16017942-Anaemia

of 83
-
Upload
krishnakant-prajapati -
Category
Documents
-
view
220 -
download
0
Transcript of 16017942-Anaemia
-
8/3/2019 16017942-Anaemia
1/83
ANAEMIA
-
8/3/2019 16017942-Anaemia
2/83
Is present where there is a decrease in the number of circulating
red cells, a decrease in the amount of haemoglobin in the blood or a
haematocrit below the normal range.
DEFINITIONS IN HAEMATOLOGY
Mean corpuscular Haematocrit
volume (MCV) Red cells count
Mean corpuscular Haemaglobin x 10
haemaglobin (MCH) Red cells count
Mean corpuscular Haemaglobin x 10
haemaglobin Haematocrit
concentration (MHCH)
N = 80 96 =
=
=
N = 27 33 pg
N = 32 35 g/dL
-
8/3/2019 16017942-Anaemia
3/83
Clinical features
Symptoms (all non - specific):
fatigue
headachesfaintness
breathlessness
angina of effort
intermitent claudication
palpitations
-
8/3/2019 16017942-Anaemia
4/83
Signs:
2. Non / specific signs include: pallor
tachycardia a full pulse systolic flow murmur cardiac failure ankle oedema rarely papilloedema and retinal haemorrhage in an acute
bleed
3. Specific signs:
koilonychia spoon-shape nails seen in iron deficiencyanaemia
jaundice haemolytic anaemia bone deformities thalassemia major
leg ulcers sickle cell disease
-
8/3/2019 16017942-Anaemia
5/83
Classification:2. Hypochromic microcytic with low mean corpuscular volume
(MCV)3. Normochromic normocytic with a normal MCV
4. Macrocytic with a high MCV
Special investigations: bone marrow aspiration from the sternum or posterior illiaccrest is performed to:
confirm a diagnostic made from peripheral blood count
determine the cellularity of the marrow determine the type of erythropoiesis
determine the proportion of the various lines
see wether the marrow is unfiltrated
determine the size of the iron stores
-
8/3/2019 16017942-Anaemia
6/83
MYCROCYTIC ANAEMIA
small cells (microcytes)
low MCV (< 80 L)
iron content
ragged normoblasts
small cells (microcytes)
low MCV (< 80 L)
normal iron content hyperplastic
Iron deficiency anaemia
Thalassaemia
Sideroblastic anaemia
}
}
-
8/3/2019 16017942-Anaemia
7/83
1.IRON DEFICIENCY
the commonest cause of mycrocitic anaemia
the average daily diet contains 15 20 mg of iron, but only 10%is absorbed
absorption: duodenum and jejunum
ferrous iron is absorbed better than ferric
gastric acidity helps to keep iron in the ferrous state andsoluble in the upper gut
-
8/3/2019 16017942-Anaemia
8/83
transport in the blood:
transported in the plasma bound to transferin, beta globulinesynthesized in the liver
iron stores in the tissues as ferritin and haemosiderin (1000 1500 mg)
requirements:
each day 0.5 1 mg of iron are lost in the faeces, urine andsweat
menstruating women lose 0.7 mg iron / day of menstruation
pregnancy and groth iron demand
-
8/3/2019 16017942-Anaemia
9/83
CAUSES OF IRON DEFICIENCY
2. Poor intake
3. Decreased absorption
4. Increased demands
5. Blood loss
The commonest cause of iron deficiency:
Blood lost from G.I. tractMenstruation
-
8/3/2019 16017942-Anaemia
10/83
-
8/3/2019 16017942-Anaemia
11/83
-
8/3/2019 16017942-Anaemia
12/83
Clinical features:
brittle nails
spoon shaped nails (koilonychia)
atrophy of the papillae of the tongue
angular stomatitis
brittle hair
dysphagia and glossitis (plummer Vinson or Paterson Brown
Kelly syndrome)parotid gland enlargement, splenomegaly and failure to grow
-
8/3/2019 16017942-Anaemia
13/83
-
8/3/2019 16017942-Anaemia
14/83
-
8/3/2019 16017942-Anaemia
15/83
investigations:
the red cells are microcytic (MCV < 80 fL) and hypochromic(MCV < 27 pg)
poikilocytosis (variation in shape) and anisocytosis (variation insize)
target cells
hypersegmentation of polymorphs
serum iron falls
iron blinding capacity
bone marrow erythroid hyperplasia with ragged normoblasts
ring sideroblast
other investigations:
the G.I. tract - endoscopy
-
8/3/2019 16017942-Anaemia
16/83
-
8/3/2019 16017942-Anaemia
17/83
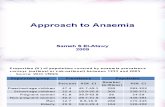
Bone marrow in iron deficiency
-
8/3/2019 16017942-Anaemia
18/83
1.sideroblastic anaemiaClassification:
A. Congenital:
X linked disease transmitted by females
B. Acquired:
primary or idiopathic
secondary: drugs
alcohol
lead
myeloproliferative disorders leukaemias
secondary carcinoma
other systemic disorders (connective tissuedisease)
-
8/3/2019 16017942-Anaemia
19/83
1.thalassaemia
Deficiency in the synthesis of the globin chains of haemoglobin
in addition, the accumulation of abnormal chains within the redcell leads to its early destruction.
