15 th RBM Partnership Board Meeting 10 th November 2008 A. P. Dash Director National Institute of...
15
15 15 th th RBM Partnership Board Meeting RBM Partnership Board Meeting 10 10 th th November 2008 November 2008 A. P. Dash Director National Institute of Malaria National Institute of Malaria Research, Delhi Research, Delhi alaria Case Management at Point of Car
-
Upload
ashley-thompson -
Category
Documents
-
view
215 -
download
0
Transcript of 15 th RBM Partnership Board Meeting 10 th November 2008 A. P. Dash Director National Institute of...

1515thth RBM Partnership Board Meeting RBM Partnership Board Meeting1010thth November 2008 November 2008
1515thth RBM Partnership Board Meeting RBM Partnership Board Meeting1010thth November 2008 November 2008
A. P. DashDirector
National Institute of Malaria Research, National Institute of Malaria Research, DelhiDelhi
Malaria Case Management at Point of Care
National Institute of Malaria Research
Mandate
National Institute of Malaria Research
Mandate Basic and applied research Test and validate new drugs, vaccines,
diagnostics & insecticides Epidemic investigations Networking and linkages. Maintain parasite and vector repositories as a
national facility Human resource development Technical support to National Programme.

NIMR and Its Field UnitsNIMR and Its Field Units

Networking
of NIMR
NIV
IOP
VCRC
CRME
NIMS, DMRC
RMRCB
RMRCTJ
RMRC D
ICMR INSTITUTES
NIMR
INDIAN
UNIVERSITIES
DU Goa RDVV GGS IPJamia
RohtakBangalore
Sambalpur
DRUG MANUFACTURERS
Sanofi Aventis
Shin Poong
Emcure
Ranbaxy
EmcurePfizer
INSECTIC
IDE
MANUFACTURERS
Bayer
Vestergaard
Reliance
Sumitomo
Biotech
BASF
WHO
USAID
WHOPES
MMV
DNDi
PATH
Michigun Uni.
NY Univers
ity
INTERNATIO
NAL
AGENCIES
HO
SP
ITALS
TMHIGH
Wenlock
CWSBirla Hosp.
GO
VT.
OR
GA
NIS
ATI
ON
S
NICDNVBDCP
State Health
INT
ER
NA
TIO
NA
L
OR
GA
NIS
AT
ION
S
US Embassy
CDC NIH
MEDICAL COLLEGESCuttackGoa
Jabalpur
Goa
ICGEBDRDE
VA
CC
INE
/
OT
HE
RS
Liverpool
Morehouse
DBT
Min of Env & Forest
TribalWelfare Dept
GuwahatiDowntown
IISc
ISRO DRL
AIIMS
Central Facilities• Malaria Parasite Bank
– More than 750 Pf, about 100 Pv, 5 Pm strains, 50+ non human strains
• Insectory– NIMR maintains more than ten mosquito species in the insectory
• Animal House– The animal facility of NIMR maintains mice, rabbits etc.
• Central Instrumentation Facility– Has all the modern equipments including :
• 96 capillary DNA sequencer• LCMS/MS• Real Time PCR• HPLC• Flowcytometer• PCR machines etc.
• Library– More than 100 journals and 7000 books

Malaria case management: Treatment practices
• Assessment of malaria treatment practices in Public and Private Health Sector’s (2005-07)
• Operational research on drug use practice and pre-packaged blister pack drugs (2006-07)
• Extent of use of artemisinin monotherapy in malaria endemic states (2008)
• Operational research on drug use practice among children in Jharkhand (Initiated)
Treatment Practices in Public and Private Health Sector
• Study conducted (n=1107) in Low (Delhi), Moderate (Gujarat) and High Endemic areas (Orissa)
• Reporting of malaria cases from private sector was low (15-28%) as compared to public sector (48-98%)
• Diagnostic facilities (Microscopy) inadequate in Private Sector (14-74%)
• Awareness of new diagnostic techniques higher in high endemic state of Orissa (93%) than other states (38-66%)
• Knowledge about drug policy and treatment guidelines is inadequate – 63-98% in public and 50-77% in private sector

Treatment Practices with reference to change in Drug
Policy (Jharkhand)
0%
20%
40%
60%
80%
100%
Med
ical
Offi
cer
AngaraPHC
Silli &Namkum
JaldegaPHC
KoleberaPHC
Drugs prescribed for treatment of uncomplicated falciparum malaria
Artemisinin compounds
CQ or SP
CQ
• Despite change in drug policy in Angara & Jaldega districts, CQ/SP is used
• In Namkum recommended drug chloroquine is prescribed
• In Kolebera where first line drug is CQ, Artemisinin is prescribed by 50% clinicians

