
The Neuroscience of Critical Thinking Sandra Johnson, Ph.D., MSW, CASAC.
Upload
alejandro-kanito-alvarez-sCategory
view
220download
0
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 1/34
Recent Advances in Critical Care
Medicine: A Case Based ReviewMargaret M. Johnson, MD
Associate Professor of Medicine
Chair, Division of Pulmonary MedicineMayo Clinic Florida

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 2/34
33 year old non-smoking, previously
healthy female
• No prior hospitalizations
• T 38.9 (po)
• RR 22 bpm
• HR 138 bpm• BP 70/40
• Coarse rhonchi bilaterally
• O2 saturation 82%
– Up to 95% on face mask
• Mottled skin
• Anuric
• Lactate 6.2

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 3/34
Overview
• Updated Surviving Sepsis Guidelines – Management of shock
• Fluid resuscitation
• Vasopressor support
• Role of steroids
• Respiratory management
– Intubation
– Ventilator management• High frequency ventilation, prone ventilation
• Management strategies to decrease delirium
• Outcome

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 4/34
SURVIVING SEPSIS GUIDELINES: 2012
Joint collaboration between SSCM and European Respiratory
Society
Third edition
No industry funding used in revision process
Critical Care Medicine February 2013www.survivingsepsis.org
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 5/34
Sepsis: Fluid Resuscitation
• Crystalloid, normally saline, is primary choice
– Initial: 30 ml/kg = 2.1 L for 70 kg
– Subsequent boluses to defined endpoint
– Endpoints:• Normal mixed venous oxygen saturation 65-70%
• Normal lactate
• Urine output > 0.5 ml/kg/hr
• MAP > 65 mm Hg• Weak indication for albumin (Grade 2B)
• Avoid hetastarch with high molecular weight (> 200 kD)

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 6/34
Potential Dangers of Saline
• Saline administration
– Hypertonic relative to blood
– Often causes hyperchloremic metabolic acidosis
• Does it cause renal injury ?• Prospective, sequential, single institution pilot study
• Chloride restrictive v. chloride liberal
– Restrictive
• Lactated solution or plasma-lyte• N = 776 (liberal)
• N = 773 (restrictive)
Nor’azim MY. JAMA 2012; 308(15):1566-1572

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 7/34
Results
• Limiting use of normal saline
– Less acute kidney injury and reduced need for dialysis in
hospital
– No difference in length of stay or mortality – No difference in need for dialysis after hospital discharge
• Current take home
– Uncertain
– Have a reason for giving saline – Probably should consider alternative fluid if large volume
required
Nor’azim MY. JAMA 2012; 308(15):1566-1572
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 8/34
Sepsis:Vasopressors
• Norepinephrine is first choice – Grade 1B
• Epinephrine is an alternative
• Vasopressin can be added to norepinephrine• Dopamine use limited by tachycardia
– NO INDICATION FOR RENAL DOSE
DOPAMINE
• Dobutamine if cardiac dysfunction or
persistent shock despite volume
• Value of Bedside ECHO

