to stripcortex around the partial segment as opposed to
the full ring structure.CTR implantation before cataract removal
may result in further iatrogenic zonular damage.Ahmed and coworkers [26] have demonstrated us-
ing Miyake-Apple video analysis that early CTRimplantation in cases with a dense cataract andmoderate zonulysis results in significant zonular
elongation and capsular displacement of up to4 mm compared with later CTR implantation.Furthermore, if a capsular tear occurs there is
risk of CTR subluxation into the vitreous body[12,14]. It is the authors’ recommendation thatthe optimal timing of CTR or M-CTR insertion
into the capsular bag be as late as safely possible(CTS may be implanted early because of its atrau-matic insertion). For cases of serious zonularweakness, the CTS may be used in conjunction
with an iris retractor for intraoperative supportas described previously. Alternatively, iris retrac-tors or modified capsule retractors (Mackool
Cataract Support System, Duckworth andKent, Hertfordshire, England) placed on the cap-sulorrhexis (Fig. 7) may provide support; how-
ever, this risks capsular tear or dislodgement,which is less likely with the CTS. Performingphaco in profound zonular instability withoutthe support of CTS or iris-capsular retractors
risks capsule bag dislocation and lens subluxation,even if a CTR has been implanted.
Pseudoexfoliation and capsular tension devices
Because pseudoexfoliation is associated withzonular weakness, these patients are potentialcandidates for CTR implantation [2]. There is
debate, however, as to whether all pseudoexfolia-tion patients should receive CTRs. These patientsare at an increased risk for intraoperative compli-
cations and postoperative IOL dislocationespecially from superior zonular dialysis [32,33].Postoperative capsular phimosis is also at

516 HASANEE & AHMED
increased risk in pseudoexfoliation syndrome.
Moreno-Montanes and Rodriguez-Conde [34]have recommended that CTR placement shouldbe mandatory when operating on all patients
with pseudoexfoliation. There is currently no evi-dence, however, demonstrating that pseudoexfoli-ation patients without any zonulopathy requireprophylactic CTR insertion. Furthermore, even
with CTR implantation, certain progressive casesmay still dislocate years later [4].
Capsule phimosis
Capsule phimosis may occur in cases of
zonulopathy because weak zonules result indecreased centrifugal forces. The contractileforces of an anterior fibrosing capsule may be
overwhelming leading to capsular phimosis. Cap-sular contraction forces may be symmetric orasymmetric. Asymmetric forces cause the IOL to
shift to one side (usually the stronger side),whereas symmetric contraction is less likely toresult in lens decentration.
Tehrani and coworkers [35] demonstrated apos-itive correlation between capsular bag shrinkageand axial length in their studywith the capsulemea-suring ring (HumanOptics, Erlangen, Germany).
Using preoperative biometric data, a regressionformula of moderate validity was determined topredict the amount of capsular bag shrinkage.
Although it was initially believed that anteriorcapsule contraction following cataract surgerywith CTR placement may be prevented [3,36],
more recent reports have indicated that capsularphimosis is still a postoperative concern despiteCTR implantation [31]. Capsular contraction to
Fig. 7. Iris retractors placed at capsulorrhexis edge to
stabilize loose capsular-zonular complex. They run the
risk of inadvertent dislodgement or anterior capsular
tear.
the point of complete capsulorrhexis openingocclusion has also been reported despite CTR us-age [36,37]. Capsular contraction has occurred
following CTR implantation with IOLs madefrom silicone, PMMA, and acrylic materials [36].CTRs are still beneficial in these situations, how-ever, because the capsular contraction is typically
symmetric as opposed to asymmetric without theuse of a CTR.
To reduce the risk of capsule contraction
syndrome further, one may create a capsulorrhexisopening of 5.5 to 6 mm, use an acrylic IOL [33,38–40], and aspirate lens epithelial cells on the under-
surface of the anterior capsule to reduce lensepithelial cells proliferation and metaplasia [41].Lens epithelial cells metaplasia and fibrosis mayalso be reduced by the presence of an endocapsu-
lar ring by decreasing contact between the opticand anterior capsule [17]. To prevent decentra-tion, anterior capsule relaxing incisions either
intraoperatively with microscissors or postopera-tively with a neodymium:yttrium-aluminum-garnet laser anterior capsulotomy is invaluable
(Fig. 8).The spring constant of a CTR has been shown
by Kurz and Dick [42] to be a suitable mechanical
characteristic to facilitate the choice of CTRmodel. CTRs with lower spring constants weremore advantageous for the management of zonu-lar dialysis, where higher spring constant CTRs
were more ideal for the prevention of capsularbag shrinkage.
Kurz and coworkers [43] examined the effect of
the CTR and CBR on capsular bag shrinkage. Ina series of 92 eyes, a capsular measuring ring wasimplanted after phacoemulsification to measure
Fig. 8. CTS with neodymium:yttrium-aluminum-garnet
laser radial cuts to anterior capsule for capsule
contracture. Intraocular lens is well centered.

517CAPSULAR TENSION RINGS
capsular bag size in vivo. Patients were random-ized into three groups: (1) capsular measuringring and CBR, (2) capsular measuring ring andCTR, and (3) capsular measuring ring alone.
Measurements were performed preoperatively,intraoperatively, and postoperatively at 3 days,1 month, and 3 months. Clinical end points
included capsular bag size and capsulorrhexisdiameter. Eyes implanted with the CBR showedshrinkage of the capsular bag from 10.6 to
10.4 mm after a median of 3 months (sign test;P ¼ .023); eyes with a CTR showed a comparablemedian capsular bag shrinkage from 10.5 to
10.2 mm (P ! .001), whereas eyes withouta CTR showed a median shrinkage from 10.5 to10 mm (P ! .001). This study concluded that cap-sular bag shrinkage can be inhibited by a CBR
and to a lesser extent with a CTR. This gain inshrinkage prevention is limited, however, whencompared with a capsular measuring ring. This re-
duction of capsule bag shrinkage after CTR im-plantation may reduce IOL dislocation and tilt.
Management of capsular tension ring dislocation
Subluxation or dislocation of the CTR post-operatively is a risk for patients with severe orprogressive zonulysis. In a retrospective interven-
tional case series of 11 patients, Ahmed andcoworkers [4] demonstrated that CTR decentra-tions, including into posterior vitreous, may beeffectively managed with scleral-suture fixation
of the CTR through the fibrotic capsular bag, orwith the placement of a CTS under the anteriorcapsule to reposition the displaced apparatus.
Moreno-Montanes and coworkers [44] have alsoreported their technique of late IOL and CTRdislocation using two 10-0 polypropylene sutures
placed transsclerally 180 degrees apart throughboth the anterior and posterior capsules capturingthe CTR complex.
Several techniques of CTR retrieval have beenreported in cases where it has displaced into thevitreous cavity. Lang and coworkers [14] have re-ported the successful removal of an intact ring
through a sclerotomy site. Another possibleapproach is to cut the fallen ring into two halvesand remove each half by using two forceps and
a bimanual technique [45]. A third technique pro-posed by Ma and coworkers [46] seems to be themost viable and safest option. This approach en-
compasses the use of a CTR injector to withdrawthe ring in one piece through the initial phacoincision.
Posterior capsule opacification
Posterior capsule opacification has still beenreported postoperatively [27], although the inci-dence of posterior capsule opacification is
reduced with the use of CTRs [8]. To minimizethis risk, Nishi’s CBR may be used, with theadded feature of a square-edge design [17]. Thismodel has been shown significantly to reduce the
risk of posterior capsule epithelial growth [17].Additionally, Dick and coworkers [47] reportthat combining a viscoadaptive viscoelastic agent
and a CBR not only enhances the safety ofprimary and secondary PCIOL implantation andIOL exchange in pediatric cases, but also reduces
posterior capsule opacification. A square-edgedIOL design used in conjunction with a CTRmay also decrease the incidence of posteriorcapsule opacification [40].
Posterior capsule opacification was reported tobe of particular concern when using the CionniM-CTR [25]. With the fixation hook protruding
anterior to the capsulorrhexis margin, it hasbeen suggested that the anterior capsule may beslightly lifted away from the optic and this may
facilitate lens epithelial cells migration in thiszone [25].
