2) Megaloblastic Anemia
17
Department of Medical Sciences Faculty of Medicine University of Brawijaya MEGALOBLASTIC ANEMIA RED CELL DISORDERS
-
Upload
krishnakant-prajapati -
Category
Documents
-
view
228 -
download
0
Transcript of 2) Megaloblastic Anemia
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 1/17
Department of MedicalSciences Faculty of Medicine
University of Brawijaya
MEGALOBLASTIC ANEMIA
RED CELL DISORDERS
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 2/17
Faculty of Medicine University of Brawijaya
Clinical Competencies
Be able to describe:- the etiology of megaloblastic anemia caused byvitamin B12 and folate deficiency
- the pathophysiology of megaloblastic anemia
- the principal management of megaloblastic anemiacaused by vitamin B12 and folate deficiency
Be able to diagnose megaloblastic anemia based onclinical features and laboratory findings
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 3/17
Faculty of Medicine University of Brawijaya
Introduction
Megaloblastic anemiaA heterogeneous group of anemia characteristics:
- RBC are larger: nuclear-to-cytoplasmic ratio >normoblast
- The maturation of nuclei is delayed, cytoplasmicdevelopment is normal
Based on the appearance of developing erythroblasts inthe bone marrow: megaloblastic & non-megaloblastic
There are several causes, but megaloblastic anemia isusually caused by vitamin B12 or folate deficiency.
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 4/17
Faculty of Medicine University of Brawijaya
Etiology
In clinical practice, this is usually caused by vitamin B12 (cobalamine) or folate deficiency .
Causes of vitamin B12 deficiencyNutritional
Malabsorption: gastric and intestinal causesCauses of folate deficiency
NutritionalMalabsorptionExcess urinary folate lossDrugsExcess utilizationMixed
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 5/17
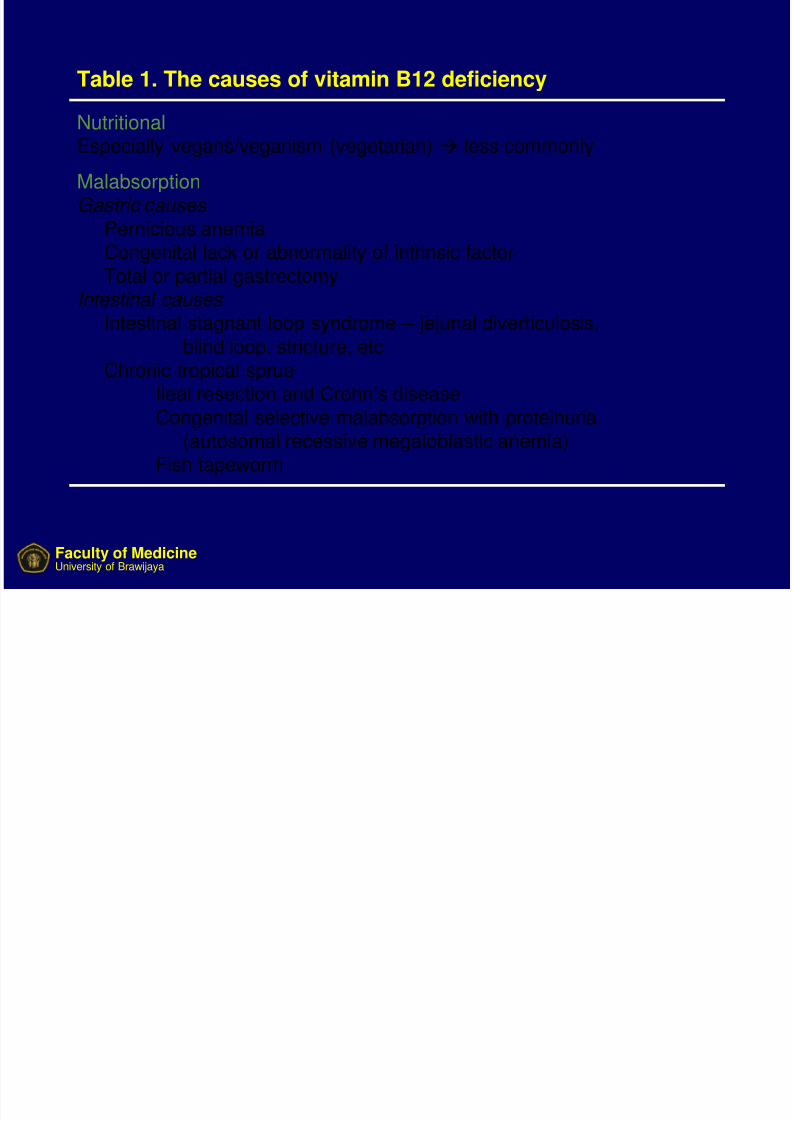