Prescribing pattern of antimalarials : Use of
Artemisinin Monotherapy
0.010.020.030.040.050.060.070.080.090.0
100.0
AS alone CQ SP MQ Am+Lum AS+SP AS+Other
Drug
% r
espo
nse
Assam Goa Gujarat Delhi Jharkhand Orissa
• 65% clinicians prescribe AS monotherapy• 32% prescribe SP alone• 35% prescribe AS+SP

Availability of antimalarials across the counter
Availability of Artemisinin Monotherapy in Chemist Shops (n = 493)
Not Available
23%
Available77%
Antimalarial sold without prescription(n = 493)
Selling without
prescription44%
With prescription
56%
• AS monotherapy AS monotherapy
available with 77% available with 77%
chemistschemists
• 44% chemists sale 44% chemists sale
antimalarials without antimalarials without
prescriptionprescription
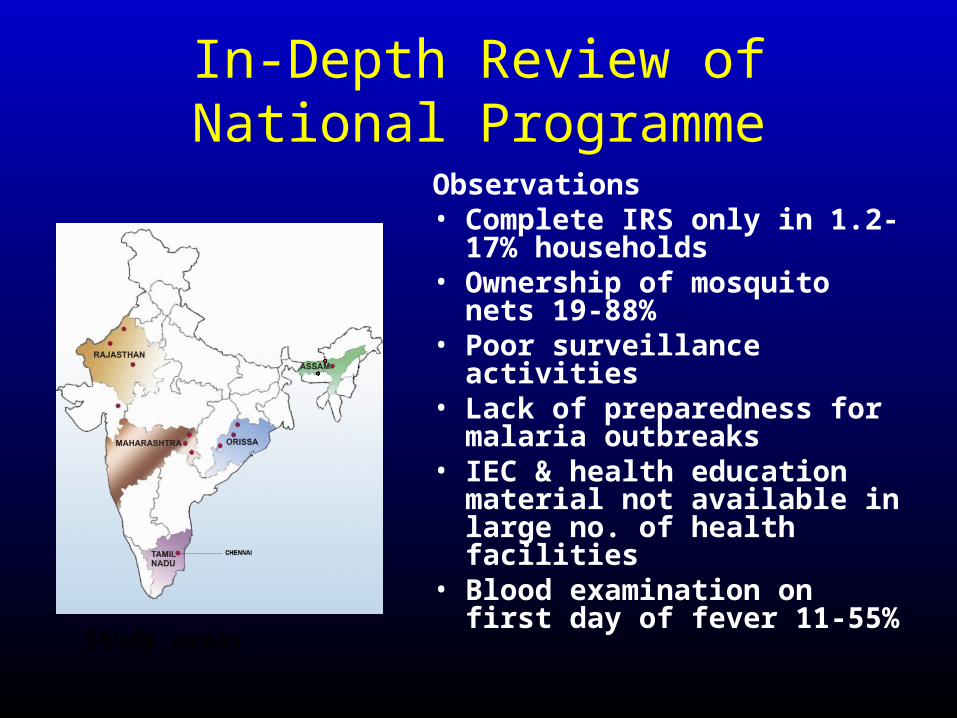
In-Depth Review of National Programme
Observations• Complete IRS only in 1.2-17%
households• Ownership of mosquito nets
19-88%• Poor surveillance activities• Lack of preparedness for
malaria outbreaks• IEC & health education
material not available in large no. of health facilities
• Blood examination on first day of fever 11-55%
Study areas

Recommendations• Actions to improve
vector control • Improvement in
surveillance and epidemic preparedness
• Community information and mobilization
• Review of constraints in diagnosis and treatment through policy development
Conclusions
• Knowledge about new drug policy and treatment guidelines inadequate both in public & private sectors
• AS monotherapy available & prescribed at all levels
• Irrational practices– Antimalarials prescribed even in confirmed negative
cases– Injectables used for uncomplicated malaria– Concomitant use of injectable Artesunate & Quinine
in severe malaria– Use of Mefloquine/AS in vivax malaria– Incorrect dosing (even in tertiary care level)

Recommendations
• Increasing awareness– Persistent & repeated
effort required through various forums
– Short messages / treatment guidelines to be distributed through periodicals
• Making prescribed treatment available (ACTs)
NIMR-IMA workshop on Malaria & Dengue: September 17, 2008

Thank you