Summary
In cases of zonular weakness, capsular tensiondevices offer numerous advantages including de-creased risk of posterior capsule opacification,decreased capsular bag collapse and risk of
aspiration, re-establishment of the capsular bagcontour, limited late IOL decentration caused byasymmetric capsule contraction, decreased irriga-
tion fluid passing behind the capsule, decreasedrisk of vitreous herniation, decreased IOL decen-tration, reduced closure of the capsule, and de-
creased extension of zonular dialysis [46,48,49].There have been dramatic advances in the
management of zonular weakness over the past10 years. The evolution of capsular tension de-
vices, from the CTR to the more recent CTS, hasserved to play a specific role in the management ofweak zonules in cataract surgery.
References
[1] Jacob S, Agarwal A, Agarwal A, et al. Efficacy of
a capsular tension ring for phacoemulsification in
eyes with zonular dialysis. J Cataract Refract Surg
2003;29:315–21.
[2] Bayraktar S, Alton T, Kucuksumer Y, et al. Capsu-
lar tension ring implantation after capsulorrhexis in
518 HASANEE & AHMED
phacoemusification of cataracts associated with
pseudoexfoliation syndrome: intraoperative compli-
cations and early postoperative findings. J Cataract
Refract Surg 2001;27:1620–8.
[3] Gimbel HV, SunR,Heston JP.Management of zon-
ular dialysis in phacoemulsification and IOL implan-
tation using the capsular tension ring. Ophthalmic
Surg Lasers 1997;28:273–81.
[4] Ahmed IK, Chen SH, Kranemann C, et al. Surgical
repositioning of dislocated capsular tension rings.
Ophthalmology 2005;112:1725–33.
[5] Leger U, Witschel BM, Lim SJ, et al. The capsular
ring: a new device for complicated cataract surgery.
Presented at the third American-International Con-
gress onCataract, IOL andRefractive Surgery. Seat-
tle, Washington, May 11, 1993.
[6] Osher RH. History and experience with capsular
tension rings. Cataract and Refractive Surgery To-
day 2005;Jan:1–5.
[7] Sun R, Gimbel HV. In vitro evaluation of the effi-
cacy of the capsular tension ring for managing zon-
ular dialysis in cataract surgery. Ophthalmic Surg
Lasers 1998;29:502–5.
[8] DEliseo D, Longanesi L, Grisanti F, et al. Preven-
tion of posterior capsule opacification using capsular
tension ring for zonular defects in cataract surgery.
Eur J Ophthalmol 2003;13:151–4.
[9] Kohnen T, Baumeister M, Buhren J. Scheimpflug
imaging of bilateral foldable in-the-bag intraocular
lens implantation assisted by a scleral-sutured capsu-
lar tension ring in Marfan’s syndrome. J Cataract
Refract Surg 2003;29:598–602.
[10] Hayashi K, Hayashi H, Matsuo K, et al. Anterior
capsular contraction and intraocular lens disloca-
tion after implant surgery in eyes with retinitis pig-
mentosa. Ophthalmology 1998;105:1239–43.
[11] Mizuno H, Yamada J, Nishiura M, et al. Capsular
tension ring use in a patient with congenital
coloboma of the lens. J Cataract Refract Surg
2004;30:503–6.
[12] Bopp S, LuckeK. Chronic cystoid macular edema in
an eye with a capsule defect and posteriorly
dislocated capsular tension ring. J Cataract Refract
Surg 2003;29:603–8.
[13] Bhattacharjee H, Bhattacharjee K, Das A, et al.
Management of a posteriorly dislocated endocapsu-
lar tension ring and a foldable acrylic intraocular
lens. J Cataract Refract Surg 2004;30:243–6.
[14] Lang Y, Fineberg E, Garzozi HJ. Vitrectomy to
remove a posteriorly dislocated endocapsular ten-
sion ring. J Cataract Refract Surg 2001;27:474–6.
[15] Hara T, Hara T, Yamada Y. Equator ring for
maintenance of the completely circular contour of
the capsular bag equator after cataract removal.
Ophthalmic Surg 1991;22:358–9.
[16] Nagamoto T, Bissen-Miyajuma H. A ring to sup-
port the capsular bag after continuous curvilinear
capsulorrhexis. J Cataract Refract Surg 1994;20:
417–20.
[17] Nishi O, Nishi K, Menapace R. Capsule-bending
ring for the prevention of capsular opacification:
a preliminary report. Ophthalmic Surg Lasers 1998;
29:749–53.
[18] Cionni RJ, Osher RH,Marques DM, et al. Modified
capsular tension ring for patients with congenital
loss of zonular support. J Cataract Refract Surg
2003;29:1668–73.
[19] Hasanee K, Ahmed IIK, Kranemann C, et al. Cap-
sular tension segment: clinical results and complica-
tions. Presented at the American Academy of
Ophthalmology Meeting. New Orleans, October
25, 2004.
[20] Lee DH, Shin SC, Joo CK. Effect of a capsular
tension ring on intraocular lens decentration and
tilting after cataract surgery. J Cataract Refract
Surg 2002;28:843–6.
[21] Price FW, Mackool RJ, Miller KM, et al. Interim
results of the United States investigational device
study of Ophtec capsular tension ring. Ophthalmol-
ogy 2005;112:460–5.
[22] Vass C, Menapace R, Schetterer K, et al. Prediction
of pseudophakic capsular bag diameter based on
biometric variables. J Cataract Refract Surg 1999;
25:1376–81.
[23] Lam DS, Young AL, Leung AT, et al. Scleral
fixation of a capsular tension ring for severe ectopia
lentis. J Cataract Refract Surg 2000;26:609–12.
[24] Ahmed IIK, Crandall AS, Kranemann C, et al. Clin-
ical results of the Cionni modified capsular tension
ring for sever zonular weakness. Presented at the
American Academy of Ophthalmology Meeting,
New Orleans, October 25, 2004.
[25] Moreno-Montanes J, Sainz C, Maldonado MJ.
Intraoperative and postoperative complications of
Cionni endocapsular ring implantation. J Cataract
Refract Surg 2003;29:492–7.
[26] Ahmed IIK, Cionni RJ, Kranemann C, et al. Opti-
mal timing of capsular tension ring implantation:
a Miyake-Apple video analysis. J Cataract Refract
Surg 2005;31:1809–13.
[27] Ahmed IK, Butler M. Capsular tension devices for
the glaucoma surgeon. Glaucoma Today 2004;
Nov–Dec:1–4.
[28] Dick HB. Closed foldable capsular rings. J Cataract
Refract Surg 2005;31:467–71.
[29] Cionni RJ, Osher RH. Management of profound
zonular dialysis or weakness with a new endocapsu-
lar ring designed for scleral fixation. J Cataract
Refract Surg 1998;24:1299–306.
[30] Ahmed II, Crandall AS. Ab-externo scleral fixation
of the Cionni modified capsular tension ring. J Cat-
aract Refract Surg 2001;27:977–81.
[31] WaheedK,EleftheriadisH, LiuC.Anterior capsular
phimosis in eyes with a capsular tension ring.
J Cataract Refract Surg 2001;27:1688–90.
[32] Crandall A. Capsular tension rings and pseudoexfo-
liation. Cataract and Refractive Surgery Today
2004;Jan:46–7.
519CAPSULAR TENSION RINGS
[33] Jehan FS, Mamalis N, Crandall AS. Spontaneous
late dislocation of intraocular lens within the
capsular bag in pseudoexfoliation patients.
Ophthalmology 2001;108:1727–31.
[34] Moreno-Montanes J, Rodriguez-CondeR. Capsular
tension ring in eyes with pseudoexfoliation. J
Cataract Refract Surg 2002;28:2241–2.
[35] Tehrani M, Dick HM, Krummenauer F, et al. Cap-
sule measuring ring to predict capsular bag diameter
and follow its course after foldable intraocular lens
implantation. J Cataract Refract Surg 2003;29(11):
2127–34.
[36] Moreno-Montanes J, Sanchez-Tocino H, Rodri-
guez-Conde R. Complete anterior capsule contrac-
tion after phacoemulsification with acrylic
intraocular lens and endocapsular ring implanta-
tion. J Cataract Refract Surg 2002;28:717–9.
