HARDWARE OPAL-RT MARC PASTOR Real-Time 2009 Montreal, Quebec, Canada.

José M. Miró,1 Miguel Montejo,2 Lluis Castells,3 Juan C. Meneu,4 Antonio Rafecas,5 Marino Blanes,6 Jesús Fortún,7 Gloria de la Rosa,8 Iñaki Pérez,1Antonio Rimola,1 and the Spanish OLT in HIV-Infected Patients Working
Group.1Hosp. Clínic-IDIBAPS. Univ. of Barcelona, Barcelona; 2Hosp. Cruces, Bilbao; 3Hosp. Univ. Vall d’Hebrón, Barcelona;
4Hosp. Univ. 12 de Octubre, Madrid; 5Hosp Bellvitge-IDIBELL, Barcelona; 6Hosp. La Fe, Valencia; 7Hosp. Ramón y Cajal, Madrid; 8Organización Nacional de Trasplante (ONT), Madrid, Spain.
José M. Miró,1 Miguel Montejo,2 Lluis Castells,3 Juan C. Meneu,4 Antonio Rafecas,5 Marino Blanes,6 Jesús Fortún,7 Gloria de la Rosa,8 Iñaki Pérez,1Antonio Rimola,1 and the Spanish OLT in HIV-Infected Patients Working
Group.1Hosp. Clínic-IDIBAPS. Univ. of Barcelona, Barcelona; 2Hosp. Cruces, Bilbao; 3Hosp. Univ. Vall d’Hebrón, Barcelona;
4Hosp. Univ. 12 de Octubre, Madrid; 5Hosp Bellvitge-IDIBELL, Barcelona; 6Hosp. La Fe, Valencia; 7Hosp. Ramón y Cajal, Madrid; 8Organización Nacional de Trasplante (ONT), Madrid, Spain.
Poster H-124: 5-year Survival of HCV-HIV Coinfected Liver Transplant Recipients
(OLT): A Case-Control Study
16th CROI 2009, Montreal (Canada) - 200916th CROI 2009, Montreal (Canada) - 2009
E-mail address: [email protected] address: [email protected]
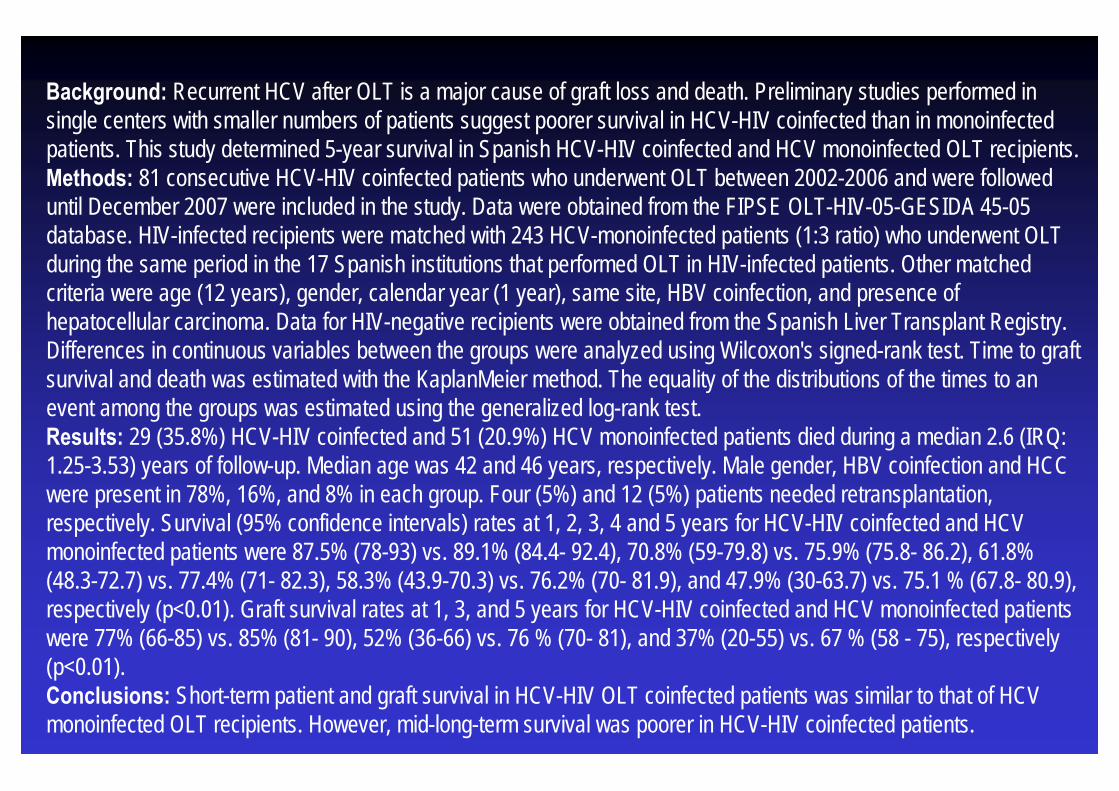
Background: Recurrent HCV after OLT is a major cause of graft loss and death. Preliminary studies performed in single centers with smaller numbers of patients suggest poorer survival in HCV-HIV coinfected than in monoinfectedpatients. This study determined 5-year survival in Spanish HCV-HIV coinfected and HCV monoinfected OLT recipients. Methods: 81 consecutive HCV-HIV coinfected patients who underwent OLT between 2002-2006 and were followed until December 2007 were included in the study. Data were obtained from the FIPSE OLT-HIV-05-GESIDA 45-05 database. HIV-infected recipients were matched with 243 HCV-monoinfected patients (1:3 ratio) who underwent OLT during the same period in the 17 Spanish institutions that performed OLT in HIV-infected patients. Other matched criteria were age (12 years), gender, calendar year (1 year), same site, HBV coinfection, and presence of hepatocellular carcinoma. Data for HIV-negative recipients were obtained from the Spanish Liver Transplant Registry. Differences in continuous variables between the groups were analyzed using Wilcoxon's signed-rank test. Time to graft survival and death was estimated with the KaplanMeier method. The equality of the distributions of the times to an event among the groups was estimated using the generalized log-rank test. Results: 29 (35.8%) HCV-HIV coinfected and 51 (20.9%) HCV monoinfected patients died during a median 2.6 (IRQ: 1.25-3.53) years of follow-up. Median age was 42 and 46 years, respectively. Male gender, HBV coinfection and HCC were present in 78%, 16%, and 8% in each group. Four (5%) and 12 (5%) patients needed retransplantation, respectively. Survival (95% confidence intervals) rates at 1, 2, 3, 4 and 5 years for HCV-HIV coinfected and HCV monoinfected patients were 87.5% (78-93) vs. 89.1% (84.4- 92.4), 70.8% (59-79.8) vs. 75.9% (75.8- 86.2), 61.8% (48.3-72.7) vs. 77.4% (71- 82.3), 58.3% (43.9-70.3) vs. 76.2% (70- 81.9), and 47.9% (30-63.7) vs. 75.1 % (67.8- 80.9), respectively (p<0.01). Graft survival rates at 1, 3, and 5 years for HCV-HIV coinfected and HCV monoinfected patients were 77% (66-85) vs. 85% (81- 90), 52% (36-66) vs. 76 % (70- 81), and 37% (20-55) vs. 67 % (58 - 75), respectively (p<0.01). Conclusions: Short-term patient and graft survival in HCV-HIV OLT coinfected patients was similar to that of HCV monoinfected OLT recipients. However, mid-long-term survival was poorer in HCV-HIV coinfected patients.
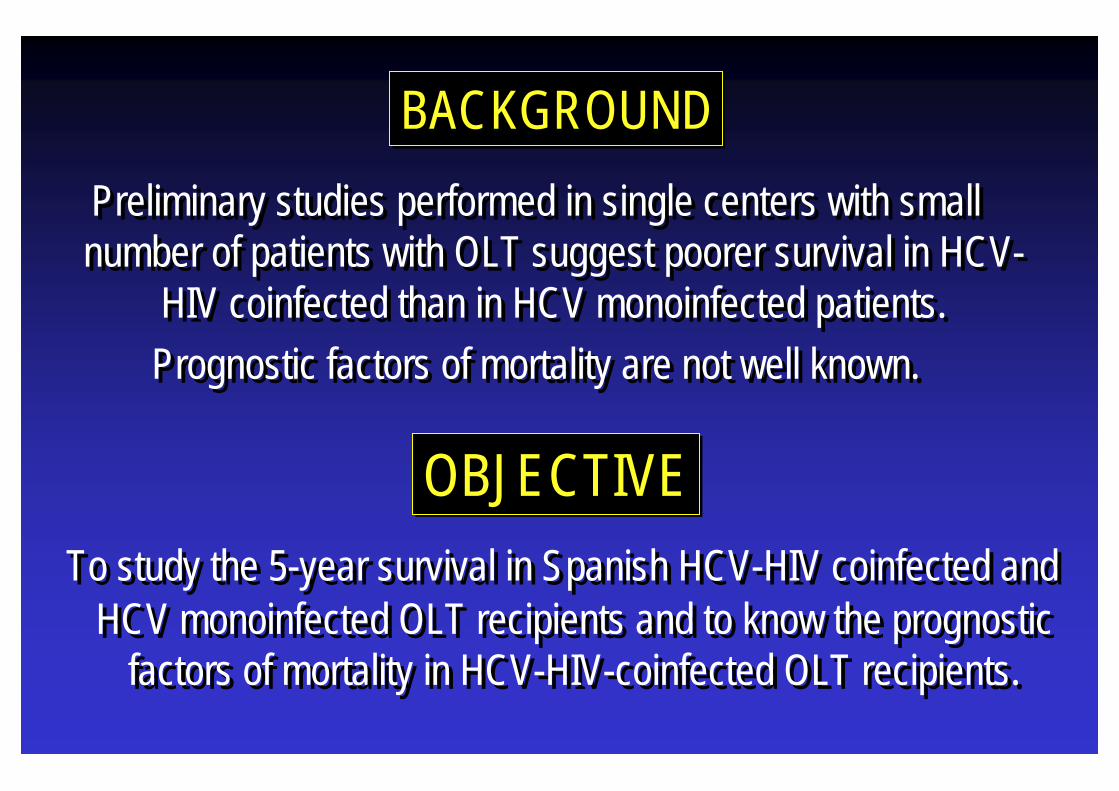
Preliminary studies performed in single centers with small number of patients with OLT suggest poorer survival in HCV-
HIV coinfected than in HCV monoinfected patients. Prognostic factors of mortality are not well known.