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 9/34
Are Steroids Indicated ???
Sigh….Will we ever know
• Current recommendations
– Don’t perform cosotropyn stimulation test to decide need forsteroids
– Consider steroids with persistent shock despite fluids andvasopressors
– Hydrocortisone 200 mg/day
• Boluses or infusion
• Avoid dexamethasone
– Don’t need fludrocortisone if hydrocortisone used
– Wean steroids when off vasopressors
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 10/34
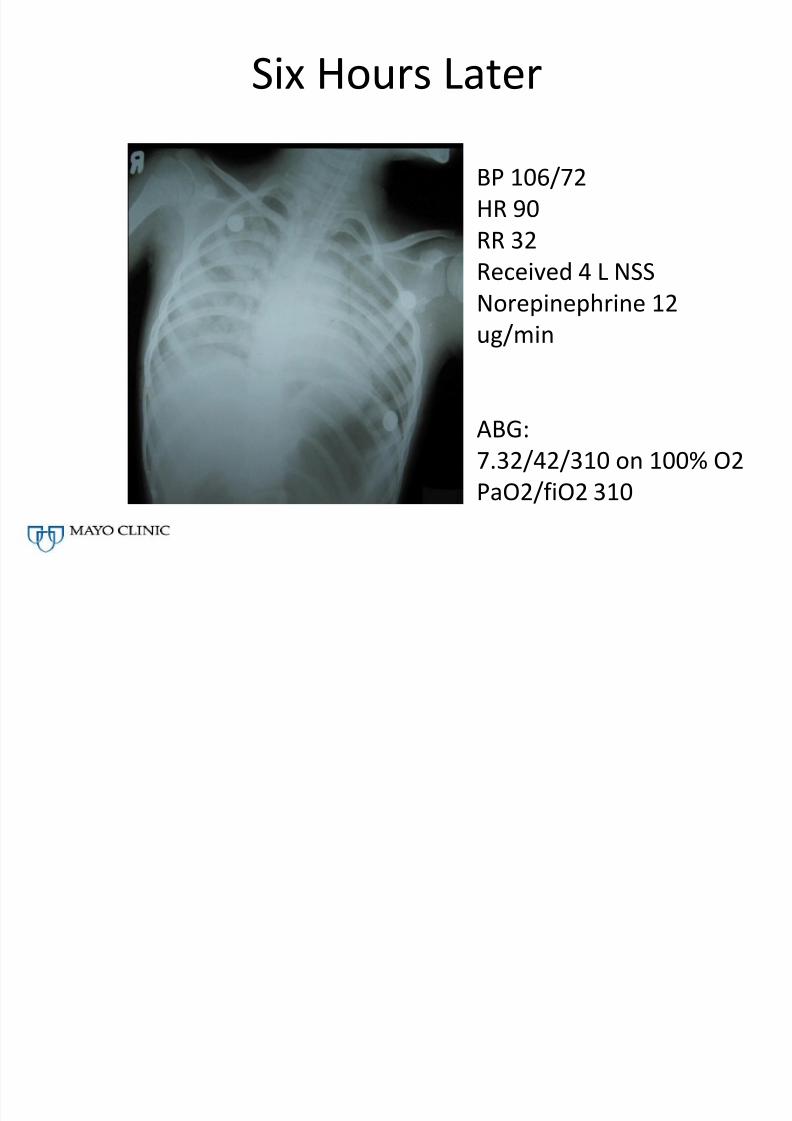
Six Hours Later
BP 106/72
HR 90
RR 32
Received 4 L NSSNorepinephrine 12
ug/min
ABG:
7.32/42/310 on 100% O2
PaO2/fiO2 310

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 11/34
Intubation: Safety of Etomidate
• Meta-analysis: Etomidate associated with
– Increased risk of death
• 865 evaluated for mortality, RR 1.2 (1.02-1.42)
– Increased risk of adrenal insufficiency• 1303 evaluated with cosotropyn stimulation test, RR
1.33 (1.22-1.46)
• Take home
– Causality not concluded, but….alternative should beconsidered, especially in sepsis
Chan CM Crit Care Med 2012 40(11) 2945

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 12/34
Does She Have ARDS ?
New Berlin Definition
• Maintains emphasis on PaO2/fiO2 ratio – < 300 but > 200 = mild – < 200 but > 100 = moderate – < 100 = severe
• Other components – Acute ( < 7 days)
• Difficulty with chronic disease
– Bilateral infiltrates• Either computed tomography or chest x-ray
– No need to exclude heart failure• Heart failure can’t “solely explain respiratory
failure” JAMA 2012; 307 (23):2526

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 13/34
Value of “New Berlin” Definition
• Improved prognostic value:
– PaO2/fiO2 < 300 but > 200 = mild• 27% mortality
– PaO2/fiO2 < 200 but > 100 = moderate• 32% mortality
– PaO2/fiO2 < 100 = severe
• 45% mortality

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 14/34
Lower tidal volumes associated
with decreased mortality
6 cc/kg IBW v. 12 cc/kg
ARDSNet NEJM 2000