The severity of the thalassaemia will depend on the amount othe haemoglobin A2 and F present.
Clinically -thalassaemia can be divided into:
thalassaemia mayor, with severe anaemia
intermedia, with moderate anaemia rarely requiring
transfusion
minor, the symptomless heterozygous carrier state
-
8/3/2019 16017942-Anaemia
20/83
-
8/3/2019 16017942-Anaemia
21/83
-
8/3/2019 16017942-Anaemia
22/83
symptoms:
failure to thrive
intermittent infection
severe anaemia
extramedullary haemopoiesis hepatosplenomegaly and boneexpansion thalassaemic facies
-
8/3/2019 16017942-Anaemia
23/83
-
8/3/2019 16017942-Anaemia
24/83
investigation:
blood count:
moderate to severe anaemia (MCV, MCH)
reticulocyte
white cells and platelets = N
blood film:
hypochromic and microcytic picture
Howell Jolly bodieshigh ferritin levels
haemoglobin electrophoresis (HbF ; HbA absent)
-
8/3/2019 16017942-Anaemia
25/83
-Thalassaemia trait (minor)
asymptomatic
no anaemia, red cells hypochromic and microcytic
-Thalassaemia
two main form:
deletion of only alpha chain gene
deletion of both alpha chain genes no alpha chains are
produced
-
8/3/2019 16017942-Anaemia
26/83
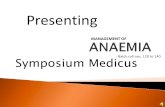
Thalassemia major
Thalassemia minor
-
8/3/2019 16017942-Anaemia
27/83
Macrocytic anaemia
The presence in the bone marrow of erytroblasts with delayednuclear maturation because of defective DNA synthesis(megaloblasts).
Occurs in:
vitamin B12 deficiency
folic acid deficiencydiseritropoetic anaemia
Haematological values:
anaemia
MCV > 96 fL
blood film (peripheral): macrocytes and hypersegmentedpolymorphs
neutropenia
thrombocytopenia
-
8/3/2019 16017942-Anaemia
28/83
vitamin b12 (Addison Biermer anaemia)
average daily diet 5 30 g B12
average adult stores 1000 g liver
absorption and transport:
gut binder complex (R binder + B12) intrinsec
factor (glycoprotein from the gastric juice)
Transcobalamin
Ileum Marrow
-
8/3/2019 16017942-Anaemia
29/83
Pernicious anaemia (Addison Biermer) affect:
particularly nordic people: fair haired; blue eyed.