Preliminary studies performed in single centers with small number of patients with OLT suggest poorer survival in HCV-
HIV coinfected than in HCV monoinfected patients. Prognostic factors of mortality are not well known.
To study the 5-year survival in Spanish HCV-HIV coinfected and HCV monoinfected OLT recipients and to know the prognostic
factors of mortality in HCV-HIV-coinfected OLT recipients.
To study the 5-year survival in Spanish HCV-HIV coinfected and HCV monoinfected OLT recipients and to know the prognostic
factors of mortality in HCV-HIV-coinfected OLT recipients.
OBJECTIVEOBJECTIVE
BACKGROUNDBACKGROUND

• Prospective study of the first 84 HCV/HIV-1-infected patients who underwent OLT in Spain (2002-06).
• Variables analyzed: - Pre-OLT recipient variables: HIV (stage, CD4 cell count,
plasma HIV-1 RNA viral load, cART regimens) & liver disease(MELD, Child, plasma HCV RNA viral load)
- Donor and operative variables- Post-OLT variables: immunosuppression, rejection, infection,
toxicity & the same HIV variables described above).• HIV-infected recipients were administered the same
immunosuppression & prophylaxis as HIV-negative patients.
• Prospective study of the first 84 HCV/HIV-1-infected patients who underwent OLT in Spain (2002-06).
• Variables analyzed: - Pre-OLT recipient variables: HIV (stage, CD4 cell count,
plasma HIV-1 RNA viral load, cART regimens) & liver disease(MELD, Child, plasma HCV RNA viral load)
- Donor and operative variables- Post-OLT variables: immunosuppression, rejection, infection,
toxicity & the same HIV variables described above).• HIV-infected recipients were administered the same
immunosuppression & prophylaxis as HIV-negative patients.
PATIENTS & METHODSPATIENTS & METHODS

ACCEPTANCE CRITERIA FOR OLT*ACCEPTANCE CRITERIA FOR OLT*
* Miró JM et al. Enferm Infecc Microbiol Clin. 2005; 23:353-362.* Mir* Miróó JM et al. JM et al. EnfermEnferm InfeccInfecc MicrobiolMicrobiol ClinClin. 2005; 23:353. 2005; 23:353--362.362.
• Liver criteria: the same as for the non-HIV-infected population.
• HIV criteria:1) Clinical: no previous C events (CDC, 1993) except some OIs (TB, Can, PCP); and,2) Immunological: pre-OLT CD4 cell count >100 cells/mm3 for OLT; and, 3) Virological: RNA HIV-1 viral load BDL on cART or, if detectable,post-SOT suppression predicted.
• Drug abuse criteria: A) No heroin or cocaine abuse for >2 years; B) No alcohol abuse for >6 months.
• Liver criteria: the same as for the non-HIV-infected population.
• HIV criteria:1) Clinical: no previous C events (CDC, 1993) except some OIs (TB, Can, PCP); and,2) Immunological: pre-OLT CD4 cell count >100 cells/mm3 for OLT; and, 3) Virological: RNA HIV-1 viral load BDL on cART or, if detectable,post-SOT suppression predicted.
• Drug abuse criteria: A) No heroin or cocaine abuse for >2 years; B) No alcohol abuse for >6 months.
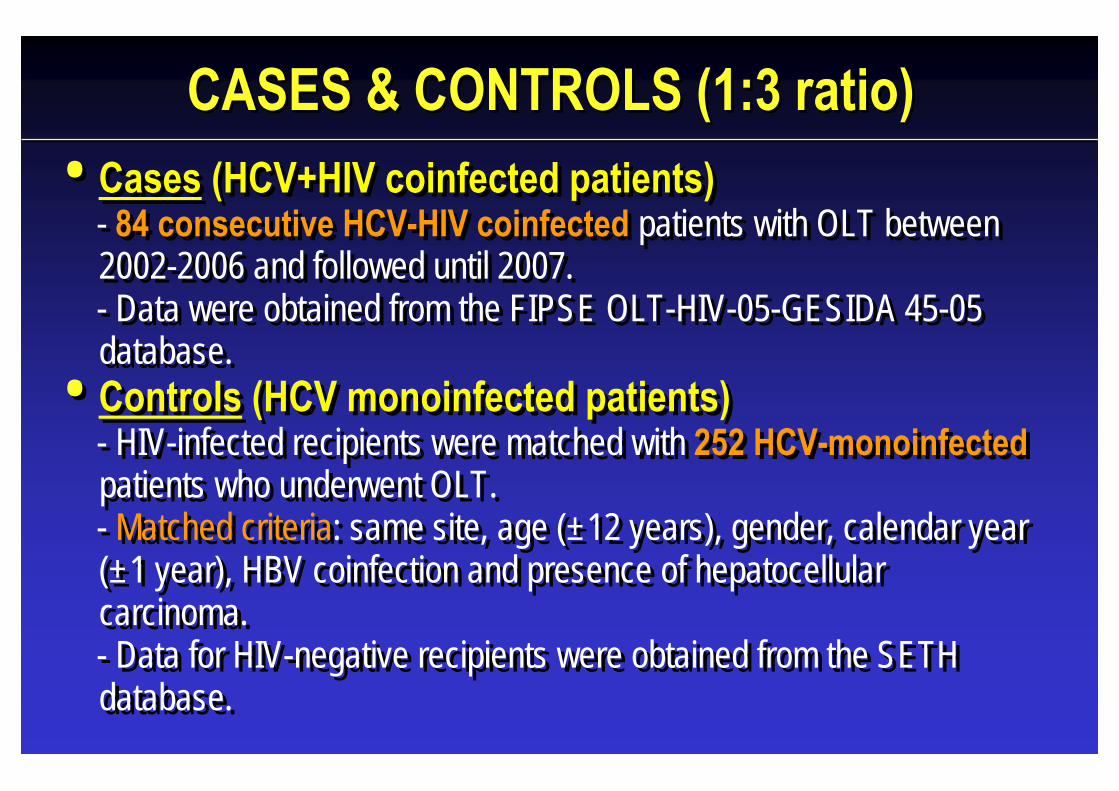
CASES & CONTROLS (1:3 ratio)CASES & CONTROLS (1:3 ratio)• Cases (HCV+HIV coinfected patients)
- 84 consecutive HCV-HIV coinfected patients with OLT between 2002-2006 and followed until 2007. - Data were obtained from the FIPSE OLT-HIV-05-GESIDA 45-05 database.
• Controls (HCV monoinfected patients)- HIV-infected recipients were matched with 252 HCV-monoinfectedpatients who underwent OLT.- Matched criteria: same site, age (±12 years), gender, calendar year (±1 year), HBV coinfection and presence of hepatocellularcarcinoma.- Data for HIV-negative recipients were obtained from the SETH database.
• Cases (HCV+HIV coinfected patients)- 84 consecutive HCV-HIV coinfected patients with OLT between 2002-2006 and followed until 2007. - Data were obtained from the FIPSE OLT-HIV-05-GESIDA 45-05 database.
• Controls (HCV monoinfected patients)- HIV-infected recipients were matched with 252 HCV-monoinfectedpatients who underwent OLT.- Matched criteria: same site, age (±12 years), gender, calendar year (±1 year), HBV coinfection and presence of hepatocellularcarcinoma.- Data for HIV-negative recipients were obtained from the SETH database.
• Continuous variables were assessed using the t test for normally distributed data or the Mann-Whitney U test otherwise, and the Fisher exact test for categorical data.
• The Cox model was used to analyze the time to death, and all covariates with a P<0.10 on univariate analysis were used to identify independent predictors of mortality.
• Patient survival analysis was performed using the Kaplan-Meier method and groups were compared using the log-rank test and Cox regression analysis.
• The analysis was performed using SAS version 9.1.3 software (SASInstitute, Cary, NC, USA) and the level of significance was established at 0.05 (two-sided).
• Continuous variables were assessed using the t test for normally distributed data or the Mann-Whitney U test otherwise, and the Fisher exact test for categorical data.
• The Cox model was used to analyze the time to death, and all covariates with a P<0.10 on univariate analysis were used to identify independent predictors of mortality.
• Patient survival analysis was performed using the Kaplan-Meier method and groups were compared using the log-rank test and Cox regression analysis.
