
130 Hobbs Ave., Suite B - wyoleg.govwyoleg.gov/arules/2012/rules/ARR17-034.pdf · 2.10 Previously...
55
Transcript of 130 Hobbs Ave., Suite B - wyoleg.govwyoleg.gov/arules/2012/rules/ARR17-034.pdf · 2.10 Previously...

130 Hobbs Ave., Suite B • Cheyenne, Wyoming 82002 • Phone: 307-777-7601 • FAX: 307-777-3519 • http://nursing.state.wy.us
Statement of Principal Reasons
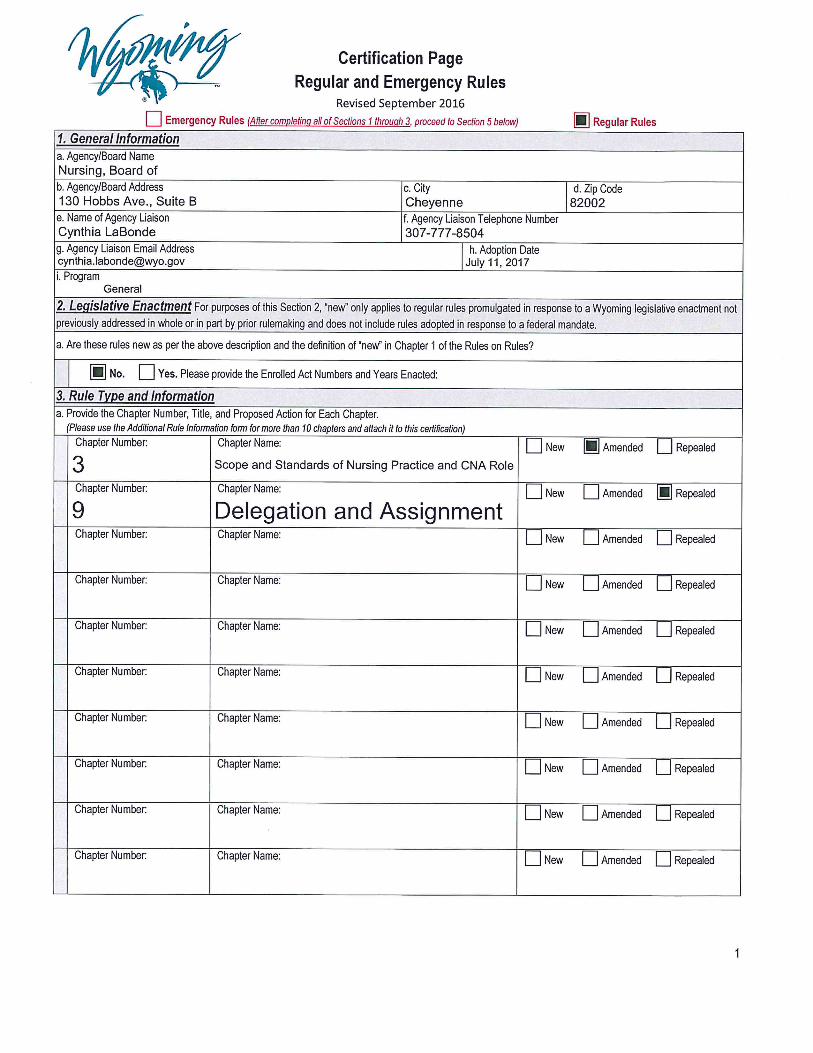
Chapter 3 - Scope and Standards of Nursing Practice and CNA Role
Chapter 9 - Delegation and Assignment
The Wyoming State Board of Nursing is proposing Chapter 3: Scope and Standards of Nursing
Practice and CNA Role, and repeal Rules in Chapter 9: Delegation and Assignment. The
amendments update language in Chapter 3 to reflect the suggested language provided by the
National Council of State Boards of Nursing’s model rules and add relevant language from
Chapter 9. Combining the two chapters is necessary for clarity and to keep the common concepts
in the same chapter. The new language reflects modern processes and standards of the nursing
profession. Enclosed is a “crosswalk” identifying the specific amendments and supporting
documentation or direction for each section. Also included in the crosswalk are the reasoned
references and authoritative sources for the changes.
The major changes to Chapter 3 relate to the Board's authority to regulate the scope and practice
of nursing and provide guidance for APRNs, RNs, LPNs and CNAs via the establishment of
acceptable standards of safe nursing tasks. The proposed language also provides the Board with
criteria to evaluate safe and competent nursing tasks and removes redundancy.
The amendments to Chapter 3 also add language from Chapter 9 relating to the Board’s power to
establish acceptable standards of delegation by defining responsibilities among nursing
professionals. The new language provides the Board with criteria to evaluate safe and competent
delegation of nursing tasks and removes redundancy. Chapter 9 will be repealed in its entirety
and the content integrated into Chapter 3, a more appropriate location for its concepts.
By combining Chapter 3 and Chapter 9, the Board can clarify any ambiguity that may occur
from redundancy and provide succinct and comprehensive regulatory framework. This
amendment promotes a common understanding of what constitutes the practice of nursing and
the process of delegation among nursing professionals.
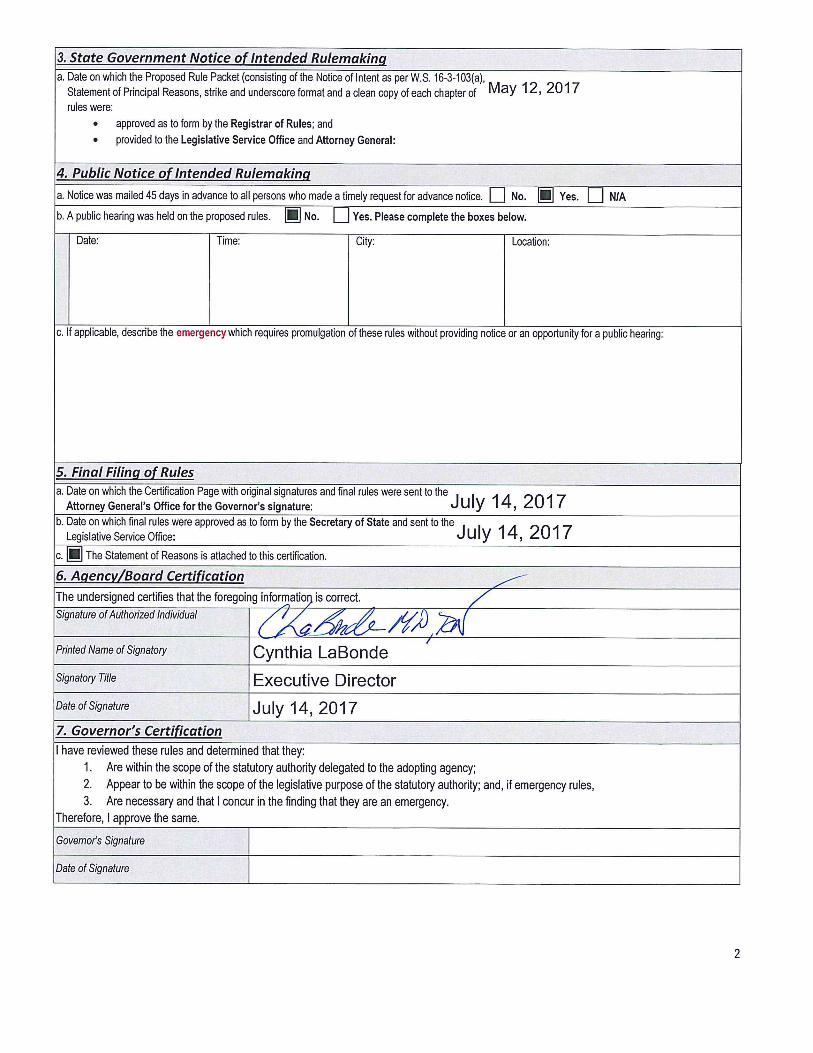
Respectfully submitted,
Cynthia LaBonde MN, RN
Executive Director, WSBN
Matthew H Mead
Governor
Wyoming STATE BOARD OF NURSING
Cynthia LaBonde MN, RN
Executive Director

Page 1 of 1
Wyoming STATE BOARD OF NURSING
Summary of Comments and Responses to proposed revisions to
Chapter 3: Scope and Standards of Nursing Practice and CNA Role
and repeal of Chapter 9: Delegation and Assignment
Licensing base notified by:
o Notice of Intent published in Casper Star Tribune newspaper May 12,
2017.
o Documentation posted on WSBN website May 12, 2017.
Comment period open from May 12, 2017 to June 30, 2017.
o WSBN received NO comments during the comment period.
Matthew H. Mead
Governor
Cynthia LaBonde, MN RN
Executive Director
130 Hobbs Avenue, Suite B • Cheyenne, Wyoming 82002 • Phone: 307-777-7601 • FAX: 307-777-3519 • http://nursing.state.wy.us
Updated 6.3.16 Page 1 of 25
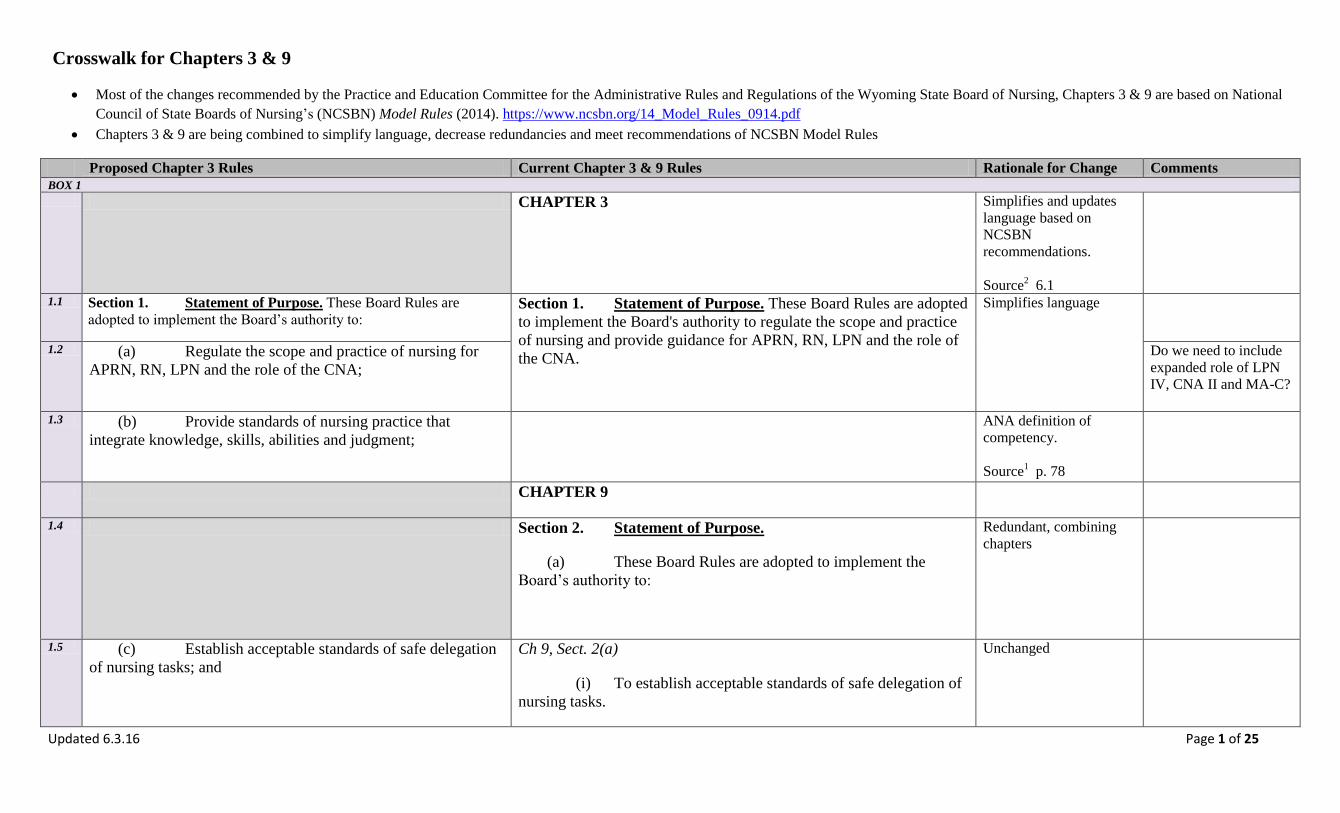
Crosswalk for Chapters 3 & 9
Most of the changes recommended by the Practice and Education Committee for the Administrative Rules and Regulations of the Wyoming State Board of Nursing, Chapters 3 & 9 are based on National
Council of State Boards of Nursing’s (NCSBN) Model Rules (2014). https://www.ncsbn.org/14_Model_Rules_0914.pdf
Chapters 3 & 9 are being combined to simplify language, decrease redundancies and meet recommendations of NCSBN Model Rules
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
BOX 1
CHAPTER 3 Simplifies and updates
language based on
NCSBN
recommendations.
Source2 6.1
1.1 Section 1. Statement of Purpose. These Board Rules are
adopted to implement the Board’s authority to: Section 1. Statement of Purpose. These Board Rules are adopted
to implement the Board's authority to regulate the scope and practice
of nursing and provide guidance for APRN, RN, LPN and the role of
the CNA.
Simplifies language
1.2 (a) Regulate the scope and practice of nursing for
APRN, RN, LPN and the role of the CNA;
Do we need to include
expanded role of LPN
IV, CNA II and MA-C?
1.3 (b) Provide standards of nursing practice that
integrate knowledge, skills, abilities and judgment;
ANA definition of
competency.
Source1 p. 78
CHAPTER 9
1.4 Section 2. Statement of Purpose.
(a) These Board Rules are adopted to implement the
Board’s authority to:
Redundant, combining
chapters
1.5 (c) Establish acceptable standards of safe delegation
of nursing tasks; and
Ch 9, Sect. 2(a)
(i) To establish acceptable standards of safe delegation of
nursing tasks.
Unchanged
Updated 6.3.16 Page 2 of 25
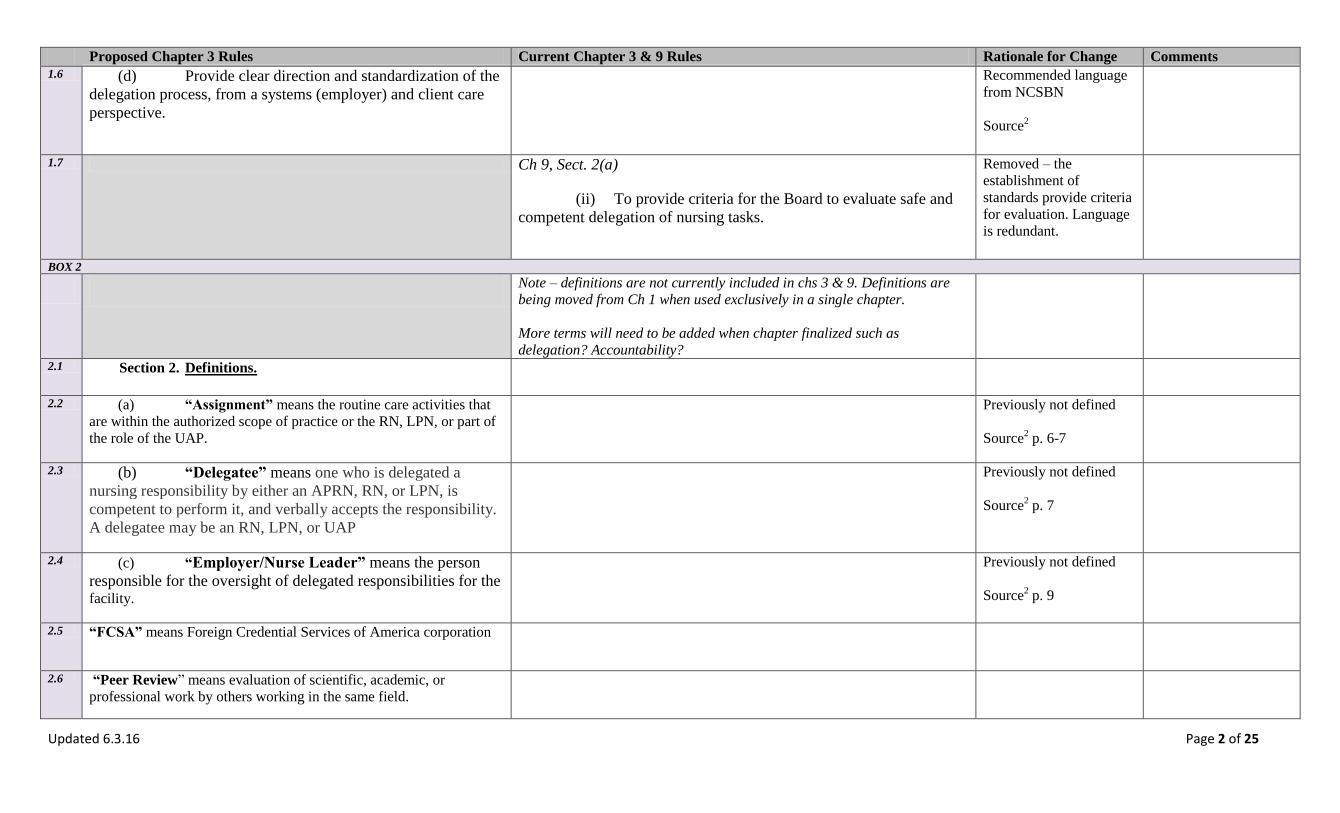
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
1.6 (d) Provide clear direction and standardization of the
delegation process, from a systems (employer) and client care
perspective.
Recommended language
from NCSBN
Source2
1.7 Ch 9, Sect. 2(a)
(ii) To provide criteria for the Board to evaluate safe and
competent delegation of nursing tasks.
Removed – the
establishment of
standards provide criteria
for evaluation. Language
is redundant.
BOX 2
Note – definitions are not currently included in chs 3 & 9. Definitions are
being moved from Ch 1 when used exclusively in a single chapter.
More terms will need to be added when chapter finalized such as
delegation? Accountability?
2.1 Section 2. Definitions.
2.2 (a) “Assignment” means the routine care activities that
are within the authorized scope of practice or the RN, LPN, or part of
the role of the UAP.
Previously not defined
Source2 p. 6-7
2.3 (b) “Delegatee” means one who is delegated a
nursing responsibility by either an APRN, RN, or LPN, is
competent to perform it, and verbally accepts the responsibility.
A delegatee may be an RN, LPN, or UAP
Previously not defined
Source2 p. 7
2.4 (c) “Employer/Nurse Leader” means the person
responsible for the oversight of delegated responsibilities for the
facility.
Previously not defined
Source2 p. 9
2.5 “FCSA” means Foreign Credential Services of America corporation
2.6 “Peer Review” means evaluation of scientific, academic, or
professional work by others working in the same field.

