
195445265-Acls
73
Advanced Cardiovascular Life Support (ACLS) 2010 Heart and Stroke Foundation of Canada Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiovascular Care (ECC)
-
Upload
ramon-carlo-almiranez -
Category
Documents
-
view
5 -
download
0
description
algorithm
Transcript of 195445265-Acls

Advanced Cardiovascular
Life Support (ACLS)
2010 Heart and Stroke Foundation of
Canada Guidelines for Cardiopulmonary
Resuscitation (CPR) and Emergency
Cardiovascular Care (ECC)

2010 ACLS Guidelines
Science updates to CPR and ECC
• Basic Life Support
• ACLS
• Acute Coronary Syndrome
• Electrical Therapies
• CPR Techniques and Devices
• Stroke
• Ethical Issues
• Education, Implementation, and Teams

Evidence Evaluation Process
• International consensus • Extensive review of resuscitation literature • Peer-reviewed studies • Rigorous disclosure and management of conflicts of
interest
The road to change
BLS Survey
2010 Heart and Stroke Foundation of
Canada Guidelines for Cardiopulmonary
Resuscitation (CPR) and Emergency
Cardiovascular Care (ECC)

High Quality Chest Compressions
“push hard and push fast”
Chest Compressions
To deliver effective chest compressions, you must: • Rate: at least 100/minute • Depth:
• 2 inches [5 cm] in adults and children • 1.5 inches [4 cm] infants
• Allow full chest recoil • Minimize interruptions • Avoid excessive ventilation
High-Quality Chest Compression

For adults, at least 2 inches (5 cm)
Compression Depth At Least 2 Inches

Compression -to- ventilation ratio

Questions?
Change “A-B-C” to “C-A-B”

Chest compressions
and early defibrillation.
Chest compressions

Elimination of Look, Listen, and Feel

Cricoid pressure is a technique
of applying pressure to the
victim’s cricoid cartilage to push
the trachea posteriorly and
compress the esophagus against
the cervical vertebrae. Cricoid
pressure can prevent gastric
inflation and reduce the risk of
regurgitation and aspiration
during bag mask ventilation, but
it may also impede ventilation.
Definition of Cricoid Pressure
Cricoid Pressure During Ventilation Not Recommended
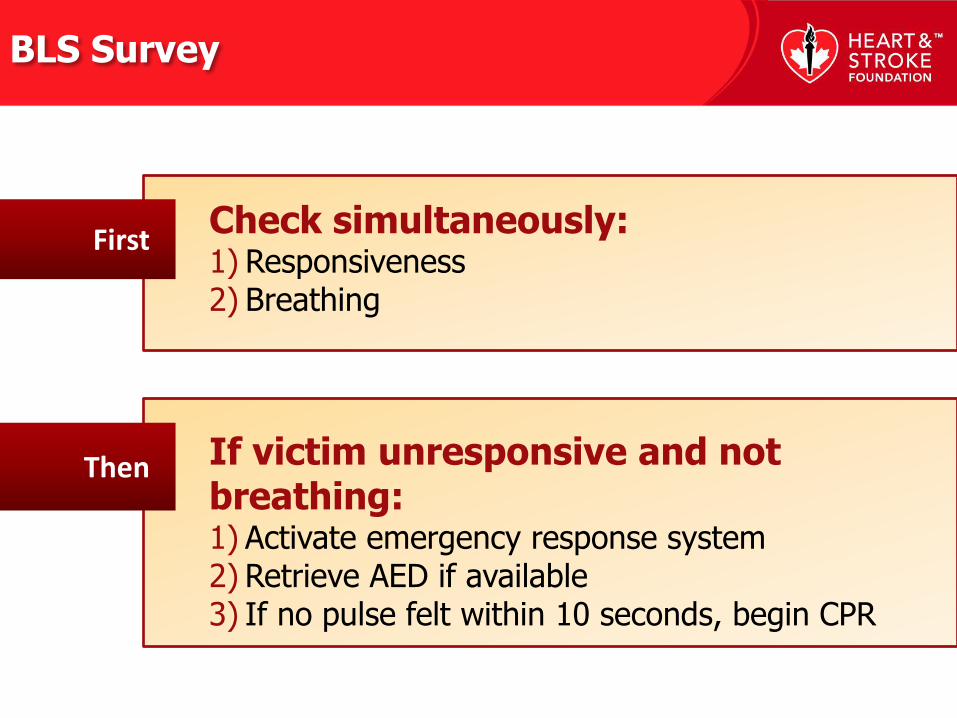
Check simultaneously: 1) Responsiveness 2) Breathing
If victim unresponsive and not breathing: 1) Activate emergency response system 2) Retrieve AED if available 3) If no pulse felt within 10 seconds, begin CPR
First
Then
BLS Survey