• The analysis was performed using SAS version 9.1.3 software (SASInstitute, Cary, NC, USA) and the level of significance was established at 0.05 (two-sided).
STATISTICAL ANALYSISSTATISTICAL ANALYSIS
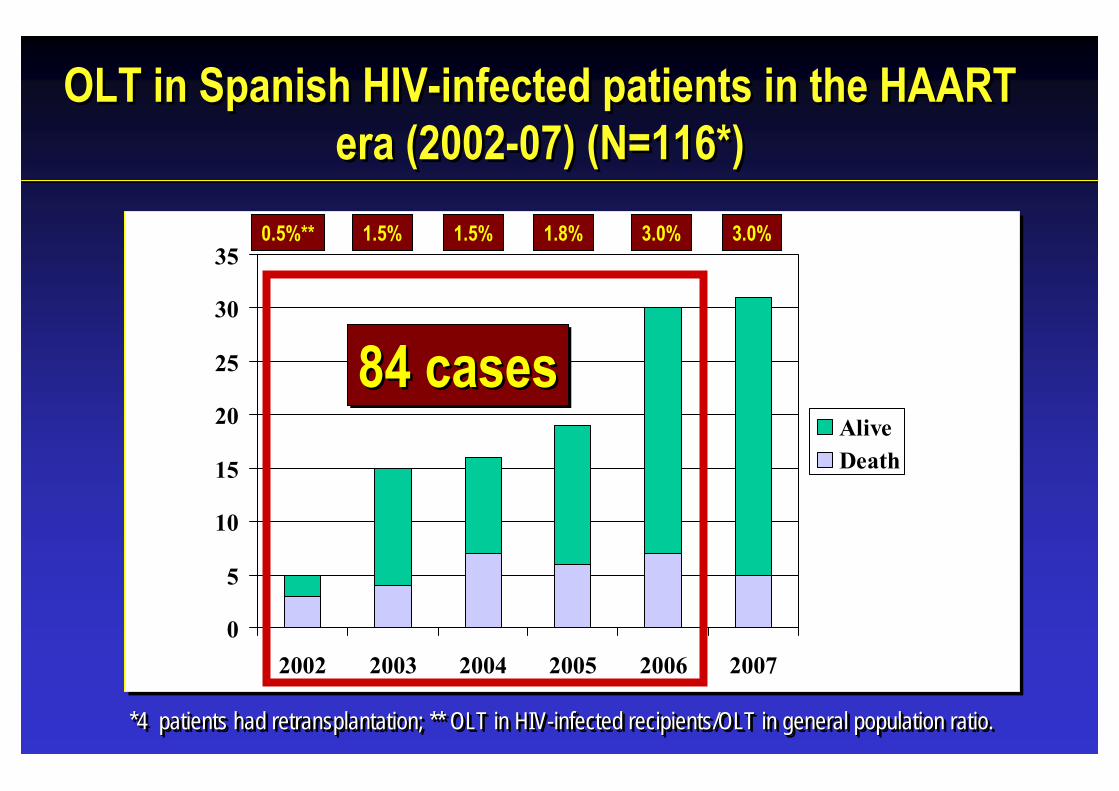
OLT in Spanish HIV-infected patients in the HAART era (2002-07) (N=116*)
OLT in Spanish HIV-infected patients in the HAART era (2002-07) (N=116*)
0
5
10
15
20
25
30
35
2002 2003 2004 2005 2006 2007
AliveDeath
*4 patients had retransplantation; ** OLT in HIV-infected recipients/OLT in general population ratio.*4 *4 patientspatients hadhad retransplantationretransplantation; ** OLT in HIV; ** OLT in HIV--infectedinfected recipientsrecipients/OLT in general /OLT in general populationpopulation ratio.ratio.
0.5%** 1.5% 1.8% 3.0% 3.0%1.5%
84 cases84 cases84 cases

Main Characteristics & OutcomeMain Characteristics & Outcome
Male genderAge (years)*HBV coinfectionHCC**Follow-up (yrs)*RetransplantationDeath
Male Male gendergenderAgeAge ((yearsyears)*)*HBV HBV coinfectioncoinfectionHCC**HCC**FollowFollow--up (up (yrsyrs)*)*RetransplantationRetransplantationDeathDeath
78%42
16%8%2.6
4 (5%)30 (36%)
78%78%4242
16%16%8%8%2.62.6
4 (4 (55%)%)30 (36%)30 (36%)
* Median; ** Hepatocellular carcinoma. * * MeMediandian; ** ; ** HepatocellularHepatocellular carcinoma. carcinoma.
78%46
16%8%1.9
12 (5%)50 (20%)
78%78%4646
16%16%8%8%1.91.9
12 (12 (55%)%)50 (20%)50 (20%)
HIV+HCVN=84
HIV+HCVN=84
HCVN=252
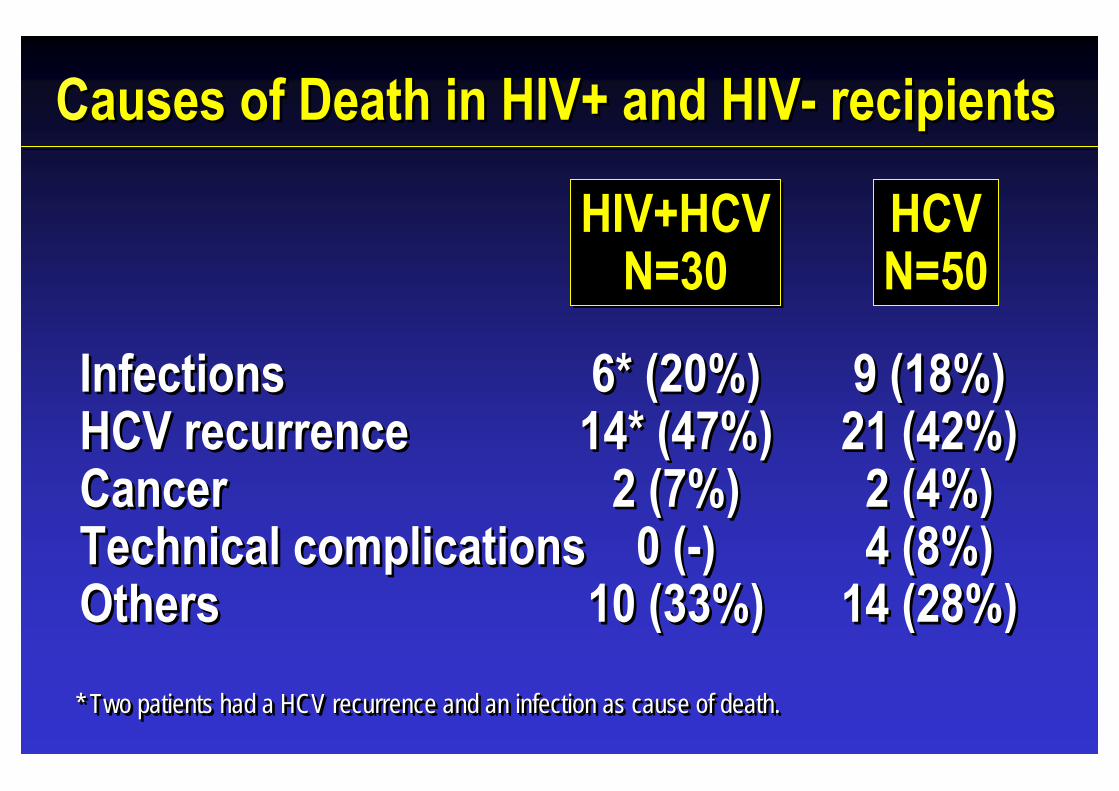
Causes of Death in HIV+ and HIV- recipientsCauses of Death in HIV+ and HIV- recipients
InfectionsHCV recurrenceCancerTechnical complicationsOthers
InfectionsInfectionsHCV HCV recurrencerecurrenceCancerCancerTechnical complicationsTechnical complicationsOthersOthers
6* (20%)14* (47%)
2 (7%)0 (-)
10 (33%)
6* (20%)6* (20%)14* (47%)14* (47%)
2 (7%)2 (7%)0 (0 (--))
10 (33%)10 (33%)
HIV+HCVN=30
HIV+HCVN=30
HCVN=50
9 (18%)21 (42%)2 (4%)4 (8%)
14 (28%)
9 (18%)9 (18%)21 (42%)21 (42%)2 (4%)2 (4%)4 (8%)4 (8%)
14 (28%)14 (28%)* Two patients had a HCV recurrence and an infection as cause of death. * Two patients had a HCV recurrence and an infection as cause of* Two patients had a HCV recurrence and an infection as cause of death. death.
