2. facial,glossopharyngeal,cervical plexus
84
G O O D M O R N I N G
-
Upload
shruti-singh -
Category
Health & Medicine
-
view
18 -
download
2
Transcript of 2. facial,glossopharyngeal,cervical plexus

GOOD
MORNING

Facial Nerve ,
Glossopharyngeal
Nerve & Cervical
Plexus of Nerves

IntroductionFunctional componentsNucleiCourse Branches & DistributionGanglia AssociatedBlood supplyAge changesVariation in branching patternsNerve lesions : supranuclear infranuclearCauses of facial paralysisBells palsyManagement of facial palsyNerve disorders in childrenTesting of facial nerve Applied Anatomy
CONTENTS :FACIAL NERVE

7th cranial nerve
Mixed nerve
motor components
sensory components
2nd arch
INTRODUCTION

SPECIAL VISCERAL EFFERENT (BRANCHIAL)
muscle response for
1, facial expression
2. Elevation of hyoid bone
Functional components

Special visceral afferent
These fibers carry taste sensation from anterior 2/3 rd of tongue& palate

GENERAL VISCERAL EFFERENT (parasympathetic)
Secretomotor to the
•Submandibular gland
•sublingual gland ,
• lacrimal gland ,
• glands of the nose,the palate,and the pharynx

GENERAL SOMATIC EFFERENT
General sensation
from the skin of the concha of the auricle &from a small area behind the ear.

Nuclei
Motor Nucleus
Superior Salivatory nucleus
Upper part of nucleus of tractus solitarius
Upper part of spinal nu of trigeminal nerve

Cranial nerve nuclei


Course of a facial nerve
INTRA CRANIAL
INTRA TEMPORAL
EXTRA CRANIAL

Intra cranial course:
Two roots…..lower border of pons..
motor root medial to sensory root
stylomasoid divide…
Sensory root & motor root passes forwards and laterally leave the …….


Intra Temporal (within Facial Canal )


Extracranial part

Submandibular gland


BRANCHES
Within facial canal
1.Greater petrosal nerve
2.Nerve to stapedius
3.Chorda tympani
At its exits from the stylomastoid foramen
1.Posterior auricular
2.Digastric
3.stylohyoid
Terminal branches
1.Temporal
2.Zygomatic
3.Buccal
4.Mandibular
5.cervical


Greater Petrosal Nerve


Nerve to Stapedius

CHORDA TYMPANI

At its exits from the stylomastoid foramen

TERMINAL BRANCHES


GANGLIA ASSOCIATED WITH THE FACIAL NERVE

location…..
Sensory and parasympathetic -nervus intermedius.
Motor fibers are carried via the facial nerve proper.
greater petrosal nerve, which carries sensory fibers as well as preganglionic parasympathetic fibers
Geniculate ganglion

Pterygopalatine Ganglion

BRANCHES OF PTERYGOPALATINE GANGLION
orbital
palatine
Nasal1.Lateral post.sup nasal nerve
2.Medial post.sup nasal nerve
3.nasopalatine
pharyngeal

SUBMANDIBULAR GANGLION it lies on ….
topograpically…
functionally…

Motor
Superior salivatory nucleus
Nervus intermedius
chorda tympani
Lingual nerve
Ganglion
GLAND
Sympathetic root
Plexus around the facial artery
supply vasomotor fibers to submandibular & sublingual gland
Sensory root
Lingual nerve

Facial nerve – Blood SupplyIntracranial/Meatal: labyrinthine branches from ant .
inf cerebellar artery
Perigeniculate: superficial petrosal branch of middle meningeal artery
Tympanic/Mastoid: stylomastoid branch of posterior auricular artery

Branching Patterns
13%
20%
28%
6%
9%
24%

AGE CHANGES

CLINICAL CONSIDERATION & TESTING OF FACIAL NERVE

CLINICO ANATOMICAL CONSIDERATION by using knowledge of the anatomy of the facial nerve the location of a lesion can be determined by presence or absence of certain deficits



Testing of facial nerve
Topographic testing
1.schirmer’s test
2.Stapedial reflex
3.Taste testing
4.Salivary flow rate & salivary ph
Electro-physiological testing
Nerve excitability testing( NET)
Maximum stimulation test(MST)
Electroneuronography| (ENOG)
Electromyography (EMG)

Topographic testingschirmer’s test

Stapedial reflex
Evaluates…
Impedance audiometry

Taste testing
Electrogustometer

Salivary Flow rate & salivary pH
Normal values:
Saliva ph - 6.7-7.4
Volume – 600-1000 ml/day
Resting flow rate – 0.2-0.4 ml/m
Stimulated flow rate - 2-5 ml/m

Facial paralysis
Upper motor neuron palsy
Lesion above the level of pons
Lower motor neuron palsy
Lesion is in the pons or in the pathway from pons to its exit

UMN LMN
Paralysis of lower ½ of face on C/L side
Total facial paralysis on same side
Emotional movements (e.g. Laughing) are intact.
Emotional movements are lost
Associated hemiplegia No hemiplegia
Hypertonia (spastic). Hypotonia (flaccid).
No fasiculation. Fasiculations are present.
No muscle atrophy. Muscle atrophy occurs later.

