19.bronchial asthma
30
BRONCHIAL ASTHMA
-
Upload
drmanish-kumar -
Category
Health & Medicine
-
view
44 -
download
0
Transcript of 19.bronchial asthma
BRONCHIAL ASTHMA
LEARNING OBJECTIVES
• To know the commonly used drugs in bronchial asthma
• To understand the mechanism of action of the major classes of drugs used in bronchial asthma
• To know the adverse effects of these drugs
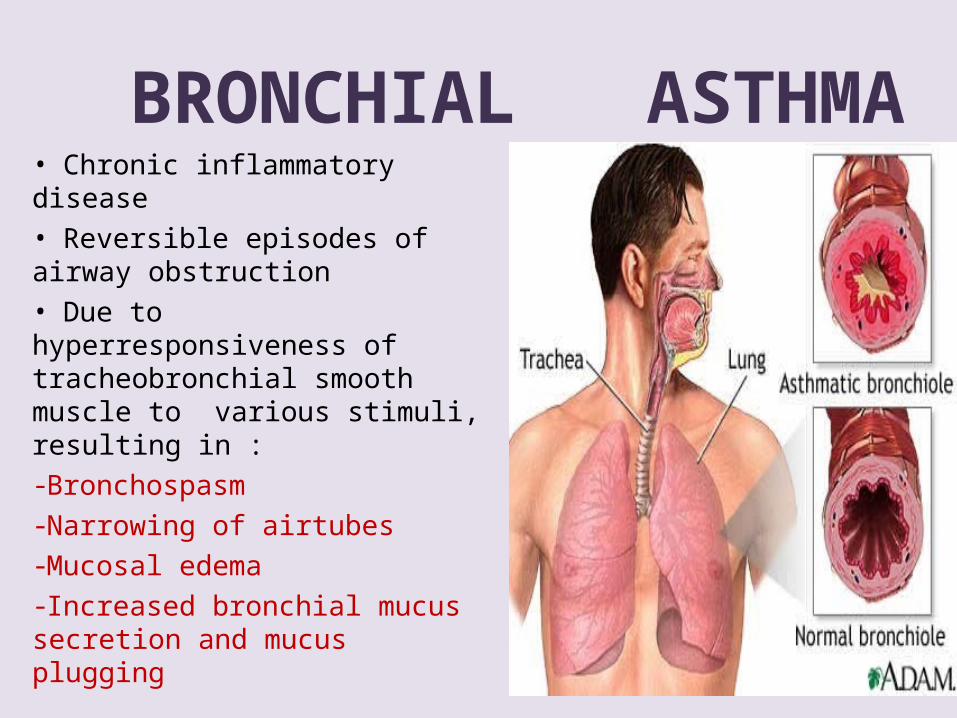
BRONCHIAL ASTHMA• Chronic inflammatory disease• Reversible episodes of airway obstruction• Due to hyperresponsiveness of tracheobronchial smooth muscle to various stimuli, resulting in :-Bronchospasm-Narrowing of airtubes-Mucosal edema-Increased bronchial mucus secretion and mucus plugging
Cardinal symptoms
• Breathlessness
• Wheezing
• Cough
• Chest tightness
Trigger factors for asthma
• Infection• Irritants (pollen, house dust mites, chemical etc.)• Pollutants• Exercise• Exposure to cold air• Psychogenic
Different types of asthma
• Acute asthma• Chronic asthma
• Extrinsic asthma• Intrinsic asthma
Status asthmaticus
Pathophysiology Inflammation underlying hyperactivity• Early reaction – Reversible airway obstruction• Late reaction – Worsening of disease
• Increased vagal discharge to bronchial muscle
Bronchoconstriction and increased mucus secretion
• Adenosine - bronchoconstriction

Approaches to treatment• Prevention of Ag-Ab reaction – avoidence of antigen• Suppression of inflammation and bronchial hyperactivity
– corticosteroids• Prevention of release of mediators – mast cell stabilizers• Antagonism of released mediators – LT antagonists• Blockade of constrictor neurotransmitter –
anticholinergics• Mimicking dilator neurotransmitter – sympathomimetics• Directly acting bronchodilators – methylxanthines
ClassificationA. Bronchodilatorsi. Non-selective sympathomimetics – Adrenaline,
ephedrine, isoprenalineii. Selective beta2 agonists - Salbutamol, terbutaline,
salmeterol, formoteroliii.Anticholinergics – Ipratropium bromide, atropine
methonitrateiv.Methylxanthines – Theophylline, aminophylline, choline
theophyllinate
B. Corticosteroidsi. Systemic – Oral: Prednisone Parenteral : Methylprednisolone,
hydrocortisoneii. Non- systemic – Inhalational : Beclomethasone,
fluticasone, budesonideC. Mast cell stabilizers – Nedocromil, ketotifen, sodium
cromoglycateD.Leukotrine (LT) modulatorsi. 5’- lipoxygenase inhibitors – Zileutonii. LT receptor antagonist – Zafirlukast, montelukast
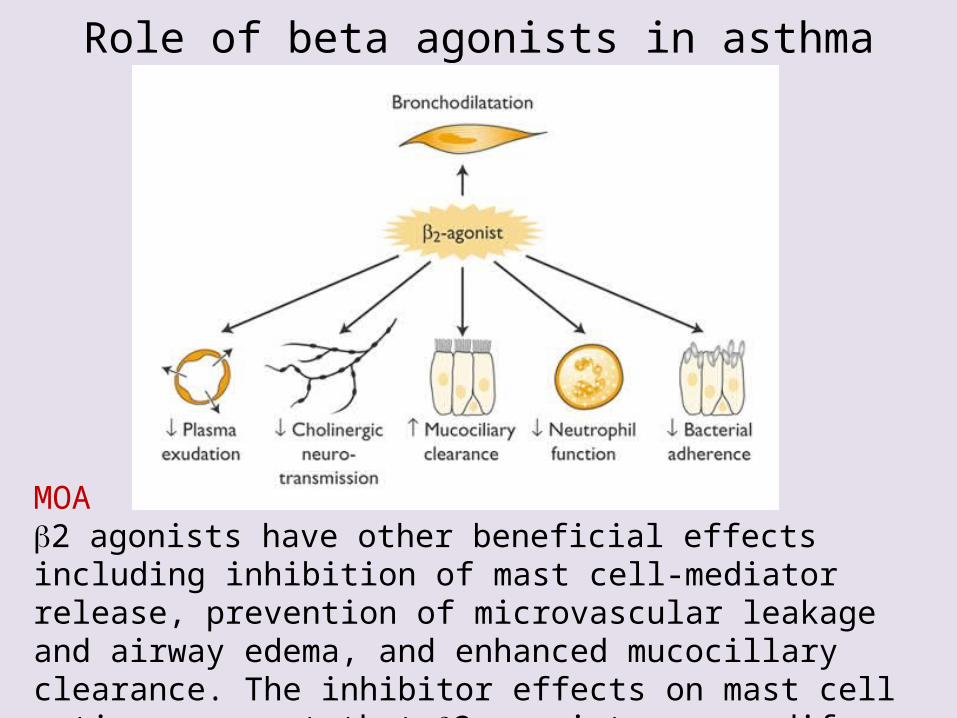
Role of beta agonists in asthma
MOA 2 agonists have other beneficial effects including inhibition of mast cell-mediator release, prevention of microvascular leakage and airway edema, and enhanced mucocillary clearance. The inhibitor effects on mast cell actions suggest that 2 agonists may modify acute inflammation.
SympathomimeticsMode of administration• Inhalation – metered dose
inhaler, nebulizer, spinhaler, rotahaler, spray
• Oral• i.m. or i.v. injection
• Adrenaline – prompt but short-lasting action; rarely used because of adverse effects
• Isoprenaline – prompt and marked bronchodilatation; disadvantage – tachycardia
• Ephedrine – mild slowly developing bronchodilatation; used for mild to moderate asthma
• Salbutamol – inhaled drug – rapid onset, short duration of action; used for acute attack