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 15/34
Low Tidal Volume Ventilation in
Absence of ARDS
• Meta-analysis of patients WITHOUT ARDS
• Tidal volume
– 6.5 v. 10.6 cc/kg IBW
• Lower tidal volumes associated with:
– Lower chance of developing ARDS
– Decreased pulmonary infection or atelectasis
– Mortality
Neto AS. JAMA 2012; 307 (23):2526

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 16/34
Is High Frequency Ventilation Helpful?
• OSCAR Trial – 795 patients
– Multi-centered in UK
– Identical 30 day mortality (41%)» Young D NEJM 2013;368:806
• OSCILLATE Trial
– High frequency oscillator trial stopped
prematurely due to increased mortality
• 47% v. 35%
» Ferguson N. NEJM 2013

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 17/34
Is Prone Positioning Beneficial ?
• Background
– Prone positioning has previously been shown to
improve oxygenation but not mortality in ARDS
• 237 patients proned v. 229 control
– Severe ARDS PaO2: fiO2 < 150
• Started early
– Within 36 hrs of ARDS
– 16 hrs/session
• 28 day mortality
– 16% (prone) v. 32.8% (control) (p< 0.001)
Guerin C. NEJM 2013;368:2159
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 18/34
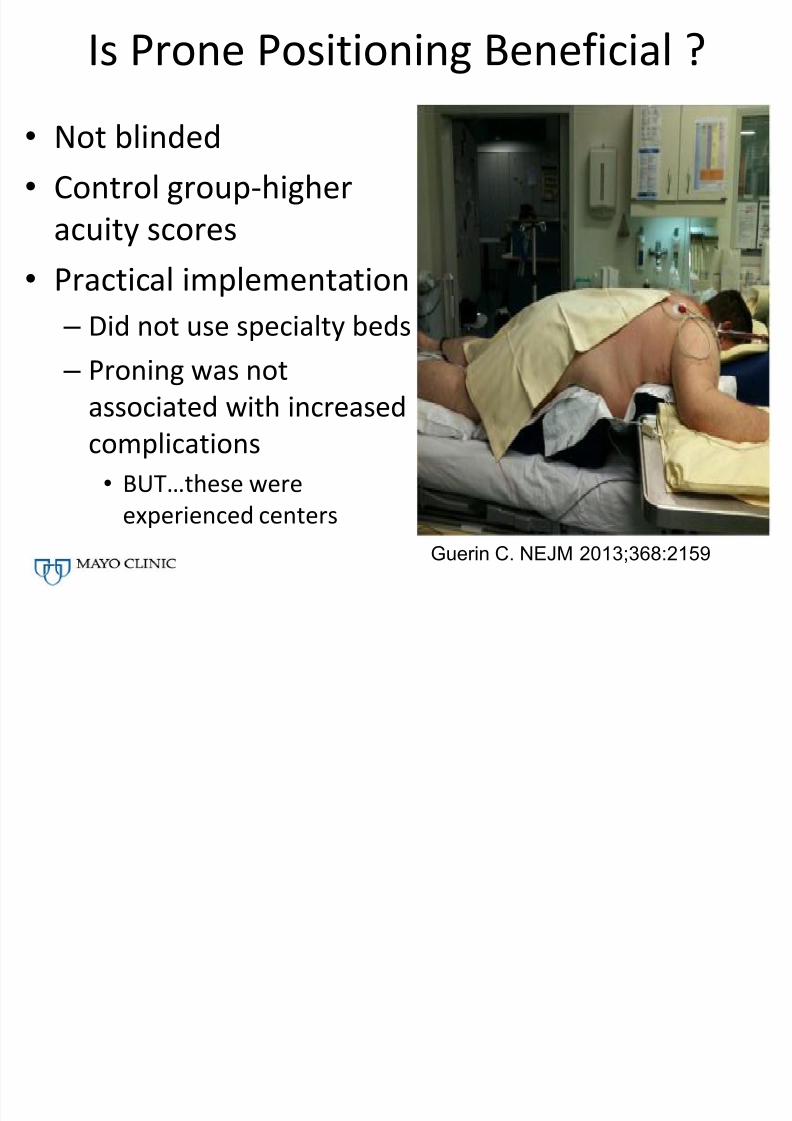
