13377834 absorption-final
29
ABSORPTION OF DRUG Submitted To Dr. Santa Raj Joshi Department of Pharmacy School of Science Kathmandu University Submitted By Feb 2008 Table of Content Anana Sharmat Deep Piyati Yasodha Manandhar M Pharm, 1 st Sem M Pharm, 1 st Sem M Pharm, 1 st Sem Roll No. 070019 Roll No. Roll No.000
-
Upload
debasish-bhattacharjee -
Category
Health & Medicine
-
view
164 -
download
0
Transcript of 13377834 absorption-final

ABSORPTION OF DRUG
Submitted ToDr. Santa Raj Joshi
Department of Pharmacy
School of ScienceKathmandu University
Submitted By
Feb 2008
Table of Content
Anana Sharmat Deep Piyati Yasodha Manandhar M Pharm, 1st Sem M Pharm, 1st Sem M Pharm, 1st SemRoll No. 070019 Roll No. Roll No.000


1. Introduction
Drug absorption is defined as the process of movement of unchanged drug from the site of
administration to systemic circulation.
Most of the drugs produce their effects only after they have entered into the bloodstream.
The rapidity of absorption and site of absorption depend on chemical and physical
properties of the drug. The rate of absorption affects the duration and intensity of the drug
action.
There always exist a correlation between the plasma concentration of a drug and the
therapeutic response and thus the absorption can also be defined as the process of
movement of unchanged drug from the site of administration to the site of measurement i.e.
plasma.
A drug that is completely but slowly absorbed may fail to show therapeutic response as the
plasma concentration for desired effect is never achieved. On the contrary, a rapidly
absorbed drug attains the therapeutic level easily to elicit pharmacological effect, thus both
the rate and the extent of drug absorption are important. Such an absorption pattern has
several advantages:
1. Lesser susceptibility of the drug for degradation or interaction due to rapid
absorption.
2. Higher blood levels and rapid onset of action.
3. More uniform, greater and reproducible therapeutic response.
1

2. Methods of absorption
2.1 Oral absorption
After oral administration, absorption of drugs may occur at various body sites between the
mouth and the rectum. In general, the higher is the absorption of drug along the length of
the alimentary tract, the more rapid will be its action. However, because of drug substances
differ in their chemical and physical properties and in the forms in which they are
represented to the body a given drug may be better absorbed from the environment of one
position than from that of another. Physically the oral absorption of drug is managed by
allowing the drug substances to be dissolved and withheld in the oral cavity. Drugs capable
of being absorbed in the mouth may be in concentrated form because they are further
diluted with gastrointestinal fluids in the alimentary tract .Many drugs like nitroglycerine,
sex hormones, morphine, glycerylnitate have been shown to be absorbed faster in
sublingual administration than when swallowed. Drugs which are absorbed through the
buccal mucosa enter the systematic circulation directly and are distributed to the whole
body without passing through the liver fast.
2.2 Rectal absorption
The rectum and t he colon are capable of absorbing many soluble drugs intended for
systemic action. Also, drugs absorbed rectally donot pass through the liver prior to their
entry into the systemic circulation .However rectal absorption is often irregular and
incomplete and therefore many drugs cause irritation of the rectal mucosa.
2.3Parentral absorption
The parentral route is preferred when rapid absorption is desired as in emergency.
Absorption by the parentral route is faster than oral administration and the blood level of
drug that result are is certain because little is lost after subcutaneous or intramuscular
injections. Therefore, subcutaneous or intramuscular injections make sure that the desired
dose of the drug is within the tissues of the body where it is capable of being absorbed into
the circulation. However, such an injection may prove at times failure to ensure rapid or
predictable absorption. If rapid, predictable drug delivery into the circulations is required,
2

the intravenous administration is preferable. However, the rate of absorption by parentral
route depends on the blood flow.
2.4 Absorption of drugs through the skin
Drugs are usually applied to the skin for their local actions. Absorption through the skin is
inefficient and variable when systemic actions are required. Drug entry may take place
more easily through the cells lining sweat, sebacious glands, hair follicles and other
anatomic structured of the skin surface. Since blood capillaries are present just below the
epidermal cells, a drug that penetrates the skin is able to traverse the capillary finds ready
access to the general circulation. The rate of absorption of a drug through the skin to some
extent is determined by the site of the skin as well.
2.5Absorption through the respiratory tact
Gaseous and volatile drugs may be inhaled and absorbed through the pulmonary epithelium
and mucosa membrane of the respiratory tract. Here, the access of the drug to the
circulation is rapid because the surface area is large. However, the rate of absorption
depends on the size of the particles of the drug. The size largely determines the depth to
which the particles penetrate the alveolar region, their solubility potential, and the extent to
which they are absorbed. After they come into contact with inner surface of the lungs,
insoluble drug particles are caught in the mucus. Soluble drug particles that are
approximately 0.5 to 1.0 micron in size reach the minute alveolar sacs. They are most
prompt and efficient in providing systemic effects.
3