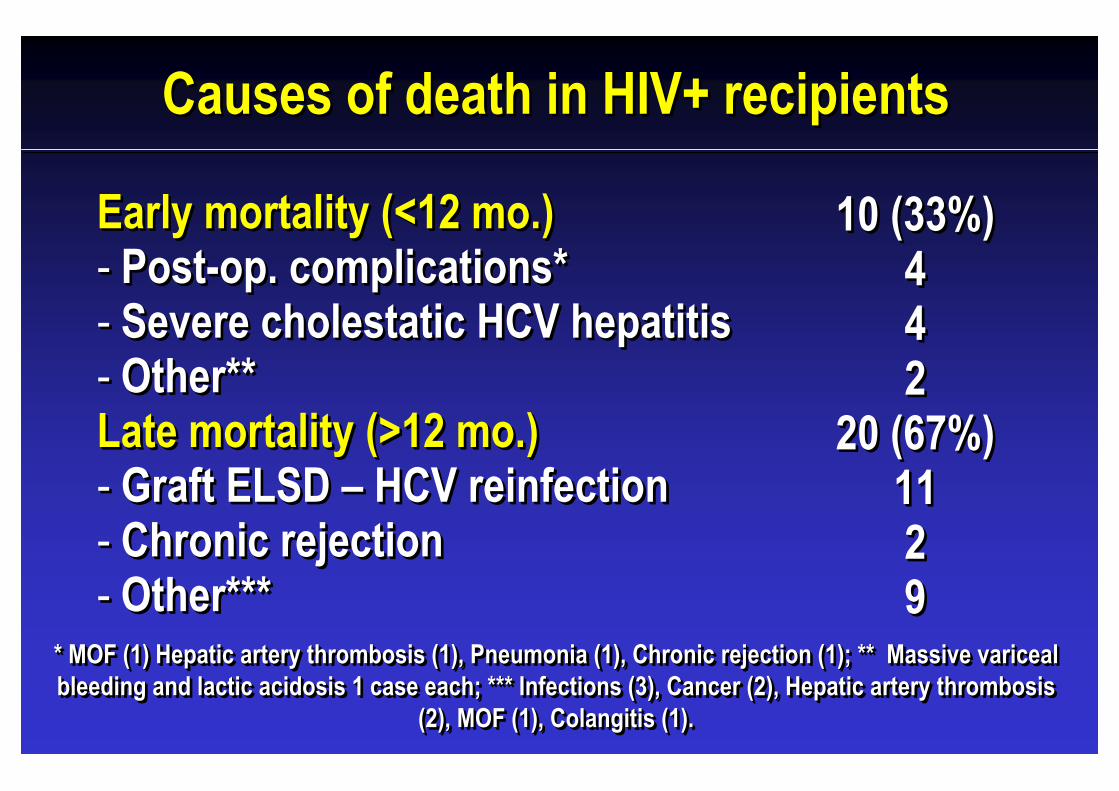
Early mortality (<12 mo.)- Post-op. complications* - Severe cholestatic HCV hepatitis- Other** Late mortality (>12 mo.)- Graft ELSD – HCV reinfection- Chronic rejection- Other***
EarlyEarly mortalitymortality (<12 (<12 momo.).)-- PostPost--op. complications* op. complications* -- Severe Severe cholestaticcholestatic HCV hepatitisHCV hepatitis-- OtherOther** ** Late mortality (>12 mo.)Late mortality (>12 mo.)-- Graft ELSD Graft ELSD –– HCV HCV reinfectionreinfection-- Chronic rejectionChronic rejection-- OtherOther******
10 (33%)442
20 (67%)1129
1010 (33%)(33%)444422
20 (67%)20 (67%)11112299
Causes of death in HIV+ recipientsCauses of death in HIV+ recipients
* MOF (1) Hepatic artery thrombosis (1), Pneumonia (1), Chronic rejection (1); ** Massive varicealbleeding and lactic acidosis 1 case each; *** Infections (3), Cancer (2), Hepatic artery thrombosis
(2), MOF (1), Colangitis (1).
* MOF (1) Hepatic artery thrombosis (1), Pneumonia (1), Chronic * MOF (1) Hepatic artery thrombosis (1), Pneumonia (1), Chronic rejection (1); ** Massive rejection (1); ** Massive varicealvaricealbleeding and lactic acidosis 1 case each; *** Infections (3), Cableeding and lactic acidosis 1 case each; *** Infections (3), Cancer (2), Hepatic artery thrombosis ncer (2), Hepatic artery thrombosis
(2), MOF (1), (2), MOF (1), ColangitisColangitis (1). (1).
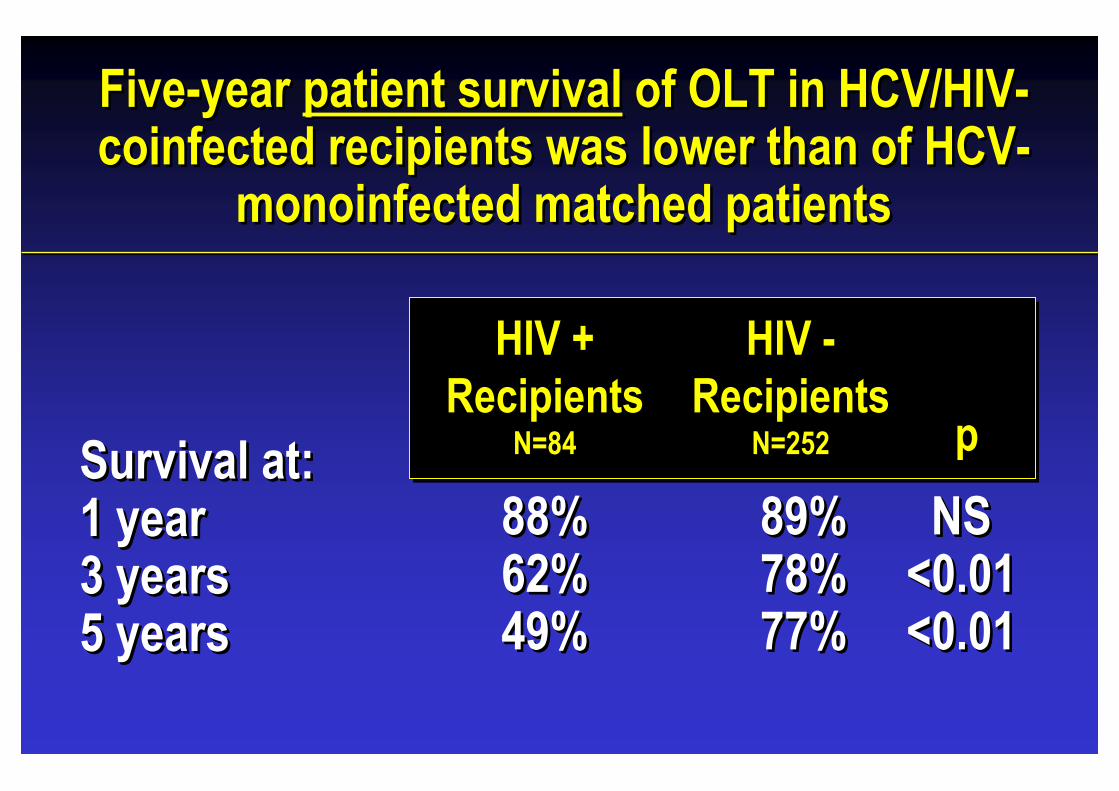
Five-year patient survival of OLT in HCV/HIV-coinfected recipients was lower than of HCV-
monoinfected matched patients
Five-year patient survival of OLT in HCV/HIV-coinfected recipients was lower than of HCV-
monoinfected matched patients
Survival at:1 year3 years5 years
SurvivalSurvival atat::1 1 yearyear3 3 yearsyears5 5 yearsyears
HIV +Recipients
N=84
HIV +HIV +RecipientsRecipients
N=84N=84
HIV -Recipients
N=252
HIV HIV --RecipientsRecipients
N=252N=252 ppp
88%62%49%
88%88%62%62%49%49%
89%78%77%
89%89%78%78%77%77%
NS<0.01<0.01
NSNS<0.01<0.01<0.01<0.01