Updated 6.3.16 Page 3 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments 2.7 (d) “Licensed Nurse” means those holding an active
Wyoming license as an APRN, RN, or LPN.
2.8 (e) “Predictable” means behaving or occurring in a
way that is expected.
2.9 (f) “Scope and Standard”
2.10 (g) “UAP” means unlicensed assistive personnel
trained to function in a supportive role, regardless of title, to
whom a nursing responsibility may be delegated. This includes
but is not limited to CNAs, patient care technicians, CMAs,
certified medication aides, and home health aides.
Previously not defined
Source2 p. 7
2.11 (h) “WCSA”
2.12 (i) “WPA”
BOX 3
3.1 Section 3. Scope and Standards of Nursing Practice for
the APRN.
Unchanged – ch 3
3.2 (a) APRN Scope and Standards.
Unchanged – ch 3
3.3 (i) The APRN is subject at all times to the standards
and scope of practice established by national professional
organizations and/or accrediting agencies representing the
various core, role and population focus areas for APRNs, and
the NPA.
Unchanged – ch 3
3.4 (ii) The Board recognizes APRN core, role and
population focus areas described in the scope of practice
statements for APRNs issued by national professional
Unchanged – ch 3

Updated 6.3.16 Page 4 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
organizations and/or accrediting agencies.
3.5 (iii) Role and population focus of the APRN shall be
declared, and the role and population focus to be utilized shall
be the title(s) granted by nationally recognized professional
organization(s) and/or accrediting agency(ies) or the title(s) of
the role and population focus of nursing practice in which the
APRN has received postgraduate education preparation.
Unchanged – ch 3
3.6 (iv) In order to practice in one of the four roles and in
a defined population, the APRN shall be recognized by the
Board in that particular role with a population focus of advanced
practice nursing.
Unchanged – ch 3
3.7 (b) Prescriptive Authority. Unchanged – ch 3
3.8 (i) The Board may authorize an APRN to prescribe,
order, procure, administer, dispense and furnish over the
counter, legend and controlled substances pursuant to applicable
state and federal laws and within the APRN’s role and
population focus.
Ch 3, Sect. 2(b)
(i) The Board may authorize an APRN to prescribe
medications and devices, within the recognized scope of APRN’s role
and population focus, and in accordance with all applicable state and
federal laws including, but not limited to, the WPA, WCSA, the
FCSA, and their applicable Rules and Regulations.
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 11.5.1
Do WPA, WCSA, etc
all need to be listed?
What about DEA?
3.9 (ii) Authorized prescriptions by an APRN shall: Ch 3, Sect. 2(b)(iii)
Wording unchanged ch
3– relocated for better
comprehension
3.10 (A) Comply with all current and applicable
state and federal laws; and
3.11 (B) Be signed by the APRN with the initials
"APRN" or the initials of the nationally recognized role and
population focus.

Updated 6.3.16 Page 5 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
3.12 (iii) APRNs may receive, sign for, record and
distribute samples to clients. Distribution of drug samples shall
be in accordance with state law and DEA laws, regulations and
guidelines.
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 11.5.2
3.13 (iv) The Board shall transmit to the Board of
Pharmacy a list of all APRNs who have prescriptive authority.
The list shall include:
Ch 3, Sect. 2(b)(ii)
Unchanged – ch 3
3.14 (A) The name of the authorized APRN; Ch 3, Sect. 2(b)(ii)(A-C
Unchanged – ch 3
3.15 (B) The RN license number, role and
population focus of the APRN recognized by the Board; and
Unchanged – ch 3 Does this need to be
changed to APRN
number?
3.16 (C) The effective date of prescriptive
authority authorization.
Unchanged – ch 3
3.17 (v) The Board will notify the Board of Pharmacy
within two working days after termination of or change in the
prescriptive authority of an APRN.
Ch 3, Sect. 2(b)(vi)
Wording unchanged ch
3– relocated for better
comprehension
3.18 (c)
3.19 (i)
3.20 (ii)
3.21 (iii)
3.22 (A)

Updated 6.3.16 Page 6 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
3.23 (B)
3.24 (C) Ch 3, Sect. 2(b)
(iv) Prescriptive authorization will be terminated if the
APRN has:
(A) Prescribed outside the scope of recognized
APRN's role and population focus or for other than therapeutic
purposes;
3.25 (D)
3.26 Ch 3, Sect. 2(b)
(iv) Prescriptive authorization will be terminated if the
APRN has:
(A) Not maintained current recognition as an
APRN;
(C) Not completed four hundred (400) hours of
practice as an APRN within the past two (2) years;
(D) Not documented fifteen (15) contact hours of
pharmacology within the past two (2) years; or
(E) Violated the standards of practice, Board Rules,
or the NPA.
Removed – information
redundant from Ch 2 /8
3.27 (d) Applicability. Ch 3, Sect. 2(c)
Unchanged – ch 3
3.28 (i) The provisions of this chapter are only applicable
to an APRN who is recognized as an APRN, whose
authorization to perform advanced and specialized acts of
nursing practice, advanced nursing and medical diagnosis, and
the administration and prescription of therapeutic and corrective
Updated 6.3.16 Page 7 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
measures comes from educational preparation, national
certification, and recognition to practice in compliance with
Board Rules.
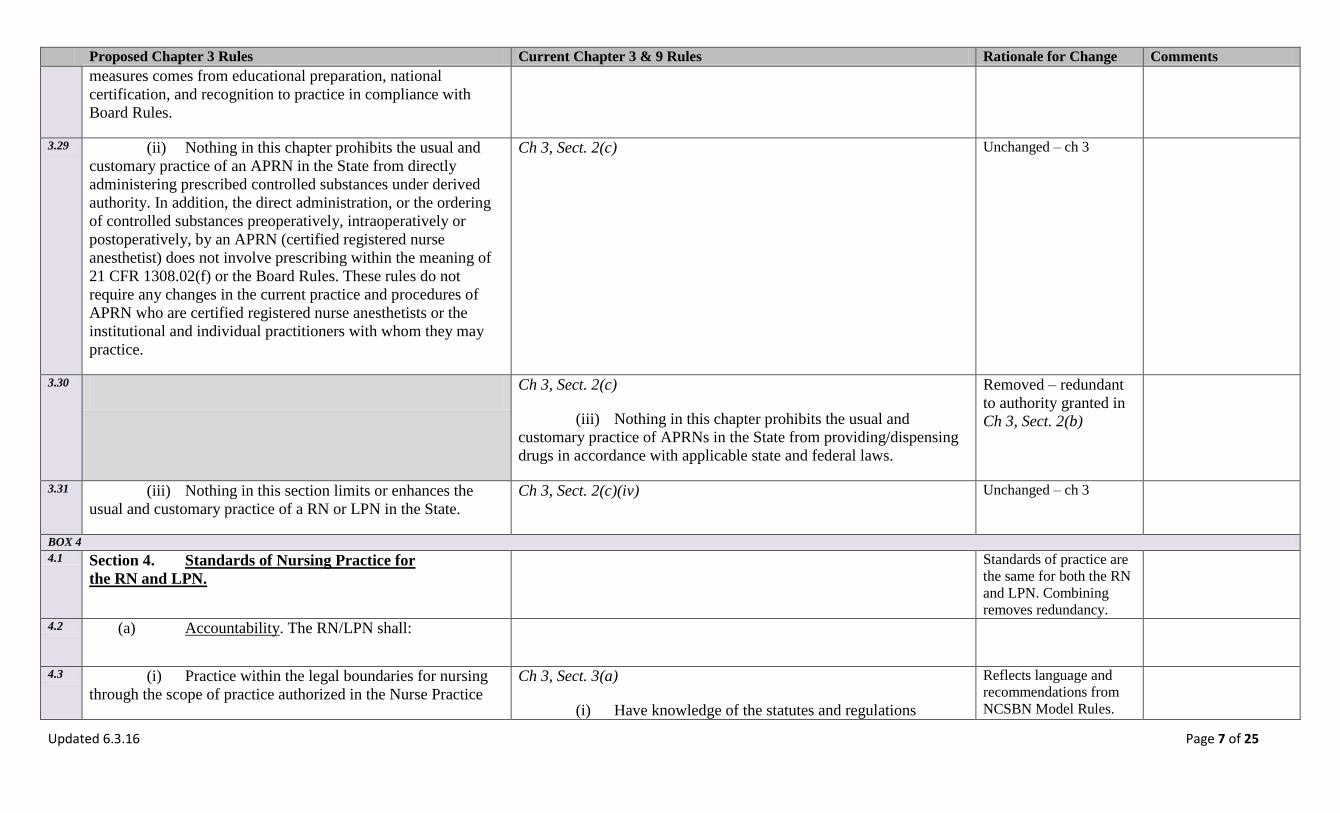
3.29 (ii) Nothing in this chapter prohibits the usual and
customary practice of an APRN in the State from directly
administering prescribed controlled substances under derived
authority. In addition, the direct administration, or the ordering
of controlled substances preoperatively, intraoperatively or
postoperatively, by an APRN (certified registered nurse
anesthetist) does not involve prescribing within the meaning of
21 CFR 1308.02(f) or the Board Rules. These rules do not
require any changes in the current practice and procedures of
APRN who are certified registered nurse anesthetists or the
institutional and individual practitioners with whom they may
practice.
Ch 3, Sect. 2(c)
Unchanged – ch 3
3.30 Ch 3, Sect. 2(c)
(iii) Nothing in this chapter prohibits the usual and
customary practice of APRNs in the State from providing/dispensing
drugs in accordance with applicable state and federal laws.
Removed – redundant
to authority granted in
Ch 3, Sect. 2(b)
3.31 (iii) Nothing in this section limits or enhances the
usual and customary practice of a RN or LPN in the State.
Ch 3, Sect. 2(c)(iv)
Unchanged – ch 3
BOX 4 4.1 Section 4. Standards of Nursing Practice for
the RN and LPN.
Standards of practice are
the same for both the RN
and LPN. Combining
removes redundancy.
4.2 (a) Accountability. The RN/LPN shall:
4.3 (i) Practice within the legal boundaries for nursing
through the scope of practice authorized in the Nurse Practice
Ch 3, Sect. 3(a)
(i) Have knowledge of the statutes and regulations
Reflects language and
recommendations from
NCSBN Model Rules.