3. Mechanism of drug absorption
The principal mechanisms for transport of drug molecules across the cell membrane are:
1. Passive diffusion
2. Pore transport
3. Facilitated diffusion
4. Active transport
5. Ionic or electrochemical diffusion
6. Ion pair transport
7. Endocytosis
3.1 Passive diffusion
It is also called non-ionic diffusion. The driving force for this process is the
electrochemical gradient. It is defined as the difference in the drug concentration on either
side of the membrane. Since no energy is required, the process is called as passive
diffusion.
Passive diffusion is best expressed by Fick’s first law of diffusion, which states that the
drug molecules diffuse from a region of higher concentration to one of lower concentration
until equilibrium is attained and that the rate of diffusions directly proportional to the
concentration gradient across the membrane.
Mathematically,
[da/dt =DcPcS dc/dx]
Where,
Dc is the diffusion coefficient of the drug through the membrane
Pc if the partition coefficient between membrane and the donor medium containing drug
S is the membrane surface area
And dc & dx are concentration differential across the membrane & membrane thickness
respectively.
4

In actual practice concentration on the receptor side of the membrane are low because of
continuous blood flow. Thus when the concentration onto donor side is relatively high,
above equation can be changed to ;da/dt=PmSc
Where c=drug concentration at absorption site & Pm =permeability constant
Pm =DcPc/dx
For the solid dosage forms drug concentration at the absorption site is a function of the
dissolution rate of the drug in the medium at that site
The dissolution is given by the Nayes Whitney equation, dc/dt=Dc S/h (Cs-C)
Where,
C =concentration at time t
Dc=diffusion coefficient of drug in the medium
S =surface area of drug particles
h=thickness of diffusion layer surrounding the particles
Cs=solubility of drug in the diffusion layer
3.2 Pore transport
It is also called as convective transport, bulk flow or filtration. The process is important in
absorption of low molecular weight, low molecular size and water-soluble drug through
narrow, aqueous field channels or pores in the membrane structure e.g. urea, water and
sugar. The driving force is constituted by the hydrostatic pressure or the osmotic
differences across the membrane. Water flux that promotes such a transport is called as
solvent drag.
3.3 Carrier mediated transport
The mechanism is thought to involve a component of the membrane called as the carrier
that binds reversibly or noncovalently with the solute molecules to be transported. This
carrier solute complex traverses across the membrane to the other side where it dissociates
and discharges the solute molecule. The carrier may be an enzyme or some other
component of the membrane.
Important characteristic of carrier mediated transport:
• The transport process is structure specific.
5

• Drug having similar to essential nutrient called as false nutrients are absorbed by
the same carrier system.
• There is competition between agents having similar structure.
• A drug absorbed by passive diffusion ,the rate of absorption increases linearly with
the concentration but in the case of carrier mediated processes the drug absorption
increases linearly with concentration until the carriers become saturated after which
it becomes curvilinear and approach a constant value at higher doses. Such a
capacity limits process can be adequately described by mixed order kinetics. Such a
system decrease with increasing dose e.g. vitamins like B1, B2 & B12. Hence, the
administration of a large single oral dose of such vitamins is irrational.
• Occurs from specific sites of the intestinal tract, which are rich in number of
carriers known as absorption window.
Two types of carrier mediated transport systems have been identified, they are
• Facilitated diffusion
• Active transport
Facilitated diffusion:
• It operates down the concentration gradient (downhill transport), driving
force is concentration gradient. E.g. entry of glucose into RBCs and
intestinal absorption of vitamins B1 & B2.
Active transport:
• Drug is transported from a region of lower to higher concentration i.e.
against the concentration gradient or uphill transport.
• Energy is required
• Can be inhibited by metabolic poisons that interfere with energy production
like fluorides, cyanide & lack of oxygen etc.
6