A/E: tremors, tachycardia, palpitation, nervousness
• Terbutaline – can be used safely during pregnancy
• Salmeterol – slow onset of action, long acting; used for maintenance therapy and nocturnal asthma
• Formoterol – faster onset of action, long acting; used for acute attack and maintenance therapy
Limitations• Non-selective sympathomimetics – cardiac side effects
(β1 action) – not preferred in elderly or heart patients
• Long term use of salbutamol and terbutaline – downregulation of receptors – diminished responsiveness – worsening of disease
Anticholinergics• MOA• Atropine and ipratropium antagonize
the actions of Ach at parasympathetic, postganglionic, effector cell junctions by competing with Ach for M3 receptor sites.
• This antagonism of Ach results in airway smooth muscle relaxation and bronchodilation.
Anticholinergics• Mode of administration - inhalation• Slow onset of action – better suited for regular
prophylactic use • Indications –
– Asthmatic bronchitis– Psychogenic asthma
COPD Nebulized ipratropium + salbutamol – refractory asthma
Methylxanthines• MOA –i. Inhibition of phosphodiesterase – increased
cAMP and cGMP level ii. Blockade of adenosine receptors• Mode of administration - oral, i.m., i.v. , rectal
suppositories
Plasma therapeutic range – 5-20 µg/mlSide effects :• GIT: nausea, vomiting, gastritis, aggravation of
peptic ulcer• CVS: tachycardis, palpitation, arrhythmias,
hypotension• CNS: insomnia, headache, delirium,
restlessness, tremor• Diuresis, flushing• Rapid i.v. – syncope and sudden death
Methylxanthines x Sympathomimetics
potentiate the effects of sympathomimetics • Bronchodilatation – beneficial• Cardiac stimulation - harmful
CorticosteroidsMOA:• Decreases the synthesis of inflammatory mediators• Prevent recruitment, proliferation and activation of
leukocytesSystemic steroid therapy – • Severe chronic asthma• Status asthmaticus Inhaled steroids – Long term treatment of asthma
• Others Indications RhinitisNasal polyposisAdverse effects Inhaled steroids– drymouth, dysphonia, sore throat,
oropharyngeal candidiasis
Systemic steroids – mood changes, osteoporosis, hyperglycemia, hypertension, HPA axis suppression
• MOA – They block IgE-regulated calcium channels
essential for mast cell degranulation– Prevent the release of histamine and related
mediators.
Mast cell stabilizers
Mast cell stabilizers
Mode of administration - inhalation, oralIndications• Bronchial asthma• Allergic rhinitis – nasal spray• Allergic conjunctivitis – eye dropsAdverse effects - irritation, cough, dry mouth,
sedation, headache, rashes
Leukotriene modulators
IndicationsProphylactic treatment of mild to moderate
asthmaAdverse effectsHepatotoxicity, headache, GI distress, rashesZafirlukast – Churg-Strauss syndrome
Treatment of status asthmaticus• Humidified oxygen inhalation• Nebulized salbutamol+ ipratropium• Systemic steroids – hydrocortisone,prednisolone i.v.• IV fluids – correct dehydration• Potassium supplements – correct hypokalemia• Sodium bicarbonate – treat acidosis• Antibiotics – treat infection
Drugs contraindicated in bronchial asthma
• Beta blockers• Cholinergic drugs• NSAIDs ( expect paracetamol)
Recent advances
Omalizumab - anti IgE antibody