Updated 6.3.16 Page 8 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
Act (NPA) and rules governing nursing; governing nursing;
(ii) Practice within the legal boundaries for nursing
through the scope of practice authorized in the NPA and the Board
Rules;
Ch 3, Sect. 4(b)
(i) Have knowledge of the statutes and regulations
governing nursing;
Source3 3.1.1/3.2.1
Removes redundancy by
combining RN/LPN
standards
4.4 (ii) Demonstrate honesty and integrity in nursing
practice;
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.1.1/3.2.1
Removes redundancy by
combining RN/LPN
standards
4.5 (iii) Base nursing decisions on nursing knowledge
and skills, the needs of clients and nursing standards;
Ch 3, Sect. 3(a)
(iv) Base professional decisions on nursing knowledge and
skills, the needs of clients and the expectations delineated in
professional standards;
Ch 3, Sect. 4(a)(ii)
(E) Base nursing decisions on nursing knowledge,
skills, and needs of clients.
4.6 (iv) Accept responsibility for judgments, individual
nursing actions, competence, decisions and behavior in the
course of nursing practice;
Ch 3, Sect. 4(b)
(ii) Accept individual responsibility and accountability for
nursing actions and competency;
4.7 (v) Seek clarification of orders when needed;
4.8 (vi) Maintain competence through ongoing learning
and application of knowledge in nursing practice;
Ch 3, Sect. 3(a)
(v) Maintain continued competence through ongoing
learning and application of knowledge to nursing practice;
Updated 6.3.16 Page 9 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
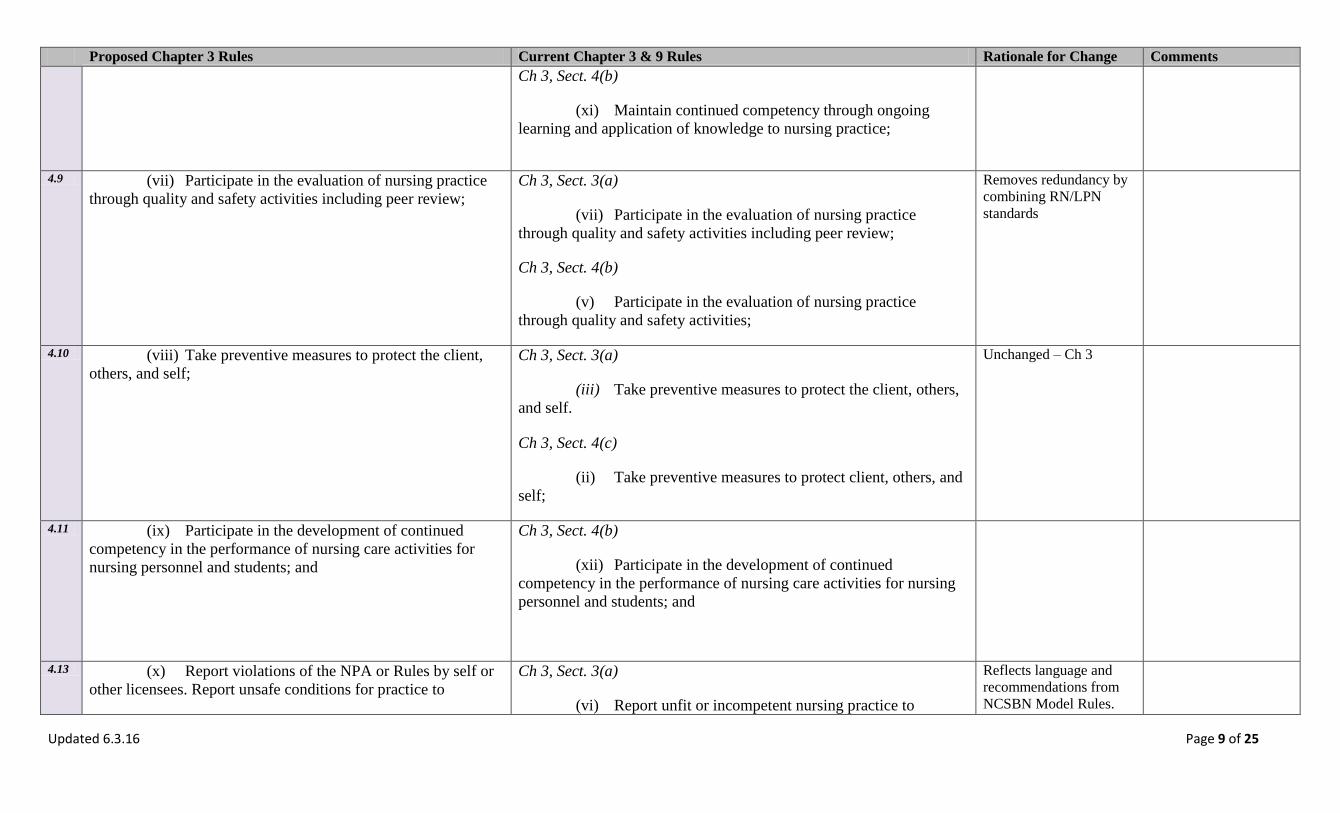
Ch 3, Sect. 4(b)
(xi) Maintain continued competency through ongoing
learning and application of knowledge to nursing practice;
4.9 (vii) Participate in the evaluation of nursing practice
through quality and safety activities including peer review;
Ch 3, Sect. 3(a)
(vii) Participate in the evaluation of nursing practice
through quality and safety activities including peer review;
Ch 3, Sect. 4(b)
(v) Participate in the evaluation of nursing practice
through quality and safety activities;
Removes redundancy by
combining RN/LPN
standards
4.10 (viii) Take preventive measures to protect the client,
others, and self;
Ch 3, Sect. 3(a)
(iii) Take preventive measures to protect the client, others,
and self.
Ch 3, Sect. 4(c)
(ii) Take preventive measures to protect client, others, and
self;
Unchanged – Ch 3
4.11 (ix) Participate in the development of continued
competency in the performance of nursing care activities for
nursing personnel and students; and
Ch 3, Sect. 4(b)
(xii) Participate in the development of continued
competency in the performance of nursing care activities for nursing
personnel and students; and
4.13 (x) Report violations of the NPA or Rules by self or
other licensees. Report unsafe conditions for practice to
Ch 3, Sect. 3(a)
(vi) Report unfit or incompetent nursing practice to
Reflects language and
recommendations from
NCSBN Model Rules.
Updated 6.3.16 Page 10 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
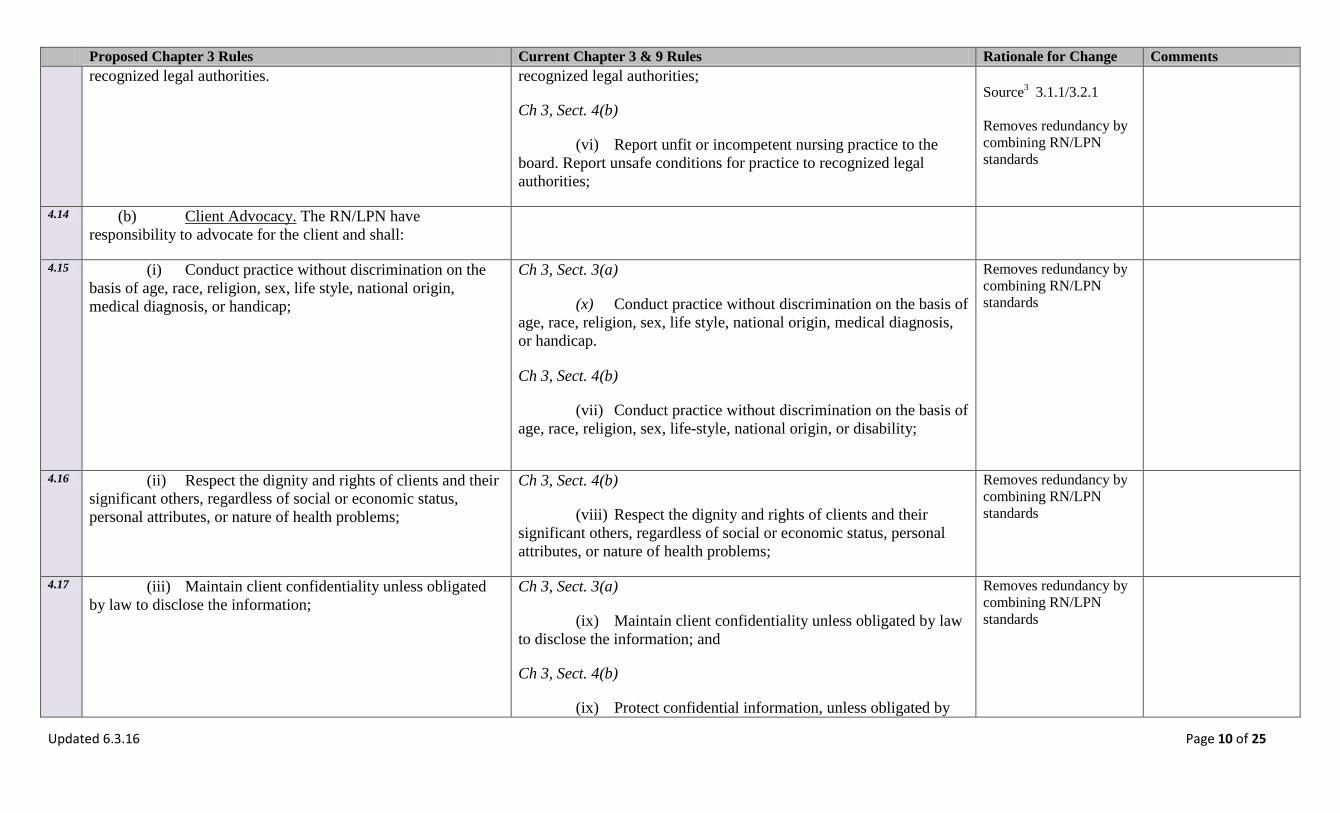
recognized legal authorities. recognized legal authorities;
Ch 3, Sect. 4(b)
(vi) Report unfit or incompetent nursing practice to the
board. Report unsafe conditions for practice to recognized legal
authorities;
Source3 3.1.1/3.2.1
Removes redundancy by
combining RN/LPN
standards
4.14 (b) Client Advocacy. The RN/LPN have
responsibility to advocate for the client and shall:
4.15 (i) Conduct practice without discrimination on the
basis of age, race, religion, sex, life style, national origin,
medical diagnosis, or handicap;
Ch 3, Sect. 3(a)
(x) Conduct practice without discrimination on the basis of
age, race, religion, sex, life style, national origin, medical diagnosis,
or handicap.
Ch 3, Sect. 4(b)
(vii) Conduct practice without discrimination on the basis of
age, race, religion, sex, life-style, national origin, or disability;
Removes redundancy by
combining RN/LPN
standards
4.16 (ii) Respect the dignity and rights of clients and their
significant others, regardless of social or economic status,
personal attributes, or nature of health problems;
Ch 3, Sect. 4(b)
(viii) Respect the dignity and rights of clients and their
significant others, regardless of social or economic status, personal
attributes, or nature of health problems;
Removes redundancy by
combining RN/LPN
standards
4.17 (iii) Maintain client confidentiality unless obligated
by law to disclose the information;
Ch 3, Sect. 3(a)
(ix) Maintain client confidentiality unless obligated by law
to disclose the information; and
Ch 3, Sect. 4(b)
(ix) Protect confidential information, unless obligated by
Removes redundancy by
combining RN/LPN
standards