3.4 Ionic or electrochemical diffusion
The charge in the membrane influences the permeation of drugs. Of the ionic forms, the
anionic solute permeates faster than the cationic form. Thus at a given pH the rate of
permeation is in the following order-
unionized molecules> anions>cations.
The cationic drugs depend on the potential difference or electrical gradient as the driving
force across the membrane. A cationic drug is repelled due to positive charge on the outside
of the membrane. As a result, only those cations with a high kinetic energy penetrate the
ionic barrier, however, once inside the membrane, the cations are attracted to negatively
charged intracellular
membrane thereby creating an electrical gradient. Such a drug is then said to be moving
downhill with electrical g radiant and the phenomena is called a electrochemical diffusion.
3.5 Ion –pair transport
Absorption of drug like ammonium compounds & sulfonic acids, which ionize under all
pH condition, is ion pair transport.
3.6 Endocytosis
It involves engulfing extra cellular materials with in a segment of the cell membrane to
form a saccule or a vesicle, which is then pinched off intracellularly.
This phenomenon is responsible for the cellular uptake of macromolecular nutrient like fat,
starch vit A, D, E, K & insulin.
This includes two types of processes:
Phagocytosis; adsorptive uptake of solid particulates &
Pinocytosis; uptake of fluid solute
Sometime endocytic vesicle is transferred from one extra cellular compartment to another;
such phenomenon is called as transcytosis.
7

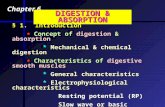
Fig.1: Summary of various means of transport processes and drug absorption through them
4. Factors affecting bioavailability8

To achieve the desired therapeutic objective the drug product must deliver the active drug
at an optimal rate & amount. The process consists of four steps:
1. Disintegration of the drug product.
2. Deaggregation & subsequent release of the drug.
3. Dissolution of the drug in the aqueous fluids at the absorption site.
4. Movement of the dissolved drug through the GI membrane into the systemic
circulation and away from the absorption site.
The rate at which the drug reaches the systemic circulation is determined by the slowest of
the various steps involved in the sequence. Such a step is called as rate determining or rate
limiting step.
Fig.2: Schematic representation of sequences of drug absorption from a tablet dosage form
5. Factors influencing absorption of drug
5.1Biological factors
9

5.2Physicochemical factors
5.3Formulation factors
5.4Patient Related factors
5.1Biological factors
Biological factors are considered to be related to the system in which the drug is absorbed
.Some of the biological factors influencing the absorption rate of drugs are
5.1.1Anotomy of gastrointestinal tract
The gastrointestinal tract is composed of the stomach, small intestine and large intestine or
colon. Although the entire gastrointestinal tract is qualitatively identical, the biological
environment and surface area available for absorption of drugs differ from one end to
another.
Because of the highly convulated surface of its mucusa and villia, the small intestine has
enormous area i.e. 30 times larger than that of the large intestine. It is with blood enough to
carry away tha absorbed material. The small intestine serves as the major absorption
pathway because it has suitable PH and a large surface area approximately 20 feet long
extending from the pylorus at the base of the stomach to the junction with the large
intestine at the cecum.
5.1.2 Gastric motility
Since from the intestines most drugs are absorbed more effectively than that from the
stomach, it is generally desirable to have the drug pass from the stomach into the intestine
as rapidly as possible. Therefore, the gastric emptying time is an important factor in drug
action dependent upon intestinal absorption. A delayed gastric emptying would naturally
delay the absorption of drugs resulting ultimately in the delay the drug action. The gastric
emptying rate also influences the absorption of drugs that are not stable in stomach
example benzyl penicillin. The rate of emptying from the stomach is to be proportional to
the volume of the material present.
Gastric emptying time may be increased by a number of factors as
• The Presence of fatty foods.
10

• Position of the body.
• The presence of drugs like morphine that have a qeuting effect on the movements of
the gastrointestinal tract.
• Temperature and viscosity of the meals and their contents. Liquid of lower viscosity
are emptied faster than those of higher viscosity are.
• Similarly, the social status and mental state of the individual may also influence the
gastric emptying rate.
The peristaltic movements of the intestine help to dissolve the drug in intestinal fluid
and bring the drug into intimate contact with a large surface of mucosal surface. Thus
causing increases in absorption.
5.1.3 Gastro intestinal PH
The PH of the gastrointestinal tract increases progressively along its length from a PH of
about 1 in the stomach to approximately a PH of 8 at the far end of the intestines. The
acidity or alkalinity of the gastrointestinal fluids can influence absorption of drugs in the
form of weak organic acids or bases. As a rule, weak acids are largely unionized in the
stomach and are absorbed fairly well from the site whereas weak bases are highly ionized
in the stomach and are not significantly absorbed from the gastric surface. Similarly weakly
basic drugs are rapidly absorbed from the intestines because of the alkaline PH.Srong acids
and bases are generally poorly absorbed on account of their high degree of ionization.
The small intestine acts as the major absorption area for drugs because of its suitable
PH.The PH of the lumen of the intestine is about 6.5 and both weakly acidic and weakly
basic drugs are well absorbed from the intestinal surface. The PH however does not
influence the absorption of drugs that are actively transported through the gastrointestinal
walls.
5.1.4 Blood flow
The carriage of drug in circulation of blood to the site also affects drug absorption
.Increased in blood flow caused by massage or local application of heat enhances
absorption. Decrease in blood blood flow caused by vasoconstrictor agents, shock or other
disease factors can slow down absorption.
11