[37] Faschinger CW, Eckhardt M. Complete capsulor-
rhexis opening occlusion despite capsular tension
ring implantation. J Cataract Refract Surg 1999;
25:1013–5.
[38] Werner L, Pandey SK, Escobar-GomezM, et al. An-
terior capsule opacification: a histopathological
study comparing different IOL styles. Ophthalmol-
ogy 2000;107:463–71.
[39] Hayashi K, Hayashi H. Intraocular lens factors that
may affect anterior capsule contraction. Ophthal-
mology 2005;112:286–92.
[40] Saco S, Menapace R, Findl O, et al. Long-term
efficacy of adding a sharp posterior optic edge to
a three-piece silicone intraocular lens on capsule
opacification: five-year results of a randomized study
Am J Ophthalmol 2005;139:696–703.
[41] Joo CK, Shin JA, Kim JH. Capsular opening con-
tracture after continuous curvilinear capsulorrhexis
and intraocular lens implantation. J Cataract Re-
fract Surg 1996;22:585–90.
[42] Kurz S,DickHB. Spring constants and capsular ten-
sion rings. J Cataract Refract Surg 2004;30:1993–7.
[43] Kurz S, Krummenauer F, Hacker P, et al. Capsular
bag shrinkage after implantation of capsular bend-
ing or capsular tension ring. J Cataract Refract
Surg 2005;31:1915–20.
[44] Moreno-Montanes J, Heras H, Fernandez-Hortela-
no A. Surgical treatment of a dislocated intraocular
lens-capsular bag-capsular tension ring complex.
J Cataract Refract Surg 2005;31:270–3.
[45] Bopp S, Lucke K. Removal of a capsular tension
ring. Ophthalmology 2004;111:196–7.
[46] Ma PE, Kaur H, Petrovic V, et al. Technique for re-
moval of a capsular tension ring from the vitreous.
Ophthalmology 2003;110:1142–4.
[47] Dick HB, Schwenn O, Pfeiffer N. Implantation of
the modified capsular bending ring in pediatric
cataract surgery using a viscoadaptive viscoelastic
agent. J Cataract Refract Surg 1999;25:1432–6.
[48] Kim JH, KimH, Joo CK. The effect of capsular ten-
sion ring on posterior capsule opacity in cataract
surgery. Korean J Ophthalmol 2005;19:25–8.
[49] Menapace R, Findl O, Georgopoulos M, et al. The
capsular tension ring: designs, applications, and
techniques. J Cataract Refract Surg 2000;26:898–912.

Ophthalmol Clin N Am 19 (2006) 521–533
Contrast Sensitivity and MeasuringCataract Outcomes
Mark Packer, MD*, I. Howard Fine, MD,Richard S. Hoffman, MD
Department of Ophthalmology, Oregon Health and Sciences University, 1550 Oak Street,
Suite 5, Eugene, OR 97401, USA
Functional visionmeans the ability of the visualsystem to receive, transmit, and report informa-
tion. The optical system of the eye allows reception,whereas the neurosensory retina and the neuralpathways to the visual cortex govern transmission.Cortical elements in turn report information.
Images form the elements of visual data. Theformation of the image on the retina depends onthe optical elements of the eye, including all of the
ocular media: the tear film, cornea, aqueoushumor, lens, and vitreous body. The principalelements in this system, the cornea and the lens, lie
within the province of the anterior segmentsurgeon or ophthalmologist who performs cata-ract and refractive surgery.
The evaluation of functional vision in the clinicor laboratory may take a variety of approaches.Wavefront aberrometry, ray tracing, corneal to-pography, and double-pass devices enable one
objectively to measure retinal image quality.Contrast-sensitivity testing, reading speed, anddriving simulations represent subjective tests that
measure the neural and the optical performance ofthe visual system. Both approaches add to theknowledge of functional vision.
As the understanding of the visual system hasadvanced, the evaluation of surgical techniquesand devices has also evolved. Clinical studies havemeasured the outcomes of both corneal refractive
Drs. Packer and Fine are consultants for Advanced
Medical Optics and Bausch and Lomb.
* Corresponding author.
E-mail address: [email protected] (M. Packer).
0896-1549/06/$ - see front matter � 2006 Elsevier Inc. All ri
doi:10.1016/j.ohc.2006.07.006
surgery and lenticular surgery with the full arma-mentarium of functional vision testing. The re-
sults of ongoing research help to guide furtherdevelopments in these fields.
Patients’ heightened expectations providea challenge for the increasing sophistication of
anterior segment surgeons. The methods used inclinical research today will likely become stan-dards of clinical practice tomorrow. These
methods highlight the limitations of currentlyentrenched techniques, such as measurement ofSnellen acuity. Now the American National
Standards Institute has adopted sine wave gratingcontrast sensitivity at five spatial frequencies andthe Early Treatment of Diabetic Retinopathy
Study logarithmic letter chart. Cataract and re-fractive surgeons should take notice of develop-ments in visual science that will strongly affecttheir practices in the very near future.
Although the achievement of 20/20 uncorrectedvisual acuity remains a laudable target for anycataract or refractive surgeon, the goal of high-
quality vision increasingly reflects the understand-ing of the visual system as a whole. In fact, Snellenacuity represents only a small portion of functional
vision. A comparison of vision and hearing high-lights the limitations of standard visual acuity tests:the auditory equivalent of a standard high-contrastSnellen eye chart is a hearing test with only one
high level of loudness for all sound frequencies.Today, contrast-sensitivity testing is emerging asa more comprehensive measure of vision that will
probably replace Snellen letter acuity testing, justas audiometric testing replaced the ‘‘click’’ andspoken-word tests used before World War II [1].
ghts reserved.
ophthalmology.theclinics.com

522 PACKER et al
Engineers understand that Fourier analysisallows the representation of any visual object asa composite of sine waves of various frequencies,
amplitudes, and orientations. In fact, visual pro-cessing in the human nervous system works likeFourier analysis in reverse, with functionallyindependent neural channels filtering images to
create what is seen [2]. Sine wave gratings are thebuilding blocks of vision, just as pure tones are thebuilding blocks of audition.
Ophthalmologists realize that patients maycomplain about haziness, glare, and poor nightvision despite 20/20 Snellen acuity. This anomaly
can be understood when one realizes that theSnellen acuity letter recognition test uses very highcontrast. The jet black letters on the bright whitebackground have a great deal of reserve contrast,
so that even a patient with severely reducedcontrast sensitivity can still read the chart. Thatpatient perceives the letters as gray on white
rather than black on white, but still is able torecognize them. The examiner has no way ofknowing just how gray the letters look to any
particular patient. Snellen acuity is a relativelyinsensitive test of visual function.
Contrast-sensitivity testing has the ability to
detect differences in functional vision whenSnellen visual acuity measurements cannot [3].For example, a patient with loss of low-frequencycontrast sensitivity may be able to read 20/20 but
be unable to see a truck in the fog. Although blurcaused by refractive error alone affects only thehigher spatial frequencies, scatter of light caused
by corneal or lenticular opacities causes loss atall frequencies. Glaucoma and other optic neurop-athies generally produce loss in the middle and
low frequencies. Contrast sensitivity testing offerscritical information to help elucidate patients’diagnoses.
Numerous studies have demonstrated the re-
lationship of contrast sensitivity and visual per-formance. From driving difficulty [4] and crashinvolvement [5], to falls [6] and postural stability
in the elderly [7], to activities of daily living andvisual impairment [8], to the performance of pilotsin aircraft simulators [9], contrast sensitivity has
consistently been found to provide a high degreeof correlation with visual performance.
Contrast sensitivity declines because
of increasing aberrations
Unfortunately, contrast sensitivity declineswith age even in the absence of ocular pathology,
such as cataract, glaucoma, or macular degener-ation (Fig. 1). The pathogenesis of this decline invision likely involves changes in the spherical ab-
erration of the crystalline lens.Spherical aberration is a property of spherical
lenses. A spherical lens does not refract all parallelrays of incoming light to a single focal point.The lens
bendsperipheral raysmorestrongly so that these rayscross the optical axis in front of the paraxial rays. Asthe aperture of the lens increases the average focal
point moves toward the lens, so that a larger pupilproduces greater spherical aberration.
