15c.Endometriosis
59
Endometriosis and Aden Endometriosis and Aden omyosis omyosis
-
Upload
deep-deep -
Category
Health & Medicine
-
view
4.431 -
download
1
Transcript of 15c.Endometriosis

Endometriosis and AdenomyEndometriosis and Adenomyosisosis

Endometriosis and adenEndometriosis and adenomyosis are benign conomyosis are benign conditions in which endomeditions in which endometrial glands and stroma trial glands and stroma are found beyond outsidare found beyond outside of the uteruse of the uterus..

EndometriosisEndometriosis

Endometriosis is a benign condition in whicEndometriosis is a benign condition in which endometrial glands and stroma are preseh endometrial glands and stroma are present outside the endometrial cavity, usually in nt outside the endometrial cavity, usually in the ovary or on the pelvic peritoneum. It assthe ovary or on the pelvic peritoneum. It assumes great importance in gynecology becaumes great importance in gynecology because of its frequency, distressing symptomatuse of its frequency, distressing symptomatology, association with infertility, and poteology, association with infertility, and potential for invasion of adjacent organ systemsntial for invasion of adjacent organ systems, such as the gastrointestinal or urinary trac, such as the gastrointestinal or urinary tracts. In addition, endometriosis often presentts. In addition, endometriosis often presents a difficult diagnostic problem, and few gys a difficult diagnostic problem, and few gynecologic conditions require such difficult snecologic conditions require such difficult surgical dissections.urgical dissections.

Incidence Incidence The exact incidence of endometriThe exact incidence of endometri
osis is not known, but it is estimatosis is not known, but it is estimated that more than 15 per cent of ed that more than 15 per cent of women have some degree of the women have some degree of the disease. It is noted in about 20% odisease. It is noted in about 20% of gynecologic laparotomies, and of gynecologic laparotomies, and of these it is an unexpected finding f these it is an unexpected finding in approximately one half of the cin approximately one half of the cases. ases.

Generally, endometriosis is Generally, endometriosis is initiated in the third decade of initiated in the third decade of life, becomes clinically apparent life, becomes clinically apparent in the thirties, and regresses in the thirties, and regresses after the menopause. It may, on after the menopause. It may, on occasion, occur in infancy, occasion, occur in infancy, childhood, or adolescence, but at childhood, or adolescence, but at these early ages it is almost these early ages it is almost always associated with always associated with obstructive genital anomalies.obstructive genital anomalies.

PathogenesisPathogenesis Three main theories for Three main theories for the development of the development of endometriosis have endometriosis have been proposedbeen proposed..

The The lymphatic-spread theorylymphatic-spread theory of Hal of Halban suggests that endometrial tissuban suggests that endometrial tissues are taken up into the lymphatics es are taken up into the lymphatics draining the uterus and are transpodraining the uterus and are transported to the various pelvic sites wherrted to the various pelvic sites where the tissue grows ectopically. Endoe the tissue grows ectopically. Endometrial tissue has been found in pelmetrial tissue has been found in pelvic lymphatics in up to 20% of patievic lymphatics in up to 20% of patients with the diseasents with the disease..

The The mullerian metaplasia themullerian metaplasia theoryory of Meyer proposes that en of Meyer proposes that endometriosis results from the dometriosis results from the metaplastic transformation of metaplastic transformation of peritoneal mesothelium into eperitoneal mesothelium into endometrium under the influendometrium under the influence of certain unidentified stince of certain unidentified stimuli.muli.

The The retrograde menstruation retrograde menstruation theorytheory of Sampson proposes that of Sampson proposes that endometrial fragments endometrial fragments transported through the fallopian transported through the fallopian tubes at the time of menstruation tubes at the time of menstruation implant and grow in various intra-implant and grow in various intra-abdominal sites. Endometrial abdominal sites. Endometrial tissue normally sheds at the time tissue normally sheds at the time of menstruation is viable and of menstruation is viable and capable of growth in vivo or in capable of growth in vivo or in vitro.vitro.

