1362397148 intensive insulin therapy for managing diabetic foot
25
Intensive insulin Intensive insulin therapy for therapy for managing diabetic managing diabetic foot foot Dr. Bipin Kumar Sethi Dr. Bipin Kumar Sethi
-
Upload
dfsimedia -
Category
Health & Medicine
-
view
151 -
download
1
Transcript of 1362397148 intensive insulin therapy for managing diabetic foot

Intensive insulin Intensive insulin therapy for therapy for
managing diabetic managing diabetic footfoot
Dr. Bipin Kumar SethiDr. Bipin Kumar Sethi

Intensified insulin Intensified insulin therapy ..mythstherapy ..myths
Costly !Costly ! Not for this patient ! Not for this patient ! Not yet ..not so soon !Not yet ..not so soon ! Why this headache?Why this headache? Why another specialist ?Why another specialist ? Patient won’t accept !Patient won’t accept !

Glycemic control is one of the important facets Glycemic control is one of the important facets of management of diabetic foot & is of management of diabetic foot & is complimentary to the general care, complimentary to the general care, antimicrobial therapy and surgeryantimicrobial therapy and surgery
Most hospitalised patients require insulin and Most hospitalised patients require insulin and the regimens depend uponthe regimens depend upon Route of nutritional delivery/sensoriumRoute of nutritional delivery/sensorium Hemodynamic statusHemodynamic status Co-morbid conditions esp. hepatic and renal Co-morbid conditions esp. hepatic and renal
insufficiencyinsufficiency Monitoring facilitiesMonitoring facilities Degree of hyperglycemia/ decompensationDegree of hyperglycemia/ decompensation
Hyperglycemia in a hemodynamically stable Hyperglycemia in a hemodynamically stable patient should not be a deterrent to delivery of patient should not be a deterrent to delivery of adequate foot care (debridement, desloughing, adequate foot care (debridement, desloughing, amputation)amputation)

Why does glycemic control Why does glycemic control worsen ?worsen ?
Never checked before – natural Never checked before – natural coursecourse
RecumbencyRecumbency InfectionInfection DietDiet Drugs- steroidsDrugs- steroids Hospital “schedules/protocols”Hospital “schedules/protocols” StressStress

Benefits of intensified Benefits of intensified insulin regimensinsulin regimens
Quick(er) metabolic controlQuick(er) metabolic control Anabolic effectAnabolic effect Better insulinisationBetter insulinisation
Lesser mismatchLesser mismatch Lesser hyposLesser hypos
OthersOthers

For patients taking For patients taking nutrients orallynutrients orally
MSIMSI R + R + R + Basal (N/L/G/D)R + R + R + Basal (N/L/G/D) S + S + S + Basal (N/L/G/D)S + S + S + Basal (N/L/G/D) Premixed + S/R + PremixedPremixed + S/R + Premixed

International Diabetes CenterInternational Diabetes Center
Rel
ativ
e In
sulin
Effe
ctR
elat
ive
Insu
lin E
ffect
Time (Hours)Time (Hours)
0 2 4 6 8 10 12 14 16
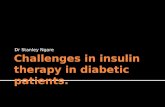
Long (Glargine)Long (Glargine)
18 20
Intermediate (NPH)Intermediate (NPH)Short (Regular)Short (Regular)
Rapid (Lispro, Aspart)Rapid (Lispro, Aspart)
Insulin Time Action Curves

220220
Blo
od s
ugar
B
lood
sug
ar
(mg%
)(m
g%)
210210
200200
180180
160160
140140
6 am6 am 12 noon12 noon 6 pm6 pm 12 midnight12 midnight 5 am5 am
BreakfastBreakfast LunchLunch DinnerDinner
INSULIN
Biphasic Rapid insulin Monophasic
Blood sugar :Blood sugar :
Multiple Daily Insulin InjectionsMultiple Daily Insulin Injections

International Diabetes CenterInternational Diabetes Center
RA RA RA
Physiologic Insulin S/R – S/R – S/R– G/D/N
Seru
m in
sulin
(mU
/L)
Hours
S/R S/R S/R G/D/N
Glargine0
10
20
30
40
50
0 2 4 6 8 10 12 14 16 18 20 22 24

For patients not taking For patients not taking nutrients orallynutrients orally
Insulin infusionInsulin infusion GIKGIK Non GIKNon GIK
1.1. Infusion pumpInfusion pump2.2. NeutralisedNeutralised3.3. Pediatric dripPediatric drip

Short term NBM requiring Short term NBM requiring procedureprocedure
Insulin + Dextrose infusionInsulin + Dextrose infusion GIKGIK Non GIKNon GIK

AlgorithmsAlgorithms1.1. Guidelines rather than sacrosanct Guidelines rather than sacrosanct
rulesrules2.2. Go by antecedent responses, Go by antecedent responses,
memory and current blood glucose memory and current blood glucose 3.3. Revise if response is suboptimalRevise if response is suboptimal
Target BG 80-110mg/dlMonitoring key to successDon’t leave it to paramedics

Team approachTeam approach Not just numbers but interacting Not just numbers but interacting
dedicated membersdedicated members Flexibility to change regimensFlexibility to change regimens Monitoring, record keepingMonitoring, record keeping

A chain is as strong as its A chain is as strong as its weakest linkweakest link
AnonymousAnonymous

Case scenarioCase scenario Mr. MRLS, 55yMr. MRLS, 55y T2DM 10y, Gliclazide + Mixtard 30 & T2DM 10y, Gliclazide + Mixtard 30 &
20 units20 units HTNHTN No CVA, PVDNo CVA, PVD CAD ?CAD ? Cataract bilaterallyCataract bilaterally Neuropathy +, PVD +Neuropathy +, PVD + Admitted on 31.3.04Admitted on 31.3.04