Is Prone Positioning Beneficial ?
• Not blinded• Control group-higher
acuity scores
• Practical implementation – Did not use specialty beds
– Proning was not
associated with increasedcomplications
• BUT…these were
experienced centers
Guerin C. NEJM 2013;368:2159
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 19/34
9 Days Later
• “Agitated and combative”
• Receiving continuous infusions of
lorazepam and fentanyl• Agitation limits weaning attempts
• Is she delirious?
– Assessment of delirium
– Prevention and treatment
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 20/34
ICU Delirium
• Exact incidence is unknown but common – Up to 85% in some series
• Negatively impacts both short and long term
outcomes• Short term
• Length of stay & duration of ventilation
• Mortality
• Long term
• Cognition
• Depression and post traumatic stress disorder
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 21/34
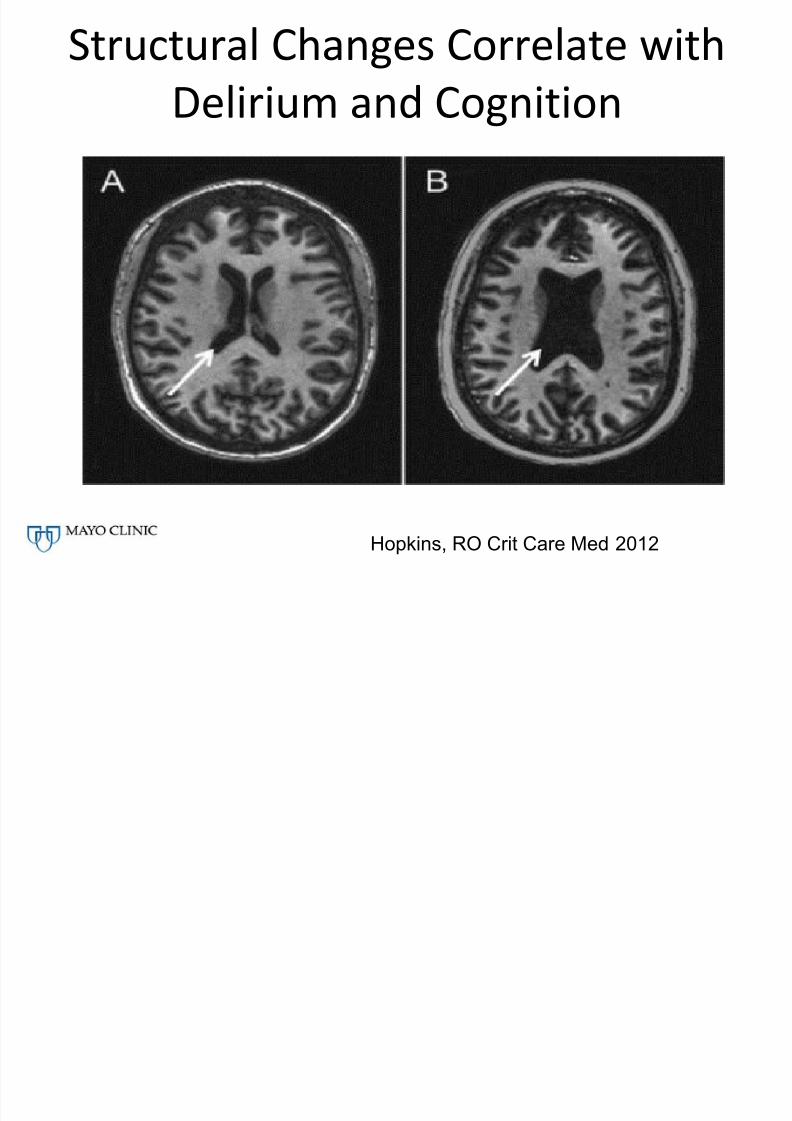
Structural Changes Correlate with
Delirium and Cognition
Hopkins, RO Crit Care Med 2012

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 22/34
Greater Ventricle/Brain Ratio
Correlates with Delirium
Hopkins, RO Crit Care Med 2012