16 16

Advanced
Cardiovascular Life
Support
2010 Heart and Stroke Foundation of
Canada Guidelines for Cardiopulmonary
Resuscitation (CPR) and Emergency
Cardiovascular Care (ECC)

Simplified Cardiac Arrest Algorithm
Monitoring to Optimize CPR
Post-Cardiac Care
Airway Management
Advanced Cardiovascular Life Support
Overview

Simplified ACLS Algorithm

Adult arrest algorithm


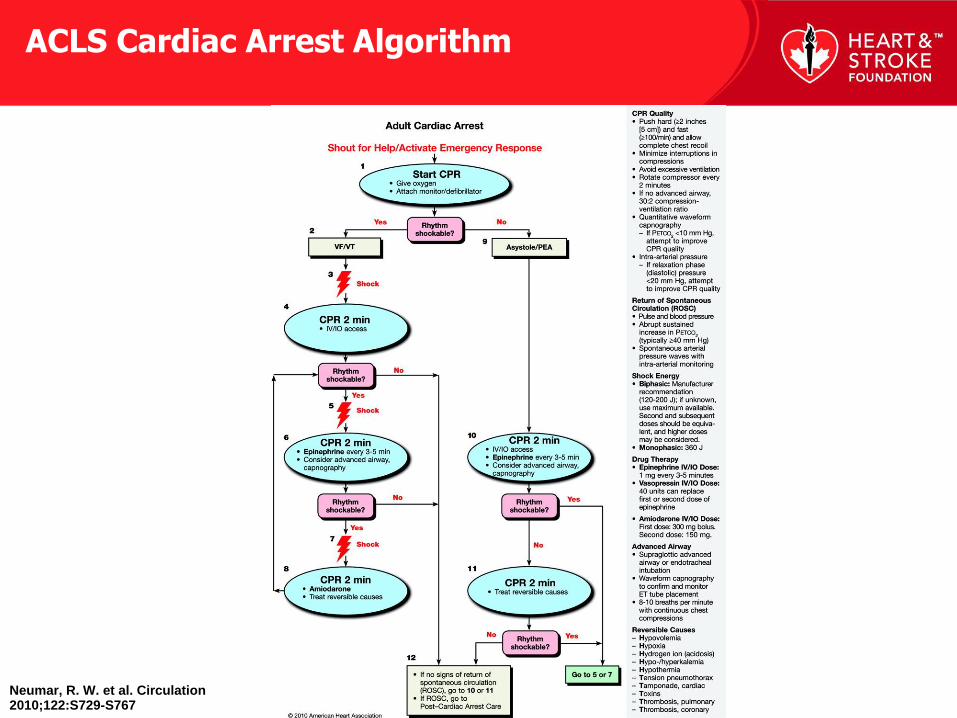
Neumar, R. W. et al. Circulation 2010;122:S729-S767
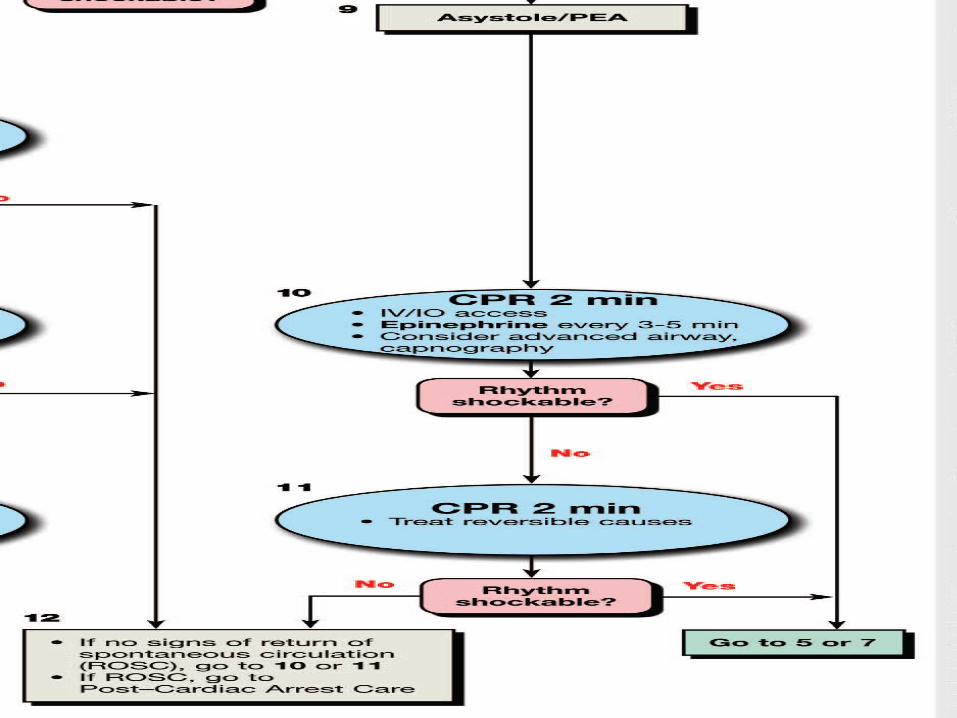
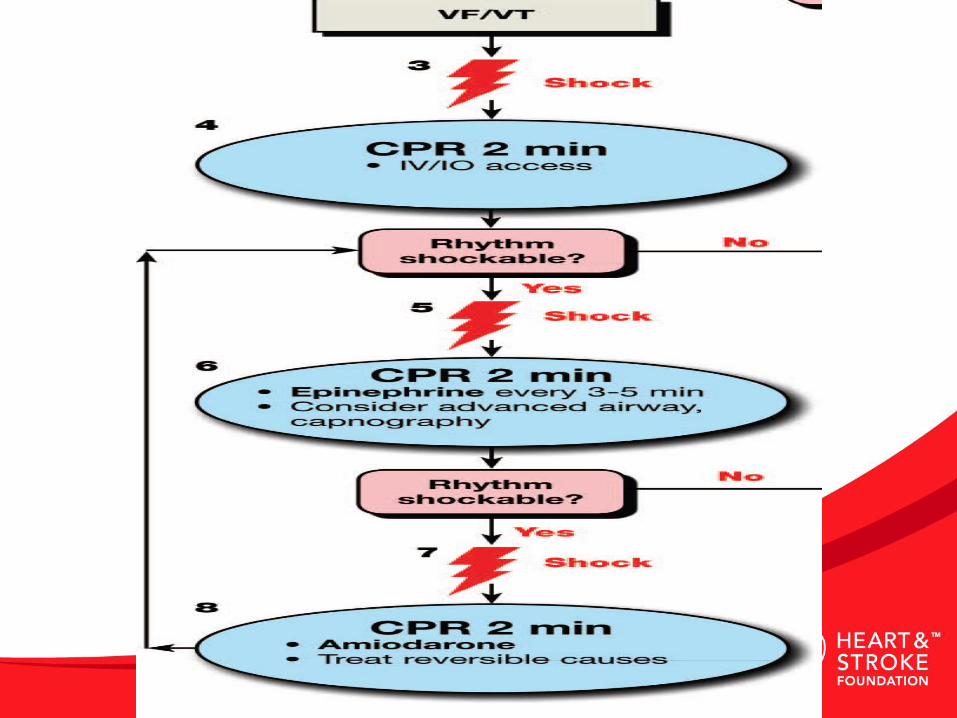
ACLS Cardiac Arrest Algorithm