Updated 6.3.16 Page 11 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
law to disclose the information;
4.18 (iv) Maintain appropriate professional boundaries,
including sexual boundaries;
Ch 3, Sect. 3(a)
(viii) Maintain appropriate professional boundaries,
including sexual boundaries;
Ch 3, Sect. 4(b)
(x) Maintain boundaries, including sexual boundaries;
4.19 (v) Promote a safe and therapeutic environment by: Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.2.4
4.20 (A) Appropriate monitoring and surveillance
of the care environment;
4.21 (B) Identifying unsafe care situations; and
4.22 (C) Correcting problems or referring
problems to appropriate management level when needed.
5.1 Section 5. Scope of Nursing Practice for
the RN.
5.2 (a) RN Standard. The RN has the responsibility to
organize, manage, and supervise the practice of nursing.
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.2.4
5.3 (b) RN Scope of Practice. The RN shall:
5.4 (i) Retain professional accountability for nursing
care;
Ch 3, Sect. 3(a) Unchanged – ch 3
Updated 6.3.16 Page 12 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
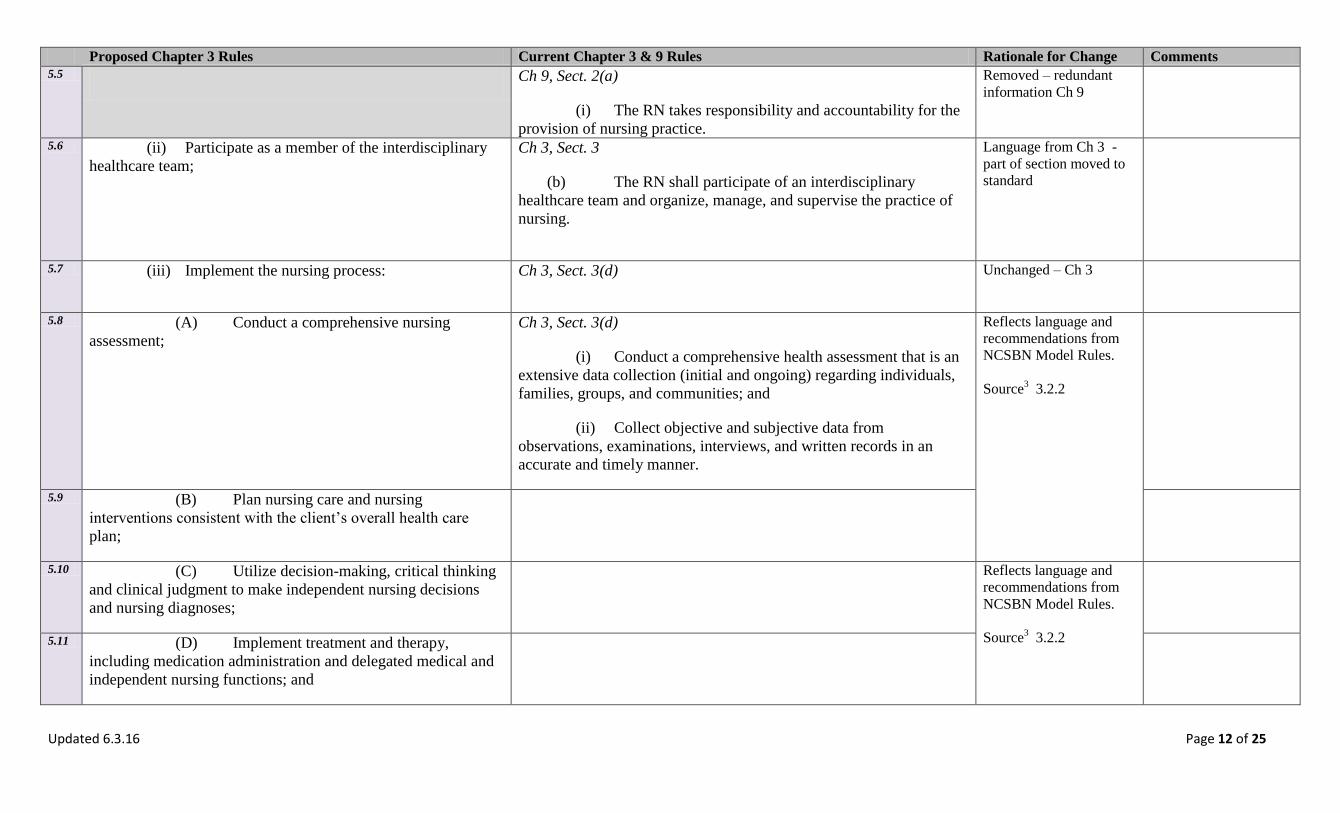
5.5 Ch 9, Sect. 2(a)
(i) The RN takes responsibility and accountability for the
provision of nursing practice.
Removed – redundant
information Ch 9
5.6 (ii) Participate as a member of the interdisciplinary
healthcare team;
Ch 3, Sect. 3
(b) The RN shall participate of an interdisciplinary
healthcare team and organize, manage, and supervise the practice of
nursing.
Language from Ch 3 -
part of section moved to
standard
5.7 (iii) Implement the nursing process: Ch 3, Sect. 3(d)
Unchanged – Ch 3
5.8 (A) Conduct a comprehensive nursing
assessment;
Ch 3, Sect. 3(d)
(i) Conduct a comprehensive health assessment that is an
extensive data collection (initial and ongoing) regarding individuals,
families, groups, and communities; and
(ii) Collect objective and subjective data from
observations, examinations, interviews, and written records in an
accurate and timely manner.
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.2.2
5.9 (B) Plan nursing care and nursing
interventions consistent with the client’s overall health care
plan;
5.10 (C) Utilize decision-making, critical thinking
and clinical judgment to make independent nursing decisions
and nursing diagnoses;
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.2.2
5.11 (D) Implement treatment and therapy,
including medication administration and delegated medical and
independent nursing functions; and
Updated 6.3.16 Page 13 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
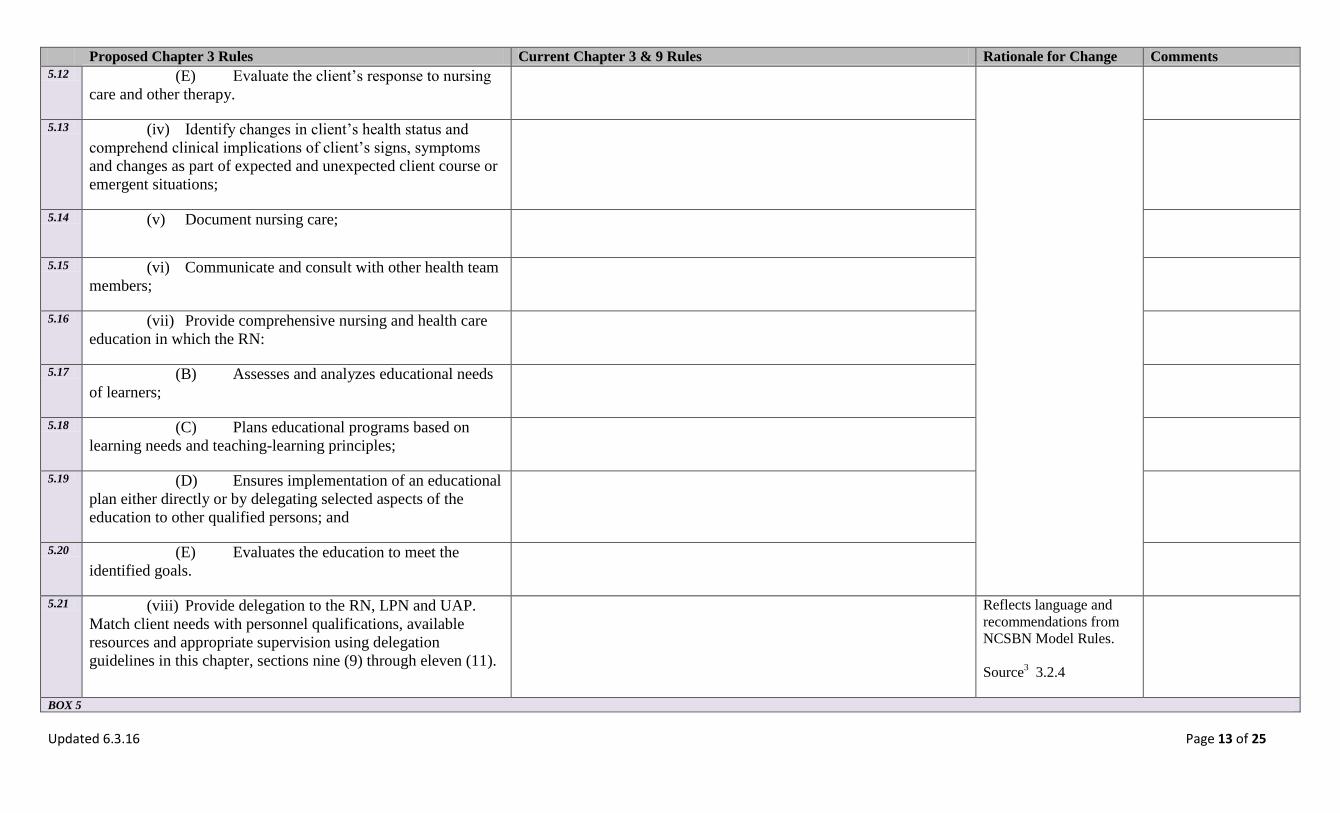
5.12 (E) Evaluate the client’s response to nursing
care and other therapy.
5.13 (iv) Identify changes in client’s health status and
comprehend clinical implications of client’s signs, symptoms
and changes as part of expected and unexpected client course or
emergent situations;
5.14 (v) Document nursing care;
5.15 (vi) Communicate and consult with other health team
members;
5.16 (vii) Provide comprehensive nursing and health care
education in which the RN:
5.17 (B) Assesses and analyzes educational needs
of learners;
5.18 (C) Plans educational programs based on
learning needs and teaching-learning principles;
5.19 (D) Ensures implementation of an educational
plan either directly or by delegating selected aspects of the
education to other qualified persons; and
5.20 (E) Evaluates the education to meet the
identified goals.
5.21 (viii) Provide delegation to the RN, LPN and UAP.
Match client needs with personnel qualifications, available
resources and appropriate supervision using delegation
guidelines in this chapter, sections nine (9) through eleven (11).
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.2.4
BOX 5
Updated 6.3.16 Page 14 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
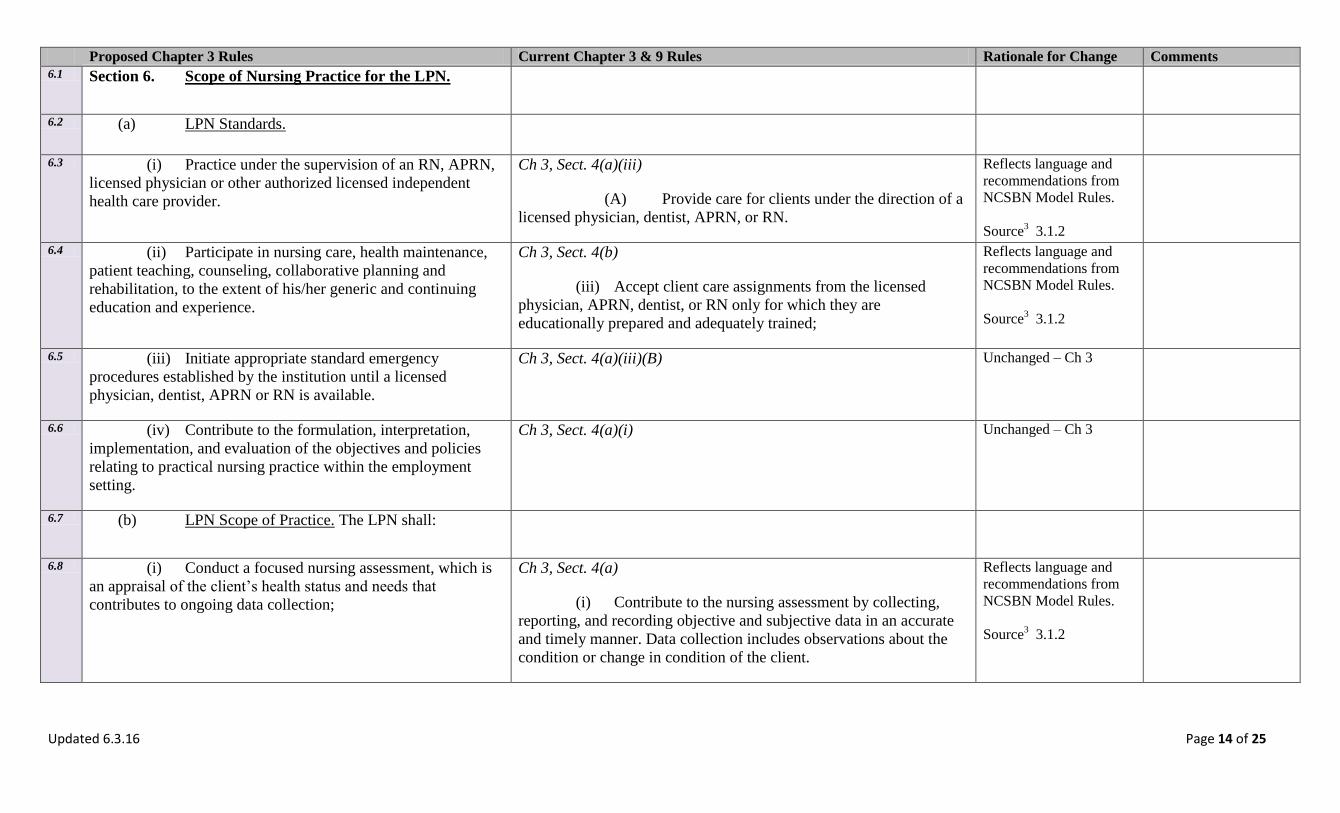
6.1 Section 6. Scope of Nursing Practice for the LPN.
6.2 (a) LPN Standards.
6.3 (i) Practice under the supervision of an RN, APRN,
licensed physician or other authorized licensed independent
health care provider.
Ch 3, Sect. 4(a)(iii)
(A) Provide care for clients under the direction of a
licensed physician, dentist, APRN, or RN.
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.1.2
6.4 (ii) Participate in nursing care, health maintenance,
patient teaching, counseling, collaborative planning and
rehabilitation, to the extent of his/her generic and continuing
education and experience.
Ch 3, Sect. 4(b)
(iii) Accept client care assignments from the licensed
physician, APRN, dentist, or RN only for which they are
educationally prepared and adequately trained;
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.1.2
6.5 (iii) Initiate appropriate standard emergency
procedures established by the institution until a licensed
physician, dentist, APRN or RN is available.
Ch 3, Sect. 4(a)(iii)(B) Unchanged – Ch 3
6.6 (iv) Contribute to the formulation, interpretation,
implementation, and evaluation of the objectives and policies
relating to practical nursing practice within the employment
setting.
Ch 3, Sect. 4(a)(i) Unchanged – Ch 3
6.7 (b) LPN Scope of Practice. The LPN shall:
6.8 (i) Conduct a focused nursing assessment, which is
an appraisal of the client’s health status and needs that
contributes to ongoing data collection;
Ch 3, Sect. 4(a)
(i) Contribute to the nursing assessment by collecting,
reporting, and recording objective and subjective data in an accurate
and timely manner. Data collection includes observations about the
condition or change in condition of the client.
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.1.2
Updated 6.3.16 Page 15 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
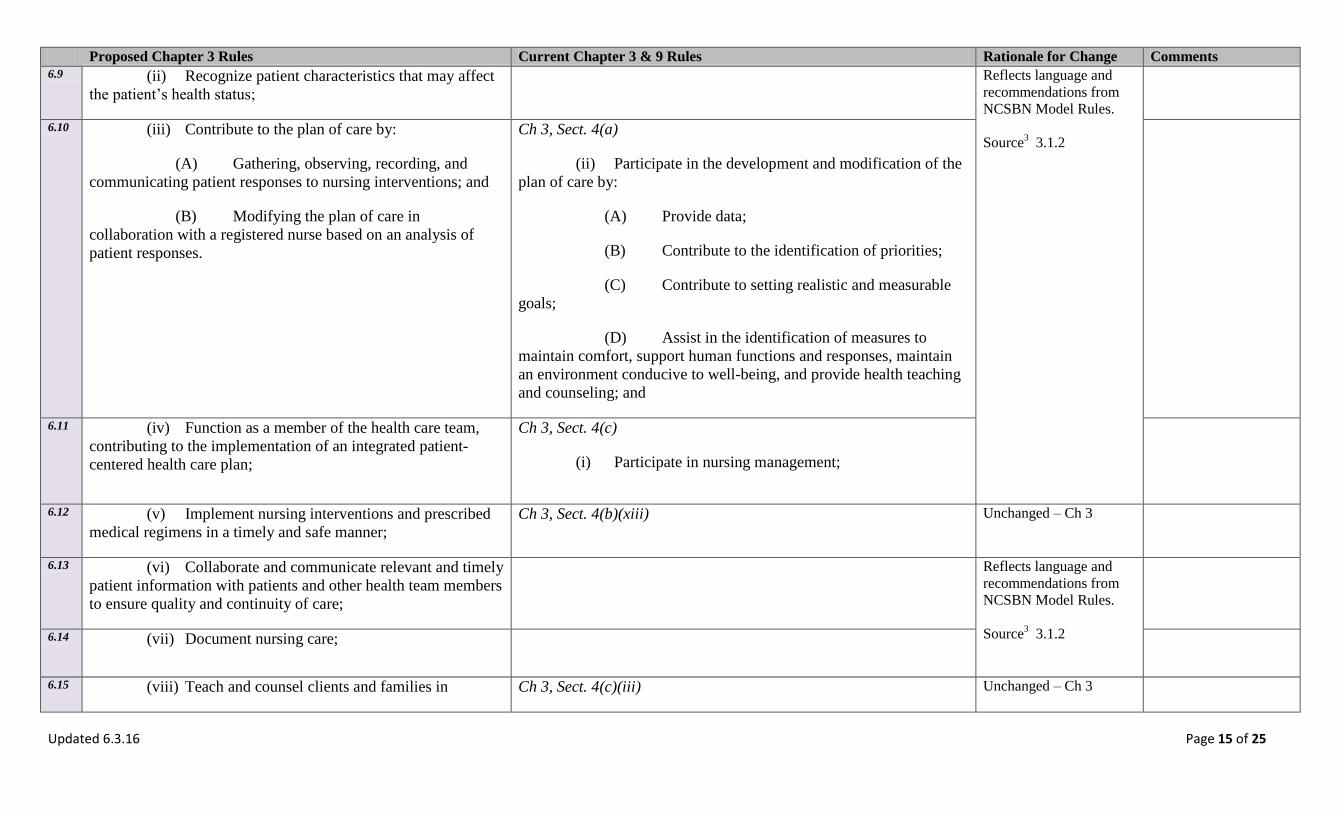
6.9 (ii) Recognize patient characteristics that may affect
the patient’s health status;
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.1.2
6.10 (iii) Contribute to the plan of care by:
(A) Gathering, observing, recording, and
communicating patient responses to nursing interventions; and
(B) Modifying the plan of care in
collaboration with a registered nurse based on an analysis of
patient responses.
Ch 3, Sect. 4(a)
(ii) Participate in the development and modification of the
plan of care by:
(A) Provide data;
(B) Contribute to the identification of priorities;
(C) Contribute to setting realistic and measurable
goals;
(D) Assist in the identification of measures to
maintain comfort, support human functions and responses, maintain
an environment conducive to well-being, and provide health teaching
and counseling; and
6.11 (iv) Function as a member of the health care team,
contributing to the implementation of an integrated patient-
centered health care plan;
Ch 3, Sect. 4(c)
(i) Participate in nursing management;
6.12 (v) Implement nursing interventions and prescribed
medical regimens in a timely and safe manner;
Ch 3, Sect. 4(b)(xiii) Unchanged – Ch 3
6.13 (vi) Collaborate and communicate relevant and timely
patient information with patients and other health team members
to ensure quality and continuity of care;
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.1.2
6.14 (vii) Document nursing care;
6.15 (viii) Teach and counsel clients and families in Ch 3, Sect. 4(c)(iii) Unchanged – Ch 3