Table 1. The causes of vitamin B12 deficiency
Nutritional Especially vegans/veganism (vegetarian) less commonly
MalabsorptionGastric causes
Pernicious anemiaCongenital lack or abnormality of intrinsic factor
Total or partial gastrectomyIntestinal causes
Intestinal stagnant loop syndrome – jejunal diverticulosis,blind loop, stricture, etc
Chronic tropical sprueIleal resection and Crohn’s disease
Congenital selective malabsorption with proteinuria(autosomal recessive megaloblastic anemia)
Fish tapeworm
Faculty of Medicine University of Brawijaya
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 6/17
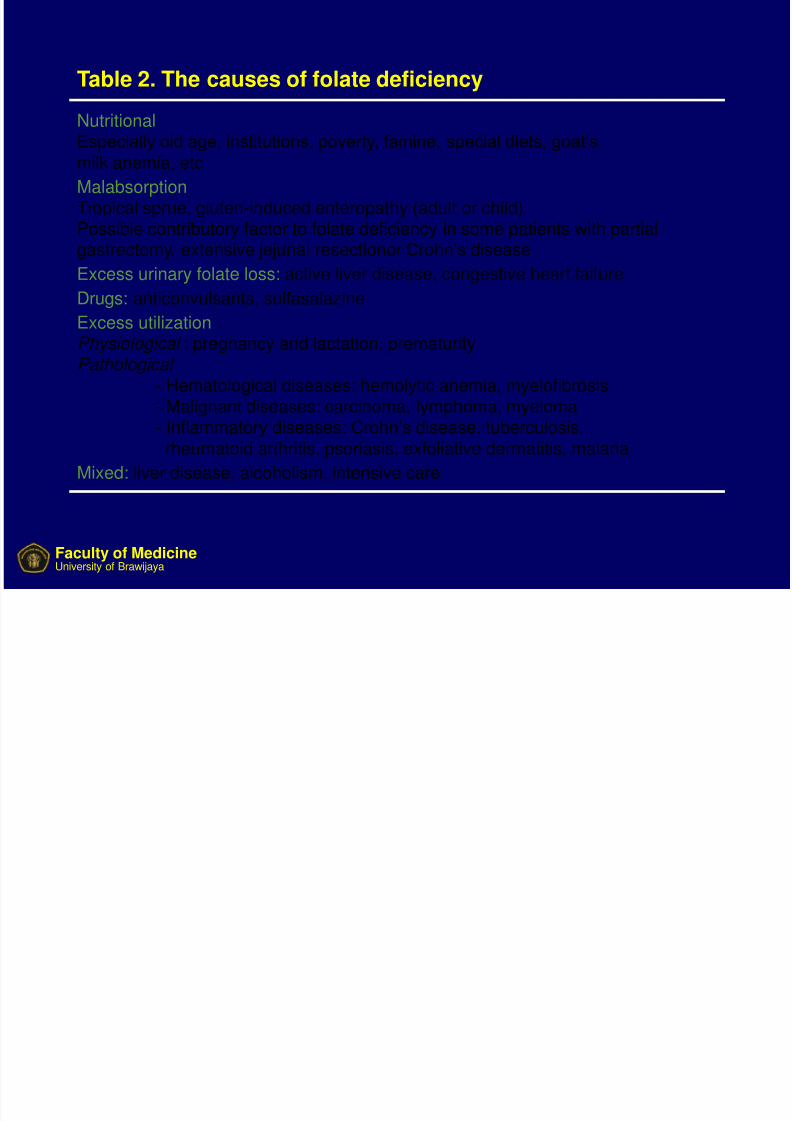
Table 2. The causes of folate deficiency
Nutritional
Especially old age, institutions, poverty, famine, special diets, goat’smilk anemia, etc
MalabsorptionTropical sprue, gluten-induced enteropathy (adult or child)Possible contributory factor to folate deficiency in some patients with partialgastrectomy, extensive jejunal resectionor Crohn’s disease
Excess urinary folate loss: active liver disease, congestive heart failureDrugs: anticonvulsants, sulfasalazine
Excess utilization Physiological : pregnancy and lactation, prematurity Pathological
- Hematological diseases: hemolytic anemia, myelofibrosis
- Malignant diseases: carcinoma, lymphoma, myeloma- Inflammatory diseases: Crohn’s disease, tuberculosis,rheumatoid arthritis, psoriasis, exfoliative dermatitis, malaria
Mixed: liver disease, alcoholism, intensive care
Faculty of Medicine University of Brawijaya
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 7/17
Faculty of Medicine University of Brawijaya
Pathophysiology
The molecular basis: a failure in the synthesis andassembly of DNA.
Cobalamin & folate metabolism are intricately related, andabnormalities in these pathways are believed to lead
to the attenuated production of DNA.Megaloblastosis is caused by interference of folate
metabolism by the inhibition of methionine synthesis.