To explain some rare examples oTo explain some rare examples of endometriosis in distant sites, sf endometriosis in distant sites, such as the forehead or axilla, it is uch as the forehead or axilla, it is necessary to postulate hematogenecessary to postulate hematogenous spread. Quite probably, all onous spread. Quite probably, all of these postulated mechanisms plf these postulated mechanisms play a role in the development of eay a role in the development of endometriosis, and no single mecndometriosis, and no single mechanism explains allhanism explains all cases. cases.

Sites of OccurrenceSites of Occurrence

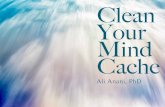
Endometriosis occurs most commonly in thEndometriosis occurs most commonly in the ovaries, the broad ligament, the peritoneae ovaries, the broad ligament, the peritoneal surfaces of the cul-de-sac including the utl surfaces of the cul-de-sac including the uterosacral ligaments and posterior cervix, anerosacral ligaments and posterior cervix, and in the rectovaginal septum (Fig. 1). Quite fd in the rectovaginal septum (Fig. 1). Quite frequently, the rectosigmoid colon is involverequently, the rectosigmoid colon is involved, as is the appendix and the vesicouterine fd, as is the appendix and the vesicouterine fold of the peritoneum. Endometriosis is occold of the peritoneum. Endometriosis is occasionally seen in laparotomy scars, developasionally seen in laparotomy scars, developing especially after cesarean sections or mying especially after cesarean sections or myomectomies when the endometrial cavity homectomies when the endometrial cavity has been entered. In spite of the great variety as been entered. In spite of the great variety of sites, 60% of patients with endometriosis of sites, 60% of patients with endometriosis have ovarian involvement.have ovarian involvement.


Fig. 1. Common site of endometriosis in decreFig. 1. Common site of endometriosis in decreasing order of frequency:asing order of frequency:
(1) ovary, (2) cul-de-sac, (3) uterosacral liga(1) ovary, (2) cul-de-sac, (3) uterosacral ligaments, (4) broad ligaments, (5) fallopian tuments, (4) broad ligaments, (5) fallopian tubes, (6) uterovesical fold, (7) round ligamenbes, (6) uterovesical fold, (7) round ligaments, (8) vermiform appendix, (9) vagina, (10) rts, (8) vermiform appendix, (9) vagina, (10) rectovaginal septum, (11) rectosigmoid coloectovaginal septum, (11) rectosigmoid colon, (12) cecum, (13) ileum, (14) inguinal, (15) n, (12) cecum, (13) ileum, (14) inguinal, (15) abdominal scars, (16) ureters, (17) urinary babdominal scars, (16) ureters, (17) urinary bladder, (18) umbilicus, (19) vulva, and (20) pladder, (18) umbilicus, (19) vulva, and (20) peripheral sites.eripheral sites.

PathologyPathology Characteristically, an endometriosis Characteristically, an endometriosis
of the ovary forms a small cyst. It is filof the ovary forms a small cyst. It is filled with thick, chocolate-colored fluiled with thick, chocolate-colored fluid that sometimes has the black color d that sometimes has the black color and tarry consistency of crankcase oiand tarry consistency of crankcase oil. This characteristic fluid represents l. This characteristic fluid represents aged, hemolyzed blood and desquaaged, hemolyzed blood and desquamated endometriummated endometrium..



Usually, endometrial glands and sUsually, endometrial glands and stroma are present in the cyst wall. troma are present in the cyst wall. Sometimes, however, the pressurSometimes, however, the pressure of the enclosed fluid destroys te of the enclosed fluid destroys the endometrial lining of the endohe endometrial lining of the endometrioma, leaving only a fibrotic cmetrioma, leaving only a fibrotic cyst wall infiltrated with large numyst wall infiltrated with large numbers of hemosiderin-laden macrobers of hemosiderin-laden macrophagesphages. .