5.1.5 Interaction between drugs and gastrointestinal tract components
Drugs may be altered within the gastrointestinal tract into forms that render them less or
more slowly available for absorption. This alteration may be of the result of the association
of the drug with gastrointestinal constituents, foodstuffs are another drugs. The absorption
of teracyclines group of antibiotics is greatly interfered by the presence of calcium. Various
kinds of protein reduce the activity of aluminium antacids by complexation.Bile salts being
surface active enhance dissolution of sparingly soluble drugs thereby promoting their
absorption. Enzymes have been shown to react with drugs in a number of ways, viz.
Removal of acetyl groups from N-acylated compounds.
Transformation of ester compounds into parent compounds by esterase.
Conversion of chloramphenicol palmitate to chloramphenicol by the pancreatic enzyme.
5.1.6 Presence of foods
The presence of food in the stomach generally delays absorption of drug. The food content
of the stomach tends to over dilute the drug concentration and decrease absorption. The
absorption of teracyclines has shown to be markedly reduced in the presence of milk, milk
products. Therefore, tetracycline drugs must not be taken with milk or other calcium
containing food or drug. Although most drugs are absorbed faster and to a greater extent if
taken into stomach, certain drugs that are irritating to the gastrointestinal tract are
frequently administered with meals to reduce their concentration and irritant action. For
instance, absorption of griseofulvin is enhanced nearly 200 percent by fatty meal. Many
drugs e.g. the analgesic paracetamol and the urinary antibacterial agent nitrofurantoin are
absorbed more rapidly if given when patient is fasting than if given after a meal.
5.2Physicochemical factors
The physiochemical factors that significantly influence the absorption are
12

5.2.1 Disintegration and Dissolution
In order for a drug to be absorbed, it must get dissolved in body at the absorption sitse.A
drug taken orally in tablet or capsule form cannot be absorbed until its particles are
solubalized by the fluids at the same point in gastrointestinal tract. When a tablet or capsule
is swallowed, it enters the stomach through oesophagus.Break of tablets into particles is
called disintegration and the time required to complete this process is called disintegration
time. It should be less than 15 minutes for compressed tablets and 60 minutes for coated
tablets. The process by which drug particles dissolve after disintegration is termed
dissolution and the time required for the dissolution of 70 % of the drug is called
dissolution time. Tablet must thus disintegrate and their contents dissolve in gastrointestinal
fluids before they are absorbed from the intestinal wall.
By its solubility in an acidic or basic medium, the drug is solubalized in the stomach and
intestine. Drugs that disintegrate within a specified time may not dissolve adequately in the
fluids. The dissolution rate changes by increase in temperature, agitation and surface
enhances the dissolution rate. The chemical or physical form a drug also enhances the rate
of dissolution.
Sometimes the dissolution of a drug particle is slow. Owing to the physico chemical
characteristics of the drug substance or the dosage form, the dissolution process itself
would be a rate-limiting factor in the absorption process .Some slow soluble drugs may be
incompletely absorbed and some may even remain unabsorbed in the stomach or intestinal
tract after oral administration because of natural time limit. Thus incompletely absorbed or
unabsorbed drug particles are excreted unchanged out of the system.
5.2.2 Drug stability in gastrointestinal tract
Gastro intestinal fluids contain various enzymes and provide a highly reactive media. In
degradation of drug molecules in the gastric fluids, hydrolytic decomposition is most
commonly observed. Penicillin G and insulin are inactivated by this reaction.
5.2.3 Complex formation
13

Some drugs may form a complex materials in the gastrointestinal tract.Complexatation
usually slows down the dissolution rate because drug molecules are bound. The rate of
dissolution in such cases is dependent on the rate of release of drug molecules from the
complex.
5.2.4 Viscosity
The viscosity of a suspension will influence the dissolution rate of a drug in body fluids.
The more viscous the suspension, the lesser is the rate of dissolution because viscosity
reduces the diffusion rate.
5.2.5 Surfactants
Surfactants reduce interfacial tension between drug particles and the solvent causing them
to come in contact with each other. The increased contact increases the dissolution rate.
Moreover, some surfactants form micelles that help to solubalize some lipophilic
components.
5.2.6 Drug Concentration
The concentration of a drug influences its rate of absorption .Drugs in solution of high
concentration are absorbed more rapidly than the drugs in solutions of low concentration.
Thus, the absorption rate is propotional to concentration of drug.
5.3Formulation factors
14