Spherical aberration of the cornea changes
little with age. Total wavefront aberration of theeye increases more than threefold, however, be-tween 20 and 70 years of age [10]. Wavefront ab-erration measurements combined with data from
corneal topography demonstrate that the opticalcharacteristics of the youthful crystalline lenscompensate for aberrations in the cornea, reduc-
ing total aberration in younger people. Unfortu-nately, the aging lens loses its balance with thecornea, because both the magnitude and the sign
of its spherical aberration change significantly[11]. A loss of balance between corneal and lentic-ular spherical aberration causes the degradation
of optical quality in the aging eye.The sine wave grating contrast sensitivity of
a pseudophakic patient with a spherical intraoc-ular lens (IOL) implanted is no better than that of
Fig. 1. Contrast sensitivity in five age groups 3 cd/m2.
The decline in contrast sensitivity with age was demon-
strated in a multicenter study of healthy normal subjects.
(From Packer M. Contrast sensitivity in healthy subjects
20 to 69 years old. Presented at the Symposium on Cat-
aract, IOL and Refractive Surgery, American Society of
Cataract and Refractive Surgery. San Francisco, April
12, 2003; with permission.)
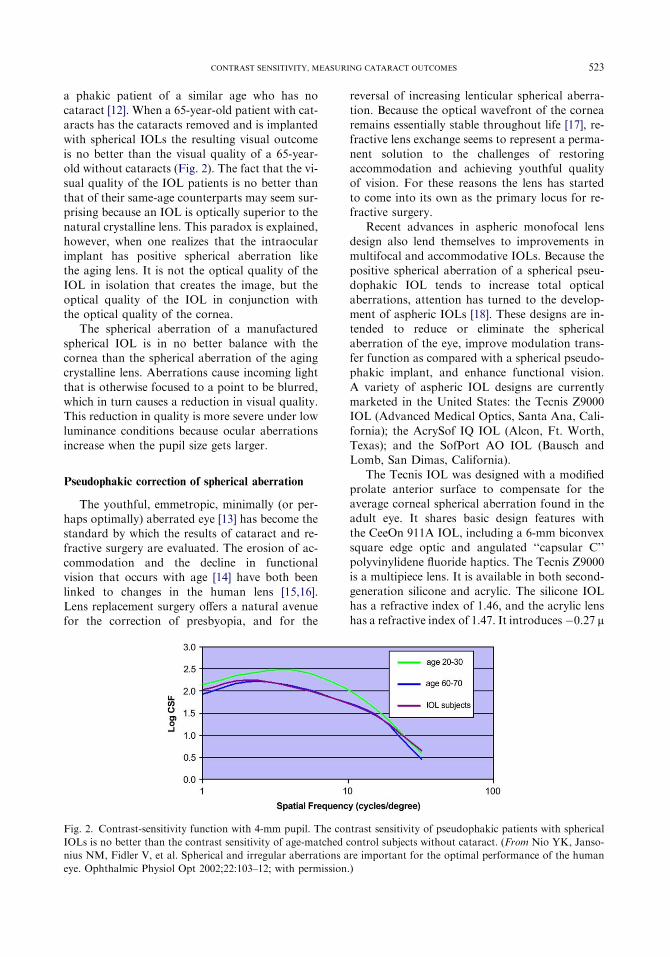
523CONTRAST SENSITIVITY, MEASURING CATARACT OUTCOMES
a phakic patient of a similar age who has nocataract [12]. When a 65-year-old patient with cat-aracts has the cataracts removed and is implantedwith spherical IOLs the resulting visual outcome
is no better than the visual quality of a 65-year-old without cataracts (Fig. 2). The fact that the vi-sual quality of the IOL patients is no better than
that of their same-age counterparts may seem sur-prising because an IOL is optically superior to thenatural crystalline lens. This paradox is explained,
however, when one realizes that the intraocularimplant has positive spherical aberration likethe aging lens. It is not the optical quality of the
IOL in isolation that creates the image, but theoptical quality of the IOL in conjunction withthe optical quality of the cornea.
The spherical aberration of a manufactured
spherical IOL is in no better balance with thecornea than the spherical aberration of the agingcrystalline lens. Aberrations cause incoming light
that is otherwise focused to a point to be blurred,which in turn causes a reduction in visual quality.This reduction in quality is more severe under low
luminance conditions because ocular aberrationsincrease when the pupil size gets larger.
Pseudophakic correction of spherical aberration
The youthful, emmetropic, minimally (or per-haps optimally) aberrated eye [13] has become thestandard by which the results of cataract and re-
fractive surgery are evaluated. The erosion of ac-commodation and the decline in functionalvision that occurs with age [14] have both been
linked to changes in the human lens [15,16].Lens replacement surgery offers a natural avenuefor the correction of presbyopia, and for the
reversal of increasing lenticular spherical aberra-tion. Because the optical wavefront of the cornearemains essentially stable throughout life [17], re-fractive lens exchange seems to represent a perma-
nent solution to the challenges of restoringaccommodation and achieving youthful qualityof vision. For these reasons the lens has started
to come into its own as the primary locus for re-fractive surgery.
Recent advances in aspheric monofocal lens
design also lend themselves to improvements inmultifocal and accommodative IOLs. Because thepositive spherical aberration of a spherical pseu-
dophakic IOL tends to increase total opticalaberrations, attention has turned to the develop-ment of aspheric IOLs [18]. These designs are in-tended to reduce or eliminate the spherical
aberration of the eye, improve modulation trans-fer function as compared with a spherical pseudo-phakic implant, and enhance functional vision.
A variety of aspheric IOL designs are currentlymarketed in the United States: the Tecnis Z9000IOL (Advanced Medical Optics, Santa Ana, Cali-
fornia); the AcrySof IQ IOL (Alcon, Ft. Worth,Texas); and the SofPort AO IOL (Bausch andLomb, San Dimas, California).
The Tecnis IOL was designed with a modifiedprolate anterior surface to compensate for theaverage corneal spherical aberration found in theadult eye. It shares basic design features with
the CeeOn 911A IOL, including a 6-mm biconvexsquare edge optic and angulated ‘‘capsular C’’polyvinylidene fluoride haptics. The Tecnis Z9000
is a multipiece lens. It is available in both second-generation silicone and acrylic. The silicone IOLhas a refractive index of 1.46, and the acrylic lens
has a refractive index of 1.47. It introduces�0.27 m
Fig. 2. Contrast-sensitivity function with 4-mm pupil. The contrast sensitivity of pseudophakic patients with spherical
IOLs is no better than the contrast sensitivity of age-matched control subjects without cataract. (From Nio YK, Janso-
nius NM, Fidler V, et al. Spherical and irregular aberrations are important for the optimal performance of the human
eye. Ophthalmic Physiol Opt 2002;22:103–12; with permission.)

524 PACKER et al
of spherical aberration to the eye. The clinicalinvestigation of the Tecnis IOL submitted to theUS Food and Drug Administration (FDA) dem-
onstrated elimination of mean spherical aberrationand significant improvement in functional visionwhen comparedwith a standard spherical IOL [19].The US Centers for Medicare and Medicaid Ser-
vices announced New Technology IOL Status forthe Tecnis IOL on January 26, 2006 [20]:
‘‘Today’s announcement of coverage with addi-
tional payment for an innovative type of in-
traocular lens reflects Medicare’s attention to
improved clinical benefits,’’ said CMS Adminis-
trator, Mark McClellan, MD, PhD. ‘‘For these
lenses, there is clear evidence of improved func-
tional vision and contrast acuity.’’
The AcrySof IQ shares the UV and blue light–filtering chromophores found in the single-piece
acrylic AcrySof Natural IOL. The special featureof this IOL is the posterior aspheric surfacedesigned to compensate for spherical aberration
by addressing the effects of overrefraction at theperiphery. The AcrySof IQ is a single-piece lensmade of hydrophobic acrylic, and it has a re-
fractive index of 1.55. It adds �0.20 m of sphericalaberration to the eye.