Most often, the ovarian endometriomMost often, the ovarian endometrioma is tightly adherent to the posterior la is tightly adherent to the posterior leaf of the broad ligament bound by aeaf of the broad ligament bound by adhesions. An ovarian endometrioma dhesions. An ovarian endometrioma may reach dimensions as large as 20cmay reach dimensions as large as 20cm in diameter. Most instances of ovarm in diameter. Most instances of ovarian endometriosis are bilateral, and tian endometriosis are bilateral, and there is usually involvement of parietahere is usually involvement of parietal and visceral peritoneal surfaces. l and visceral peritoneal surfaces.


When endometriosis involves the peritoneaWhen endometriosis involves the peritoneal surfaces, it appears as flat, brownish discoll surfaces, it appears as flat, brownish discolorations, often referred to as “powder burorations, often referred to as “powder burns” or, if they are raised and bluish in colorns” or, if they are raised and bluish in color, as “mulberry spots.” The tissues surroun, as “mulberry spots.” The tissues surrounding these lesions are puckered and scarred ding these lesions are puckered and scarred as a result of fibrosis. Frequently, the rectosas a result of fibrosis. Frequently, the rectosigmoid colon becomes tightly bound by denigmoid colon becomes tightly bound by dense endometriotic adhesions to the posterior se endometriotic adhesions to the posterior wall of the lower uterine segment and cerviwall of the lower uterine segment and cervix, resulting in fixed retroversion of the uterux, resulting in fixed retroversion of the uterus and obliteration of the cul-de-sac.s and obliteration of the cul-de-sac.


The characteristic triad of symptoms assThe characteristic triad of symptoms associated with endometriosis is ociated with endometriosis is dysmenorrdysmenorrhea, dyspareunia, and dyschezia.hea, dyspareunia, and dyschezia. Genera Generally, secondary dysmenorrhea first appearlly, secondary dysmenorrhea first appears or worsens in the late twenties or early s or worsens in the late twenties or early thirties. If the endometriosis is associatethirties. If the endometriosis is associated with obstructive genital anomalies, sevd with obstructive genital anomalies, severe dysmenorrhea may commence at meere dysmenorrhea may commence at menarche.narche.

Dyspareunia is generally associated Dyspareunia is generally associated with deep penetration and occurs with deep penetration and occurs mainly when the cul-de-sac, uterosmainly when the cul-de-sac, uterosacral ligaments, and portions of the acral ligaments, and portions of the posterior vaginal fornix are involveposterior vaginal fornix are involved. Endometriomata in these sites ard. Endometriomata in these sites are usually exquisitely tender to touce usually exquisitely tender to touch.h.

Dyschezia is experienced with uterosacralDyschezia is experienced with uterosacral, cul-de-sac, and rectosigmoid colon invol, cul-de-sac, and rectosigmoid colon involvement. As the stool passes between the vement. As the stool passes between the uterosacral ligaments, the characteristic uterosacral ligaments, the characteristic dyschezia is experienced. This symptom idyschezia is experienced. This symptom is highly characteristic and is much more cs highly characteristic and is much more common with endometriosis than with chrommon with endometriosis than with chronic salpingo-oophoritis, a condition that onic salpingo-oophoritis, a condition that is often confused with endometriosis. is often confused with endometriosis.

Premenstrual and postmenstrual spotting Premenstrual and postmenstrual spotting is a characteristic symptom of endometriois a characteristic symptom of endometriosis. Menorrhagia is uncommon, the amousis. Menorrhagia is uncommon, the amount of menstrual flow usually diminishing wnt of menstrual flow usually diminishing with endometriosis. If the ovarian capsule is ith endometriosis. If the ovarian capsule is involved with endometriosis, ovulatory painvolved with endometriosis, ovulatory pain and midcycle vaginal bleeding often bein and midcycle vaginal bleeding often become a problem. Rarely, as other organ sycome a problem. Rarely, as other organ systems are involved, menstrual hematochestems are involved, menstrual hematochezia, hematuria, and other forms of vicariozia, hematuria, and other forms of vicarious menstruation become evident.us menstruation become evident.