association with other autoimmune diseases: thyroid disease,
Addisons disease, vitiligo
higher incidence of gastric carcinoma
-
8/3/2019 16017942-Anaemia
30/83
Causes of vitamin b12 deficiency: low dietary intake (vegans) impaired absorption:
A. stomach (gastrectomy)B. small bowel: coeliac disease tropical sprue bacterial overgrowth
ileal disease or resectionC. pancreas:
chronic pancreatic disease Zollinger Ellison syndrome
D. miscellaneous and rare:
fish tape worm (diphyllobothrium latum) congenital deficiency:
intrinsec factor transcobalamin III
nitrous oxide (inactivates B12)
-
8/3/2019 16017942-Anaemia
31/83
Clinical features:
2. Anaemic syndrome
3. Neurological syndromes:
Peripheral neuropathy progressively involving theposterior and lateral columns of the spinal cord:
symmetrical paraesthesia in the fingers and toes
loss of vibration sense and proprioception progressive weakness and ataxia
paraplegia
Mental changes:
somnolence
irritability
psychosis
dementia
-
8/3/2019 16017942-Anaemia
32/83
1. Digestive syndrome:
glossitis (red sore tongue)
angular stomatitis
hepatosplenomegaly
gastric atrophy and achlorhydria
2. Others:
skin lemon-yellow tint due to hyperbilirubinaemia
heart failure
fever
-
8/3/2019 16017942-Anaemia
33/83
-
8/3/2019 16017942-Anaemia
34/83
Investigations:
peripheral blood film shows features of megaloblastic
anaemia: reticulocytes
the serum bilirubin
bone marrow megaloblastic erythropoiesis
the Schilling test (a radioactive dose of B12 is given orally
and the total body activity is measured)
G.I. investigations endoscopy
-
8/3/2019 16017942-Anaemia
35/83
-
8/3/2019 16017942-Anaemia
36/83
Bone marrow
pernicious anaemia
-
8/3/2019 16017942-Anaemia
37/83
Folic acid
Daily requirement 100 g
Causes of folate deficiency:
poor intake:
old age
poor social conditions
starvation
alcohol excess
poor intake due to anorexia:
G.I. disease (partial gastrectomy, coeliac disease, Crohns
disease, cancer)
excess utilization
-
8/3/2019 16017942-Anaemia
38/83
clinical features:
B. Physiological:
pregnancy lactation
prematurity
C. Pathological:
haemolysis
malignant disease
inflammatory disease
metabolic disease
haemolysis
malabsorption
antifolate drugs
-
8/3/2019 16017942-Anaemia
39/83
Normocytic anaemia
1. Acute blood loss
2. Aplastic anaemia
3. Anaemia of chronic disease
4. Haemolytic anaemia
-
8/3/2019 16017942-Anaemia
40/83
1.Acute blood loss
Stage I:
Hb, Ht, Rc, N or
white cells
platelets
Stage II (2 4 days):
Hb, Ht, Rc
reticulocytosis
white cells platelets
Stage III (2 3 weeks):
Hb, Ht, Rc
Wc N
Platelets
-
8/3/2019 16017942-Anaemia
41/83
1.Aplastic anaemia
Aplasia of the bone marrow with peripheral blood pancytopenia.
Causes:
congenital: Fanconis anaemia
acquired:
chemicals, drugs, insecticides
ionizing radiation
infections: viral hepatitis measles
miscellaneous infection: tuberculosis tyhmona
pregnancy
unknown
-
8/3/2019 16017942-Anaemia
42/83
clinical features:
anaemia
bleeding (ecchymoses, bleeding gums and epistaxis)
infection (fungal infections)
investigations:
elevated serum iron
low haemoglobin
white cell
count 500 / mmc
platelet 20,000 / mmc
reticulocytes virtual absent
hypocellular or aplastic bone marrow
-
8/3/2019 16017942-Anaemia
43/83
1.Haemolytic anaemia
The red cells normally survives about 120 days, but inhaemolysis the cell survival times are considerably shortened.
Causes of haemolytic anaemia:
D. Inherited:
1. red cell membrane defect:
hereditary spherocytosis hereditary eliptocytosis
2. haemoglobin abnormalities:
thalassaemia
sickle cell disease
3. metabolic defects:
glucose 6 phosphate dehydrogenize deficiency
pyruvate kinase deficiency
-
8/3/2019 16017942-Anaemia
44/83
(Causes of haemolytic anaemia)
B. Acquired:
1. immune:
autoimmune
isoimmune (Rh or ABO incompatibility)
2. non-immune:
membrane defects: paroxysmal nocturnalhaemoglobinuria, liver disease, renal disease
mechanical: damaged vessels, valve prosthesis, marchhaemoglobinuria
3. miscellaneous:
infections
drugs and chemicals
hypersplenism
-
8/3/2019 16017942-Anaemia
45/83
site of haemolysis:
3. Intravascular red cells are rapidly destroyed within the
circulation, haemoglobin is liberated;
4. Extravascular red cells are removed from the circulation by
macrophages in the reticuloendothelial system (liver and
spleen)
evidence for haemolysis
-
8/3/2019 16017942-Anaemia
46/83
evidence for haemolysis:
Increased red cell breakdown leads to:
iron stercobilinogen
elevated serum bilirubin (unconjugated)
excess urinary urobilinogen
reduced plasma haptoglobin
abnormal red cell fragments in peripheral blood
Increased red cell production leads to:
reticulocytosis
erythroid hyperplasia of the bone marrow
li i l fi di
-
8/3/2019 16017942-Anaemia
47/83
clinical findings:
skin jaundice
splenomegaly
abdominal pain (infarction or acute sequestration as in sicklesyndromes)
gall stones
growth impaired (e.g. spherocytosis) ulcers on the leg
dark urine (in haemolytic crises)
black in pmn
septic necrosis of the bone (sickle sdr.)