The SofPort Advanced Optics (LI61AO) IOL
is an aspheric IOL that has been specificallydesigned with zero spherical aberration so that itdoes not contribute to any pre-existing higher-order aberrations. It is a foldable silicone IOL
with polymethyl methacrylate haptics and squareedges, and it was specifically designed for use withthe Bausch and Lomb SofPort System, an in-
tegrated, single-use, single-handed planar deliveryIOL insertion system. The SofPort lens is a mul-tipiece lens made of second-generation silicone. It
has a refractive index of 1.43, and it introduces nospherical aberration to the eye.
Peer-reviewed, prospective, randomized scien-tific publications have demonstrated reduction of
spherical aberration and excellent contrast sensi-tivity and contrast acuity with the Tecnis mod-ified prolate IOL when compared with a variety
of spherical IOLs (as of this writing there are nopeer-reviewed publications evaluating clinical re-sults with either of the other two aspheric IOLs
available in the United States) [21–28].Mester [29] compared the quality of vision ob-
tained with the Tecnis IOL and a spherical sili-
cone IOL (SI 40, Advanced Medical Optics,Santa Ana, California). A total of 45 patientswere enrolled and randomized to receive the
Tecnis IOL in one eye and the SI 40 in the felloweye. The average photopic contrast-sensitivityvalues demonstrated a statistically significant ad-
vantage for the Tecnis IOL at all spatial frequen-cies (Fig. 3). The contrast-sensitivity curves showan even greater difference under mesopic condi-tions (Fig. 4), an expected result caused by the
larger pupil size and consequent greater contri-bution from spherical aberration in dim light.A comparison of corneal and total ocular aberra-
tions demonstrates the improved wavefront of theeye with the Tecnis Z9000 IOL (Fig. 5). This im-provement in total aberrations demonstrates the
critical compensatory relationship of cornea andlens in reducing spherical aberration.
Packer and coworkers [30] compared peakcontrast sensitivity in healthy, normal eyes, strat-
ified by age of patient, with eyes implanted witheither the Tecnis IOL or an acrylic sphericalIOL (AR40e, Advanced Medical Optics, Santa
Ana, California). They reported that mesopic con-trast sensitivity declined with age. Among 69 eyesof 36 patients, ranging in age from 21 to 61, they
found mean peak mesopic contrast sensitivity atthree cycles per degree of 72.4 units for the 20 to30 year olds, whereas subjects aged 30 to 50 years
demonstrated mean peak mesopic contrast sensi-tivity of 51.9 units. Ten eyes implanted with theTecnis IOL in patients of average age 69.5 yearsachieved mean peak mesopic contrast sensitivity
at three cycles per degree of 83.8, better than the20 to 30 year old group. Meanwhile, 11 eyes im-planted with the control IOL in patients of aver-
age age 69.4 years demonstrated mean peakmesopic contrast sensitivity at three cycles per
Fig. 3. Photopic contrast sensitivity of subjects im-
planted with the Tecnis Z9000 and SI40 IOLs. (From
Mester U. Improved optical and visual quality with
aspheric IOL. Presented at the American Society of Cat-
aract and Refractive Surgery Symposium. Philadelphia,
June 2, 2002; with permission.)

525CONTRAST SENSITIVITY, MEASURING CATARACT OUTCOMES
degree of 47.1, worse than the 30 to 50 year oldage group (Fig. 6).
The results of peer-reviewed publications on
the Tecnis IOL are summarized in Table 1. Theweight of evidence demonstrating superior func-tional vision and contrast sensitivity with themodified prolate IOL has continued to grow.
That the pseudophakic elimination of sphericalaberration reverses the age-related decline in con-trast sensitivity confirms the hypothesis that de-
creased functional vision results primarily fromaging changes in the human lens.
The effect of tilt and decentration on
wavefront-corrected intraocular lenses
Optical laboratory studies have cast doubt onthe efficacy of aspheric IOLs with negative
Fig. 4. Mesopic contrast sensitivity of subjects im-
planted with the Tecnis Z9000 and SI40 IOLs. (From
Mester U. Improved optical and visual quality with
aspheric IOL. Presented at the American Society of Cat-
aract and Refractive Surgery Symposium. Philadelphia,
June 2, 2002; with permission.)
spherical aberration, such as the Tecnis andAcrySof IQ, because of the range of tilt anddecentration of pseudophakic lenses in general
[31,32]. The eye model used to design the TecnisIOL assumed a rotationally symmetric cornea re-flecting the mean spherical aberration in a popula-tion of patients presenting for cataract surgery
[18]. This model assumed monochromatic lightand a symmetric cornea. Criticism of the modelsuggested, however, that it oversimplified the ac-
tual effects of the wavefront-corrected IOL by ig-noring the contributions of polychromatic lightand the implications of asymmetric corneal aber-
rations, such as coma [33].
Fig. 6. Peak mesopic contrast sensitivity of subjects im-
planted with the Tecnis IOL is higher than that of
healthy, normal subjects in their twenties. (From Packer
M, Fine IH, Hoffman RS. Quality of vision with a mod-
ified anterior prolate aspheric intraocular lens. Presented
at the European Society of Cataract and Refractive Sur-
gery Symposium. Nice, France, September 11, 2002;
with permission.)
Fig. 5. Photopic and mesopic contrast sensitivity of subjects implanted with the Tecnis Z9000 and SI40 IOLs. (From
Mester U. Improved optical and visual quality with aspheric IOL. Presented at the American Society of Cataract and
Refractive Surgery Symposium. Philadelphia, June 2, 2002; with permission.)
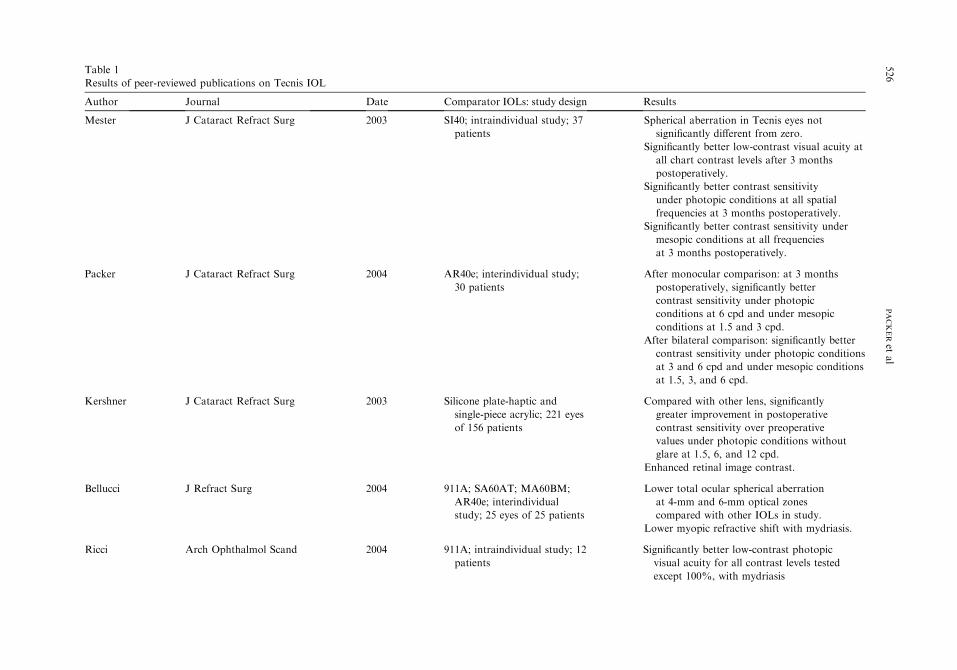
Table 1
Results
Spherical aberration in Tecnis eyes not
significantly different from zero.
Significantly better low-contrast visual acuity at
all chart contrast levels after 3 months
postoperatively.
Significantly better contrast sensitivity
under photopic conditions at all spatial
frequencies at 3 months postoperatively.
Significantly better contrast sensitivity under
mesopic conditions at all frequencies
at 3 months postoperatively.
After monocular comparison: at 3 months
postoperatively, significantly better
contrast sensitivity under photopic
conditions at 6 cpd and under mesopic
conditions at 1.5 and 3 cpd.
After bilateral comparison: significantly better
contrast sensitivity under photopic conditions
at 3 and 6 cpd and under mesopic conditions
at 1.5, 3, and 6 cpd.