Neumar, R. W. et al. Circulation 2010;122:S729-S767
Tachycardia Algorithm
Neumar, R. W. et al. Circulation 2010;122:S729-S767
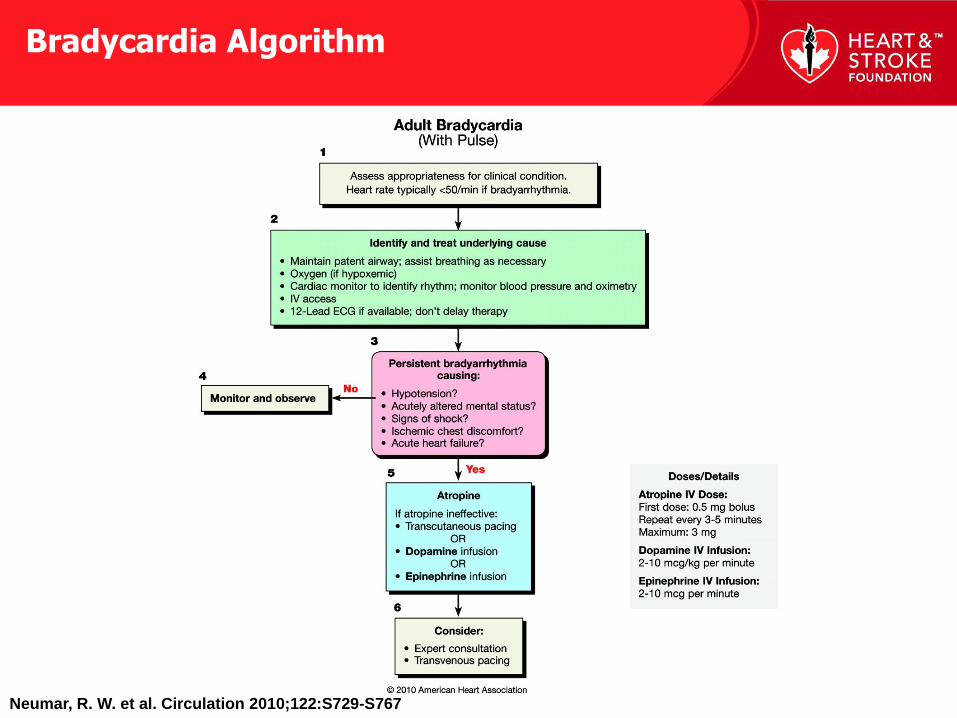
Bradycardia Algorithm