Updated 6.3.16 Page 16 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
accordance with the nursing care plan; and
6.16 (ix) Provide delegation to the LPN and UAP. Match
client needs with personnel qualifications, available resources
and appropriate supervision using delegation guidelines in this
chapter, sections nine (9) through eleven (11).
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 3.2.4
BOX 6
7.1 Section 7. Role of CNA.
7.2 (a) Standard. The CNA, regardless of title or care
setting shall be under the direction of an APRN, RN, or LPN.
Ch 3, Sect. 6(a) Unchanged – Ch 3
7.3 Ch 9, Sect. 4
(b) CNA may complement the APRN, RN, or LPN in the
performance of nursing functions but shall not substitute for the
APRN, RN, or LPN.
Removed - outdated and
inaccurate language. It is
not within the CNA role
to substitute for the
licensed nurse.
7.4 (b) CNA Role. After appropriate client assessment
and delegation by the an APRN, RN, or LPN, the CNA shall
utilize knowledge of client’s rights, legal and ethical concepts,
communication skills, safety, and infection control while
performing the following:
(i) Basic Nursing Skills;
(ii) Personal Care Skills;
(iii) Basic Restorative Skills Assistance;
(iv) Mental Health and Psychosocial Skills;
(v) Communication Skills; and
(vi) Nursing Team Member Skills of the CNA.
Ch 3, Sect. 6(b)
Unchanged – Ch 3
BOX 7

Updated 6.3.16 Page 17 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
8.1 Section 8. Expanded Role for LPN IV, MA-C and CNA.
With successful completion of a Board-approved curriculum,
the LPN or CNA may obtain certification which expands the
LPN scope of practice or CNA role.
Ch 3, Sect. 5 Unchanged – Ch 3
BOX 8 9.1 Section 9. Standards of Delegation.
9.2 (a) All decisions related to delegation and
assignment shall be based on the fundamental principles of
protection of the health, safety and welfare of the public.
Ch 9, Sect. 2(a)
(a) All decisions related to delegation and assignments are
based on the fundamental principles of protection of the health, safety
and welfare of the public.
No significant change
9.3 (b) The delegating APRN, RN, or LPN must
delegate only those tasks which are within his/her area of
responsibility and scope of practice;
Ch 9, Sect. 4(e)
(i) The delegating APRN, RN, or LPN must delegate only
those tasks which:
(A) Are within his/her area of responsibility and
scope of practice;
No significant change
9.4 (c) Delegation shall be at the discretion of the
licensed nurse, with consideration of the particular situation.
Ch 9, Sect. 2(a)
(ii) The RN directs care and determines the appropriate
utilization of any CNA involved in providing direct client care.
(iv) The decision of whether or not to delegate or assign is
based upon the RN’s judgment concerning the condition of the
patient, the competence of members of the nursing team and the
degree of supervision that will be required of the RN if a task is
delegated.
Reflects language and
recommendations from
NCSBN National
Delegation Guidelines
Source2 p. 10
9.5 (d) The RN may delegate components of assessment
and care but shall retain responsibility for the nursing process
itself.
Ch 9, Sect. 2(a)
(iii) The RN may delegate components of care but does not
delegate the nursing process itself. The functions of assessment,
planning, evaluation and nursing judgment are pervasive to nursing
Simplified current
language to remove
redundancies.
Updated 6.3.16 Page 18 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
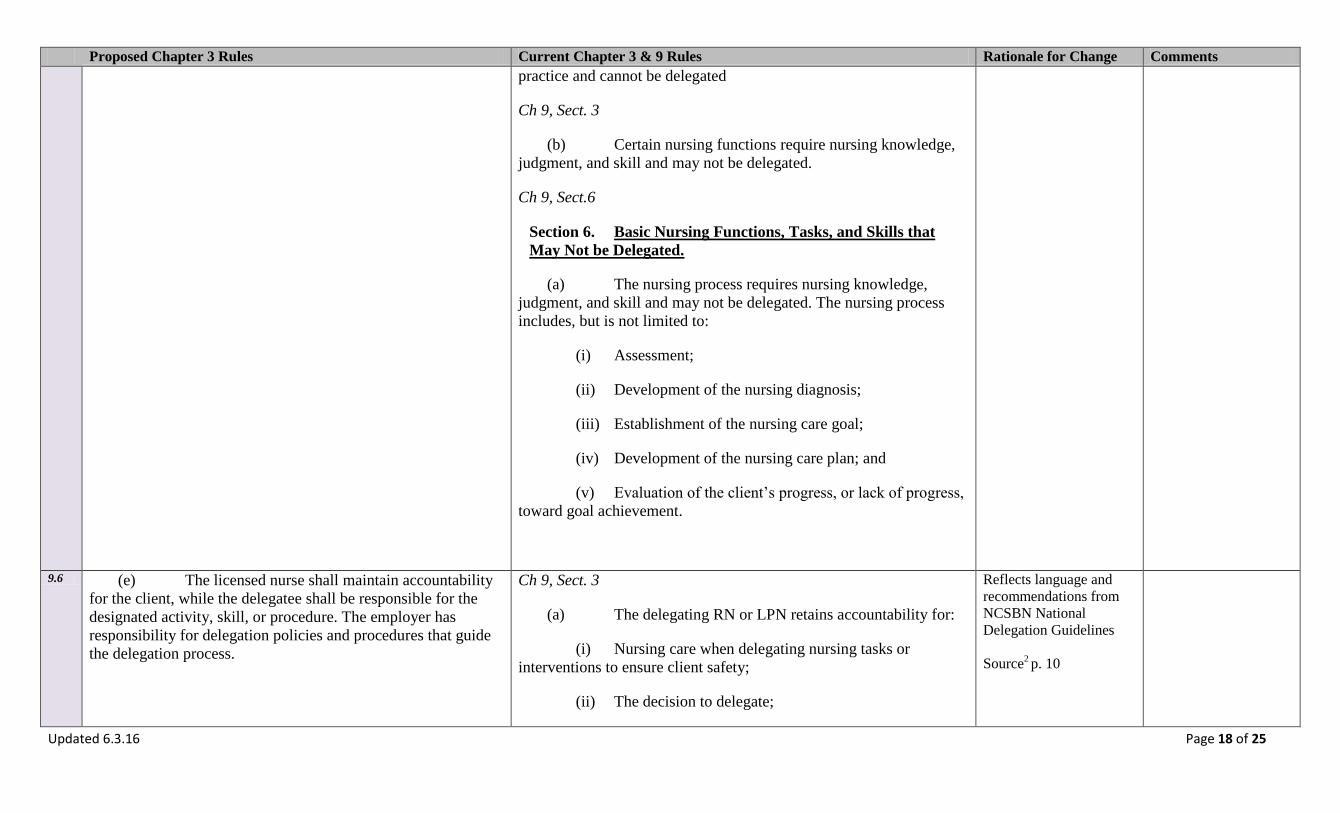
practice and cannot be delegated
Ch 9, Sect. 3
(b) Certain nursing functions require nursing knowledge,
judgment, and skill and may not be delegated.
Ch 9, Sect.6
Section 6. Basic Nursing Functions, Tasks, and Skills that
May Not be Delegated.
(a) The nursing process requires nursing knowledge,
judgment, and skill and may not be delegated. The nursing process
includes, but is not limited to:
(i) Assessment;
(ii) Development of the nursing diagnosis;
(iii) Establishment of the nursing care goal;
(iv) Development of the nursing care plan; and
(v) Evaluation of the client’s progress, or lack of progress,
toward goal achievement.
9.6 (e) The licensed nurse shall maintain accountability
for the client, while the delegatee shall be responsible for the
designated activity, skill, or procedure. The employer has
responsibility for delegation policies and procedures that guide
the delegation process.
Ch 9, Sect. 3
(a) The delegating RN or LPN retains accountability for:
(i) Nursing care when delegating nursing tasks or
interventions to ensure client safety;
(ii) The decision to delegate;
Reflects language and
recommendations from
NCSBN National
Delegation Guidelines
Source2 p. 10

Updated 6.3.16 Page 19 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
(iii) Verifying the delegate’s competency to perform the
tasks;
(iv) Providing direction or supervision;
(v) The performance of the delegated task;
(vi) Evaluating the effectiveness of the delegated nursing
task or interventions performed under direction or supervision.
(Also covered in Section 9 Responsibilities of Delegation and
Assignment)
9.7 (f) It shall be considered assignment rather than
delegation if the particular activity or task is already within the
legally recognized scope of practice or role of the individual.
Ch 9, Sect. 4(e)
(iii) Delegation is unnecessary if the particular activity or
task is already within the legally recognized scope of practice or role
of the individual who is to perform the activity or task;
Change to positive
wording and includes
language of assignment
as suggested by NCSBN.
Source2
9.8 Ch 9, Sect. 2(a)
(vi) The RN individualizes communication regarding
delegation to the CNA and client situation. The communication
should be clear, concise, correct and complete. The RN verifies
comprehension with the CNA and that the CNA accepts the
delegation and the responsibility that accompanies it.
Deleted – describes the
process for delegation.
Moved to Advisory
Opinion
9.9 Ch 9, Sect. 2(a)
(vii) Communication must be a two-way process. CNA
must have the opportunity to ask questions and/or for clarification of
expectations.
Deleted – describes the
process for delegation.
Moved to Advisory
Opinion
9.10 Ch 9, Sect. 2(a)
(viii) The RN uses critical thinking and professional
Deleted – describes the
process for delegation.
Moved to Advisory
Opinion

Updated 6.3.16 Page 20 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
judgment when following the Five Rights of Delegation:
(A) Right task;
(B) Right circumstances;
(C) Right person;
(D) Right directions and communication; and
(E) Right supervision and evaluation.
9.11 (g) Transfer of responsibility of care between
licensed nurses shall be considered a handoff of care rather than
delegation.
Clarification of the
delegation process.
Source2 p. 9
10.1 Section 10. Responsibilities of Delegation and
Assignment. The employer, individual licensed nurse, and
delegatee each shall have specific responsibilities within the
delegation and assignment process.
Reflects language and
recommendations from
NCSBN National
Delegation Guidelines
Source2 p. 9
10.2 (a) Employer Responsibilities. The employer shall: Reflects language and
recommendations from
NCSBN National
Delegation Guidelines
Source2 p. 9
10.3 (i) Identify a nurse leader responsible for oversight
of delegated responsibilities for the facility;
Ch 9, Sect. 2
(b) Chief nursing officers are accountable for establishing
systems to assess, monitor, verify and communicate ongoing
competence requirements in areas related to delegation.
10.4 (ii) Develop policies for delegation; and
10.5 (iii) Assess, monitor and verify competency of staff.
10.6 (b) Licensed Nurse Responsibilities. The licensed
nurse shall:

Updated 6.3.16 Page 21 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
10.7 (i) Direct care and determine appropriate assignment
and delegation in client care;
Ch 9, Sect. 2(a)
(ii) The RN directs care and determines the appropriate
utilization of any CNA involved in providing direct client care.
Simplifying language
10.8 (ii) Assign or delegate to another, those nursing
measures the individual has the education, legal authority and
demonstrated competency to perform safely including:
Ch 9, Sect. 2(a)
(v) The RN delegates only those tasks for which she or he
believes the other health care worker has the knowledge and skill to
perform, taking into consideration training, cultural competence,
experience and facility/agency policies and procedures.
Reflects language and
recommendations from
NCSBN Model Rules and
National Delegation
Guidelines
Source3 3.2.4 (a-b)
Source2 p. 9-10
10.9 (A) The APRN or RN may assign or delegate
nursing care to the RN, LPN or UAP;
10.10 (B) The LPN may assign or delegate nursing
care to the LPN or UAP;
10.11 (iii) Provide direction, guidance, and evaluation for
assignment or delegation;
Ch 9, Sect. 5
Section 5. Degree of Direction or Supervision.
(l) The degree of required direction or supervision for the CNA
shall comply with the following criteria:
(i) Direction or supervision means a licensed nurse
providing appropriate guidance in the accomplishment of a nursing
task, including but not limited to:
(A) Periodic observation and evaluation of the
performance of the task; and
(B) Validation that the task has been performed
according to established standards of practice.
10.12 (iv) Be readily available in person, by
telecommunication, text or other alternative method of
communication; and
Ch 9, Sect. 5(a)
(iii) The delegating APRN, RN, or LPN or another
qualified nurse shall be readily available either in person or by
Simplifying language.
Updating to support
current technology.
Updated 6.3.16 Page 22 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
telecommunication.
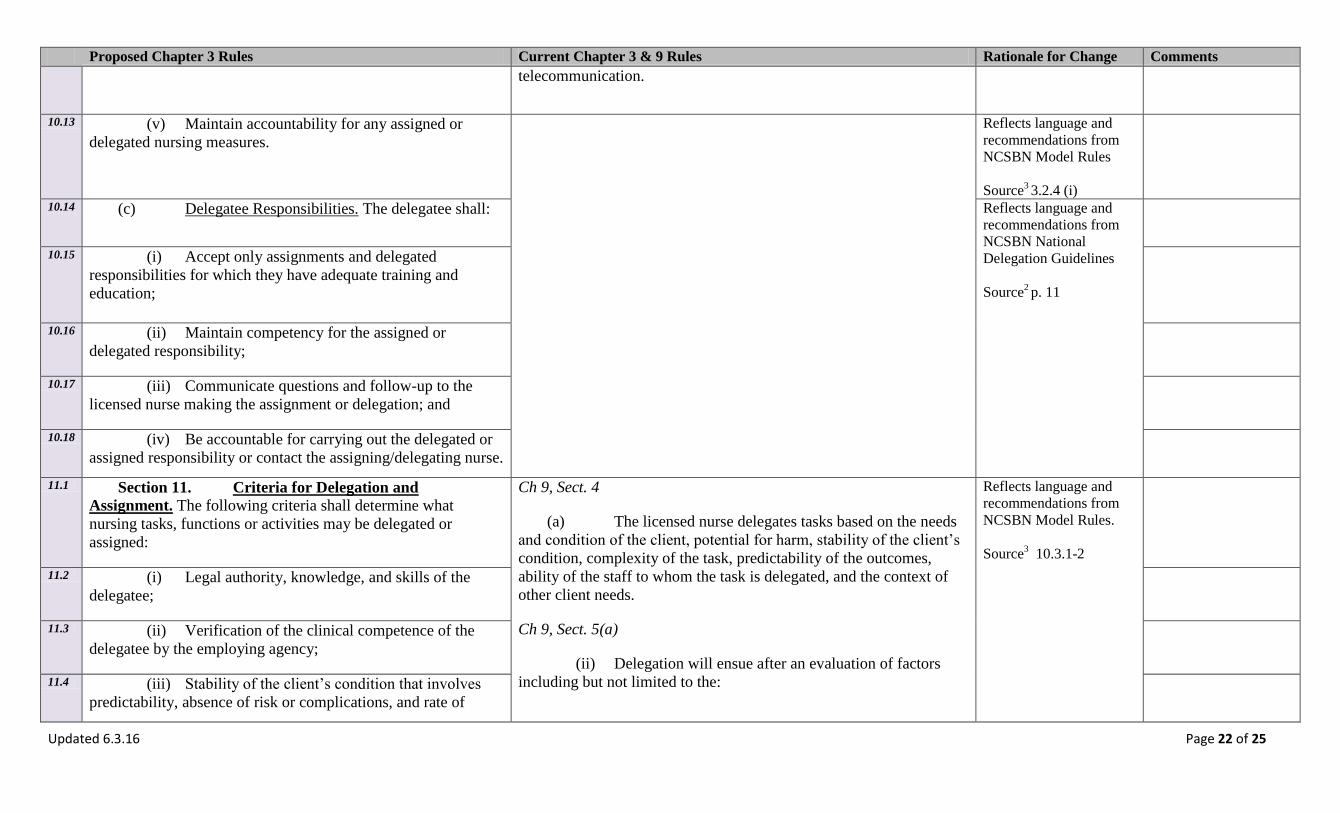
10.13 (v) Maintain accountability for any assigned or
delegated nursing measures.
Reflects language and
recommendations from
NCSBN Model Rules
Source3 3.2.4 (i)
10.14 (c) Delegatee Responsibilities. The delegatee shall: Reflects language and
recommendations from
NCSBN National
Delegation Guidelines
Source2 p. 11
10.15 (i) Accept only assignments and delegated
responsibilities for which they have adequate training and
education;
10.16 (ii) Maintain competency for the assigned or
delegated responsibility;
10.17 (iii) Communicate questions and follow-up to the
licensed nurse making the assignment or delegation; and
10.18 (iv) Be accountable for carrying out the delegated or
assigned responsibility or contact the assigning/delegating nurse.
11.1 Section 11. Criteria for Delegation and
Assignment. The following criteria shall determine what
nursing tasks, functions or activities may be delegated or
assigned:
Ch 9, Sect. 4
(a) The licensed nurse delegates tasks based on the needs
and condition of the client, potential for harm, stability of the client’s
condition, complexity of the task, predictability of the outcomes,
ability of the staff to whom the task is delegated, and the context of
other client needs.
Ch 9, Sect. 5(a)
(ii) Delegation will ensue after an evaluation of factors
including but not limited to the:
Reflects language and
recommendations from
NCSBN Model Rules.
Source3 10.3.1-2
11.2 (i) Legal authority, knowledge, and skills of the
delegatee;
11.3 (ii) Verification of the clinical competence of the
delegatee by the employing agency;
11.4 (iii) Stability of the client’s condition that involves
predictability, absence of risk or complications, and rate of