The nature of pelvic pain caused by eThe nature of pelvic pain caused by endometriosis is variable. It has been sndometriosis is variable. It has been stated that the degree of pain varies intated that the degree of pain varies inversely with the extent of the disease. versely with the extent of the disease. Minimal endometriosis in the cul-de-sMinimal endometriosis in the cul-de-sac is generally much more painful thaac is generally much more painful than a huge endometrioma within the ovn a huge endometrioma within the ovary that is expanding freely into the aary that is expanding freely into the abdominal cavity.bdominal cavity.

Infertility as a symptom of endometriosis Infertility as a symptom of endometriosis is difficult to understand completely and is difficult to understand completely and even more difficult to quantify. Although even more difficult to quantify. Although approximately 10% of “normal” couples approximately 10% of “normal” couples are infertile, some 30% to 40% of are infertile, some 30% to 40% of couples are infertile if the female couples are infertile if the female presents with endometriosis. The presents with endometriosis. The condition is found in 40% to 50% of condition is found in 40% to 50% of women who undergo surgery for women who undergo surgery for infertility.infertility.

SignsSigns Endometriosis presents with a wiEndometriosis presents with a wi
de variety of signs varying from thde variety of signs varying from the presence of a small, exquieitely e presence of a small, exquieitely tender nodule in the cul-de-sac or tender nodule in the cul-de-sac or on the uterosacral ligaments to a on the uterosacral ligaments to a huge, relatively nontender, cystic huge, relatively nontender, cystic abdominal mass. abdominal mass.

Occasionally, a small tender mulberry spoOccasionally, a small tender mulberry spot may be seen in the posterior fornix of tht may be seen in the posterior fornix of the vagina. Characteristically, a tender, fixee vagina. Characteristically, a tender, fixed adnexal mass is abserved on bimanual d adnexal mass is abserved on bimanual examination. The uterus is retroverted in examination. The uterus is retroverted in a substantial number of women surgically a substantial number of women surgically explored for endometriosis. Frequently, nexplored for endometriosis. Frequently, no signs at all are abserved on physical exao signs at all are abserved on physical examination. The characteristic sharp, firm, emination. The characteristic sharp, firm, exquisitely tender “barb” felt in the uterxquisitely tender “barb” felt in the uterosacral ligament is the diagnostic sine quosacral ligament is the diagnostic sine qua non of endometriosis.a non of endometriosis.

Differential DiagnosisDifferential Diagnosis
The main differential diagnosis cThe main differential diagnosis confused with endometriosis are (onfused with endometriosis are (1) chronic pelvic inflammatory dis1) chronic pelvic inflammatory disease or recurrent acute salpingitisease or recurrent acute salpingitis, (2) hemorrhagic corpus luteum, (, (2) hemorrhagic corpus luteum, (3) benign or malignant ovarian ne3) benign or malignant ovarian neoplasm, and, occasionally, (4) ectoplasm, and, occasionally, (4) ectopic pregnancy.opic pregnancy.

DiagnosisDiagnosis
The diagnosis of endometriosis shThe diagnosis of endometriosis should be suspected in an afebrile pould be suspected in an afebrile patient with the characteristic symatient with the characteristic symptom triad of endometriosis, a firptom triad of endometriosis, a firm, fixed, tender adnexal mass, anm, fixed, tender adnexal mass, and tender nodularity in the cul-de-sd tender nodularity in the cul-de-sac and uterosacral ligaments. ac and uterosacral ligaments.

This diagnosis is even more likely if tThis diagnosis is even more likely if the leukocyte count and erythrocyte she leukocyte count and erythrocyte sedimentation rate are normal. The seedimentation rate are normal. The serum CA-125 level is frequently elevatrum CA-125 level is frequently elevated. An ultrasonic evaluation may indied. An ultrasonic evaluation may indicate an adnexal mass of complex echcate an adnexal mass of complex echogenicity. The definitive diagnosis is ogenicity. The definitive diagnosis is generally made by the characteristic generally made by the characteristic gross and histologic findings at lapargross and histologic findings at laparoscopy or laparotomy.oscopy or laparotomy.