Questions?
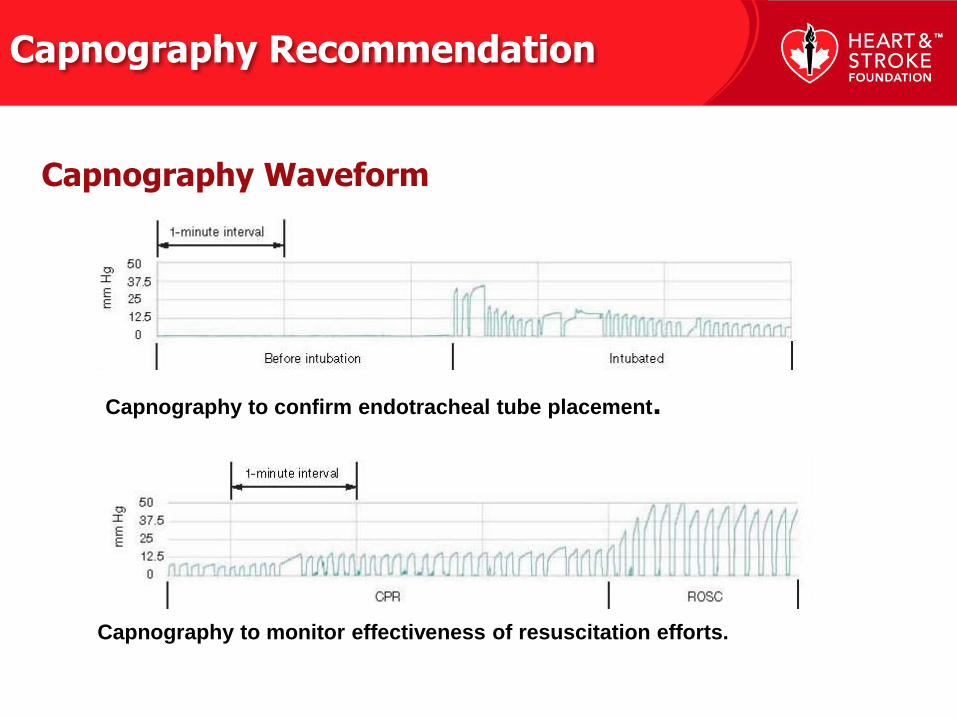
Capnography Recommendation
Capnography to confirm endotracheal tube placement.
Capnography to monitor effectiveness of resuscitation efforts.
Capnography Waveform
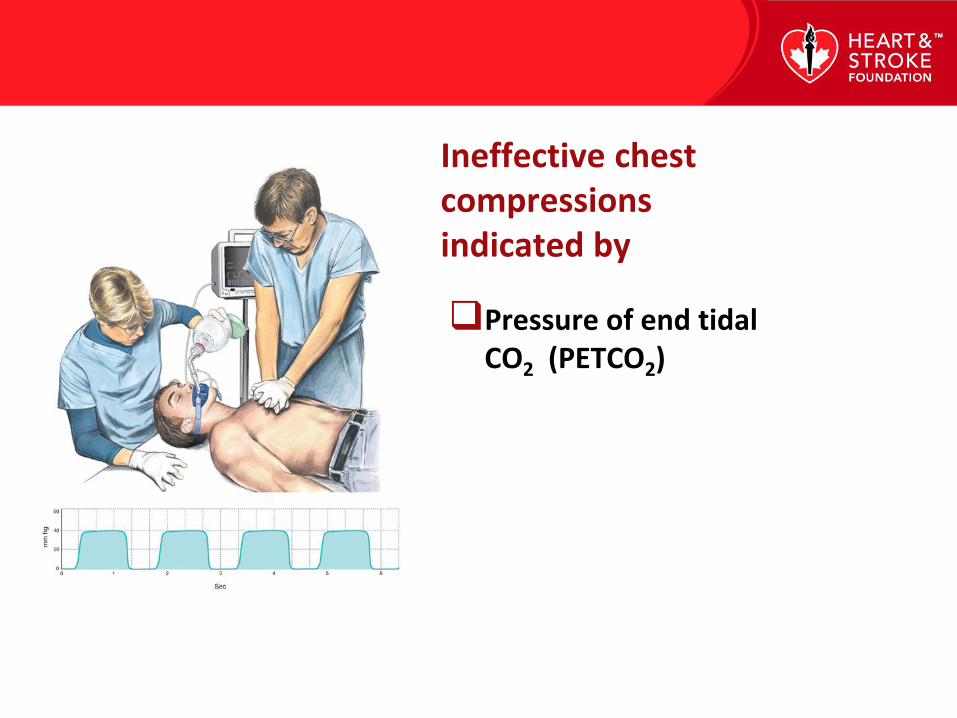
Pressure of end tidal CO2 (PETCO2)
Ineffective chest compressions indicated by
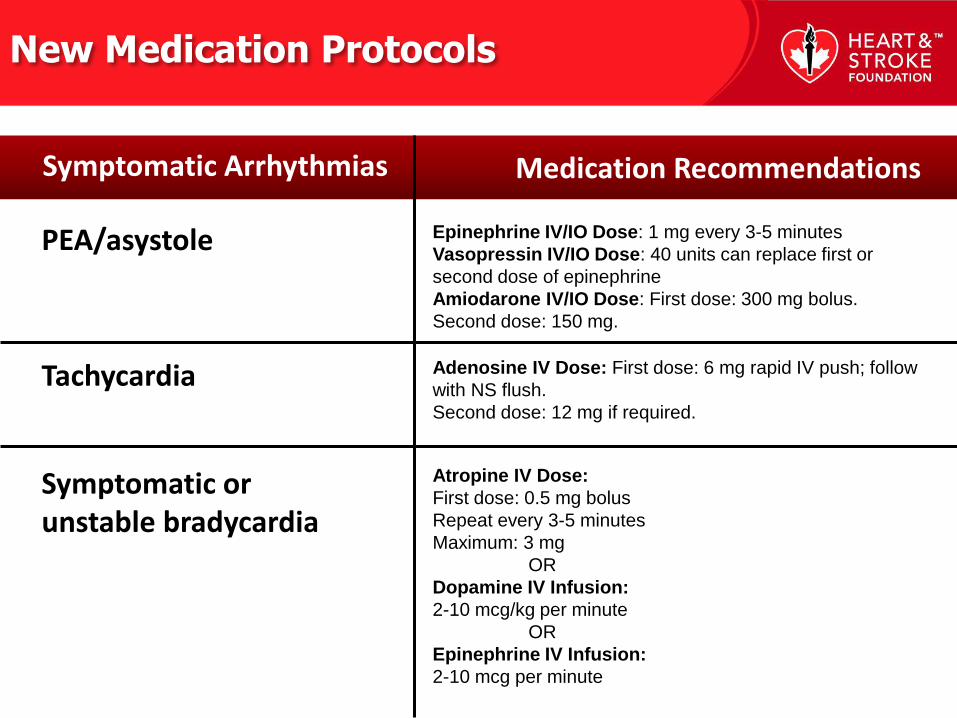
PEA/asystole
Medication Recommendations Symptomatic Arrhythmias
New Medication Protocols
Epinephrine IV/IO Dose: 1 mg every 3-5 minutes
Vasopressin IV/IO Dose: 40 units can replace first or
second dose of epinephrine
Amiodarone IV/IO Dose: First dose: 300 mg bolus.
Second dose: 150 mg.
Atropine IV Dose:
First dose: 0.5 mg bolus
Repeat every 3-5 minutes
Maximum: 3 mg
OR
Dopamine IV Infusion:
2-10 mcg/kg per minute
OR
Epinephrine IV Infusion:
2-10 mcg per minute
Adenosine IV Dose: First dose: 6 mg rapid IV push; follow
with NS flush.
Second dose: 12 mg if required.
Tachycardia
Symptomatic or unstable bradycardia