Updated 6.3.16 Page 23 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
change; and (A) Stability of the client;
(B) Training and capability of the delegate;
(C) Nature of the nursing task being delegated; and
(D) Proximity and availability of the delegator to
the delegate.
11.5 (iv) Variables in the clinical setting including, but not
limited to:
11.6 (A) The accessible resources and established
policies that lend support to the type of nursing tasks, functions ,
and activities being delegated;
11.7 (B) The complexity and frequency of care
needed by a given client population;
11.8 (C) The proximity of the client to staff;
11.9 (D) The number and qualifications of staff;
and
11.10 (E) The accessibility of the licensed nurse.
11.11 Ch 9, Sect. 4
(c) Delegation shall be task-specific, client-specific, and
CNA specific.
(d) The CNA role evolves from the performance of
delegated nursing related tasks and services regardless of an
individual's title or care setting.
(e) Delegation shall be directed by a APRN, RN, or LPN.
Removed – information
is redundant.
11.12 Ch 9, Sect. 4(e)
(i) The delegating APRN, RN, or LPN must delegate only
those tasks which:
Removed – information
is redundant.

Updated 6.3.16 Page 24 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
(B) A reasonable, prudent APRN, RN, or LPN
would find, within his/her sound nursing judgment, appropriate to
delegate;
(C) In the opinion of the APRN, RN, or LPN, shall
be properly and safely performed by the CNA without jeopardizing
the client's welfare;
(D) Does not require the CNA to exercise nursing
judgment, complex observations or nursing assessments, critical
decision making or interventions except in an emergency situation;
and
(E) Are client specific, task specific, and CNA
specific and outcomes are predictable.
11.13 Ch 9, Sect. 4(e)
(ii) When delegating a nursing task, the APRN, RN, or
LPN shall:
(A) Make an initial assessment of the client's
nursing care needs before delegating the task;
(B) Verify the CNA’s competence to perform any
nursing task prior to delegation;
(C) Verify appropriate continuing education for
each CNA for each task to be performed;
(D) Communicate with CNA allowing the
opportunity to ask questions, provide feedback, or clarification;
(E) Inform the client of the decision to delegate;
Reflects the process of
delegation, which
provides suggestions on
how to apply the rules.
This information is
covered in the Advisory
Opinion.
Updated 6.3.16 Page 25 of 25
Proposed Chapter 3 Rules Current Chapter 3 & 9 Rules Rationale for Change Comments
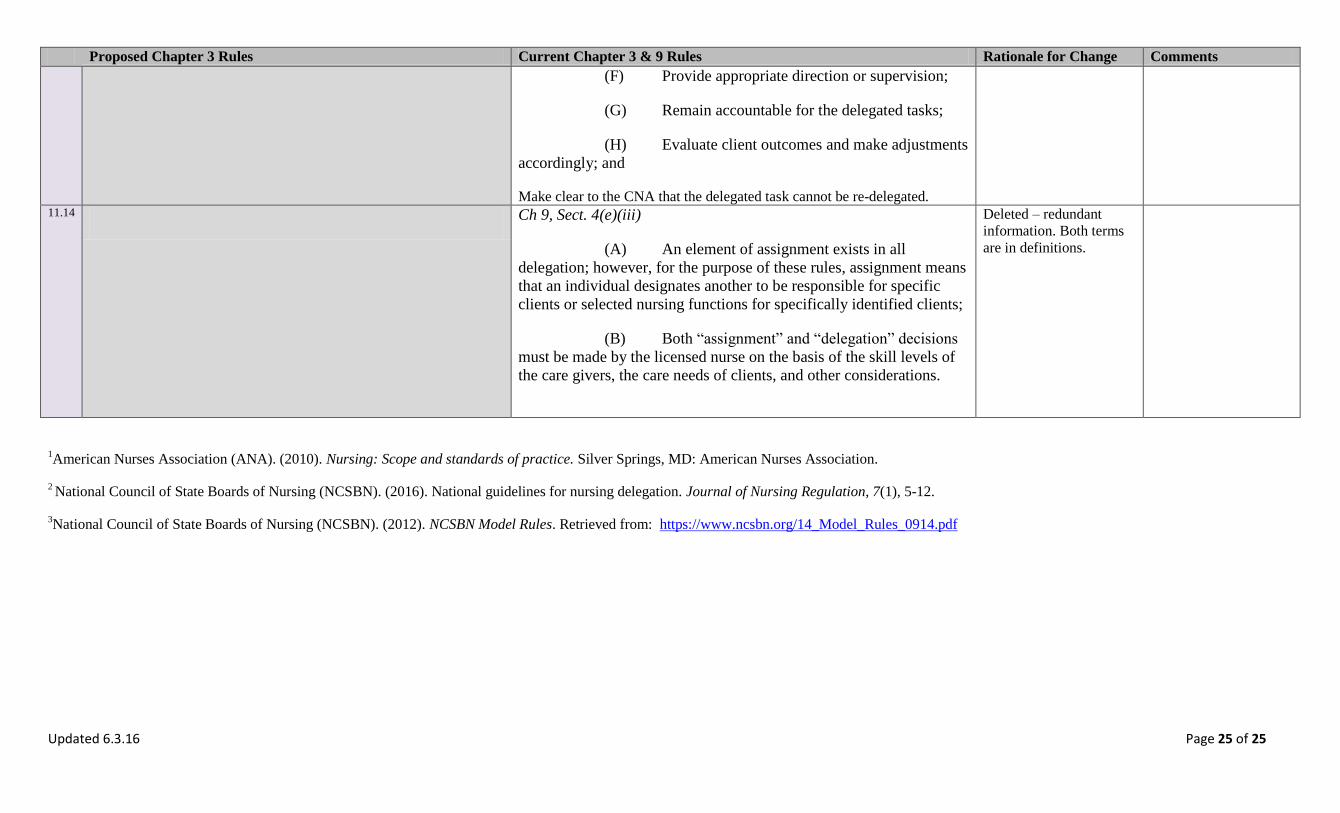
(F) Provide appropriate direction or supervision;
(G) Remain accountable for the delegated tasks;
(H) Evaluate client outcomes and make adjustments
accordingly; and
Make clear to the CNA that the delegated task cannot be re-delegated. 11.14 Ch 9, Sect. 4(e)(iii)
(A) An element of assignment exists in all
delegation; however, for the purpose of these rules, assignment means
that an individual designates another to be responsible for specific
clients or selected nursing functions for specifically identified clients;
(B) Both “assignment” and “delegation” decisions
must be made by the licensed nurse on the basis of the skill levels of
the care givers, the care needs of clients, and other considerations.
Deleted – redundant
information. Both terms
are in definitions.
1American Nurses Association (ANA). (2010). Nursing: Scope and standards of practice. Silver Springs, MD: American Nurses Association.
2 National Council of State Boards of Nursing (NCSBN). (2016). National guidelines for nursing delegation. Journal of Nursing Regulation, 7(1), 5-12.
3National Council of State Boards of Nursing (NCSBN). (2012). NCSBN Model Rules. Retrieved from: https://www.ncsbn.org/14_Model_Rules_0914.pdf
3-1
CHAPTER 3
SCOPE AND STANDARDS OF NURSING PRACTICE AND CNA ROLE.
Section 1. Statement of Purpose. These Board Rules are adopted to implement the
Board’s authority to:
(a) Regulate the scope and practice of nursing for APRN, RN, LPN, and the role of
the CNA;
(b) Provide standards of nursing practice that integrate knowledge, skills, abilities,
and judgment;
(c) Establish acceptable standards of safe delegation of nursing tasks; and
(d) Provide clear direction and standardization of the delegation process, from a
systems (employer) and client care perspective.
Section 2. Definitions.
(a) “Delegatee” means the person who is delegated a nursing responsibility by either
and APRN, RN, or LPN, is competent to perform it, and verbally accepts the responsibility. A
delegate may be either an RN, LPN or UAP.
(b) “Delegation” means the transition of a performance of an activity, skill or
procedure by a licensed nurse to a Delegatee. Pervasive functions of clinical reasoning, nursing
judgment, or critical decision making cannot be delegated.
(c) “Employer/Nurse Leader” means the person responsible for the oversight of
delegated responsibilities for the facility.
(d) “Licensed Nurse” mean those persons holding an active Wyoming license as an
APRN, RN, or LPN.
(e) “UAP” means unlicensed assistive personnel trained to function in a supportive
role, regardless of title, to which a nursing responsibility may be delegated. This includes, but is
not limited to CNAs, patient care technicians, certified medication aides, and home health aides.
Section 3. Scope and Standards of Nursing Practice for the APRN.
(a) Scope and Standards for APRN:
(i) The APRN is subject at all times to the standards and scope of practice
established by national professional organizations and/or accrediting agencies representing the
various core, role and population focus areas for APRNs, and the NPA.

3-2
(ii) The Board recognizes APRN core, role and population focus areas
described in the scope of practice statements for APRNs issued by national professional
organizations and/or accrediting agencies.
(iii) Role and population focus of the APRN shall be declared upon application
for licensure, and the role and population focus to be utilized shall be the title(s) granted by
nationally recognized professional organization(s) and/or accrediting agency(ies) or the title(s) of
the role and population focus of nursing practice in which the APRN has received postgraduate
education preparation.
(iv) In order to practice in one of the four roles and in a defined population, the
APRN shall be recognized by the Board in that particular role with a population focus of
advanced practice nursing.
(b) Prescriptive Authority:
(i) The Board may authorize an APRN to prescribe, order, procure,
administer, dispense and furnish over the counter, legend and controlled substances pursuant to
applicable state and federal laws and within the APRN’s role and population focus.
(ii) Authorized prescriptions by an APRN shall:
(A) Comply with all current applicable state and federal laws; and
(B) Be signed by the APRN with the initials “APRN” or the initials of
the nationally recognized role and population focus.
(iii) APRNs may receive, sign for, record, and distribute samples to clients.
Distribution of drug samples shall be in accordance with state law and Drug Enforcement
Agency laws, regulations, and guidelines.
(iv) The Board shall transmit to the Board of Pharmacy a list of all APRNs
who have prescriptive authority. The list shall include:
(A) The name of the authorized APRN;
(B) The RN license number, role and population focus of the APRN
recognized by the Board; and
(C) The effective date of prescriptive authority authorization.
(v) The Board will notify the Board of Pharmacy within two working days
after termination of or change in the prescriptive authority of an APRN.
(c) Applicability:

3-3
(i) The provisions of this chapter are only applicable to an APRN who is
recognized as an APRN, who is authorized to perform advanced and specialized acts of nursing
practice, advanced nursing and medical diagnosis, and the administration and prescription of
therapeutic and corrective measures comes from educational preparation, national certification,
and recognition to practice in compliance with Board Rules.
(ii) Nothing in this chapter prohibits the usual and customary practice of an
APRN in the State from directly administering prescribed controlled substances under derived
authority. In addition, the direct administration, or the ordering of controlled substances
preoperatively, intraoperatively or postoperatively, by an APRN (certified registered nurse
anesthetist) does not involve prescribing within the meaning of 21 CFR 1308.02(f) or the Board
Rules. These rules do not require any changes in the current practice and procedures of APRN,
who are certified registered nurse anesthetists or the institutional and individual practitioners
with whom they may practice.
(iii) Nothing in this section limits or enhances the usual and customary practice
of an RN or LPN in the State.
Section 4. Scope of Nursing Practice for the RN and the LPN.
(a) Accountability. The RN/LPN shall:
(i) Practice within the legal boundaries for nursing through the scope of
practice authorized in the Nurse Practice Act (NPA) and the Board Rules;
(ii) Demonstrate honesty, integrity and ethical behaviors in nursing practice;
(iii) Base nursing decisions on nursing knowledge, evidence-based practice,
skills, standards, and the needs of the clients;
(iv) Accept responsibility for judgments, individual nursing actions,
competence, decisions and behavior in the course of nursing practice;
(v) Seek clarification of orders or direction when needed;
(vi) Maintain competence through ongoing learning and application of
knowledge in nursing practice;
(vii) Participate in the evaluation of nursing practice through quality and safety
activities, including peer review;
(viii) Take preventative measures to protect the client, others, and self;
(ix) Participate in the development of continued competency in the
performance of nursing care activities for nursing personnel and students; and
3-4
(x) Report violations of the Nurse Practice Act or Rules by self or other
licensees. Report unsafe conditions for practice to recognized legal authorities.
(b) Client Advocacy. The RN/LPN have the responsibility for the client and shall:
(i) Conduct practice without discrimination on the basis of age, race, religion,
sex, life style, national origin, culture, medical diagnosis, or disability;
(ii) Respect the dignity and rights of clients and their significant others,
regardless of social or economic status, personal attributes, culture or nature of health problems;
(iii) Maintain client confidentiality unless obligated by law to disclose the
information;
(iv) Maintain appropriate professional boundaries, including sexual
boundaries;
(v) Promote a safe and therapeutic environment by;
(A) Monitoring and surveillance of the care environment;
(B) Identifying unsafe care situations; and
(C) Correcting problems or referring problems to appropriate
management level when needed.
Section 5. Scope and Standards of Nursing Practice for the RN.
(a) RN Standard. The RN has the responsibility to organize, manage, and supervise
the practice of nursing.
(b) RN Scope of Practice. The RN shall:
(i) Retain professional accountability for nursing care;
(ii) Participate as a member of the inter disciplinary healthcare team;
(iii) Implement the nursing process:
(A) Conduct a comprehensive assessment;
(B) Plan nursing care and nursing interventions consistent with the
client’s overall health care plan;
(C) Utilize decision-making, critical thinking and clinical judgment to

3-5
make independent nursing decisions and nursing diagnosis;
(D) Implement treatment and therapy, including medication
administration and delegated medical and independent nursing functions; and
(E) Evaluate the client’s response to nursing care and other therapy.
(iv) Identify changes in the client’s health status and comprehend clinical
implications of the client’s signs, symptoms and changes as part of expected or unexpected client
course and emergent situations;
(v) Document nursing care;
(vi) Communicate and consult with other health team members;
(vii) Provide comprehensive nursing and health care education in which the
RN:
(A) Assesses and analyzes educational needs of learners;
(B) Plans educational programs based on learning needs and teaching-
learning principles;
(C) Ensures implementation of an educational plan either directly or by
delegating selected aspects of the education to other qualified persons; and
(D) Evaluates the education to meet the identified goals.
(viii) Provide delegation to the RN, LPN, and UAP. Match the client needs with
personnel qualifications, available resources and appropriate supervision using delegation
guidelines in this Chapter, Sections nine (9) through eleven (11).
Section 6. Scope and Standards of Nursing Practice for the LPN.
(a) LPN Standard.
(i) Practice under the supervision of an APRN, RN, licensed physician, or
other authorized licensed independent health care provider.
(ii) Participate in nursing care, health maintenance, patient teaching,
counseling, collaborative planning and rehabilitation, to the extent of his/her generic and
continuing education and experience.
(iii) Initiate appropriate standard emergency procedures established by the
institution until an APRN, RN, licensed physician, or dentist is available.