Compared with other lens, significantly
greater improvement in postoperative
contrast sensitivity over preoperative
values under photopic conditions without
glare at 1.5, 6, and 12 cpd.
Enhanced retinal image contrast.
Lower total ocular spherical aberration
at 4-mm and 6-mm optical zones
compared with other IOLs in study.
Lower myopic refractive shift with mydriasis.
Significantly better low-contrast photopic
visual acuity for all contrast levels tested
except 100%, with mydriasis
526
PACKERet
al
Results of peer-reviewed publications on Tecnis IOL
Author Journal Date Comparator IOLs: study design
Mester J Cataract Refract Surg 2003 SI40; intraindividual study; 37
patients
Packer J Cataract Refract Surg 2004 AR40e; interindividual study;
30 patients
Kershner J Cataract Refract Surg 2003 Silicone plate-haptic and
single-piece acrylic; 221 eyes
of 156 patients
Bellucci J Refract Surg 2004 911A; SA60AT; MA60BM;
AR40e; interindividual
study; 25 eyes of 25 patients
Ricci Arch Ophthalmol Scand 2004 911A; intraindividual study; 12
patients

Kennis Bull Soc Belge Ophthalmol 2004 AR40e; SN60AT; Compared with the AR40e, significantly better
contrast sensitivity at 3 and 12 cpd under
photopic conditions without glare; at
3, 12, and 18 cpd under photopic conditions
with glare; at 1.5, 12, and 18 cpd under
mesopic conditions without glare; and at
12 and 18 cpd under mesopic conditions
with glare.
Compared with the SN60AT, significantly
better contrast sensitivity at 19 of 20 spatial
frequencies tested (photopic and mesopic
conditions with and without glare).
Significantly better contrast sensitivity for
spatial frequencies higher than 1.5 cpd
under both photopic and mesopic
conditions.
Statistically significant difference in mean spher-
ical aberration coefficient (Z4.0) of the whole
eye for a 5-mm pupil between the SA30AL,
AR40e, and Tecnis groups, and the MA30BA
group.
Compared with the other IOLs, a lower
percentage of patients experienced photic
phenomena while driving at night at
2 months postoperatively.
Significantly better monocular and binocular
visual acuity 3 months postoperatively.
Better monocular and binocular mesopic
contrast sensitivity at 3 months
postoperatively.
527
CONTRASTSENSIT
IVIT
Y,MEASURIN
GCATARACTOUTCOMES
interindividual study; 98 eyes
of 71 patients randomly
received one of the three
lenses
Bellucci J Cataract Refract Surg 2005 SA60AT; interindividual
study; 60 eyes of 60 patients
randomly received one
type of lens
Casprini Acta Ophthalmol Scand 2005 MA30BA; AR40; SA30AL;
AR40e; interindividual
study; 175 patients randomly
received one type of lens
Martinez-
Palmer
Arch Soc Esp Oftalmol 2005 SA60AT; Inter-individual;
bilateral implantation of
same lens in 58 patients
Abbreviation: cpd, cycles per degree.

528 PACKER et al
In fact, the eye model using monochromatic,symmetric optics does suggest tight tolerances fortilt and decentration of IOL correcting spherical
aberration. For example, the model eye used in theTecnis IOL design study demonstrates a toleranceof 0.4 mm decentration and 7-degree tilt for themodified prolate IOL with Z (4,0) ¼ �0.27 m [18].
At this degree of decentration or tilt the 15 cycleper degree contrast ratio of the wavefront-correctedIOL with negative spherical aberration becomes
equivalent to that of a standard spherical IOL.The reason that decentration reduces the
optical efficiency of an aspheric lens may be
explained by the induction of higher-order aber-ration, such as coma [34]. As an example, consideran aspheric IOL decentered 0.5 mm along the 180-degree meridian for a 6-mm pupil. Given a coeffi-
cient of fourth-order spherical aberration in theIOL of �0.29 mm, then the coefficient of inducedthird-order horizontal coma is �0.30 mm.
A meta-analysis of the peer-reviewed literatureon the subject of IOL tilt and decentration hasbeen performed to determine the approximate
percentage of pseudophakic eyes that may beexpected to reside within the tolerances set bythe reported Tecnis design eye model [35]. The se-
lected studies required a complete, continuouscurvilinear capsulorrhexis and in-the-bag IOL fix-ation. Postoperative measurement of IOL positionwas measured using Scheimpflug photography,
which measures along the visual axis. When asym-metric aberrations and polychromatic light aretaken into account, however, a newly developed
model has suggested relatively relaxed tilt and de-centration tolerances for wavefront-corrected
IOLs. This model was developed using cornealwavefront data from patients presenting for cata-ract surgery, including both symmetric and asym-
metric aberrations, and was subsequently verifiedwith these patients’ clinical postoperative data[33]. In the verification study, three surgeons ran-domly assigned a wavefront-corrected IOL to one
eye and a standard spherical IOL to the fellow eyeof 79 patients. The Zernike terms predicted by themodel for both the wavefront-corrected IOL and
the control IOL closely approximated the clinicalresults. In particular, this model very closelypredicted the Z (4,0) term for both the wavefront-
corrected and the control IOL. This validated eyemodel was then used to evaluate the effects of de-centration and tilt on the modulation transferfunction of the wavefront-corrected IOL. Assum-
ing polychromatic illumination and incorporatingthe effects of the clinically validated asymmetricaberrations, the degradation of modulation trans-
fer function with decentration to the level of a con-trol standard spherical IOL occurred at 0.8 mminstead of 0.4 mm as in the simplified, symmetric
eyemodel. The degradation ofmodulation transferfunction with tilt to this level occurs at 10 degreesinstead of 7 degrees (Figs. 7 and 8).
By analyzing the peer-reviewed literature ondecentration in terms of a tolerance of 0.8 mm, asdemonstrated by the clinically verified eye model,a significant reduction in the percentage of cases
outside of tolerance emerges. For example, thepercentage of eyes with a three-piece silicone IOLwith polymethyl methacrylate haptics decentered
greater than 0.8 mm is expected to be 0.0001%(Table 2). The number of IOLs expected to tilt
Fig. 7. Average radial modulation transfer function (MTF) versus decentration. Assuming polychromatic illumination
and incorporating the effects of the clinically validated asymmetric aberrations, the degradation ofMTFwith decentration
to the level of a standard spherical IOL occurs at 0.8 mm instead of 0.4 mm as in the simplified, symmetric eye model.
(From Packer M. Tilt and decentration: toward a new definition of tolerance. EyeWorld 2005;10:65–6; with permission.)

529CONTRAST SENSITIVITY, MEASURING CATARACT OUTCOMES
Fig. 8. Average radial modulation transfer function (MTF) versus tilt. Assuming polychromatic illumination and incor-
porating the effects of the clinically validated asymmetric aberrations, the degradation of MTF with tilt occurs at 10
degrees instead of 7 degrees as in the simplified, symmetric eye model. (From Packer M. Tilt and decentration: toward
a new definition of tolerance. EyeWorld 2005;10:65–6; with permission.)
Table 2
Percentage of eyes with a decentration O0.8 mma
Overall 0.06
Optic-haptic materials
Silicone-PMMA 0.0001
PMMA-PVDF 4.27
Silicone-prolene 0.33
PMMA 1 piece 0.07
Acrylic-PMMA 0.06
Hydrogel-PMMA 0.0002
Abbreviations: PMMA, polymethyl methacrylate; PVDF, polyvlnylidene fluoride.a In this analysis of the available peer-reviewed literature on decentration and tilt the means and standard deviations
for each IOL design were used to calculate the percentage of IOLs expected to decenter more than 0.8 mm, the point at
which the MTF of the modified prolate Tecnis IOL is equivalent to that of a standard spherical IOL. The analysis in-
cluded the following reports:
Akkin C, Ozler SA, Mentes J. Tilt and decentration of bag-fixated intraocular lenses: a comparative study between
capsulorhexis and envelope techniques. Doc Ophthalmol 1994;87:199–209.
Hayashi K, Harada M, Hayashi H, et al. Decentration and tilt of polymethyl methacrylate, silicone, and acrylic soft
intraocular lenses. Ophthalmology 1997;104:793–8.