papillary necrosis affecting the kidney haematuria (S.S.)
painful priaprism
cerebral damage
-
8/3/2019 16017942-Anaemia
48/83
-
8/3/2019 16017942-Anaemia
49/83
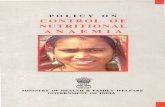
Peripherical blood in
hemolytic anaemia
-
8/3/2019 16017942-Anaemia
50/83
-
8/3/2019 16017942-Anaemia
51/83
Polycythaemia
Is defined as a haemoglobin level greater than 18 g/dL, a red
cell count above 6x1012/L. The red cell volume is greater than
36 mL/kg in males and 32 mL/kg in females.
Causes of polycythaemiaPrimary:
Polycythaemia vera
Secondary:
-
8/3/2019 16017942-Anaemia
52/83
Secondary:
A. due to an appropriate increase in erythropoetin:
high altitude
lung disease cardiovascular disease (right left shunt)
heavy smoking
B. due to an inappropriate increase in erithropoetin:
renal disease, carcinoma, Wilms tumor hepatocellular carcinoma
adrenal tumors
cerebellar haemangioblastoma
massive uterine fibromaRelative:
stress or spurious polycythaemia
dehydration
burns
Policitemia era
-
8/3/2019 16017942-Anaemia
53/83
Policitemia veraCaused by chronic sustained proliferation of the erithroid
population of the bone marrow.
red cell volume
blood viscosity
compensated by an
increase plasmavolume and
cardiac output
Ht
myocardial infarctionstroke
-
8/3/2019 16017942-Anaemia
54/83
clinical findings:
tiredness
depression
vertigo
tinitus and visual disturbance
hypertension
angina
intermitent claudication
tendency to bleed itching after bath
peptic ulcerations
-
8/3/2019 16017942-Anaemia
55/83
investigations:
Hb, Ht, WBC, platelets
erythroid hyperplasia and abnormal megakaryocytes in bonemarrow
red cell volume
serum uric acid levels
leucocyte alkaline phosphatase (LAP)
vitamin B12 binding protein is
h hi ll
-
8/3/2019 16017942-Anaemia
56/83
The white cell
The five types of leucocytes found in peripheral blood are:
polymorphonuclear leucocytes (neutrophil leucocytes)
eosinophil leucocytes
basophil granulocytes
lymphocytes
monocytes
Polymorphonuclear leucocytes originate in the bone marrow and
are carried to tissues via the blood, where they are involved in
immune defense and may continue to circulate between the
lymphatic tissue and blood stream.