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 23/34
Recognition of Delirium
• Objective tools
– Confusion Assessment Method CAM-ICU
• Performed in conjunction with assessment of level of
sedation (Richmond agitation and sedation score-RASS)• www.icudelirium.org
• May be “hyperactive” or “hypoactive”

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 24/34
Ely EW. 2002
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 25/34
THINK…Rather than prescribe…
• Toxic environments
– Shock, CHF
– “Delirogenic Drugs”
• Hypoxemia
– Consider Haloperidol
• Infection/Immobilization
• Nonpharmacologic interventions/Nutrition
– Eyeglasses, Hearing aides, re-orientation, sleep wake
cycle restoration, sleep hygiene, noise control
• K+ electrolyte abnormalities
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 26/34
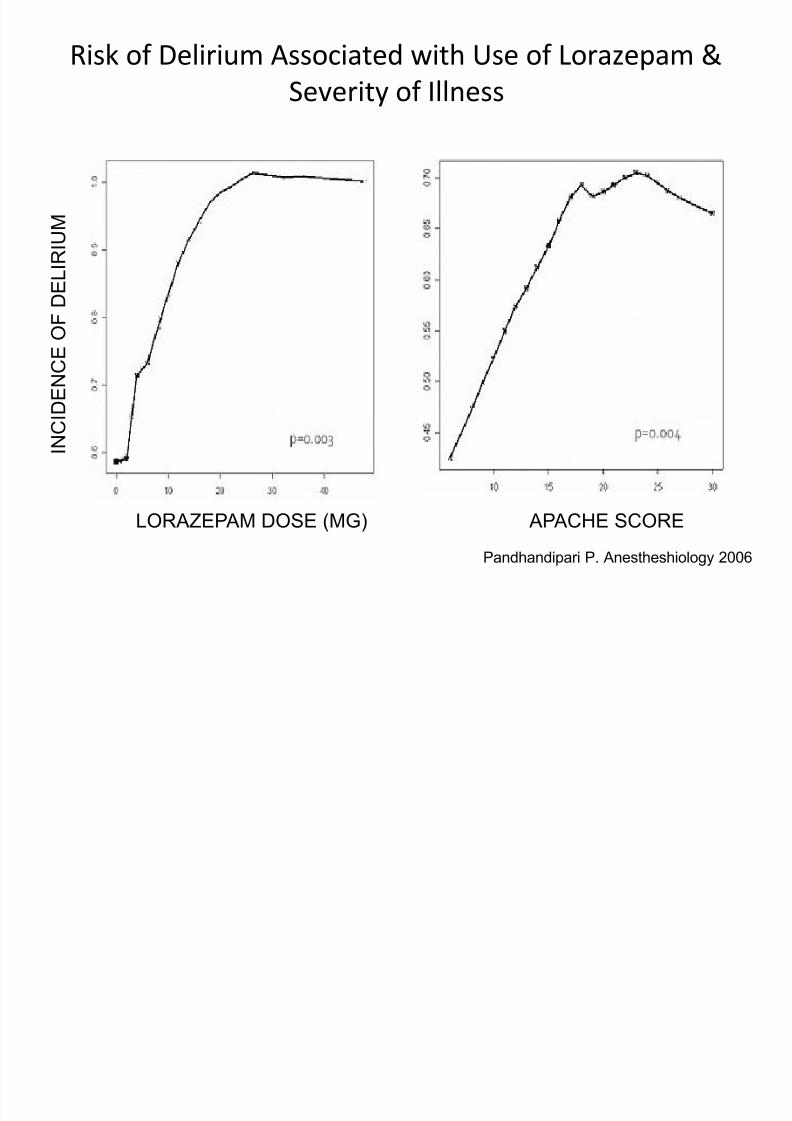
Risk of Delirium Associated with Use of Lorazepam &
Severity of Illness
Pandhandipari P. Anestheshiology 2006
LORAZEPAM DOSE (MG) APACHE SCORE
I N C I D E N C E
O F D E L I R I U M
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 27/34
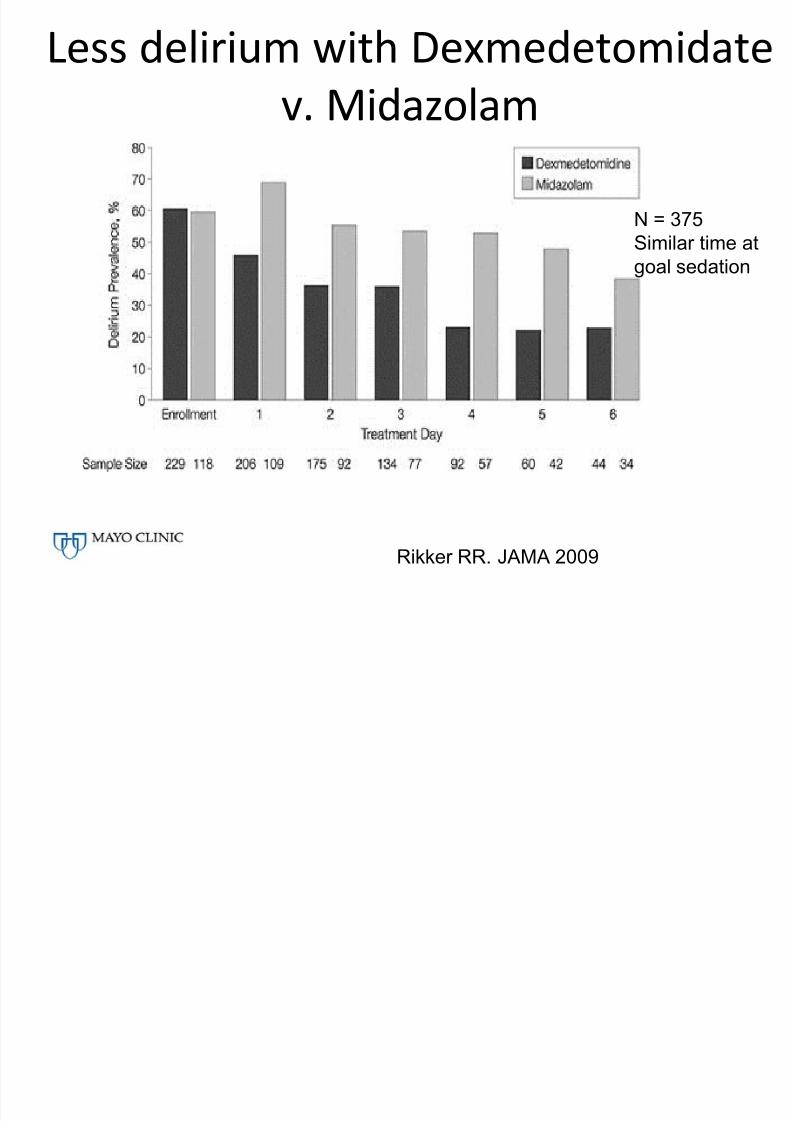
Less delirium with Dexmedetomidate
v. Midazolam
Rikker RR. JAMA 2009
N = 375
Similar time at
goal sedation