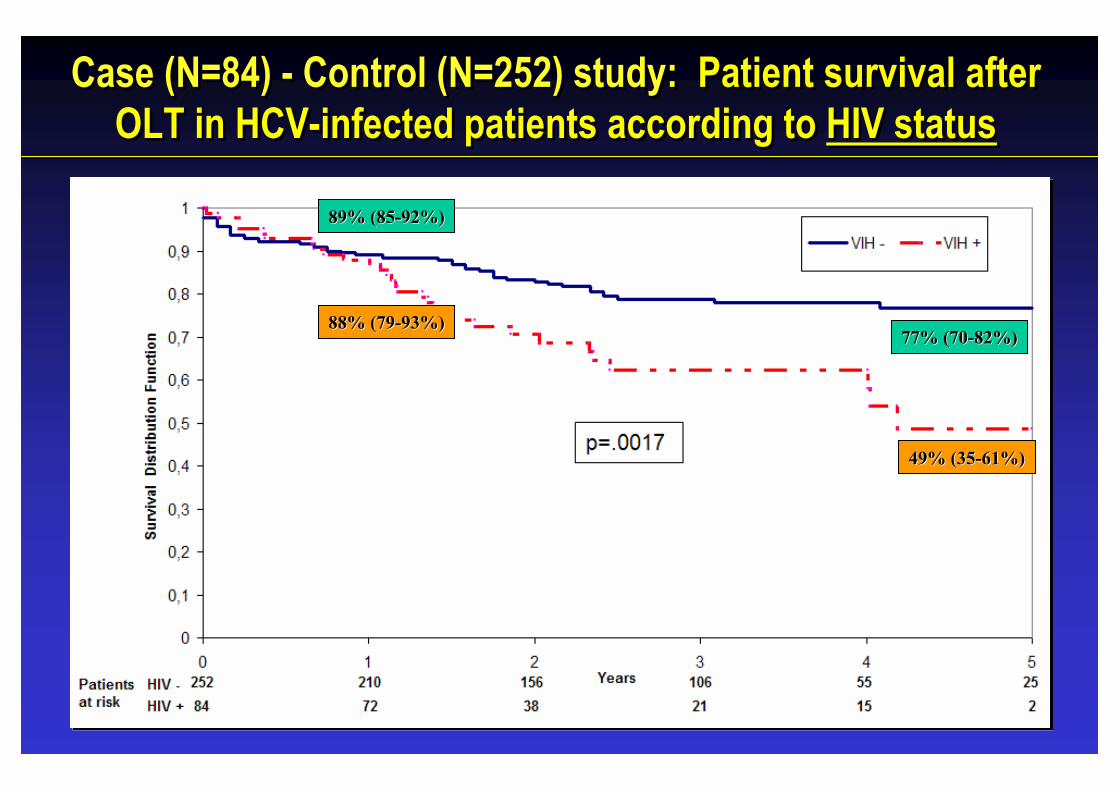
Case (N=84) - Control (N=252) study: Patient survival afterOLT in HCV-infected patients according to HIV status
Case (N=84) - Control (N=252) study: Patient survival afterOLT in HCV-infected patients according to HIV status
49% (3549% (35--61%)61%)
77% (7077% (70--82%)82%)
89% (8589% (85--92%)92%)
88% (7988% (79--93%)93%)
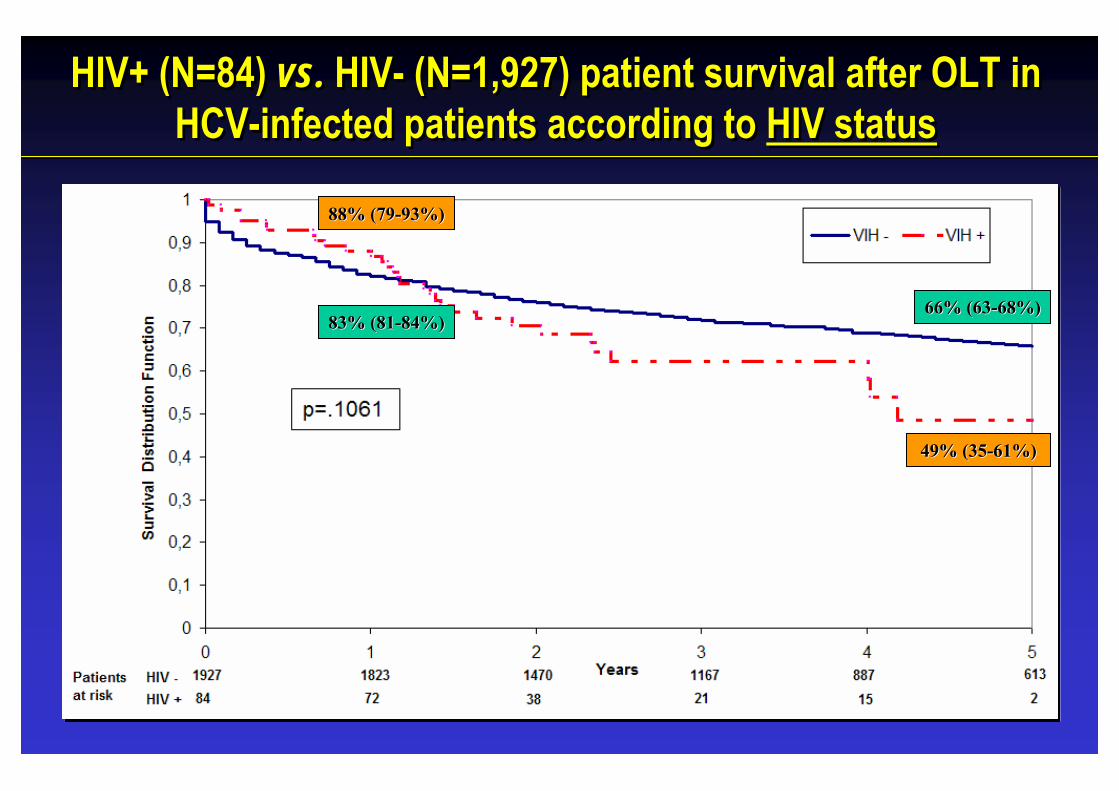
HIV+ (N=84) vs. HIV- (N=1,927) patient survival after OLT in HCV-infected patients according to HIV status
HIV+ (N=84) vs. HIV- (N=1,927) patient survival after OLT in HCV-infected patients according to HIV status
49% (3549% (35--61%)61%)
88% (7988% (79--93%)93%)
66% (6366% (63--68%)68%)83% (8183% (81--84%)84%)
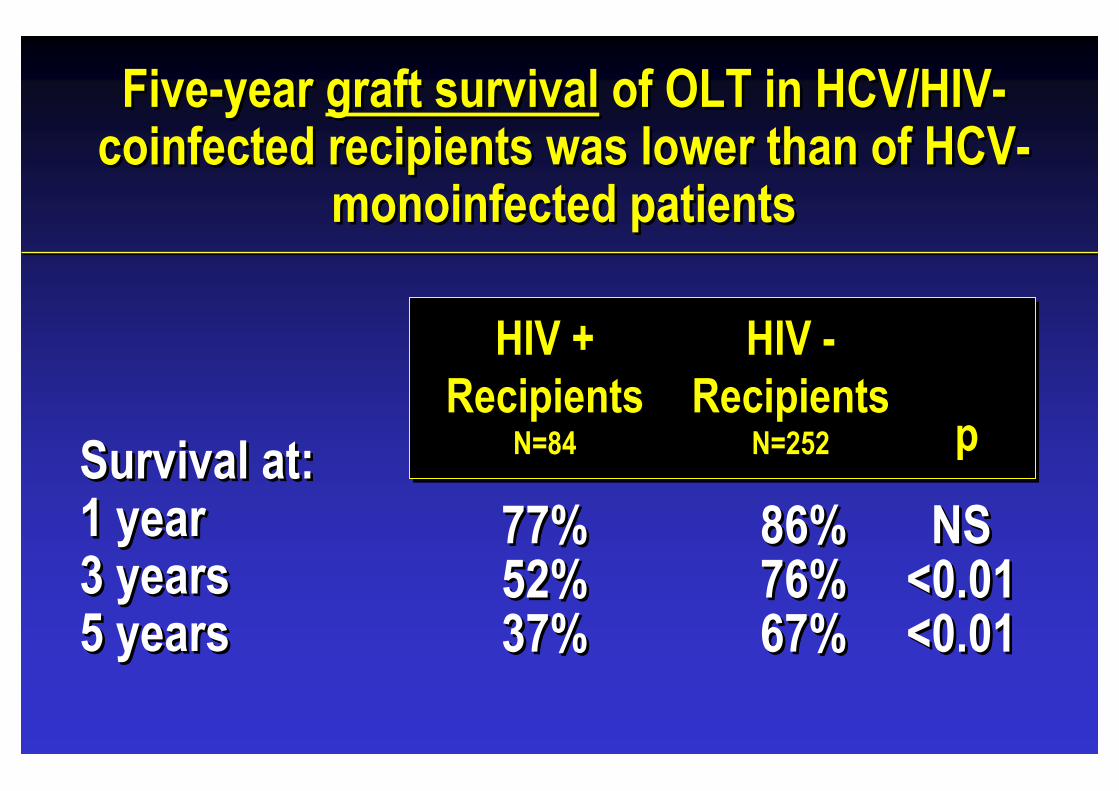
Five-year graft survival of OLT in HCV/HIV-coinfected recipients was lower than of HCV-
monoinfected patients
Five-year graft survival of OLT in HCV/HIV-coinfected recipients was lower than of HCV-
monoinfected patients
Survival at:1 year3 years5 years
SurvivalSurvival atat::1 1 yearyear3 3 yearsyears5 5 yearsyears
HIV +Recipients
N=84
HIV +HIV +RecipientsRecipients
N=84N=84
HIV -Recipients
N=252
HIV HIV --RecipientsRecipients
N=252N=252 ppp
77%52%37%
77%77%52%52%37%37%
86%76%67%
86%86%76%76%67%67%
NS<0.01<0.01
NSNS<0.01<0.01<0.01<0.01
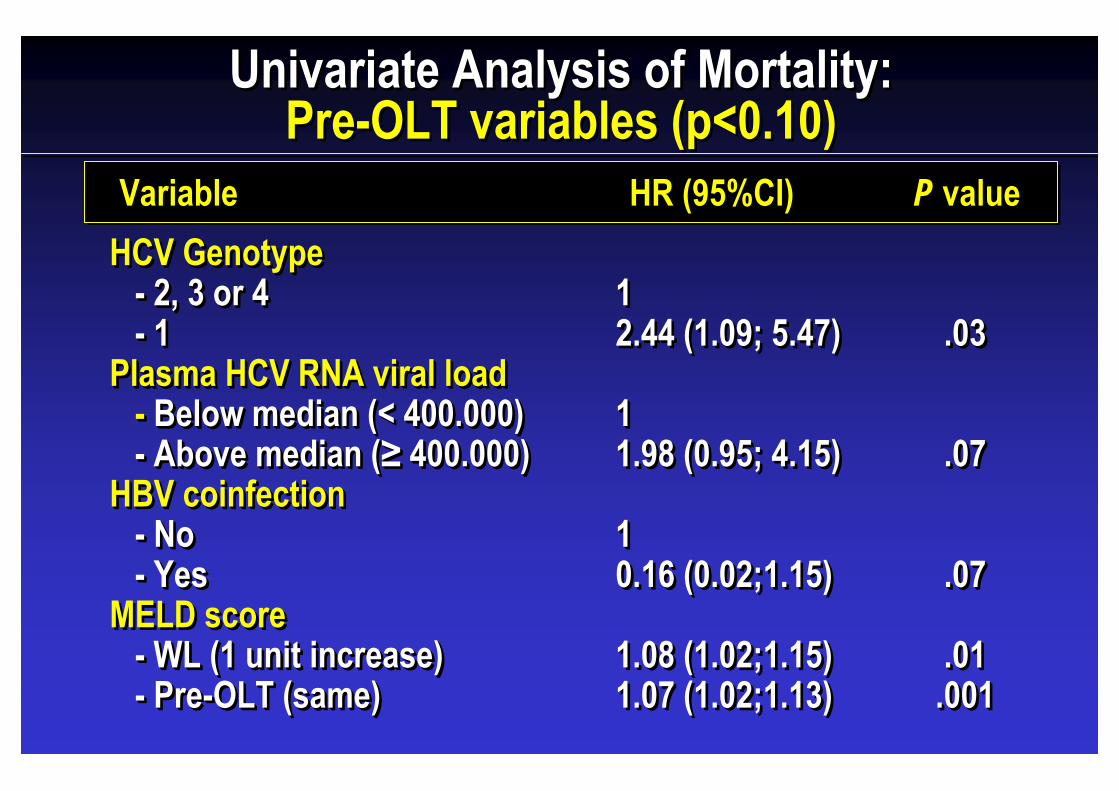
HCV Genotype - 2, 3 or 4- 1
Plasma HCV RNA viral load- Below median (< 400.000)- Above median (≥ 400.000)
HBV coinfection- No- Yes
MELD score- WL (1 unit increase)- Pre-OLT (same)
HCV Genotype -- 2, 3 or 42, 3 or 4-- 11
Plasma HCV RNA viral loadPlasma HCV RNA viral load-- BelowBelow median (< 400.000)median (< 400.000)-- Above median (Above median (≥≥ 400.000)400.000)
HBV HBV coinfectioncoinfection-- NoNo-- YesYes
MELD score-- WL (1 WL (1 unitunit increaseincrease))-- PrePre--OLT (OLT (samesame))
VariableVariableVariable HR (95%CI)HR (95%CI)HR (95%CI)
12.44 (1.09; 5.47)
1 1.98 (0.95; 4.15)
1 0.16 (0.02;1.15)
1.08 (1.02;1.15)1.07 (1.02;1.13)
12.44 (1.09; 5.47)