Dietary folate deficiency the size of the deoxythymidine
triphosphate (dTTP) pool is normal or increased inpersons with megaloblastosis.
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 8/17
Faculty of Medicine University of Brawijaya
Impairment in the deoxyuridine monophosphate (dUMP) &deoxythymidine monophosphate (dTMP) pathway may be
responsible for nutritional megaloblastosis .
The cobalamin-related neuropathy: megaloblastic
changes in hematopoietic cells.Hypothesis for the cause of cobalamin neuropathy:
a defect exists in the conversion of adenosyl-
cobalamin-dependent conversion of methylmalonyl
coenzyme A to succinyl coenzyme A.
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 9/17
Faculty of Medicine University of Brawijaya
A hallmark of megaloblastic anemia is ineffectiveerythropoiesis, as evidenced by :
- erythroid hyperplasia in the bone marrow- a decreased peripheral reticulocyte count
- an elevation in lactate dehydrogenase (LDH) andindirect bilirubin levels.
The pathogenesis of these findings is the intramedullarydestruction of fragile and abnormal megaloblastic
erythroid precursors.
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 10/17
Faculty of Medicine University of Brawijaya
Diagnosis
Based on clinical features and laboratory findings
Clinical Features
Mildly jaundice (lemon yellow tint)
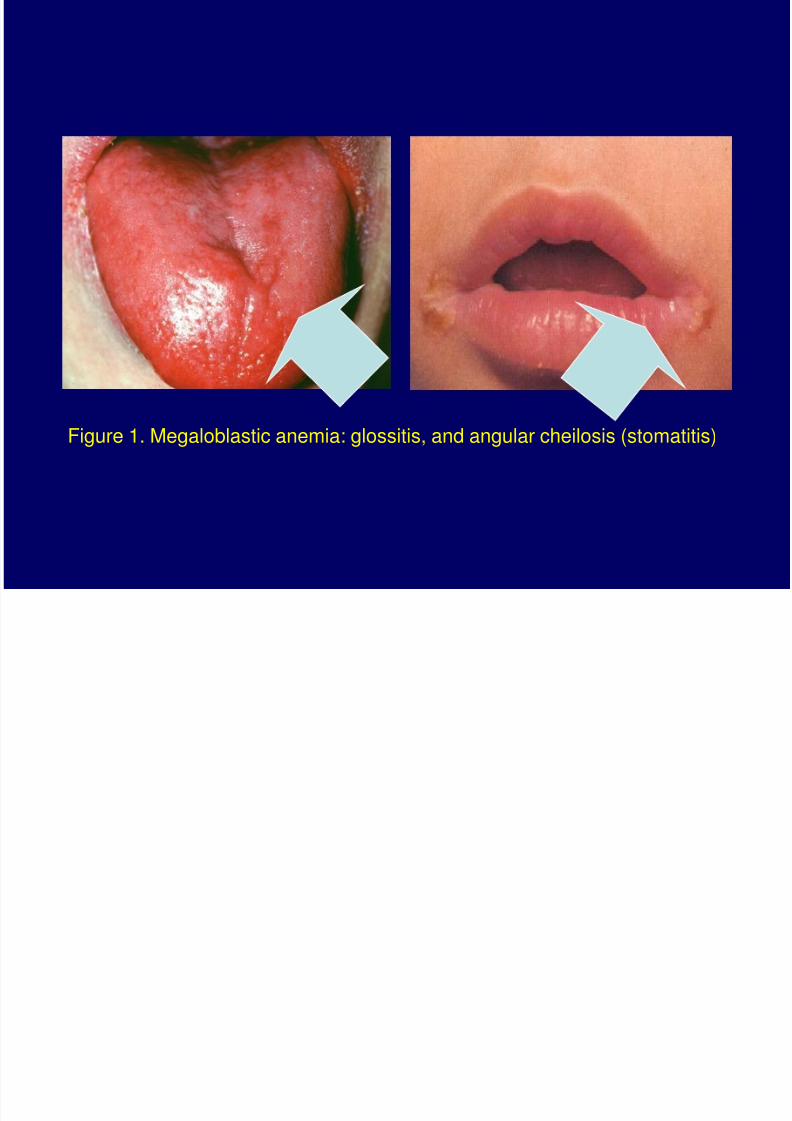
Glossitis (a beefy-red, sore tongue)Angular stomatitis
Mild symptoms of malabsorption with loss of weight
caused by epithelial abnormality
Purpura as a result of thrombocytopenia andwidespread melanin pigmentation
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 11/17
Faculty of Medicine University of Brawijaya
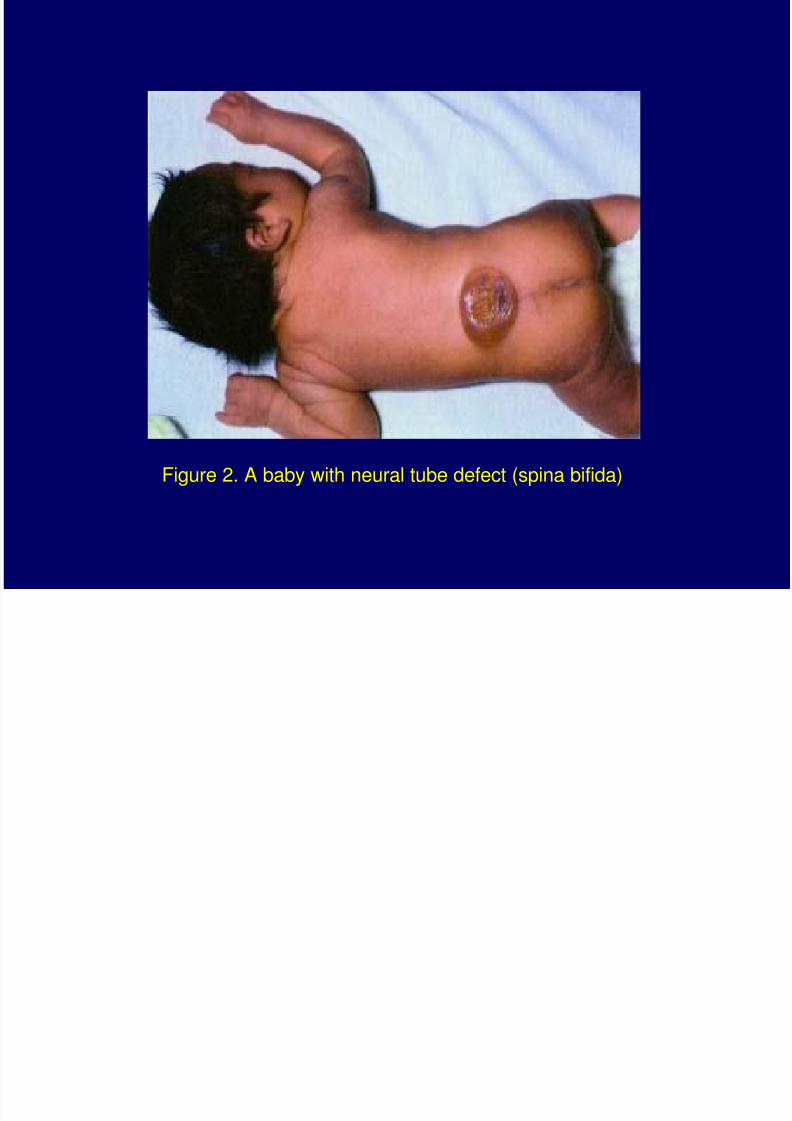
Vitamin B12 neuropathyNeural tube defect (anencephaly, spina bifida or