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 28/34
Sedation Comparison
• MENDS Trial (n = 106)
– Dexmetomonidine v. lorazepam in mechanically
ventilated
– More days alive without delirium or coma with
dexmetomidine» Pandharipande JAMA 2007
• Reade, et al ( n=20)
– Dexmetomidine v. haldoperidol intubated patientswhose delirium prevented extubation
– Extubation sooner in dexmetomidine group» Crit Care 2009
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 29/34
Sleep, Delirium, and Cognition
• Observational pre and post intervention study
• Daily checklist to improve sleep and maintain
day-night cycles
• 634 (pre) v. 826 (post) patient days
• Subjective ratings of sleep not improved but
less delirium and less noise post intervention
Kamdar BB. Crit Care Med 2013
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 30/34
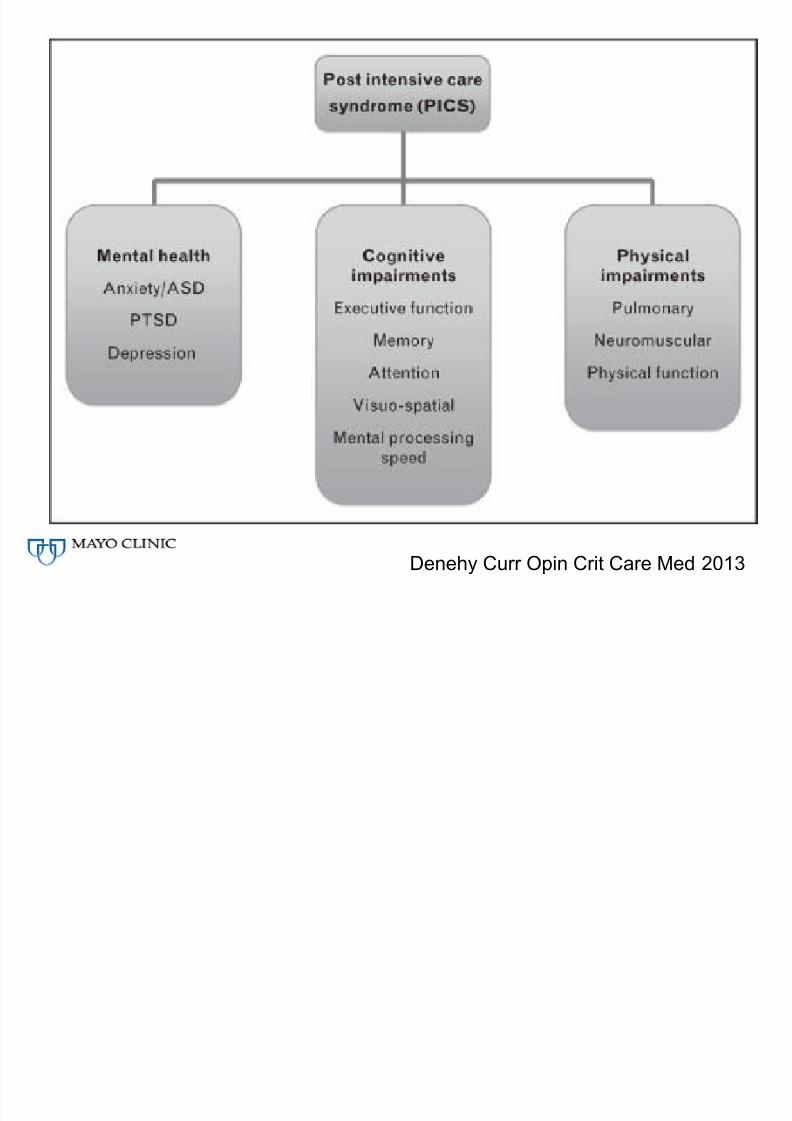
Now What
• Discharged from the ICU on Day 17
• Home on Day 23
• What should she and her family expect?
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 31/34
Denehy Curr Opin Crit Care Med 2013