1 1 1.98 (0.95; 4.15)
1 1 0.16 (0.02;1.15)
1.08 (1.02;1.15)1.07 (1.02;1.13)
P valuePP valuevalue
.03
.07
.07
.01.001
.03.03
.07.07
.07.07
.01.01.001.001
Univariate Analysis of Mortality:Pre-OLT variables (p<0.10)
Univariate Analysis of Mortality:Pre-OLT variables (p<0.10)
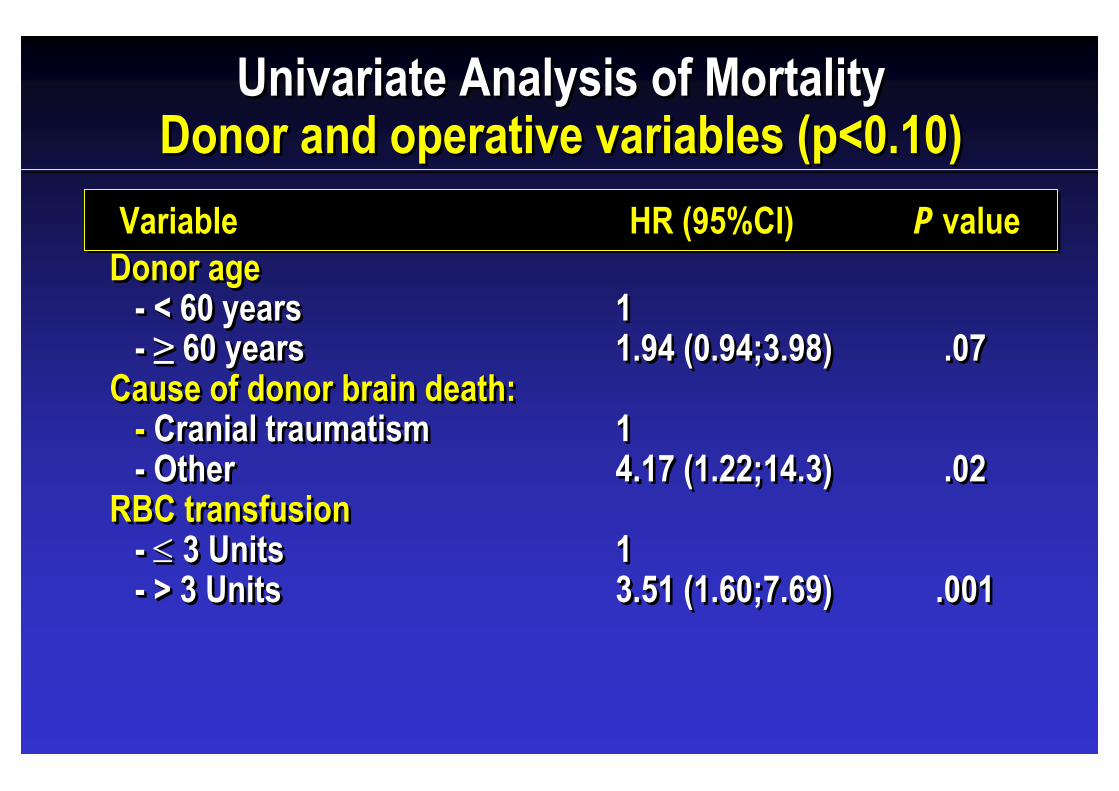
Donor age - < 60 years- ≥ 60 years
Cause of donor brain death:- Cranial traumatism- Other
RBC transfusion- ≤ 3 Units- > 3 Units
Donor age -- < 60 years< 60 years-- ≥≥ 60 years60 years
Cause of donor brain death:Cause of donor brain death:-- CranialCranial traumatismtraumatism-- OtherOther
RBC transfusion-- ≤≤ 3 Units3 Units-- > 3 Units> 3 Units
VariableVariableVariable HR (95%CI)HR (95%CI)HR (95%CI)
11.94 (0.94;3.98)
1 4.17 (1.22;14.3)
13.51 (1.60;7.69)
11.94 (0.94;3.98)
1 1 4.17 (1.22;14.3)
113.51 (1.60;7.69)
P valuePP valuevalue
.07
.02
.001
.07.07
.02.02
.001.001
Univariate Analysis of MortalityDonor and operative variables (p<0.10)
Univariate Analysis of MortalityDonor and operative variables (p<0.10)
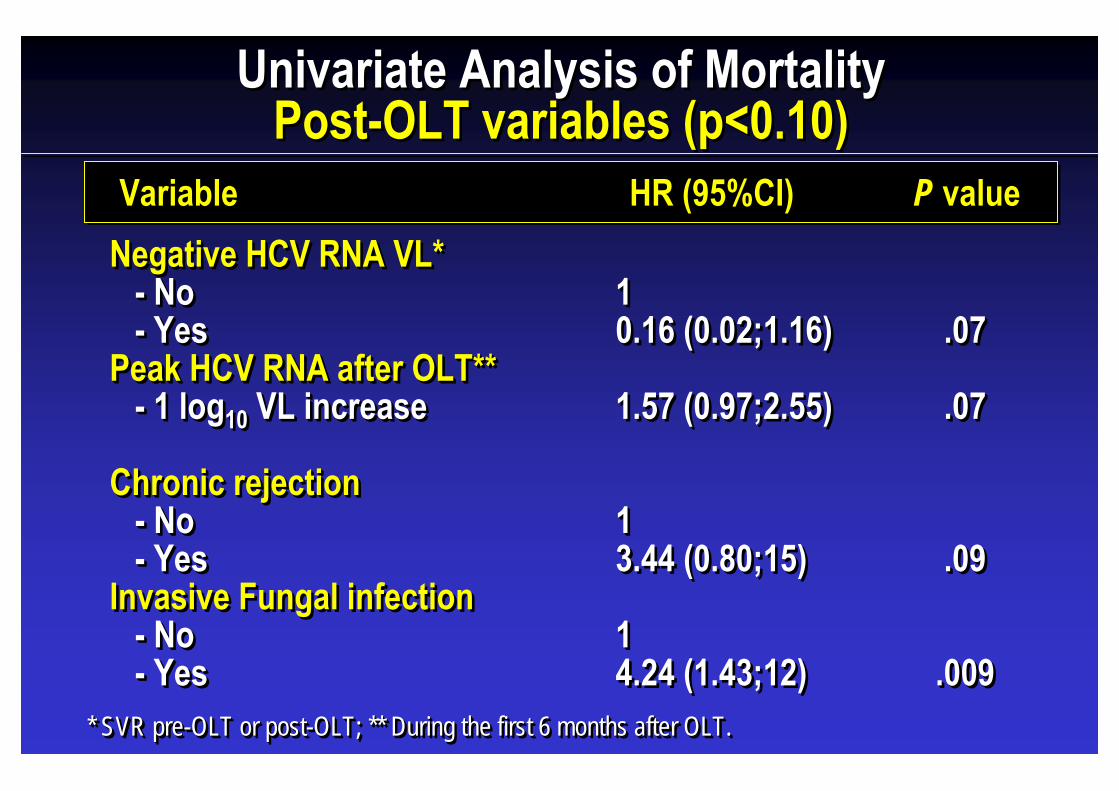
Negative HCV RNA VL*- No- Yes
Peak HCV RNA after OLT**- 1 log10 VL increase
Chronic rejection- No- Yes
Invasive Fungal infection- No- Yes
Negative HCV RNA VL*-- NoNo-- YesYes
Peak HCV RNA after OLT**Peak HCV RNA after OLT**-- 1 log1 log10 VL VL increaseincrease
Chronic rejectionChronic rejection-- NoNo-- YesYes
Invasive Fungal infection-- NoNo-- YesYes
VariableVariableVariable HR (95%CI)HR (95%CI)HR (95%CI)
10.16 (0.02;1.16)
1.57 (0.97;2.55)
1 3.44 (0.80;15)
14.24 (1.43;12)
10.16 (0.02;1.16)
1.57 (0.97;2.55)
1 1 3.44 (0.80;15)
114.24 (1.43;12)
P valuePP valuevalue
.07
.07
.09
.009
.07.07
.07.07
.09.09
.009.009
Univariate Analysis of MortalityPost-OLT variables (p<0.10)
Univariate Analysis of MortalityPost-OLT variables (p<0.10)
* SVR pre-OLT or post-OLT; ** During the first 6 months after OLT.* SVR * SVR prepre--OLT OLT oror postpost--OLT; ** OLT; ** DuringDuring thethe firstfirst 6 6 monthsmonths afterafter OLT.OLT.