ManagementManagement The management of endometriosis The management of endometriosis
depends on certain key depends on certain key considerations: (1) the certainty of the considerations: (1) the certainty of the diagnosis, (2) the severity of the diagnosis, (2) the severity of the symptoms, (3) the extent of the symptoms, (3) the extent of the disease, (4) the desire for future disease, (4) the desire for future fertility, (5) the age of the patient, and fertility, (5) the age of the patient, and (6) the threat to the gastrointestinal or (6) the threat to the gastrointestinal or urinary tracts or both.urinary tracts or both.

Medical Medical TherapyTherapy

If endometriosis is minimal in extent aIf endometriosis is minimal in extent and the symptoms are tolerable, no trend the symptoms are tolerable, no treatment is necessary, but the patient satment is necessary, but the patient should be observed at 6-month intervahould be observed at 6-month intervals. The use ofls. The use of
medroxyprogesterone acetate or a comedroxyprogesterone acetate or a combined estrogen and progestin oral cmbined estrogen and progestin oral contraceptive on a cyclic basis may inhontraceptive on a cyclic basis may inhibit the growth of endometriosis, sincibit the growth of endometriosis, since this treatment effects an “exhaustie this treatment effects an “exhaustion atrophy” of the normally placed oon atrophy” of the normally placed or ectopic endometrium. r ectopic endometrium.

If the disease is minimal and symptoms are If the disease is minimal and symptoms are incapacitating or if infertility is a problem, tincapacitating or if infertility is a problem, the endometriosis may be treated by a he endometriosis may be treated by a pseupseudopregnancy regimendopregnancy regimen, using either escalati, using either escalating continuous doses of combined oral contng continuous doses of combined oral contraceptives or progestin only over a period oraceptives or progestin only over a period of 6 to 9 months. Although most cases treatef 6 to 9 months. Although most cases treated with pseudopregnancy result in temporard with pseudopregnancy result in temporary relief of symptoms and up to 40% may bey relief of symptoms and up to 40% may become pregnant following cessation of treatcome pregnant following cessation of treatment, this regimen is poorly tolerated by mment, this regimen is poorly tolerated by most patients, and the endometriosis generalost patients, and the endometriosis generally redevelops following cessation of treatmly redevelops following cessation of treatment. Continuous progestin may be more effent. Continuous progestin may be more effective than continuous oral contraceptives.ective than continuous oral contraceptives.

Danazol, an androgen dervative, Danazol, an androgen dervative, may also be used in a “may also be used in a “pseudompseudomenopause”enopause” regimen to suppress regimen to suppress symptoms of endometriosis if fertsymptoms of endometriosis if fertility is not a present concern. It is ility is not a present concern. It is given over a period of 6 to 9 montgiven over a period of 6 to 9 months, and a dose of 100 to 800 mg dhs, and a dose of 100 to 800 mg daily may be necessary to suppress aily may be necessary to suppress menstruationmenstruation. .

Endometriosis may be treated witEndometriosis may be treated with a gonadotropin-releasing hormh a gonadotropin-releasing hormone (GnRH) agonist that effects a one (GnRH) agonist that effects a temporary medical castration, thtemporary medical castration, thereby bringing about a marked, alereby bringing about a marked, albeit temporary, regression of endbeit temporary, regression of endometriosis. Side effects of treatmometriosis. Side effects of treatment and expense restrict longterm ent and expense restrict longterm use. dose of 200 μg twice daily. use. dose of 200 μg twice daily.

Mifepristone (RU 486), which iMifepristone (RU 486), which is widely used as an abortifacies widely used as an abortifacient in Europe, is also used in thnt in Europe, is also used in the medical management of ende medical management of endometriosis. It is a synthetic anometriosis. It is a synthetic analogue of progesterone with aalogue of progesterone with antiprogestational and anticortntiprogestational and anticorticoid activity. It binds directly icoid activity. It binds directly with progesterone receptorswith progesterone receptors. .