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 32/34
Ways to Improve Functional Recovery
• In ICU – Limit sedation use and development of delirium
– Utilize early mobility programs, physical, and
occupational therapy
– Try to enhance sleep
• After ICU
– Coordinated post-discharge care including
physical, occupational, and cognitive rehabilitation
– Inform patients and caregivers that functional
limitations' commonly persist
7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 33/34
Take Home Points
• New sepsis guidelines – Fluid 30 cc/kg normal saline
– No renal dose dopamine
– Avoid high molecular weight hetastarch – Norepinephrine (+/- vasopressin)
– No role for cosotropyn stimulation test
– Use hydrocortisone as steroid for stress dose – Chloride rich solutions associated with
development of kidney injury

7/27/2019 1200 - Johnson - Critical Care
http://slidepdf.com/reader/full/1200-johnson-critical-care 34/34
Take Home Points
• Caution with the use of etomidate -especially in sepsis• Low tidal volume ventilation beneficial even in absence of ARDS
• High frequency ventilation has not shown mortality benefit
• Prone positioning associated with improved mortality
• Delirium is common and associated with worsened outcomes – Objectively assess
– ? Avoid/Limit benzodiazepines
– Consider nonpharmacological therapies
• Long term impairments often follow critical illness
– Inform patients and caregivers
– Strategies to improve long term outcomes are ongoing


