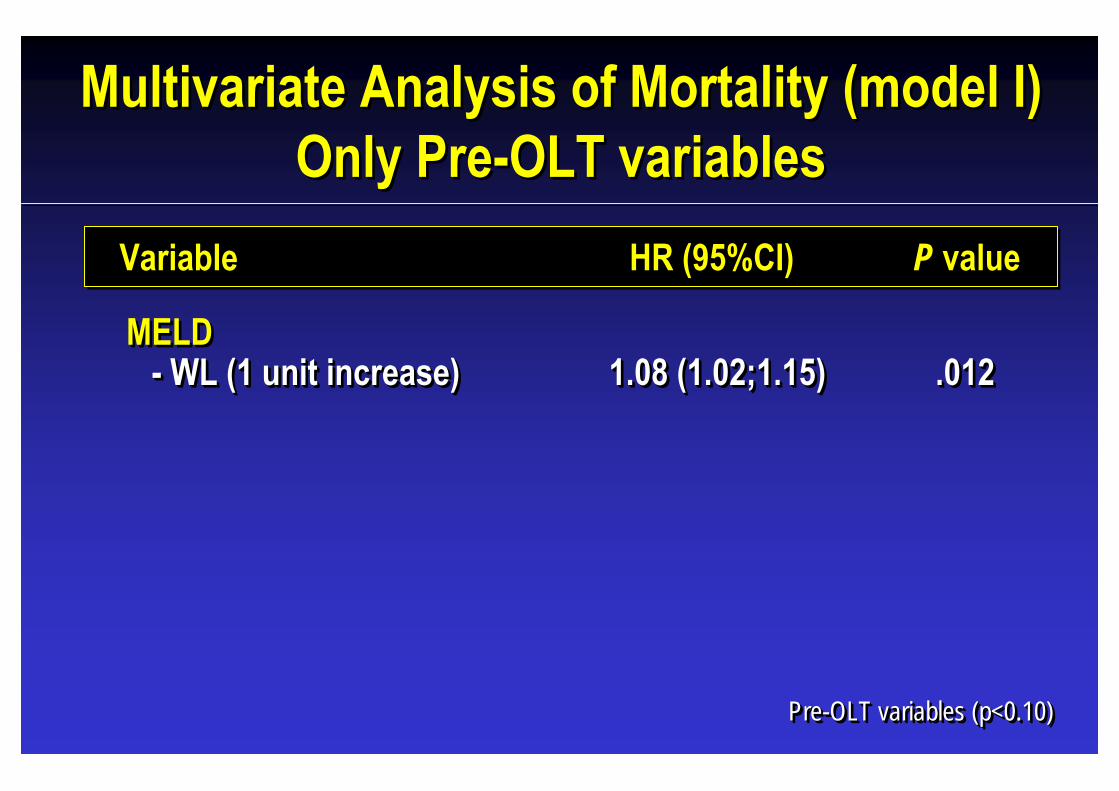
MELD- WL (1 unit increase)
MELD-- WL (1 WL (1 unitunit increaseincrease))
VariableVariableVariable HR (95%CI)HR (95%CI)HR (95%CI)
1.08 (1.02;1.15)1.08 (1.02;1.15)1.08 (1.02;1.15)
P valuePP valuevalue
.012.012.012
Multivariate Analysis of Mortality (model I) Only Pre-OLT variables
Multivariate Analysis of Mortality (model I) Only Pre-OLT variables
Pre-OLT variables (p<0.10)PrePre--OLT variables (p<0.10)OLT variables (p<0.10)
VariableVariableVariable HR (95%CI)HR (95%CI)HR (95%CI) P valuePP valuevalue
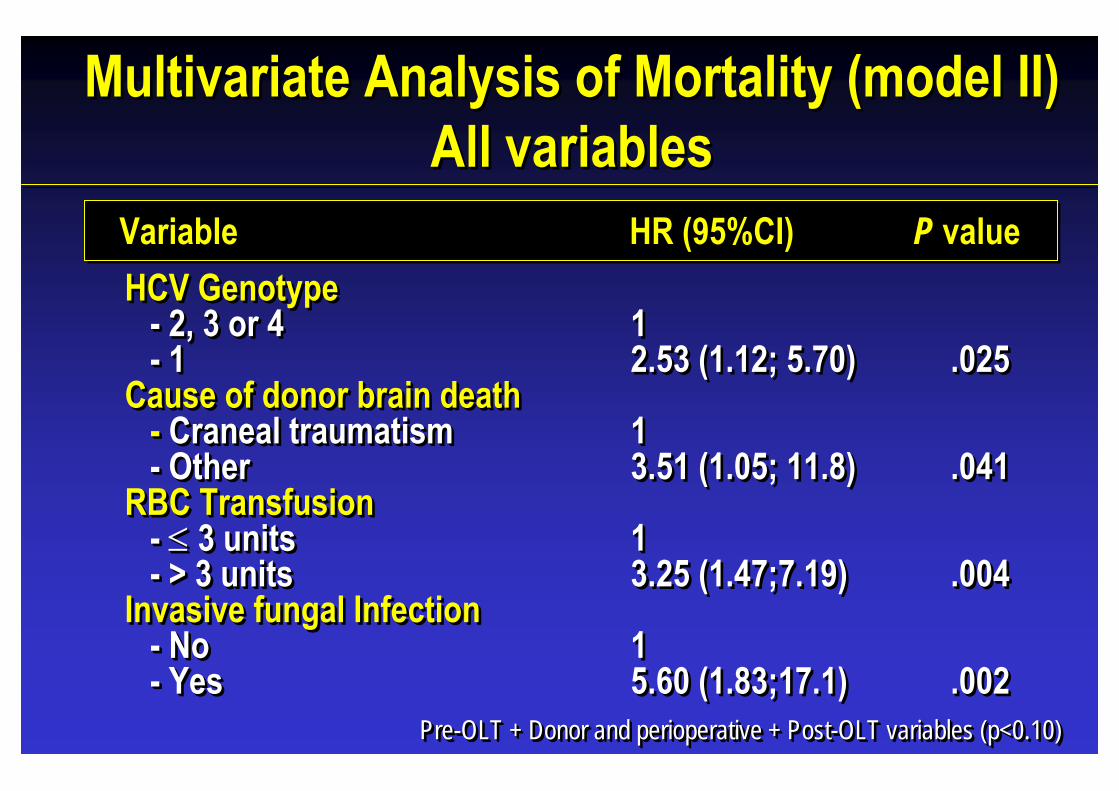
Pre-OLT + Donor and perioperative + Post-OLT variables (p<0.10)PrePre--OLT + OLT + DonorDonor andand perioperativeperioperative + Post+ Post--OLT variables (p<0.10)OLT variables (p<0.10)
Multivariate Analysis of Mortality (model II) All variables
Multivariate Analysis of Mortality (model II) All variables
HCV Genotype - 2, 3 or 4- 1
Cause of donor brain death- Craneal traumatism- Other
RBC Transfusion- ≤ 3 units- > 3 units
Invasive fungal Infection- No- Yes
HCV Genotype -- 2, 3 or 42, 3 or 4-- 11
Cause of donor brain deathCause of donor brain death-- Craneal Craneal traumatismtraumatism-- OtherOther
RBC TransfusionRBC Transfusion-- ≤≤ 3 units3 units-- > 3 units> 3 units
Invasive fungal Infection-- NoNo-- YesYes
12.53 (1.12; 5.70)
1 3.51 (1.05; 11.8)
1 3.25 (1.47;7.19)
15.60 (1.83;17.1)
12.53 (1.12; 5.70)
1 1 3.51 (1.05; 11.8)
1 1 3.25 (1.47;7.19)
15.60 (1.83;17.1)
.025
.041
.004
.002
.025.025
.041.041
.004.004
.002.002
• OLT is a safe and effective short-term (1 year) procedure in HCV-HIV-coinfected recipients. However, graft and patient survival at 5 years was lower than the matched HCV monoinfected patients.