Facial nerve disorders

TRAUMA: birth trauma, temporal bone fractures,
skull base fractures, facial injuries middle ear injuries, surgical trauma.
Nervous system disease: Opercular syndrome, Millard-Gubler syndrome.
Infection: of the ear or face,
Herpes zoster of the facial nerve (Ramsey-Hunt syndrome).
Factors causing Facial Nerve Disorders

Metabolic: diabetes mellitus Tumors: acoustic neuroma schwannoma, cholesteatoma, malignant parotid tumors, glomus tumors. Toxins: alcoholism carbon monoxide poisoning.
Bell's palsy: Also called idiopathic facial nerve paralysis

Facial nerve disorders in children

Bell’s palsy
Sudden occurrence of a flaccid facial paralysis in a apparently healthy individual
(1774-1882)

Bell’s phenomenon:

DRUG DOSE PREDNISOLONE Adults: 60 mg daily for five
days, then 40 mg daily for five days
Children: 2 mg per kg daily for seven to 10 days
ACYCLOVIR (ZOVIRAX) Adults: 400 mg five times daily for seven days
Children older than two years: 80 mg per kg daily divided every six hours for five days
Treatment plan
recent research shown that no added benefit of acylovir compared to prednisolone alone for treatment of bell’s palsy

Eye protection Lubricating eye drops, such as artificial tears eye ointments or gels eye patches Facial massage and exercises
Moist heat
Surgical decompression & cosmetic reconstructive surgery
To preventExposure keratitis
About 80% of patients recover spontaneously within 12 weeks

Syndromes associated with Bell’s Palsy
JamesRamsayHuntSyndrome
MelkerssonRosenthalSyndrome
Moebius Syndrome
Gullian barre syndrome

James Ramsay Hunt Syndrome

Melkersson Rosenthal SyndromeFacial palsy
cheilitis
Fissured tongue

Moebius Syndrome
Facial diplegia
Bilateral paralysis of ocular muscles.

Glossopharyngeal nerve
Contents:IntroductionNucleiFunctional componentsCourse Branches & DistributionGanglia AssociatedApplied Anatomy

INTRODUCTIONNinth cranial nerve
3rd arch
Mixed nerve
o Branchio Motor…
o Preganglionic secretomotor…
o general somatic Sensation….
oSpecial visceral (taste) sensation ….
o general visceral sensory…baro n chemo

nuclei

COURSE & RELATIONS
Intra cranial
Attached to lateral side of upper part of the medulla between olivary body & the inferior cerebellar peduncle
It leaves the cranial cavity ….

Extra Cranial Course


Branches
communication
distribution
TympanicCarotid
PharyngealMuscularTonsillarlingual

OTIC GANGLION
Located in…
Topographically…..
Functionally ……

Glossopharyngeal Nerve Testing 1.Taste sensation
2, gag reflex
Afferent – 9th
Efferent – 10th
On tickling the posterior wall of the pharynx ,there is reflex contraction of the throat muscles.
No such contraction occurs when ninth nerve is paralysed

Transient or sustained hypertension : may follow surgical section of nerve reflecting involvement of carotid branch.
Isolated lesions of the nerve are ………
Glossopharyngeal neuralgia:
• bohm & strang
•Middle age
•M = F
• etiology : ……..
Applied anatomy

• Sharp & shooting Pain in the ear, the pharynx, nasopharynx,
tonsil
• Almost invariably unilateral
• Trigger zone - posterior oropharnx, tonsillar fossa
Treatment
Carbamazepine, gabapentin
Surgical : Microvascular decompression Rhizotomy

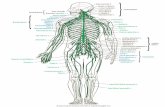
Cervical plexus
Contents:
1.Formation
2.Branches & relations
3.Ansa cervicalis
4.Applied anatomy

Formation of Cervical plexus
Formed by union of……
Each of cervical nerve divides into…….
Ascending branch of the second nerve joins the first nerve
Descending branch of second nerve joins the ascending branch of the third nerve

branches
Cutaneous branch1, lesser occipital nerve
2, greater auricular nerve
3, transverse cutaneous nerve
4, supraclavicular nerve
Muscular branch1, branches to prevertebral nerve
2. Branches to muscle forming boundaries of the posterior triangle
3, pherenic nerve
4, branches to infra hyoid muscle


Course and distribution

muscular branches

Pherenic nerve
•Arises from the…..
•Descends vertically through the lower part of neck and then through the thorax to reach the diaphragm & it enters abdomen also

Formation of Ansa cervicalis
It formed by…….
Superior root is derived from….
Inferior root derived from …..
Two roots join in front of CCA


Applied anatomyAn effective cervical plexus block produces anesthesia over the • neck, • occipital region, • shoulder region• upper pectoral region.
Analgesic solution is infiltrated subcutaneously around the midpoint of the posterior border of sternocleidomastoid

Occasional inadvertent injections into the phrenic and vagus nerves
Miosis (constriction of pupils)Ptosis (drooping of eyelid)Anhydrosis (affected side)enopthalmos
Horner’s syndrome

1. Gray’s anatomy– The anatomical basis of clinical practice, 39th
edition
2.Textbook of anatomy- Inderbir singh, 4th edition
3.B.D. Chaurasias human anatomy, vol 3, 4th edition
4.Cunningham’s Manual Of Practical Anatomy. Vol 3: Head & Neck
& Brain. 15th ed.
5.Clinically oriented anatomy – Moore 6th edition
6.Clinical anatomy by regions – Snells 9th edition
7.The facial nerve – Mays 2nd edition
8. Textbook of human neuroanatomy – Inderbeer Singh 8th edition
9. Head and neck anatomy for dental medicine – Baker
References

Thank you…..