-
8/3/2019 16017942-Anaemia
57/83
neutrophilis
The neutrophil granulocyte originates in the bone marrow asmyeloblast promyelocyte myelocyte (stored up to 10 days)
Function
ingest and kill bacteria
accumulation of degenerate neutrophils gives rise to pus
Neutrophil luecocytosis
rise in the number of neutrophils to > 10x105/l in bacterialinfection or tissue damage
exercise
corticosteroid administration
-
8/3/2019 16017942-Anaemia
58/83
Neutrophil leucocytosis
leukaemia
myeloproliferative disease
leukaemoid reaction
leucoerytroblastic anaemia
the leucocytosis may be accompanied by a pyrexia due to
the production of a leucocyte pyrogen
a leukaemoid reaction (the overproduction of white cells,
many of them primitive) may occur in - severe infections
- tuberculosis
-malignant infiltration
t hili
-
8/3/2019 16017942-Anaemia
59/83
neutrophilis
Neutropenia and agranulocytosis
defined as a circulatory neutrophil count below 1,5x10
9
/l the absence of heutrophilis is called agranulocytosis
causes of neutropenia
rasial (neutropenia is common in black rases)
viral infection
severe bacterial infection (typhoid)
Feltys syndrome
megaloblastic anaemia
drugs
pancytopenia from any cause
-
8/3/2019 16017942-Anaemia
60/83
Clinical features:
infections
glazed mucositis occurs in the mouth and ulceeration is
common
septicaemia
investigation
blood film shows neutropenia
bone marrow absence of cells from the neutrophil
granulocyte series
eosinophils
-
8/3/2019 16017942-Anaemia
61/83
Occur when the number of eosinophils is > 1x109/l
causes of eosinophils Parasitic infestation ascaris
strongyloides
Allergic disorders
hayfever (allergic rhinitis)
other hypersensitivity reactions, including drug reactions
Skin disorders
urticaria
eczema
pemphigus
Pulmonary disorders
-
8/3/2019 16017942-Anaemia
62/83
y
bronchial asthma
tropical pulmonary eosinophilia
allergic bronchopulmonary aspergillosis polyarteritis nodosa (Churg Strauss syndrome)
Malignant disorders
lymphoma
carcinoma
melanoma
eosinophilic leukemia
Miscellaneous sarcoidosis
hypoadrenalism
eosinophilic gastroenteritis
hypereosinophilic syndrome
l h
-
8/3/2019 16017942-Anaemia
63/83
lymphocytes
Form nearly the circulating white cells
Originate in the lymph glands, spleen, Peyers patches, bonemarrow, thymus
2 types:
thymus dependent or T lymphocytes concerned with
cellular immunity bursa dependent or B lymphocytes concerned with
humoral immunity
Lymphocytosis occurs in:
viral infections: Epstein Barr, cytomegalvirus
chronic infections: syphilis, tuberculosis
acute viral infections: pertussis, brucellosis
The leukaemias
-
8/3/2019 16017942-Anaemia
64/83
The leukaemias
Characterized by the proliferation of a single malignantly
transformed progenitor cell in the haemopoietic system.
clasification
There are TWO MAJOR of acute leukemia:F. Acute lymphoblastic leukaemia
G. Acute non-lymphocytic leukaemia (called also acutemyelogenous leukaemia)
The CHRONIC FORMS of these conditions are:
Chronic granulocytic leukaemia
Chronic lymphatic leukaemia
-
8/3/2019 16017942-Anaemia
65/83
incidence
the commonest childhood leukaemia is acute lymphoblastic in
type (80%) adults B and in elderly chronic forms
aetiology
remains unknown
Genetic factors:
are important: low frequency of all in black children
a high incidence of leukaemia in the identical twin
risk of developing acute leukaemia in children with Downssyndrome (who have chromosomal abnormalities)
-
8/3/2019 16017942-Anaemia
66/83
Enviromental factors:
radiation (in survivors of the atomic bomb of Hiroshima)
chemicals
drugs and chemotherapeutic agents viruses (human leukaemia virus type I) which was first
discovered in Japanese with T cell leukaemia andhypercalcaemia
-
8/3/2019 16017942-Anaemia
67/83
Acute leukaemia
Cellular types
3. Acute lymphoblastic leukaemia
blast cells involved may vary
histologically: L1, L2 and L3 types
the phenotypic markers have proved to be of considerable
importance assessing the likelihood importance of
response and the long-term outlook4. Acute non-lymphocytic leukaemia
classification predominant myeloblasts distinctAcute myelocytic
-
8/3/2019 16017942-Anaemia
68/83
bizzare, multinucleated megaloblastederythroblasts predominate
myeloblasts also present
ErytroleukaemiaM6
completely with differentiation undifferentiated blast cells
Acute monoblasticleukaemiaM5
A
promonocytes predominant with
differentiation
Acute monocytic
leukaemiaM5
myelocytic and monocytic maturationevident may be peripheral auer rods rare