Women with laparoscopically Women with laparoscopically confirmed endometriosis treaconfirmed endometriosis treaded with 50 mg of RU 486 daily ded with 50 mg of RU 486 daily for 6 months have a significant for 6 months have a significant reduction of their disease.reduction of their disease.

Surgical ResectionSurgical Resection Large (6 to 20 cm) endometriomata Large (6 to 20 cm) endometriomata
are amenable to surgical resection oare amenable to surgical resection only. If the patient is older than 45yeanly. If the patient is older than 45years, the preferred treatment is a total rs, the preferred treatment is a total abdominal hysterectomy (TAH) and abdominal hysterectomy (TAH) and bilateral salpingo-oophorectomy (Bbilateral salpingo-oophorectomy (BSO), even if the disease is entirely reSO), even if the disease is entirely resectable. sectable.

If fertility is desired, conservative surgery If fertility is desired, conservative surgery must be considered, such as resection of must be considered, such as resection of endometriomas and lysis of tubal adhesiendometriomas and lysis of tubal adhesions. Following the surgical resection of eons. Following the surgical resection of endometriosis, 50% to 60% of patients bendometriosis, 50% to 60% of patients become pregnant, usually in the first 2 yearcome pregnant, usually in the first 2 years following surgery. Even with minimal es following surgery. Even with minimal endometriosis, laparoscopic resection has ndometriosis, laparoscopic resection has been reported to significantly improve febeen reported to significantly improve fertility rates.rtility rates.

AdenomyosisAdenomyosis
Adenomyosis is defined aAdenomyosis is defined as the extension of endoms the extension of endometrial glands and stroma ietrial glands and stroma into the uterine musculatnto the uterine musculature. ure.

It is generally accepted that about 15% of It is generally accepted that about 15% of women develop varying degrees of adenwomen develop varying degrees of adenomyosis in their late 30s and early 40s. Oromyosis in their late 30s and early 40s. Originally, adenomyosis was referred to as iginally, adenomyosis was referred to as endometrosis interna, but these terms haendometrosis interna, but these terms have become archaic. About 15 % of patientve become archaic. About 15 % of patients with adenomyosis have associated ends with adenomyosis have associated endometriosis. The basal layers of the endoometriosis. The basal layers of the endometrium extend in continuity to sites witmetrium extend in continuity to sites within the myometrium and generally do nohin the myometrium and generally do not participate in the proliferative and secret participate in the proliferative and secretory cycles induced by the ovary.tory cycles induced by the ovary.

PathologyPathology Generally, the uterus grossly is difGenerally, the uterus grossly is dif
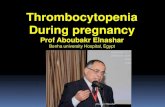
fusely enlarged with a thickened fusely enlarged with a thickened myometrium containing charactemyometrium containing characteristic glandular irregularities (Fig. ristic glandular irregularities (Fig. 2). The endometrial cavity is also 2). The endometrial cavity is also enlarged, consistent with the increnlarged, consistent with the increased myometrium. eased myometrium.

Histologically, the extent of thiHistologically, the extent of this process varies a great deal frs process varies a great deal from superficial extension into tom superficial extension into the underlying myometrium, to he underlying myometrium, to extension throughout the myoextension throughout the myometrium, occasionally with pemetrium, occasionally with penetration of the peritoneal surnetration of the peritoneal surface of the uterus.face of the uterus.

Occasionlly, the adenomyosis Occasionlly, the adenomyosis may be confined to one portiomay be confined to one portion of the myometrium and take n of the myometrium and take the form of a fairly well-circumthe form of a fairly well-circumscribed adenomyoma. Contrarscribed adenomyoma. Contrary to the picture in a uterine myy to the picture in a uterine myoma, no distinct capsular maroma, no distinct capsular margin can be detected on cut secgin can be detected on cut section between the adenomyomtion between the adenomyoma and the surrounding myomea and the surrounding myometrium. trium.