Organized Post-Cardiac Care

Hemodynamic Neurologic Metabolic
Improved Survival
Effect of Hypothermia on Prognostication
Positive results from therapeutic hypothermia

Oxygen Saturation
Oxygen Saturation

Asthma
Anaphylaxis
Pregnancy
Morbid obesity
Pulmonary embolism
Electrolyte imbalance
Ingestion of toxic substances
Trauma
Accidental hypothermia
Avalanche
Drowning
Electric shock/lightning strikes
Percutaneous coronary intervention
Cardiac tamponade
Cardiac surgery
Special Resuscitation Situations

Acute Coronary
Syndromes
2010 Heart and Stroke Foundation of
Canada Guidelines for Cardiopulmonary
Resuscitation (CPR) and Emergency
Cardiovascular Care (ECC)
The primary goals of therapy for patients with ACS include the need to:
• Reduce the amount of myocardial necrosis • Prevent major adverse cardiac events • Treat acute, life-threatening complications
ACS
Systems of Care for Patients With ST-Elevation Myocardial Infarction (STEMI)
1 • Educational programs
2 • EMS protocols
3 • ED & hospital transports
STEMI Systems of Care

Triage to Capable Hospital

Cardiac Catheterization

Questions?

Electrical Therapies
2010 Heart and Stroke Foundation of
Canada Guidelines for Cardiopulmonary
Resuscitation (CPR) and Emergency
Cardiovascular Care (ECC)

Defibrillation | Cardioversion | Pacing
Electrical Therapy

Healthcare Provider AED Recommendations

AED Use in Children Includes Infants

1-shock defibrillation protocol followed by immediate CPR
One-Shock Protocol Versus Three-Shock Sequence
Defibrillation Waveforms and Energy Levels
200 J

Pediatric Defibrillation
2 J/kg

Fixed and Escalating Energy
0
50
100
150
200
250
300
350
400
Escalating Energy Levels
Joules
Electrode Placement
Anterior-lateral
Anterior-posterior
Anterior-left infrascapular
Anterior-right infrascapular

Defibrillation With Implanted Cardioverter Defibrillator
Anterior-posterior or
Anterior-lateral
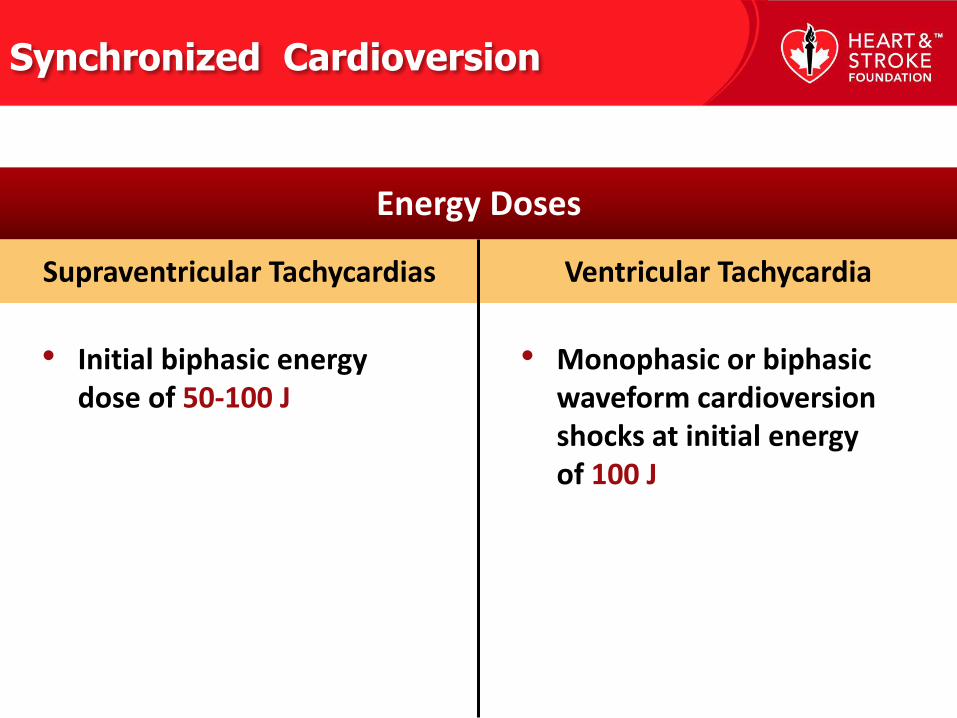
Ventricular Tachycardia Supraventricular Tachycardias
• Initial biphasic energy dose of 50-100 J
• Monophasic or biphasic waveform cardioversion shocks at initial energy of 100 J
Synchronized Cardioversion
Energy Doses