Acutemyelomonocytic
leukaemiaM4
promyelocytes predominatehipergranular
auer rods rare
Acutepromyelocytic
leukaemia
M3
myeloblasts and promyelocytespredominant further maturation abnormal auer rods many
Acute myelocyticLeukaemia withDifferentiation
M2
predominant myeloblasts, distinctnucleoli few granules Auer rods rare
Acute myelocyticleukaemia without
differentiation
M1
Acute leukaemia
-
8/3/2019 16017942-Anaemia
69/83
clinical features
Hystory short symptoms of anaemia and maladive
acute infections such as mouth ulceration, sore throat,
pneumonia, perianal and skin infections
painful and enlarging lymphadenopathy
bruising and bleeding
bone pain (particularly common in children with all)
symptoms due to infiltration of tissues with leukaemic blast
cells, marked gum hypertrophy
headache, nausea, vomiting and blurred vision (raised
intracranial pressure)
Signs
-
8/3/2019 16017942-Anaemia
70/83
Signs
These may be relatively few, but commonly they are:
pallor
bruising, petechial haemorrages, bleeding gums and gum
hypertrophy
lymphadenopathy
splenomegaly and hepatomegaly
haemorrhages in the optic fundi with characteristic central
white deposit in the middle of the fundal haemorrhage
leukaemic retinopathy
meningeal leukaemia
boys hard enlarged testicles (infiltrated with leukaemic
tissue)
investigation
-
8/3/2019 16017942-Anaemia
71/83
investigation2. Peripheral blood film and bone marrow
normochromic and normocytic anaemia
the white cell count may be normal or raised; rarely a fewblast cells may be seen in the peripheral blood, or none atall
the platelet count is usually reduced
hypercellular bone marrow with characteristic blasts in thetrail of the fragments on the microscope slide
3. The CSF should be examined will contain blasts cells ifmeningeal leukaemia is present
4. Test of renal function
5. Serum uric acid6. Serum calcium
7. Serum electrolytes (potassium)
8. Blood cultures
9. Chest X ray (to determine the presence of a mediastinal mass)
-
8/3/2019 16017942-Anaemia
72/83
Gum-hypertrophy ALL
-
8/3/2019 16017942-Anaemia
73/83
Blasts-and-Auer-body
-
8/3/2019 16017942-Anaemia
74/83
ALL
ALL Blast
-
8/3/2019 16017942-Anaemia
75/83
ALL-L1-Marrow
Chronic granulocytic leukaemia
-
8/3/2019 16017942-Anaemia
76/83
g y
occurs in middle-aged and elderly people
it occurs in the myeloproliferative syndromes, which include:polycythaemia vera, myelofibrosis, essential trombocytosis
it is characterised by the presence of Philadelphiachromosome
Clinical features often of insidious onset (may only be discovered on a routine
blood count)
anaemia
bruising and bleeding manifestations
pain or discomfort due to a very large spleen gastrointestinal disturbance
sweating, fever and loss of weight as the result of a highmetabolic rate
-
8/3/2019 16017942-Anaemia
77/83
Phisical signs anaemia
lymphadenopathy (uncommon)
a large spleen (common) haemorrhage and thrombosis; bruising, bleeding, priapism
may occur
gout
Investigations
-
8/3/2019 16017942-Anaemia
78/83
g
normal Hb (initially), than a normocytic, normochromic
anaemia
white cell count is greater than 100 000 /mmc (100 000 500000 /mmc)
blood film: abundance of neutrophils, mielocytes and even a
few blast cell are presentplatelets count: N or
bone marrow: hypercellular marrow with the granulocyteprecursors markedly increased
a chromosome preparation shows the Philadelphiachromosome
the leucyte alkaline phosphatase (lap) is very low
levels of serum vit. B12 and B12 binding proteins are elevated
-
8/3/2019 16017942-Anaemia
79/83
-
8/3/2019 16017942-Anaemia
80/83
-
8/3/2019 16017942-Anaemia
81/83
Chronic lymphatic leukaemia
-
8/3/2019 16017942-Anaemia
82/83
y p
disease of late middle-aged and elderly people
disorder of B cells, with accumulation of mature lymphocytesin the tissues and peripheral blood
few cases the lymphocytes are T cells and skin involvement
can occur (mycosis fungoides, the Szary syndrome,
peripheral T cell lymphoma)
clinical features
the onset is insidous
lethargy
fever and sweating
loss of weight
signs
-
8/3/2019 16017942-Anaemia
83/83
signs
moderate enlargement of lymph nodes in the neck, axilla and
groin
splenic and hepatic enlargement, but not usually massive
investigations mild anaemia, normochromic, normocytic
white cell count > 15x109 &l, which more than 40%
lymphocytes
platelet count is usually normal as the disease progresses,
anaemia may become severe due to Coombs positive
haemolysis and the number of lymphocytes