Fig. 2. Grossly enlarged uterus with mFig. 2. Grossly enlarged uterus with markedly thickened myometrium contaarkedly thickened myometrium containing adenomyosisining adenomyosis


SymptomsSymptoms
Typical symptoms of adenomyosiTypical symptoms of adenomyosis are severe s are severe secondary dysmenorrsecondary dysmenorrheahea and and menorrheagiamenorrheagia. The meno. The menorrhagia is consistent with the enlarrhagia is consistent with the enlarged surface area of the endometrrged surface area of the endometrial cavity and the increased volumial cavity and the increased volume of sloughed endometrium.e of sloughed endometrium.

The dysmenorrhea is of the colicky tThe dysmenorrhea is of the colicky type. Many patients are asymptomatiype. Many patients are asymptomatic. In about 30 to40 per cent of patienc. In about 30 to40 per cent of patients with adenomyosis, the disease is a ts with adenomyosis, the disease is a surprise pathologic finding in a patiesurprise pathologic finding in a patient without menorrhagia, dysmenorrnt without menorrhagia, dysmenorrhea, or uterine enlargement. Occasiohea, or uterine enlargement. Occasionally, in a patient with a large adenonally, in a patient with a large adenomyoma, pressure on the bladder or rmyoma, pressure on the bladder or rectum may create a problem.ectum may create a problem.

SignsSigns On pelvic examination, the uterus is sOn pelvic examination, the uterus is s
ymmetrically enlarged. Occasionally, iymmetrically enlarged. Occasionally, it may enlarge asymmetrically and mat may enlarge asymmetrically and make it impossible to distinguish this conke it impossible to distinguish this condition from that of a myomatous uterdition from that of a myomatous uterus. The consistency of the enlarged adus. The consistency of the enlarged adenomyomatous uterus is generally sofenomyomatous uterus is generally softer than that of a uterine myoma. On rter than that of a uterine myoma. On rare occasions, endometrial cancer maare occasions, endometrial cancer may arise in a focus of adenomyosis.y arise in a focus of adenomyosis.

TreatmentTreatment

The treatment of adenomyosis deThe treatment of adenomyosis depends entirely on the symptoms apends entirely on the symptoms and the possibility of other diagnosnd the possibility of other diagnoses. Any menorrhagia in an older paes. Any menorrhagia in an older patient (>35 years) should be investigtient (>35 years) should be investigated by endometrial biopsy or fracated by endometrial biopsy or fractional dilatation and curettage antional dilatation and curettage and/or hysteroscopy to rule out endod/or hysteroscopy to rule out endometrial cancer. metrial cancer.

If the menorrhagia is severe and rIf the menorrhagia is severe and recurrent following a dilatation anecurrent following a dilatation and curettage or if the dysmenorrhed curettage or if the dysmenorrhea is disabling, the use of a GnRH aa is disabling, the use of a GnRH agonist or mifepristone may providgonist or mifepristone may provide relief. Total abdominal or vagine relief. Total abdominal or vaginal hysterectomy, however, may bal hysterectomy, however, may be indicated. The ovaries should be e indicated. The ovaries should be preserved if they are normal, unlepreserved if they are normal, unless the patient is older than 45 yeass the patient is older than 45 yearsrs..

All of the following conditons have been imAll of the following conditons have been implicated in the pathogenesis of endometrioplicated in the pathogenesis of endometrio
sis EXCEPTsis EXCEPT
A coelomic metaplasiaA coelomic metaplasiaB endometrial hyperplasiaB endometrial hyperplasiaC retrograde menstruationC retrograde menstruationD immunologic deficiencyD immunologic deficiencyE lymphatic spread of endometrial fragmE lymphatic spread of endometrial fragm
entent

Dyspareunia in endometriosis is associated Dyspareunia in endometriosis is associated with all of the following EXCEPT:with all of the following EXCEPT:
A endometrioma of posterior vaginal foA endometrioma of posterior vaginal fornixrnix
B fixed retroversion of the uterusB fixed retroversion of the uterusC uterosacral implantsC uterosacral implantsD periadnexal adhesionsD periadnexal adhesions