The value of VF waveform analysis to guide defibrillation management during resuscitation is uncertain.
Fibrillation Waveform Analysis

CPR Techniques and
Devices
2010 Heart and Stroke Foundation of
Canada Guidelines for Cardiopulmonary
Resuscitation (CPR) and Emergency
Cardiovascular Care (ECC)

Recommended Devices
No resuscitation device other than a
defibrillator has consistently improved long-term survival from out-of-hospital cardiac arrest.
The precordial thump is a CPR technique used by healthcare professionals in the initial response to a witnessed cardiac arrest when no defibrillator is immediately available.
Definition of Precordial Thump
Use of Precordial Thump Not Recommended

Stroke
2010 Heart and Stroke Foundation of
Canada Guidelines for Cardiopulmonary
Resuscitation (CPR) and Emergency
Cardiovascular Care (ECC)
Stroke Care
• Detection
• Dispatch
• Delivery
• Door
• Data
• Decision
• Drug
• Disposition

Stroke-Prepared Hospital
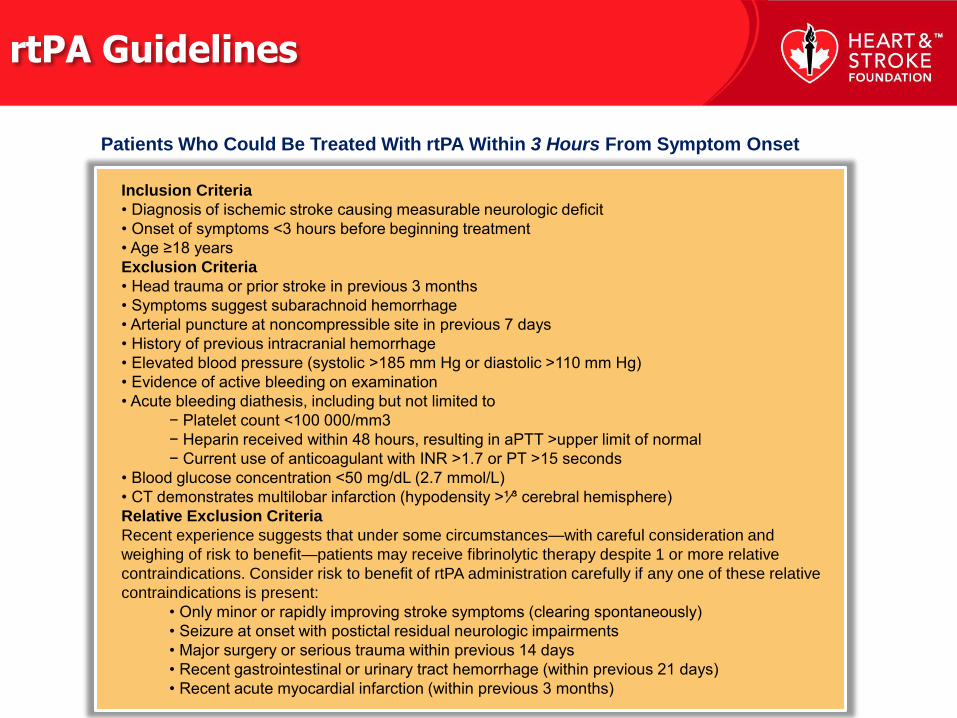
rtPA Guidelines
Inclusion Criteria
• Diagnosis of ischemic stroke causing measurable neurologic deficit
• Onset of symptoms <3 hours before beginning treatment
• Age ≥18 years
Exclusion Criteria
• Head trauma or prior stroke in previous 3 months
• Symptoms suggest subarachnoid hemorrhage
• Arterial puncture at noncompressible site in previous 7 days
• History of previous intracranial hemorrhage
• Elevated blood pressure (systolic >185 mm Hg or diastolic >110 mm Hg)
• Evidence of active bleeding on examination
• Acute bleeding diathesis, including but not limited to
− Platelet count <100 000/mm3
− Heparin received within 48 hours, resulting in aPTT >upper limit of normal
− Current use of anticoagulant with INR >1.7 or PT >15 seconds
• Blood glucose concentration <50 mg/dL (2.7 mmol/L)
• CT demonstrates multilobar infarction (hypodensity >¹⁄³ cerebral hemisphere)
Relative Exclusion Criteria
Recent experience suggests that under some circumstances—with careful consideration and
weighing of risk to benefit—patients may receive fibrinolytic therapy despite 1 or more relative
contraindications. Consider risk to benefit of rtPA administration carefully if any one of these relative
contraindications is present:
• Only minor or rapidly improving stroke symptoms (clearing spontaneously)
• Seizure at onset with postictal residual neurologic impairments
• Major surgery or serious trauma within previous 14 days
• Recent gastrointestinal or urinary tract hemorrhage (within previous 21 days)
• Recent acute myocardial infarction (within previous 3 months)
Patients Who Could Be Treated With rtPA Within 3 Hours From Symptom Onset