encephalocele) in the fetus
Cardiovascular disease: myocardial infarct, peripheral
& cerebral vascular disease & venous thrombosisOther tissues abnormalities
- Sterility is frequent in either sex with severe B12 or
folate deficiency
- Morphological abnormalities of cervical, buccal,bladder and other epithelia
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 12/17
Figure 1. Megaloblastic anemia: glossitis, and angular cheilosis (stomatitis)
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 13/17
Figure 2. A baby with neural tube defect (spina bifida)
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 14/17
Faculty of Medicine University of Brawijaya
Laboratory Findings
PancytopeniaIncreased MCV and MCHC
Hypersegmented neutrophils (five lobes or more in
segmented neutrophils)
Increased bilirubinIncreased LDH
Hyperplasia in the bone marrow
Decreased M:E ratio
Reticulocytopenia
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 15/17
Faculty of Medicine University of Brawijaya
Treatment of Megaloblastic Anemia
Vitamin B12 Deficiency Compound: hydroxocobalamine
Route: intramuscular, oral
Dose: 1000 g
Initial dose: 6x1000 g over 1-3 weeks
Maitenance: 1000 g every 3 months
Prophylactic: total gastrectomy, ileal resection
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 16/17
Faculty of Medicine University of Brawijaya
Folate Deficiency Compound: folic acid
Route: oral
Dose: 5 mg
Initial dose: daily for 4 months
Maitenance: depends on underlying disease; life-long
therapy may be needed in chronic inherited hemolytic
anemia, myelofibrosis, renal dialysis
Prophylactic: pregnancy, severe hemolytic anemia,
dialysis, prematurity
8/3/2019 2) Megaloblastic Anemia
http://slidepdf.com/reader/full/2-megaloblastic-anemia 17/17
Faculty of Medicine University of Brawijaya