5.3.1 Dosage form
The dosage of a drug may be in tablet, capsule, mixture, suspension or injection form. The
tablet or capsule form should disintegrate or dissolve prior to absorption. Therefore, its
action is slow compared to the action of any other dosage form. A drug administered in the
form of solution e.g. syrup or an elixir passes into the intestines more rapidly because it
does not have to disintegrate and dissolve.Similarly, suspensions and emulsions contain
drugs in undissolved form. Therefore, they need to be dissolve before absorption. Injections
administered intramuscularly or intradermally have to be absorbed before they pass into the
blood stream. Intravenous injection, which is administered directly into bloodstream so
they shows rapid effect.
Thus, prompt action is observed with parentral dosage forms (injections), intermediate
action with liquids (solution, suspensions) and slow with tablets and capsules
5.3.2 Excipients
Drugs are generally modified into convenient dosage form to ensure acceptability,
physicochemical stability during the shelf life, uniformity of composition and dosage, and
optimum bioavailability and function ability of the drug product and are then administered
by a suitable route. Such modification contains inclusion of a number of excipients (non-
drug components of a formulation). Despite their inertness and utility in the dosage form,
excipients can influence absorption of drugs as the number of excipients is increased in a
dosage form, more complex it becomes and greater will be the potential for absorption and
bioavailability problems. Commonly used excipients in various dosage forms are vehicles,
diluents (fillers), binders and granulating agents, disintegrants, lubricants, coatings,
suspending agents, emulsifiers, surfactants, buffers, complexing agents, colorants,
sweeteners, crystal growth inhibitors, etc.
Vehicle
Vehicle or solvent system is the major component of liquid orals and parenterals. The three
categories of vehicles in use are—aqueous vehicles (water, syrup, etc.), nonaqueous water
miscible vehicles (propylene glycol, glycerol, sorbitol) and nonaqueous water immiscible
vehicles (vegetable oils).
15

1. Miscibility: Bioavailability of a drug from vehicles depends to a large extent on its
miscibility with biological fluids. Aqueous and water miscible vehicles are miscible
with the body fluids and drugs from them are rapidly absorbed. Quite often, a drug
is more soluble in water miscible vehicles like propylene glycol (serving as a co-
solvent) and show better bioavailability. Sometimes dilution of such vehicles with
the body fluids results in precipitation of drug as fine particles which, however,
dissolve rapidly.
2. Solubilizers: such as tween 80 are sometimes used to promote solubility of a drug in
aqueous vehicles.
3. Partitioning: In case of water immiscible vehicles, the rate of drug absorption
depends upon its partitioning from the oil phase to the aqueous body fluids, which
could be a rate-limiting step.
4. Viscosity: of the vehicles is another factor in the absorption of drugs. Diffusion into
the bulk of GI fluids and thus absorption of a drug from a viscous vehicle may be
slower.
Diluents (Fillers)
Diluents are commonly added to tablet (and capsule) formulations if the required dose is
inadequate to produce the necessary bulk. A diluent may be organic or inorganic. Among
organic diluents, carbohydrates are very widely used—for example, starch, lactose,
microcrystalline cellulose, etc.
1. Hydrophilic powders are very useful in promoting the dissolution of poorly water-
soluble, hydrophobic drugs like spironolactone and triamterene by forming a coat
onto the hydrophobic surface of drug particles and rendering them hydrophilic.
2. Drug-diluent interaction can occur resulting in poor bioavailability for example
tetracycline and DCP. The cause is formation of divalent calcium-tetracycline
complex which is poorly soluble and thus, un-absorbable.
16

Binders and Granulating Agents
These materials are used to hold powders together to form granules or promote cohesive
compacts for directly compressible materials and to ensure that the tablet remains intact
after compression. Popular binders include polymeric materials (natural, semi synthetic and
synthetic) like starch, cellulose derivatives, acacia, PVP, etc. Others include gelatin and
sugar solution. In general, like fillers, the hydrophilic (aqueous) binders show better
dissolution profile with poorly
Wettable drugs like phenacetin by imparting hydrophilic properties to the granule surface.
However, the proportion of strong binders in the tablet formulation is very critical. Large
amounts of such binders increase hardness and decrease disintegration/dissolution rates of
tablets. PEG 6000 was found to be a deleterious binder for phenobarbital as it forms a
poorly soluble complex with the drug. Non-aqueous binders like ethyl cellulose also retard
drug dissolution.
Disintegrants
These agents overcome the cohesive strength of tablet and break them up on contact with
water which is an important prerequisite to tablet dissolution. Almost all the disintegrants
are hydrophilic in nature. A decrease in the amount of disintegrant can significantly lower
bioavailability. Adsorbing disintegrants like bentonite and veegum should be avoided with
low dose drugs like digoxin, alkaloids and steroids since a large amount of dose is
permanently adsorbed and only a fraction is available for absorption. Microcrystalline
cellulose is a very good disintegrant (and a binder too) but at high compression forces, it
may retard drug dissolution.
Lubricants/Antifrictional Agents
These agents are added to tablet terminations to aid flow of granules, to reduce interparticle
friction and sticking or adhesion of particles to dies and punches. The commonly used
lubricants are hydrophobic in nature (several metallic stearates and waxes) and known to
inhibit wettability, penetration of water into tablet and their disintegration and dissolution.
This is because the disintegrant gets coated with the lubricant if blended simultaneously
which however can be prevented by adding the lubricant in the final stage. The best
17