Foot infection on left side for 2 months, Foot infection on left side for 2 months, ulcer is located below the left great toe, ulcer is located below the left great toe, redness, edema and tenderness extending redness, edema and tenderness extending up to forefoot.up to forefoot.
Disarticulation of 2Disarticulation of 2ndnd toe with wide local toe with wide local excision done on 9.4.04excision done on 9.4.04
Continued to be febrile and hyperglycemicContinued to be febrile and hyperglycemic Wound remained unhealthy despite radical Wound remained unhealthy despite radical
excision of all sloughexcision of all slough 15.4.04 endocrinology consultation taken, 15.4.04 endocrinology consultation taken,
started on MSI with A20,20,20; M26unitsstarted on MSI with A20,20,20; M26units

DateDate FPGFPG PPGPPG RapidRapid BasalBasal MixMix15.4.15.4.0404
293293 364364 20,20,220,20,200
2626
16.4.16.4.0404
160160 28,28,228,28,288
16,3016,30
18.4.18.4.0404
314314 384384 20,20,220,20,244
2626
19.4.19.4.0404
176176 226226 24,24,224,24,244
24,2424,24
20.4.20.4.0404
5454 136136 15,15,115,15,155
1515
21.4.21.4.0404
183183 16,16,116,16,166
1818
25.4.25.4.0404
7878 186186 24,224,244

Mid tarsal amputation done on 17.4.04, as his oral Mid tarsal amputation done on 17.4.04, as his oral intake remained very poor after surgery he was intake remained very poor after surgery he was given infusion of DNS with added insulingiven infusion of DNS with added insulin
He experienced hypoglycemia on 20.4.04He experienced hypoglycemia on 20.4.04 Below knee amputation on 4.5.04Below knee amputation on 4.5.04 Post surgery intake remained poor and had vomitingPost surgery intake remained poor and had vomiting Surgery team would change to insulin as per sliding Surgery team would change to insulin as per sliding
scale, insulin would be stopped altogether whenever scale, insulin would be stopped altogether whenever hypos occurredhypos occurred
Parenteral nutrition was also given with no provision Parenteral nutrition was also given with no provision of insulinof insulin
Altered sensorium with hypotension on 11.5.04Altered sensorium with hypotension on 11.5.04

DateDate FPGFPG PPGPPG RapidRapid BasalBasal CommenCommentsts
5.5.05.5.044
203203 264264 10,10,10,10,1010
1010
7.5.07.5.044
078078 114114 8,8,88,8,8 88
8.5.08.5.044
123123 212212 12,1212,12 Nil Nil orallyorally
9.5.09.5.044
253253 324324 12,12,12,12,1212
1212
10.5.10.5.0404
243243 16,16,16,16,1616
1616
11.5.11.5.0404
65,665,633
9696

DateDate FPGFPG PPGPPG RapidRapid BasalBasal Pre Pre MixeMixedd
15.5.15.5.0404
134134 184184 10,10,10,10,1010
1010
19.5.19.5.0404
111111 161161 15,15,15,15,1515
1515
24.5.24.5.0404
7474 101101 35,235,255

Hyponatremia (Na112),Hypokalemia Hyponatremia (Na112),Hypokalemia (K 2.8) Hypotension 90/50 mmHg, (K 2.8) Hypotension 90/50 mmHg, Pyrexia, Metabolic alkalosisPyrexia, Metabolic alkalosis
Blood culture grew Blood culture grew Klebsiella,Enteococcus speciesKlebsiella,Enteococcus species
Was managed in AMC, received IV Was managed in AMC, received IV insulin infusion insulin infusion
Discharged on 25.5.04 !Discharged on 25.5.04 !

Intensified insulin regimens work but are Intensified insulin regimens work but are introduced rather lateintroduced rather late
Insulin requirements fluctuate but hypos Insulin requirements fluctuate but hypos should not deter from achieving the goalshould not deter from achieving the goal
Shifting from oral to parenteral nutrition does Shifting from oral to parenteral nutrition does occurs and needs closer monitoring and occurs and needs closer monitoring and better insulinisationbetter insulinisation
Unplanned procedures often result in Unplanned procedures often result in interruption of insulininterruption of insulin
At all times provide for nutrient/fluid and insulinAt all times provide for nutrient/fluid and insulin

SummarySummary Most patients with diabetic foot ulcers have Most patients with diabetic foot ulcers have
significant hyperglycemia necessitating insulin significant hyperglycemia necessitating insulin therapytherapy
Glycemic control is an important though not the Glycemic control is an important though not the only management tool in the care of diabetic foot only management tool in the care of diabetic foot ulcers ,sadly it is often neglected ulcers ,sadly it is often neglected
Regimens for glycemic control vary among other Regimens for glycemic control vary among other things with the severity of things with the severity of hyperglycemia ,monitoring facilities, co-morbid hyperglycemia ,monitoring facilities, co-morbid conditions but are driven largely by the enthusiasm conditions but are driven largely by the enthusiasm for euglycemia of treating team and must ensure for euglycemia of treating team and must ensure continuity of insulin therapycontinuity of insulin therapy
Admission for diabetic foot offers an opportunity Admission for diabetic foot offers an opportunity for salvaging/protecting the individual against for salvaging/protecting the individual against further ravages of micro/macrovascular diseasefurther ravages of micro/macrovascular disease

AcknowledgementAcknowledgement

Thanks…if at Thanks…if at all you could all you could
keep awake!!keep awake!!