• When a multivariate analysis was performed taking into account pre-OLT, donor, operative and post-OLT variables, factors associated with mortality risk were: HCV Genotype 1, non-traumatic cause of donor brain death, operative high blood transfusion requirements and invasive fungal infection.
• OLT is a safe and effective short-term (1 year) procedure in HCV-HIV-coinfected recipients. However, graft and patient survival at 5 years was lower than the matched HCV monoinfected patients.
• When a multivariate analysis was performed taking into account pre-OLT, donor, operative and post-OLT variables, factors associated with mortality risk were: HCV Genotype 1, non-traumatic cause of donor brain death, operative high blood transfusion requirements and invasive fungal infection.
CONCLUSIONSCONCLUSIONS

• When a multivariate analysis was performed taking into account only pre-OLT variables, a high MELD score at the time of listing for OLT was the only variable associated with death.
• A better recipient and donor selection and effective anti-HCV therapies could improve the long term outcome of HCV OLT in HIV-infected recipients.
• When a multivariate analysis was performed taking into account only pre-OLT variables, a high MELD score at the time of listing for OLT was the only variable associated with death.
• A better recipient and donor selection and effective anti-HCV therapies could improve the long term outcome of HCV OLT in HIV-infected recipients.
CONCLUSIONS (II)CONCLUSIONS (II)

HOSP. DE BELLVITGE – U.B. (BARCELONA)G. Rufi, A. Rafecas, FX Xiol, J.Fabregat, J.Torras , E.Ramos, L. Lladó, M. Santín, J. Figueras, C. Peñas , R.. Lastra.
HOSP. RAMON Y CAJAL (MADRID)R. Barcena, E. de Vicente, J. Fortún, C. Quereda, S. Moreno, P. Martín,M. García, AM. Moreno., S. Del Campo
HOSP. VALL D´HEBRON – U.A.B. (BARCELONA)V. Vargas, C. Margarit, Ll. Castells, E. Ribera, A. Pahissa, JI. Esteban, J. Gavaldá.
HOSP. DE CRUCES (VIZCAYA)M. Montejo, A. Valdivieso, M. Gastaka, J.R. Fernandez, M. Testillano, J. Bustamante, M.J. Suarez, K. Aguirrebengoa, J. Goikoetxea, J. Ortiz de Urbina, E. Montejo.
HOSP. CLINIC - IDIBAPS – U.B. (BARCELONA)JM Miró, A. Rimola, A. Moreno, M. Laguno, F.Aguero, M. López-Dieguez, M. Tuset, M. Brunet,C. Cervera, M. Monras, J. Mallolas, J. Blanch, C. Lanaspa, I. Pérez, E. de Lazzari, JM Gatell.
HOSP. UNIV. GREGORIO MARAÑON (MADRID)R. Bañares, P. Miralles, M. Salcedo, J. Cosín, JC López Bernaldo de Quirós, J. Berenguer
HOSP. UNIV. VIRGEN DEL ROCIO (SEVILLA)E. Cordero, JM. Cisneros, MA. Gómez, A. Bernardos, J. Serrano, F. Pareja et al.
HOSP. DE BELLVITGE – U.B. (BARCELONA)G. Rufi, A. Rafecas, FX Xiol, J.Fabregat, J.Torras , E.Ramos, L. Lladó, M. Santín, J. Figueras, C. Peñas , R.. Lastra.
HOSP. RAMON Y CAJAL (MADRID)R. Barcena, E. de Vicente, J. Fortún, C. Quereda, S. Moreno, P. Martín,M. García, AM. Moreno., S. Del Campo
HOSP. VALL D´HEBRON – U.A.B. (BARCELONA)V. Vargas, C. Margarit, Ll. Castells, E. Ribera, A. Pahissa, JI. Esteban, J. Gavaldá.
HOSP. DE CRUCES (VIZCAYA)M. Montejo, A. Valdivieso, M. Gastaka, J.R. Fernandez, M. Testillano, J. Bustamante, M.J. Suarez, K. Aguirrebengoa, J. Goikoetxea, J. Ortiz de Urbina, E. Montejo.
HOSP. CLINIC - IDIBAPS – U.B. (BARCELONA)JM Miró, A. Rimola, A. Moreno, M. Laguno, F.Aguero, M. López-Dieguez, M. Tuset, M. Brunet,C. Cervera, M. Monras, J. Mallolas, J. Blanch, C. Lanaspa, I. Pérez, E. de Lazzari, JM Gatell.
HOSP. UNIV. GREGORIO MARAÑON (MADRID)R. Bañares, P. Miralles, M. Salcedo, J. Cosín, JC López Bernaldo de Quirós, J. Berenguer
HOSP. UNIV. VIRGEN DEL ROCIO (SEVILLA)E. Cordero, JM. Cisneros, MA. Gómez, A. Bernardos, J. Serrano, F. Pareja et al.
SITES AND INVESTIGATORS (I)SITES AND INVESTIGATORS (I)
HOSP. UNIV. LA FE (VALENCIA)M. Blanes, M. Prieto et al.
HOSP. UNIV. REINA SOFIA (CORDOBA)J.Torre-Cisneros, M. de la Mata, JJ Castón, S. Rufian, P. López, A. Rivero, R. Lara.
HOSP. UNIV. CENTRAL DE ASTURIAS (OVIEDO)M. Rodríguez, I. González-Pinto, V. Asensi, ML. González-Diéguez.
HOSP. UNIV. VIRGEN DE LA ARRIXACA (MURCIA)JA. Pons et al.
HOSP. CARLOS HAYA (MALAGA)M. Jiménez, J. Rodrigo, A. De la Fuente, J. Santoyo, JL. Fernández, JM. Antúnez.
HOSP. 12 DE OCTUBRE (MADRID)JC. Meneu, F. Pulido, R. Rubio, E. Moreno, S. Olivares et al.
HOSP. UNIV. JUAN CANALEJO (LA CORUÑA)JD. Pedreira, F. Suárez, M. Gómez, S. López, P. Vázquez, A. Otero, MA. Castro.
HOSP. UNIV. MARQUES DE VALDECILLA (SANTANDER)MC. Fariñas, JD. García, S. Echevarría, E. Fábrega, G. Saravia et al.
HOSP. UNIV. SANTIAGO DE COMPOSTELA (LA CORUÑA)A. Antela, M. Delgado, A. Prieto, S. Tome et al.
HOSP. CLINICO LOZANO BLESA (ZARAGOZA)A. García-Gil, E. Tejero, S. Letona, R. Lozano, JJ. Araiz, P. Luque et al.
HOSP. UNIV. LA FE (VALENCIA)M. Blanes, M. Prieto et al.
HOSP. UNIV. REINA SOFIA (CORDOBA)J.Torre-Cisneros, M. de la Mata, JJ Castón, S. Rufian, P. López, A. Rivero, R. Lara.
HOSP. UNIV. CENTRAL DE ASTURIAS (OVIEDO)M. Rodríguez, I. González-Pinto, V. Asensi, ML. González-Diéguez.
HOSP. UNIV. VIRGEN DE LA ARRIXACA (MURCIA)JA. Pons et al.
HOSP. CARLOS HAYA (MALAGA)M. Jiménez, J. Rodrigo, A. De la Fuente, J. Santoyo, JL. Fernández, JM. Antúnez.
HOSP. 12 DE OCTUBRE (MADRID)JC. Meneu, F. Pulido, R. Rubio, E. Moreno, S. Olivares et al.
HOSP. UNIV. JUAN CANALEJO (LA CORUÑA)JD. Pedreira, F. Suárez, M. Gómez, S. López, P. Vázquez, A. Otero, MA. Castro.
HOSP. UNIV. MARQUES DE VALDECILLA (SANTANDER)MC. Fariñas, JD. García, S. Echevarría, E. Fábrega, G. Saravia et al.
HOSP. UNIV. SANTIAGO DE COMPOSTELA (LA CORUÑA)A. Antela, M. Delgado, A. Prieto, S. Tome et al.
HOSP. CLINICO LOZANO BLESA (ZARAGOZA)A. García-Gil, E. Tejero, S. Letona, R. Lozano, JJ. Araiz, P. Luque et al.
SITES AND INVESTIGATORS (II)SITES AND INVESTIGATORS (II)
ACKNOWLEDGEMENTSACKNOWLEDGEMENTS- Fundación para la Investigación y Prevención del SIDA en España (FIPSE).- Grupo de Estudio de Sida (GESIDA/SEIMC).- Sociedad Española de Trasplante Hepático (SETH).- Grupo de Estudio de Infecciones en Trasplantados. (GESITRA/SEIMC).- Fundación SEIMC-GESIDA (FSG)- Secretaria del Plan Nacional del Sida (SPNS) del Ministerio de Sanidad y Consumo (MSC).- Organización Nacional de Trasplante (ONT).
Our patients.
- Fundación para la Investigación y Prevención del SIDA en España (FIPSE).- Grupo de Estudio de Sida (GESIDA/SEIMC).- Sociedad Española de Trasplante Hepático (SETH).- Grupo de Estudio de Infecciones en Trasplantados. (GESITRA/SEIMC).- Fundación SEIMC-GESIDA (FSG)- Secretaria del Plan Nacional del Sida (SPNS) del Ministerio de Sanidad y Consumo (MSC).- Organización Nacional de Trasplante (ONT).
Our patients.