
15 unilateral lobar or localized hyperlucency of the
14
15 Unilateral Lobar or Localized Hyperlucency of the Lung
-
Upload
muhammad-bin-zulfiqar -
Category
Education
-
view
170 -
download
1
Transcript of 15 unilateral lobar or localized hyperlucency of the

15 Unilateral Lobar or Localized Hyperlucency of the Lung
CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL

• Fig C 15-1 Congenital emphysematous bulla. Large thin-walled air cyst (arrows) in the mid-portion of the right lung.

• Fig C 15-2 Giant emphysematous bulla. The air-containing mass fills most of the left hemithorax.

• Fig C 15-3 Compensatory overaeration in agenesis of the left lung. There is virtually total absence of aerated lung in the left hemithorax. The right lung is markedly overinflated and has herniated across the midline. The entire mediastinum lies within the left hemithorax. The chest wall is asymmetric, and the ribs are somewhat close together on the left.

• Fig C 15-4 Westermark's sign of pulmonary embolism. (A) Baseline chest radiograph demonstrates normal vascularity in the left upper lobe. (B) Striking hyperlucency of the left upper lobe coincided with the onset of the patient's symptoms. (C) Arteriogram performed on the same day the film in (B) was made shows an occluding clot in the left upper lobe and multiple emboli in the right lung.

• Fig C 15-5 Unilateral hyperlucent lung. (A) Frontal radiograph exposed at total lung capacity reveals a marked discrepancy in the radiolucency of the two lungs, with the left showing severe oligemia but normal lung volume. (B) Frontal radiograph at residual volume after bronchography demonstrates severe air trapping in the left lung and little change in volume from total lung capacity. Because the deflation of the right lung is normal, the mediastinum has swung sharply to the right. (C) A pulmonary arteriogram shows the discrepancy in blood flow to the two lungs. The left pulmonary artery is present, although diminutive, differentiating this appearance from congenital absence of the left pulmonary artery.7
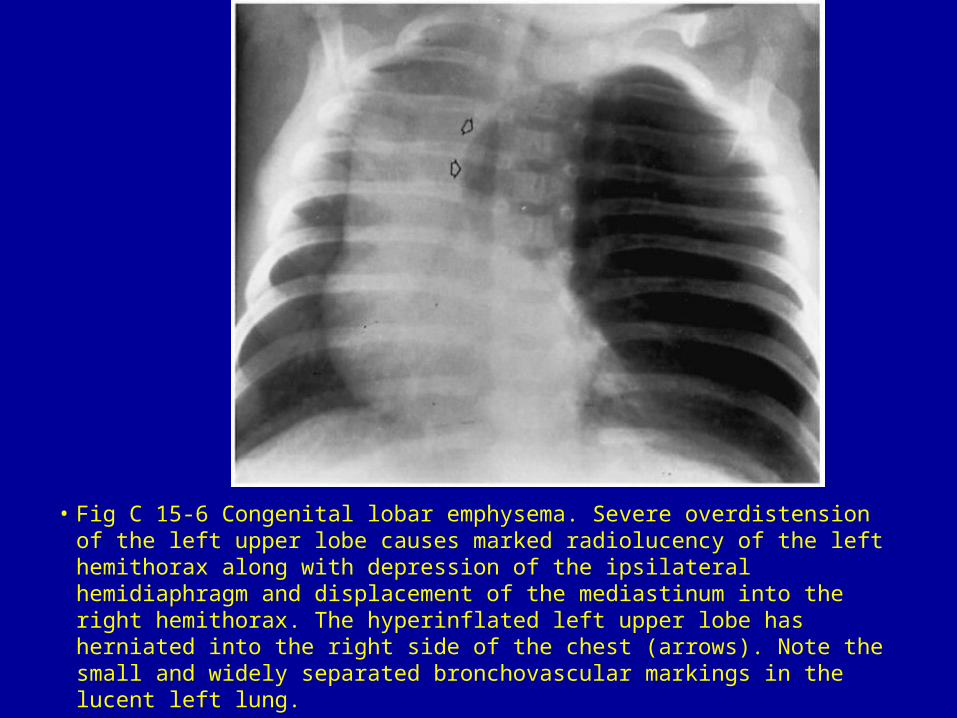
• Fig C 15-6 Congenital lobar emphysema. Severe overdistension of the left upper lobe causes marked radiolucency of the left hemithorax along with depression of the ipsilateral hemidiaphragm and displacement of the mediastinum into the right hemithorax. The hyperinflated left upper lobe has herniated into the right side of the chest (arrows). Note the small and widely separated bronchovascular markings in the lucent left lung.

• Fig C 15-7 Cystic adenomatoid malformation. Frontal radiograph of an infant's chest and abdomen at 1 hour of age demonstrates a large lucent mass in the right hemithorax with shift of the mediastinal structures to the left. In the lower right chest, the mass appears multicystic and resembles air-filled loops of bowel. Ascites is also present.33

• Fig C 15-8 Hydrocarbon poisoning. (A) Large thin-walled pneumatocele (arrows). (B) Multiple thin-walled pneumatoceles bilaterally but more marked on the right.

• Fig C 15-9 Absence of the right pectoralis muscles. Asymmetry of the thoracic cage with hypoplasia of the anterior ribs (arrows). The lower portion of the right lung appears hyperlucent, whereas the apex seems comparatively opaque.





















