20 Procedures in Obstetrics and Gynaecology Textbook. Chapter 20. Fetal blood sampling
3
8/12/2019 20 Procedures in Obstetrics and Gynaecology Textbook. Chapter 20. Fetal blood sampling http://slidepdf.com/reader/full/20-procedures-in-obstetrics-and-gynaecology-textbook-chapter-20-fetal-blood 1/3 91 Chapter 20 Fetal Blood Sampling (scalp pH) Linda Rogers Indication To confirm/exclude fetal hypoxia in the presence of an abnormal CTG. Risks Trauma to the fetus Vertical transmission of HIV (therefore only proceed if mother is known to be HIV negative) Accepted normal values pH > 7.25 normal; repeat every 30 minutes if the abnormal CTG pattern continues pH 7.2 – 7.25 repeat as indicated (usually every 30 minutes) pH 7.1 – 7.19 fetal acidosis – expedite delivery pH < 7.1 severe fetal acidosis – deliver immediately Requirements Mother to be at least 4cm dilated Conical Speculum/Amnioscope and KY jelly Ethyl chloride Sponge-holder Cotton wool / 4 x 3cm swabs Petroleum jelly Heparinised capillary tube Blood gas machine Large gauge needle/stylette Method This can be done with the mother in lithotomy, or in the left lateral position with the legs drawn up. Insert the speculum/amnioscope into the vagina, so that the narrow end rests on the fetal scalp (away from any fontanelles). Clean any blood/mucous off the fetal scalp, and spray with ethyl chloride. Dab with petroleum jelly (prevents the fetal blood from flowing away), and make a small nick in the fetal scalp with the needle/stylette. Collect the resulting blood in the heparinised capillary tube, insert into the blood gas machine in order to obtain the pH. Interpret results as above.
Transcript of 20 Procedures in Obstetrics and Gynaecology Textbook. Chapter 20. Fetal blood sampling

8/12/2019 20 Procedures in Obstetrics and Gynaecology Textbook. Chapter 20. Fetal blood sampling
http://slidepdf.com/reader/full/20-procedures-in-obstetrics-and-gynaecology-textbook-chapter-20-fetal-blood 1/3
91
Chapter 20
Fetal Blood Sampling (scalp pH)
Linda Rogers
Indication
To confirm/exclude fetal hypoxia in the presence of an abnormal CTG.
Risks
Trauma to the fetus
Vertical transmission of HIV (therefore only proceed if mother is known to be HIV negative)
Accepted normal values
pH > 7.25 normal; repeat every 30 minutes if the abnormal CTG pattern continuespH 7.2 – 7.25 repeat as indicated (usually every 30 minutes)pH 7.1 – 7.19 fetal acidosis – expedite deliverypH < 7.1 severe fetal acidosis – deliver immediately
Requirements
Mother to be at least 4cm dilated
Conical Speculum/Amnioscope and KY jelly
Ethyl chloride
Sponge-holder
Cotton wool / 4 x 3cm swabs
Petroleum jelly
Heparinised capillary tube
Blood gas machine
Large gauge needle/stylette
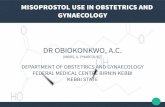
Method
This can be done with the mother in lithotomy, or in the left lateral position with the legsdrawn up. Insert the speculum/amnioscope into the vagina, so that the narrow end rests on thefetal scalp (away from any fontanelles). Clean any blood/mucous off the fetal scalp, and spraywith ethyl chloride. Dab with petroleum jelly (prevents the fetal blood from flowing away), andmake a small nick in the fetal scalp with the needle/stylette. Collect the resulting blood in theheparinised capillary tube, insert into the blood gas machine in order to obtain the pH.Interpret results as above.

8/12/2019 20 Procedures in Obstetrics and Gynaecology Textbook. Chapter 20. Fetal blood sampling
http://slidepdf.com/reader/full/20-procedures-in-obstetrics-and-gynaecology-textbook-chapter-20-fetal-blood 2/3

8/12/2019 20 Procedures in Obstetrics and Gynaecology Textbook. Chapter 20. Fetal blood sampling
http://slidepdf.com/reader/full/20-procedures-in-obstetrics-and-gynaecology-textbook-chapter-20-fetal-blood 3/3
93
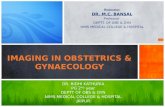
Figure 3
Figure 4