alternative is use of soluble lubricants like SLS and carbowaxes which promote drug
dissolution.
Coatings
In general, the deleterious effect of various coatings on drug dissolution from a tablet
dosage form is in the following order: enteric coat > sugar coat > nonenteric film coat. The
dissolution profile of certain coating materials change on aging; e.g. shellac coated tablets,
on prolonged storage, dissolve more slowly in the intestine. This can, however, be
prevented by incorporating little PVP in the coating formulation.
Suspending Agents/Viscosity Imparters
Suspending agents are hydrophilic polymers like vegetable gums (acacia, tragacanth, etc.),
semisynthetic gums (CMC, MC) and synthetic gums which primarily stabilize the solid
drug particles by reducing their rate of settling through an increase in the viscosity of the
medium. These agents and some sugars are also used as viscosity imparters to affect
palatability and pourability of solution dosage forms. The macromolecular gums often form
unabsorbable complexes with drugs as incase of sodium CMC forming a poorly soluble
complex with Amphetamines or an increase in viscosity acting as a mechanical barrier to
the diffusion of drug from the dosage form into the bulk of GI fluids and from GI fluids to
the mucosal lining by forming a viscid layer on the GI mucosa. Moreover, they also retard
the GI transit time.
Surfactants
They are widely used as wetting agents, solubilizers, emulsifiers, etc in formulations and
may either enhance or retard drug absorption by interacting with the drug or membrane or
both. Mechanisms involved in the increased absorption of drug by use of surfactants
include;
1. Promotion of wetting by increase in effective surface area and dissolution of drugs.
E.g.; Tween 80 with Phenacetin.
2. Better membrane of the drug for absorption.
3. Enhanced membrane permeability of the drug.
18

The beneficial effect at pre-critical micelle concentration levels has also been observed.
However, physiologic surfactants like bile salts and lysolecithin promote absorption of
hydrophobic drugs as such steroids, oil soluble vitamins and Griseofluvin by their micellar
solubilizing property.
Likewise, decreased absorption of drugs due to surfactants is due to;
1. Formation of unabosrbable drug-micelle complex at surfactant concentrations
above critical micelle concentration.
2. Laxative action induced by a large surfactant concentration.
Buffers
Sometimes buffers are useful in creating the right atmosphere for drug dissolution as was
observed for buffered aspirin tablets. However, certain buffer systems containing potassium
cations inhibit the drug absorption as incase of vitamin B2 and sulfanilamide and the reason
attributed to it was the uptake of fluids by the intestinal epithelial cells due to which the
effective drug concentration in the tissue is reduced and the absorption rate is decreased.
Such an inhibitory effect of the various buffer cations on the drug transfer rate is in the
following order: K+ > NH41> Li+ > Na+ > TRIS+. Hence, the buffer system for a salt of a
drug should contain the same cation as the drug salt and introduce no additional cations.
Complexing Agents
Alteration of physicochemical and biopharmaceutical properties of a drug can be achieved
through complex formation. A complexed drug may have altered stability, solubility,
molecular size, partition coefficient and diffusion coefficient. Basically, such complexes are
pharmacologically inert and must dissociate either at the absorption site or following
absorption into the systemic circulation. Several examples where complexation has been
used to enhance drug bioavailability are:
• Enhanced dissolution through formation of a soluble complex e.g. ergotamine
tartarate-caffeine complex and hydroquinone-digoxin complex.
• Enhanced lipophilicity for better membrane permeability e.g. caffeine-PABA
complex.
19