3-6
(iv) Contribute to the formulation, interpretation, implementation and
evaluation of the objectives and policies relating to practical nursing practice within the
employment setting.
(b) LPN Scope of Practice. The LPN shall:
(i) Conduct a focused nursing assessment, which is an appraisal of the
client’s health status and needs that contributes to ongoing data collection;
(ii) Recognize patient characteristics that may affect the patient’s health
status;
(iii) Contribute to the plan of care by:
(A) Gathering, observing, recording, and communicating patient
responses to nursing interventions; and
(B) Contributing to the plan of care in collaboration with a RN based
on an analysis of patient responses.
(iv) Function as a member of the health care team, contributing to the
implementation of an integrated patient-centered health care plan;
(v) Implement nursing interventions and prescribed medical regimes in a
timely and safe manner;
(vi) Collaborate and communicate relevant and timely patient information with
patients and other health team members to ensure quality and continuity of care;
(vii) Document nursing care;
(viii) Teach and counsel clients and families in accordance with the nursing care
plan; and
(ix) Provide delegation to the UAP. Match client needs with personnel
qualification, available resources and appropriate supervision using delegation guidelines in this
Chapter, Sections nine (9) through eleven (11).
Section 7. Role of the CNA
(a) Standard. The CNA, regardless of title or care setting, shall be under the direction
of an APRN, RN, or LPN.
(b) CNA Role. After appropriate client assessment and delegation by the APRN, RN
or LPN, the CNA shall utilize knowledge of client’s rights, legal and ethical concepts,
communications skills, and safety and infection control practices while performing the
3-7
following:
(i) Basic nursing skills;
(ii) Personal care skills;
(iii) Basic restorative skills;
(iv) Mental health and psychological support;
(v) Communication skills; and
(vi) Nursing team member technical skills of the CNA.
Section 8. Expanded Role for the LPN IV, MA-C and CNA II. With successful
completion of a Board-approved program, the LPN or CNA may obtain certification which
expands the LPN scope of practice or CNA role.
Section 9. Standards of Delegation
(a) All decisions related to delegation and assignment shall be based on the
fundamental principles of protection of the health, safety, welfare of the public and doctrine of
client rights.
(b) The licensed nurse must delegate only those tasks that are within his/her area of
responsibility and scope of practice.
(c) Delegation shall be at the discretion of the licensed nurse, with consideration of
the particular situation.
(d) The RN may delegate components of assessment and care tasks, but shall retain
responsibility for the nursing process itself.
(e) The licensed nurse shall maintain accountability for the client, while the
Delegatee shall be responsible for the designated activity, skill, task, or intervention. The
employer has responsibility for delegation policies and procedures that guide the delegation
process.
(f) It shall be considered assignment rather than delegation if the particular activity or
task is already within the legally recognized scope of practice or role of the individual Delegatee.
(g) Transfer of responsibility of care between licensed nurses shall be considered a
handoff of care rather than delegation.
Section 10. Responsibilities of Delegation and Assignment. The employer,
individual licensed nurse, and Delegatee each shall have specific responsibilities within the
3-8
delegation assignment process.
(a) Employer Responsibilities. The Employer shall:
(i) Identify a nurse leader responsible for oversight of delegated
responsibilities for the facility;
(ii) Develop policies for delegation; and
(iii) Assess, monitor, and verify competency of staff.
(b) Licensed Nurse Responsibilities. The licensed nurse shall:
(i) Direct care and determine appropriate assignment and delegation in client
care;
(ii) Assign or delegate to another, those nursing skills the individual has the
education, legal authority, and demonstrated competency to perform safely including:
(A) The APRN or RN may assign or delegate nursing care to the RN,
LPN, or UAP; and
(B) The LPN may assign or delegate nursing care to the LPN or UAP;
(iii) Provide direction, guidance, and evaluation for assignment or delegation;
(iv) Be readily available in person, by telecommunication, text or other
alternative method of communication; and
(v) Maintain accountability for any assigned or delegated nursing measures.
(c) Delegatee Responsibilities. The Delegatee shall:
(i) Accept only assignments and delegated responsibilities for which they
have adequate training, skills, and education;
(ii) Maintain competency for the assigned or delegated responsibility;
(iii) Communicate questions and concerns to the licensed nurse creating the
assignment or delegation; and
(iv) Be accountable for carrying out the delegated or assigned responsibility or
contact the assigning/delegating nurse.
Section 11. Criteria for Delegation and Assignment. The following criteria shall
determine what nursing tasks, functions, or activities may be delegated or assigned:

3-9
(a) Legal authority, knowledge, skills, and scope of practice of the Delegatee;
(b) Verification of the clinical competence of the Delegatee by the employing
agency;
(c) Stability of the client’s condition that involves predictability, absence of risk or
complications, and rate of change; and
(d) Variables in the clinical setting including, but not limited to:
(i) The accessible resources and established policies that lend support to the
type of nursing tasks, functions, and activities being delegated;
(ii) The complexity and frequency of care by a given client population;
(iii) The proximity of the client to staff;
(iv) The number and qualifications of staff; and
(v) The accessibility of a licensed nurse.
9-1
CHAPTER 9
DELEGATION AND ASSIGNMENT
These rules have been repealed.

3-1
CHAPTER 3
SCOPE AND STANDARDS OF NURSING PRACTICE AND CNA ROLE
Section 1. Statement of Purpose. These Board Rules are adopted to implement the
Board's authority to: regulate the scope and practice of nursing and provide guidance for APRN,
RN, LPN and the role of the CNA.
(a) Regulate the scope and practice of nursing for the APRN, RN, LPN, and the role
of the CNA.
(b) Provide standards of nursing practice that integrate knowledge, skills, abilities
and judgment;
(c) Establish acceptable standards of safe delegation of nursing tasks; and
(d) Provide clear direction and standardization of the delegation process, from a
systems (employer) and client care perspective.
Section 2. Definitions
(a) “Delegatee” means the person who is delegated a nursing responsibility by either
and APRN, RN, or LPN, is competent to perform it, and verbally accepts the responsibility. A
delegate may be either an RN, LPN or UAP.
(b) “Delegation” means the transition of a performance of an activity, skill or
procedure by a licensed nurse to a Delegatee. Pervasive functions of clinical reasoning, nursing
judgment, or critical decision making cannot be delegated.
(c) “Employer/Nurse Leader” means the person responsible for the oversight of
delegated responsibilities for the facility.
(d) “Licensed Nurse” mean those persons holding an active Wyoming license as an
APRN, RN, or LPN.
(e) “UAP” means unlicensed assistive personnel trained to function in a supportive
role, regardless of title, to which a nursing responsibility may be delegated. This includes, but is
not limited to CNAs, patient care technicians, certified medication aides, and home health aides.
Section 23. Scope and Standards of Nursing Practice for the APRN.
(a) Scope and Standards for APRN:
(i) The APRN is subject at all times to the standards and scope of practice
established by national professional organizations and/or accrediting agencies representing the
various core, role and population focus areas for APRNs, and the NPA.

3-2
(ii) The Board recognizes APRN core, role and population focus areas
described in the scope of practice statements for APRNs issued by national professional
organizations and/or accrediting agencies.
(iii) Role and population focus of the APRN shall be declared, and the role and
population focus to be utilized shall be the title(s) granted by nationally recognized professional
organization(s) and/or accrediting agency(ies) or the title(s) of the role and population focus of
nursing practice in which the APRN has received postgraduate education preparation.
(iv) In order to practice in one of the four roles and in a defined population, the
APRN shall be recognized by the Board in that particular role with a population focus of
advanced practice nursing.
(b) Prescriptive Authority:
(i) The Board may authorize an APRN to prescribe medications and devices,
within the recognized scope of APRN’s role and population focus, and in accordance with all
applicable state and federal laws including, but not limited to, the WPA, WCSA, the FCSA, and
their applicable Rules and Regulations. The Board may authorize an APRN to prescribe, order,
procure, administer, dispense and furnish over the counter, legend and controlled substances,
pursuant to applicable state and federal laws and within the APRN’s role and population focus.
(ii) The Board shall transmit to the Board of Pharmacy a list of all APRNs
who have prescriptive authority. The list shall include:
(A) The name of the authorized APRN;
(B) The RN license number, role and population focus of the APRN
recognized by the Board; and
(C) The effective date of prescriptive authority authorization.
(iii) (ii) Authorized prescriptions by an APRN shall:
(A) Comply with all current and applicable state and federal laws; and
(B) Be signed by the APRN with the initials “APRN” or the initials of
the nationally recognized role and population focus.
(iii) APRNs may receive, sign for, record, and distribute samples to clients.
Distribution of drug samples shall be in accordance with state law and Drug Enforcement
Agency laws, regulations, and guidelines.
(iv) The Board shall transmit to the Board of Pharmacy a list of all APRNs
who have prescriptive authority. The list shall include:
3-3
(A) The name of the authorized APRN;
(B) The RN license number, role and population focus of the APRN
recognized by the Board; and
(C) The effective date of prescriptive authority authorization.
(iv) Prescriptive authorization will be terminated if the APRN has:
(A) Not maintained current recognition as an APRN;
(B) Prescribed outside the scope of recognized APRN's role and
population focus or for other than therapeutic purposes;
(C) Not completed four hundred (400) hours of practice as an APRN
within the past two (2) years;
(D) Not documented fifteen (15) contact hours of pharmacology within
the past two (2) years; or
(E) Violated the standards of practice, Board Rules, or the NPA.
(v) APRN’s prescriptive authority shall be renewed biennially.
(vi)(v) The Board will notify the Board of Pharmacy within two working days
after termination of or change in the prescriptive authority of an APRN.
(c) Applicability:
(i) The provisions of this chapter are only applicable to an APRN who is
recognized as an APRN, whose authorization who is authorized to perform advanced and
specialized acts of nursing practice, advanced nursing and medical diagnosis, and the
administration and prescription of therapeutic and corrective measures comes from educational
preparation, national certification, and recognition to practice in compliance with Board Rules.
(ii) Nothing in this chapter prohibits the usual and customary practice of an
APRN in the State from directly administering prescribed controlled substances under derived
authority. In addition, the direct administration, or the ordering of controlled substances
preoperatively, intraoperatively or postoperatively, by an APRN (certified registered nurse
anesthetist) does not involve prescribing within the meaning of 21 CFR 1308.02(f) or the Board
Rules. These rules do not require any changes in the current practice and procedures of APRN
who are certified registered nurse anesthetists or the institutional and individual practitioners
with whom they may practice.
(iii) Nothing in this chapter prohibits the usual and customary practice of
APRNs in the State from providing/dispensing drugs in accordance with applicable state and
3-4
federal laws.
(iv)(iii) Nothing in this section limits or enhances the usual and customary
practice of an RN or LPN in the State.
Section 34. Scope and Standards of Nursing Practice for the RN and the LPN.
(a) Accountability. The RN/LPN shall: retain professional accountability for nursing
care:
(i) Have knowledge of the statutes and regulations governing nursing;
(ii)(i) Practice within the legal boundaries for nursing through the scope of
practice authorized in the Nurse Practice Act (NPA) and the Board Rules;
(iii) Take preventive measures to protect the client, others, and self;
(ii) Demonstrate honesty, integrity, and ethical behaviors in nursing practice;
(iv)(iii) Base professional nursing decisions on nursing knowledge and skills, the
needs of clients and the expectations delineated in professional standards, skills, evidence-based
standards and the needs of the clients;
(iv) Accept responsibility for judgments, individual nursing actions,
competence, decisions and behavior in the course of nursing practice;
(v) Seek clarification of orders or directions when needed;
(v)(vi) Maintain continued competence through ongoing learning and application
of knowledge in nursing practice;
(vi) Report unfit or incompetent nursing practice to recognized legal
authorities;
(vii) Participate in the evaluation of nursing practice through quality and safety
activities including peer review;
(viii) Maintain appropriate professional boundaries, including sexual
boundaries;
(ix) Maintain client confidentiality unless obligated by law to disclose the
information; and
(x) Conduct practice without discrimination on the basis of age, race, religion,
sex, life style, national origin, medical diagnosis, or handicap.