Magnitude of benefits from treatment in a stroke unit are comparable to magnitude of effects achieved with rtPA.
Stroke Unit Care

Management of Hypertension
Potential Approaches to Arterial Hypertension in Acute Ischemic Stroke
Patients Who Are Potential Candidates for Acute Reperfusion Therapy
Patient otherwise eligible for acute reperfusion therapy except that blood pressure is >185/110 mm Hg:
• Labetalol 10-20 mg IV over 1-2 minutes, may repeat × 1, or
• Nicardipine IV 5 mg per hour, titrate up by 2.5 mg per hour every 5-15 minutes, maximum 15 mg per hour;
when desired blood pressure is reached, lower to 3 mg per hour, or
• Other agents (hydralazine, enalaprilat, etc) may be considered when appropriate
If blood pressure is not maintained at or below 185/110 mm Hg, do not administer rtPA.
Management of blood pressure during and after rtPA or other acute reperfusion therapy:
Monitor blood pressure every 15 minutes for 2 hours from the start of rtPA therapy, then every
30 minutes for 6 hours, and then every hour for 16 hours.
If systolic blood pressure 180-230 mm Hg or diastolic blood pressure 105-120 mm Hg:
• Labetalol 10 mg IV followed by continuous IV infusion 2-8 mg per minute, or
• Nicardipine IV 5 mg per hour, titrate up to desired effect by 2.5 mg per hour every 5-15 minutes, maximum
15 mg per hour
If blood pressure not controlled or diastolic blood pressure >140 mm Hg, consider sodium nitroprusside.

Questions?

Ethical Issues
2010 Heart and Stroke Foundation of
Canada Guidelines for Cardiopulmonary
Resuscitation (CPR) and Emergency
Cardiovascular Care (ECC)
Ethical issues relating to resuscitation are complex.

Arrest not witnessed by EMS provider or first responder
No ROSC after three complete rounds of CPR and AED analyses
No AED shocks were delivered
Terminating Resuscitative Efforts in Adults with Out-of-Hospital Cardiac Arrest (OHCA)
Arrest not witnessed No bystander CPR
was provided No ROSC after
complete ALS care in the field
No shocks were delivered
“ALS termination of resuscitation” rule was established to consider terminating resuscitative efforts prior to ambulance transport if all of the following criteria are met:
v
Prognostic Indicators in the Adult Post-Arrest Patient Treated with Therapeutic Hypothermia

Education,
Implementation, and
Teams 2010 Heart and Stroke Foundation of
Canada Guidelines for Cardiopulmonary
Resuscitation (CPR) and Emergency
Cardiovascular Care (ECC)

Learn and Live
Chain of Survival

Thank you.


