• Enhanced membrane permeability e.g. enhanced GI absorption of heparin (normally
not absorbed from the GIT) in presence of EDTA which chelates calcium and
magnesium ions of the membrane.
Complexation can be deleterious to drug absorption due to formation of poorly soluble or
poorly absorbable complex e.g. complexation of tetracycline with divalent and trivalent
cations like calcium (milk, antacids), iron (hematinics), magnesium (antacids) and
aluminium (antacids). Poor bioavailability results because of some complexes fails to
dissociate at the absorption site and large molecular size of the complex cannot diffuse
through the cell membrane—for example, drug-protein complex.
Colorants
A very low concentration of water-soluble dye can have an inhibitory effect on dissolution
rate of several crystalline drugs. The dye molecules get adsorbed into the crystal faces and
inhibit drug dissolution e.g.; brilliant blue retards dissolution of sulfathiazole. Dyes have
also been found to inhibit micellar solubilization effect of bile acids which may impair the
absorption of hydrophobic drugs like steroids. Cationic dyes are more reactive than the
anionic ones due to their greater power for adsorption on primary particles.
Crystal Growth Inhibitors
The initial physical properties of a drug in suspension can be inhibited by crystal growth
inhibitors like PVP and PEG by conversion of a high energy metastable polymorph into
stable, less soluble polymorph.
Nature and Type of Dosage Form
The proper selection of dosage form of a drug relates to clinical success to a great extent.
For a given drug, a 2 to 5 fold or perhaps more difference could be observed in the oral
bioavailability of a drug depending upon the nature and type of dosage form. Such a
difference is due to the relative rate at which a particular dosage form releases the drug to
the biological fluids and the membrane. The relative rate at which a drug from a dosage
form is presented to the body depends upon the complexity of dosage form. The more
20

complex a dosage form, greater the number of rate-limiting steps and greater the potential
for bioavailability problems.
Fig.3: Course of events that occur following oral administration of various dosage forms
The bioavailability of a drug among various dosage forms decreases in the following order:
Solutions > Emulsions > Suspensions > Capsules > Tablets > Coated Tablets > Enteric
Coated tablets >Sustained Release Products. Thus, absorption of a drug from solution is
21

fastest with least potential for bioavailability problems whereas absorption from a sustained
release product is slowest with greatest bioavailability risk.
Several factors, especially the excipients which influence bioavailability of a drug from its
dosage form are:
Solutions
A drug in a solution (syrups, elixirs, etc.) is most rapidly absorbed since the major rate-
limiting step drug dissolution is absent. Factors that influence bioavailability of a drug from
solution dosage form include the nature of solvent (aqueous, water miscible, etc.),
viscosity, surfactants, solubilizers, stabilizers, etc. Quite often, dilution of a drug in solution
with GI fluids results in precipitation of drug as fine particles which generally dissolve
rapidly. Factors that limit the formulation of a drug in solution form include stability,
solubility, taste, cost of the product, etc.
Emulsions
Emulsion dosage forms have been found to be superior to suspensions in administering
poorly aqueous soluble lipophilic drugs. Emulsion dosage form present a large surface area
of oil to the GIT for absorption of a drug. Scientists have claimed that a drug administered
in oily vehicle (emulsified and solubilized in the GIT by bile salts to form mixed micelles)
can direct the distribution of drug directly into the lymphatic system thereby avoiding the
hepatic portal vein and first-pass metabolism.
Suspensions
The major rate-limiting step in the absorption of a drug from suspension dosage form is
drug dissolution which is generally rapid due to the large surface area of the particles.
Important factors in the bioavailability of a drug from suspensions include particle size,
polymorphism, wetting agents, viscosity of the medium, suspending agents, etc.
Powders
Major factors to be considered in the absorption of a drug from powders are particle size,
polymorphism, wettability, etc.
22

Capsules
Powders and granules are popularly administered in hard gelatin capsules whereas viscous
fluids and oils in soft elastic shells. Factors of importance in case of hard gelatin capsules
include drug particle size, density, polymorphism, intensity of packing and influence of
diluents and excipients. Hydrophilic diluents like lactose improve wettability,
deaggregation and dispersion of poorly aqueous soluble drugs whereas inhibitory effect is
observed with hydrophobic lubricants like magnesium stearate. A hydrophobic drug with a
fine particle size in capsule results in a decrease in porosity of powder bed and thus,
decreased penetrability by the solvent with the result that clumping of particle occurs and
can be overcome by incorporating a large amount of hydrophilic diluent (upto 50%), a
small amount of wetting agent cum lubricant such as SLS (upto 1%) and/or by wet
granulation to convert an impermeable powder bed to the one having good permeability.
Other factors like possible interaction between the drug and the diluent (e.g. tetracycline-
DCP) and between drug and gelatin shell.
Soft elastic capsules as such dissolve faster than hard gelatin capsules and tablets and show
better drug availability from oily solutions, emulsions or suspensions of medicaments
(especially hydrophobic drugs). E.g.; faster dissolution of indoxole (equivalent to that of an
emulsion dosage form) when formulated as soft gel in comparison to hard gelatin capsule
and aqueous suspension. Such poorly soluble drugs can be dissolved in PEG or other
suitable solvent with the aid of surfactants and encapsulated without difficulty. Soft gels are
thus of particular use where the drug dose is low, drug is lipophilic or when oily or lipid
based medicaments are to be administered. A problem with soft gels is the high water
content of the shell (above 20%). This moisture migrates into the shell content and
crystallization of drug occurs during the drying stage resulting in altered drug dissolution
characteristics.
Tablet
Due to the most convenience and cost effective dosage forms compressed tablets are most
widely used. The bioavailability problems with tablets arise from the reduction in the
effective surface area due to granulation and subsequent compression into a dosage form.
23