3-5
(viii) Take preventative measures to protect the client, others, and self;
(ix) Participate in the development of continued competency in the
performance of nursing care activities for nursing personel and students; and
(x) Report violations of the NPA or Rules by self or other licensees. Report
unsafe condition for practice to recognized legal authorities.
(b) Client Advocacy. The RN/LPN have responsibility to advocate for the client and
shall:
(i) Conduct practice without discrimination on the basis of age, race, religion,
sex, life style, national origin, culture, medical diagnosis, or disability;
(ii) Respect the dignity and rights of clients and their significant others,
regardless of social or economic status, personal attributes, culture or nature of health problems;
(iii) Maintain client confidentiality unless obligated by law to disclose the
information;
(iv) Maintain appropriate professional boundaries, including sexual
boundaries;
(v) Promote a safe and therapeutic environment by:
(A) Monitoring and surveillance of the care environment;
(B) Identifying unsafe care situations; and
(C) Correcting problems or referring problems to appropriate
management level when needs.
(b) The RN shall participate of an interdisciplinary healthcare team and organize,
manage, and supervise the practice of nursing.
(c) The RN shall advocate for the client.
(d) The RN shall implement the nursing process:
(i) Conduct a comprehensive health assessment that is an extensive data
collection (initial and ongoing) regarding individuals, families, groups, and communities; and
(ii) Plan nursing care and nursing interventions consistent with the client’s
overall health care plan;
Section 5. Scope and Standards of Nursing Practice for the RN.
3-6
(a) RN. Standard. The RN has the responsibility to organize, manage, and supervise
the practice of nursing.
(b) RN Scope of Practice. The RN shall:
(i) Retain professional accountability for nursing care;
(ii) Participate as a member of the inter disciplinary healthcare team
(iii) Implement the nursing process:
(A) Concdcut a comprehensive assessment;
(B) Plan nursing care and nursing interventions consistent with the
client’s overall health care plan;
(C) Utilize decision-making, critical thinking and clinical judgment to
make independent nursing decisions and nursing diagnosis;
(D) Implement treatment and therapy, including medication
administration and delegated medical and independent nursing functions; and
(E) Evaluate the client’s response to nursing care and other therapy.
(iv) Identify changes in clients health status and comprehend clinical
implications of client’s sign, symptoms and changes as part of expected or unexpected client
course and emergent situations;
(v) Document nursing care;
(vi) Communicate and consult with other health team members;
(vii) Provide comprehensive nursing and health care education in shich the RN:
(A) Assesses and anlayzes educational needs of learners;
(B) Plans educational programs based on learning needs and teaching-
learning principles;
(C) Ensures implementation of an educational plan either directly or by
delegating selected aspects of the education to other qualified personsl; and
(D) Evaluates the education to meet the identified goals.
(viii) Provide delegation to the RN, LPN, and UAP. Match the client needs with
personnel qualifications, available resources and appropriate supervision using delegation

3-7
guidelines in this chapter, Sections nine (9) through eleven (11).
Section 46. Scope and Standards of Nursing Practice for the LPN.
(a) LPN Standards. related to the LPN's contribution to the nursing process. The LPN
shall:
(i) Practice under the supervision of an APRN, RN, licensed physician, or
other authorized licensed independent health care provider.
(ii) Participate in nursing care, health maintenance, patient teaching,
counseling, collaborative planning and rehabilitation, to the extent of his/her generic and
continuing education and experience.
(iii) Initiate appropriate standard emergency procedures established by the
institution until a licensed physician, dentist, APRN, or RN is available.
(iv) Contribute to the formulation, interpretation, implementation and
evaluation of the objectives and policies relating to practical nursing practice within the
employment setting.
(i) Contribute to the nursing assessment by collecting, reporting, and
recording objective and subjective data in an accurate and timely manner. Data collection
includes observations about the condition or change in condition of the client.
(ii) Participate in the development and modification of the plan of care by:
(A) Provide data;
(B) Contribute to the identification of priorities;
(C) Contribute to setting realistic and measurable goals;
(D) Assist in the identification of measures to maintain comfort,
support human functions and responses, maintain an environment conducive to well-being, and
provide health teaching and counseling; and
(A) Base nursing decisions on nursing knowledge, skills, and needs of
clients.
(iii) Participate in the implementation of the plan of care by:
(A) Provide care for clients under the direction of a licensed physician,
dentist, APRN, or RN.
(B) Initiate appropriate standard emergency procedures established by the

3-8
institution until a licensed physician, dentist, APRN or RN is available.
(b) Accountability. LPN Scope of Practice.The LPN shall:
(i) Conduct a focused nursing assessment, which is an appraisal of th client’s
health status and needs that contributes to ongoing data collection;
(ii) Recognize patient characteristics that may affect the patient’s health
status;
(iii) Contribute to the plan of care by;
(A) Gathering, observing, recording, and communicating patient
responses to nursing interventions; and
(B) Contributing to the plan of care in collaboration with a registered
nurse based on an analysis of patient reponses.
(iv) Function as a member of the health care team, contributing to the
implementation of an integrated patient-centered health care plan;
(v) Impement nursing interventions and prescribed medical regimens in a
timely and safe manner;
(ii) Collaborate and communicate relevant and timely patient information with
patients and other health team members to ensure quality and continuity of care;
(iii) Document nursing care;
(iv) Teach and counsel clients and families in accordance with the nursing care
plan; and
(v) Provide delegation to the LPN and UAP. Match client needs with
personnel qualifications, available resources and appropriate supervision using delegation
guidelines in this chapter and, sections nine (9) through eleven (11).
(i) Have knowledge of the statutes and regulations governing nursing;
(ii) Accept individual responsibility and accountability for nursing actions and
competency;
(iii) Accept client care assignments from the licensed physician, APRN,
dentist, or RN only for which they are educationally prepared and adequately trained;
(iv) Contribute to the formulation, interpretation, implementation, and
evaluation of the objectives and policies relating to practical nursing practice within the

3-9
employment setting;
(v) Participate in the evaluation of nursing practice through quality and safety
activities;
(vi) Report unfit or incompetent nursing practice to the board. Report unsafe
conditions for practice to recognized legal authorities;
(vii) Conduct practice without discrimination on the basis of age, race, religion,
sex, life-style, national origin, or disability;
(viii) Respect the dignity and rights of clients and their significant others,
regardless of social or economic status, personal attributes, or nature of health problems;
(ix) Protect confidential information, unless obligated by law to disclose the
information;
(x) Maintain boundaries, including sexual boundaries;
(xi) Maintain continued competency through ongoing learning and application
of knowledge to nursing practice;
(xii) Participate in the development of continued competency in the
performance of nursing care activities for nursing personnel and students; and
(xiii) Implement appropriate aspects of client care in a timely manner.
(c) Implementation. The LPN shall:
(i) Participate in nursing management;
(ii) Take preventive measures to protect client, others, and self; and
(iii) Teach and counsel clients and families in accordance with the nursing care
plan.
Section 5. Expanded Role for LPN IV, MA-C and CNA II. With successful
completion of a Board-approved curriculum, the LPN or CNA may obtain certification which
expands the LPN scope of practice or CNA role
Section 67. Role of CNA.
(a) Standard. A The CNA, regardless of title or care setting, shall be under the
direction of an APRN, RN, or LPN;
(b) CNA Role. After appropriate client assessment and delegation by the an APRN,

3-10
RN, or LPN, the CNA shall utilize knowledge of client’s rights, legal and ethical concepts,
communication skills, safety, and infection control practices while performing the following:
(i) Basic Nnursing Sskills;
(ii) Personal Ccare Sskills;
(iii) Basic Rrestorative Sskills Assistance;
(iv) Mental Hhealth and Ppsychosocial Sskills;
(v) Communication Sskills; and
(vi) Nursing Tteam Mmember Ttechnical Sskills of the CNA.
Section 8. Expanded Role for LPN IV, MA-C and CNA II. With successful
completion of a Board-approved curriculum, the LPN or CNA may obtain certification which
expands the LPN scope of practice or CNA role.
Section 9. Standards of Delegation
(a) All decision related to delegation and assignment shall be based on the
fundamental principles of protection of the health, safety, welfare of the public and doctrine of
client rights.
(b) The delegating APRN, RN, or LPN must delegate only those tasks which are
within his/her area of responsibility and scope of practice.
(c) Delegation shall be at the discretion of the licensed nurse, with consideration of
the particular situation.
(d) The RN may delegate components of assessment and care tasks, but shall retain
responsibility for the nursing process itself.
(e) The licensed nurse shall maintain accountability for the client, while the
Delegatee shall be responsible for the designated activity, skill, task, or intervention. The
employer has responsibility for delegation policies and procedures that guide the delegation
process.
(f) It shall be considered assignment rather than delegation if the particular activity or
task is already within the legally recognized scope of practice or role of the individual Delegatee.
(g) Transfer of responsibility of care between licensed nurses shall be considered a
handoff of care rather than delegation.
Section 10. Responsibilities of Delegation and Assignment. The employer,
individual licensed nurse, and Delegatee each shall have specific responsibilities within the
delegation assignment process.

3-11
(a) Employer Responsibilities. The Employer shall:
(i) Identify a nurse leader responsible for oversight of delegated
responsibilities for the facility;
(ii) Develop policies for delegation; and
(iii) Assess, monitor and verify competency of staff.
(b) Licensed Nurse Responsibilities. The licensed nurse shall:
(i) Direct care and determine appropriate assignment and delegation in client
care;
(ii) Assign or delegate to another, those nursing skills the individual has the
education, legal authority, and demonstrated competency to perform safely including:
(A) The APRN or RN may assign or delegate nursing care to the RN,
LPN, or UAP;
(B) The LPN may assign or delegate nursing care to the LPN or UAP;
(iii) Provide direction, guidance, and evaluation for assignment or delegation;
(iv) Be readily available in person, by telecommunication, text or other
alternative method of communication; and
(v) Maintain accountability for any assigned or delegated nursing measures.
(c) Delegatee Responsibilities. The Delegatee shall:
(i) Accept only assignments and delegated responsibilities for which they
have adequate training, skills, and education;
(ii) Maintain competency for the assigned or delegated responsibility;
(iii) Communicate questions and concerns to the licensed nurse creating the
assignment or delegation; and
(iv) Be accountable for carrying out the delegated or assigned responsibility or
contact the assigning/delegating nurse.
Section 11. Criteria for Delegation and Assignment. The following criteria shall
determine what nursing tasks, functions, or activities may be delegated or assigned:
(a) Legal authority, knowledge, skills, and scope of practice of the Delegatee;
(b) Verification of the clinical competence of the Delegatee by the employing
agency;

3-12
(c) Stability of the client’s condition that involves predictability, absence of risk or
complications, and rate of change; and
(d) Variables in the clinical setting including, but not limited to:
(i) The accessible resources and established policies that lend support to the
type of nursing tasks, functions, and activities being delegated;
(ii) The complexity and frequency of care by a given client population;
(iii) The proximity of the client to staff;
(iv) The number and qualifications of staff; and
(v) The accessibility of a licensed nurse.
9-1
CHAPTER 9
DELEGATION AND ASSIGNMENT
These rules have been repealed.
Section 1. Statement of Purpose.
(a) These Board Rules are adopted to implement the Board’s authority to:
(i) To establish acceptable standards of safe delegation of nursing tasks.
(ii) To provide criteria for the Board to evaluate safe and competent delegation of
nursing tasks.
Section 2. Principles of Delegation.
(a) All decisions related to delegation and assignments are based on the fundamental
principles of protection of the health, safety and welfare of the public.
(i) The RN takes responsibility and accountability for the provision of nursing
practice.
(ii) The RN directs care and determines the appropriate utilization of any CNA
involved in providing direct client care.
(iii) The RN may delegate components of care but does not delegate the nursing
process itself. The functions of assessment, planning, evaluation and nursing judgment are
pervasive to nursing practice and cannot be delegated.
(iv) The decision of whether or not to delegate or assign is based upon the RN’s
judgment concerning the condition of the patient, the competence of members of the nursing
team and the degree of supervision that will be required of the RN if a task is delegated.
(v) The RN delegates only those tasks for which she or he believes the other health
care worker has the knowledge and skill to perform, taking into consideration training, cultural
competence, experience and facility/agency policies and procedures.
(vi) The RN individualizes communication regarding delegation to the CNA and
client situation. The communication should be clear, concise, correct and complete. The RN
verifies comprehension with the CNA and that the CNA accepts the delegation and the
responsibility that accompanies it.
(vii) Communication must be a two-way process. CNA must have the opportunity to
ask questions and/or for clarification of expectations.
(viii) The RN uses critical thinking and professional judgment when following the Five
Rights of Delegation:
9-2
(A) Right task;
(B) Right circumstances;
(C) Right person;
(D) Right directions and communication; and
(E) Right supervision and evaluation.
(b) Chief nursing officers are accountable for establishing systems to assess, monitor,
verify and communicate ongoing competence requirements in areas related to delegation.
Section 3. Accountability.
(a) The delegating RN or LPN retains accountability for:
(i) Nursing care when delegating nursing tasks or interventions to ensure client
safety;
(ii) The decision to delegate;
(iii) Verifying the delegate’s competency to perform the tasks;
(iv) Providing direction or supervision;
(v) The performance of the delegated task;
(vi) Evaluating the effectiveness of the delegated nursing task or interventions
performed under direction or supervision.
(b) Certain nursing functions require nursing knowledge, judgment, and skill and may
not be delegated.
Section 4. Standard for Delegation of Basic Nursing Tasks and Skills.
(a) The licensed nurse delegates tasks based on the needs and condition of the client,
potential for harm, stability of the client’s condition, complexity of the task, predictability of the
outcomes, ability of the staff to whom the task is delegated, and the context of other client needs.
(b) CNA may complement the APRN, RN, or LPN in the performance of nursing
functions but shall not substitute for the APRN, RN, or LPN.
(c) Delegation shall be task-specific, client-specific, and CNA specific.
(d) The CNA role evolves from the performance of delegated nursing related tasks
and services regardless of an individual's title or care setting.
(e) Delegation shall be directed by a APRN, RN, or LPN.
9-3
(i) The delegating APRN, RN, or LPN must delegate only those tasks which:
(A) Are within his/her area of responsibility and scope of practice;
(B) A reasonable, prudent APRN, RN, or LPN would find, within his/her
sound nursing judgment, appropriate to delegate;
(C) In the opinion of the APRN, RN, or LPN, shall be properly and safely
performed by the CNA without jeopardizing the client's welfare;
(D) Does not require the CNA to exercise nursing judgment, complex
observations or nursing assessments, critical decision making or interventions except in an
emergency situation; and
(E) Are client specific, task specific, and CNA specific and outcomes are
predictable.
(ii) When delegating a nursing task, the APRN, RN, or LPN shall:
(A) Make an initial assessment of the client's nursing care needs before
delegating the task;
(B) Verify the CNA’s competence to perform any nursing task prior to
delegation;
(C) Verify appropriate continuing education for each CNA for each task to be
performed;
(D) Communicate with CNA allowing the opportunity to ask questions,
provide feedback, or clarification;
(E) Inform the client of the decision to delegate;
(F) Provide appropriate direction or supervision;
(G) Remain accountable for the delegated tasks;
(H) Evaluate client outcomes and make adjustments accordingly; and
(I) Make clear to the CNA that the delegated task cannot be re-delegated.
(iii) Delegation is unnecessary if the particular activity or task is already within the
legally recognized scope of practice or role of the individual who is to perform the activity or
task;
(A) An element of assignment exists in all delegation; however, for the
purpose of these rules, assignment means that an individual designates another to be responsible
for specific clients or selected nursing functions for specifically identified clients;

9-4
(B) Both “assignment” and “delegation” decisions must be made by the
licensed nurse on the basis of the skill levels of the care givers, the care needs of clients, and
other considerations.
Section 5. Degree of Direction or Supervision.
(a) The degree of required direction or supervision for the CNA shall comply with
the following criteria:
(i) Direction or supervision means a licensed nurse providing appropriate guidance in
the accomplishment of a nursing task, including but not limited to:
(A) Periodic observation and evaluation of the performance of the task; and
(B) Validation that the task has been performed according to established
standards of practice.
(ii) Delegation will ensue after an evaluation of factors including but not limited to
the:
(A) Stability of the client;
(B) Training and capability of the delegate;
(C) Nature of the nursing task being delegated; and
(D) Proximity and availability of the delegator to the delegate.
(iii) The delegating APRN, RN, or LPN or another qualified nurse shall be readily
available either in person or by telecommunication.
Section 6. Basic Nursing Functions, Tasks, and Skills that May Not be Delegated.
(a) The nursing process requires nursing knowledge, judgment, and skill and may not
be delegated. The nursing process includes, but is not limited to:
(i) Assessment;
(ii) Development of the nursing diagnosis;
(iii) Establishment of the nursing care goal;
(iv) Development of the nursing care plan; and
(v) Evaluation of the patient’s progress, or lack of progress, toward goal achievement.


