Kim JS, Shyn KH. Biometry of 3 types of intraocular lenses using Scheimpflug photography. J Cataract Refract Surg
2001;27:533–6.
Hayashi K, Hayashi H, Nakao F, et al. Comparison of decentration and tilt between one piece and three piece poly-
methyl methacrylate intraocular lenses. Br J Ophthalmol 1998;82:419–22.
Mutlu FM, Bilge AH, Altinsoy HI, et al. The role of capsulotomy and intraocular lens type on tilt and decentration
of polymethylmethacrylate and foldable acrylic lenses. Ophthalmologica 1998;212:359–63.
Hayashi K, Hayashi H, Nakao F, et al. Intraocular lens tilt and decentration after implantation in eyes with glau-
coma. J Cataract Refract Surg 1999;25:1515–20.
Wang MC, Woung LC, Hu CY, et al. Position of polymethyl methacrylate and silicone intraocular lenses after pha-
coemulsification. J Cataract Refract Surg 1998;24:1652–7.
Hayashi K, Hayashi H, Nakao F, et al. Anterior capsule contraction and intraocular lens decentration and tilt after
hydrogel lens implantation. Br J Ophthalmol 2001;85:1294–7.
Taketani F, Matuura T, Yukawa E, et al. Influence of intraocular lens tilt and decentration on wavefront aberra-
tions. J Cataract Refract Surg 2004;30:2158–62.
Dick HB, Schwenn O, Krummenauer F, et al. Refraction, anterior chamber depth, decentration and tilt after implan-
tation of monofocal and multifocal silicone lenses. Ophthalmologe 2001;98:380–6.

530 PACKER et al
10 degrees or more is vanishingly small andinsignificant.
If common levels of tilt and decentration
significantly affected the functioning of wave-front-corrected IOLs, it would be difficult toexplain the evidence of elimination of sphericalaberration and improved functional vision found
in multiple investigations of the Tecnis IOL. Thenew clinically validated eye model described byPiers and coworkers [33] helps relieve this poten-
tial paradox. Areas for future research includeverification of the decentration and tilt of thewavefront-corrected IOL itself.
Customizing the correction of spherical aberration
Another important consideration for the gen-eral applicability of aspheric IOLs involves the
range of spherical aberration in the humancornea. In the design study of the Tecnis IOL, itwas determined that approximately 90% of thepatient population would demonstrate a benefit
from implantation of the IOL [18]. The distribu-tion of corneal spherical aberration found in thestudy population clustered around the mean
such that 10% of subjects would demonstrategreater absolute spherical aberration after implan-tation of the modified prolate IOL than they
would have demonstrated after implantation ofa spherical IOL. Additional data collection sug-gests that the proportion may in fact be closer
to 4% of the population (Fig. 9). Regardless ofthe precise proportion of outliers, it is clear that
Fig. 9. Distribution of corneal spherical aberration
values (N ¼ 202 patients). The Tecnis IOL was designed
to correct the population mean corneal spherical aberra-
tion. A certain percentage of individuals to the left of the
mean are not expected to show a demonstrable benefit
from implantation of an IOL with negative spherical
aberration.
further customization of the spherical aberrationof IOLs could potentially create a wider benefit.
One approach to customization entails selection
of patients based on their preoperative cornealspherical aberration. A limitation, however, of theselection process remains corneal aberrations in-duced by surgery with IOL implantation, particu-
larly astigmatism and trefoil terms [36].Nevertheless, selection has been shown capable ofproducing enhanced results, as demonstrated by
sine wave grating contrast sensitivity with targetedpostoperative total ocular spherical aberration[37]. In his study, Beiko [37] used the Easygraph
corneal topographer (Oculus, Lynnwood, Wash-ington) to select patients with corneal spherical ab-erration ofþ0.37 m, targeting a postoperative totalocular spherical aberration of þ0.10 m (the Easy-
graph includes an optional software package thatprovides Zernike analysis). The selected patientgroup demonstrated significantly better contrast
sensitivity than an unselected group of control pa-tients under bothmesopic andphotopic conditions.
The development and popularization of wave-
front-corrected and aspheric IOLs represents a sig-nificant trend in current cataract and refractive lenssurgery. With preoperative corneal topography
and wavefront analysis, surgeons can achieveenhanced results through patient selection. Onemethod of proceeding with this approach mightinvolve the following protocol:
1. Preoperative testing to include corneal to-
pography and axial length determination, an-terior chamber depth, phakic lens thickness,and corneal white-to-white diameter.
2. Application of a software package, such asVOL-CT (Sarver and Associates, Carbon-dale, Illinois) to transform the topography el-
evation data into preoperative cornealZernike coefficients, with special attentionto Z (4,0), fourth-order spherical aberration.
3. Application of an IOL calculation formula,such as the Holladay 2 (available as part ofthe Holladay IOL Consultant and SurgicalOutcomes Assessment Program, Jack T. Hol-
laday, Houston, Texas) to determine correctIOL power for desired postoperative spheri-cal equivalent.
4. Determination of desired postoperative totalocular spherical aberration and selection ofIOL type.
For example, if the desired postoperative total
ocular spherical aberration is zero and the

531CONTRAST SENSITIVITY, MEASURING CATARACT OUTCOMES
preoperative corneal spherical aberration mea-sures about þ0.27 m, the Tecnis with �0.27 m isselected. If the preoperative corneal sphericalaberration is negative, a spherical IOL might
represent the best choice because it adds to thetotal. This might be the case in a patient who hadundergone previous hyperopic laser in situ kera-
tomileusis or conductive keratoplasty.One challenge of customization, however, is
determining the desired postoperative state. Cat-
aract and refractive surgeons have already facedthis dilemma in terms of lower-order aberrationswhen they decide to target emmetropia, or achieve
slight residual with-the-rule astigmatism. It seemsthat there exists a trade-off between sphericalaberration and depth of focus: ‘‘Although bestcorrected optical quality is significantly better
with aspheric IOLs, tolerance to defocus tendedto be lower’’ [36]. The evidence of the clinical in-vestigation of the Tecnis IOL, and in particular
the results of the wavefront aberrometry and nightdriving simulation, offer a compelling argumentfor setting the postoperative spherical aberration
to zero. The data show that the mean sphericalaberration in the eyes implanted with the TecnisIOL was, in the words approved by the FDA,
‘‘not different from zero,’’ whereas the subjectsperformed functionally better in 20 of 24 drivingconditions (and statistically better in 10 condi-tions) when using best-spectacle correction with
the eye implanted with the Tecnis IOL, as com-pared with best-spectacle correction with the eyeimplanted with the AcrySof spherical IOL [19].
These findings represent the basis for the FDA la-beling indication for improved functional vision,which may improve patient safety for other life
situations under low-visibility conditions.The ability to achieve superior functional
vision with best spectacle correction reflects boththe strength and weakness of wavefront-corrected
IOLs. Given the state of the art of biometry andIOL power calculation, it is not possible toachieve precise emmetropia in all eyes. Many
pseudophakic patients find that their uncorrectedvision is adequate for most tasks of daily livingand do not wear spectacles. The amount of
defocus and astigmatism they accept may negatethe pseudophakic correction of their sphericalaberration. Nio and coworkers [12] noted in
2002, ‘‘Both spherical and irregular aberrationsincrease the depth of focus, but decrease the mod-ulation transfer at high spatial frequencies at opti-mum focus. These aberrations, therefore, play an
important role in the balance between acuity
and depth of focus.’’ For some patients with ade-quate uncorrected distance acuity, the advantagesof a bit more depth of focus may be worth a littleloss of contrast. The ultimate expression of this
trend is embodied in the multifocal IOL, whichby its design reduces optical quality to enhancespectacle independence. The Tecnis multifocal
IOL, currently under study in the United Statesthrough an FDA Investigational Device Exemp-tion, represents a conscious compromise between
optical efficiency and functional vision, and qual-ity of life.