Since dissolution is most rapid from primary drug particles due to their large surface area,
disintegration of a tablet into granules and subsequent deaggregation of granules into fine
particles is very important. However, incase of coated tablets the coating acts as yet another
barrier which must first dissolve or disrupt to give way to disintegration and dissolution of
tablet. Of the two types of coatings, the film coat, which is thin, dissolves rapidly and does
not significantly affect drug absorption. The sugar coat which though soluble, is generally
tough and takes longer to dissolve however, the sealing coating is generally of shellac type,
which is deleterious and is difficult to coat. Hence, press coated tablets are superior to
sugar coated.
Likewise, Enteric coated tablets targeted to dissolve in alkaline PH of intestine only have
great potential in creating bioavailability problems and may take as long as 2 to 4 hours for
such a tablet to empty from the stomach into the intestine depending upon the meals and
the GI motility. Hence, the pharmacologic response may eventually be delayed by as much
as 6 to 8 hours. The problem of gastric emptying can, however, be overcome by enteric
coating the granules or pellets and presenting them in a capsule or compressing into a
tablet. The thickness during aging of enteric coat is yet another determinant factor in drug
dissolution, hence increasing thickness being more problematic.
Sustained Release Products
Drug release from such products is most unpredictable, the problems ranging from dose
dumping to unsatisfactory or no drug release at all. However, with the development of
newer innovations and technologies, it is becoming increasingly reliable and the results
reproducible with little intersubject variations. A number of changes, especially in the
physicochemical properties of a drug in dosage form, can result due to aging and alterations
in storage conditions which can adversely affect bioavailability. With solution dosage form,
precipitation of drug due to altered solubility, especially due to conversion of metastable
into poorly soluble, stable polymorph can occur during the shelf life of the product.
Changes in particle size distribution have been observed with a number of suspension
dosage forms resulting in decreased rate of drug dissolution and absorption. In case of solid
dosage forms, especially tablets, disintegration and dissolution rates are greatly affected
due to aging and storage conditions. An increase in these parameters of tablets has been
attributed to excipients that harden on storage (e.g. PVP, acacia, etc.) while the decrease is
24

mainly due to softening/crumbling of the binder during storage (e.g. CMC). Changes that
occur during the shelf life of a dosage form may be due to large variations in temperature
and humidity.
5.3.3 Manufacturing Process
Manufacturing processes influence drug dissolution.Processes of such importance in the
manufacture of tablets are
• Method of granulation
• Compression force
The processing factor of importance in the manufacture of capsules that can influence its
dissolution is the intensity of packing of capsule contents.
5.4 Patient related factors
It includes factor relating to the anatomic, physiologic and pathologic caracteristics of the
patient such as
• Age
• Sex
• Disease state
• Body weight
• Food
• Medicines
• Activity and posture
25

6. Conclusion
Thus, absorption may be defined as the movement of active drugs from the administration
site, across biological barriers, into a site where it is measured in the blood. Absorption
affects bioavailability how quickly and how much of a drug reaches its intended (target)
site of action. Factors that affect absorption its bioavailabilty and chemical properties, and
the physiologic characteristics of the person taking the drug vary individually. Physiologic
characteristics that may affect the absorption of drugs taken by mouth include how long the
stomach takes to empty, what the acidity (pH) of the stomach is, and how quickly the drug
is moved through the digestive tract.
A drug product is the actual dosage form of a like tablet, capsule, suppository, transdermal
patch, or solution that consists of the active ingredient and additives as in case of
formulation of tablet which is a mixture of drug and diluents, stabilizers, disintegrants, and
lubricants. The mixture is granulated and compressed into a tablet. The type and amount of
additives and the degree of compression affect how quickly the tablet disintegrates and the
drug is absorbed. Drug manufacturers adjust these variables to optimize absorption.
26

7. References
1. Dr. Shanta Raj Joshi, A Text Book of Pharmaceutics.
2. D.M. Brahmankar and Sunil B.Jaiswal, Biopharmaceutics and Pharmacokinetics A
Treatise.
3. Dr.Javed Ali, Dr R.K.Khar, Dr AlkaAhuja, A Text Book of Biopharmaceuticss
and Pharmacokinetics.
4. J.S Kulkarni, A.P Pawar, V.P Shedbalkar, Biopharmaceutics and Pharmacokinetics.
27