Practical implementation of contrast-sensitivity
testing
The implementation of contrast-sensitivitytesting in practice requires investment in both
technology and training. When shopping for newequipment it behooves the physician to comparetesting systems with respect to validation, func-
tionality, and ease of use. Critical parametersinclude control of luminance, consistency ofviewing distance, and correction of refractive
error. Standardization of testing methods in theoffice ensures comparability of results. Techni-cians should become proficient at practicing theestablished protocols for test administration with
each specific system. In the United States, practi-tioners should note the systems accepted by theFDA in clinical investigations of cataract and
refractive surgery. Frequently cited products in-clude the CSV-1000 (VectorVision, Greenville,Ohio) and the Optec 6500 (Stereo Optical, Chi-
cago, Illinois). A newly introduced product is theHolladay Automated Contrast Sensitivity TestingSystem (M & S Technologies, Skokie, Illinois).
As advances in technology allow cataract andrefractive surgeons to address higher-order opticalaberrations, the measurement of functional visionbecomes increasingly critical as a gauge of progress.
Contrast-sensitivity testing is assuming a pro-minent place in the evaluation of surgical modali-ties because it reflects functional vision, correlates
with visual performance, and provides a key tounderstanding optical and visual processing ofimages.
References
[1] Ginsburg AP. The evaluation of contact lenses and
refractive surgery using contrast sensitivity. Contact
Lenses: Update 1987;56(17):1–56.
532 PACKER et al
[2] Ginsburg AP. Visual form perception based on bio-
logical filtering. In: Spillman L, Wooten DR, editors.
Sensory experience, adaptation and perception. Hill-
sdale (NJ): Lawrence Erlbaum Associates; 1984. p.
53–72.
[3] Evans DW, Ginsburg AP. Contrast sensitivity pre-
dicts age-related differences in highway sign discrim-
inability. Hum Factors 1985;27:637.
[4] McGwin G Jr, Chapman V, Owsley C. Visual risk
factors for driving difficulty among older drivers.
Accid Anal Prev 2000;32:735–44.
[5] Owsley C, Stalvey BT, Wells J, et al. Visual risk fac-
tors for crash involvement in older drivers with cat-
aract. Arch Ophthalmol 2001;119:881–7.
[6] Lord SR, Dayhew J. Visual risk factors for falls in
older people. J Am Geriatr Soc 2001;49:508–15.
[7] Lord SR, Menz HB. Visual contributions to pos-
tural stability in older adults. Gerontology 2000;
46:306–10.
[8] RubinGS, Bandeen-RocheK,HuangGH, et al. The
association of multiple visual impairments with self-
reported visual disability: SEE project. Invest Oph-
thalmol Vis Sci 2001;42:64–72.
[9] Ginsburg AP, Evans DW, Sekule R, et al. Contrast
sensitivity predicts pilots’ performance in aircraft
simulators. Am JOptomPhysiol Opt 1982;59:105–9.
[10] Artal P, Berrio E, Guirao A, et al. Contribution of
the cornea and internal surfaces to the change of oc-
ular aberrations with age. J Opt Soc Am A Opt Im-
age Sci Vis 2002;19:137–43.
[11] Glasser A, Campbell MC. Presbyopia and the opti-
cal changes in the human crystalline lens with age.
Vision Res 1998;38:209–29.
[12] Nio YK, Jansonius NM, Fidler V, et al. Spherical
and irregular aberrations are important for the opti-
mal performance of the human eye. Ophthalmic
Physiol Opt 2002;22:103–12.
[13] Schallhorn SC. Deciphering wavefront higher-order
aberrations. Cataract and Refractive Surgery To-
day. Available at: http://www.crstodayarchive.com/
03_archive/0102/crst0102_1_161.html. Accessed De-
cember 22, 2005.
[14] Rohaly AM,Owsley C.Modeling the contrast-sensi-
tivity functions of older adults. J Opt Soc Am A
1993;10:1591–9.
[15] Artal P, Berrio E, Guirao A, et al. Contribution of
the cornea and internal surfaces to the change of oc-
ular aberrations with age. J Opt Soc Am A 2002;19:
137–43.
[16] Glasser A, Campbell MC. Biometric, optical and
physical changes in the isolated human crystalline
lens with age in relation to presbyopia. Vision Res
1999;39:1991–2015.
[17] Wang L, Dai E, Koch DD, et al. Optical aberrations
of the human anterior cornea. J Cataract Refract
Surg 2003;29:1514–21.
[18] Holladay JT, Piers PA, Koranyi G, et al. A new in-
traocular lens design to reduce spherical aberration
of pseudophakic eyes. J Refract Surg 2002;18:
683–91.
[19] Tecnis foldable ultraviolet light-absorbing posterior
chamber IOL. Package insert. Santa Ana (CA):
Advanced Medical Optics; 2005.
[20] Medicare News. Available at: http://new.cms.hhs.
gov/apps/media/press/release.asp?Counter¼1762.Accessed February 14, 2006.
[21] Packer M, Fine IH, Hoffman RS, et al. Initial clini-
cal experience with an anterior surface modified pro-
late intraocular lens. J Refract Surg 2002;18:692–6.
[22] Mester U, Dillinger P, Anterist N. Impact of a mod-
ified optic design on visual function: clinical compar-
ative study. J Cataract Refract Surg 2003;29:652–60.
[23] Packer M, Fine IH, Hoffman RS, et al. Improved
functional vision with a modified prolate intraocular
lens. J Cataract Refract Surg 2004;30:986–92.
[24] Bellucci R, Scialdone A, Buratto L, et al. Visual acu-
ity and contrast sensitivity comparison between Tec-
nis and AcrySof SA60AT intraocular lenses: a
multicenter randomized study. J Cataract Refract
Surg 2005;31:712–7.
[25] Kennis H, Huygens M, Callebaut F. Comparing the
contrast sensitivity of a modified prolate anterior
surface IOL and of two spherical IOLs. Bull Soc
Belge Ophtalmol 2004;294:49–58.
[26] Kershner RM. Retinal image contrast and func-
tional visual performance with aspheric, silicone,
and acrylic intraocular lenses: prospective evalua-
tion. J Cataract Refract Surg 2003;29:1684–94.
[27] Ricci F, Scuderi G, Missiroli F, et al. Low contrast
visual acuity in pseudophakic patients implanted
with an anterior surfacemodified prolate intraocular
lens. Acta Ophthalmol Scand 2004;82:718–22.
[28] Martinez Palmer A, Palacin Miranda B, Castilla
Cespedes M, et al. Spherical aberration influence in
visual function after cataract surgery: prospective
randomized trial [in Spanish]. Arch Soc Esp Oftal-
mol 2005;80:71–7.
[29] Mester U. Improved optical and visual quality with
aspheric IOL. Presented at the American Society of
Cataract and Refractive Surgery Symposium. Phila-
delphia, June 2, 2002.
[30] Packer M, Fine IH, Hoffman RS. Quality of vision
with a modified anterior prolate aspheric intraocular
lens. Presented at the European Society of Cataract
and Refractive Surgery Symposium. Nice, France,
September 11, 2002.
[31] Dietze HH, Cox MJ. Limitations of correcting
spherical aberration with aspheric intraocular
lenses. J Refract Surg 2005;21:S541–6.
[32] Altmann GE, Nichamin LD, Lane SS, et al. Optical
performance of 3 intraocular lens designs in the pres-
ence of decentration. J Cataract Refract Surg 2005;
31:574–85.
[33] Piers P, Weeber H, Artal P. A verifiedmodel for cus-
tomized IOLs. Presented at the sixth International
Congress on Wavefront Sensing and Optimized
533CONTRAST SENSITIVITY, MEASURING CATARACT OUTCOMES
Refractive Corrections. Athens, Greece, February
12, 2005.
[34] Wang L, Koch DD. Effect of decentration of wave-
front-corrected intraocular lenses on the higher-
order aberrations of the eye. Arch Ophthalmol
2005;123:1226–30.
[35] Packer M. Tilt and decentration: toward a new def-
inition of tolerance. EyeWorld 2005;10:65–6.
[36] Marcos S, Barbero S, Jimenez-Alfaro I. Optical
quality and depth-of-field of eyes implanted with
spherical and aspheric intraocular lenses. J Refract
Surg 2005;21:223–35.
[37] Beiko G. Personalized correction of spherical aber-
ration in cataract surgery. Presented at the American
Academy of Ophthalmology 2005meeting. Chicago,
October 18, 2005.